Embed Size (px)
Citation preview

ANAEMIA IN PREGNANCY
Presented ByUnit D Medical
Students

INTRODUCTIONAnemia in pregnancy continues to be a major health problem in many developing countries
It is associated with increased rate of maternal and perinatal mortality, premature delivery, low birth weight and other adverse outcomes
It is the most common pregnancy complication worldwide
» Mohamed K, 2004

DEFINITIONSAnaemia is a condition in which the number of red blood
cells or their oxygen carrying capacity is insufficient to meet
physiologic needs, which vary by age, sex, altitude and
pregnancy status
Anaemia in Pregnancy is defined as hemoglobin
concentration of less than 11g/dl and a hematocrit of less
than 33%
WHO, 2014

DEFINITIONSIn this environment, Hemoglobin concentration is usually less than 10g/dl.

PREVALENCE.
40% of world’s population is said to be anemic
Developed countries 15%Developing countries 33% - 75%Nigeria 30 – 50 %
In a study at University of Nigeria Teaching Hospital Enugu: 40.4% were anemic at booking (90.7% were mild)
Hyacinth .E. Onah 2007

ANAEMIA IN PREGNANCY IN OOUTH
In a study done by our own Lamina and Shorunmu in 2003 of patients who attended antenatal booking at OOUTH
55.3% were found to be anemic
- 88.9% - Mild
- 10.4% - Moderate
- 0.7% - Severe
69% occurred in 2nd trimester
72% fall into the Low socioeconomic class Lamina and Sorunmu
2003

Mortality rates attributed to Anaemia in Pregnancy
Africa 3.9%Asia 12.8%Latin America 0.1%
In Nigeria it accounts for 11% of Maternal mortality rates
WHO, 2006

WHY IS ANAEMIA COMMON IN PREGNANCY?
1. Physiological anaemia of pregnancy– Plasma volume expands by 46-55%
– Red cell mass expands by approx. 33%
2. Increased demand for nutrient– Fetus
– Placenta
– Lactation
3. Increased susceptibility to malaria because of altered immunity in nulliparous
women.
4. Short inter-pregnancy interval.
Also common in: Teenage/ Grand Multiparae/ Multiple pregnancy

CLASSIFICATION Severity PCV %• Mild 25-29• Moderate 20-24• Severe 15-19• Very severe/critical < 14
Morphological Based on RBC size and Hemoglobin content • Hypochromic microcytic e.g. Iron Deficiency Anemia• Macrocytic anaemia e.g. Folate and Vitamin B12 deficiency• Normochromic-Normocytic e.g. Dilutional anaemia of
pregnancy, hemorrhage• Dimorphic - Multifactorial

AETIOLOGY I DECREASED RED CELL PRODUCTION
• Nutritional anaemia – Iron deficiency
- Folate deficiency
• Bone marrow failure – Aplastic anaemia
- pure red cell aplasia
• Associated with systemic diseases (multiple mechanism) -CRF
• Bone marrow infiltration.

AETIOLOGY IIINCREASED RED CELL DESTRUCTION (HAEMOLYTIC
ANAEMIA)
a. Intrinsic abnormality• Haemoglobinopathy: Sickle cell disease/ Thalassemias• Membrane disorder: Ellipsocytosis/spherocytosis• Enzyme deficiency: G6PD /pyruvate kinase
b. Extrinsic abnormality.• Malaria, septicaemia• Antibody mediated :Autoimmune/mismatched transfusion• Chemical or Physical Agents: drugs/Toxins• Hypersplenism.• Immune haemolytic anaemia

AETIOLOGY IIIBLOOD LOSS• Acute blood loss: APH (Abruptio placentae)• Chronic blood loss: Hookworm infestation.
Most common in developing countries.• Nutritional deficiencies – Iron / Folic acid• Malaria• Haemoglobinopathies• Acute Blood loss• Hookworm infestation • HIV

IRON DEFICIENCY ANAEMIAThe commonest type of anaemia in pregnancy worldwide…Nyuke RB,2000
Iron balance in a healthy state involves regulation of intake and loss.
• Loss: intestinal mucosa, lactation, skin, menstruation.
• regulated by: absorption.
• Iron requirement in pregnancy: vary with
– maternal body weight
– size of fetus
– maturity of fetus
• 2.5mg/day in early pregnancy
• 5.5mg/day 20-32wks.
• 6-8mg/day >32wks.

SOURCES OF IRON
Non-haem
Cereals
Vegetable
Seeds
Milk
Egg
Haem
Meat
Viscera (liver, kidney)

CAUSES OF HIGH PREVALENCE OF IRON DEFICIENCY ANAEMIA
• Diet and Dietary habit
• Decrease absorption – worm, tropical sprue, HIV enteropathy,
• Depletion
–multiple pregnancy
-Short inter-pregnancy interval
-excess loss at delivery (no active mgt.)
• GIT blood loss
-Hemorrhoids
-Chronic duodenal ulcer
-Amebiasis

IRON ABSORPTION
Absorption enhancers Absorption inhibitors• Ascorbic acid Phytates• Gastric acidity Tannates• Protein Tea and coffee• Alcohol Calcium • Erythropoietic activites Herbal drinks
– High altitude – Haemolysis– haemorrhage

FOLATE & B12 DEFICIENCY
Folic acid Vitamin B 12
Daily requirement. 50-100µg 3-5µgBody Store 5-10 mg 3-5 mgDepletion 4 months 3-5 years Required in pregnancy
3.0ug
Average daily diet 2.6ug 5-30ug Amount absorbed 1-5ugBody reserves Low highSources Green vegetables,
Fruits, Liver, Kidneymeat/milk, fish, Eggs
Heat lability Easily destroyed Little effectAbsorption Duodenum, jejunum Distal ileum

FOLATE & B12 DEFICIENCYFolic acid
Low intake
• Anorexia, nausea vomiting,
• Goat milk poor in folate
• Malabsorption syndrome, GIT disease.
High demand: pregnancy, hookworm infestation, chronic anaemia
Loss: folate excretion high in pregnancy
Prolonged cooking
Antifolate drugs: Phenytoin Pyrimethamine &Trimethoprinm
Vit B 12
Low intake
Vegetarian
Intrinsic factor lack
• Gastrectomy
• Pernicious anaemia
• Intestinal causes Ileal
diseases & resection
Diphyllobothrium latum

DIAGNOSIS
• History
• Examination
• Investigations

HISTORY• Some may be asymptomatic• Symptoms include: o Easy fatigabilityo Dizzinesso Weaknesso Headacheso Palpitationso Leg swellingo Breathlessnesso Fainting attacks

HISTORYHistory should also covero Dietary habito Duration of symptoms (Acute or Chronic)o Drug and chemical useo Burning sensations in the tongueo Brittle and discoloured fingernailso Fever, urine colouro Occupationo Blood genotype - for Sickle Cell Disease

EXAMINATION• Pallor (Conjunctiva, buccal, palmar, capillary refill)
• Jaundice
• Dehydration (Acute blood loss)
• Enlarged lymph nodes
• Organ enlargement (Spleen, liver)
• Petechial Hemorrhages
• Koilonychia (IDA)
• Glossitis, angular stomatitis
• Signs of anaemic heart failure

INVESTIGATIONSGeneral and Specific
–FBC (PCV, WBC, platelet count)
–Blood Film (M/P & RBC morphology)
–Stool microscopy , occult blood in stool
–Urinalysis & Urine m/c/s
–HB Electrophoresis
–Red cell Indices (MCV, MCH, MCHC)

Red blood cell indices:
INVESTIGATION
Iron deficiency anaemia
Megaloblastic anaemia
Hemoglobin concentration Reduced Reduced
Mean corpuscular volume <80 fL >96 fL
Mean corpuscular hemoglobin 27 pg >33 pg
Mean corpuscular hemoglobin concentration
Low Normal

Megaloblastic anaemia: Blood film showing Oval Macrocytes

Iron Deficiency Anaemia : Blood film showing Microcytic Hypochromic cells

OTHER INVESTIGATIONS• Serum Ferritin <12 = IDA (Normal =15-300µg/L)
– 1st lab test to be deranged in IDA
• Transferrin Saturation <15% = IDA
– Deficient iron supply to the tissues
• Serum Iron<60µg/dl=IDA (N=60-120)
• TIBC>350µg/dl = IDA (N= 300-350)
• Free erythrocyte Protoporphyrin ↑ (FEP)
• Serum transferrin receptors: ↑ in IDA (best indicator)
• Bone marrow stainable iron using potassium ferrocyannate

OTHER INVESTIGATIONS• CXR (with abdominal shield)
• Sputum for AFB
• Renal Function Test
• Reticulocyte count
• Coombs tests
• Red cell folate
• Serum folate
• Bone marrow aspirations

EFFECT OF ANEMIA ON PREGNANCY
ON FETUS
•Neural Tube defects (esp.
folate def.)
•Miscarriage
•IUGR/ Low birth weight
•Prematurity
•Anaemia in infancy
•IUFD
ON MOTHER
•Susceptibility to infection
•Heart decompensation and
Heart failure
•Preterm labour and Preterm
delivery
•Post -partum hemorrhage
•Mental lassitude & Loss of
working hours
•Death

EFFECT OF PREGNANCY ON ANEMIA
Anemia is worsened by pregnancy.

Treatment involves
(I) Treatment of any identifiable cause
(II) Correction of anemia by the most appropriate method depending on:
o Severity of the anemia
o Gestational age
TREATMENT

TREATMENT OF ANY IDENTIFIABLE CAUSEMalaria in Pregnancy:
Quinine is drug of choice in 1st trimester
•Artemisinin based combination therapy is safe
•Oral Artemisinin + SP
•Oral Artemisinin + Amodiaquine
•Quinine + SP
All anaemic patients should receive antimalarial therapy…
Ojengbede O. 1999

URINARY TRACT INFECTIONS
• Pyelonephritis
• Cystitis
• Appropriate antibiotics
• 1st give Intravenously for 48 – 72 hours
Then orally for 10 - 14 days
Repeat Urine culture
Rule out – Persistent or Recurrent Infection

Hookworm Infestation(Helminthiasis)
• Albendazole 400mg statOR
• Mebendazole 100mg bd x 3/7Plus
• Iron supplement Given to all anemic women in the 2nd & 3rd
trimester of pregnancy for better result

(II) CORRECTION OF ANAEMIA
The following are the methods available
for correcting anemia in pregnancy
• Oral Hematinics
• Parenteral iron
• Erythropoietin
• Blood transfusion

ORAL THERAPY
Haematinics• Fersolate 200mg tid• Folic acid 5mg daily

• Various oral preparation exists.
• No scientific evidence that any one brand is
superior to the others
NB: Slow release preparation
- Cause less side effects
- expensive

• For treatment about 120mg of elemental
iron per day is required…WHO, 2014
• Response to the dosage is fast
• Rise in reticulocyte count within 5-10days
• Addition of Folic acid helps in improving
the results

If the treatment is working, Hemoglobin rises by 0.3 to 1g/dl per week
Side Effects of iron preparationsSeen in 10% of women• Nausea• Vomiting• Constipation• Abdominal cramps• Diarrhoea

MANAGEMENT OF SIDE EFFECTS
• Reduce the dose• Use tablets with meals• Give another Fe preparation

DISADVANTAGES OF ORAL IRON
• Intolerance to medication• Unpredictable absorption• Non – compliance• Replenishing Fe stores requires
continuation of Rx for longer period

Parenteral Fe (IRON)• Iron Dextran compound (Imferon) (IV)
• Iron sorbitol citric Acid complex (Jectofer) (IM)• Iron sorbitol citric Acid+ Vit. Bco + Folic Acid
(Jectofer Plus)
NB: there is NO advantage over the oral iron if the oral is well tolerated

INDICATIONS
• Non compliance to oral Fe• Intolerance to oral Fe • Malabsorption syndrome• Slow response to oral Fe• Severe Fe deficiency anaemia.

CALCULATION OF IRON DEFICIT• Elemental Iron needed in mg = (Normal Hb – patients Hb) X Body weight
(kg) x 2.21 + 1000mg (For stores)Simple method• 250mg of Fe for each of Hb below normal
or 5mg/Kg • + another 50% should be given to replenish
iron stores

IRON DEXTRAN COMPOUND (IMFERON)
• Given intravenously in a single dose of not more than:
• 50ml in 1litre of N/S i.e 25ml in 500ml N/S ( 5% Dextrose)
• Given slowly for 10 mins as test dose• Observe for 1-2 hours after infusion.NB: if calculated dose >2500mg of Fe, it should
be given in 2 doses on 2 consecutive days

MODE OF ADMINISTRATION• In hospital setting• No known history of Allergy/Asthma
-Antihistamines-Adrenaline-Hydrocortisone-Oxygen-FLUIDS
+Normal saline+5% dextrose

ADVERSE REACTIONS• Anaphylactic reaction
• Circulatory collapse
• Chest pain
• Chills
• Rigor
• Dyspnoea
• Haemolysis
• Arthralgia
• Myalgia
• Fever
• Thrombophlebitis at the injection site

IRON SORBITOL• Given I.M• More popular/convenient• Associated with less side effects• Stop oral preparation• Total dose needed to replace body iron store
varies from 1g (moderate anaemia) to 2.5g (severe anaemia)
• Total dose = (Normal Hb – patients Hb) x Body wt. (kg) x 3

MODE OF ADMINISTRATION
Deep I.M with a thick needles on the upper outer quadrant using a Z technique to prevent dark staining of the skin
• Test dose of 50mg of Fe sorbitol citrate Followed by 100mg daily or alternate buttocks

DISADVANTAGES• Pain at injection site • Skin discoloration• Abscess formation• GIT irritation• Headache• Fever• Allergic reactions• Lymphadenopathy• Rarely anaphylaxis

RESPONSE TO THERAPY(i) Clinical• Feeling of well being• Improved outlook• Better Appetite
(ii) Hematological
• Reticulocyte response in 5-10 days • Rise in [Hemoglobin] & haematocrit subsequently
(0.3 – 1.0 g/dl per week)

• Diagnostic re-evaluation is needed if there is no clinical or haematological response or improvement within three weeks.
• This could be due to
– Inaccurate diagnosis
– Faulty absorption
– Continuous blood loss
– Co-existing infection
– Concomitant folate deficiency

TREATMENT OF FOLIC ACID DEFICIENCY
• Folic acid 5mg daily• Continue for at least 4/52• Response is indicated by a fall in LDH level
within 3-4days • An increase in reticulocyte count in 3-8 days.• Gastric intolerance• Addition of vitamin C is helpful +Fe.

ERYTHROPOIETIN• Recombinant erythropoietinINDICATIONS• Chronic renal disease • End stage renal disease
- Reduced erythropoietin production - Shortened red cell survival• Jehovah witnesses• Iron deficiency anaemia• Anaemia associated with low erythropoietin levels
– Rheumatoid arthritis– AIDS– Malignancies– Sickle cell Anaemia

Dosage/Administration
• 50-500 iu /kg per week • Route – subcutaneous
• N.B: should be used with iron therapy -300 iu/kg per week + - 200mg of Fe infusion

RESPONSE• Reticulocytosis on day 4
- Hemoglobin rise of 0.7g/dl to 3.0 g/dl within 14 days without any maternal/fetal /neonatal effects

BLOOD TRANSFUSION INDICATIONS• Heart failure (PCV 18%)
• Anaemia coexisting with
– Sepsis
– Haemorrhage
– Renal failure
– Haemoglobinopathy
• Anaemic patients in labour
• Anaemic patient being prepared for surgery

• Blood transfusion is needed to -Improve oxygen delivery to the tissues-Restores cardiac function to normal
NB: - Supplemental oxygen- Physical restrictions- No sedation – (fatal respiratory depression)

• Slow blood transfusion of 1 unit for about 4-6 hrs
• Intravenous diuretics (Frusemide 40mg)N.B: -Hydrocortisone - Antihistamine - Clear instructions - Availability of personnel

ANTENATAL CARE• Routine haematinics to prevent nutritional
anaemia • Adequate nutrition with iron & folate rich local
diets• PCV/Hb surveillance• Genotype determination • Preventive measures against Hookworm• Antihelmithics• Fetal growth monitoring should be done

ANTIMALARIAL CHEMOPROPHYLAXIS
• Intermittent prophylactic therapy with
sulphadoxine/ pyrimethamine from quickening (at least 2 doses spaced 4 weeks apart)• Proguanil 200mg/day
• Insecticide Treated bed Net (ITN)

ANAEMIA IN LABOUR• Danger of maternal mortality due to severe
anemia increase sharply as soon as labour starts.
• Most maternal mortality due to severe anemia takes place during labour and 12hrs after delivery

• High incidence of fetal distress because of under lying maternal tissue hypoxia noticeable when PCV <20%.
Haemorrhage are poorlyOperative delivery toleratedGeneral anaesthesia
• Prophylactic IVFs can cause pulmonary oedema

Emphasis should be on:• Reducing & correcting blood loss• Intermittent oxygen inhalation • Avoidance of episiotomy• Prompt repair of episiotomy• Active management of of 3rd stage of labour with IV
oxytocin is preferredNB: IV Ergometrine may precipitate acute circulatory
overload.- Blood transfusion under diuretic cover

IN THE PUERPERIUM• Adequate rest should be maintained.
• Iron and folate supplementation should be continued for at
least 3 months after delivery.
• Infections should be treated
• Puerperal sepsis, failing lactation, sub involution of uterus
and thromboembolism are more common in these patients
and should be carefully watched for.
• Effective contraception for 2 years for iron stores to recover

PREVENTION OF ANAEMIA IN PREGNANCY
• Family planning can prevent maternal morbidity & mortality by– Delaying motherhood/pregnancy till adulthood– Child spacing
• Preconception care -Correction of anemia & Iron stores before the onset of pregnancy
• Education of mothers

CASE STUDYA woman attends a routine antenatal appointment at 28 weeks gestation. She is 26 years old and G4P3+0 (3 Alive). All were through spontaneous vaginal delivery at term. Her third child is 18months old and the delivery was complicated by a post-partum haemorrhage requiring a 4 unit blood transfusion. This pregnancy has been uncomplicated to date with normal booking blood tests and normal anomaly ultrasound scan.
She feels generally tired and attributes this to caring for her three young children. She reports good fetal movements. Examination shows pallor and blood pressure of 126/73mmHg.

CASE STUDY
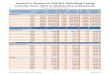
INVESTIGATIONS Normal range
Haemoglobin 7.7g/dL >/= 10g/dL Packed cell volume 23% >/= 30% Mean corpuscular volume 69fL 75 – 96fL White cell count 11.2 x 109/L 6 – 16 x 109/L Platelets 230 x 109/L 100 – 300 x 109/L Urinalysis: Negative
Genotype: AA
No atypical antibodies found

CONCLUSION• Anaemia in pregnancy is a major public health problem in many
developing countries with significant adverse effects on the mother, fetus, and the neonates.
• It affects more than 50% of pregnant women and the aetiopathogenesis is multifactorial & so management is by multidisciplinary approach
• Prevention of anaemia deserves more attentions by all and sundry
• Incorporating preconception care into the existing antenatal care programmes is essential

REFERENCES• Alfirevic Z et al: Postnatal screening for thrombophilia in women with severe pregnancy complications. Obstet Gynecol 2001;97:753. [PMID:
11339929]
• American College of Obstetricians and Gynecologists: Thromboembolism in Pregnancy. ACOG Practice Bulletin No. 19. American College of Obstetricians and Gynecologists, 2000.
• Aviles A, Neri N: Hematological malignancies and pregnancy: A final report of 84 children who received chemotherapy in utero. Clin Lymphoma 2001;2:173. [PMID: 11779294]
• Bates SM, et al: Use of antithrombotic agents during pregnancy: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126(3 Suppl):627S.
• Bazzan M, Donvito V: Low-molecular-weight heparin during pregnancy. Thromb Res 2001;101:V175.
• Burlingame J et al: Maternal and fetal outcomes in pregnancies affected by von Willebrand disease type 2. Am J Obstet Gynecol 2001;184:229. [PMID: 11174508]
• • Burns MM: Emerging concepts in the diagnosis and management of venous thromboembolism during pregnancy. J Thromb Thrombolysis 2000;10:59.
[PMID: 10947915]
• Burrows RF: Platelet disorders in pregnancy. Curr Opin Obstet Gynecol 2001;13:115. [PMID: 11315863] • • Choi JW, Pai SH: Change in erythropoiesis with gestational age during pregnancy. Ann Hematol 2001;80:26. [PMID: 11233772]
• Gerhardt A et al: Prothrombin and factor V mutations in women with a history of thrombosis during pregnancy and the puerperium. N Engl J Med 2000;342:374. [PMID: 10666427]
• Greer IA: The challenge of thrombophilia in maternal-fetal medicine. N Engl J Med 2000;342:424. [PMID: 10666435] • • Haram K, Nilsen ST, Ulvik RJ: Iron supplementation in pregnancy—Evidence and controversies. Acta Obstet Gynecol Scand 2001;80:683. [PMID:
11531608]