Embed Size (px)
Citation preview

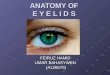
Anatomy of the Eyelids

An eyelid is a thin fold of skin that covers and protects an eye.
Thinnest skin of the whole body. Assist in distribution of tears over the
anterior surface of the eyeball. Assist in exit of tear into the drainage
system. Make an important contribution to the facial
features.

Upper eyelid from the eyebrow downward to end in a free margin
Forms the superior boundary of palpebral fissure.
Lower eyelid merge into the skin of the cheek.

Upper eyelid – Orbital part Tarsal part Formed by the insertion of the aponeurotic
fibers of the LPS into the skin.
Lower eyelid – less obvious Formed by few connections between the
skin and the orbicularis oculi muscle.

In primary position of gaze eyelid covers :
Upper – covers about 2 mm of the cornea Lower – just touches the cornea

Eyelids meet at medial and lateral canthi Medial canthus : Rounded
Lacus lacrimalis Caruncle Plica semilunaris Lateral canthus : 5-7 mm from lateral orbital margin
60˚ with eyes wide open 30-40˚ with eyes open in a normal way


2 mm in width Divided into 2 parts by the lacrimal
papilla. Lacrimal portion (medial) – rounded and
no lashes or glands. Ciliary portion (lateral) – rounded
anterior, sharp posterior border & inter-marginal strip.
Grey line – junction of skin & conjunctiva, divides inter-marginal strip.

In 2-3 rows 100-150 in upper lid 50-75 in lower lid Do not interlace when lids close Lifespan of some 3-4 months The sebaceous glands of Zeis & glands of
Moll open into each follicle or into the eyelid margin.

Elliptical space between upper & lower margins At birth : 18-21 mm horizontally 8 mm vertically Adult : 28-30 mm & 9-11 mm respectively.
Lateral canthus > Medial canthus (less than 2 mm)

1. Skin2. Subcutaneous areolar tissue3. Layer of striated muscles4. Submuscular areolar tissue5. Fibrous layer6. Layer of non-striated muscle fibres7. Conjunctiva


Epidermis : 6-7 layers of stratified squamous
epithelium Basal layer – unicellular sebaceous
glands,sweat glands. Dermis : Thin layer of dense connective tissue Rich in elastic fibers, blood vessels,
lymphatics & nerves. Variable number of melanocytes.

Loose areolar connective tissue No fat Thus readily distended by oedema or blood.

Orbicularis muscle – thin oval sheet across the eyelids.
Levator muscle – in upper eyelid.

Striated muscle, surrounds the orbital margin. Originates from ant. Part of medial palpebral
ligament & the adjacent bones. At the lateral angle of the eye the fibers
interlace at the lateral palpebral raphe. Orbital part – onto the temporal region &
cheek. Palpebral part – into the eyelids. Lacrimal part – behind the lacrimal sac.


ACTION : Forced closure of eyelids & thus pull the
eyebrows downward (Orbital). Gentle closing of eyelids during blinking,
sleep & soft voluntary closure (Palpebral). Pumping mechanism (Lacrimal). NERVE SUPPLY : Temporal & Zygomatic br.of
Facial nerve. ANTAGONIST – Orbital part : Frontal belly of occipitofrontalis
ms. Palpebral part : LPS.

ORIGIN : at apex of the orbit from under surface of lesser wing of the sphenoid.
Above the annulus of zinn By a short tendon, blended with underlying origin
of superior rectus muscle. INSERTION : into pretarsal skin of upper eyelid,
ant. Surface of tarsus, sup. Conjunctival fornix (few).
NERVE SUPPLY : superior division of oculomotor nerve
ACTION : elevation of the upper eyelid.

Thickened band of orbital fascia Formed by condensation of the superior
sheath of levator muscle. PTOSIS SURGERY : Recognition of this is
important. Severing of Whitnall’s ligament failure of
LPS function.

Nerves & vessels of the lids Injection – to anaesthetise the lid

Framework of the lids Tarsal plate – central thick part Orbital septum – peripheral thin part Medial & Lateral palpebral ligaments

Dense fibrous tissue Firmness & shape of eyelids 10 mm in height in upper lid & 5 mm in lower
lid in center Upper & lower plates join at medial & lateral
canthi To the orbital margins through medial &
lateral palpebral ligaments. Tarsal (Meibomian) glands are embedded in
the substances of the tarsal plates.

Thin membrane of connective tissue Continuous with the periosteum (periorbita) Separates eyelid from contents of orbital
cavity. perforated by nerves, vessels & LPS fibres,
which enter the lids from the orbit.


MEDIAL PALPEBRAL LIGAMENT Attached to frontal process of maxilla Form ant. Lacrimal crest
LATERAL PALPEBRAL LIGAMENT Attached to Whitnall’s tubercle (laterally) & tarsal
plates (medially).

Palpebral muscle (smooth) of muller. Arises from the fibres of LPS muscle in upper
lid & from prolongation of inferior rectus muscle in lower lid.
Inserted on peripheral margins of the tarsal plates.
Supplied by – Sympathetic nerve fibres.
Sympathetic irritation : Lid retraction. Paralysis : Horner’s syndrome.

Palpebral conjunctiva Firmly adherent to post. Surface of tarsal
plate & muller’s muscle.

MEIBOMIAN GLANDS : Present in stroma of tarsal plate arranged vertically in single row. About 20-30. They are modified sweat glands & ducts open on lid margin. Secretions are oily.
GLANDS OF ZEIS : Modified sebaceous glands which open into the follicles of eyelashes.

GLANDS OF MOLL : Modified sweat gland situated near the hair follicles or into the duct’s of Zeis glands. They do not open directly into the skin surface as elsewhere.
ACCESSORY LACRIMAL GLANDS OF WOLFRING : These are present near the border of tarsal plate.


Mainly by medial & lateral palpebral arteries.Marginal arterial arcades Superior or peripheral arterial arcadesTarsal arcades

VENOUS DRAINAGE : Arranged in two plexus – Pre-tarsal drains into subcutaneous veins and post-tarsal into the ophthalmic vein.
LYMPHATICS : Arranged as pre-tarsal & post-tarsal plexus.
Those from lateral two-third into parotid lymph nodes and from medial angle into submandibular nodes.

MOTOR NERVES are Facial (supplies orbicularis muscle), Oculomotor (supplies LPS muscle), Sympathetic fibres (supply muller’s muscle).
SENSORY NERVES derived from the first & second division of Trigeminal nerve.
Arrangement of nerve in the sumuscular plane.

Opening movements : Levator pupebrae superioris (primary) Frontalis Muller’s muscle
Bilateral symmetric Upper lid – Vertically upwards & Lower lid –
Laterally horizontal.

Closing movements : Orbicularis oculi
Upper lid – Vertically downwards & Lower lid – Medially horizontal

BENIGN NODULES & CYSTS Chalazion Dermoid

Caplliary haemangioma Xanthelasma Neurofibroma

Basal cell carcinoma Squamous cell carcinoma Kaposi sarcoma

Trichiasis Distichiasis Trichomegally Madarosis Poliosis

External hordeolum Molluscum contagiosum Herpes zoster ophthalmicus Herpes simplex Blepharitis

Ptosis Ectropion Entropion

Epicanthic fold Telecanthus Blepharophymosis syndrome Lid coloboma Cryptophthalmos