Embed Size (px)
Citation preview

BY: DR. KOMAL SHARMA PG 1 S T YEAR
ANATOMY OF MAXILLA AND ITS DEVELOPMENT

CONTENTS
INTRODUCTIONDEVELOPMENT OF MAXILLAFEATURES OF MAXILLAARTICULATION OF MAXILLAAGE CHANGESPERIODONTAL CONSIDERATIONSCONCLUSION

INTRODUCTION
Maxilla is the 2nd largest bone of the face.
The 2 maxillae form the whole of the upper jaw.
3 cavities: the roof of the mouth, the floor & lateral wall of the nose & the floor of the orbit.
.

2 fossae, the infratemporal & pterygopalatine.
2 fissures, the inferior orbital & pterygomaxillary.

DEVELOPMENT OF MAXILLA:PRENATAL EMBROYOLOGY OF MAXILLA:
4th week of IUL a prominent bulge appears on the ventral aspect of the embryo.
Shallow depression primitive mouth stomodeum
Separated from the foregut by the buccopharyngeal membrane
5 branchial arches form in the region.
1st branchial arch is mandibular arch – responsible for the development of nasomaxillary region.

The mesoderm covering the developing forebrain proliferates to form the frontonasal process.
The stomodeum is overlapped superiorly by frontonasal process & laterally by mandibular arches of both sides.
Formation of nasal pits divides frontonasal process into 2 parts :a) The medial nasal processb) The lateral nasal process

•The mandibular arch gives off a bud from its dorsal end called the maxillary process which grows ventro-medio-cranial to the mandibular process.
•At this stage the stomodeum is overlapped from above by the frontal process, below by the mandibular process & on either side by the maxillary process.
•The two mandibular processes grow medially & fuse to form the lower lip & the lower jaw.

•Maxillary process undergoes growth, frontonasal process becomes narrower so that 2 nasal pits come closer.
•Line of fusion of maxillary process & the medial nasal process corresponds to the nasolacrimal duct.

DEVELOPMENT OF PALATE: Palate is formed by:
A. Maxillary processB. Palatal shelvesC. Frontonasal process
The frontonasal process premaxillary region while palatal shelves form rest of the palate.
Medial growth of palatal shelves & their union is prevented by the presence of the tongue, thus palatal shelves grow vertically downwards initially.

7th week - IUL transformation in the position of palatal shelves occurs i.e from a vertical to a horizontal position.
8 ½ weeks- IUL c/t of palatal shelves intermingle with each other resulting in their fusion
Initial palatal contact occurs in the central region of the secondary palate posterior to the premaxilla.
Mesial edges of the palatal processes fuse with the free lower end of the nasal septum & thus separates the 2 nasal cavities from each other & the oral cavity.

OSSIFICATION OF THE PALATE:
It occurs from the 8th week of intra-uterine life.
Its an intramembranous type of ossification.
The palate ossifies from a single centre derived from the maxilla.
The most posterior part of the palate does not ossify & forms the soft palate.
The mid-palatal suture ossifies by 12-14 years.

Tongue 5th week , rapidly proliferating
mesenchymal swellings, covered with a layer of epithelium, appear on the internal aspect of the mandibular arch known as the lateral lingual swellings
Between the swellings arises a small medial projection, the tuberculum impar
Caudal to the tuberculum impar, the copula unites the 2nd & the 3rd branchial arches to form a mid central elevation extending backward to the epiglottis

Mesodermal tissue from the 2nd, 3rd & 4th arches grow on either side of the copula & form the tongue structure
Point at which the 2nd & 3rd branchial arches merge marked by the foramen caecum just behind the sulcus terminalis, which marks a boundary between root of the tongue and its active portion
Mucosal sac or covering of the body of the tongue originates from 1 st lateral lingual swelling of the mandibular arch.
11th week of fetal age papillae of the tongue are seen .
By 14 weeks the taste buds can be observed in the fungiform papillae, & they appear in circumvallate papillae at about 12 weeks

DEVELOPMENT OF MAXILLARY SINUS:
The maxillary sinus forms sometime around the 3rd month of intrauterine life.
It develops by expansion of the nasal mucous membrane into the maxillary bone.
Later sinus enlarges by resorption of the internal wall of maxilla.

POST-NATAL GROWTH OF MAXILLA
Maxillary complex is attached to the cranial base it influences the development of this region.
The growth of the maxilla is dependent on the spheno-occipital & spheno-ethmoidal synchondroses.
The growth of the nasomaxillary complex is produced by the following mechanisms: Displacement Growth at Sutures Surface Remodeling

Displacement Growth of the cranial base
passive /secondary displacement of nasomaxillary complex in downward & forward direction.
As middle cranial fossa grows it moves the nasomaxillary complex to a more anterior position.
Growth of the maxillary tuberosity primary type of displacement in a forward direction,due to the enlargement of the bone itself.

Growth At Sutures :Maxilla is connected to the cranium
& cranial base by a number of sutures:
The fronto-nasal suture The fronto-maxillary
suture The zygomatico-temporal
suture The zygomatico-maxillary
sututre The pterygo-palatine
suture

Surface Remodeling : Massive surface remodeling by
bone deposition & resorption increase in size; change in shape of bone; & change in functional relationship.
Resorption occurs on lateral surface of the orbital rim
lateral movement of the eyeball, to compensate for this resorption there is bone deposition on the external surface of the lateral rim.

Bone deposition occurs along the posterior margin of the maxillary tuberosity, lengthening of dental arch & enlargement of antero-posterior dimension of entire maxillary body & helps to accommodate developing molars.
Bone resorption on the lateral wall of the nose leads to an increase in the size of the nasal cavity.

Bone resorption on floor of the nasal cavity compensated by deposition on palatal side, downward shift an increase in maxillary height.
The zygomatic bone moves in posterior direction, which is achieved by resorption on anterior surface & deposition on posterior surface.

Face enlarges in width by bone formation on lateral surface of zygomatic arch & resorption on its medial surface.
As teeth start erupting, bone deposition occurs at alveolar margins.
Increases the maxillary height & depth of palate: the expanding “V” principle.

Anatomy of maxilla
BODY OF MAXILLA: Body of maxilla is pyramidal in
shape, with its base directed medially at the nasal surface, and the apex directed laterally at the zygomatic process.
It has four surfaces and encloses a large cavity; the maxillary sinus.
(1)Anterior or facial (2)Posterior or infratemporal (3)Superior or orbital (4) Medial or nasal

MEDIAL OR NASAL SURFACE

Four Processes of Maxilla:
Zygomatic Process Frontal Process Alveolar Process Palatine Process

PALATINE PROCESS

The Maxillary Sinus or Antrum of Highmore (sinus maxillaris)
Large cavity in body of maxilla. Pyramidal in shape, with base :
Medially towards lateral wall of nose
Apex directed laterally into zygomatic process of maxilla.
Roof formed by floor of orbit and traversed by infraorbital canal.
The floor is formed by alveolar process of maxilla ,lies about 1.2 cm below level of floor of nose.

FUNCTIONS : Speech and voice resonance Reduce the weight of scull Filtration of inspired air Immunological barrier Regulation of intranasal pressure

Articulations of Maxilla
Superiorly, it articulates with- 3 bones1) Nasal2) frontal 3) lacrimal.
Medially : 5 bones1) Ethmoid2) Inferior nasal concha3) Vomer4) Palatine 5) Opposite maxilla

Laterally : 1 bone
1) Zygomatic bone

Age Changes
At birth : Transverse and anteroposterior diameters >vertical diameter; Frontal process is well marked Body consists of a little more than the alveolar process; The tooth sockets close to floor of orbit Maxillary sinus is a mere furrow on the lateral wall of the nose.
In Adults: Vertical diameter is greatest due to developed alveolar process increase in the size of the sinus.
In Old Infantile condition Its height is reduced as a result of absorption of the alveolar process.


Nerve supply

Arterial supply

Muscle attachment

LYMPHATICS

PERIODONTAL CONSIDERATIONS
Palatal flaps and donor sites for gingival grafts should be carefully performed and selected to avoid invading these areas, as profuse haemorrhages may ensue, if vessels are damaged at palatine foramen.
Severance of greater palatine artery must be avoided as it is very difficult to stop the hemorrhage by local clamping or by tamponade. In certain instances stoppage has only been accomplished by ligation of external carotid artery.

Distal wedge procedure

ANATOMIC SPACES
Spaces contain loose c/t , can be easily distended by inflammatory fluid and infection. Surgical invasion of these areas may result in dangerous infections and should be carefully avoided. Canine fossa contains varying
amounts of c/t & fat and is bounded Infection of this area results
in swelling of upper lip, obliterating nasolabial fold, & of upper and lower eyelids, closing the eye.

Infection of this area results in swelling of the cheek but may extend to the temporal space or the submandibular space, with which the buccal space communicates.

ANTERIOR FACIAL REGION
Maxillary incisor teeth eccentrically placed in the alveolus, Facial alveolar bone being very thin or absent over prominent incisor or canine roots.
selecting a surgical procedure which leaves bone covered with periosteum & c/t, one may prevent p.o osseous and gingival recession.
Alveolar process have clinical importance in periodontal surgery because of several muscle attachments.

During periodontal surgery in the canninus muscle attachment arise from canine fossa below infraorbital foramen should not damage infraorbital nerve and vessels.

POSTERIOR FACIAL REGION
Severe bone loss in this region could result in the base of the periodontal pocket approximating both zygomaticoalveolar ridge of the zygomatic process of the maxilla and the attachment of the buccinator muscle. Each could complicate any surgical attempt to deepen the vestibule or increase the zone of attached gingiva.
Attachment of buccinator muscle may also limit the apical extent to which one could establish the mucogingival junction and an adequate width of attached gingiva.
Alveolar bone overlying buccal roots of maxillary molar teeth is frequently found to be very thin or absent. As in anterior facial region of the maxilla, a surgical technique may be employed which prevents exposure of the bone and possible postoperative recession.

PALATE Nasopalatine nerve emanates from
incisive foramen to supply the sensory innervation for palatal mucosa from canine to canine.
Surgery to eliminate periodontal pockets in this region often requires removing or undermining the incisive papilla, which could result in servering the nasopalatine nerve and a temporary paresthesia of the area supplied.

Osseous considerations in the palate include the presence of tori and the shape of the palatal vault.
Prominent exostoses or a flat, shallow palatal roof make osseous interproximal ramping either impossible or difficult to accomplish.

In gingivectomy procedures on the palate, If the alveolar process is very short due to a shallow palatal vault, it would be very difficult to achieve a properly beveled result without making an extremely wide incision with its probable postoperative discomfort.

IMPLANTS:Age as compromising factor for implant insertion:
Transverse growth:
The width of ant. portion of the arch is completed prior to the adolescent growth spurt, but for post. portion, the width increase is closely tied to the increasing jaw length.
The width in the ant. portion ses mainly by growth at the midpalatal suture ,a growth is 3x larger in 1st molar area than in front.
The intercanine distance will change only little after the age of 10 (0.9 mm)
Thus if a central incisor was replaced with an implant shortly after eruption, diastema could develop between the implant and the adjacent natural central incisor ,resulting in subsequent shifting of the midline to the implant side.
In most post. area changes can occur until complete tooth eruption.
The midpalatal suture usually closes after puberty around the age of 15 .

Sagital growth: Maxilla ses in length due to both sutural growth & bone apposition at maxillary
tuberosity. The ant. part of max. is rather stable. When max. is displaced & during growth ,up to 25% of displacement is lost via
resorption at anterior site, latter could result in an implant gradually losing labial bone. Teeth have a spontaneous mesial drift. The lat. segment moves on average 5 m mesially but
max. incisors move only 2.5 mm buccally ,causing net loss in space ,lead to crowding. Implant does not take part in spontaneous tooth migration. Thus an implant in lat. region
could stop the mesial drift resulting in asymmetric arch.Vertical growth: Occurs via displacement and drift. An implant inserted in ant. part at age of 7 will 9 years later be located 10 mm more
apically than the neighbouring teeth.

Bone density Description Tactile analog Typical anatomical location
D1 Dense cortical Oak or maple wood Anterior mandible
D2 Porous cortical and coarse trabecular
White pine or spruce wood
Anterior mandible, posterior mandible, Anterior maxilla
D3 Porous cortical and fine trabecular
Balsa wood Anterior & posterior maxilla
D4 Fine trabecular Styrodoam Posterior maxilla
Misch bone density classification

IMPLANTS
In maxilla,7 mm of bone height is sufficient to accommodate short implants.
Use of 7-10 mm long implants is a greater concern in the maxilla
because implant failure rate is higher in the maxilla.Therefore,13 mm recommended minimum occlusocervical bone dimension in maxilla.
In case of not having enough bone height can opt for sinus lift, which is a surgical procedure, aims to increase amount of bone in the posterior maxilla.

AUTOGENOUS BONE GRAFT
Osseous coagulum: Sources were: Exostoses Edentulous ridges Bone distal to terminal tooth Lingual surface of maxilla at least 5 mm from the roots.

Cancellous bone marrow transplants obtained from:
Maxillary tuberosity Edentulous areas Healing sockets
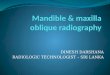
Maxillary tuberosity contains good amount of cancellous bone, care should be taken not to extend the incision (made distally from last molar) too far distally to avoid sectioning the tendons of the palatine muscle

A) radiographic appearance, showing the possibility of removing bone from the right maxillary tuberosity, B) in the dry skull, the presence of medullary bone C) tuberosity detached for graft removal.

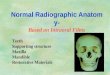
Radiographic considerations:
Here shown radiographic anatomy of maxillary area in the periapical, panoramic, occlusal, cephalometric radiographs and finally in volumetric computed tomography.
Periapical radiographs-incisor area

Cephalometric radiographs Panoramic radiographs

Occlusal radiographs Periapical radiographs – canine area

Computed tomography: Maxillary Central area

ANESTHESIA
Posterior superior alveolar nerve: (PSA)Descends from the main trunk
of the maxillary division in the pterygopalatine fossa just before the maxillary division enters the infraorbital canal.
Passing downward through the pterygopalatine fossa, they reach the inferior temporal surface of maxilla .

Nerve block: Commonly used, Successful technique. Technique:
Advance needle slowly upward: Superiorly at a 45 degree angle to occlusal plane
Inward: Medially toward midline at 45 degree to occlusal plane. Backward : Posteriorly at 45 degree angle to long axis of 2nd molar
in one movement.

Alternative: Supraperiosteal injections: requires multiple needle penetrations , provides shorter duration of anesthesia.
When combined with anterior superior alveolar block –entire maxillary arch on one side can be anesthetized (except palatal tissues).
Prevention: the risk of hematoma can be minimized by using a short 25 or 27 gauge needle, aspirating in two planes multiple times before and during the slow deposition of anestheic.
If anesthesia of posterior palate is needed, greater palatine block should be provided in addition to psa block.

Middle superior alveolar nerve : (MSA) Nerve branches off the main nerve
trunk(V2) within the infraorbital canal to form a part of superior dental plexus, composed of posterior, middle, and anterior superior alveolar nerve.
Nerve block:
SITE OF ORIGIN: from posterior portion of infraorbital canal to anterior portion ,near the infraorbital foramen.
Insertion: at the height of mucobuccal fold above max.2nd premolar.
If deposition too low, only 2nd pm will be anesthetized.
Alternative: infraorbital nerve block.

Anterior superior alveolar nerve: (ASA) Relatively large branch ,is given off the infraorbital nerve approx. 6-10 mm
before latter’s exit from infraorbital foramen. Descending within the anterior wall of maxillary sinus ,provides pulpal
innervations to central and lateral incisors and the canine, and secondary innervations to periodontal tissues, buccal bone and mucous membranes.
ASA nerve communicates with MSA nerve and gives off a small nasal branch that innervates the anterior part of nasal cavity along with branches of pterygopalatine nerves.
Nerve block: Target area : Infraorbital foramen

Precautions: For pain on insertion of needle and
tearing of the periosteum, reinsert the needle in a more lateral way (away from bone) position or deposit solution as the needle advances through soft tissues.
For overinsertion of needle,estimate the depth of penetration before injection and exert finger pressure over infraorbital foramen.

Greater palatine nerve: Descends through the pterygopalatine
canal emerging on the hard palate through the greater palatine foramen.
Nerve block: Technique: 27 gauge short needle recommended Locate the greater palatine foramen: By using a cotton tipped applicator to
firmly palpate from 1st molar region at the junction of alveolar process and the hard palate towards third molar
Small depression will be felt between distal of 1st molar and mesial to 3rd molar

Nasopalatine nerve: Passes across the roof of nasal cavity downward and forward ,where it lies
between the mucous membrane and the periosteum of nasal septum. It continues downward, reaching the floor of the nasal cavity and giving
branches to anterior part of nasal septum and floor of nose. It then enters the incisive canal through it passes into oral cavity via incisive
foramen located in midline of the palate about 1 cm posterior to maxillary central incisiors.

Nerve block: Highly traumatic Technique: A 27 gauge short needle recommended. Approach the injection site at a 45 degree angle towards the incisive papilla. Apply enough pressure to bow the needle slightly.

CONCLUSION
Consideration of the surgical anatomy serves as a basis for surgical procedures involving periodontal tissues and implants. damage to nerves can be avoided with proper technique and treatment planning that should include three dimensional radiographs when these structures are likely to be within vicinity of surgical approaches.
Inadvertent surgical incision of major blood vessels, such as the greater palatine artery and the middle and posterior superior alveolar artery, can be avoided by knowledge of their anatomic positioning.

REFERENCES
B.D Chaurasia’s Human Anatomy 4TH ed vol.3.THE HEAD AND NECK. Carranza’s clinical periodontology. Michael G. Newman, Henry H. Takei,
Fermin A. Carranza .11th ed. Elsevier publication 2012. Grey’s anatomy of the human body.20th ed. philadelphia 1918 Orthodontics THE ART AND SCIENCE. S.I Bhalajhi. 5TH ed. Arya Medi-
2012. Human Embryology. Inderbir Singh. 10TH ed. Jaypee Brothers 2014.• Orban’s B. Oral Histology & Embryology. 7th ed. St. Louis. Mosby Inc – 1972 Carl.E.Misch. Contemporary implant dentistry.3rd ed. Elsevier 2011 Michael A. Clarke, D.D.S., M.S, Kenneth W. Bueltmann, D.D.S., M.S.
Anatomical Considerations in Periodontal Surgery. j. Periodont, 42:610-625, 1971.

Handbook of local anesthetics. Stanley F. Malamed.6th ed. Elsevier publication 2012
Normal Radiographic Anatomy – Maxillary Central Area. Carmen Elena Georgescu, Gabriela Tãnase, Augustin Mihai. OHDMBSC - Vol. VI - No. 3 - September, 2007
Leonardo Perez Faverani , Gabriel Ramalho-Ferreira , Paulo Henrique Dos Santos , Eduardo Passos Rocha , Idelmo Rangel Garcia Júnior , Cláudio Maldonado Pastori , Wirley Gonçalves Assunção .Surgical techniques for maxillary bone grafting - literature review.. Rev. Col. Bras. Cir. Rio de Janeiro 41:1,Jan./Feb. 2014.
Laura J. Webb. Anesthesia during perio: Maxillary injections useful for adult nonsurgical periodontal therapy. June 12, 2015
Danny G. op heij, Heidi opdebeeck, Daniel van steenberghe,Mark quirynen. Age as compromising factor for implant insertion.periodontology 2000,33:172-184;2003