Embed Size (px)
Citation preview

SKIN & ITS APPLIED ANATOMY
Snehal Kharche

Contents INTRODUCTIONBASIC STRUCTURE OF SKINBASIC LESION OF SKINSURGERY OF SKIN
◦ BIOMECHANICAL PROPERTIES OF SKIN◦ SKIN LINES◦ COSMETIC UNIT OF FACE◦ PRINCIPAL OF INCISION AND SUTURING OF FACE◦ WOUND DRESSING◦ SCAR AND SCAR REVISION (OVERVIEW)◦ ADVANCES IN SKIN SURGERY

IntroductionSkin is the largest organ of the
body which forms 8% of total body mass
Covers entire external surface of body
Is continuous around body orifices

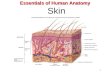
Basic structure of skin• Skin may be viewed as a double-
layered sheath, cushioned by underlying subcutaneous fat,
the layers are
Epidermis Dermis

EpidermisEpidermis is a continually
renewing, keratinizing, stratified, squamous epithelium
Layers of epidermis Stratum basale Stratum spinosum Malpighian
layer Stratum granulosum Stratum corneum

The cells present in skin are keratinocytes(80%), melanocytes, langerhans cells & merkel cells

Dermal-epidermal junctionFirmly attaches epidermis to
dermisMechanical support to epidermisActs as a semi-penetrable
membrane

Epidermal appendages

Epidermal AppendagesHair follicle: is main component of pilosebaceous
unit which is composed of sebaceous gland, arrector pili muscle & sensory end organ
Sebaceous gland: it is unilocular or multilocular st. which connects hair follicle by a sebaceous duct
Eccrine sweat glands: reticular dermis, duct opens directly on skin, innervated by cholinergic nerve fibres
Apocrine sweat gland: adregenic innervation, duct connects to hair follicle above sebaceous duct

DermisConnective tissue between
epidermis & dermisIt is divided into papillary &
reticular dermisIt is composed primarily of
collagen, elastin & ground substance

Regional skin variationGlabrous skin(non hairy skin)Non glabrous skin(hair bearing skin)

Vascular supply of skin

It originates from three main sources Direct cutaneous: main arterial trunk Musculocutaneous: arise from
intramuscular vasculature, pass through surface of muscle, pierce deep fascia to reach skin
Fasciocutaneous: perforating branches from vessels deep to deep fascia, pass along intermuscular septa, fan out at level of deep fascia
Plexi Subpapillary Reticular dermal Deep dermal

Basic lesions of skinMacules (1 - 2cm, different color, flat)Patches (large macule)Papule (elevated, less than 1 cm)Nodule (dome shaped, more than 1 cm)Wheals (round pale red)Vesicle (contains fluid, less than 0.5cm)Bullae (more than 0.5cm)Erosion (break in epidermis)Pustules (raised, purulent)Fissures (cracks in skin)

Burns woundBurns cause damage in no. of diff.
ways, but most common affected organ is skin
Assessing size (for treatment plan & morbidity) Pt. Whole hand is 1% TBSA and is
useful guide for small burns Rule of nine(wallace’s) UL-9%, LL-
18%, Torso-18% each side, H&N-9%, GR-1% only for initial approx.
Browder chart for large burns

Wallace chart(rule of nine)

BROWDER CHART

Classification of burnsSuperficial partial thickness
(papillary)
Deep partial thickness (reticular)
Full thickness (whole dermis)

Biomechanical properties of skinNonlinearity:1. Flat section- considerable extension with
little force2. Intermediate section- rapid transition3. Terminal section- little or no extension
despite increased forces Anisotropy:
variation in skin tension atdiff. sites of bodydirectional considerations for skin movement

Viscoelasticity:At high stresses skin shows viscoelastic
properties, two time-dependent properties of skin are
Creep: (permanent stretching)increase in length of skin compared to original length when placed under const. stress
Stress relaxation: decrease in stress when skin is held under tension at a const. strain as relaxation occurs as tissue creeps

Skin linesRelaxed Skin tension lines
(RSTL) correspond to the directional pull when skin is relaxed do not always correspond to wrinkle lines result from orientation of
collagen fibre of skin used for incision making Lines of maximum extensibility


Wrinkle line – caused by contraction of underlying muscle, perpendicular to their axis of shortening
Kraissl’s line – exaggerated wrinkles lines
Langers line- lie at right angle to RSTL

Aesthetic regions of faceCovered by skin having common
characteristicsPrinciple aesthetic regions of face
are Forehead Cheek (five subunits) Eyes & eyebrow Nose (nine subunits) Lips & chin

Esthetic units of nose

Principals of incision Incisions placed on exposed surface
of face must follow some basic principles so the scar is inconspicuous Avoid imp. Neurovascular structures Use as long incision as necessary Place incision perpendicular to surface of
nonhair-hair bearing skin Place incisions in line of minimal tension Seek for other favorable sites for incision
placement

Commonly used skin incision

Suturing

Optimizing outcome of sutured woundShould be at even level to prevent “step off
deformity”Prior to placement of top stitch all tension
should be off the wound edgesTo reduce wound tension buried absorbable
suture should be usedEverted wound edges for thinner and flatter
scar In cosmetic areas fine caliber suture or
subcuticular suture are used


Post operative careSuture left for long promotes infec.Remove suture at appropriate time to
prevent “Rail Road” scarRecommended suture removal time Eyelid – 2 to 4 days Face – 4 to 6 days Neck and scalp – 5 to 7 days Extremities – 10 to 14 days

Wound dressing Functions: Maintain a moist wound healing environment Absorb exudate Provide a barrier against bacteria Reduce edema Eliminate dead space Protect against further injury from trauma,
pressure and sheer

Scar and scar revisionThe trace of healed wound sore, or burn.
A fault or blemish remaining as a trace of some former condition or resulting from some particular cause
Ideal scar: Imperceptible Not cause distortion of adjacent structure Lie in aesthetic borders or in RSTL Flat and in level with surrounding tissues Same color and texture as surrounding skin

Adverse scar: Wrong direction Poor alignment Stretched scar Contracted scar Pigment alteration Contour deformity (trapdooring) Tattooing Stitch mark (after 7 days) Hypertrophic scar Keloid scar

Hypertrophic scar- Not familial- Not race related- Female = Male- Children- Remains with wound- Subsides with time- Flexor surface- Tension related
Keloid scar- May be familial- Black > White- Female > Male- 10 – 30 yrs- Outgrows wound- Rarely subsides- Sternum , shoulder- Unknown

Scar revisionReconstructive ladder

Timing of scar revisionScar should be mature
Collagen remodeling and reorientation takes upto 18 months
If scar is grossly deforming revision is recommended 2-3mnths- dermal scar serves as wound base

Techniques for scar revision Non surgical methods Massage (1month post operative) Silicone gel (topical application) Intralesional steroids Lasers Vitamin E Vitamin A Herbal extract (allium cepa) Make up (camouflage)

Surgical Methods
Scar excision Scar irregularization• Z-plasty• W-plasty• Geometric broken line

Scar excisionMost common excisional tech. is elliptical
excisionReserved for scars that are parallel to RSTL,
less than 2cm in length or short straight wide depressed or raised scars
Fusiform shaped incisions made parallel to RSTL
Angle<30 degree to prevent skin rebundancy & l:w ratio – 3:1

Scar irregularizationZ- plasty:• Classic z-plasty is 60 degree transposed flap
• Used for scar not along RSTL
• It alters the direction of scar to be parallel with RSTL
• Two points in Z- plasty are critical (a) Angle size (tissue lengthening ) (b) Length of common diagonal (scar)
• In larger scar multiple z-plasty is done



W- plasty:
• Based on principle that irregular line is less visible than straight line
• Used for scar not along RSTL
• Zigzag incision on one side and its mirror image on opposite side

Geometric broken line:
• used for longer scar
• outline is made on one side using geometric designs (circles, triangles)
• undermine and suture

V-Y & Y-V advancement flap: V-Y adv. Flap is unique in that V shaped flap
is not stretched or pulled into recipient site It is particularly useful when a structure or
region requires lengthening or release from contracted scar

Y-V advancement is similar to V-Y flap except that V shaped flap is stretched or pulled
The maximum wound closure tension is at apex of flap

DermabrasionSuperficial injury to papillary dermisDeposition of new organized collagenImproves surface irregularities &
pigmentation

TechniqueSkin preparation (1 month prior) (optional) - 4 % Hydroquinone (depigmentation) - retinoic acid & tertinoin Entire scar & adjacent skin is dermabraded
Abrasion is carried to the level of upper to midreticular dermis
End point of abrasion is appearance of pinpoint bleeding – indicates invasion of dermal papillae

ArmamentariumElectric powered rotary Hand piece
Diamond Fraise & Files (round, wheel)
Derma abrasion is carried out at 10,000 to 15,000 rpm

Advances in skin surgery
LASERS – Light amplification by stimulated emission of radiation
- Principles :A quantum of electromagnetic energy called photon can stimulate an EXCITED atom to emit another photon with same energy and wavelength
- Key word is EXCITED atom, as resting atom will simply absorb the photon

Parts of a Laser system A gas, solid or liquid medium that can be
excited to emit laser light Mirror, reflects light back and forth,
increases intensity A source of energy to excite medium Delivery system (fibro-optic cable)
Type of Laser Continuous laser Pulsed Laser

Chromophores – medium that absorb light Three primary chromophores in skin: (a) Water (b) Hemoglobin (blue, green) (c) Melanin (Broad spectrum) The laser light absorbed by the tissue is
converted into HEAT Time required by the tissue to loose half its
heat to surrounding tissue is thermal
relaxation time (TRT)

SELECTIVE PHOTOTHERMOLYSIS - When pulse duration is shorter than
TRT of target – localized heating
CO2 laser and Er:YAG laser for skin resurfacing (wrinkle , scar)
Argon laser for vascular lesion

Skin graftsTwo main forms
Split-thickness (Thiersch graft) Full-thickness (Wolfe graft)
- Composite graft – Contains skin plus other structure eg. cartilage

SPLIT-THICKNESS (STSG)
DONOR SITE-large area -heals spontaneously-site reusable
RECEPIENT SITE-contracts more-easily abraded -poor color match-inferior cosmetics-reliable ‘take’-inelastic-over large areas
FULL-THICKNESS (FTSG)
DONOR SITE-smaller area-site must be closed-site scars
RECEPIENT SITE-contracts less-abrasion resistant-good color-good cosmetics-less reliable ‘take’-normal texture, elastic-used over face