Embed Size (px)
Citation preview

Anaemia in Heart Failure
PRESENTER- DR ABHISHEK RATHORE SJIC&R ,Bangalore

IntroductionAnemia – poor prognosis in HF
Anemia itself can cause HF (Hb < 5gm/dl)*, but uncommon to be the sole mechanism.
Elderly, IHD, Renal dysfunction and even General population with anemia are at risk of HF.
ESPs or iron therapy may have role in HF with anemia.
*ACC/AHA 2005 Guideline update for diagnosis and management of CHF in adults.

Potential Therapeutic Targets

Definition of AnemiaWHO- Hb < 13g/dl (Men) Hb < 12g/dl (Women)
NKF criteria- Hb < 12g/dl (Men and
Postmenopausal women) Hb < 11g/dl (Premenopausal
women)

PrevalenceDepend on population studied and
definition of anemia used.
ARIC (Atherosclerosis Risk in Communities) study-
A/c to WHOAge: 45-64 yearsN= 15,792
9% patients were found Anemic.

ANCHOR study
N= 59,772 43% had anemia.
N= 12,065 (New onset heart failure)
Prevalence- 17% Ezekowitz JA et al, Circulation.2003;107:223–5
AS GO et al, Circulation.2006;113:2713-23

Anemia in patients with heart failure
Hb = hemoglobinHct = hematocritHF = heart failure
The prevalence of anemia in heart failure patients is approximately:– 30% for Inpatients– 20% for Outpatients

4 – 61% (Median 18%) by Tang and Katz from 15 papers.
Circulation.2006;113:2454-61

The prevalence of anemia and the severity of heart failure
Source: STAMINA Registry – 45 General Cardiologist sites, n=673, 12 Academic sites (incl. HF Specialists), n=337
2% 2% 4%6% 8%
29% 30%
40%
60%
12%
44%
11%
52%
19%14%13%
29%21%20%
56%
0%10%20%30%40%50%60%70%
I (n=158) II (n=467) III (n=340) IV (n=25)
Pati
ents
Hb<10g/dL (n=32)Hb<=11g/dL (n=97)Hb<=11.5g/dL (n=165)Hb<=12.0g/dL (n=244)Hb<=12.5g/dL (n=337)
NYHA Class

Mechanism of Anemia in HFConcominant CKD (in 40-50% patients)—M.C.
Inflammation and Cytokine activation ( TNF-alpha, IL-6 and CRP)
Aspirin usage (GI loss)
ACE inhibitor and ARBs
Decrease Fe absorption (Bowel edema, Inc Hepecidin)
Hemodilution
Nutritional


Type of AnemiaM.C.- Normocytic normochromic
Anand et al- Prevalence of Fe deficiency anemia- 5 to 21%#
De Silva et al*. 43% pts had low serum iron or ferritin, but only 6% had Microcytic anemia.
Nanas JN et al$. Found depleted bone marrow stores in 73% pts despite normal serum iron, ferritin and EPO levels.
#Anand IS.JACC.2008;52:501-11*Am J Cardiol.2006;98:391-8$ JACC.2006;48:285-9

Prognostic significance of anemia in HF
Poor prognosis
Increase mortality and hospitalisations

Study Design N Anemia Risk Assessment Limitations
Alexander1Retrospective cohort study of a population based HF database
90,316Anemia was an independent risk factor of 1-year rehospitalization (RR 1.162; 95% CI: 1.134 to 1.191)
no confirmation of the HF diagnosis; undercounts of minorities and biased results.
Polanczyk2Prospective, single center, observational study
205 Anemia was an independent predictor of 3-month rehospitalization (p=0.002)
Too small of a population to resolve a small difference in readmission rates; role of confounding variables due to lack of control
OPTIME-CHF3 Retrospective chart review 906
Anemia was an independent predictor of 60-day death or rehospitalization (odds ratio of 0.89 per 1 g/dL increase in hemoglobin; 95% CI: 0.82 to 0.97)
Anemia may have been caused by hemodilution in hospitalized patients
Kosiborod4 Retrospective chartreview 2,281
Patients had 2% higher risk of 1-year rehospitalization for every 1% lower hematocrit (95% CI: 1.01 to 1.03; p=0.0002)
Lack of data on transfusions or other treatments for anemia; study generalizability to non-study population
COPERNICUS5Randomized,double blind,placebo controlledtrial
2,286Anemia was an independent risk factor for 1-year morbidity (HF hospitalization) and mortality outcomes
-
Anemia is associated with increased risk for hospitalization in heart failure patients
1Alexander M, et al. Am Heart J. 1999;137:919-9272Polanczyk CA, et al. J Card Failure. 2001;7:289-298
3Felker GM, et al. Am J Cardiol. 2003;92:625-6284Kosiborod M, et al. Am J Med. 2003;114:112-119
5Anker SD, et al. J Am Coll Cardiol. 2004;43(suppl A):Abstract 842-2

Hemoglobin and mortality in heart failure patients

Groenveld HF et al*. Anemia and mortality in heart failure patients: a systematic review and metaanalysis.
Meta-analysis of 34 studies, Includes 1,53,180patients
JACC.2008;52:817-28

If Anemia as mediator of HF - T/t is beneficial
If Anemia as marker of HF - Benefits limited
Should we treat anemia in a patient with heart failure?

What is the rationale for anemia correction?
Potential Benefits Improved oxygen
delivery Improved exercise
tolerance Attenuate adverse
remodeling Improved Quality of Life Antiapoptotic? Decrease in
hosp./death?
Potential Risks Increased thrombosis Platelet activation Hypertension Endothelial activation
Adapted from Felker and O’Connor J Am Coll Cardiol. 2004;44:959-966.
Potential benefits and risks of treating anemia in HF:

Treatment options for anemia in HFBlood transfusion
ESPs
Iron therapy

Blood Transfusion in HF The clinical utility in CV disease is controversial.
“Transfusion Threshold” Hematocrit < 30% in CV disease Based on expert opinion
May be considered as an acute treatment for severe anemia.
Not a strategy for the longterm management in CHF.

Saftey concern of ESP in variety of anemic patients.
1. In CKD

Pivotal Clinical Trials in CKD with Anemia
NHCT(1998): National Hematocrit Cardiac Trial--- N-1200, high hemoglobin was conferred with high death and the trial was thereby prematurely stopped.
Canadian Cardiac Trial(2005)---similar trial with very similar observation.
CREATE(2006): Cardiovascular Risk Reduction by Early Anemia Treatment with Epoetin beta
CHOIR(2006): Correction of Hemoglobin and Outcomes in Renal Insufficiency
TREAT(2009): Trial to Reduce Cardiovascular Events with Aranesp Therapy.

2. In Cancer patients (N=1473 pts)
Conclusion- DA not associated with significant reduction in transfusions and also patients had shorter survival time.

3. In Ischemic Stroke
Ehrenreich H et al*- Recombinant human erythropoietin in patients presenting in 6 hrs of ischemic stroke had higher death rates.
*Stroke.2009;40:e647-e56

Erythropoietin Stimulating Proteins in HF

STAMINA HeFT trial
Circulation. 2008;117:526-535

STAMINA HeFT trial
Largest(319 pts) and longest (53 weeks) completed study of ESP in HF patients.
Patients with EF ≤40% , Hb ≥ 9g/dl and ≤ 12.5 g/dl were randomised.
Target Hb was 14.0 ± 1.0 g/dl
Ghali JK et al.Circulation.2008;117:526-35

Conclusion: Darbepoetin alfa not associated with significant clinical benefits. DA was well tolerated and effectively raised Hb. A trend of lower risk of morbidity and mortality observed.
27 weeks 53 weeksHb rise Exercise
durationHb rise
Deaths
Darbepoietin group(n = 162)
1.8g/dl +57.3 secs
+2.1g/dl
11(7%)
Placebo group(n = 157)
0.3g/dl +46.5 secs
+0.5g/dl
18 (11%)
Circulation. 2008;117:526-535

RED-HF trial (Reduction of Events by Darbepoetin Alfa in Heart Failure)
March 28, 2013N Engl J Med 2013;368:1210-19

Darbepoetin alfa group (target hemoglobin 13.0 to 14.5 g/dL)N = 1200
Placebo groupN = 1200
Study Population•Hemoglobin 9 to 12 g/dL•LVEF ≤ 35%•NYHA Class II to IV
Approximately 620 global sites
1:1 randomization
Timelines
Event driven: ~1150 eventsStudy End September 1 2012
Began enrolling June 2006
Site Evaluation & Selection
Follow-up
RED-HF trial

KCCQ primary analysis: Change from baseline to month 6
KCCQ Symptom Frequency Score Mean Change From Baseline to Month 6
0
1
2
3
4
5
6
7
8
9
10
6.20
3.91
2.4695% CI: (0.90,
4.02)
P = 0.011
Chan
ge fr
om B
asel
ine
in K
CCQ
Sy
mpt
om F
requ
ency
Sco
reDarbepoetin
alfa (n = 925)
Placebo(n = 927)
Mixed effects model estimating treatment effect adjusted for region, type of device, and baseline KCCQ score; scale scores range from 0 to 100, with higher scores indicating better functioning.
KCCQ Overall Summary Score Mean Change From Baseline to Month 6
0123456789
10
6.68
4.48
2.2095% CI: (0.65, 3.75)
P = 0.005
Chan
ge fr
om B
asel
ine
in K
CCQ
O
vera
ll Su
mm
ary
Scor
e
Placebo(n = 929)
Darbepoetin alfa
(n = 928)

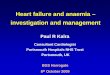
Primary outcome: All cause death or first hospitalization for worsening heart failure
Years of Randomization
Prop
. of S
ubje
ct W
ith
Even
t (%
)
Subjects at risk:
11361142
975956
855818
712695
581591
473497
385395
281290
212211
161154
10192
Stratified Log-rank, p = 0.87
PlaceboDarbepoetin alfa
100
80
60
40
20
00 1 2 3 4 5

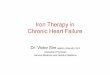
Selected adverse events of interestn (%)
Darbepoetin alfa(N = 1133)
Placebo(N = 1140)
Risk difference (95% CI) p-value
Ischaemic cerebrovascular conditions 51 (4.5) 32 (2.8) 1.7 (0.2, 3.2) 0.031
Embolic and thrombotic events 153 (13.5) 114 (10.0) 3.5 (0.9, 6.1) 0.009
Hypertension 81 (7.1) 69 (6.1) 1.1 (-0.9, 3.1) 0.292
Malignancies 69 (6.1) 68 (6.0) 0.1 (-1.8, 2.1) 0.900
Hypersensitivity reactions 99 (8.7) 96 (8.4) 0.3 (-2.0, 2.6) 0.787
Conclusion: Treatment with darbepoetin alfa did not improve clinical outcomes in patients with systolic heart failure and mild to moderate anemia. Our findings do not support use of DA in HF.

IV Iron Therapy for anemia in HF
Table 1 Randomized, controlled studies with intravenous iron in patients with heart failure

FAIR-HF trial
Anker SD et al. N Engl J Med 2009;361:2436–48

FAIR HF Trial
Aim To determine whether treatment with IV iron (ferric
carboxymaltose) would improve symptoms in patients who had HF, reduced LV function, and iron deficiency either with or without anemia.
Anker SD et al. N Engl J Med 2009;361:2436–48

MethodStudy design: A randomized, double-blind, multicenter study.
Study population: N= 459 patients. NYHA class II or III, a LVEF of 40–45% or less, a Hb from 9.5 to 13.5 g/dL and iron deficiency..
Treatment regimen: 4 ml Ferric carboxymaltose or saline was administered. Weekly injections were continued until Fe was repleted( usually within 8 weeks) and then at 4 weekly intervals upto 24 weeks.
End point: The primary end point was a self-reported Patient Global Assessment (PGA) form and NYHA functional class in the 24th week.
Safety end points were serious and non-serious adverse effects, hospitalization and death up to the 26th week of study.
The FAIR-HF trial
Anker SD et al. N Engl J Med 2009;361:2436–48

Result
The evaluation of PGA forms showed much or moderate i.e., around 50% improvement in the ferric carboxymaltose group as compared to the 28% in the placebo group. 47% in the ferric carboxymaltose group had NYHA functional class I or II as compared to 30% in the placebo group.
Anker SD et al. N Engl J Med 2009;361:2436–48

Anker SD et al. N Engl J Med 2009;361:2436–48

Anker SD et al. N Engl J Med 2009;361:2436–48

Anker SD et al. N Engl J Med 2009;361:2436–48

Anker SD et al. N Engl J Med 2009;361:2436–48

The administration of ferric carboxymaltose in patients with chronic heart failure and iron deficiency with or without anemia was beneficial.
Anker SD et al. N Engl J Med 2009;361:2436–48

FAIR HF Trial
Conclusion Ferric carboxymaltose for a period of 24 weeks in patients with chronic
heart failure and Fe deficiency with or without anemia showed improvement in the symptoms, functional capacity and the QoL.
No additional side-effects were observed during this time-span. This treatment was beneficial to both patients with and without anemia.
Anker SD et al. N Engl J Med 2009;361:2436–48

CONFIRM HF Trial

A multi-centre, double-blind, placebo-controlled trial.N= 304 patientswith LVEF ≤ 45%, elevated natriuretic peptides, and Fe
deficiency (ferritin <100 ng/mL or 100–300 ng/mL if transferrin saturation ,20%).
FCM, n = 152 or placebo (saline, n =152) for 52 weeks given.
FCM significantly prolonged 6MWT distance, improvement in NYHA class, PGA, QoL, and Fatigue Score at Week 24 and was sustained to Week 52.
Treatment with FCM was associated with a significant reduction in the risk of hospitalizations for worsening HF [ P = 0.009]. The number of deaths (FCM: 12, placebo: 14 deaths) and the incidence of adverse events were comparable between both groups.

CONFIRM HF Trial
Conclusion: Treatment of symptomatic, Fe-deficient HF patients with FCM over a 1-year period resulted in sustainable improvement in functional capacity, symptoms, and QoL and may be associated with risk reduction of hospitalization for worsening HF.

RECOMMENDATIONS

Practical Tip: Symptomatic patients with low transferrin and/or ferritin levels should be considered for supplementary iron therapy principally with a goal of improving symptoms
Anemia recommendations
We suggest that for patients with documented iron deficiency, oral or intravenous iron supplement be initiated to improve functional capacity (Weak Recommendation, Low-Quality Evidence).
Values and Preferences:The iron supplement recommendation was derived mostly from the experience of clinicians, small clinical trials, and 2 large randomized controlled trials (RCTs).
Recommendation

EPO recommendation
Values and Preferences:The recommendations against the use of erythropoiesis-stimulating agents (ESAs) were derived from robust data from RCTs.
RecommendationWe recommend erythropoiesis stimulating agents not be routinely used to treat anemia in HF (Strong Recommendation, High-Quality Evidence).

Take Home MessageAnemia is a independent predictor of morbidity and mortality of
HF.
Anemia has emerged as a possible treatment target in HF.
ESPs is a major concern for safety in HF patients.
ESPs should not be used routinely in HF.
For patients with documented Fe deficiency, oral or intravenous iron supplement may be initiated to improve functional capacity.
Larger controlled clinical trials are needed for further information and therapy guidelines.