Embed Size (px)
Citation preview

Adaptive Research in Practice:
Running Tighter, Faster Studies
Michael Rosenberg, MD, MPH
CEO/President
Health Decisions Inc

2
Disclaimer
• The views and opinions expressed in the following PowerPoint slides are those of the individual presenter and should not be attributed to Drug Information Association, Inc. (―DIA‖), its directors, officers, employees, volunteers, members, chapters, councils, Special Interest Area Communities or affiliates, or any organization with which the presenter is employed or affiliated.
• These PowerPoint slides are the intellectual property of the presenter’s organization and are protected under the copyright laws of the United States of America and other countries. Used by permission. All rights reserved. Drug Information Association, DIA and DIA logo are registered trademarks or trademarks of Drug Information Association Inc. All other trademarks are the property of their respective owners.
3
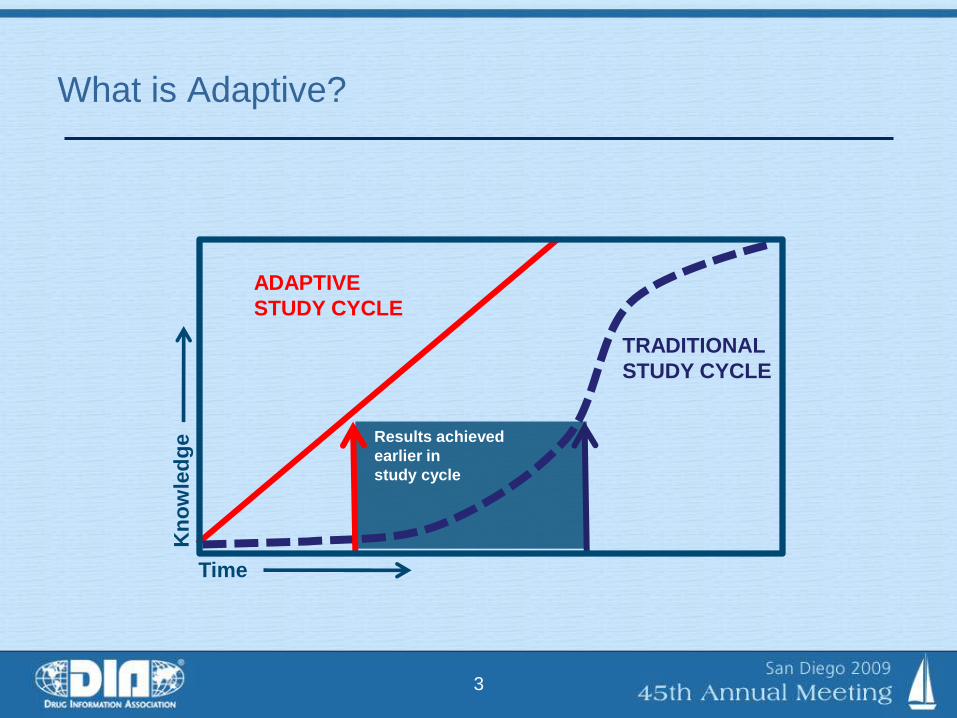
What is Adaptive?
ADAPTIVE
STUDY CYCLE
Results achieved
earlier in
study cycle
TRADITIONAL
STUDY CYCLE
Kn
ow
led
ge
Time
4
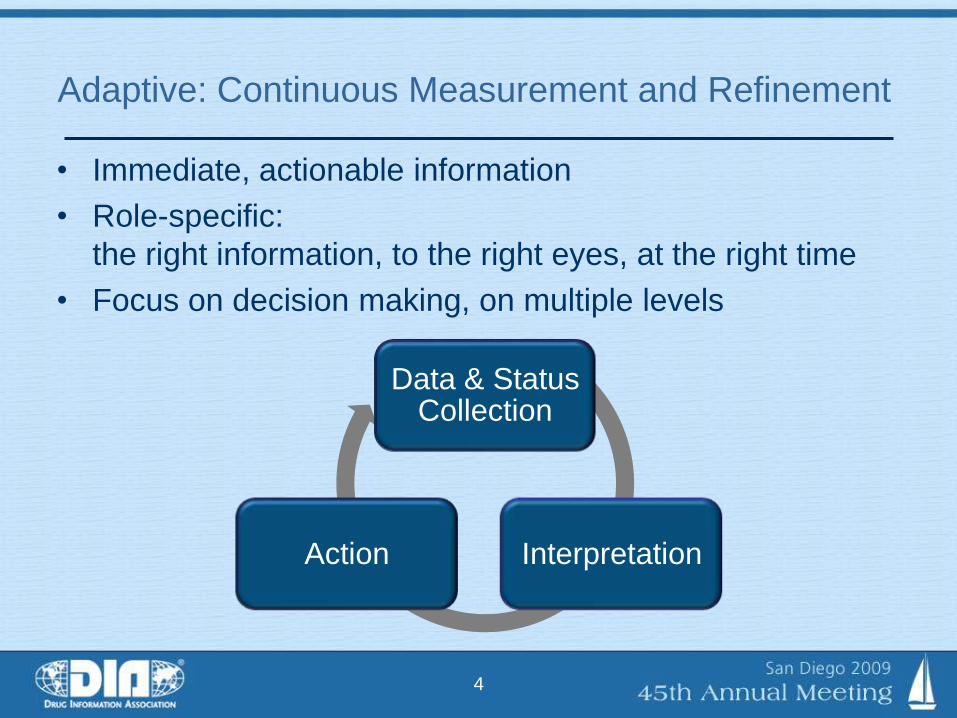
Adaptive: Continuous Measurement and Refinement
• Immediate, actionable information
• Role-specific:
the right information, to the right eyes, at the right time
• Focus on decision making, on multiple levels
Data & Status Collection
InterpretationAction

Adaptive
Design
5
Adaptive Design plus Adaptive Operations
Design adaptations
Study Timeline
Traditional

Adaptive
Design
6
Adaptive Design plus Adaptive Operations
Design adaptations
Operational adaptations
Study Timeline
TraditionalAdaptive
Design &
Operations

7
Traditional Process
Adaptive/Agile Process

8
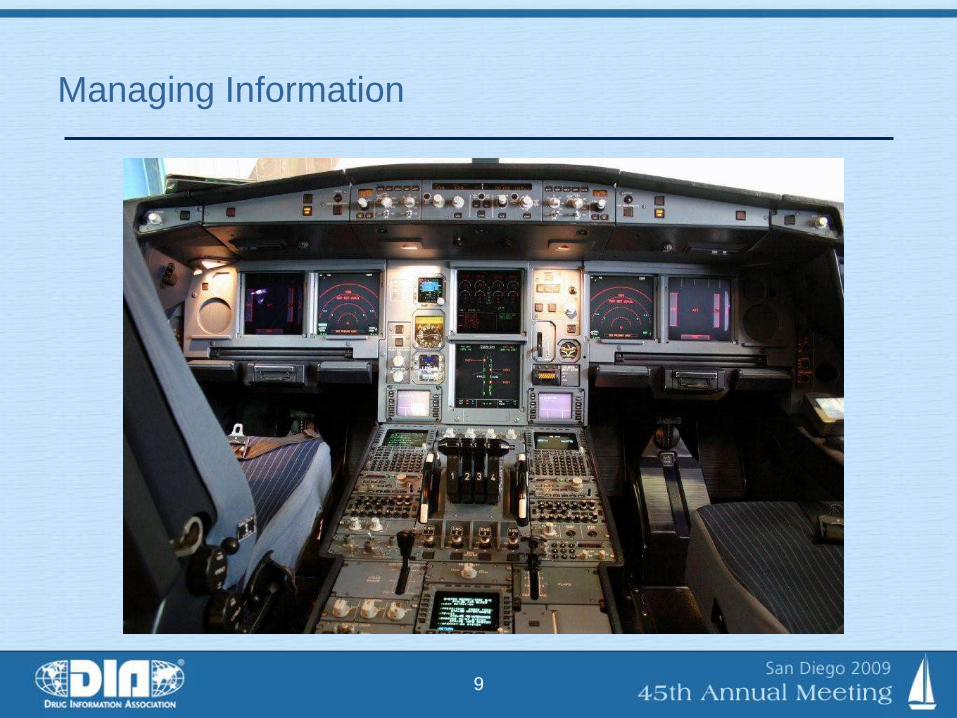
Managing Information
9
Managing Information

10
Common Pain Points
Traditional Agile
Enrollment (% on time) 15% 76%
Database lock (weeks) 10+ <2
Monitoring (# visits) X X/2
Waste (queries/100 fields) 5-7 web; 15+ paper 1

11
Real Results
• Rescue (renal)
– Target of 140 pts; in 6 mo, 14 enrolled
– Agile was implemented with new systems; in 6 mos, 140 pts
• Pivotal (CNS / Alzheimer’s)
– Study run under Agile completed ~1 yr ahead of companion
study run under conventional program—avg 96 pts/mo
• Registration (Oncology / mBrCa)
– Product brought to marked one year ahead of schedule
– Main contributors were speed of enrollment (31.7 pts/mo), SSRE
• Registration (device)
– 4,000 subjects completed three months ahead of schedule

12
A Simple Adaptation: Sample Size Re-Estimation
• Planning is done with estimates that are always wrong—
only question is how much off
• Implications are profound, ranging from failure of study
to overbuilding and wasted resources
• SSRE allows size to be checked during study using
actual data to date

13
The Cost of Not Doing SSRE
δ less
δ less
δ equal
δ equal
δ greater
δ greater
No SSRE
SSRE
0.33
0.33
0.33
OUTCOMERelative
to SSRE
COST(m)
Probability
weighted
Failure
Success
Success
- $5
- $1
- $2
- $1.65
- $0.34
- $0.66
- $2.7
Total
Success
Success
Success
$5
$5
$5
$5
$4
$3
0.33
0.33
0.33
Assumes study cost $5m, 20% buffer in non-SSRE, fixed and linear subject cost, 20% difference in δ

14
$0.0
$1.0
$2.0
$3.0
0 0.1 0.2 0.3
Probability of Effect Size (δ) Differing from Planned by >20%
Ad
dit
ion
al
co
st
of
no
SS
RE
(m
)The Cost of Not Doing SSRE
15
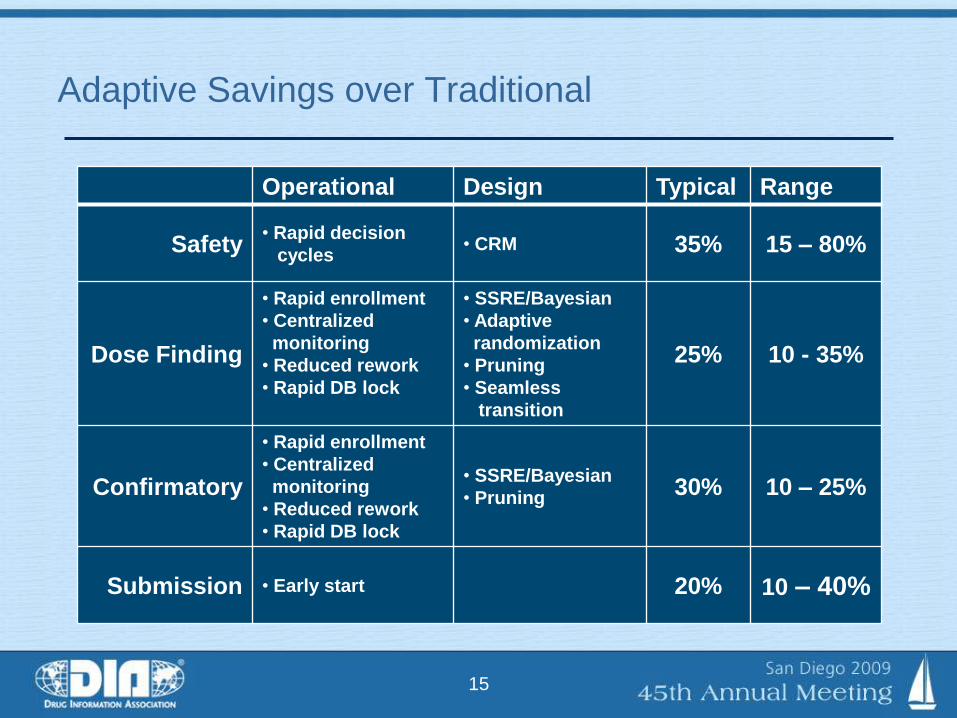
Operational Design Typical Range
Safety• Rapid decision
cycles• CRM 35% 15 – 80%
Dose Finding
• Rapid enrollment
• Centralized
monitoring
• Reduced rework
• Rapid DB lock
• SSRE/Bayesian
• Adaptive
randomization
• Pruning
• Seamless
transition
25% 10 - 35%
Confirmatory
• Rapid enrollment
• Centralized
monitoring
• Reduced rework
• Rapid DB lock
• SSRE/Bayesian
• Pruning30% 10 – 25%
Submission • Early start 20% 10 – 40%
Adaptive Savings over Traditional

16
Trial & Program Time Savings (months)

17
Getting Started with Agile
• Get informed on adaptive options
• Design RFP to encourage better approaches
• Leverage CRO expertise in creating a
customized trial
• Demand transparency at operational level; it
means control and your ability to make better,
faster decisions
• Build capabilities progressively; can start slowly

18
An Unprecedented Opportunity
• Adaptive, agile tools are here today, tested, and
robust
• The opportunities are enormous; greater than
ever experienced in our industry
• Adaptive design elements as appropriate;
adaptive operational elements are universal
• Bottom line are for consistent time and cost of
projects—10-50% reduction

19
If you want the same results,
keep doing the same thing.