- 1. Acute Promyelocytic Leukemia Ranjita Pallavi,MD Internal
Medicine PGY-2
2. Acute Promyelocytic Leukemia FAB: AML M3 WHO 2008: AML with
recurrent genetic abnormalities APL with
t(15;17)(q22;q12);(PML-RARA) 10-15% of all AML cases (~1300/year in
US) 80-90% cure rate, though morbidity and mortality is high before
and during induction Disseminated intravascular coagulation
relatively common at diagnosis Highly sensitive to anthracyclines
t(15;17) and PML-RARa fusion gene required All-trans retinoic acid
(ATRA) targets RARa Arsenic trioxide (ATO) targets PML Patients
have high cure rates, once they survive induction 3. Molecular
Features of APL PML/RARa gene product forms homodimer Homodimer
represses target genes needed for differentiation Mechanisms act
via aberrant histone modification and DNA methylation Mechanism of
ATRA: ATRA causes a conformational change of the PML/RARa protein
Downstream targets that had been repressed become activated,
leading to normal differentiation Wang, Blood, 2008 4. Acute
Promyelocytic Leukemia Without treatment, APL is the most malignant
form of AML with a median survival of less than one month. Modern
therapy has dramatically changed its prognosis and APL is now
associated with the highest proportion of AML patients who are
cured of their disease. APL represents a medical emergency with a
high rate of early mortality, due mainly to hemorrhagic
complications from a characteristic coagulopathy. The first golden
rule that has to be followed as soon as the diagnosis of APL is
suspected based upon cytologic criteria is: to immediately start
treatment with all-trans retinoic acid (ATRA) without delay, even
before definitive (cyto)genetic confirmation of the diagnosis has
been made. If the diagnosis is not confirmed, ATRA can always be
discontinued and treatment changed to that used for other types of
AML. 5. A review of blasts 6. APL morphology: Hypergranular
Tallman, Blood, 2009 7. APL Morphology: Microgranular Tallman,
Blood, 2009 8. The Action of Differentiation Wang, Blood, 2008 9.
Treatment Approaches Can the patient tolerate anthracyclines? What
is the risk-stratification based on the Sanz criteria? (WBC and
platelet count) Induction Consolidation Maintenance Relapse Several
established treatment protocols Important not to mix and match
induction from one trial with consolidation from another 10. Risk
Stratification Low: WBC < 10,000 and platelets > 40,000
Intermediate: WBC < 10,000 and platelets < 40,000 High: WBC
> 10,000 Sanz, Blood, 2000 11. Treatment Guidelines 12.
Treatment Guidelines 13. Treatment Guidelines 14. Treatment
Guidelines 15. Treatment Guidelines 16. APL and DIC APL associated
with significant coagulopathy. Coagulation parameters (fibrinogen,
FDP/XDP, PT, aPTT, and platelet counts) should be monitored
closely. Transfusions of platelets or fresh frozen plasma are
traditionally used to maintain the platelet count above 20,000 to
30,000/L and the plasma fibrinogen concentration above 150 mg/dL.
Heparin must not be used for prophylaxis in this setting. In case
of life-threatening bleeding, inhibitors of fibrinolysis should be
considered. Invasive procedures such as central venous
catheterization, lumbar puncture, and bronchoscopy should be
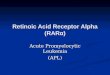
avoided before and during induction remission. 17. ATRA and
Coagulopathy 18. ATRA and Coagulopathy Principal pathways of APL
cell interactions with the hemostatic system, which can be affected
by ATRA. APL cell expresses: (a) cellular procoagulants (TF and CP)
that activate the clotting cascade; ATRA decreases the expression
of both TF and CP, thus reducing the procoagulant activity; (b)
fibrinolysis proteins (u-PA, t- PA, PAI) and receptor (u-PAR); ATRA
increases both plasminogen activators and inhibitors, resulting in
unchanged or reduced fibrinolytic activity; (c) nonspecific
proteases, including granule elastase, that proteolyze
fibrinogen/fibrin and other coagulation factors; ATRA does not
affect this cellular mechanism; and (d) cytokines, including IL-1
and TNF-, that induce the endothelium thrombogenicity; ATRA
increases the production of cytokines. 19. Coagulation markers in
newly diagnosed APL patients (n=9) receiving ATRA for induction
therapy. Barbui T et al. Blood 1998;91:3093-3102 1998 by American
Society of Hematology 20. Differentiation Syndrome Previously named
Retinoid acid syndrome Occurs in 1025% of APL patients within 2 to
21 days after initiation of treatment. More frequently in patients
with a high white blood cell count at diagnosis. Characterized by
fever, peripheral edema, pulmonary infiltrates, hypoxemia,
respiratory distress, hypotension, renal and hepatic dysfunction,
and serositis resulting in pleural and pericardial effusions.
Symptoms of fever, hypotension, dyspnea, and pulmonary infiltrates
can mimic sepsis. Sometimes, the syndrome is accompanied by
hyperleukocytosis Early recognition and aggressive management with
dexamethasone therapy (10 mg IV every 12 hours for 3-5 days with a
2 week taper ) has been effective in most patients. Continue to
hold ATRA till symptoms resolv.e ATRA or ATO can be restarted in
most cases once the syndrome has resolved. 21. Differentiation
Syndrome 22. Differentiation Syndrome 23. Hyperleucocytosis Marked
increase in WBC count due to the rapid maturation induced by ATRA
of a large mass of leukemic cells, may result in leukostasis. Most
current remission induction regimens now combine ATRA with
cytotoxic chemotherapy, the frequency of hyperleukocytosis has
decreased. 24. Pseudotumour Cerebri Idiopathic intracranial
hypertension (IIH), commonly called pseudotumor cerebri, can
complicate the treatment of APL with ATRA. More common in children
and adolescents treated with ATRA and the incidence in this
population decreased with the use of lower dose ATRA (25
mg/m2/day). Diagnosis of IIH is suspected in patients with
headache, papilledema, and/or vision loss. Evaluation includes a
physical examination including lumbar puncture, cerebral imaging
studies (computed tomography or magnetic resonance) and fundus
oculi. diagnosis is confirmed in patients with increased
intracranial pressure, normal cerebrospinal fluid, and negative
cerebral imaging studies. If symptoms persist, therapeutic options
include the temporary discontinuation or dose reduction of ATRA,
analgesics, and/or the administration of steroids and
acetozolamide. 25. Management of special situations: Pregnant Women
Treatment approach depends largely upon the trimester of pregnancy
during which APL is diagnosed. First Trimester: Both ATRA and ATO
are considered to be highly teratogenic and are contraindicated
during the first trimester of pregnancy. if elective termination of
the pregnancy is unacceptable to the patient, the only available
treatment option is the administration of chemotherapy alone. If
treatment with chemotherapy alone is chosen, daunorubicin may be
the preferred anthracycline for pregnant women because there is
greater experience with this drug during pregnancy. If a remission
is achieved and the pregnancy continues normally, ATRA may be added
during the second or third trimester. 26. Management of special
situations: Pregnant Women Second or Third Trimester: Two main
options are available: 1.Remission induction with ATRA alone and
chemotherapy postponed until after delivery. 2.Simultaneous
administration of ATRA plus chemotherapy. Simultaneous
administration of ATRA plus chemotherapy offers the best chance of
cure. Vaginal delivery is generally preferred since it is
associated with a reduced risk of bleeding. After delivery,
breastfeeding is contraindicated while on chemotherapy or ATO. 27.
Management of special situations: Therapy related APL Develops
usually less than 3 years after a primary neoplasm (especially
breast carcinoma). Particularly with topoisomerase IItargeted drugs
(anthracyclines or mitoxantrone and less often etoposide). t-APL
appear to have a similar prognosis as de novo APL and benefit from
standard APL therapy. In patients with a history of anthracycline
exposure or cardiac impairment that limits their ability to receive
further treatment with anthracyclines, alternative regimens, such
as ATRA plus ATO may be used. 28. Management of special situations:
Genetic variants of APL More than 90% of patients with APL have
t(15;17)(q22;q12) translocation resulting in the PML/RARA fusion
gene. Very rarely have been described alternative fusion genes
resulting in leukemias classified as "AML with a variant RARA
translocation" Some of these conditions are sensitive to ATRA
therapy while others are not. In general, patients with alternative
fusion genes ATRA-sensitive are treated with standard ATRA-based
therapy. Patients with variants known to be resistant to ATRA are
treated with standard AML induction therapy. 29. Management of
special situations: Genetic variants of APL The following are the
alternative fusion genes identified as ATRA- sensitive: NuMA/RARA
and t(11;17) NPM1/RARA and t(5;17) FIP1L1/RARA The following are
ATRA-resistant variants: STAT5b/RARA and interstitial chromosome 17
deletion PLZF/RARA and t(11;17) In case APL patients have
additional cytogenetic abnormalities, as trisomy 8, or particular
molecular abnormalities (gene mutations in FLT3) the prognosis is
not worsened and they are considered to have the same prognosis as
standard APL.