Embed Size (px)
Citation preview

JIONG HU, MDShanghai, China
• Hematologist and a clinical researcher in the Department of Hematology at Rui Jin Hospital, Shanghai, China
• Dr. Jiong Hu has published in several national and international peer reviewed journals on topics including hematopoietic stem cell transplantation, leukemia, hematological malignancies, and hematopathology. Dr. Hu is a pioneer in actute promyelocytic leukemia and his research interests include myeloma and leukemia. He is a principal investigator for several national level clinical trials. Dr. Hu holds the position of Lead, Leukemia Subdivision for APHCON.

Long term survival outcomes of APL:
How will we treat APL in the
future?Jiong HU
Shanghai Institute of Hematology, Department of Hematology, Rui-Jin Hospital, Shanghai Jiao Tong
University School of Medicine

• Overview
• Front-line combination therapy with ATRA and
arsenic
• Future direction:
- Oral arsenic
- APL therapy without chemotherapy

Overview of APL treatment
• pre-ATRA period: chemotherapy
• ATRA:
- introduction of ATRA
- optimization of ATRA-chemo combination regimens
• Arsenic:
- introduction of ATO in relapsed APL
- ATRA/ATO combination as front-line therapy
- Oral arsenic

Blood 2008 Mar 1;111(5):2505-15.
ATRA + chemotherapy in APL- Chemotherapy + ATRA:
anthracycline (Ida, DNR, Mitoxantrone, or HHT) and Ara-C
- Induction:
high remission rate
reduce differentiation syndrome
- Consolidation/maintenance:
3 monthly courses of anthracycline-based chemo/low-dose
maintenance (6-MP+MTX with ATRA)
5-year EFS/DFS: up to 70%

ATRA + chemotherapy improve outcome
Tallman M, Blood 2009;114(25):5126

Arsenic as salvage therapy
- arsenic developed as TCM in Northeastern China
- Harbin group(1992): iv 1% ATO
32 APL, 21 obtained CR
10-year survival 30%
- SIH(1996~1997):
47 relapsed and 11 newly diagnosed APL
CR rate of 85.1% and 72.7%
molecular remission documented ~60%
long-term survival in relapsed APL: 50~60%
Blood 2008 Mar 1;111(5):2505-15.

Treatment of APL: guidelines
ELN guideline / NCCN guideline / Consensus of CSH:
- Newly-diagnosed APL: simultaneous administration of
ATRA and anthracycline-based chemotherapy as standard
- Relapse disease: arsenic is the best option with or without
chemotherapy
Blood 2009;113:1875Chin J Hematol 2010;31:69

Rationale of arsenic and ATRA combination as front-line treatment
- ATRA/arsenic: efficacy in newly-diagnosed and relapse
patients with high remission rate with sizable proportion of long-
term survival
- front-line ATRA with salvage arsenic: long-term survival
observed

Rationale of arsenic and ATRA combination: Synergy in degrading PML-
RARα

ATRA increase aquaglyceroporin 9(AQP9) expression associated with
arsenic sensitivity
Relationship of AQP9 with arsenic uptake and sensitivity in leukemia cells. Blood 2007; 109: 740-746.
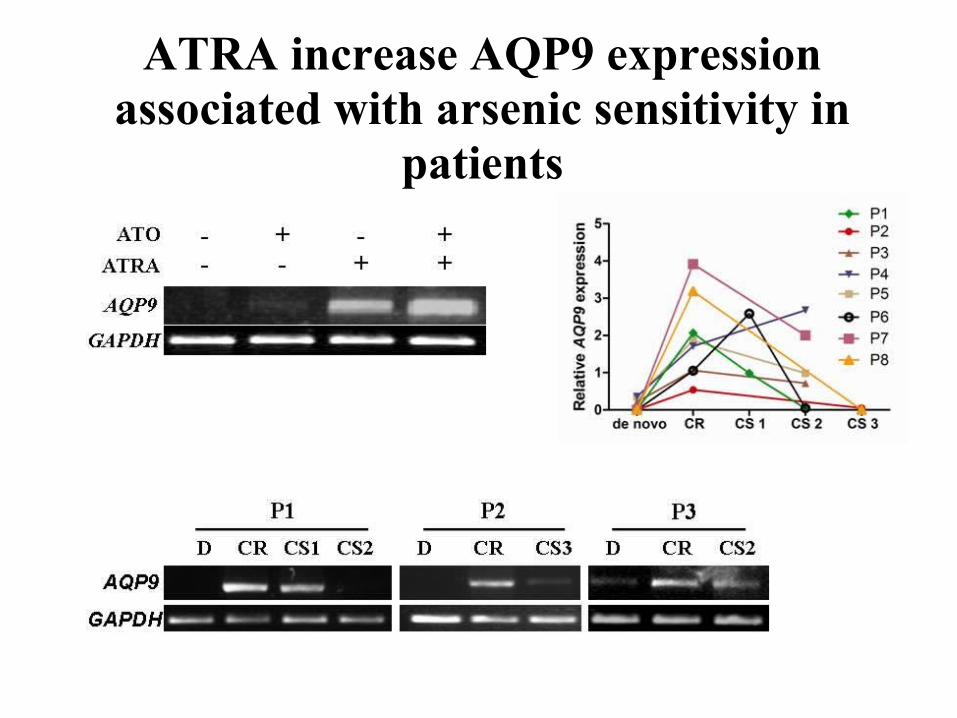
ATRA increase AQP9 expression associated with arsenic sensitivity in
patients

ATRA and arsenic synergy in targeting APL
- ATRA/Arsenic targeting PML-RARα
- ATRA ↑ of expression of AQP9, ↑ arsenic uptake
- Degradation PML-RARα rapidly clears LIC and eradication
in murine APL models; blocked PR degradation by
bortezomib reversed the curative effect of arsenic
Nat Med. 2008;14:1333Clin Cancer Res 2009 Oct 6.
Synergy of ATRA and arsenic in eradicating leukemia stem cells
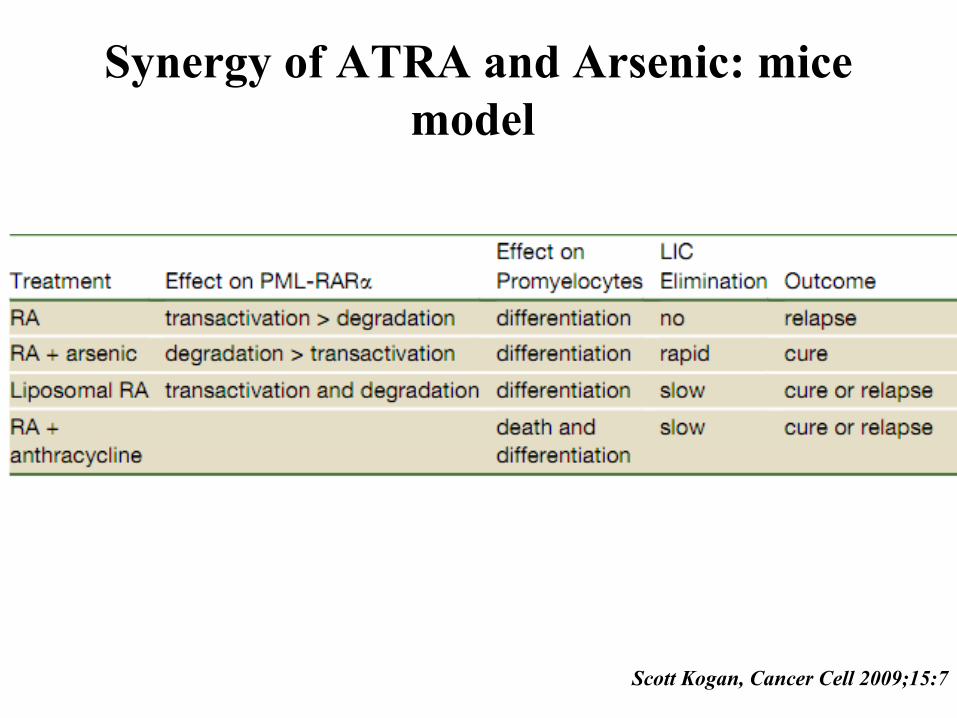
Synergy of ATRA and Arsenic: mice model
Scott Kogan, Cancer Cell 2009;15:7
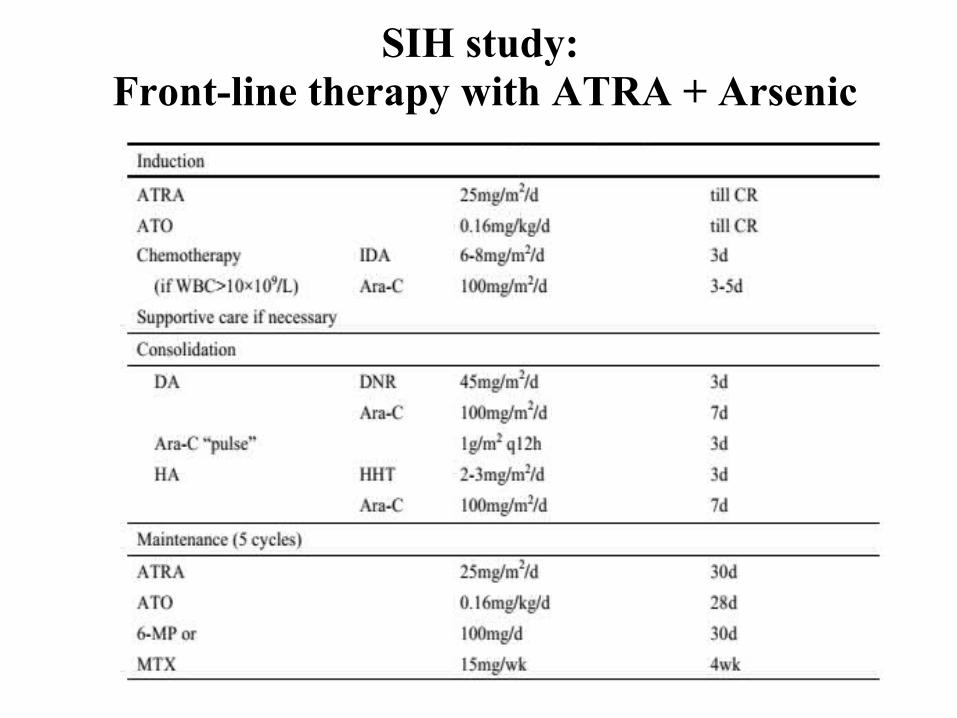
SIH study: Front-line therapy with ATRA + Arsenic

Overall survival at 70 months Event-free survival at 70 months
n=85, 91.7±3.0% n=85, 89.2±3.4%
Hu J, PNAS 2009;106:3342
SIH study: Follow-up for all patients

Overall survival at 70 months Relapse-free survival at 70 months
n=80, 97.4±1.8% n=80, 94.8±2.5%
Hu J, PNAS 2009;106:3342
SIH study: Follow-up for patients in CR

Hu J, PNAS 2009;106:3342
SIH study: safety of front-line arsenic therapy
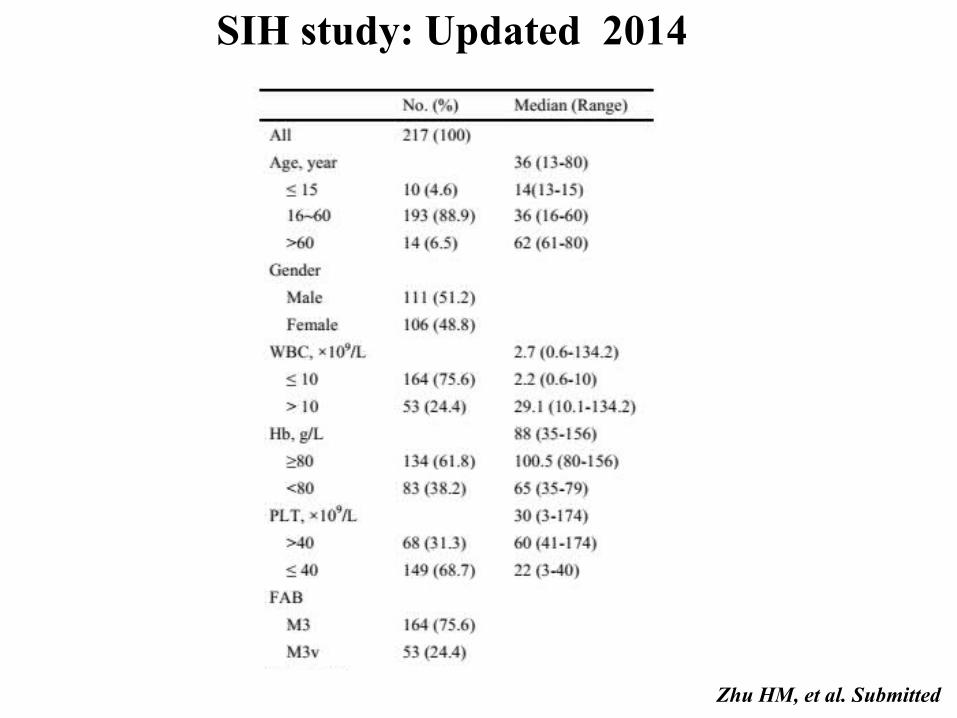
SIH study: Updated 2014
Zhu HM, et al. Submitted

Zhu HM, et al. Submitted
SIH study: Updated 2014

SIH study updated 2014: all patients
Zhu HM, et al. Submitted
median follow-up 72 months (range, 0-136)

SIH study: Updated 2014

SIH study: Updated 2014
Zhu HM, et al. Submitted

Mean 95%CI
Global Health Status 79.2 76.0~ 82.5Functional Scale 92.7 91.0~ 94.5Symptom Scale 6.9 5.3~ 8.5
Main Complaints Percentage
Mild to Moderate Weakness 55.4%
Difficulty remembering things 41.1%
Financial Difficulties 33.0%
EORTC QLQ-C30 (version 3.0) based Questionnaire was performed for evaluation of quality of life.
Scores were analyzed according to the EORTC QLQ-C30 scoring manual.
Zhu HM, et al. Submitted
SIH study updated 2014: Quality of Life

Conclusion of long-term follow-up
Good Long-term SurvivalGood Long-term Survival• Particularly for low-to-intermediate risk patients
Few Long-term ComplicationsFew Long-term Complications• Except for liver dysfunction and hepatic steatosis
No Significant Arsenic RetentionNo Significant Arsenic Retention• Back to normal after 6 months off ATO at most
Satisfactory Quality of LifeSatisfactory Quality of Life
Zhu HM, et al. Submitted

- No chemotherapy for low/Int risk APL
outcome of minimal chemo or no chemo regimen
ongoing study
- Oral arsenic
outcome of initial studies
ongoing study
… future direction …

Ravandi F, J Clin Oncol 2009;27:504
MDACC Study: ATRA + Arsenic ± GO

Ravandi F, J Clin Oncol 2009;27:504
MDACC Study: ATRA + Arsenic ± GO

3 cycles of ATRA + ATO in induction/consolidation; 1 cycle of idarubicin in induction
Iland HJ, Blood. 2012;120(8):1570-1580
ATRA/ATO reduce significantly use of chemotherapy: Australian APML4 study

ATRA/ATO reduce significantly use of chemotherapy: Australian APML4 study
2-year relapse-free survival 97.5%; failure-free survival 88.1%, and overall survival 93.2%.
Iland HJ, Blood. 2012;120(8):1570-1580

ATRA + ATO vs. AIDA in newly-diagnosed non high-risk APL: Gimema-SAL-AMLSG
ASH 2012, Plenary Scientific Session
ATRA+ATO AIDA P
CR 75/75 (100%) 75/79 (95%) 0.12
2 year EFS 97% (93.1-100) 86.7% (80.3-93.6) 0.03
Event 1 death in CR; 2 rel 7 deaths (4 ED/3 in CR) ; 4 rel
OS 98.7% 91.1% 0.03
DFS 97% 91.6% (P=0.19) 0.19
CIR 1.6% 4.3% 0.41
• Patients: -162 enrolled 154 evaluable- median age 45.3(18.7-70.2); median WBC 1.50 x 109/L- risk: 61.8% intermediate and 38.2% low-risk- median FU: 31 months (range 0.07-50.4)

ASH 2012, Plenary Scientific Session
ATRA + ATO vs. AIDA in newly-diagnosed non high-risk APL: Gimema-SAL-AMLSG
For newly diagnosed non-high-risk APL, the front-line chemo-free ATO+ATRA therapy is at least not inferior to
AIDA in terms of 2 year EFS.
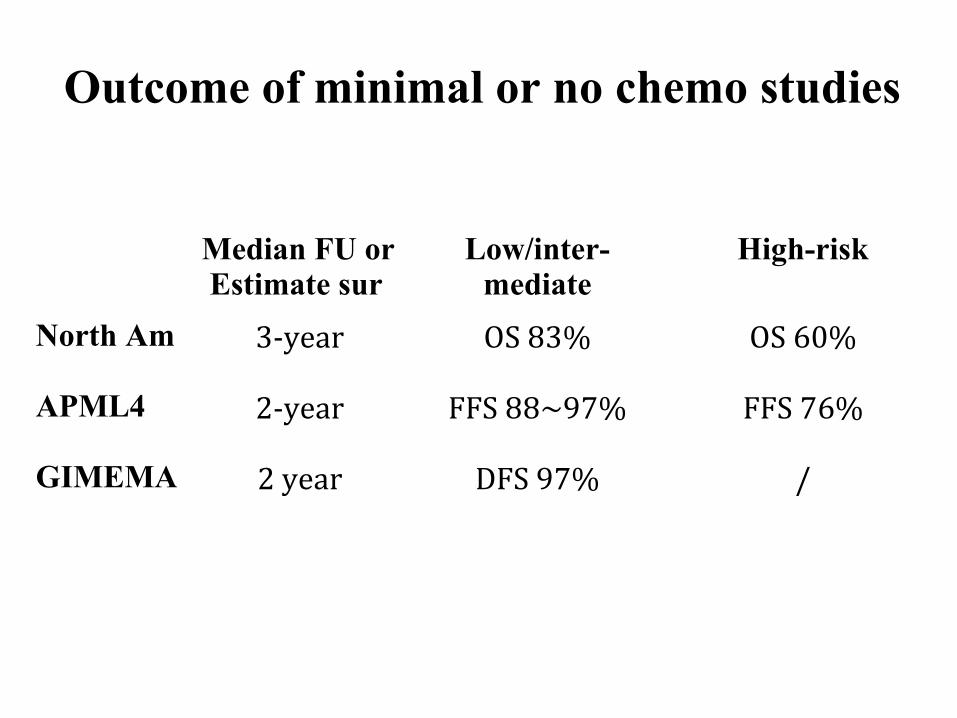
Outcome of minimal or no chemo studies
Median FU or Estimate sur
Low/inter-mediate
High-risk
North Am 3-year OS 83% OS 60%
APML4 2-year FFS 88~97% FFS 76%
GIMEMA 2 year DFS 97% /
• Chinese 863 Key program: multiple-center randomized study
• Newly-diagnosed APL
• Risk stratification: low/int-risk vs. high-risk
- Low/Int-risk: ATO replacing chemotherapy ?
- high- risk: ATO replace Ara-C
• 20 clinical centers: enrolled from Aug 2012 to Aug 2015
Ongoing study

Oral Arsenic trioxide in China: oral As2O3
Au WY et al. Blood. 2011;118(25):6535-6543
• Retrospective analysis of 76 APL in 1st CR
• Treatment:
- Induction/consolidation: daunorubicin and Ara-C
- Maintenance: oral arsenic trioxide based regimen
oral ATO (10 mg/day);
oral ATO + ATRA(45mg/m2);
oral ATO + ATRA + ascorbic acid (1000 mg/day)
given 2 weeks every 2 months for 2 years

Au WY et al. Blood. 2011;118(25):6535-6543
Develop of oral Arsenic trioxide in China: oral arsenic trioxide
• Median follow-up of 24 months (range, 1-115 months):
- relapse only in 8 patients; 3-year LFS and OS: 87.7% and
90.6%

Blood 2002 May 1;99(9):3136-43.
newly diagnosed Rel1 CR
No of pts 19 7 103
Follow-up 13.5 mths (2~40) / 23 mths(2~71)
Mol remission 14/16 5/7 35/44
1-year DFS 86.1% / 96.7%
3/6-year DFS 76.6% / 87.4%
- Retrospective study: - 50 mg/kg daily (750mg 4 times) until CR; post-remission pts: 2
weeks on and 2 weeks off in 1st year and every 2 months for 4
years
Develop of oral Arsenic trioxide in China: Crystallized realgar (high-purity As4S4)

Blood 2002 May 1;99(9):3136-43.
Develop of oral Arsenic trioxide in China: Crystallized realgar (high-purity As4S4)

Realgar-Indigo Naturalis Formula (RIF; As4S4) vs. ATO: Multi-Center Randomized Trial APL07
Newly-diagnosed APL
Zhu et al, J Clin Oncol. 2013 Nov 20;31(33):4215-21.
oral RIF (60 mg/kg) vs. ATO (0.16 mg/kg)

RIF iv ATO p n=112 n=121
CR 98% 98% >0.05Time to CR 30 days 29 days >0.05 PML/RARα level CR 15.0% 2.1% <0.05 End consolidation 0 0 >0.05 Mol CR 100% 100% >0.05Median Time to Mol CR 60 days 60 days >0.05 Relapse 0.9% 0.8% >0.05
Bei Jin University, Institute of Hematology
Zhu et al, J Clin Oncol. 2013 Nov 20;31(33):4215-21.

Bei Jin University, Institute of Hematology
Zhu et al, J Clin Oncol. 2013 Nov 20;31(33):4215-21.

Bei Jin University, Institute of Hematology
Oral Realgar-Indigo naturalis formula yielded comparable high remission and long-term survival with ATO in newly
diagnosed APL.
Zhu et al, J Clin Oncol. 2013 Nov 20;31(33):4215-21.

… future direction …
Zhu et al, NEJM 2014( Dec4);371;23
• Single center pilot study with 20 patients with non high-risk APL
• Protocol:
Induction:
- oral arsenic RIF (60mg/kg)
- ATRA (25mg/m2)
Post-remission therapy:
- RIF 4 weeks on and 4 weeks off
- ATRA 2 weeks on and 2 weeks off for 7 months.

… future direction …
Zhu et al, NEJM 2014( Dec4);371;23

… future direction …
Zhu et al, NEJM 2014( Dec4);371;23
- Complete molecular remission: 100% at 6 months
- Excellent QOL: 50% of patients without hospitalization
- Total medical costs: $4,675 (range, $3,174 to $12,698).

• Combination of ATRA and arsenic as front-line treatment
improve the outcome of APL: mainstay of front-line treatment
for newly-diagnosed APL
• Arsenic + ATRA without chemo: promising outcome in low or
low/intermediate risk pts
• Importance of chemotherapy remains in high-risk group
• Oral arsenic + oral ATRA: better tolerance/convenience and
promising short-term outcome
Summary

Acknowledgements
• Prof Zhen-yi Wang; Zhu Chen and Sai-juan Chen;
Zhi-xiang Shen;
• Dr Jun-min Li and Hong-min Zhu
• Colleagues at Shanghai Institute of Hematology,
Department of Hematology, RuiJin Hospital