Embed Size (px)
Citation preview

D.BASEM ELSAID ENANYLECTURER OF CARDIOLOGY
AINSHAMS UNIVERSITY
Pathophysiology of Unstable angina and
NSTEMI

Unstable angina and NSTEMI result from a disparity between myocardial oxygen delivery and demand, which usually presents as angina occurring with limited physical activity or at rest (a crescendo pattern). It can occur because of:-arterial spasm-Progressive, severe, flow-limiting atherosclerosis due to intimal hyperplasia or to lipid, calcium, and thrombus deposition, or tofibrointimal hyperplasia after percutaneous coronaryintervention (PCI)-Coronary artery dissection-“secondary” UA because of conditions that alter myocardial oxygen demand or supply, such as intense emotion, tachycardia, or uncontrolled systemic hypertension

The most frequent mechanism:rupture or ulceration of a vulnerable atherosclerotic Plaque exposes the highly thrombogenic subendothelium to circulating platelets and white blood cellsTissue factor activates the extrinsic coagulation Cascade (Factor VII, and also cleavage of factor IX, contribute to activation of intrinsic pathway) activated platelets release powerful promoters of vasoconstriction and platelet aggregation (thromboxane A2, serotonin, adenosine diphosphate, and platelet-activating factor) platelet adhesion and aggregation transient thrombosis or subtotal coronary artery occlusion with dynamic vasoconstriction.


If ischemia is neither severe nor prolonged(usually <20 min) and often recurs at rest, patientsare given a diagnosis of UA. However, if ischemialasts longer than 30 minutes (usually 1–2 hr) and isassociated with elevated cardiac markers, a diagnosisof MI is made.

UA, NSTEMI, and STEMI represent a pathophysiologic continuum development of effective pharmacologic therapies that, used in conjunction with careful and rapid risk assessmentstrategies and catheter-based therapies, improveoutcomes in UA/NSTEMI patients

Atherosclerosis
-Chronic inflammatory and multifocal disease -Involves medium and large-sized arteries.-Progressive in nature-May begin in the subendothelium as early as in the 1st decade of life-Usually develops in lesion-prone vascular areas as a response to chronic, multifactorial injury to the arterial wall.-Various causes of endothelial injury include: flow shear stress, hypertension, immune-complex deposition and complement activation, smoking, diabetes mellitus, aging,substance abuse, infection, and mechanical injury to theendothelium (consequent to coronary angioplasty, stent placement, or heart transplantation).

-Endothelial injury reduce Nitric oxide (NO) and prostacyclin (PGI2) {both play key roles in the maintenance of endothelial homeostasis}-Cardiovascular disease risk factors, such as hypertension, dyslipidemia, diabetes, and smoking, induce oxidative stress overproduction of reactive oxygen species accelerate the degradation of NO and up-regulation of redox-sensitive genes, including:adhesion molecules (for example, vascular-cell adhesion molecules [VCAMs] and intercellular adhesion molecules [ICAMs]), cytokines (for example, tumor necrosis factor-α [TNF-α] and interleukin-1β [IL-1β]), and chemokines (for example, monocyte chemoattractant protein-1 [MCP-1]) recruitment and infiltration of inflammatory cells into the vascular wallmonocytes differentiate into macrophages, which laterchange into foam cells. Smooth muscle cells also migrate from the tunica media to the intima. Together, these cells proliferate and secrete a rich and complex extracellularmatrix and matrix metalloproteinase (MMP).

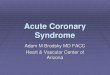
most common type of atheroscleroticvulnerable plaque (no sig luminal narrowing)

Inflammatory cytokines and inflammatory mediatorsinhibit de novo synthesis of interstitial collagen and increase the production of MMPs, which degrade thefibrous cap and make the atherosclerotic plaque vulnerable to rupture.

Diagnosis and Risk Stratification
Early risk stratification is vital in the timely diagnosis and treatment of ACS.
I- Clinical presentation:*Chest pain or discomfort that may or may not radiate to the arm, back, neck, jaw, or epigastrium*Women and elderly patients are more likely to present with atypical features,such as shortness of breath, weakness, diaphoresis, nausea, and lightheadedness--Rest angina= at rest; usually prolonged, lasting longer than 20 minutes--New-onset angina=(within the past 2 months); at least a CCS class III in severity--Increasing angina Previously diagnosed angina that has become distinctly more frequent, longer in duration, or lower in threshold (i.e., increasing by 1 or more CCS classes to at least a CCS class III in severity)
{In some cases, the patient cannot qualify the nature of the discomfort but places his or her clenched fist in the center of the chest, known as the "Levine sign.“}



more typical of NONischemic chest discomfort
•Pleuritic pain, sharp or knife-like pain related to respiratory movements or cough•Primary or sole location in the mid or lower abdominal region•Any discomfort localized with one finger•Any discomfort reproduced by movement or palpation•Constant pain lasting for days•Fleeting pains lasting for a few seconds or less•Pain radiating into the lower extremities or above the mandible


II- Physical Examination:Often normal but Attention must be paid to the presence of complications of ACS, includingacute left ventricular failure secondary to ischemia, hypotension, an S3 gallop, new or worsening mitral regurgitation, and pulmonary edema•A screening neurologic examination should be performed to assess for focal lesions or cognitive deficits that might preclude safe use of thrombolytic therapy (if STEMI occurs)

III- ECG:-Within 10 minutes, repeated after 20-30 min-Test of 1st choice as high specificity for diagnosing STEMI-Complete (>90%) occlusion of the coronary arteries alters the electrical potentials of the epicardial surface and usually manifests itself as ST-segment elevation in 2 or more adjacent leads.-ST-segment depression associated with UA/NSTEMI is transient and dynamic. Its appearance is usually flat or down-sloping. Concurrent T-wave inversion may or may not be present-Some clinicians assume that an ECG obtained while the patient is experiencing chest pain that fails to show evidence of ischemia rules out the possibility of ACS. This assumption is false

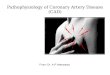
LBBB
Sgarbossa criteria :•ST segment elevation of 1 mm or more that was in the same direction (concordant) as the QRS complex in any lead — score 5.•ST segment depression of 1 mm or more in any lead from V1 to V3 — score 3.•ST segment elevation of 5 mm or more that was discordant with the QRS complex (ie, associated with a QS or rS complex) — score 2.---Sgarbossa score of ≥3 had a sensitivity of 20 percent and a specificity of 98 percent (few false positive). The sensitivity may increase if serial or previous ECGs are available

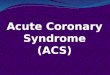
V pacing
The only ECG criterion with a high specificity and statistical significance for the diagnosis of an acute MI was ST segment elevation ≥5 mm in leads with a negative QRS complex.
Two other criteria with acceptable specificity were:•ST elevation ≥1 mm in leads with concordant QRS polarity•ST depression ≥1 mm in leads V1, V2, or, V3

IV- Biochemical Markers:-Myocardial necrosis the integrity of the myocytic membrane is lostCardiac enzymes and other substances leak into the peripheral blood-Currently, cardiac troponins (subunits of the thin-filament–associated troponin-tropomyosin complex, which help regulate muscle contraction) are the gold standard.-Excellent independent markers of short-term andlong-term prognoses initial risk stratification of patients with ACS-Troponin T, I are detectable in the serum 4 to 12 hoursafter onset of myocardial necrosis, and both peak 12 to48 hours from symptom onset baseline sample then at 8-12h interval
V-Echo, chest Xray: usually performed in patients suspected of having ACS, as alternative diagnoses such as aortic dissection, pulmonary embolism, or acute pericardial disease may be detected





Risk Stratification
*The Thrombolysis in Myocardial Infarction (TIMI) score*The Global Registry of Acute CoronaryEvents (GRACE) score***AIM= identify high-risk patients who may benefit from early revascularization procedures and to predict major adverse cardiac events up to 1 year

TIMI
-Age ≥65 years-At least 3 risk factors for CAD, including a family history, hypercholesterolemia, diabetes, or being a current smoker-Significant coronary artery stenosis (e.g., previous coronary stenosis ≥50%)-ST-segment deviation-Severe angina symptoms (e.g., 2 or more events in the past 24 hours)-Use of aspirin within the past 7 days-Elevated serum cardiac markers
*The 7 clinical variables for calculating the TIMI risk score.Each variable is given 1 point, for a total score ranging from0–7.* Even in patients with low TIMI risk scores (0–2), there is still a 5% riskof their having a significant adverse cardiac event within 30 days

GRACE





Even in patients with normal or nondiagnostic ECG, normal biomarkers, and low risk for adverse events, up to 10 percent may still have ACS and 2 to 4 percent may have early adverse events. Thus, subsequent noninvasive provocative testing is an important part of the evaluation of these low-risk patients with possible acute coronary syndrome.