Embed Size (px)
Citation preview

Abnormal lung
• An attempt to get the
• whole book in one small
• presentation.

Introduction
• This presentation is just an effort to
classify the visualized abnormalities by their radiological appearances.

Homogeneous shadows grouped according to shape , size and
distribution.• Bilateral total homogeneous
shadows • Bil.homo.opacity in the major part
of the lung• Unilateral total homo. Opacity• Large opacity in a part of the lung • Long line or band type shadows • Circular or oval type

Bilateral total homogeneous shadows
• Extensive pulmonary oedema • Terminal stages of a failing left ventricle• Excessive oxygen in a respirator circuit• Newborns where proper aeration of the
lungs is delayed• Respiratory distress syndrome of
newborn premature baby

Excessive oxygen in a respirator circuit

Extensive pulmonary oedema

Newborns where proper aeration of the lungs
is delayed

Bil.homo.opacity in the major part of the
lung• Bat’s wing shadow –Pulmonary oedema• Alveolar Proteinosis• SLE• Polyarteritis nodosa• Inhalation of gastric contents after
vomiting• Bilateral pneumonia • Acute interstitial pneumonia

Bat’s wing

Alveolar proteinosis

• Alveolar proteinosis,• A disease characterized by filling of alveolar spaces
by proteinaceous material, rich in lipid, and related to surfactant. The majority of cases are idiopathic, but some cases result from exposure to dusts (particularly silica) or from immunological disturbances (immunodeficiency, haematologic and lymphatic malignancy, chemotherapy). Symptoms are usually mild and insidious. Treatment consists of bronchoalveolar lavage. Radiographic findings are bilateral, patchy, diffuse, or perihilar air-space consolidation or ground-glass opacity, often most severe at the lung bases. High resolution CT (HRCT) findings are confluent ground glass opacity or air-space consolidation.ground glass opacity or consolidation is sharply demarcated from surrounding normal lung. A combination of geographic ground glass opacity and interlobular septal thickening in the same regions is typical of alveolar proteinosis ; this finding is termed "crazy-paving"


Bilateral pneumonia
Pneumonia,infectious or noninfectious inflammation of the airspaces and or interstitium of the lung.



Aspiration pneumonia, a common cause of pneumonia in young children and in those with an impaired cough reflex or swallowing mechanism. There is direct injury to the mucosa of the airways and acinar epithelial cells. This may be evident radiographically as pulmonary oedema or focal consolidation. If there is no superimposed infection this may clear in a few days.When food particles or salivary secretions are aspirated there may be obstruction of small airways or inflammatory alveolar change, particularly in the dependent parts of the lung. This may be seen as patchy focal opacities on the chest radiograph. Atelectasis may also be seen, often in isolation. If the aspirate contains significant numbers of pathogens, bacterial pneumonia may develop. Depending on the organism, lung abscess may complicate the picture.

Inhalation of gastric contents after
vomiting

Unilateral total homogeneous opacity
• Massive pleural effusion• Total collapse• Acute total pneumonic consolidation• Supine x ray taken in
hydropneumothorax or haemopneumothorax
• Massive neoplasm of the lung • Agenesis of the lung

Total collapse

Supine x ray taken in hydropneumothorax or haemopneumothorax

Acute total pneumonic consolidation

Lung agenesis,(also called lung aplasia), complete absence of a whole lung and its bronchus. In lung aplasia there is no lung tissue but a blind main bronchus is present. Both anomalies are characterized by an opaque hemithorax with displacement of the mediastinal structures, diaphragm and contralateral lung from the affected hemithorax. The herniated isolated lung can simulate an hypoplastic lung. The variable volume of the single lung during respiration can also simulate a pleural effusion of the diseased side. It can be easily ruled out when performing an ultrasonography. Due to the left-sided position of the aortic arch and the ductus arteriosus, the left main bronchus may be narrowed in the presence of a right-sided lung agenesis or aplasia, triggering a rotational distorsion of the mediastinum.



collapse

Effusion

pneumonia

pneumonectomy
pneumonectomy

Large shadows occupying part of one lung
• Pleural shadows
• Lobar consolidation
• Segmental consolidation
• Partial collapse

Pleural shadows
• Mod. Sized pleural effusion• Small pleural effusion• Sub –pulmonary pleural effusion• Encysted pleural effusion• Interlobar pleural effusion.• Thickened pleural opacity• Mediastinal pleural effusion.

pleural effusion




Lobar consolidation



Segmental consolidation

Atelectasis, (also called collapse), a loss of volume of lung parenchyma caused by a reduced inflation. Several mechanisms may be responsible for atelectasis. They include the following: · resorption or obstructive atelectasis resulting from bronchial obstruction;· compression or passive atelectasis which is collapsed caused by extrinsic compression such as pleural fluid or air, or the presence of any space-occupying intrathoracic lesion resulting in extrinsic compression of adjacent parenchyma;· cicatrization atelectasis resulting from lung parenchymal fibrosis; and· adhesive atelectasis which is collapse resulting from loss of surfactant.Atelectasis may involve one or more lobes or segments (see lobar atelectasis). In other circumstances, atelectasis can have a nonanatomical distribution. Air within the collapsed or atelectatic lung parenchyma can be entirely resorbed and partially replaced by fluid or fibrosis (nonaerated lung collapse). It appears radiologically as an opacification. When air within the collapsed lung parenchyma is only partially resorbed and not replaced by any fluid or tissue, no radiological opacification is depicted (aerated lung collapse).

Partial collapse

Long line & band –like shadows
• Segmental collapse


Circular or homogeneous intrapulmonary shadows > 2 cms• Bronchial carcinoma
• Secondary deposit• Bronchial adenoma• Leiomyoma• Fibroma• Hamartoma• Arterio-venous aneurysm• Fluid containing cyst• Sequestrated segment• Tuberculous focus• Infected lesion• Hydatid cyst• Toruloma• Mycetoma• Infarct• Non specific granuloma• Syphilitic lesion• Paraffin granuloma• Interlobar pleural effusion.

Bronchial carcinoma

Secondary deposits

Hydatid Cyst

Tuberculous focus

Granuloma,a histological microscopic organization, consisting of focal and chronic conglomeration of inflammatory cells. According to the type of prominent cells, different categories of granuloma may be described.Polymorphic granuloma that is a chronic nonspecific inflammatory reaction to different types of infection, is characterized by a collection of macrophages associated with other leukocytes.Tuberculoid granuloma is characterized histologically by the grouping of macrophages in follicules. Some of the macrophages may display a transformation in epitheloid cells and giant cells. Lymphocytes and plasma cells may also be present. Necrosis may occur in the centre of the follicules. Later a fibroplastic proliferation may be present. Tuberculoid granuloma corresponds to a specific inflammatory reaction. It may occur in a wide variety of lung diseases, including pneumoconiosis (foreign body reaction), lung infection (tuberculosis ,fungal infection , infection pulmonary ,autoimmune disease , rheumatoid lung disease , weneners granulomatosis chest and sarcoidosis.

Non specific granuloma

Fibroma, pulmonary,rare benign pulmonary neoplasm that may represent one-dimensional histological expression of pulmonary hamartoma. Lung fibromas present as a solitary pulmonary nodule. Fibromas may also develop from the pleura, representing the most common benign pleural neoplasm


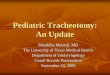
Hamartoma, pulmonary, the most common benign pulmonary neoplasm and the third commonest cause of a solitary pulmonary nodule. Hamartomas orginate in fibrous connective tissue beneath the mucous membrane of the bronchial wall. They contain mixtures of connective tissue, epithelial-lined clefts, nests of cartilage and variable amounts of bone, vessels, fat and smooth muscles.Hamartomas occur mainly between the fifth and the sixth decade with an age range of 3070. Most patients are asymptomatic and the tumour is incidentally discovered on a chest radiograph as a solitary pulmonary nodule that typically grows slowly. Occasionally hamartomas may be endobronchial in location, producing obstructive symptoms Radiographically, hamartoma usually appears as a well-defined spherical nodule or mass generally less than 4 cm in diameter. Calcifications are frequent in large lesions. The classic popcorn appearance of the calcification suggests the presence of cartilage. Hamartomas may be diagnosed confidently on CT scans when the nodule is less than 2 cm in diameter, appearing spherical with a smooth contour and sharp outline and containing fat collection more or less associated with popcorn calcifications

Hamartoma

CT scan in a patient with pulmonary hamartoma. There is a round smooth well-defined nodule containing popcorn calcification and a collection of fat.

A V Fistula

Fungal ball



Cyst

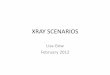
Pulmonary infarct,condition in which radiologically a pulmonary opacity develops distal to an occluded pulmonary artery. From a pathological point of view it encompasses both haemorrhage and infarction. Typically Hampton's hump is a wedge-shaped consolidation with its base in contact with the pleura and its apex towards the hilum. It is more often seen on CT than on chest radiography

Infarct


CT demonstrate wedge-shaped, nonenhancing pulmonary infarction in the anterior and posterior basal segment. Clot is visible in anterior and posterior basal segment arteries (arrows). Right pleural effusion is also present.

Multiple Large Circular or oval homogeneous shadows > 2-5 cms
• Cannon ball – secondary deposits• Multiple hydatid cysts• Rheumatoid nodules• neurilommoma

Cannon ball – secondary deposits

Multiple hydatid cysts

Rheumatoid lung disease,Rheumatoid arthritis (RA) is commonly associated with thoracic abnormalities, including interstitial pneumonitis and fibrosis,pleural effusion or pleural thickening, necrobiotic nodules, bronchiolitis obliterans organizing pneumonia (BOOP), bronchiectasis and bronchiolitis obliterans. The prevalence of radiologically detectable interstitial disease in patients with rheumatoid arthritis is probably around 10%. Histologically, radiologically, and on HRCT, the appearance of RA with interstitial fibrosis is usually indistinguishable from that of idiopathic pulmonary fibrosis (IPF). Clinical evidence of arthritis precedes the development of pulmonary fibrosis in about 90% of patients, and 90% have a positive serum rheumatoid factor.HRCT findings reported in patients with rheumatoid arthritis include nodules which are predominantly subpleural in location, bronchial abnormalities and bronchiectasis , ground glass opacity ,pulmonary fibrosis with or without honeycombing, consolidation, enlarged lymph nodes and pleural abnormalities. In patients with rheumatoid arthritis, the presence of ground glass opacity, consolidation and fibrosis probably reflects the presence of interstitial pneumonia, while the small and large nodules probably represent necrobiotic nodules . Bronchiectasis can be associated with chronic infection, which has an increased incidence in rheumatoid patients, or bronchiolitis obliterans.

Rheumatoid nodules



A single small circular homogeneous shadow 2 mm - 2 cms
• Tuberculous lesion• Blocked cavity• Endobronchial Tuberculous lesion• Neoplasm• Infarct• A V aneurysm• Dilated bronchus full of secretions• Rheumatoid nodule

Neoplasm

Tuberculosis

A single secondary deposit

Pulmonary angiography showing a Rasmussen's aneurysm of the right lower lobe incidentally discovered in a patient with a previous history of cavitary tuberculosis of the same lobe. The cavity is replaced by a pulmonary nodule. Its aneurysmal origin is proved by CT angiography

Localized small circular shadows or
patchy clouding 3-4 shadows ---1 cms• Tuberculosis• Inflammatory condition caused due to
bacterial ,viral ,neoplasm • Sensitivity reactions as in farmer’s
lung ,bird fancier’s lung.• Early stages of bronchopneumonia• Chronic bronchitis with inflammatory
episode• Silent chronic pulmonary infarcts

Tuberculosis

Pigeon breeder's lung,(also called bird fancier's disease), is a hypersensitivity pneumonitis caused by inhalation of proteins contained in serum, droppings and feathers of pigeons and other birds . Hypersensitivity pneumonitis, (also called extrinsic allergic alveolitis), an allergic lung disease caused by the inhalation of antigens contained in a variety of organic dusts. The radiographic and pathological abnormalities seen in patients with hypersensitivity pneumonitis are quite similar, regardless of the organic antigen responsible; these abnormalities can be classified into acute, subacute and chronic stages. In the acute stage, heavy exposure to the inciting antigen can cause diffuse ill-defined air-space consolidation visible on radiographs; this reflects alveolar filling by neutrophils, eosinophils, lymphocytes and large mononuclear cells, or obstructive pneumonitis. After resolution of the acute abnormalities, or between episodes of acute exposure, a fine nodular pattern is often visible on radiographs. This pattern is characteristic of the subacute stage of hypersensitivity pneumonitis. The nodular appearance correlates with the presence of alveolitis, interstitial infiltrates, small granulomas and cellular bronchiolitis; histological abnormalities are usually most severe in a peribronchiolar distribution. The chronic stage of hypersensitivity pneumonitis is characterized by the presence of fibrosis, which may develop months or years after the initial exposure.The HRCT findings of hypersensitivity pneumonitis depend on the stage of disease. In the subacute stage, weeks to months following first exposure to the antigen, typical findings include patchy ground glass opacity and small ill-defined nodules, usually centrilobular in distribution. Chronic hypersensitivity pneumonitis is characterized by the presence of fibrosis, although findings of active disease are often superimposed. Findings of fibrosis in patients with chronic disease most often show a milling zone predominance or are evenly distributed throughout the upper, mid and lower lung zones

Bird fancier’s disease :farmer’s lung


Multiple widely disseminated small circular shadows 1- 2cms
• Secondary deposits & indolent tuberculosis 1-2 cms
• Ossifying secondary deposits-osteogenic sarcoma
• Pneumoconiosis with rheumatoid nodules• Fungoid deposits• Pleural secondary deposits

Ossifying secondary deposits-osteogenic sarcoma

Fungoid deposits

Single ill-defined Moderate sized homogeneous shadows
• Partial consolidation• Asthmatics• Periarteritis nodosa• Diffused lupus erythematosus• Very early stages of coal miner’s
pneumoconiosis

Partial consolidation

Pneumoconiosis,a term used to describe the non-neoplastic reactions of the lungs to inhaled dust particles. Although some authors include organic as well as mineral dust, many limit the term to inorganic dust, notably coal, silica and asbestos (Table 1).Pneumoconiosis, Table 1. List of pneumoconioses.
Fibrogenic dust silicosis asbestosis Coal workers pneumoconiosis Hard metal pneumoconiosisNonfibrogenic dust (benign pneumoconioses) Aluminosis Anthracosis Antimony pneumoconiosis Baritosis Siderosis (iron pneumoconiosis) Stannosis (tin pneumoconiosis) Talcosis (talc pneumonoconiosis)Mixed pneumoconioses Siderosilicosis Silicoasbestosis


Diffused lupus erythematosus

Poorly defined small homogeneous shadow
[ a smudge] < 2 cms
• Usually in the upper zones :• Tuberculous focus
• If present in the lower ½ of the lung near the pleura :
• Infract

Infract

Multiple widely disseminated amorphous
ill-defined shadows 1-2 cms• Secondary deposits : prostate , breast Stomach or lymphosarcoma Intra alveolar spread of a bronchiolar
adenocarcinomaPulmonary oedemaPeriarteritis nodosaInhalation of irritant gas Lung purpura Cystic fibrosisFungoid lesions

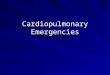
Cystic fibrosis

Cystic fibrosis
PA chest radiograph (a) and HRCT scan (b) in a 25-year-old patient with cystic fibrosis. Chest radiograph shows diffuse overinflation and cicatrization atelectasis of the right upper lobe. Tubular shadows underlying dilated bronchi are present in the right lung bases and left lung. HRCT scan shows decreased lung attenuation and mosaic perfusion representing lesions of constrictive bronchiolitis. Mucoid impactions within dilated bronchi are present within the collapsed right upper lobe and the superior segment of the right lower lobe.

Intra alveolar spread of a bronchiolar adenocarcinoma

Secondary deposits

Nodular or Miliary shadows pinpoint – 5 mm
• Miliary tuberculosis• Viral infection.• Haemosiderosis• Pneumoconiosis• Allergic pneumonias• Alveolar carcinoma of the lung • Sarcoidosis• Fibrosing alveolitis

Miliary tuberculosis


Pneumoconiosis



HaemosiderosisPulmonary haemosiderosis,condition resulting from recurrent intrapulmonary bleeding with haemosiderin depositions in the lungs, leading to pulmonary fibrosis and restrictive airways disease. Clinical presentation typically is with haemoptysis, cough, dyspnoea, during an acute attack, with remissions. There is in associated microcytic hypochromic anaemia. The diagnosis is made by bronchoalveolar lavage in which iron-laden macrophages are demonstrated in the sputum. Children, however, do not always present with haemoptysis as they often swallow their saliva. They may instead present with apparent chest infection and anaemia. Radiologically, the appearances in the acute situation are those of extensive alveolar shadowing in the lungs which as it clears becomes a more ground glass appearance with small nodules . With recurrent attacks, interstitial fibrosis develops.Pulmonary bleeding associated with renal diseases is called Goodpastures syndrome

Pulmonary haemosiderosis13-year-old girl who presented with haemoptysis. Admission film (a) shows acute alveolar shadowing. b. Repeat film 3 days later shows improvement in the alveolar oedema but there is now a reticular nodular pattern developing. A diagnosis of pulmonary haemosiderosis made by bronchoalveolar lavage. c. CT scan done during the recovery phase demonstrates airspace shadowing, particularly in the left lung.

Alveolar carcinoma of the lung

Allergic

Nodular shadows with ground glass haze [pin point]
• Respiratory distress syndrome • Fibrosing alveolitis• Microlithiasis alveolaris

Fibrosing alveolitis

Pulmonary alveolar microlithiasis is a rare condition characterised by a diffuse bilateral filling of the majority of alveoli by calcific concretions called "Calcospherites". The aetiology and pathogenesis are obscure; a familial incidence has been reported in several instances. Pulmonary alveolar microlithiasis is rare and less than 100, cases have been reported in the world literature. The radiological picture that is very characteristic shows bilateral sand-like micro nodules of calcific density, usually most marked in the middle and lower zones with relative sparing of the apices. Although the radiological picture is diagnostic, many cases are mistaken for miliary tuberculosis, silicosis, berylliosis, sarcoidosis, haemosiderosis, fungal infections and carcinomatosis. Most patients remain symptom-free for many years despite extensive radiological changes. In over half the reported cases, a familial incidence has been demonstrated almost invariably among Siblings and only in two instances in a parent and child; cases in infants have also been reported. A genetic factor has been postulated because of familial occurrence. It has been suggested the possibility of congenital error of metabolism at the level of alveolar surface membrane, possibly an enzymatic fault, resulting in the precipitation of calcium in the presence of undue alkalinity.

Microlithiasis alveolaris


Nodular shadows with short line shadows 1-2
cms horizontal lines
Pneumoconiosis – asbestosis –coal workers & tin handlers
• Fibrosing alveolitis

Pneumoconiosis – asbestosis

Nodular shadows with long line & septal line shadows 2-4 cms hair like shadows
Lymphangitis carcinomatosa

Lymphangitic carcinomatosis, tumour growth in the lymphatic system of the lungs. It occurs most commonly in patients with carcinomas of the breast, lung, stomach, pancreas, prostate, cervix or thyroid, and in patients with metastatic adenocarcinoma from an unknown primary site. It usually results from haematogenous spread to lung, with subsequent interstitial and lymphatic invasion, but can also occur because of direct lymphatic spread of tumour from mediastinal and hilar lymph nodes. Symptoms of shortness of breath are common and can predate radiographic abnormalities.The radiographic manifestations of pulmonary lymphangitic carcinomatosis include reticular opacities, Kerley lines, hilar and mediastinal lymphadenopathy and pleural effusion. However, these findings are nonspecific. Tumour growth in the peribronchovascular and septal lymphatics located within these compartments, and associated oedema, result in the characteristic HRCT findings of lymphangitic carcinoma. Lymphangitic carcinomatosis is characterized on HRCT by reticular opacities. Specific findings include:· thickening of the peribronchovascular interstitium surrounding vessels and bronchi in the parahilar lung;· interlobular septal thickening and subpleural interstitial thickening that is smooth, or nodular;· thickening of the peribronchovascular axial interstitium in the centrilobular regions; and· a preservation of normal lung architecture at the lobular level, despite the presence of these findings.Hilar lymphadenopathy is visible on CT in only 50% of patients with lymphangitic carcinoma. Lymph node enlargement can be symmetrical or asymmetrical. pleural effusion may also be present.




Nodular shadows with small ring shadows [ring diameter 3- 8
mm]• Fibrosing alveolitis – late stage
cryptogenic form • Asbestos induced fibrosis• Systemic sclerosis• Allergic alveolitis – farmers , bird
fanciers , malt workers • Xanthomatous lung disease• Idiopathic Haemosiderosis

Fibrosing alveolitis


Nodular shadows with shrunken upper lobes
Chronic tuberculosisSarcoidosis

Chronic tuberculosis

Sarcoidosis

Nodular shadows with large homogeneous
shadows
Sarcoidosis - late stage Broncho-pulmonary aspergillosis
with eosinophiliaPneumoconiosis with massive
fibrosis

Sarcoidosis


Nodular shadows with raised dome of the diaphragm
Fibrosing alveolitis Lymphangitis carcinomatosaTuberculosis

Nodular shadows with abnormalities seen in the
heart shadow Lesions are secondary to heart
condition.
Pulmonary oedemaHaemosiderosis

Nodular shadows with hilar gland enlargement
SarcoidosisTuberculosisHodgkin’s diseaseSecondary deposits from a
carcinoma

Sarcoidosis with hilar glands

Hilar glands

Hodgkin’s

Nodular shadows with cavities , bronchiectasis or bullae
Tuberculosis Sarcoidosis Broncho-pulmonary aspergillosis
with eosinophiliaResolved Xanthomatous lesions

Tuberculosis

Sarcoidosis

Tuberculosis

Bronchopulmonary aspergillosis,invasion of the lungs and bronchial tree of the spores of Aspergillus fumigatus, caused by inhalation of the spores. Two types are described, allergic bronchopulmonary aspergillosis, typically seen in asthmatic patients, but rare in children, and invasive infection seen in immunocompromised patients in which disseminated infection may occur.In allergic bronchopulmonary aspergillosis the symptoms are mainly those of cough, wheeze and chest pain with expetoration of mucous plugs. The repeated damage to the bronchial tree caused by deposition of the spores leads to bronchiectasis. It is thought that the inhaled organisms grow within the bronchi and release an antigen which causes sensitisation and later provokes an immune reaction. Mucin produced as part of this reaction is thick and tenacious and plugs the bronchi. This traps the fungus within the airway, with resultant bronchiectasis. Within a bronchiectatic cavity a mycetoma may develop. Radiographically, they appear as a mass lesion over which there is a crescent of air In invasive aspergillosis, the radiographic pattern is one of multiple areas of consolidation. These may also cavitate and produce a crescent of air. Lesions, which are fungal abscesses, may also be found in the brain, liver, kidneys and spleen Aspergillosis infection also occurs in children with cystic fibrosis and is a cause of deterioration in pulmonary function. The radiographic appearances are nonspecific but infection may be suspected if there is a large area of consolidation, often basal, which is out of proportion to the extent of the disease elsewhere.

Bronchopulmonary aspergillosis

Linear shadows : line , band , tubular & ring shadows
• Line shadows :Horizontal pleural line :• Horizontal fissure • Fissure over apical lower lobe• Accessory fissure between apical lower and basal segments• Aerated but shrunken lobeVertical Pleural line shadows The accessory lobe of the azygosMain interlobar pleural fissureVertical line shadow from the dome of the diaphragmTriangular shadow from the diaphragmAxillary & Diaphragmatic pleuraVisceral pleura in pneumothoraxMediastinal pleural hernia



Intrapulmonary line shadows
• Horizontal line shadow above the diaphragm also known as Fleischer’s line
• Septal line shadows – kerley B lines• Kerley A lines• Isolated line shadows in upper half of the
lung• Line shadows radiating out from circular
shadow

Kerley’s lines


Band like shadows
• Pleural • Collapsed lung• Foreign body• Bronchial shadows• Vessel shadows

Collapsed lung

Tubular shadows
• Normal – caused by two vessels running parallel to each other.
• Abnormal -- tram like seen in cases of Asthma , cystic fibrosis , allergic lung
conditions , pulmonary oedema , bronchiectasis

Tubular shadows


Rest of it next time