Embed Size (px)
Citation preview
“ABC, GCB and Double-Hit diffuse large B cell lymphoma: Does subtype make a
difference in Therapy Selection?”
Journal ClubModerator: Dr. Suresh Babu MC
Presenter: Dr. Gita R Bhat
Authors: Grzegorz S. Nowakowski, Myron S. Czuczman
ASCO 2015, Educational Book

Overview • Personalized therapy for treatment of patients with cancer is rapidly
approaching and is an achievable goal in the near future.• DLBCL is the most common NHL• 40% patients have refractory disease or disease that will relapse after
initial response• 2 major biologically distinct molecular subtypes of DLBCL: GCB and ABC• Double hit lymphomas (approx 5%-10%) of patients and double
expressor lymphomas are aggressive and associated with poor prognosis.
• Early clinical trials evaluating combination of novel targeted agents in combination with R-CHOP have shown encouraging results.
• Hence, molecular classification: Prognostication + personalization of therapy for DLBCL.

• Addition of rituximab (R) to CHOP in patients with DLBCL: dramatic improvements in PFS and OS.
• Inspite of this, 40% relapse or have refractory disease.
• Various strategies to improve outcomes: intensification of chemotherapy, use of maintenance therapy, novel agents.

• Alternate regimens for front-line R-CHOP :• Dose –dense R-CHOP 14: Phase III trial
showed no additional clinical benefit• Dose-adjusted R-EPOCH• R-CEOP 90• Phase III trial: 1080 patients – No additional
clinical benefit was observed in patients treated wih R-CHOP14 vs. R-CHOP21.
• Addition of novel agents (X) to R-CHOP:• XR-CHOP• “DLBCL has molecular heterogeneity”• “X – targets specific oncogenic pathways”

• Classification of DLBCL based on the cell of origin (COO):
• GCB (CD10, BCL6)• Non-GCB ABC (poor outcome) Primary mediastinal B-cell types• Associated with differences in clinical outcome

GCB DLBCL ABC DLBCL
Markers of germinal centre differentiation (CD10 and BCL6)
-
- NF-κB pathway is constitutively activeHigh expression of NF-κB genes
BCL2 + BCL2+ (> 4 fold higher than in GCB DLBCL)
Arises from germinal centre B cell Post-germinal centre B cell, blocked during plasmacytic differentiation
Outcome of GCB DLBCL and ABC DLBCL treated with RCHOP
Primary mediastinal B cell lymphoma
Arises from Thymic B cell
Predominantly in young women
Shares many features with CHL-NS
OCT-2 and BOB-1 (B cell transcription factors) are positive, Immunoglobulin production is defective
Agents predominantly active in Non-GCB (ABC) DLBCL
• Pathways that are constitutively activated in ABC DLBCL:
• B-cell receptor (BCR) pathway • Pathways downstream of BCR pathway• Constitutive activation of NF-kB genes
• Proteasome inhibitors• Immunomodulatory agents• B-cell receptor signaling pathway inhibitors

B-cell receptor pathways
• Plays an important role in proliferation and survival in B-NHL
• Targets: • Spleen tyrosine kinase (SyK): Survival• Bruton tyrosine kinase (BTK): BCR signaling
and maturation

Proteasome inhibitors
• Inhibit transcription factor NFkB• Downstream pathway of BCR pathway• Bortezomib combined with DA-EPOCH:• ORR: GCB DLBCL (13%) vs. ABC DLBCL (83%)• Median OS: GCB (10.8 months) vs. ABC ( 3.4
months)
IMiDs
• Structural and functional analogues of thalidomide• Regulate production of T-helper cells• Inhibit cytokine production• Inhibit production of TNFa• Induce G0/G1 cell cycle arrest• Inhibit angiogenesis through suppression of VEGF
and FGF• Decrease NFkB activity

• Single agent Lenalidomide in relapsed refractory/refractory NHL including DLBCL
• Phase II study, n= 217 patients• DLBCL subpopulation: median PFS (2.7
months) and Response duration (4.6 months)
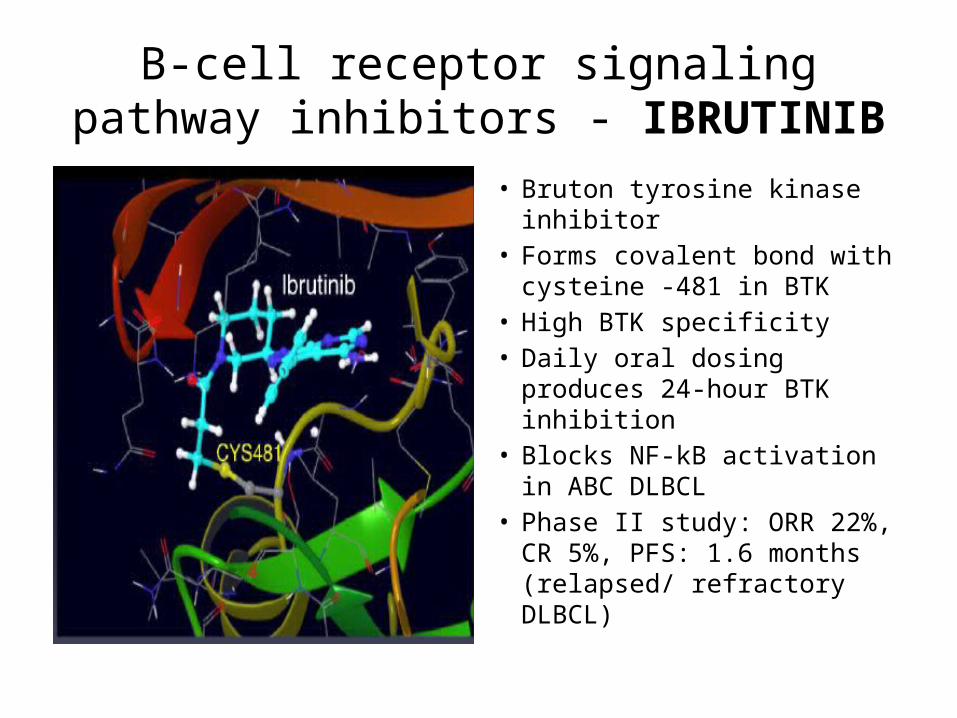
B-cell receptor signaling pathway inhibitors - IBRUTINIB
• Bruton tyrosine kinase inhibitor
• Forms covalent bond with cysteine -481 in BTK
• High BTK specificity• Daily oral dosing produces 24-
hour BTK inhibition• Blocks NF-kB activation in
ABC DLBCL• Phase II study: ORR 22%, CR
5%, PFS: 1.6 months (relapsed/ refractory DLBCL)
• SYK inhibitor: FOSTAMATANIB
• Phase II study, 23 patients• Median PFS 2.7 months• ORR: 22%

Agents with potential activity in GCB DLBCL
• GCB DLBCL has better outcomes than ABC subtype
• 20% of patients with GCB DLBCL relapse after R-CHOP or R-CHOP like chemotherapy
• Associated with poor outcomes

• BCL6: highly expressed in GCB subtype• Key transcription factor• Translocations/ mutations enhance the
inhibitory effect of BCL6 on apoptotic stress response
• This leads to tumor proliferation and treatment failure

Therapeutic implications
A) Small molecule inhibitor of BCL-6:• 79-6 complex• Binds to the co-repressor binding groove of
the BCL6 domain and kills BCL-6 positive linesB) HDAC inhibitors to overcome the effects of
BCL6 repression on p53

• C) Etoposide: Topoisomerase II inhibition – ubiquitin mediated protein degradation and transcriptional inhibition --- downregulates BCL6
• DSHNHL study: better EFS in those who received CHOEP vs. CHOP alone
• GCB DLBCL has higher incidence in younger patients, hence they benefit more from the addition of Etoposide.

• D) DA-EPOCH-R• Inhibition of Topo II is optimised by continuous
delivery of drugs over 96 hours• This ensures steady state concentration• 5 years of follow-up: EFS (95% to 100%)• E) EZH2: EZH2 inhibitors• Gain of function mutations in EZH2 result in
increased H3K27 methylation

BCL2 inhibitors• Members of BCL-2 family (BCL-2, BCL-XL, BCL-w, MCL-1,
BFL1/A-1, and BCL-B):• Suppress apoptosis through interaction with, and
inactivation of, pro-apoptotic proteins such as BH3• BCL2 inhibitors are active in ABC and GCB DLBCL• In GCB: BCL2 is overexpressed as a result of translocation• In ABC: BCL2 is overexpressed at the protein level• ABT-737 and ABT-263: target BCL-2, BCL-Xl and BCL-w• ABT-199: potently and selectively inhibits BCL2
Front-line treatment: XR-CHOP
• Bor-RCHOP• R2-CHOP• IR-CHOP

Bor-RCHOP
• Untreated DLBCL or mantle cell lymphoma
• Ongoing Phase III RCT: CHOP vs. Bor-RCHOP in DLBCL
ORR – 100%
CR or Cru: 86%
2-year PFS: 64%
2-year OS: 70%

R2-CHOP
• R2-CHOP:• Lenalidomide-RCHOP• Improves the poor prognosis usually reported
in non-GCB DLBCL• Grade 3 and 4 AEs: Neutropenia (31%),
leucopenia (28%), thrombocytopenia (13%)

• Phase II trial: newly diagnosed DLBCL• Treated with R2-CHOP vs R-CHOP
• Addition of Lenalidomide can improve the poor prognosis in non-GCB population
2-year OS
GCB DLBCL Non-GCB DLBCL
R2-CHOP 75% 83%
R-CHOP 78% 46%
• IR-CHOP:• Phase I randomized trial, 33 patients• Newly diagnosed DLBCL (22 patients) , Mantle
cell lymphoma, Follicular lymphoma• ORR 100% (CR 64% and PR 36%)• Most common AEs: Neutropenia, nausea,
thrombocytopenia, vomiting, anemia

• IR-CHOP:• Bruton’s tyrosine kinase inhibitor• Ibrutinib• Phase Ib: Newly diagnosed DLBCL, mantle cell
lymphoma, follicular lymphoma
MYC-positive and Double-hit DLBCL
• MYC is a transcription factor• Potent proto-oncogene• Regulates 10%-15% of human genome• Member of the helix-loop-helix leucine zipper
family of nuclear transcription factors• Key to formation and maintenance of germinal
centres

• It can be activated via 3 modes: “Avalanche effect”
• Translocation (5% - 14%)• Copy gain (19% to 38%)• Amplification (2%)• Mutation (32%)

Target genes of MYCProcess involved Function Target genes induced Target genes repressed
Cell cycle Transit through cell cycle G0 to S transition
Cyclin D2, CDK4 P21, p15, GADD45
Differentiation Blocks many cellular systems
LDH, ribosomal proteins, EIF4E, EI2A
Growth and metabolism Increase in cell size and number
N-cadherin, integrin
Adhesion/migration Enables anchorage dependent growth
Thrombospondin
Angiogenesis Induces angiogenesis IL 16, mir 17-92
Chromosomal instability Telomere aggregation, ROS production
MAD2, TOP1, BUBR1, Cyclin B1
Stem cell self renewal Potentiates induced pluripotent stem cells
? ?
Transformation Drives tumorigenesis Several genes Several genes

MYC-associated pathways of regulation of proliferation and survival


MYC-driven lymphomagenesis


Neoplasms with MYC gene rearrangements
• Burkitt lymphoma• t(8;14)• Simple karyotype• Sole chromosomal
abnormality
• DLBCL (7% - 14%)• Unclassifiable B-cell
lymphoma (35%)• Plasmablastic lymphoma
(50%)• Plasma cell myeloma
(15% - 50%)• Mantle cell lymphoma• Complex karyotype• Secondary genetic events

Why is this important?
• MYC rearrangement predicts an inferior outcome in DLBCL
• These are seen in 58% - 83% of MYC-translocated DLBCL• OS when treated with RCHOP is ≤ 12 months
? Due to the MYC rearrangement itself
Double hit DLBCL• Concurrent BCL2 translocation• Less likely BCL6
Triple hit DLBCL• Concurrent translocations in MYC+ BCL2 +BCL6
Concurrent MYC + BCL2
MYC1) Cell growth
2) Cell cycle transit3) Angiogenesis
BCL21) Increased anti-
apoptosis (drug resistance)

• Double-expressor lymphomas:• High percentage of MYC and BCL2 protein • By IHC staining• Tumor cells should express at least 40% MYC
and at least 50% to 70% BCL2 positivity• These are primarily ABC-like• R-CHOP or CHOP-like chemotherapy: inferior
OS and PFS
FISH vs IHC for detecting Double hit DLBCL
• ? Effect of MYC alone (FISH or IHC) without BCL2 on outcome
• BCL2+ MYC by IHC or FISH has worst outlook
“Assessment of MYC and BCL2 expression by IHC represents a robust, rapid, and
inexpensive approach to risk-stratify patients with DLBCL at diagnosis”

• DHL patients have several poor prognostic factors:
• Median age: 7th decade• Stage III/IV disease• IPI: High intermediate/high• Elevated LDH• High frequency of extra-nodal sites (excluding
CNS)
• Of the several intensive chemotherapy regimens used:
• R-EPOCH• (1) has curative potential in BL• (2) is better tolerated than most dose-
intensive regimen• (3) appears to have similar efficacy compared
to other dose-intensive therapies
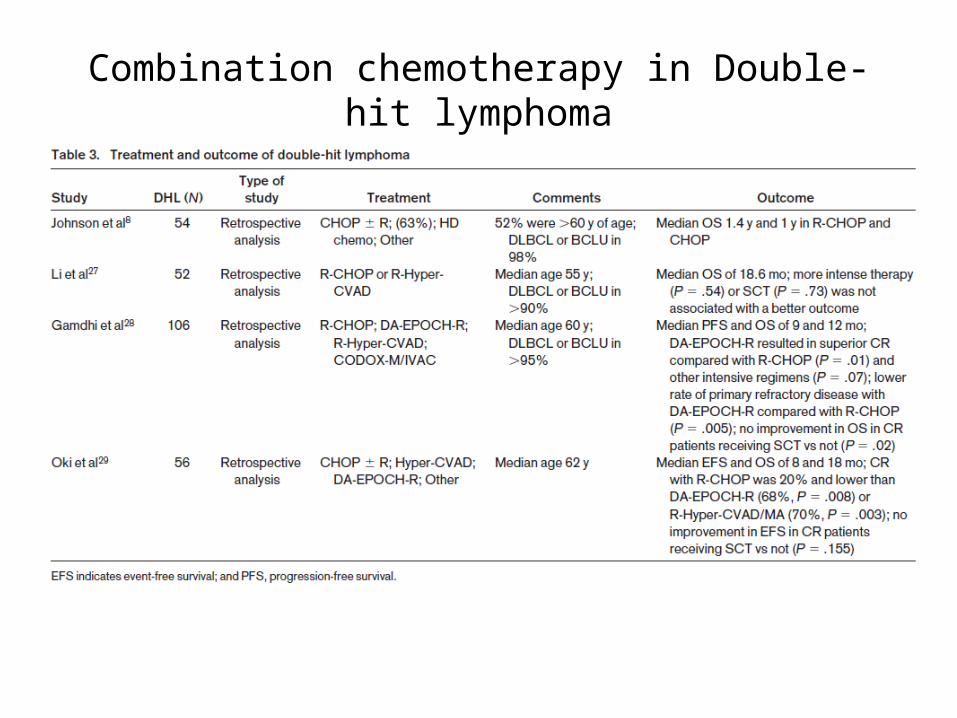
Combination chemotherapy in Double-hit lymphoma
Initial therapy for Double hit lymphoma
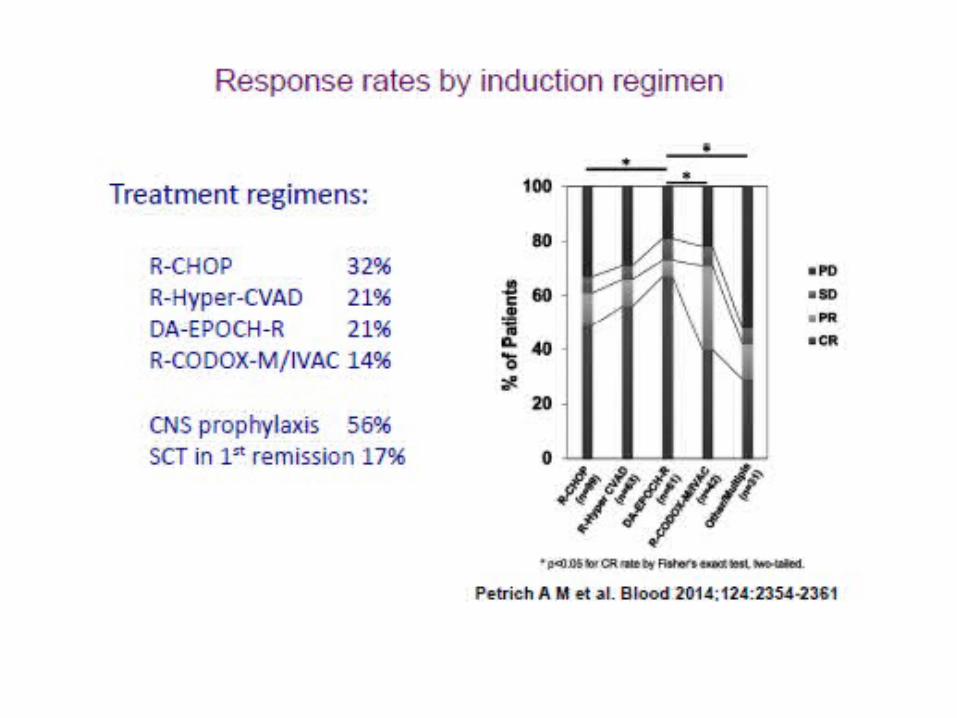
• Petrich AM et al. Blood 2014; 124:2354-2361• Retrospective study of outcomes in 23 US centres
over 12 years:• 311 patients with newly diagnosed DLBCL (154),
BCLU (150), FL (7)• MYC-R and BCL2 (87%) or BCL6 (5%) by
FISH/cytogenetics• 76% raised lDH, 33% ≥3* ULN• 65% stage IV, 41% BM +ve, &% CNS +ve
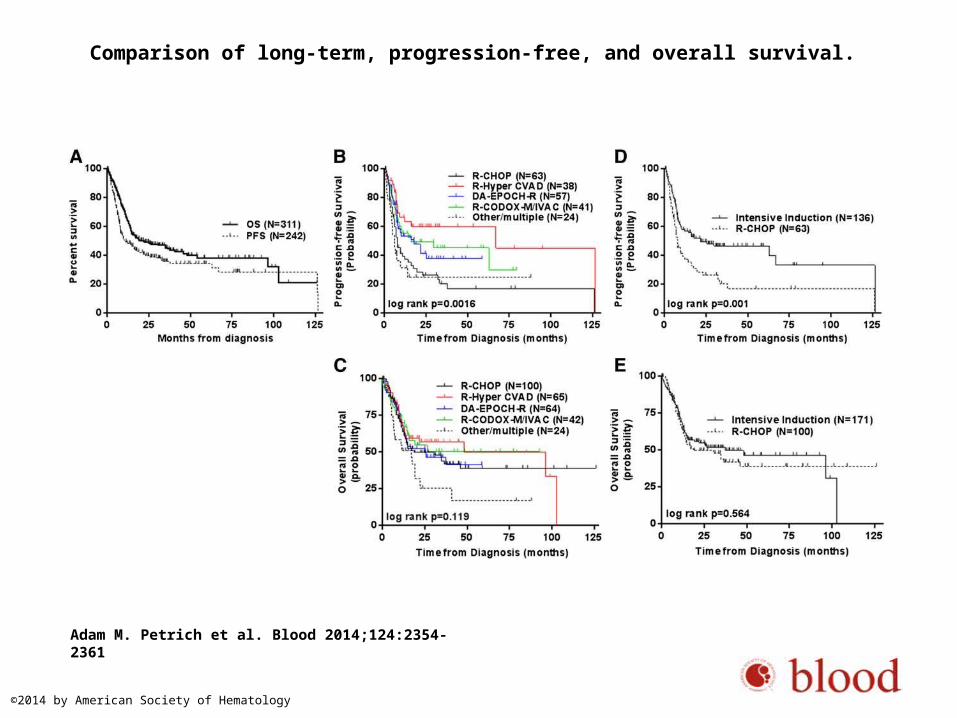
Comparison of long-term, progression-free, and overall survival.
Adam M. Petrich et al. Blood 2014;124:2354-2361
©2014 by American Society of Hematology
Role of stem cell therapy
• Autologous SCT in those who achieve CR:• Does not significantly change clinical
outcomes• Inherent rapid tumor cell growth and inherent
drug resistant DHL cells (Minimal residual disease)

• Allogenic SCT is unlikely to have a major effect since:
• 1) limited data from a small number of selected patients
• 2) the risk of relapsed disease while awaiting graft-vs-lymphoma to occur
• 3) the need for a suitable HLA-compatible donor• 4) chronic GvHD

Overall survival by SCT versus observation in first complete remission.
Adam M. Petrich et al. Blood 2014;124:2354-2361
©2014 by American Society of Hematology

• Adverse factors for OS at diagnosis:• Leukocytosis• LDH >3*ULN• Advanced Ann Arbor stage• CNS involvement

• Hence,• DA-R-EPOCH induction + CNS prophylaxis is a
reasonable approach
• Further escalation of chemotherapy, especially in the salvage setting is unlikely to be of benefit…. Hence, novel agents…

ABT - 199 Platelet sparing BCL2 inhibitor (BH3 mimetic) restores apoptosis
Bromodomain inhibitors Down-regulation of MYC-associated transcription: Decreased cell proliferation and inhibition of MYC-driven neoplasms
CAR-T cells Autologous T-cell mediated killing of CD19-positive lymphoid neoplasm
Aurora kinase inhibitors (Alisertib)
Aurora kinase is required for tumor maintenance of MYC-driven lymphoma
mTor inhibition mTor plays an important role in tumor maintenance by MYC in B lymphocytes
Second generation Proteasome inhibitor (Ixazomib)
Degrade MYC and can induce lymphoma cell death
PI3K inhibition In GCB-DLBCL: Loss of PTEN leads to activation of PI3K/AKT pathway ___ MYC upregulation
Inhibition of mitochondrial peptide deformylase
Apoptosis in MYC-over expressing hematopoietic neoplasms
SIRT4 protein Suppresses tumor formation in MYC-induced B-cell lymphoma
Key points• ABC subset of DLBCL is biologically distinct• Associated with poor outcomes when treated with a standard therapy. • Activation of the clonic B-cell receptor pathway allows for therapeutic
targeting.• Targeted agents in relapsed DLBCL can be combined with R-CHOP in front-
line therapy of DLBCL. • The germinal center B-cell (GCB) subset of DLBCL is associated with better
outcomes and may require different therapeutic approaches.• Double-hit lymphoma (DHL) is responsible for a substantial number of
relapses in GCB DLBCL • All newly diagnosed DLBCL biopsy samples should be tested for DHL by
fluorescent in situ hybridization and by immunohistochemistry for double-expressor DLBCL
• Whenever possible, patients should be referred to participation in clinical trials
• DHL: DA-R-EPOCH plus central nervous system prophylaxis until more effective novel targeted agents for this lymphoma subtype are developed
Thank you!




![Optimizing Recoveries of Planar Pesticides in Spinach ... · tandem GCB-NH 2 [8], GCB-PSA [9], and GCB SAX-PSA. [10] In this study, toluene was added into the ACN extracts in the](https://img.pdfslide.us/doc/110x75/604c961c50e57c5fb242607d/optimizing-recoveries-of-planar-pesticides-in-spinach-tandem-gcb-nh-2-8-gcb-psa.jpg)