Embed Size (px)
DESCRIPTION
A case presentation presented on December 2013 Egyptian society of Pathology meeting.
Citation preview

CASE PRESENTATION
BY
Salma Tarek Mahmoud
Assistant Fellow at Ahmed Maher Teaching Hospital

A 22 ys old female patient complaining
of left breast mass.
Excision was done

Gross examination
•A fairly defined rubbery mass measured
10x7x7 mm.
•Cut section was homogenous grayish white

Microscopic examination




PAS staining was done


Cytokeratin

c


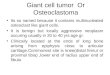
Diagnosis
Granular cell tumor

Granular cell tumor( GCTs)
Uncommon tumor thought to be derived from schwann cells.
Abrikossoff first described this tumour in 1926 as
‘‘granular cell myoblastoma’’, assuming it was of
myogenic origin; some even refer to the lesion as
‘‘Abrikossoffoma’’.
Considered benign, only rare reports of malignant
variants
Incidence
Occur in any age but are most common in
fourth, fifth and sixth decades of life, rare in
children.
It is about twice as common in women as in men.

Site
Arise in any organ as solitary painless nodule
Most frequently in oral cavity typically the tongue
Internal organs, particularly larynx, bronchus, stomach
and bile duct.
Clinically
Approximately 10–15% of patients have lesions at
multiple sites.
Multiple lesions may appear synchronously or over a
period of many years.
Gross picture
Poorly circumscribed nodule less than 3 cm
Cut section pale yellow-tan or gray.

Microscopically
Infiltrating compact nests or sheets
Bland looking large polygonal to spindle cells
Eosinophilic cytoplasmic granules
Nuclei are small dark monotypic
+/- vacoulization and clearing

Pseudoepitheliomatous
hyperplasia of the overlying
squamous epithelium, should
not be mistaken for squamous
cell carcinoma.
In close proximity to peripheral
nerve bundles

Special Stains and
Immunohistochemistry
S-100 protein: highlights cytoplasmic
granularity with strong cytoplasmic and
nuclear staining
Carcinoembryonic antigen (CEA): diffuse
immunoreactivity
Cytokeratin and (EMA) are negative
Myoglobin negative
(ER) and (PR) are negative
PAS positive diastease resistant cytoplasmic
granules


GCTs in breastIncidence
5%- 6% in breast.
Premenopausal women in 40’s, reported in adolescents, elderly women and men
May be more common in African-American women
Site
Superior medial quadrant (course of supra-clavicular nerve)
Clinical features
Usually solitary unilateral, rarely multiple
Painless firm mass, may be associated with skin retraction and nipple inversion

Gross
Cut surface is fairly
defined white - gray to
yellow
Less than 3 cm but
reported up to 9 cm.

Radiologically
X-ray
MammographySuggestive of malignancy due to apparent infiltration, stellatemass without calcification

Differential Diagnosis

D.D
Reactive histocytic lesion
Invasive breast carcinoma
Apocrine carcinoma
Myoblastomatoid, Lobular carcinoma histocytic variant
Alveolar soft part sarcoma
Metastatic malignant melanoma
Metastatic renal cell carcinoma

Reactive Histocytic lesions
Dispersed
histocytes with
mixed population of
inflammatory cells

Older age
Usually in outer
quadrant
large cells with
pleomorphic nuclei,
prominent nucleoli,
mitosis
Typically associated with
intra-ductal component
IHC: Positive for
cytokeratin, GCDFP-15
Apocrine carcinoma

Myoblastomatoid invasive lobular
carcinoma, histocytic variant Older age
Associated with
infiltrative
component
Loosely cohesive
tumor cells
IHC: Positive for
cytokeratin

Alveolar soft part sarcoma
• Deep soft tissue
• Pleomorphic cells
• Cells are divided into packets by thin walled vessels
• Alveolar pattern if cells discohesive
• Vascular invasion common
• IHC: Positive for Myoglobin

Metastatic malignant melanoma
Old age
History of primary
elsewhere
Nuclei usually show
nucleoli
Cytoplasmic pseudo-
inclusions
Melanin pigments
IHC: Positive HMB- 45

Metastatic renal cell tumor History of primary
elsewhere
Nests, separeted by sinasoids
Well defined cell membrane
Nuclear pleomorphism
Prominent nucleoli in high grades
Clearing of cytoplasm
IHC: positive for EMA




Take home message GCTs is an uncommon tumor occur in any age.
5%-6% incidence in breast, inner upper quadrant.
Pose a real diagnostic challenge for physicians.
Clinically and radiologically misdiagnosed as carcinoma
Preoperative diagnosis with core needle biopsy is important because treatment is with wide excision , rather than mastectomy.
Less than 1% of all GCTs, including mammary lesions, are malignant.
The prognosis for benign GCT of the breast is excellent.
Recurrence occurs in 2-8% of individuals after excision with wide margins