Embed Size (px)
Citation preview

PROF.DR.K.H.NOORUL AMEENR.Pandi chelvan
M6

16 yr old boy admitted in imcu for c/o fever - 2 days c/o seizure – 1 day
Presenting illness h/o fever -2 days intermittent fever low grade not asso. With chills and rigor h/o seizure –on the day of admission 15 episodes each episode last for 1 min

involving all four limbs tonic – clonic in nature asso with impaired consciousness asso with urinary incontinence asso with frothing from mouth h/o vomiting No h/o trauma No h/o tongue bite

Past history: known case of seizure disorder- GTCS
for last 5 yrs on regular treatment Tab. Phenytoin 100mg bd Tab. Carbamazepine 200mg tds Tab. Phenobarbitone 100mg 2od..
Tab.Sodium valproate 2oomg tds
Family history: his brother suffering from seizure
disorder since his 7 yrs of age

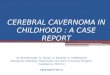
CT PICTURE TAKEN 5 YRS BEFORE

On examination unconscious not obeying oral command no response to painful stimuli dyspneic febrile no icterus no pallor no cyanosis no clubbing no lymphnode enlargement
febrile

Vitals PR 98/min BP 140/90mmhg RR 28/minCVS -S1,S2 heard no murmurs.RS NVBS no added sounds. P/A soft no organomegaly

CNS examination on the day of admission pt is unconscious
E1 V1 M1 GCS 3/15 B/L pupil 4mm equal reacting to light B/L plantar extensor Fundus- B/L papilloedema No neck stiffness
Oculocephalic reflex intact

PROVISIONAL DIAGNOSIS Seizure disorder-Status epilepticus Raised ICT-? CAUSE

16 YR OLD BOY WITH PAPILLOEDEMA AND SEIZURE
Differential diagnosis:
1.CNS infection-acute/chronic
2.SOL
3.Cerebrovascular disease
4.Cerebral venous sinus thrombosis
5.Hypertensive encephalopathy

pt treated in imcu with Nasal o2; Inj. Diazepam 100 mg iv Inj. Phenytoin 600mg iv infusion Inj .Cefotoxime 1g iv bd Inj. Mannitol 175 mg iv bd Inj .Lasix 20mg Patient had status epilepticus in imcu treated with continuous Midazolam infusionAfter controlling the status epilepticus patient transferred to general medical ward

Subsequent neurological examination in general medical ward
HMF – normal
Cranial nerves- Fundus B/L Papilloedema Left facial muscle weakness
Tone B/L normal
Power Right Left UL 5 4- LL 5 4- DTR + +
Plantar extensor extensor
Hand grip 100% 50%

16 YR BOY SEIZURE AND HEMIPARESISDIFFERENTIAL DIAGNOSIS

16 YR OLD BOY SEIZURE AND HEMIPARESISDIFFERENTIAL DIAGNOSIS
1.POST ICTAL
2.SPACE OCCUPYING LESION
3.INFANTILE DISORDER -HEMIPLEGIA HEMISEIZURE EPILEPSY(HHE) SYNDROME
-RASMUSSEN’S ENCEPHALITIS
-STURGE WEBER SYNDROME
4.VASCULAR DISORDER -ANTIPHOSPHOLIPID AB SYNDROME
-CEREBRAL VENOUS SINUS THROMBOSIS
-CEREBROVASCULAR DISEASE
-CNS VASCULITIS5.METABOLIC -HYPOGLYCEMIA

Investigations :
Urine R/E: Albumin- nil Sugar -nil Deposits- 1 -2 pus cells /hpfCBC: TC -9800 DC P60;L37;E3
ESR 6/15
Hb 13 PCV42 MCV81.6 MCHC33.9 MCH27.6 PLC1.9 lac

LFT: Total bilirubin 1 mg Direct bilirubin 0.2mg SGOT 39 SGPT 59
In view of papilloedema lumbar puncture not done
Neuromedicine opinion Seizure disorder/ recurrent seizure/A/c febrile illness suggested MRI brain continue the same


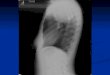
RECENT CT BRAIN PLAIN

Hetero dense lesion in right fronto parietal region
Hetero dense lesion in right fronto parietal region

MRI BRAIN T1 IMAGE


MRI BRAIN T1 CONTRAST

MRI BRAIN T2 IMAGE



Well defined T1,T2 mixed intensity cortical lesions in right fronto parietal region
Both cystic and solid areas .Mass effect on the ipsilateral lateral ventricle with
subfascial herniation to left side.No surrounding edema.
Cystic areas on contrast shows rim enhancement.
Solid areas shows moderate enhancement with some non enhancement.
Abnormal parenchymal enhancement on post contrast study.

Radiological differential diagnosis
Astroblastoma
Pilocytic astrocytoma
Pleomorphic xantho astrocytoma
Intra axial schwannnoma.

Pt transferred to neurosurgery department and operated
procedure: fronto parietal craniotomy
tumour decompression
cyst aspiration biopsy taken

CYTOLOGY REPORT Eosinophilic proteinaceous material
HISTOPATHOLOGY REPORT Macro: multiple grey brown soft tissue Micro: multiple fragments of brain
parenchyma with adjoining neoplasm composed of spindle cells arranged in fascicles and bundles disclosing hypocellular area with peripheral nuclear palisading, interspered vascular areas and areas of haemorrhage
feature suggesstive of schwannoma

SEIZURES ,PAPILLODEMA & CEREBRAL SOLA.Primary tumour
1.Gliomas-Astrocytomas Oligodendroglioma
2.Medulloblastoma
3.Schwannoma
4.Cns lymphoma-primary/secondary
5.Haemangioma
B.Secondaries
CNS Infection- TB,Cysticercosis, Toxoplamosis, Fungal infection, Hytadid cyst

SEIZURES IN TUMOUR1.Vasogenic odema
2.Raised intracranial tension
3.tumour with bleed
4.Malignant transformation
5.secondary infection
6.Irritative focus
7.chemotherapeutic drugs
8.meningeal infiltration

Convulsion seen in 20-50% of pts with cerebral tumour
Reported in 60-70%of supratentorial gliomas and parasagittal meningiomas
Rare in cases of base of the skull and posterior fossa tumours
Focal seizures helps clinical localisation
Generalised seizure- no localisation value

STATUS EPILEPTICUScontinuous seziure
repetitive discrete seizure imparied consciousness in the inter ictal
period. Subtypes: generalized convulsive generalised nonconvulsive
Duration to meet the definition of status epilepticus is about 15 – 30 min.
Practically seizure prompts the acute use of anticonvulsant therapy.

CAUSES Anticonvulsant withdrawal
Noncompliance
Metabolic disturbance
Drug toxicity
Cns infection
Cns tumour
Refractory epilepsy
Head trauma


REFRACTORY EPILEPSY 1/3 rd of pt not respond to treatment with single
drug
--focal epilepsy with structural lesion --multiple seizure types --developmental delay require multiple
drugs
Combine first line drugs i.e, carbamazepine,phenytoin,valporic acid,lamotrigine
If not controlled add topiramate,levetiracetam

Surgical treatment:
approximately 20-30% epilepsy resistant to medical therapy
temporal lobectomy amygdalohippocampectomy lesionectomy multiple subpial transection hemisperectomy or multilobar resection corus callosotomy


Seziures occuring for the 1st time in adult life/old age
Asso. With signs and symptom of raised intra cranial pressure or focal neurological deficit
The changing character/types over a period of time
Those have prolonged postictal paralysis
Those asso. With poor response to therapy
those have status epilepticus
SUSPECT NEOPLASTIC AETIOLOGY

SCHWANNOMAS
Neuromas, Neurinomas,Neurolemmomas
Arise from schwann cells of nerve roots
Mostly from 8th cn; 5th cn is 2nd most common
Arise from any CN except 1st n 2nd CN
NF2 strongly predispose to vestibular schwannoma
Schwannoma of spinal roots occur in NF2and
NF1 also


INTRA CEREBRAL SCHWANNOMARare
Fewer than 40 cases were reported since 1965
Unlike vestibular schwannoma mostly seen young people
80% were under 30 yrs
Asso. With NF in 4 cases

On MRI T1w images- hypo/iso intense lesions cystic and solid components unlike vestibular schwannoma
calcification quite characterstic surrounded by hypersignal on
T2w images due to edema or gliosis

Most frequently –Frontal or Temporal region occur any whereD/D -Pilocytic astrocytoma -Meningioma -Metastatic tumour

Origin remain unsettled
Several hypothesis say
Perivascular nervi plexi
Multipotential mesenchymal cells
Ectopic schwann cell
Pial cell converted into schwann cell Mostly benign cells
4 cases reported as malignant
Treatment complete excision



After surgery seizures free
papilloedema subside
residual neurologigal deficit improved



Carry home message
1.pt known epileptic more than 5yr with reccurent
seizure with poly therpy –not investigated
2.only after status admitted and investigated found to have SOL
3.causes of seizures in SOL understood
4.type and rarity of this case evaluated
5.further course of treatment planned

REFERRANCE: API MEDICINE
ADAMS-NEUROLOGYHARRISON