Embed Size (px)
Citation preview

INTERESTING CASE OF DEEP VEIN THROMBOSIS
PROF.DR.K.H.NOORUL AMMEN’SUNIT
M5
DR.M.ARIVUMANI

20 Year old Miss.Priya admitted on 18/7/11 withc/o fever 1 month duration intermittent fever initially,then she had
continuous fever,low grade,not asssociated with chills or rigors
h/o swelling over left leg 10 days duration associated with pain constant pain limiting movementsh/o easy fatiguability +


H/o body pain +No h/o joint painNo h/o breathlessnessNo h/o palpitationNo h/o chest pain,syncopeNo h/o abdominal distension,painNo h/o easy bruisability,rashesNo h/o bleeding tendencies on admissionNo h/o trauma

Past history no h/o similar illness in the past h/o bleeding gums occasionally +Personal history regular menstrual cycles.Family history nil significant

Examination
General examination Patient concious/oriented febrile pallor + no cyanosis,no clubbing,no icterus swelling of left lower limb + no generalised lymphadenopathy

Vital signs PR-108/min,regular,felt in all peripheral vessels BP- 110/70mmhg RR-20/min Temp- 101 degree F

• Systemic examination CVS- S1S2 Heard systolic murmur + RS-NVBS heard.no added sounds P/A-soft CNS-NFNDL/E of left leg-swelling of left leg +,tender homans sign +

• With the above clinical profile pt got admitted in vascular surgery dept.
• Provisional diagnosis of DVT(wells score 3) was made
• Hand held doppler revealed no significant thrombus in deep veins
• Patient was started on INJ.Heparin 5000u qid.• Symptoms started improving after two days

• On third day patient developed menorrhagia and malena,so heparin stopped.
• Patient had persistent fever and sever pallor so physician opinion sought.
• We took over the case

While receiving in medical ward
• Patient had h/o fever• h/o breathlessness• h/o bleeding pv• h/o malena• h/o swelling over left leg(swelling
decreased,pain subsided)

Examination
• Patient concious,irritable• Severe pallor +• Dyspnoeic,tachypnoeic • Sternal tenderness +• No cyanosis,no clubbbing,no icterus• No lymphadenopathy

• Vitals PR-120/min RR-38/min BP-100/70 mmhg febrileSystemic examination CVS-S1S2+,systolic murmur +

• RS-NVBS+,occasional creps +• P/A-Liver 4cm palpable below RCM
Spleen 3cm palpable below LCM• CNS-NFND

INVESTIGATIONS
CBC-Hb-5.4 grams TC 10400 DC P40 L 60 ESR 25/52 PCV 16% Platelet-58000RFT- WNLLFT-WNLUrine routine-WNL

QBC-negativeWIDAL-negativeMSAT-negativeUrine c&s- no growthBlood c&s-no growthPeripheral smear- RBC count reduced,normocytic RBC’S with
hypochromic cells WBC-monocytosis observed,few atypical monocytoid
cells seen Severe thromobocytopenia observed

Reticulocyte count-2.3%
22/7 24/7
PT 15.4 sec 17.8sec
PTT 34.0sec 25.6sec
INR 1.5 1.2

HIV –negativeD-Dimer 5.35 mcg( >0.5mcg positive)FDP- 20mcg/ml( >5mcg/ml positive)LDH-528U/L(135-214u/l)Serum homocysteine- WNLAPLA-WNLProtein c,PROTEIN s-not affordable

USG abdomen hepatosplenomegaly + no para aortic nodes no free fluidChest xray normalECG- Sinus tachycardia

HEMATOLOGIST OPINION OBTAINED AT RGGGH
CBC- TC 2800 DC P20%, L 10% , ATYPICAL CELLS 70 % HB 7.3 gms/dl PCV 21% Platelet 54000 ESR 18/42

Peripheral smear numerous atypical cells + platelets decreasedHematologist advised BMA To start T.Allopurinol 1 tds While waiting for BM diagnosis patient was
managed with packed cells, FFP,Platelet concentrate,antibiotics

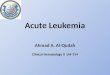
BMA done on 29/7/11



Lymphoblast & myeloblast

lymphoblast

Myeloblast

myeloblast

BMA REPORT
• Marrow contains 90% blast cells comprising of both lymphoblast and myeloblast
• Final diagnosis BILINEAL OR BIPHENOTYPIC ACUTE LEUKEMIA
with Deep vein thrombosis

BIPHENOTYPIC ACUTE LEUKEMIA(BAL)
• Biphenotypic acute leukaemia is an uncommon type of leukemia.
• The precise incidence is uncertain, it is likely to account for approximately 5% of all acute leukemias.
• BAL can be de novo or secondary to previous cytotoxic therapy.
• It has been included in the WHO classification of haemopoietic malignancies as acute leukaemia of ambiguous lineage

WHO classification of hematological malignancies
• Chronic myeloproliferative disorders• Myeloblastic syndrome• Leukemia of myeloid origin• Leukemia of lymphoid origin• Leukemia of ambiguous origin

• Acute leukemias of ambiguous lineage include 1.Undifferentiated acute leukemia Leukemic cells that can not be classified as either myeloid or lymphoid cells 2. Acute leukemias of mixed phenotype. Mixed lineage or biphenotypic acute leukemia where both types of cells are present.


EGIL scoring for biphenotypic acute leukaemia. The score for each lineage is calculated and if that lineage score > 2, that lineage is present.
POINTS T CELL LINEAGE B CELL LINEAGE MYELOID LINEAGE
2 POINTS CD 79 CD3TCR
MPO
1 POINTS cCd22CD10CD19CD20
CD2CD5CD8CD10
CD13CD33CDw65CD117
0.5 POINTS TdtCD24
TdtCd17cd1A
CD15CD15CD24
EGIL-European group for immunological classification of leukemia

TREATMENT
• BAL has proven to be very difficult to treat with many cases being resistant to induction chemotherapy and those that enter remission have a high risk of relapse.
• There is no agreement on how the disease should be treated.
• The majority of patients receive treatment according to the morphology of the blasts, with either AML or ALL induction.
• If patients enter complete remission, consideration should be given to consolidation with stem cell transplantation.

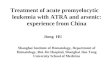
Copyright ©2009 Ferrata Storti Foundation
Zheng, C. et al. Haematologica 2009;94:1778-1780
Figure 1. Treatment schedule on the BAL patients

When immunophenotyping is not possible steroid trial should be started

Prognostic factor for CR age<60 yearsPrognostic factor for survival age<60years achievement of CRThe prognosis of biphenotypic acute leukemia patients is
poor when compared with de novo acute myeloid leukemia or acute lymphoblastic leukemia.
Biphenotypic acute leukemia patients have abnormal karyotype, extramedullary infiltration, relapse, and resistance to therapy after relapse

DVT IN ACUTE LEUKEMIA
Studies have demonstrated that the risk of VTE associated with the hematological malignancies acute leukemia, lymphoma, and multiple myeloma is considerable.
Contributing factors include hypercoagulablefactors,Hyperleukocytosis,
antineoplastic therapies such as high dose corticosteroids, L-asparaginase, and new immunomodulatory agents; central venous catheters; and hematopoietic growth factors.

• Primary and secondary pharmacological prophylaxis can be problematic in these patients who are often thrombocytopenic. Strategies to prevent VTE, especially upper extremity catheter-associated thrombosis need to be developed.

The incidence of VTE at diagnosis was 1.2 % in ALL, 3.2% in APL and 2.5 % in non-M3 AML.

• Thromboembolism is a well recognized complication of hematologic malignancy. The pathogenesis of the cancer-related prothrombotic state are
1. activation of blood coagulation via procoagulant substances,
2.impairment of fibrinolytic pathways, 3.alterations of endothelium toward a thrombogenic
state
Journal of Thrombosis and Haemostasis, 3: 1985–1992

The classic "gold standard" is contrast venography. Although very accurate, this method requires radiologic facilities and expertise and is invasive and sometimes uncomfortable for the patient.
Ultrasonography, with noncompressibility of the vein as the sole criterion, has largely replaced contrast venography
• investigation is limited to the femoral vein in the groin and the popliteal vein in the popliteal fossa

• The combination of the assessment of clinical probability and the measurement of the D-dimer has been shown to be useful. The clinical probability can be best assessed by wells score, which results in a classification of either DVT likely or DVT unlikely.
• D-Dimer is a degradation product of cross-linked fibrin and therefore concentrations of D-dimer below a certain cut-off level are considered to indicate the absence of thrombosis(higher negative predictive value)

Wells Probability score for DVT<2 DVT unlikely, >2 DVT likely
Clinical features points
Active cancer 1
Paralysis,paresis,recent immobilisation of lower extremities
1
Localised tenderness along deep venous system
1
Entire leg swollen 1
Calf swelling>3cm larger than asymptomatic side
1
u/l pitting edema 1
Collateral superficial veins(non varicose) 1
Previously documented DVT 1
Alternative diagnosis as likely or more likely than DVT
-2

NCCN Guidelines for Deep Vein Thrombosis Treatment in Cancer Patients
• The therapy guidelines are aimed at in-hospital treatment and list the following drugs for anticoagulation:
*Unfractionated heparin: 5,000 units S.C TDS *LMWH-dalteparin, enoxaparin, or tinzaparin *Pentasaccharide, fondaparinux, 2.5 mg
subcutaneous daily *If patients cannot take anticoagulation
medications, compression devices can be used, including graduated compression stockings

• The guidelines suggest using low-molecular-weight heparin for long-term therapy for prevention of recurrent deep vein thrombosis in patients with advanced or spreading cancer. The minimum time for treating deep vein thrombosis is 3–6 months; pulmonary embolism requires 6–12 months of treatment.

• Migrating venous thrombosis in acute leukemia• Musil D, Krc I.• Source:Department of Vascular Diseases, Institute of
Pathological Physiology, Palacky University, Czech Republic.
• Abstract:We present a 55-year-old man with acute migrating thrombophlebitis and deep vein thrombosis of muscle veins in both calves indicating occurrence of acute myelomonocytic leukemia. Thrombosis of superficial and deep veins of the lower limbs arose in spite of the adequate anticoagulation therapy with warfarin

Venous thromboembolism in patients with acute leukemia, lymphoma, and multiple myeloma
• Ted Wuna, b, c, d, , and Richard H. Whitee
• a Division of Hematology and Oncology, UC Davis School of Medicine, USA
• Abstract• The association of malignancies and venous
thromboembolism (VTE) is a long held axiom in medicine. A growing number of studies have demonstrated that the risk of VTE associated with the hematological malignancies acute leukemia, lymphoma, and multiple myeloma is considerable. In fact, the incidence associated with these malignancies exceeds that for many solid tumors.

Review ArticleThrombosis in children with acute lymphoblastic leukemia: Part III.
Pathogenesis of thrombosis in children with acute lymphoblastic leukemia: effects of host environment
• TE in association with childhood ALL is a multifactorial entity resulting from the interaction of the disease, chemotherapy and its effects, and possible prothrombotic states inherent to the host. The few studies conducted so far in children with ALL have reported wide variability in the prevalence of prothrombotic defects and its impact on the risk of TE.
• Thrombosis ResearchVolume 111, Issue 6, 2003, Pages 321-327

Venous thromboembolism in patients with acute leukemia: incidence, risk factors, and effect on survival
• Journal of american society of hematology( APRIL 23 2009)
• Thombosis was a clinical presenting manifestation in 13 patients of 379 (3.4%, 95% CI 1.8%–5.8%): one with ALL (1.4%), three with APL (9.6%), and nine with non-M3 AML (3.2%). After exclusion of the four patients with arterial ischemic stroke (two with APL and two with non-M3 AML),the incidence of VTE at diagnosis was 3.2% in APL and 2.5%in non-M3 AML

References:Harrisons principles of internal medicine 17th edWilliams textbook of hematology 8th edWintrobe’s clinical hematology 12 th ed