Embed Size (px)
Citation preview

1
INTRODUCTION TO CLINICAL THINKING
GROUP C PRESENTATION
Group Members
Katharine Blackburn, Steven Edwards,
Chun-Chih Jim Huang, Andre Humphrey, Aleksandar Zivkovic
August 6th, 2007

2
Patient Problem Recurring chest discomfort for last 2
weeks
12:45 a.m. Patient awakens during the night with elevated pain
Severity raises concerns to warrant Emergency Room Visit

3
• 1:00 a.m.-Wife uses online patient portal to create a cursory pre-admit ED record. The electronic form will be the basis of the Chief Complaint and will have different degrees of detail depending on how much time is taken entering data prior to the ER visit.
• (Example: from Vanderbilt Medical Center)

4
• The wife is also able to attach an electronic medical history file to the online web portal record.
• The record will:– Be in a single adopted industry format and
originate from a company specializing in the consolidation of medical record information from hospitals, pharmacy’s etc., around the country.
– The file will be encrypted and may be on a USB drive and/or a CD. (DOD encryption level with password protection via biometric fingerprint.)
– Information will be easily up-loadable to major EMR systems who have all agreed on standard formats
• In addition, estimated ED arrival time is noted on the record at 30 minutes

5
• 1:35 a.m.-the patient enters the ED for confirmation check in with front desk assistant who quickly confirms the patient portal submission record, the chief complaint, records blood pressure/vitals, and gives the condition a 1-5 rating. (5 being very urgent). (John Doe=2)
• The patient is then referred to a self service kiosk to complete the registration record where more detail may be needed.

6
• As soon as the kiosk entry is completed, the patient is now placed in the queue
• At this point in time bioterrorism syndromic decision support flags may/may not be triggered based on information entered.

7
• ER nurse receives the completed record in her work queue wirelessly on a Motion tablet C5 and reviews the information for completeness including current medications, allergies, and historical data.
• Nurse follows up with patient in private area to fill in the gaps and note any pertinent observations prior to physician visit.
• Bar code identification bracelet is printed and placed on patients wrist. Medication bracelet has photo to deter patient misidentification and possible near misses.

8
Triage Summary55-year-old man came at the emergency room because of recurrent episodes of epigastric and chest discomfort in the last two weeks. The discomfort, mild and lasting only few minutes, was unrelated to inspiration, movement or meals and was not accompanied by other symptoms. There was no previous history of angina or myocardial infarction, hypertension or hypercholesterolemia. The family history was also negative for cardiovascular diseases. The patient denied use of tobacco, alcohol or drugs. Upon arrival in the emergency room the patient was in good condition, the pain was absent. The blood pressure was 130/80 mmHg, the pulse rate 72 beats per minute.

9
Before Physician Interview
• The ER physician is able to check the patient’s information prior to the interview.
• The physician has:– Triage summary– Patient’s basic
information– Patient’s previous
medical record• Immediate
observations before speaking

10
Conduct a Clinical Interview
• Elicit a complete account of patients’ concerns– Open-ended questions– Avoid impatient, arrogant,
rushed, confusing
• Initial hypothesis– Closed-ended questions– Hypothetical-deductive
method– Looking for clues to confirm
or exclude the hypothesis

11
Physician Interview—Data Solving Process
Chief Complaint
Data Collection
1 . History taking2 . Physical examination3 . Para-clinical studies
Data Processing
1. Clue clustering2. Forming a differential3. Information suppression4. Hunch and intuition5. Algorithms / flowcharts
Problem List with--Assessment--Plan
Problem-Solving Methods

12
Physician Interview—Scenario I
• Chief Complaint– Recurrent epigastric and chest
discomfort– Mild and lasting only few
minutes– Unrelated to inspiration,
movement or meals– Not accompanied by other
symptoms• Initial obtainment
– Male, 55 years old– Good condition, no pain upon
arrival in ER
• History– No history of angina or MI,
hypertension or hypercholesterolemia
– No family history for cardiovascular diseases
– No use of tobacco, alcohol or drugs
• Physical Examination– Blood pressure: 130/80
mmHg– Pulse rate 72 beats per
minute.

13
Information Technology During Physician Interview
• Electronic medical record system helps remind the patient’s history, organize clues and form the problem list.
• Diagnostic decision-support tool helps to approach the correct diagnosis.– CACDDST (Computer-Aided Clinical Diagnostic Decision-Support
Tool)– DXplain– Med Calc3000– Incorporated into EMR system
• The physician can order/schedule the tests and track the results online.– The alert can be directly sent to the ordering physician's portable
device if any abnormal clinical results happen to the patient.

14
Physician Interview—Scenario II
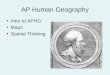
• Pretest probability of coronary artery disease according to age, sex, and character of symptoms
• Result: the pre-test probability of a cardiac origin of the pain was 21.5%
• Further data collection: ECG, blood test, echocardiogram

15
Age Asymptomatic % Non-anginal chest pain %
Atypical angina % Typical angina %
Men Woman Men Woman Men Woman Men Woman
30-39 1.9 0.3 5.2 0.8 21.8 4.2 69.7 25.8
40-49 5.5 1.0 14.1 2.8 46.1 13.3 87.3 55.2
50-59 9.7 3.2 21.5 8.4 58.9 32.4 92.0 79.4
60-69 12.3 7.5 28.1 18.6 67.1 54.4 94.3 90.6
Pretest Probability of Coronary Artery Disease According to Age, Sex, and Character of Symptoms

16
The Results for the Additional Tests
• Creatine kinase was 1200 U/l, MB isoenzyme 39 U/l;• Lactate dehydrogenase 503 U/l;• Aspartate aminotransferase 57 U/l and alanine
aminotransferase 52 U/l, serum troponins T and I were negative.
• The hematocrit was 31%,• Hemoglobin 10.8 g/ dl,• The mean corpuscolar value 95,• The white cell count 5.500/mmc,• The platelet count 256.000/mmc,• Serum cholesterol level was normal.
An echocardiogram revealed a slight pericardial effusion.

17
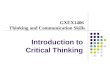
The operating characteristics of CPK-MB and Isotroponin I as found in a external source (1) were the following:
Enzyme testing (>24 hours after symptom onset)
Sensitivity Specificity Likelihood ratio +
Likelihood ratio -
Cardiac troponin I
95% 98% 47 0.03
CPK-MB 55% 97% 18 0.46
Therefore, assuming a pre-test probability of myocardial infarction of 3% (2) the post-test probability was:
3 x 0.03 x 0.46 = 0.0414
(1) Beyer IW, Karmali R, Demeester-Mirkine N, Cogan E, Fuss MJ. Serum creatinine kinase levels in overt and subclinical hypothyroidism. Thyroid 1998; 8: 1029-31.
(2) Bennett NM, Paris MC. Myocardial Infarction In: Black ER, Bordley DR, Tape TG, Panzer RJ. Diagnostic Strategies for Common Medical Problem. 2nd edition. Philadelphia: American College of Physicians, 1999.

18
More history:• Mild paleness• Liver slightly enlarged with smooth margin and normal consistence• Neurological examination was negative: the reflexes and the motor
strength were normal so were the muscular masses; there was muscular pain; the gait was normal.
Routine laboratory tests, performed one month before: • Moderate elevation of transaminases (4 times over the normal value)
with other liver function tests normal• Mild normocytic anemia (hematocrit 36%, hemoglobin 11.7 g/dl)• Markers for hepatitis virus B and C and for HIV were negative.• Ceruloplasmin, alpha-1-antitrypsin and ferritin levels were normal.
Physician ordered an abdominal ultrasound that revealed a slightly enlarged liver.

19

20
Final Diagnosis: Hypothyroidism

21
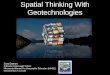
Nursing Workflow

22
New assignment for youroom 404. Please round.
Accept Communicate

23
John Doe 7/24/1952
8/5/2007 1:45 AM
Change duration Document Chose EKG View Alerts
Name: DOB:
Read Time:

24
Your bedside accessHeart Healthy LivingWhat is pericardial effusion?What is hypothyroidism?
Educational ProgramsNutrition Services InformationJohn Doe 7/24/1952 Wagner Wing Room 404
Unrestricted
Today’s Menu choices - Breakfast
Oatmeal with brown sugarBagel with cream cheeseEgg Sandwich on English MuffinFruit, yogurt and granolaAssorted muffins and toast
Order
Order
Order
Order
Order
Name DOB
Diet
Select
Select
Select
Select

25
Bedside System
John Doe 7/24/1952 Wagner Wing Room 404
Low Salt DietDietary Requirements:
Laboratory Results
Your Plan of Care
Check your mail
Pain Monitoring
Patient Survey
Call Your Nurse
Today is August 5, 2007 Your Nurse is: Nancy Smith

26
New prescription Orders are availablefor Mr. Morris.
Accept Communicate
Pyxis Machine

27

28
Date and time of entry. Mr. Doe………
New Orders for Mr. Morris… lab orders

29
12534Sample ID
Tracking Information
Creatine kinase Isoenzymes
CBC
Lipid Profile
Draw Time
8/5/2007 5:00am
8/5/2007 5:00am
8/5/2007 5:00am
8/5/2007 5:00am
Location
In transit to Lab
In transit to Lab
In transit to Lab
In transit to Lab

30
Patient Summary

31
Pharmacy Workflow

32
Pharmacy Information System Overview
• Our Electronic Pharmacy System automates the hospital’s pharmacy communication and workflow. It coordinates the medication ordering, dispensing, and administration activities. It is a modular system that can be integrated with other Enterprise Clinical Systems, and the system can deliver timely alerts, proactive guidance, and financial support suggestions throughout the treatment process.
• This portion of the presentation will demonstrate how the physician, pharmacist, and the nurse use the pharmacy electronic medical record system to ensure patient safety.

33
Medication Ordering Workflow
Medication Ordering Workflow - Physician
RX
PH
AR
MIP
RN
IMM
D (I
nter
nal M
edic
ine
Phy
sici
an)
Enter patient’s chart and go to
Order Entry, Navigators, or
Order Sets
Best Practice Alert (BPA) may trigger for allergy
documentation if not verified
Physician enters orders
MD orders the appropriate medications
MD may choose to continue with original
order, accept the alternative, or cancel
Physician signs the orders
Once the patient presents, nurse
releases the orders
Are medication(s) needed STAT?
MD changes the medication(s) to a
STAT or ASAP priority
Is this a conditional
order?
MD updates the administration instructions to
reflect conditions for the order
The instructions may say something like “start PO form
as soon as patient can tolerate
Are these preadmission
orders?
MD signs and holds the order,
selecting a reason of “preadmission”
Yes
No
YesYes
NoIs this medication on the formulary?
No
No
Yes
Medications are administered to
the patient
Pharmacist notifies physician
and documents an Intervention
Non-formulary or out of stock medications
may trigger therapeutic alternative
alerts
Pharmacist verifies
medications
Pharmacist verifies
medications

34
Order Verification Screen

35
Dispensing Meds

36
Dispensing Meds

37
Discharge

38
Prognosis
• Subacute thyroiditis is self-limited, generally subsiding in a few months; occasionally, it recurs and may result in permanent hypothyroidism when follicular destruction is extensive.

39
Treatment
• Treatment is with PREDNISONE 30 mg once/day, gradually decreasing the dose over 3 to 4 wk time.
• The prescription is written using a CPOE and the ePrescribing connection

40
Summary of Key Benefits

41
Key Benefits
• Patient Portal– Allows the patient a less stressful environment to enter data prior to ER visit– Alleviates work stress by ER staff which impacts errors/mix up/fatigue– Pre-notifies the ED of potential workload in near future prior to patient arrival
• ED Kiosk– Alleviates works stress by ER staff which impacts errors/mix up/fatigue– Adds an additional quality assurance layer by having the patient review their
own information• Medical History Secure on Secure Media
– Portability of vital piece of EMR information to assist caregivers in making best decisions
– HIPPA Compliant security access• Electronic EMR Support
– Integrated Diagnostic Decision Support– Integrated Decision Support Tools Research/Probability/Sensitivity/Specificity – Integrated Test Ordering and Results with Alerts

42
Key Benefits (Cont.)
• Nurse – Integrated biometric security sign on– PDA/voice recognition with language processing and electronic
handwriting recognition for dictation directly into medical record providing key portability, time savings to workflow processes, and reducing stress/potential errors.
– Bedside Patient System Manager-Technology at the bedside provides key benefits to patient satisfaction in dietary ordering, patient education, daily patient surveying, medical record review, TV/movie, internet, telephone, and video games options.
• Pharmacy– Integration of Pharmacist prescription review and receipt of orders
within EMR system. – Medication verification and patient safety checks built into system.– Use of EMR System with local pharmacy integration will reduce calls to
and from the pharmacist which will reduce errors, free up valuable time, and enable the Pharmacist to focus on core job functions.

43
Thank You