Embed Size (px)
Citation preview

Pediatrics
Kiyetta Alade, M.D., RDMS
Assistant Professor
Director, Pediatric Emergency Ultrasound
Section of Emergency Medicine
Department of Pediatrics
Baylor College of Medicine
Texas Children’s Hospital
Ultrasound Fundamentals

Page 2
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Goals and Objectives
•Describe and operate the basic functions of the
ultrasound machine
•Discuss the common pitfalls with ultrasound-guided
vascular access
•Integrate the “landmark technique” and dynamic
ultrasound when performing central venous
cannulation

Page 3
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Gain
•Gain: Adjusts the intensity of returned echoes
shown on display
‐ Increasing gain makes picture brighter

Page 4
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Gain
Gain will amplify all returning echoes equally

Page 5
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Gain

Page 6
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
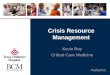
Ultrasound Fundamentals
•Depth: Can be adjusted to ensure entire structure
of interest is on the screen
Page 7
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Depth

Page 8
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Gain / Depth

Page 9
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Ultrasound Fundamentals
•Axial resolution: US machines ability to differentiate
objects in plane parallel to traveling wave
‐Increase frequency or decrease wavelength to
improve
•Lateral resolution: US machine’s ability to differentiate
objects in plane perpendicular to traveling wave

Page 10
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Resolution
Axial Lateral

Page 11
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Resolution
•Low resolution (2-4 MHz)
‐Lower frequency
‐Deeper penetration
•High resolution (8-14 MHz)
‐High frequency
‐Poor penetration (best to image superficial structures)

Page 12
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Probe Selection
•High frequency
‐Linear Array
•Low frequency
‐Curvilinear
‐Phased array

Page 13
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Ultrasound Fundamentals
•Every probe has raised marker to correlate with the
side of the screen with some type of identifier (dot,
logo)

Page 14
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Probe Marker

Page 15
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
User Orientation
•Remember the probe marker correlates with the
symbol on the screen

Page 16
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
User Orientation

Page 17
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
User Orientation
•Objects near the top of the screen correlate with
structures CLOSEST to the probe on the patient
•Objects near the bottom of the screen correlate
with structures furthest away from the probe on the
patient

Page 18
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
User Orientation
Probe
BED

Page 19
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Ultrasound Fundamentals
•D (doppler) mode: Senses the
movement of reflected US waves
toward and away from the probe by
color change or sound
‐Color represents flow toward or away from
probe… NOT arterial vs venous flow
‐(Blue Away Red Toward)

Page 20
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Color Doppler

Page 21
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Procedural
•Static ultrasound
locates structure of
interest but not used to
guide procedure
‐LP
‐Thoracentesis
‐Paracentesis
‐I&D
•Dynamic ultrasound is
used to locate structure
of interest AND allow
direct visualization of
procedure in real time
‐Vascular access

Page 22
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
The Agency for Health Care
Research and Quality (AHRQ)
•Supports the use of ultrasound guidance for the
placement of central venous catheters as a way to
improve success rates, reduce number of attempts
and reduce complications associated with their
placement
(AHRQ) AfHCRaQ. Making Health Care Safer. A Critical Analysis of Patient Safety Practices. July 20, 2001.

Page 23
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Probe Selection
•4-10 MHz frequency
•Linear Array
•Small to medium
footprint

Page 24
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Vessel Selection
Vein Artery
•Thin walled
•Compressible
•May have transmitted
pulsations from
nearby arteries
•Non compressible
•Pulsating

Page 25
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Vessel Selection
•Must be able to differentiate arteries from
veins
‐Compression (veins more compressible)
‐Distal Augmentation
‐Color flow (look for pulsations)

Page 26
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Screening Ultrasound
•Before preparing to cannulate a vessel you should
‐Screen the area of interest for a target
‐Evaluate the vessel size
‐Evaluate vessel compressibility

Page 27
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
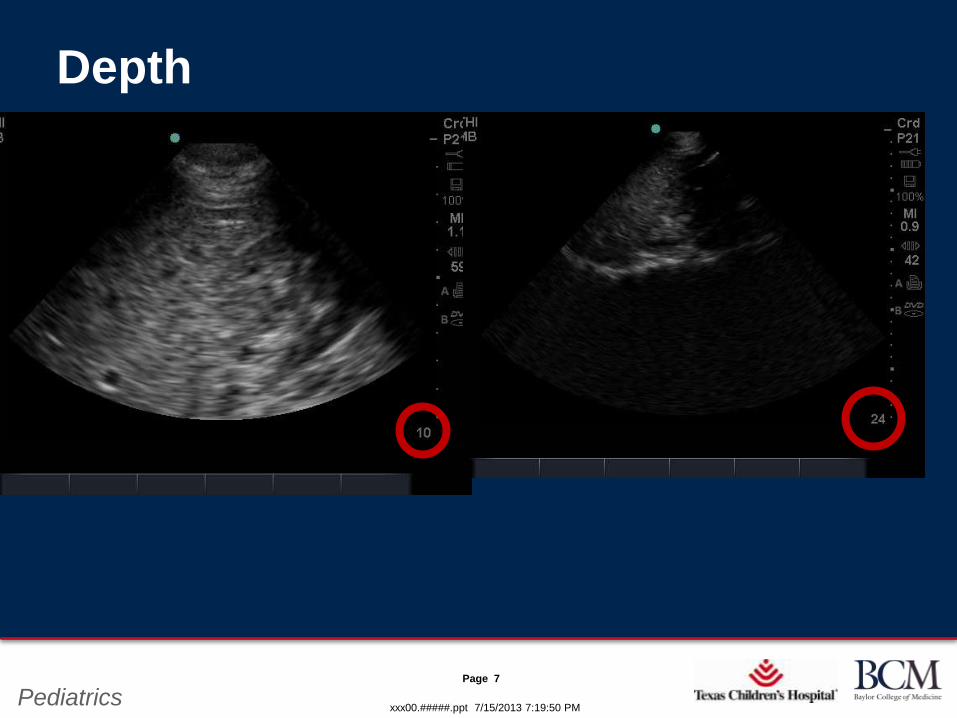
Screening Ultrasound
•Before preparing to cannulate a vessel you should
‐Ensure you are targeting the correct vessel
‐Measure the depth
Page 28
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Compression
IJ IJCA
CA

Page 29
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Distal Augmentation

Page 30
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Transverse Approach to Vessel

Page 31
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Transverse Approach
•With a transverse approach to vessel puncture you
should orient the probe with the marker to YOUR
left and the US screen in FRONT of you
‐This allows for easy manipulation
‐ If on the screen the needle looks like it is to the right of the
vessel then you change direction more to the left

Page 32
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Transverse Approach
•Locate target vessel in transverse plane
•Pucture skin adjacent to probe, locate needle
tip and follow it until it enters vessel
‐This requires you to move the probe as you advance the
needle (following the needle tip)

Page 33
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Transverse Approach

Page 34
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Transverse Approach

Page 35
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Transverse Approach
•Able to visualize surrounding structures
•Have to locate needle tip through motion or comet
artifact

Page 36
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Longitudinal Approach to Vessel

Page 37
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Longitudinal Approach
•Locate target vessel in transverse approach
•Turn probe longitudinal over selected vessel (probe
marker to patients head)
•Puncture skin adjacent to probe
•Advance needle DO NOT move probe
•Keep vessel in screen

Page 38
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Longitudinal Approach

Page 39
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Longitudinal Approach

Page 40
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Internal Jugular

Page 41
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Internal Jugular
•Position the ultrasound screen in front of you
•Orient the ultrasound probe with marker to YOUR
left
‐This allows you to move the probe in the SAME direction as
visualized on the screen

Page 42
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Internal Jugular Central Line
carotid

Page 43
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Valsalva

Page 44
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Internal Jugular Central Line
•US guided central line placement still with
complications (fewer than landmark technique)
‐Puncture of posterior wall of vein
‐Cannulation of carotid artery

Page 45
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Femoral Vein
•Complete overlap of femoral artery over
vein 4 cm below inguinal ligament about
half of the time
•At least 50% overlap of femoral artery
over vein in same location
Hughes, et al. Brit J Anes. Ultrasonography of the femoral vessel in the groin: implicationsfor vascular access. 2000:84(5):668-669

Page 46
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Femoral Vein

Page 47
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Femoral Vein
•Position the ultrasound screen in front of you
•Orient the ultrasound probe with marker to YOUR
left
‐This allows you to move the probe in the SAME direction as
visualized on the screen

Page 48
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Femoral Vein
•Single operator:
‐Hold probe with hand on outside of leg
•Left hand right leg
•Right hand left leg
‐Use free hand to access vein using Seldinger technique

Page 49
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Femoral Vein
•Locate target vessel in transverse plane
•Measure depth of vessel
•Puncture skin at a ~ 30° angle (too sharp will inhibit
passing of guidewire)

Page 50
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Sonosite M-Turbo Series

Page 51
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Remember
•ALWAYS
‐ find potential puncture sight using landmark technique before
evaluating with US
•If time allows
‐Screen BOTH sides to determine the best site for needle
puncture

Page 52
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics

Page 53
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Select your probe

Page 54
xxx00.#####.ppt 7/15/2013 7:19:50 PMPediatrics
Thank You