Embed Size (px)
Citation preview

Julia Lawrence RRT-NPS

By the end of this workshop, the learner will be able to compare and contrast the various types of oxygen delivery devices according to flow requirements and fractional inspired oxygen delivered
By the end of this workshop, the learner will be able to discuss and determine which oxygen delivery device(s) would be most appropriate given case-based examples

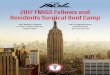
High-flow Venti-masks (air entrainment masks) Mechanical aerosol systems Non-rebreathing masks High flow nasal cannula
Low-flow Nasal cannula Simple masks Partial rebreathing masks

oxygen
room air
exhaled gas

O2 Flow rate FiO2 O2 Flow rate FiO2 O2 Flow rate FiO2
Nasal cannula Oxygen mask Mask with reservoir1 0.24 5-6 0.4 6 0.62 0.28 6-7 0.5 7 0.73 0.32 7-8 0.6 8 0.84 0.36 9 0.80+5 0.4 10 0.80+6 0.44

• Nasal Cannula• Heated high flow Nasal Cannula• Simple Face mask• Venturi mask• Non rebreather mask

Nasal Cannula up to 4 lpm (adults 6 lpm) Approximately 24-45% Fio2

Uses Optimal heated humidified O2 Higher flow which causes a “splinting”
effect to the airways Reduces WOB Flow rates exceed patients inspiratory flow rates

Patient size Color of Cannula
Flow rate Size of outer diameter cannula
< 1400 gm Red 6L/Min 2.4
>1400 gm Yellow 6 L/min 2.4
Infant Violet 7 L/min 2.7
Infant Intermediate
Blue 7 L/min 2.7
Pediatric Green 8 L/min 3.7
Sizes of Nasal CannulaSizes of Nasal Cannula

Infant/ Pediatric cannula up to 8 lpm
Adult Cannula 10 to 60 lpm

The following criteria are for patients being admitted to the acute care floors.
< 4 CRS (Clinical Respiratory Score) < 40% FiO2 > 4kg > 4 weeks


Flow Rates 6-10 lpm Approximately 35%-55%

Allow for a set O2 concentration Entrain Room Air Liter flow depends on Set Fio2 Can deliver up to 100%


Has a one way valve Can deliver close to 100% Fio2 Liter flow enough to keep the bag inflated



Weaning Highflow Nasal Cannula on Acute Care
Is patient on pediatric or adult circuit?
Pediatric Adult
Wean FiO2 to keep saturation > pre set saturation limit
Once FiO2 is decreased to 40% begin to wean liter flow
(Note: In CVICU wean according to MDs order to maintain saturation, may be to 21%)
If CRS is <4 wean flow by at least 1 lpm every 4 hours to a minimum of 4LPM
When at a flow of 4 lpm then transition to a bubble humidifier.
Wean FiO2 to keep saturation > pre set saturation limit
Once FiO2 is decreased to 40% begin to wean liter flow
(Note: In CVICU wean according to MDs order to maintain saturation, may be to 21%)
If CRS is < 4 wean flow by 5 lpm until you reach an end point of 10 lpm (Circuit RT 202 has a low flow limit of 10 lpm)
Once at 10 liters transition to another Oxygen delivery device.
Pre-determined Sat limit
Asthma > 92%Pneumonia > 90%Bronchiolitis > 90%Sickle Cell > 94%All others > 92%

Weaning patients on HFNC in Special Care Areas
Patient started on High flow(Document Clinical Respiratory
Score)
Has CRS decreased by 1 within 60 mins of initiation?
YES NO
Continue to support the patient.
Assess patient Q1-2 h and Document CRS
Increase Flow to decrease WOB
Notify Practioner if CRS increases by > 2 from initiation of HFNC
Assess patient Q1-2 h and document CRS
Wean if patient meets criteria.
Wean Fio2 to 40%, Keeping Sats greater than pre-determined level
Begin weaning flow every hour if CRS < 4
Once the patient is tolerating < 4 LPM change to regular Nasal cannula
Criteria for weaning HFNC
Sats above pre-determine sat limit
CRS < 4


Intervention Why Liter flow

14 y/o male with end-stage CF and recent sinus surgery is admitted to your service. His blood gas is as followed pH 7.35 Pco2 60 Pao2 85, HCO3 26
Vital signs O2 sat 88%, RR 30 HR 95 BP 130/90
What would you do?

16 year old soccer player is admitted to the ICU, following an acute onset of SOB after a coughing spell. His recent chest x-ray shows a moderate right sided pneumothorax. Pt is hemodynamically stable.
What would you recommend?

A 6 month old RSV+ is admitted to the ICU with increase WOB. His vital signs are as followed
HR 180 RR 80 Sat 90 What would you recommend?