Embed Size (px)
Citation preview

Rupert WL LeongDirector of EndoscopySenior Staff Specialist GastroenterologistConcord & Bankstown HospitalsConjoint Associate Professor UNSW
AIBDA SymposiumAIBDA Symposium
Colorectal Cancer SurveillanceColorectal Cancer SurveillanceWhat should we be doing? What should we be doing?
New endoscopy New endoscopy techniques and targeted techniques and targeted
biopsies are now the biopsies are now the standard of care standard of care

• standard white light & random biopsies FAIL to identify treatable flat dysplasia
• newer imaging techniques improves yield 3-10X
• newer techniques recommended by guidelines
• newer techniques are already utilized locally & overseas

Definitions• “new”
– chromoendoscopy (1977+, colitis 2003+) – high definition, zoom endoscopy (2003+)– NBI (2006+)– + targeted biopsies
• “old”– 4 quadrant biopsies every 10cm
PLUS biopsies of any lesions

– 2000cm2 colon SA vs 1.32cm2 random SA33 random biopsies sample <0.1% of the bowel

Why newer endoscopic techniques are required?
• Surveillance colonoscopy in IBD– >33 random colonic biopsies
– interval colorectal cancers (white light)
– 2% of gastroenterologists take >20 biopsies
– >33 biopsies samples only a v small part of the colon
Eaden et al. GI Endosc 2000
Connell et al. Gastroenterol 1994
Rubin et al. Gastroenterol 19921992
Kandiel et al. Visible Human J Endosc. 2008

What is being done? Australia
• online survey– 57%57% use NBI or chromoendoscopy
• others HD, zoom scopes
– 37% perform recommended biopsies
• expert opinion promotes CEFok I, et al. J Gastroenterol Hepatol 2010 (Abst)
Majority of GE already use
newer endoscopic techniques
Efthymiou, Taylor, Kamm, et al. Inflamm Bowel Dis. 2011

What is Being Done? Overseas
• Academic Medical Centre, Amsterdam: – Profs Paul Fockens, Evelien Dekker
•7
Centres of excellence use
newer techniques

Why newer endoscopic techniques are required?
Sporadic Cancer
Normal Colon
Aberrant crypt foci Adenoma Carcinoma
Normal Colon Inflammation
FlatDysplasia
Carcinoma
IBD Cancer
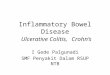
How newer techniques identify flat dysplasia?
• improved resolution, magnification– increases sensitivity, delineates extent
• differential light or dye interaction– improve the yield of dysplasia
Tada et al. Endosc. 1977;8:70–74.

Chromoendoscopy
Is chromoendoscopy difficult? No
• reusable catheter • 2 vials
1. methylene blue 0.1% absorptive (vital)2. indigo carmine 0.1-0.5% topography
1ml dye + 9ml N Saline
Is it difficult? No
– don’t need to learn Kudo classification– don’t need to describe pit pattern
• most evidence at present remains chromoendoscopy
• NBI: vascular network, lesion-mucosa interface

• CE is not required IFIF there is already visible cancer; which is TOO LATE!
• how did it get there?
poor surveillance technique!

• HGD – no invasion– no LN metastasis

Does it work? Yes

Which technique has a higher yield of dysplasia?
• New

• CE in predicting neoplasia: sensitivity 97%; specificity 93%• duration CE = 44 minutes, conventional 35 minutes (ns)
CE in UC Surveillance
• Methylene-blue magnifying CE in UC ≥ 8yr
Kiesslich et al. Gastroenterol 2003
Conventional (n = 81)
Chromoendoscopy(n = 84)
P
Intra-epithelial neoplasias - low grade- high grade
82
248 <0.005
Cancer 1 3 (2 A’s, 1 B) ns
Flat mucosa IN 4 (on random Bx) 24 <0.001

CE in UC Surveillance
• back-to-back conventional colonoscopy vs indigo carmine 0.1% CE
• n=100; 46 neoplastic lesions in 19 patients
Rutter et al. Gut 2004
Conventional (n = 100)
CE(n = 100)
P
Dysplasia:- non-targeted- pre-dye target- dye targeted
- 0/ 2,904 biopsies- 2/ 43 (15-20mm)
- *+7/ 114 (2-6mm)
0.020.06
*
Duration (median) 11min 10min ns

CE in UC Surveillance
• High magnification CE (indigo carmine 0.5%) vs conventional colonoscopy
• n=738; UC ≥ 8 years
Hurlstone et al. Endoscopy 2005
Conventional (n = 350)
High Mag-CE(n = 350)
P
Intra-epith neoplasia- non-targeted- targeted
24- 38/12,482 (0.14%)
- 3/369 (1.6%)
69- 20/12,850 (0.16%)
- 49/644 (8%)
<0.0001
Cancer 1 3 ns
Duration (median) 13min 24min <0.02

CE in Colitis Surveillance
• CE (methylene blue 0.01%) vs WLE • n=102; UC or Crohns colitis
Marion et al. Am J Gastroienterol 2008
Conventional (n = 102)
CE(n = 102)
P
Dysplasia- non-targeted- targeted
3/3264 Bx LGD12/50 LGD1/50 HGD
16/82 LGD1/82 HGD
0.001
Duration (median) 15min 22min ns
0.09%
20.7%

Dysplasia Yield
ConventionalConventional ChromoendoscopyChromoendoscopy PP
Kiesslich
Gastro. 2003 (n = 163)
3X <0.005
35min 44min ns
Rutter
Gut 2004
(n = 100)
3.5X 0.02
11min 10min ns
Hurlstone Endos. 2005
(n = 350)
10X <0.0001
13min 24min
Marion
AJG 2008
(n = 102)
230X <0.0002
15min 22min

NBI vs CE UC Surveillance
• high-res NBI vs high-res CE • n=60; randomised cross-over; colitis >8yr
• BOTH: newer techniques – equivalent
Pellise M, et al. Gastrointest Endosc 2011
NBI(n = 33/27)
CE(n = 27/33)
P
Per-Pt true pos 11/16 12/16 0.727
Withdrawal time 15.7 26.9 <0.01
• 466 surveillance colonoscopies (167 pt) • 11,772 biopsies
van den Broek Am J Gastroenterol 2011
• 1 LGD = positive on random biopsies (all others were targeted biopsies)

Is it recommended? • CCFA: endorses the incorporation of
chromoendoscopy into surveillance colonoscopy… Itzkowitz, Present. Inflamm Bowel Dis 2005
BSG 2011
chromoendoscopy should be the default technique

Does it matter?
• long term outcomes chronic colitis in Australia
• life-time colon cancer risk: 35%
Selinger et al. J Gastroenterol Hepatol. 2011(abst)

New Endoscopic Techniques
• cheap & easy • effective in finding more EARLY dysplasia • acceptable to doctors/ nurses/
pathologists• already performed & recommended
vs random biopsies• slow • difficult for doctors/ nurses/ pathologists • ineffective in finding dysplasia

• IBD Colorectal Cancer Surveillance: What should we be doing?
• purpose of surveillance: find treatable lesions not to miss them
• we should use newer endoscopy techniques

Rupert WL LeongDirector of EndoscopySenior Staff Specialist GastroenterologistConcord & Bankstown HospitalsConjoint Associate Professor UNSW
AIBDA SymposiumAIBDA Symposium
Colorectal Cancer SurveillanceColorectal Cancer SurveillanceWhat should we be doing? What should we be doing?
New endoscopy New endoscopy techniques and targeted techniques and targeted
biopsies are now the biopsies are now the standard of care standard of care

• IBD Colorectal Cancer Surveillance: What should we be doing?
• 10cm 4 quadrant biopsies –negligible yield, samples only 0.01% of colon, expensive pathology, unpopular in Australia
• purpose of surveillance: find early lesions not to miss them

Is it messy?
• A little bit
• But far fewer histology bottles!

Costs
• chromoendoscopy = cheap
• all new video endoscopes = higher resolutions
• large-screen monitors

Is it difficult? No
Strict patient selection: colitis; remission/ steroids
Unmask: bowel prep, wash, insufflation Reduce peristalsis: buscopan, glucagon
Full segmental stainAdd dyeCrypt/ surface irregularities Endoscopic targeted biopsies
Kiesslich et al. Gastroenterol 2003

Procedure/ Withdrawal Times
ConventionalConventional ChromoendoscopyChromoendoscopy PP
Kiesslich
Gastro. 2003 (n = 163)
3X <0.005
35min 44min ns
Rutter
Gut 2004
(n = 100)
3.5X 0.02
11min 10min ns
Hurlstone Endos. 2005
(n = 350)
10X <0.0001
13min 24min
Marion
AJG 2008
(n = 102)
230X <0.0002
15min 22min

Time Saving
• reduced numbers of normal and futile random biopsies
• pathology cost savings
• proper surveillance – may increase repeat colonoscopy interval time (to be validated)

What about training & safety?
• no accreditation recommendations• dyes are safe
– methylene blue: good experience – indigo carmine: inert
• can still perform random biopsies– document disease activity

New Endoscopic Techniques
• cheap & easy • effective in finding more EARLY dysplasia • acceptable to doctors/ nurses/
pathologists• already performed & recommended
vs random biopsies• slow • difficult for doctors/ nurses/ pathologists • ineffective in finding dysplasia