Embed Size (px)
Citation preview




Healthcare Industry: India Overview
Market value forecast : In 2016, the Indian
healthcare providers sector is forecast to have
a value of $167.3 billion, an increase of
104.8% since 2011. 300
Size of the health sector
Graph1: Expected to create 40 million new jobs by 2020
Category segmentation : Inpatient Care is the
largest segment of the healthcare providers
sector in India, accounting for 31.5% of the
sector's total value.
239250
300
Geography segmentation : India accounts for
7.1% of the Asia‐Pacific healthcare providers
sector value.
T t l l b l h lth dit t
150
200
D billion
Total global healthcare expenditure represent
around 10% of world GDP
India’s medical device market is currently the
4th largest in Asia with 700 medical device 65
100
50
100
US
makers, and ranks among the top 20 in the
world
0
50
2011 2015 (e) 2020 (e)
Sources: Rating agency Fitch. Department of Industrial Policy & Promotion (DIPP)
Healthcare Industry: Key Drivers of growth
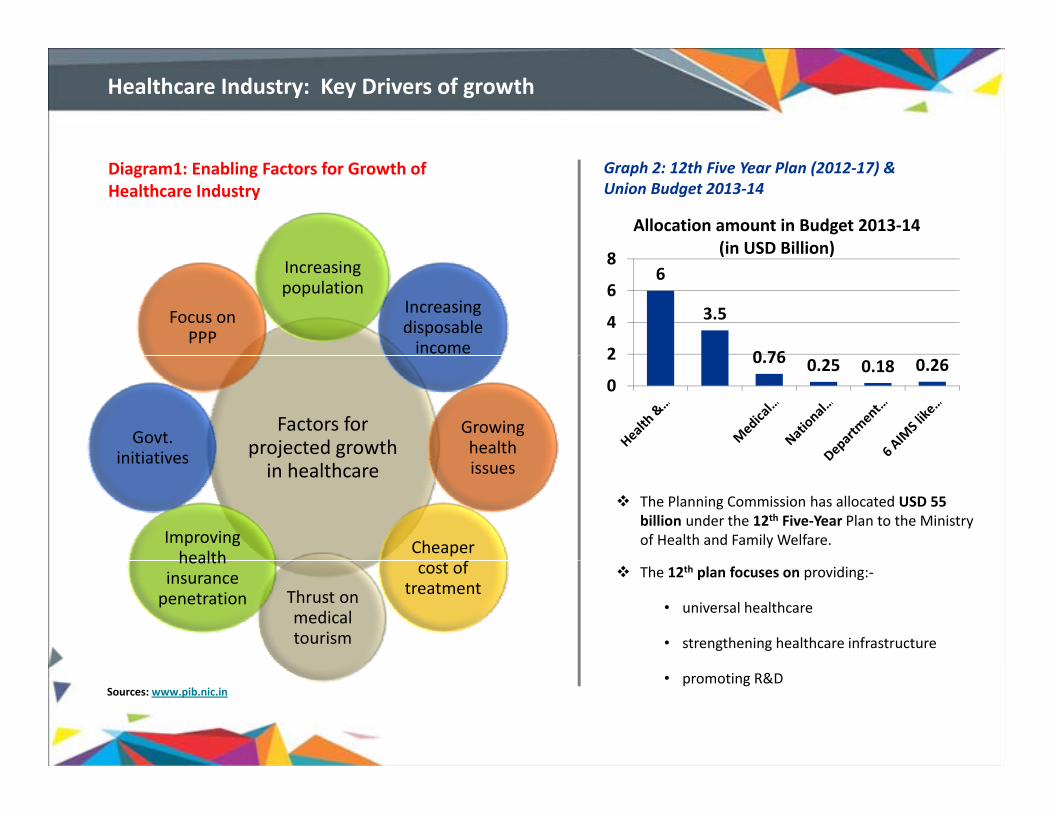
Diagram1: Enabling Factors for Growth of Healthcare Industry
8
Allocation amount in Budget 2013‐14 (in USD Billion)
Graph 2: 12th Five Year Plan (2012‐17) &Union Budget 2013‐14
Increasing population
Increasing disposable income
Focus on PPP
6
3.5
0 762
4
6
8 (in USD Billion)
Factors for projected growth
Growing health Govt.
initiatives
0.76 0.25 0.18 0.260
2
in healthcare issues
Cheaper Improving health
initiatives
The Planning Commission has allocated USD 55 billion under the 12th Five‐Year Plan to the Ministry of Health and Family Welfare.
cost of treatmentThrust on
medical tourism
health insurance penetration
The 12th plan focuses on providing:‐
• universal healthcare
• strengthening healthcare infrastructure
Sources: www.pib.nic.in• promoting R&D

Supportive Policies Drive FDI Inflows Health Insurance
Healthcare Industry: Key Drivers of growth
Supportive Policies Drive FDI Inflows
100% FDI is permitted for all health‐related
services under the automatic route
Demand growth cost advantages and policy
The health insurance premium has registered a compounded
annual growth rate (CAGR) of 32 % for the past 8 financial years.
The Indian insurance industry with gross premiums for health
Health Insurance
Demand growth, cost advantages and policy
support have been instrumental in attracting
FDI
During April 2000 – March 2013, FDI inflows for
drugs and pharmaceuticals stood at USD 10 3
insurance increased by 16 % from USD 2.12 Billion in 2011‐12
to USD 2.46 Billion in 2012‐13.
drugs and pharmaceuticals stood at USD 10.3
billion
Inflows into hospitals and diagnostic centers,
and medical appliances stood at USD 1.6 billion
d USD 0 6 billion ti l d i th 21212463
25003000
Graph 3: Health Insurance Premium in India (USD Million)
and USD 0.6 billion, respectively, during the
same period.
In the present scenario the health insurance
10601332
18462121
5001000150020002500
In the present scenario, the health insurance
industry is dominated by four public sector entities
that together have 60 per cent market share which
are as follows:‐ National New India
Oriental United India
0
FY09 FY10 FY11 FY12 FY13
Sources: Department of Industrial Policy & Promotion (DIPP) New India United India

Healthcare Industry: Strong Policy Support
Encouraging the private sector
The benefit of section 10 (23 G) of the IT Act has been extended to financial institutions that provide long‐term capital to hospitals with 100 beds or more
Government is encouraging the PPP model to improve availability of healthcare services and provide healthcare financing
Encouraging investments in
The benefit of section 80‐IB has been extended to new hospitals with 100 beds or more that are set up in rural areas; such hospitals are entitled to 100% deduction on profits for 5 years
rural areas
Customs duty on life‐saving equipment has been reduced to 5% from 25% and exempted from countervailing duty
Tax incentives countervailing duty
Import duty on medical equipment has been reduced to 7.5%
Incentives and tax holidays are being offered to hospitals and dispensaries providing health travelIncentives in the medical travel industry
Incentives and tax holidays are being offered to hospitals and dispensaries providing health travel facilities

Healthcare Industry: Opportunities
Additional 1.8 million beds needed for India to achieve the target of 2 beds per 1,000 people by 2025
Additional 1.54 million doctors required to meet the growing demand for healthcare
Investment of USD 86 billion required to achieve these targets
Healthcare Infrastructure
Contract research is a fast growing segment in the Indian healthcare industry
Cost of developing new drug is as low as 60% of the testing cost in the US
About 60% of global clinical trials is outsourced to developing countries Research
Indian medical tourism industry is expected to register a CAGR of more than 20% during 2013‐2015
Cost of surgery in India is nearly (1/10)th of the cost in developed countries MedicalTourism
Less than 15% of the Indian population is covered through health insurance
Health insurance premiums are expected to increase at a CAGR of 30% during 2012–14 HealthInsurance
Sources: From research report “Booming Medical Tourism in India”


Gujarat Healthcare Industry: Overview
Gujarat state is in the forefront of establishing and maintaining good health infrastructure at various levels.During the year 2011‐12, 31 Million patients were treated in the outdoor while 4 Million patients were treatedas indoor patients
The state's healthcare sector is witnessing an exponential growth, as evidenced by the
• growing number of
hospitals and healthcare
institutes,
• improving emergencyimproving emergency
medical services with the
help of 108 ambulance
services,
• increasing medical tourism,increasing medical tourism,
• successful public private
partnership (PPP) models
• better medical education.

Gujarat Healthcare Value Chain Analysis
Business Objectives Expected Changes Business Opportunities
Patient
• Quality searvices• Value for money• Minimum co‐pay
• Changing Diseases Pattern
• Changing socio‐economic profile
• Health Insurance• Medical Tourism
Hospital
• Minimization of the cost• Wealth maximization• Increase value perP i
economic profile• Changing life‐style
pattern• Demand for quality
healthcare• Corporatization of
• Medical Tourism• Preventive • healthcare• Healthcare BPO• Telemedicine• Laboratory and • Patient
• Operational efficiency
• Wealth maximization
Co po at at o oIndian healthcare
• Increasing penetration of private healthinsurance
• Foreign alliances
abo ato y a d• diagnostic services• Medical devices• Health IT• Consulting
InsuranceWealth maximization
• Minimum Annual payout
• Information technologyin healthcare

Gujarat Healthcare: Strong Infrastructure and Resources
Capacity building Nursing services Efficient manpower Hospital management
Research Ayurveda Homeopathy Medical Education
Support services Hotels Boarding and lodging facilities Catering
Clinical State‐Of‐Art Hospitals Blood Banks Diagnostics‐MRIs, CT Scans
Available Infrastructure
Public health Bio ‐medical engineering Physiotherapists X ray technicians
Holistic wellbeing Yoga Siddha Meditation X ‐ ray technicians Meditation
Sources: Industry Analysis


The main objective of Medical Education is to train and develop adequate manpower personnel in Medicine,
Gujarat ‐ Objective
Dental, Physiotherapy and Nursing fields
Moreover, to provide tertiary health care delivery to the needy patients in the state, free of cost to BPL patientsand at affordable rates to all.

Medical and Para Medical Colleges
Total of 19 Institutions with 2930 Seats
■ 6 Government Colleges (1080 Seats)
Total of 13 Institutions with 1240 Seats
■ 6 Government Colleges (1080 Seats)
■ 12 Private Colleges (1700 Seats)
■ 1 Deemed University (150 Seats)
■ 2 Government Colleges (200 Seats)
■ 11 Private Colleges (1040 Seats)
Total of 38 Institutions with 1715 Seats
■ 8 Government Colleges (390 Seats)
Total of 27 Institutions with 1490 Seats
■ 5 Government Colleges (360 Seats)■ 8 Government Colleges (390 Seats)
■ 30 Private Colleges (1325 Seats)■ 21 Private Colleges (1100 Seats)
■ 1 Deemed University (30 Seats)

Medical and Para Medical Colleges
Total of 16 Institutions with 1525 Seats
■ 4 Grant‐in‐Aid Colleges (400 Seats)
■ 12 Self Financed Colleges (1125 Seats)
4 S lf Fi d I tit ti
Total of 10 Institutions with 430 Seats
■ 4 Government Colleges (180 Seats)
4 Self Financed Institutions
with a total of 100 Seats■ 3 Grant‐in‐Aid Colleges
(100 Seats)
■ 3 Self Financed Colleges (150 Seats)
■ 1 Deemed University■ 1 Deemed University
1 Self Financed College with a total of 25 Seats
1 Government College with a total of 10 Seats

Grant‐in‐Aid Specialty Institutions in Gujarat
The Gujarat Cancer and Research Institute, Ahmedabad
Bed Strength: 650
U.N. Mehta Institute of Cardiology and Research, Ahmedabad
Bed Strength: 450
Institute of Kidney Diseases and Research, Ahmedabad
Bed Strength: 450
Proposed Speciality Institutions
1. Saurashtra Cancer and Research Institute, Rajkot
2. Kidney Institute, Surat
3. Stem Cell Institute, Surat

Future Growth Strategy
Additional threeIncreasing intakes in Medical Colleges
Additional three medical colleges coming up
at Vidyanagar, Junagadhand Himmatnagar
Master Planning for development of six government Hospital
Upcoming Paramedical
Future Growth Strategy
Four Tertiary Cancer
g pCampuses at Ahmedabad, Vadodara, Rajkot, Bhavnagar, Jamnagar, Surat
Paramedical
Institute
Four Tertiary Cancer Care Centres at
Rajkot, Bhavnagar, Jamnagar and Vadodara


Medical Services: Vision
To be the network of finest public healthcare institutions in the state of Gujarat, providing quality medicali ith th t t f t t h l ith ibilit ff d bilit & it t th l fcare services with the state of art technology with easy accessibility, affordability & equity to the people of
Gujarat & beyond


Medical services are meant for curative care via diagnosis and treatment. Medical Relief services mainly are centered in theurban areas of the state and are delivered through the following hospitals which are the leading hospitals at the district and
State Infrastructure
urban areas of the state and are delivered through the following hospitals, which are the leading hospitals at the district andsub‐district level for all the districts
Government Hospitals & No. of sanctioned beds
24 General DistrictHospitals3381 Beds
30 GovernmentSub‐ DistrictHospitals2828 Beds
1 InfectiousDiseasesHospital50 Beds
4 MentalHealth
Hospitals683 Beds
2 Eye DiseaseHospitals
120 Beds
1 GovernmentClass II Hospital & 2 special dispensaries
119 Grant‐in‐AidInstitutions
5129 Beds3381 Beds 2828 Beds 50 Beds 683 Beds 120 Beds dispensaries 27 Beds
5129 Beds
Chief Minister Services of Experts at Treatment Unit (CM‐SETU) for engaging specialist doctors to provide services of privateexpert in Government Hospitals. The Doctor serve in Govt. Hospitals and the cost of patient’s treatment borne by state
O l i f INR 600 h id b h f i li d i G H i lgovernment. On emulation of INR 600 per hour paid to combat severe shortage of specialist doctors in Government Hospitals.

Future Growth Strategy
• New Hospital for Mental Health will be started at Mahesana, Bhavnagar & Surat to strengthen Mental Health Programme in the State
• New Nursing School will be started to meet the growing demand of qualified nursing personnel
New Institutions
• Gujarat 108 Emergency ambulance services are being strengthened to be utilized critical hours of the treatment
• Infrastructure facility of district hospital, sub district hospital, Hospital for mental health, eye hospital & Infectious diseases hospital will be Up gradated to provide better secondary health care services
• Physical Medicine and Rehabilitation Center (PMRC) & DEIC of various hospitals will be strengthen gradually to rehabilitee disable person in the society.
Infrastructure Upgradation
• Quality assurances Programme is being implemented gradually in district & sub district hospitals to improve Health care services
Quality Assurance and
h l • Facility of Tele Radiology will be created to provide guidance regarding Diagnosis & Treatment in the interior part of the state
Technology Upgradation

Public Private Partnership (PPP) Opportunities
S
Upgrade IT Services for Healthcare
Tele‐medicine
Super‐Specialties in Cardiology, Neurology,
Ortho, Eye and Kidney Setting up of
Diagnostic services
Healthcare
and Tele‐radiology projects
Kidney
Healthcare Infrastructure
Setting up of Super specialty
hospitals
Rehabilitation Center
Non‐Emergency Ambulance transport service PPP for
Healthcare
Hospital supplies
Reform Strategy – Institutional
Healthcare facilities in
Rural Areas of State
Management, Collaboration
with the private sector (PPP)


National Leprosy Eradication Programme (NLEP)
National Leprosy Control Programme (NLCP) inGujarat was started from 1955.
With the advent of MDT (Multi DrugTreatment) this national programme was re‐designated as the National LeprosyEradication Programme (NLEP) in the year1983.
In 1983 MDT was introduced in a phasedmanner and the whole Gujarat state wascovered by MDT in the year 1991.

To reduce the prevalence rate of blindness up to 0.3 Optimal utilization of available resources through
National Programme for Control of Blindness
Goals & Objectives
by the year 2020
Elimination of cataract backlog from Gujarat state
Provide comprehensive eye care for emerging causes of blindness
public private partnership
To improve the technical skill of professionals in the government set up.
To establish uniform Infection Control policy at all levels of eye care service delivery
Goals & Objectives
Regional Institute of Ophthalmology (RIO)‐ 1
Tertiary Eye Care Centers (Medical Colleges)‐19
Secondary Eye Care Centers (Govt. + NGO Base Hospitals) ‐285
Primary Level Vision Centers – 98
Progress In Last Decade
Cataract Surgeries: 450000 to 780000
Cataract Surgical Rate (C.S.R.)/1 LAKH Population : 863 to 1292
Spectacle Distribution (SES): 10000 to 185000
Eye Donation : 4440 to 8200
Intra Ocular Lenses: Non foldable to Hydrophobic Intraocular Lens
Cataract centric
Intra Ocular Lens (IOL) Surgeries (2013‐14) : 775458
Newer Initiatives –
Budget proposed under State Plan 2014 – 15 for INR 12 Million
Special provisions like high quality hydrophobic
Regional Institute of Ophthalmology is providing extensive community level services through Mobile Van
Diabetic Retinopathy
Intraocular lenses with accessory drugs are made available by Government
All treatment are provided free of cost including transportation of the children & parents
Immense priority is being given to reduce the blindness due to diabetic retinopathy
To intensify and accelerate present prevention of blindness activities so as to achieve the goal of eliminating avoidable blindness by the year 2020

Revised National TB Control Programme (RNTCP)

Revised National TB Control Programme (RNTCP)
Expenditure trend is over 90% of approved budget consistently in last
Proportion of TB patients tested for HIV is consistently more than 90% since 3 years
Proportion of HIV infected TB patients on 5 years CPT/ART is 95% in 4Q 2013
Si h i i f C
Performance of RNTCP
Gujarat State is ranked 1st at National level based on comprehensive composite indicators formed by Central TB Division,
Gujarat screened highest no of MDR TB suspects in 2013 in the country (24984)
1652 MDR TB patients put on treatment in 2013
Since the inception of RNTCP up to March 2013 Total TB suspect Examined:
48,06,720 Total TB Patients put on
DOTS y ,Government of India Total 4999 MDR TB patients put
on treatment till datetreatment: 1,01,6381
New Smear Positive patients put on treatment : 4,34,557
Additional lives saved: 1,82,949
Gujarat is first state along with Kerala to implement TB‐Diabetes collaborative activities.70% of TB patients are screened for diabetes

National Vector Borne Disease Control Programme
Achievements
Surveillance for malaria intensified
by achieving an ABER of 20.4 in 2013
R d i i l i i id
Prevention of outbreaks:
Reduction in malaria incidence:
The Annual Parasitic Incidence
brought down to 0.94 in 2013
from 4.12 in 2004
Rapid Diagnostic Testsfor early diagnosis of Malaria
Prevention of outbreaks:
No major outbreak was reported
in the State from 2004 onwards
Sentinel surveillance for
Dengue and Chikungunya was
National Vector Borne Disease Control
New Initiatives
NS1 diagnostic test Kits available for Early diagnosis of Dengue
e gue a d C u gu ya as
made functional in all the districts
Rapid response mechanism
established for the prevention
and control of these disease
Control ProgrammeDistribution of LLIN
in high risk villages(9.52 lakhs distributed so far)
Successfully implemented the Mass Drug Administration campaign for Elimination of Lymphatic Filariasisin the state by achieving > 85 % coverage

Sickle Cell Anemia Control Program
Crisis Management
• Supportive & Referral Treatment
• Regular follow up and counseling
• Pneumococcal vaccination
20% of Sickle disease children die by the age of two years
>50% of the world Sickle gene carriers in India
30% f i kl di hild th t ib l
Crisis ManagementEarly diagnosis through
Ne Born Screening
30% of sickle disease children among the tribal community die before they reach adulthood
Early Diagnosis
Prevention
New Born Screening Prenatal Diagnosis Antenatal Screening Adolescent Screening Mass Screening on
mission mode
Regular
R l
Prevention through:• Marriage Counseling• Genetic Counseling• Building CommunityTribal Population is the target group
SCA seen in all 12 tribal districts – all covered under Sickle Cell Anemia Control Program
Regular
• Doctors and Paramedical staff
• Health care providers & ASHA
• VHSNC members & Teachers
• Building Community Awareness
Tribal Population is the target group
But any person suffering from Sickle Cell Anemia is main beneficiary
Components of the Program

Rural Health Infrastructure
State Health Facilities Current Status andRequirement as per Current Norms:
4. Target till March 2017 CHC: 358 2017
3. Target till March 2016 CHC: 342 PHC: 1368
CHC: 358 PHC: 1433 SC: 9156
2016
2. Target till March 2015 CHC: 326 PHC: 1303 SC: 8121
PHC: 1368 SC: 8641
2015
SC: 8121
20141. Current Status (Till March 2014) CHC: 300 PHC: 1208 SC: 7674
CHC: Community Health Centre
PHC: Primary Health Centre
SC: Sub Health Centre

Urban Health Program: Core Strategies
Involvement of ULBS1
Strengthening, revamping and rationalizing existing urban primary health structure2
C i f f ili i D l f HR (D ANM ASHA )3 Creation of new facilities, Deployment of HR (Doctors, ANMs, ASHAs)3
Ensuring quality healthcare services (Assured package of service)4
Community Participation: Mahila Arogya Samitis/ other CBOs like SHGs5 Community Participation: Mahila Arogya Samitis/ other CBOs like SHGs5
Capacity building of stakeholders (ULBs, ANMs, ASHAs, community, etc.)6
Prioritizing the most vulnerable among the (urban) poor7 Prioritizing the most vulnerable among the (urban) poor7
Convergence, partnerships (ESI,Profit, not‐for‐profit)8
Use of Information & Communication Technology (ICT) for better service delivery, gy ( ) y
improved surveillance and monitoring9

Urban Health Program: Convergence with other departments
National Disease Control Program
Department of AYUSH
Department of AIDS Control Ministry of Urban Development Department And Housing
Ministry of Urban Poverty Alleviation
Ministry of WCD
Ministry of Water SupplyMinistry of Human Resource Development
Goal: To improve the health status of the urban population in general, but particularly of the poor and other disadvantaged sections
NUHM has been launched under an overarching NHM for providing quality health care services to the urban population (especially urban poor and vulnerable population) with the active involvement of ULB(especially urban poor and vulnerable population) with the active involvement of ULB


Reproductive and Child Health Programs
Reduce Maternal and Child Mortality
Combat Malnutrition with multi pronged strategy
Enabling ICT as a Strategic resource and making it an integral part of Health
Governance
Goals
ProvideProvide state of the
Art Health and Medical Education relevant to local needslocal needs

Family Welfare Programme
Vision of State: Increasing life expectancy and Improving physical quality of life of people
Chiranjivi Yojana
Janani Sishu Suraksha Karyakram: Entitles all pregnant women to access public health institutions free of cost
Received the Asian
Innovations Award in 2006
institutions free of cost
S. No.
Availing facility No. of Beneficiaries(April 2013 – Dec 2013)
1 Free Drugs & Consumables
284,650Consumables
2 Free diet 182,528
3 Free blood 8,447
4 Free diagnostic 252 020
A Scheme initiated by Government of Gujarat, involves private sector specialists for providing safe delivery services, primarily for women from “below‐poverty line” (BPL) households.
4 Free diagnostic services
252,020
Normal Deliveries LSC S‐ Deliveries Complicated Deliveries
Total Deliveries No. of Doctors enrolled
Chiranjeevi Yojana status upto November‐2013:
800,079 58,699 46,329 905,107 388
Sources: Socio‐Economic Review 2012‐13

Gujarat state has initiated 'e‐Mamta', a 'Mother and Child name‐based information management system
e ‐Mamta ( Mother and Child Tracking System)
j , g y
ANC (Ante Natal Care) Registration
'e‐Mamta' is innovative and is intended to harness the
Registration count:‐ ~1.5 Million
benefits of ICT to improve effective and efficient delivery of health care services available.
e ‐Mamta( Mother and Child Tracking
System)
Total Families registered in e‐Mamta ‐ 11 Million Total Members registered in e‐Mamta ‐ 53 Million
Live birth (Child Registration) Count ‐ ~1.15 Million
Sources: Data till March 2014

Bal Sakha Yojna: An initiative under Chiranjeevi Scheme with PPP (Public Private Partnership).
Government Initiatives
Bal Sakha Yojna: An initiative under Chiranjeevi Scheme with PPP (Public Private Partnership).• Provided facilities for proper check up of newborns and infants by paediatricians. • Main aim of the scheme is to bring down the Infant Mortality Rate (IMR) and the Maternal Mortality Rate (MMR).
H l h I di N ifi d S T 2015 T 2017
Reproductive and Child Health Programme (RCH) & Integrated Management of New Born & Childhood Illness (IMNCI)
Health Indicators Notified Status Target 2015 Target 2017
Reduction in MMR 122 (10‐12 SRS) 90 < 80
Reduction in IMR 38 (SRS 2012) 29 24
Total Fertility Rate 2.3 (SRS 2012) 2.2 2.1

Vill H lth d N t iti DMamtaIn year 2012‐13, 0.23 Million pregnant women have been covered
Janani
Maternal Health: Strategies to reduce MMR
Village Health and Nutrition DayMamta
Abhiyaan
Involves private sector specialistsfor providing safe delivery services,primarily for women from “below‐
Chiranjeevi
Yojana
pregnant women have been covered under the scheme
SurakshaYojna (JSY)
Improving access to Safe Abortion services
Safe Abortionprimarily for women from below
poverty line” (BPL) householdsYojana
To ensure institutional deliveries and 48 hours stay
Mamta Kit
And Manta
Ghar
A 'Mother and Child name‐basedinformation management system toimprove effective and efficient deliveryof health care services
e‐Mamta
Medical Officers in ComprehensiveEmergency Obstetric Care, Anesthesia, Skill Birth Attendant Training to AYUSMedical Officers , Nurse Practioners
Capacity
Building
Medical Officers in Comprehensive Emergency Obstetric Care, Anesthesia,Skill Birth Attendant Training to AYUSHMedical Officers , Nurse Practioners
Capacity Building
Birth CompanionMamta
Sakhi
ASHA as motivators & mobilizersfor institutional deliveries and Postnatal visits : 30,000 ASHAs
ASHA
Complete free services duringJanani Shishu
Skill labs are set up in stateSkills Labs
Tie up with 108‐emergency transport And
Khilkhila
Complete free services duringpregnancy, delivery and up to 42 daysafter delivery and care to newborns;infants up to 1 year from 2013‐14
Janani ShishuSurakshaKaryakram(JSSK)
Chief Minister Services ofCM SETUp g y p
and drop‐back (Khilkhilat)Khilkhila‐
hatExperts at Treatment Unit CM‐SETU

Child Health: Strategies to reduce IMR
Facility Based Newborn Care (FBNC)
Bal Sakha Yojana– A PPP initiativeof GOG
Home Based New Born Care (HBNC)
Janani Shishu Suraksha Karyakram (JSSK)of GOG
Navjat Shishu ShurakshaKaryakaram (NSSK)
IMNCI (Integrated Management of Neonatal and Childhood Illnesses)
Vit A and Iron Folic acid supplementation
Diarrhoea Alleviation through ORS and Zinc Treatment (DAZT)
e‐Mamta: Mother and Child Tracking Programme
Mamta Abhiyan
Convergence under Mission Balam Sukham
Improved Tertiary Newborn care Mamta Abhiyan
Kangaroo Mother Care (KMC)Wards
through SNCUs
Bal Sakha Hospital for Newborns

Gujarat Socio Economic Development Society:Creation of Social Enterprise for Healthcare through CSR Funds
SPV will ‘compliment and supplement’ specific healthcare and educational
activities through High Impact
GSEDS will act as a Special Purpose Vehicle (SPV) combined for Health and Education activities through High Impact
Interventions in High Priority Talukas(HPTs) to target MDGs and HDI to
improve Socio‐Economic Status
for Health and Education.
Gujarat Socio Economic Development Society
Operationalize/strengthen PPP models of small hospitals with existing Govt. set‐up/private
Preventive and Curative services for Maternal and Child Health, services as per
RMNCH+A (A life cycle approach) for inclusive healthcareplayers/ NGOs in various High
Priority Talukas`
inclusive healthcareSchools for quality education in all the HPTs
with all the modern facilities.


Provides t ti
Mukhyamantri Amrutam
544 procedures f h
100% Statefunded Scheme
tertiary caretreatment for
catastrophic diseases to BPL families of the State
in any of the Private/ Government Empanelled Hospital
Cashlesshospitalization benefit of
INR 200 000
funded Scheme1
2
More than 2.144 Million BPL families
have been enrolled
Current Status of the Scheme
MukhyamantriAmrutam (MA)
INR 200,000 per BPL Family (5) per annum
Pre‐existing
3
4
25,209 claims amounting to
USD 8.70 Million h d ill
diseases are also covered from
day one
63 Super Speciality Hospitals
4
5
6have occurred till 31st march 2014
p y p(19 Government and 44 Private
Hospitals)Provision for transport allowanceof INR 300 per visit

Rashtriya Swasthya Bima Yojana (RSBY)
Current StatusWorking Objectives
To provide health insurance coverage for Below Poverty
• Every beneficiary family is issued a biometric enabled smart card containing their fingerprints and
Till date 11/04/2014 a total of 1,23,582 claims has
Line (BPL) families
• Beneficiaries under RSBY are entitled to get hospitalization coverage up to INR 30,000/‐ for most of the diseases that require
containing their fingerprints and photographs
• All the hospitals empanelled under RSBY are IT enabled and the IT platform is used for authentication verification and
occured, amounting to USD 10.48 Million
• In the year 2013‐14, the RSBY policy has been extended to Western Railway Porters and
hospitalization
• Government has even fixed the package rates for the hospitals for a large number of interventions (1090 Procedures)
authentication, verification and for creating transactions at the grass root level
• This ensures a smooth data flow regarding service utilization periodically
Western Railway Porters and MGNREGA Workers (worked for at least 15 days in previous year), in addition to the eligible BPL families of Urban & Rural areas and Building & other Construction
• Pre‐existing conditions are covered. Coverage extends to five members of the family. Newborn covered as sixth member
• Beneficiaries need to pay only INR
periodically
• The beneficiary of RSBY gets cashless benefit in any of the empanelled hospitals
• He/ she only need to carry his/
Workers.
• Total enrollment during this year is 1.838 Million (48.34%).
• Around 1,432 hospitals are empanelled under the scheme• Beneficiaries need to pay only INR
30/‐ as registration fee while Central(75%) and State(25%) Government pays the premium to the insurer selected on the basis of a competitive bidding
her smart card and provide verification through his/ her fingerprint
• Health Service Providers send online claims to the insurer and
empanelled under the scheme (957 Private hospitals and 475 Government hospitals) and are increasing day by day.
p gget paid electronically
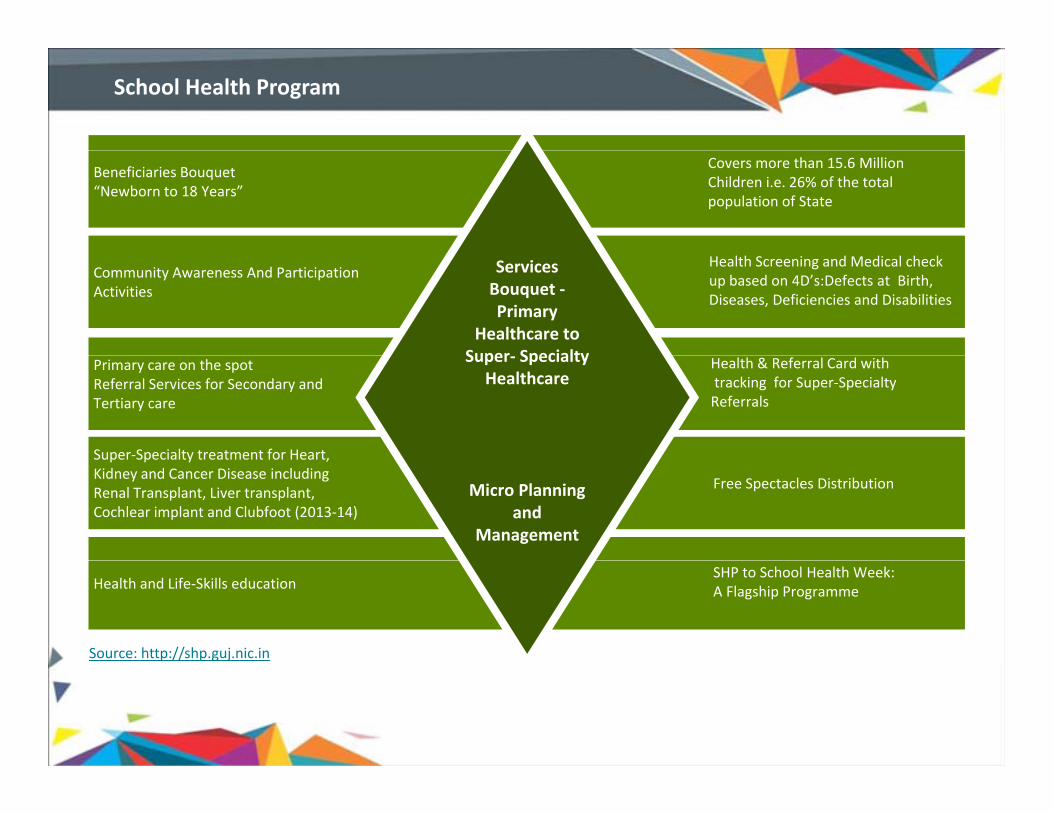
School Health Program
Beneficiaries Bouquet“Newborn to 18 Years”
Covers more than 15.6 Million Children i.e. 26% of the total population of State
Community Awareness And Participation Activities
Services Bouquet ‐Primary
Healthcare to Super Specialty
Health Screening and Medical check up based on 4D’s:Defects at Birth, Diseases, Deficiencies and Disabilities
Super‐Specialty treatment for Heart,
Primary care on the spotReferral Services for Secondary andTertiary care
Super‐ Specialty Healthcare
Health & Referral Card withtracking for Super‐Specialty Referrals
Super Specialty treatment for Heart, Kidney and Cancer Disease including Renal Transplant, Liver transplant, Cochlear implant and Clubfoot (2013‐14)
Micro Planning and
Management
Free Spectacles Distribution
Health and Life‐Skills educationSHP to School Health Week:A Flagship Programme
Source: http://shp.guj.nic.in

School Health Program
Socio‐Economic Impact:• Inclusive child healthcarebased on Social Equity
• All SC and ST children getquality and expensive
Sustainability•Demand generation from the
community due to Awareness,
Acceptance and Participation.
d
Output• Levels of awareness :
1. students in Schools ‐ 99.5%.2. In Madrassa ‐100%
• Level of satisfaction of
Community Awareness And Participation Activities• Cleaning of water sources
(wells & water works)• General cleaning in village
and schoolsquality and expensivetreatment of catastrophicdiseases free of Cost
• Substantial reduction ofhealth burden leading toHealthy Society andProsperous Nation
•Mass support and
Community Ownership
•Political commitment.
•Continuous training, capacity
building & improvisation
Level of satisfaction of the treatment facility ‐ 97.9%
• Parents attended school health program activities ‐ 66.2%
• Schools provided Health educations‐ 98.4%
and schools• Herbal Plantations• Healthy Baby Competitions• Healthy Ante Natal Competitions• Healthy Cooking Competitions• Exhibition on Nutritional
food and nutritive itemsp building & improvisation
based upon experience and
feedback
Health educations 98.4%
• PRI members suggestingcontinuation of the SHP‐ 96.8%
• Widely accessible communication network;
• Easily retrievable health data;
food and nutritive items• Parents Meetings• Dada‐Dadi Meeting• Gram Sanjivani Samiti Meetings
• Easily retrievable health data;
• Thorough micro‐planning for the entire project;
• Designated referral centers for the screened out children
Source: http://shp.guj.nic.in

Ayurveda
Teaching Institutions: Total number of Undergraduate seats in Ayurveda College = 430
Post –Graduation = 3Govt = 2
Ph. D. = 1Govt = 1
AyurvedaPharmacy = 1
Nursing = 2Govt = 2
Graduation = 9Govt = 4 Govt. 2
Self‐finance = 1Govt. 1 Pharmacy 1
Self‐finance = 1Govt. 2Govt. 4
GIA = 2Self‐finance= 3
N G t T hi i tit tNew Government Teaching institute
Government is planning to start a new Government homoeopathy Medical college at Dethali, Ta. Sidhdhapur, DI. Patan
Clinical NetworkHospital cum College = 4
Hospitals = 29Dispensaries = 545
The implementation of the Model Ayurveda College at Kolavada is in progress.
Mobile Dispensaries = 12
New Government Ayurveda College to start at Rajpipla, and Dahod and a new Government Homoeopathy College at Vansada

Admission Capacity
Homeopathy
S. No. Grant‐In‐Aid CollegesAdmission Capacity
U. G. P. G.
1 Gujarat Homeopathy Medical College, Savli, Vadodara 100 00
2 Srimati A. J. Savla Homeopathy Medical College, Mahesana 100 002 Srimati A. J. Savla Homeopathy Medical College, Mahesana 100 00
3 Dr. V. H. Dace Homeopathy Medical College, Anand 100 09
4 Anand Homeopathy Medical College & Research institute, Anand 100 18
There are 12 Self Financed Colleges also with 1125 Seats
Self‐financed naturopathy & Yoga = 1
Government Ayurveda Medicinal Plants Gardens = 9
Government Ayurveda pharmacy = 2
• Rajpipla in Narmada District
• vadodara
Total 216 Government Homoeopathy Dispensaries are providing health care facilities at far flung areas of state.
• vadodara


106 years of 40% f I di ’ 28% f I di ’33% f I di ’ h
Gujarat – The Pharmaceutical Hub
106 years ofexcellence8
40% of India’s CRAMS companies
28% of India’s pharma export
33% of India’s pharmasector turnover
Only manufacturer of a digestive enzyme, Pink
Largest Manufacturer of I.V. sets in India; Only
5,585 manufacturing licenses; Home to ~40%
Only manufacturer of ranitidine hydrochloride in
hPapain, in the worldmanufacturer of Balsumof CRO in the country the country
70% f di50% f i t l~ 40% f hi f 58% f th di 70% of cardiac stents manufactured
in Gujarat
50% of intraocular lenses manufactured
in Gujarat
~ 40% of machinery for pharma sector
manufactured by Gujarat
58% of orthopedic implants manufactured
in Gujarat
Gujarat, an established manufacturing base for bulk drugs and formulations with its inherent competitive advantages is poised to capture emerging global opportunities to become a Global Pharmaceuticals Hubpoised to capture emerging global opportunities to become a Global Pharmaceuticals Hub.
*CRO: Contract Research Organisations; IV: Intra Venous

M f i All hi A di C i H hi T l
Gujarat – The Pharmaceutical Hub
Manufacturing Units in Gujarat (till March,
2014)
Allopathic Ayurvedic Cosmetics Homeopathic Total
2,313 625 394 8 3,339
60%40%
Gujarat's Pharma Exports
in exports2820
2000
2500
3000
Pharma Exports from Gujarat $ Billion
60%40%
4 %
increase
1780
500
1000
1500
2000
Formulation Bulk Drugs 1584
0
2004 2013
Gujarat manufactures and exports different dosage forms including tablets, capsules, dry syrup, externalpreparations cyto‐toxic drugs sex hormone drugs vaccines small & large volume parental APIs biotechpreparations, cyto toxic drugs, sex hormone drugs, vaccines, small & large volume parental, APIs, biotechand bio‐pharma products, medical devices etc

State Infrastructure
46
40
45
50
Number of Blood Storage Centers
23
20
25
30
35
40
12
5
10
15
20
Government Trust Private
0
• Total number of Blood Storage Centers = 81 • Number of laboratories = 3g• Total number of Blood banks = 139• Number of FDCA offices = 25
• Number of exhibitions Vans = 1• Number of testing Vans = 1

Ahmedabad cluster
Pharma Clusters in Gujarat
Manufacturing Base:
APIs
Formulations
Bi l i l
Vadodara cluster
Manufacturing Base:
Formulations
Biogenerics Biologicals
Contract manufacturing
g
Ankleshwar cluster
Manufacturing Base:
APIs
Formulations
VaccinesBharuch and
Vapi/Valsad cluster
Manufacturing Base:
Formulations
APIs
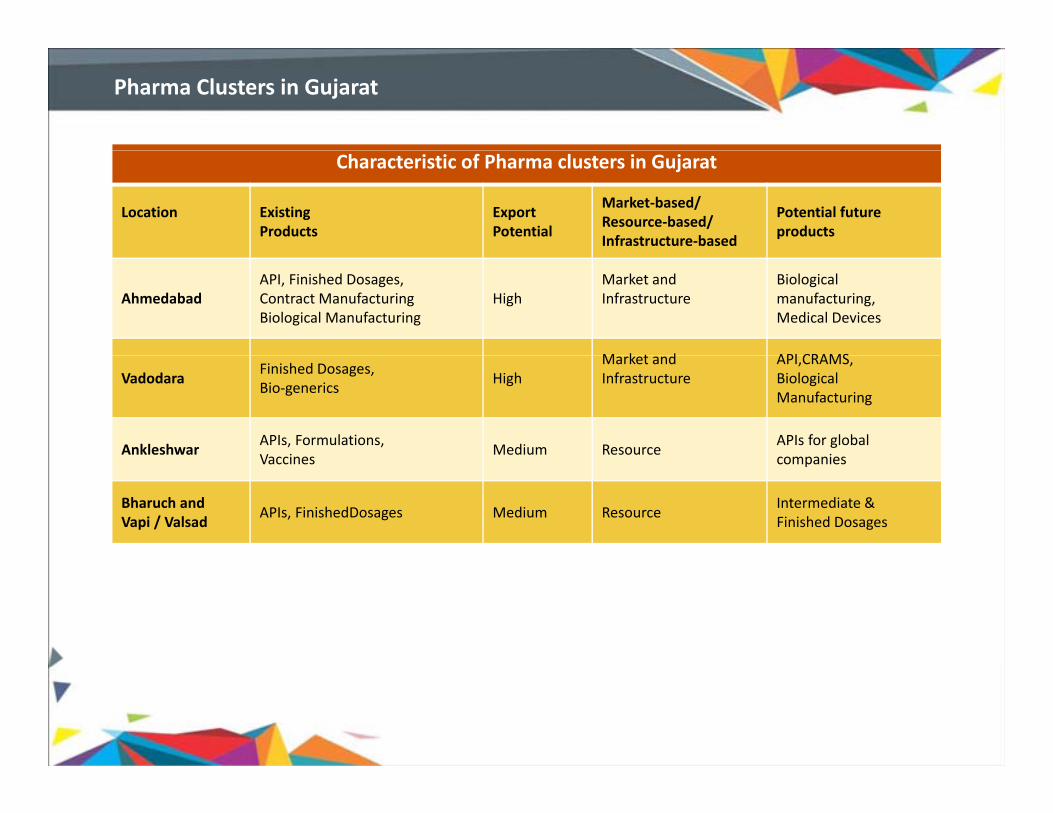
Pharma Clusters in Gujarat
Characteristic of Pharma clusters in Gujarat
Location Existing Products
Export Potential
Market‐based/ Resource‐based/ Infrastructure‐based
Potential future products
AhmedabadAPI, Finished Dosages,Contract ManufacturingBiological Manufacturing
HighMarket andInfrastructure
Biologicalmanufacturing,Medical Devices
M k t d API CRAMSVadodara
Finished Dosages,Bio‐generics
HighMarket andInfrastructure
API,CRAMS,BiologicalManufacturing
AnkleshwarAPIs, Formulations,Vaccines
Medium ResourceAPIs for globalcompaniesVaccines companies
Bharuch andVapi / Valsad
APIs, FinishedDosages Medium ResourceIntermediate &Finished Dosages

Potential in Special Economic Zone (SEZ) andSpecial Investment Region (SIR)
PHARMEZ (Zydus Cadila)Location: AhmedabadArea: 49 hectareLikely activities:
PHAEZ (Cadila Pharma)Location: AhmedabadArea: 200 hectareLikely activities: Biologicals,
Pharmaceuticals APIs & Pharmaceuticals
Jubilant PHARMA SEZLocation: BharuchArea: 200 hectare
Ahmedabad
Bharuch
Ahmedabad
Likely activities: Manufacturing hub for pharmaceuticals,fine & specialty chemicals outsourcing
Dishman PHARMA SEZLocation: Ahmedabad
J B Chemicals SEZLocation: BharuchA 130 h t
Bharuch
Location: AhmedabadArea:139 hectareLikely Activities: Bulk drugs
Area: 130 hectareLikely activities: R&D, Bulkdrugs, Intermediates & Contract manufacturing
SIR
Pharmaceuticals identified as a potential sector in 3 SIRs : Viramgam, Changodar and Okha

National Research center for Medicinal &A ti Pl t
Academic Infrastructure
Aromatic Plants National Dairy Development Board Gujarat State Fertilisers Corporation Sun Pharma research center MS University of Vadodara Anand Agriculture University
NIPER Gujarat Cancer
Research Institute
Anand Agriculture University
Navsari Agriculture University
Directorate of Forensic Science
B.V. Patel PERDcenter
Zydus Research Center National Research Center for
Sabarkantha
Surendranagar
Ahmedabad
Kutch
Mehsana
Gandhinagar
Center North Gujarat
University Department of
Biotech, Gujarat University
Nirma Institute of
National Research Center for Groundnut Central Salt and MarineChemicals Research Institute Department of Life science,Bhavnagar University J nagadh Agric lt re
Anand
Surat
Rajkot Vadodara
Amreli
Bhavnagar
Nirma Institute of Pharmacy
Junagadh Agriculture University Department of Bioscience, Saurashtra University
Valsad
First pharmacy college in India was established in Gujarat ‐ L. M. College of Pharmacy established in 1947 providing diploma,p y g j g y p g p ,bachelor and master courses in pharmacy

Industry Players

Awards and Recognition
National e‐Governance Gold Award in Year 2013 at Jaipur1
CSI IT‐Excellence Award for the 2Health Sector at Kolkata
XLN identified amongst the 2 Projects for theNational level Rapid Roll‐Out Project by the Mi i t f IT & C i ti N D lhi
3
Ministry of IT & Communications, New Delhi
Government Initiative Health Care Sector e‐INDIA – 2013 Award at Hyderabad
4

Important Links
Web Portal Link
FDCA’s Web site http://gujhealth.gov.in/food_drug
Sales License Software http://xlnfda.guj.nic.in
Manufacturing License Software – For Manufacturer http://idmla.guj.nic.in
Manufacturing License Software – For FDCA Officers http://dmla.guj.nic.in
Online Complaint Module http://gujhealth.gov.in/complaint
FDCA Toll Free Number 24 X 7 : 1800‐233‐5500

Special Economic Zone (SEZ) in healthcare
State government has sanctioned 50 SEZs covering over 16,500 acres of land. 50 SEZs include many healthcare and pharma setups. Some of them arementioned below:
• The State is setting up Biotech SEZ at Savli, Vadodara spread over a total area of g p , p1700 acres and it is touted as the largest in the country
• Zydus Cadila – 48 hectares at Ahmedabad
• Cadila Pharma – 100 hectares at Haripura
• Jubilant – 100 hectares at Vilayat
• J B Chemicals – 130 hectares at Panoli, Ankleshwar
• Dishman Pharma – 138 hectares at Ahmedabad
• Sterling Multi Product SEZ
S h //h l h fi i lSources: http://healthcare.financialexpress.com

Medical Tourism Policy was announced by State Government in 2006
3. Medical Tourism in Gujarat
Key facilitators for Advantage Gujarat are:‐
Zero waiting periods for all patient either requiring emergency treatment or otherwise
Medical Tourism Policy was announced by State Government in 2006
The following factors can further boost medical tourism:
Assisted healthcare institutions
(1/10)th ‐ (1/20)th of the costs involved for medical treatment in USA or UK
Specialized hospitals and clinics
Doctors participating in world medical conferences to understand the latest d l t i th di l fi ld
such as day care centres
Support services such as nursing associations
Linkages with infrastructure developments in the medical field.
Large percentage of NRG's among NRI's
Direct air connectivity between Ahmedabad and major international locations
Well connected with the base metros like Delhi and Mumbai
facilities for transportation of patients from airports and railway stations
Linkages with organisations/ NGOs, etc., in overseas countries to
Good roads and infrastructure compared to other states of India
,acquire knowledge and leverage opportunities

4. Investment Opportunities
Integrated medicity
Healthcare outsourcing (BPO)
Establishing global accreditations facilities
High – tech MRI/ CT scan facilities
Opportunities in the Healthcare Industry
Establishing chain of primary public / community centres
Holistic wellbeing – yoga, physiotherapy, acupressure
Computer navigated surface replacement surgery of the hip and knee‐joint
Low cost paid surrogacy through in‐itro Fertilisation
Hospital management on rehabilitate, operate and transfer (ROT) basis
Clinical research and trials
Equipment Manufacturing Units

State Health Mission (Chief Minister) and State Health Society (Chief Secretary, http://www mohfw nic in/
For Additional Information Connect Us @
State Ministry of Health and Family Welfare http://www.mohfw.nic.in/
H&FW) http://www.mohfw.nic.in/
Department of Ayush http://indianmedicine.nic.in/
Department of Health Research http://www.dhr.gov.in/
Department of AIDS Control http://www.gsacsonline.org
State Ministry of Health and Family Welfare http://www.mohfw.nic.in/
Food & Drug Commissioner http://www.gujhealth.gov.in/
Commissioner Health http://www.gujhealth.gov.in
iNDEXTb -Industrial Extension Bureau
Gujarat Industrial Development Corporation
http://www.indextb.com
http://www.gidc.gov.in

Knowledge Partner Event PartnerOrganised By Knowledge Partner Event PartnerOrganised By
Vsit us at www.vibrantgujarat.com





























