Embed Size (px)
Citation preview

Understanding Recent Progress in Multiple Myeloma:
Clinical Implications and PerspectivesCarol Ann Huff, MD
Director, Myeloma ProgramAssociate Professor of Oncology
John Hopkins Sidney Kimmel Comprehensive Cancer Center

Disclosures
Dr. Huff discloses the following commercial relationships:
Advisory Board: Celgene, Janssen, MedImmune

Learning Objectives
Distinguish therapeutic strategies for patients with low- versus high-risk MM
Evaluate safety and efficacy data on novel therapies for newly diagnosed and relapsed/refractory MM
Assess disease monitoring and supportive care strategies for patients with MM
MM = multiple myeloma.

Overall Survival From Time of Diagnosis in 6-Year Intervals
Kumar et al, 2008.

Myeloma: Scope of the Problem
Median time to first relapse with current therapies: 3-4 years
Kumar, Dispenzieri, et al, 2014.
> 100,000 patients living with myeloma

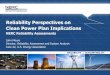
Melphalan/Prednisone
FDA Approval Bortezomib
2006
FDA ApprovalLenalidomide Thalidomide
1980s
Autologous Stem Cell Transplant
1990s
IntravenousBisphosphonates –
Reduction in Skeletal Events
1968 20041998 2013
FDA Approval Carfilzomib
2012
Initial Data onThalidomide
2015
FDA Approval Pomalidomide
FDA Approval PanobinostatDaratumumab
Ixazomib Elotuzumab
Multiple Myeloma: Evolution of Treatment

Diagnosis, Staging, and Risk Stratification

Updated IMWG Criteria for Diagnosis of Multiple Myeloma
C: Calcium elevation (>11 mg/dL or >1mg/dL higher than ULN)R: Renal insufficiency (CrCl <40 mL/min or serum creatinine >2 mg/dL)A: Anemia (Hb <10 g/dL or 2 g/dL < normal)B: Bone disease (≥1 lytic lesions on skeletal radiography, CT, or PET-CT)
IMWG = International Myeloma Working Group; BM = bone marrow; CrCl = creatinine clearance; CT = computed tomography; Hb = hemoglobin; MGUS = monoclonal gammopathy of undetermined significance; M protein = monoclonal protein; MRI = magnetic resonance imaging; PET/CT = positron emission tomography/computed tomography; ULN = upper limit of normal. Rajkumar, 2014.
MGUS
M protein <3 g/dL Clonal plasma cells in
BM <10% No myeloma-defining
events
Smoldering Myeloma
M protein ≥3 g/dL (serum) or ≥500 mg/24 h (urine)
Clonal plasma cells in BM ≥10% to 60%
No myeloma-defining events
Multiple Myeloma Underlying plasma cell
proliferative disorder AND 1 or more myeloma-
defining events ≥1 CRAB feature Clonal plasma cells in
BM ≥60% Serum free light chain
ratio ≥100 >1 MRI focal lesion

Revised International Staging System
B2M = beta-2-microglobulin; LDH = lactate dehydrogenase; NR = no response; OS = overall survival; R-ISS = revised International Staging System.Palumbo et al, 2015.
Stage Definition
I
Serum albumin ≥3.5 g/dL AND B2M ≤3.5 mg/L
Normal LDH No t(4;14), t(14;16), or
del(17p)
II Not stage I or III
III B2M ≥5.5 mg/dL PLUS Elevated LDH OR t(4;14), t(14;16), or del(17p)
1.0
0.8
0.6
0.4
0.2
00 12 24 36 48 60 72
R-ISS I NRR-ISS II 83R-ISS III 43
Median OS, Mo
MonthsPr
obab
ility
of O
S

Current Clinical Controversies
Defining high-risk disease How best to do this? Are there better therapies?
SCT indications Optimal therapy for non-SCT candidates Implications of CR vs very good partial response Minimal residual disease: Therapeutic goal or prognostic
marker? Role of consolidation/maintenance therapy Optimal sequence/combinations for relapsed/refractory
MM Aggressiveness of relapse
SCT = stem cell transplant..

Defining Risk

Are There High-Risk Features?
International Staging System Stage III Genetic abnormalities
del(13), hypodiploidy t(4;14), t(14;16), or del(17p) by FISH 1q+
Elevated LDH Gene expression profiles
FISH = fluorescent in situ hybridization.

Risk Stratification
High Risk
FISH: 17p
deletion t(14;16) t(14;20)
GEP: High risk
signature
Standard Risk
Trisomies t(11;14)
Intermediate Risk
FISH: t(4;14) 1q +
Complex karyotype
del 13 metaphase
GEP = gene expression profile. Dispenzieri et al, 2007; Kumar et al, 2009; Mikhael et al, 2013.

Survival Based on Risk
High-risk myeloma: Survival remains lower even in the era of novel
therapies
↑ risk of early mortality with ↑ risk factors: age >70 yrs, albumin <3.5 g/dL, B2M >6.5
µg/mL
Kumar, Dispenzieri et al, 2014.

SCT Considerations

Factors Affecting Transplantation Eligibility
Age >70 years of age may not be eligible Older patients more sensitive to toxicity; less physical
reserve Performance status Comorbidities
Renal impairment Cardiovascular disease Pulmonary disease Hepatic disease

High-Dose Melphalan + ASCT vs MPR in Newly Diagnosed MM
Randomized, controlled phase III trial exploring utility of high-dose melphalan + ASCT consolidation ± lenalidomide maintenance vs MPR consolidation ± lenalidomide maintenance in newly diagnosed MM
ASCT = autologous stem cell transplant; Mel = melphalan; Len = lenalidomide; MPR = melphalan, prednisone, lenalidomide; PFS = progression-free survival.Palumbo, Cavallo et al, 2014.
PFS, OS From Time of Diagnosis
Mel + ASCT + Len maintenanceMel + ASCT with no maintenance
MPR + Len maintenanceMPR with no maintenance
100
75
50
25
00 6 1
218
24
30
36
42
48
54
66
Months
PFS
(%)
21.8
60
54.737.434.2
100
75
50
25
00 6 1
218
24
30
36
42
48
54
66
Months
OS
(%)
60
(N=273)

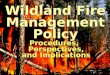
IFM/DFCI 2009: Frontline RVd ± ASCT in Younger Patients (<65 Yrs) With MM
Outcome, % RVd + ASCT(n=350)
RVd Only(n=350) HR (95% CI), P Value
4-Yr PFS 47 35 0.69 (0.56-0.84), <0.001
4-Yr OS 81 83 1.2 (0.7-1.8), NS
SPM 5 3
ORR 99 98
≥VGPR 88 78 0.001
ORR = overall response rate; RVd = lenalidomide, bortezomib, dexamethasone; SPM = second primary malignancy; NS = not significant.Attal et al, 2015.
N=700 previously untreated patients <65 years of age
PFS benefit in ASCT arm uniform across subgroups Age ≤ or >60 years), sex, lg isotype (IgG or others), ISS stage (I, II, or III),
cytogenetics (standard or high risk), and response after the first 3 cycles of RVd (complete response or not)

Induction Therapy

Case Presentation
79-year-old man presents with nausea, lower abdominal pain, and fatigue
Physical examination: T 36.4 ˚C, BP 196/95 mmHg, P 75 beats/min,R 20 breaths/min, weight 70 kg – unremarkable
Assessments Hb 9.6 g/dL Serum creatinine 1.5 mg/dL Calcium 9.9 mg/dL IgG 907 mg/dL, IgA 43 mg/dL, IgM 9 mg/dL,
lambda light chain 20,200 mg/dL B2M 20.9 mg/L Albumin 4.9 g/dL Bone marrow examination:
– 60% monoclonal plasma cells– del(13q) by cytogenetic analysis– t(4;14) by FISH
Skeletal survey shows multiple lytic lesions throughout axial skeletonT = temperature; BP = blood pressure; P = pulse rate; R = respiration rate.

Goals of Induction Therapy
Deep, rapid, and durable responses Improve performance status and quality of life Not limit PBSC mobilization in younger patients 3-drug combinations preferred Maximize the duration of response
Current questions: Optimal regimen and duration of therapy? Do these differ in
non-transplant candidates?
PBSC = peripheral blood stem cells.

Regimens Survival
Bortezomib/lenalidomide/dexamethasone (RVd)
18-mo PFS: 75% 18-mo OS: 97%
Carfilzomib/lenalidomide/dexamethasone (KRd)
12-mo PFS: 97%24-mo PFS: 92%3-yr PFS: 79%3-yr OS: 96%
Carfilzomib/thalidomide/dexamethasone (KTd) 3-yr PFS: 72%
Bortezomib/cyclophosphamide/dexamethasone (CyBorD)
5-yr PFS: 42%5-yr OS: 70%
Ixazomib/lenalidomide/dexamethasone
12-mo PFS: 88%12-mo OS: 94%
Earlier Phase Studies: Induction Regimens for Transplant-Eligible Patients
Richardson et al, 2010; Jakubowiak et al, 2012; Jasielec & Jakubowiak, 2013; Sonneveld et al, 2015; Reeder et al, 2014; Kumar, Berdeja et al, 2014.
RVdPt
s A
chie
ving
≥VG
PR (%
)KRd
KTd
CyBorD
Ixazo
mib/RD
67
81
6862 58
100
80
60
40
20
0

EVOLUTION Trial: Combinations of VD With Cyclophosphamide or Lenalidomide
Randomized phase II trial of VDC vs VDR vs VDCR in previously untreated MM
V = bortezomib; D = dexamethasone; R = lenalidomide; C = cyclophosphamide. Kumar, Flinn et al, 2012.
900
720
600
480
420
180
840
300
240
VDCR (n=48) VDR (n=42) VDC (n=33) VDC-mod (n=17)
1.0
0.8
0.6
0.4
0.2
0
Prop
ortio
n of
Pat
ient
s
Days
0 60 120
360
540
660
780
PFS, Not Censored for ASCTVDC-mod
VDR
VCDR
VDC
1.0
0.8
0.6
0.4
0.2
0
OS
VDR
VCDR
VDC
900
720
600
480
420
180
840
300
240
Days
0 60 120
360
540
660
780
Prop
ortio
n of
Pat
ient
s

MMRC: Extended KRd Treatment With ASCT in Newly Diagnosed Myeloma
Open-label, single arm phase II trial exploring utility of extended KRd treatment with transplant in NDMM (N=62) Treatment: KRd induction (4 cycles) → ASCT and KRd consolidation and maintenance
(cycles 5-18); further R maintenance off-protocol
KRd + ASCT produced a higher sCR rate at 8 cycles vs historical controls without ASCT (71% vs 30%); AEs similar to historical controls
NDMM = newly diagnosed multiple myeloma; AEs = adverse events; nCR = near complete response; sCR = serum complete response.Zimmerman et al, 2016.
Res
pons
e (%
)
100
80
60
40
20
0
85
2112 8
97
3224 22
100 100 100
717587 87 87
≥VGPR≥nCR≥CRsCR
Induction(n=48)
ASCT(n=37)
Consolidation(n=24)
End of KRd(n=8)

Modified Lenalidomide, Bortezomib, and Dexamethasone in ASCT-Ineligible Patients
Phase II trial exploring utility of modified RVd (RVd lite); N=53 Lenalidomide: single daily oral dose of 15 mg D 1-21 Bortezomib: 1.3 mg/m2 SC once weekly on D 1, 8, 15, 22 Dexamethasone: 20 mg twice weekly if ≤75 yrs or
once weekly if >75 yrs RVd lite resulted in 90% ORR (≥PR), 43% ≥VGPR
5 patients discontinued study after <4 cycles; reasons included worsening adrenal insufficiency, rash attributed to lenalidomide, travel distance
AEs manageable in an older population Grade ≥3 AEs: hypophosphatemia (31%), rash (10%)
PR = partial response; SC = subcutaneously.O’Donnell et al, 2015.

Suggested Empiric Age-Adjusted Dose Reduction in Patients With Myeloma
Agent Younger Than 65 Yrs 65-75 Yrs Older Than 75 Yrs
Dexamethasone40 mg/d D 1-4, 15-18 q4w or D 1, 8, 15, 22 q4w
40 mg/d D 1, 8,1 5, 22 q4w
20 mg/dDays 1, 8, 15, 22 q4w
Melphalan 0.25 mg/kg D 1-4 q6w 0.25 mg/kg D 1-4 q6w or 0.18 mg/kg D 1-4 q4w
0.18 mg/kg D 1-4 q6w or 0.13 mg/kg D 1-4 q4w
Cyclophosphamide300 mg/d D 1, 8, 15, 22 q4w 300 mg/d D 1, 8, 15 q4w
or 50 mg/d D 1-21 q4w
50 mg/d D 1-21 q4w or 50 mg/d QOD D 1-21 q4w
Thalidomide 200 mg/d 100 mg/d or 200 mg/d 50 mg/d to 100 mg/d
Lenalidomide 25 mg/d D 1-21 q4w 15-25 mg/d D 1-21 q4w 10-25 mg/d D 1-21 q4w
Bortezomib 1.3 mg/m2 bolus D 1, 4, 8, 11 q3w
1.3 mg/m2 bolus D 1, 4, 8, 11 q3w orD 1, 8, 15, 22 q5w
1.0-1.3 mg/m2 bolus D 1, 8, 15, 22 q5w
Palumbo et al, 2011.

Risk-Based Decision Making
Bortezomib Partially overcomes adverse effect of t(4;14) and possibly
del(17p) Lenalidomide
May improve PFS of t(4;14) and del(17p) (conflicting data) but does not improve overall survival
Pomalidomide May improve outcomes in del(17p)
Combined lenalidomide and proteasome inhibition RVd – reduces adverse effect of t(4;14) and del(17p) on PFS KRd – ASPIRE trial suggests benefit across cytogenetic groups
Sonneveld et al, 2013; Avet-Loiseau et al, 2010; Palumbo, Bringhen et al, 2014; Attal et al, 2012; Palumbo et al, 2012; McCarthy et al, 2012; Benboubker et al, 2014; Dimopoulos et al, 2015; Leleu et al, 2015; Richardson et al, 2010; Roussel et al, 2014; Stewart et al, 2015.

Other Considerations Lenalidomide
Embryo-fetal toxicity warning: – Lenalidomide, a thalidomide analogue, caused limb abnormalities in a developmental monkey study
similar to birth defects caused by thalidomide in humans. If lenalidomide is used during pregnancy, it may cause birth defects or embryo-fetal death
Venous thromboembolism (VTE) warning: – Significantly increased risk for deep vein thrombosis and pulmonary embolism, as well as risk for
myocardial infarction and stroke in MM patients receiving lenalidomide with dexamethasone. Antithrombotic prophylaxis is recommended
Bortezomib Drug interactions:
– Coadministration with strong CYP3A4 inhibitors may increase bortezomib exposure. Closely monitor patients receiving bortezomib in combination with strong CYP3A4 inhibitors
– Coadministration with strong CYP3A4 inducers may decrease bortezomib exposure. Avoid concomitant use of strong CPY3A4 inducers
Pomalidomide Embryo-fetal toxicity warning:
– Pomalidomide is contraindicated during pregnancy. Pomalidomide is a thalidomide analogue. Thalidomide is a known human teratogen that causes severe life-threatening birth defects
VTE warning:– Deep vein thrombosis and pulmonary embolism occur in MM patients receiving pomalidomide
Ixazomib Drug interactions: Avoid concomitant use with strong CYP3A inducers (eg, rifampin,
phenytoin, carbamazepine, St. John’s Wort)
Revlimid® prescribing information, 2015; Velcade® prescribing information, 2014; Pomalyst® prescribing information, 2013; Ninlaro® prescribing information, 2015.

Case Presentation
79-year-old man presents with nausea, lower abdominal pain, and fatigue
Physical examination: T 36.4 ˚C, BP 196/95 mmHg, P 75 beats/min, R 20 breaths/min, weight 70 kg – unremarkable
Assessments Hb 9.6 g/dL Serum creatinine 1.5 mg/dL Calcium 9.9 mg/dL IgG 907 mg/dL, IgA 43 mg/dL, IgM 9 mg/dL,
lambda light chain: 20,200 mg/dL B2M 20.9 mg/L Albumin 4.9 g/dL Bone marrow examination:
– 60% monoclonal plasma cells– del(13q) by cytogenetic analysis– t(4;14) by FISH
Skeletal survey shows multiple lytic lesions throughout axial skeleton

Case Presentation (cont.)
What would you choose as the optimal initial therapy? Cyclophosphamide/bortezomib/dexamethasone Lenalidomide/bortezomib/dexamethasone Carfilzomib/lenalidomide/dexamethasone Lenalidomide/dexamethasone
What factors do you take into consideration? Would your decision differ:
If the patient was 59 years old? If the patient had cardiac disease? If the patient had renal failure? If the genetics differed?

Depth of Response

Achieving ≥VGPR or CR Should Be the Goal of Therapy
Achieving ≥ VGPR
CR = complete response; PD = progressive disease; SD = stable disease.Harousseau et al, 2009; Kapoor et al, 2013.
Patients with sCR have a significantly improved outcome Estimated 5-yr OS 80% with sCR vs 53% with CR or 47% with
nCR
Prob
abili
ty o
f OS
1.00
0.8
0.4
0.2
04 5 6 7
Years Since Transplant
CR or betterVGPR
1 2 3
0.6
PRSD
PD
Achieving CR
1.00
0.75
0.50
0.25
0
Prob
abili
ty o
f OS
Years Since Transplant
CR + VGPR (n=445)
PR (n=288)
P=0.0017
4 5 6 7 81 2 30

CR Correlates With Long-Term Survival in Elderly Patients Treated With Novel Agents
Retrospective analysis: 3 randomized trials of GIMEMA and HOVON (N=1,175) First-line treatment: MP (n=332), MPT (n=332), VMP (n=257), VMPT-VT
(n=254)
MP = melphalan, prednisone; MPT = melphalan, prednisone, thalidomide; VMP = bortezomib, melphalan, prednisone; VMPT-VT = bortezomib, melphalan, prednisone, thalidomide plus maintenance bortezomib/thalidomide.Gay et al, 2011.
PFS
P<0.001 P<0 .001
Pts Older Than 75
Yrs of Age
P=0.001 P=0.004
All Pts
OS
Prob
abili
ty o
f PF
S
1.0
0.8
0.6
0.4
0.2
0
CRVGPRPR
0 24 48 72
Prob
abili
ty o
f OS
1.0
0.8
0.6
0.4
0.2
0
CRVGPRPR
0 24 48 72
Prob
abili
ty o
f PF
S
0.8
0.6
0.4
0.2
0
CRVGPRPR
0 24 48 72Months
1.0
Prob
abili
ty o
f OS
1.00.8
0.6
0.4
0.2
0
CRVGPRPR
0 24 48 72Months

Minimal Residual Disease:
Role in Myeloma

How Do We Define MRD?
Flow cytometry Next-generation sequencing Imaging – PET/CT

0 12 24 36 48 60 72
1.0
0.8
0.6
0.4
0.2
00 6 12 18 24 30 36 42
8-Color Flow Next-Gen Sequencing PET/CT
TTP
(%)
100
80
60
40
20
0100 1500 50
P=0.001
n=26
n=36
TTP (CR Pts)
MRD- MRD+
MRD-MRD+Overall
Months
PFS
(Pro
port
ion)
Months
1.0
0.8
0.6
0.4
0.2
0P=.010
PFS (CR Pts After First-line Therapy)
PET CRmedian: 90 mo
NO PET CRmedian: 50 mos
Months
PFS
PFS
(Pro
port
ion)
MRD Assessment/Outcome
TTP = time to progression.Roussel et al, 2014; Martinez-Lopez et al, 2014; Zamagni et al, 2011; Zamagni et al, 2013.

IFM 2009: Frontline RVd ± ASCT: MRD Negativity Predicts PFS
Avet-Loiseau et al, 2015.

Role of MRD Assessment
Currently a research tool but progressing rapidly toward clinical approval New IMWG response criteria forthcoming Lower levels of MRD predictive of better outcomes Potential to monitor efficacy of therapy and improve definition
of response Relapse occurs even in MRD-negative patients Many questions remain:
Optimal approach? Should therapy be changed based on results of MRD testing?

Maintenance Therapy

Lenalidomide Maintenance After ASCT in MM: Meta-Analyses
IFM = Intergroupe Francophone du Myélome; NCI = National Cancer Institute.Attal et al, 2016; McCarthy et al, 2012; Attal et al, 2012; Palumbo et al, 2014.
Study Treatment Arms Pts, n
CALGB 100104 Lenalidomide maintenancePlacebo
231229
IFM 2005-02 Lenalidomide maintenancePlacebo
307307
GIMEMA(RV-MM-PI-209)
Lenalidomide maintenanceNo maintenance
6768
3 of 17 identified studies fulfilled criteria
Lenalidomide maintenance given until progression IFM elected to discontinue lenalidomide in 2010 following
second primary malignancy signal CALGB and GIMEMA continued until progression

Cumulative Incidence of Second Primary Malignancies by Treatment
Cum Incidence, %
Solids SPM Hematological SPM3 Yrs 5 Yrs 3 Yrs 5 Yrs
Len + Mel 2.7 4.4 1.8 3.9
Len + Cyclo 3.5 NE 0.3 NE
Len + Dex 2.2 2.6 0.3 1.3
No Len 2.9 3.4 0.4 1.4
Cyclo = cyclophosphamide; Dex = dexamethasone; NE = not evaluable. Palumbo et al, 2014.
10
5
70
1 2 3 4 5 60 1 2 3 4 5 6 70
Len + MelLen + CycloLen + DexNo Len (Mel regimens)
Solid SPMs Hematological SPMsLen + MelLen + CycloLen + DexNo Len (Mel regimens)
Cum
ulat
ive
Inci
denc
e (%
)
Cum
ulat
ive
Inci
denc
e (%
) 10
5
0
Years Years

Lenalidomide Maintenance After ASCT in MM: Conclusions
Meta-analysis: Lenalidomide maintenance significantly increased OS post-ASCT in MM Effect seen in all studies; magnitude varied Estimated median OS improvement 2.5 yrs Benefit seen in most subgroups except high-risk cytogenetics HR 1.18 (95% CI:0.66-2.10)
Survival benefit outweighs risk for second primary malignancies
Evidence suggests lenalidomide maintenance post-ASCT should be standard of care in MM MRD may have role in guiding treatment decisions Unclear whether all patients benefit from maintenance
Attal et al, 2016.

FIRST Trial: Efficacy Analysis of Len/Dex vs MPT in SCT-Ineligible Patients
Rd18 = 18 weeks of lenalidomide, low-dose dexamethasone.Benboubker et al, 2014.
Median PFS, Mo
Rd (n=535) 25.5Rd18 (n=541) 20.7MPT (n=547) 21.2
HR (P Value)Rd vs MPT: 0.72 (0.00006)Rd vs Rd18: 0.70 (0.00001) Rd18 vs MPT: 1.03 (0.70349)
4-Yr OS, %Rd (n=535) 59.4Rd18 (n=541) 55.7MPT (n=547) 51.4
HR (P Value)Rd vs MPT: 0.78 (0.0168)Rd vs Rd18: 0.90 (0.307) Rd18 vs MPT: 0.88 (0.184)
100
80
60
40
20
0
100
80
60
40
20
0
Progression-Free Survival (Mo)
Prog
ress
ion-
Free
Sur
viva
l (%
)
0 6 12 18 24 30 36 42 48 54 60
72 w
ks
Overall Survival (Mo)
Ove
rall
Surv
ival
(%)
0 6 12 18 24 30 36 42 48 54 60
Overall response (continuous Rd vs MPT): 75% vs 62% (P <0.00001) Similar, tolerable safety profiles between treatment groups Incidence of second primary malignancies: 3% with continuous Rd vs 6% with Rd18 vs
5% with MPT

Relapsed and Relapsed/Refractory
Myeloma

Case Presentation
72-year-old man diagnosed with ISS stage III MM in 2010. At presentation, FISH showed hyperdiploid MM Enrolled in a clinical trial and received RVd x 8 cycles followed
by ASCT Achieved CR (MRD testing was not performed) and began
lenalidomide maintenance (10 mg) Is 5.5 years post-SCT with evidence of relapsed disease based
on emergent M spike of 0.5 g/dL What would you do next?

Case Presentation (cont.)
52-year-old man who was diagnosed with ISS stage III MM in 2015. At presentation, FISH showed 1q+, t(4;14), and del(17p). Enrolled in a clinical trial and received KRd x 8 cycles followed
by ASCT Achieved CR and began lenalidomide maintenance (10 mg) Is 1 year post-SCT with evidence of relapsed disease based on
emergent M spike of 0.5 g/dL What would you do next?

Confronting Disease Relapse in Myeloma
EFS = event-free survival.Kumar et al, 2004; Kumar, Lee et al, 2012.
Patie
nts
(%)
100
80
60
40
0
20
0 12 24 36 48 60
Months From Time Zero
OSEFS
Events/N170/286217/286
Median, Mo
9 (7-11)5 (4-6)
12
10
8
6
0
2
First Second Third Fourth Fifth Sixth
Treatment Regimen
Med
ian
Res
pons
e D
urat
ion
(Mo)
4

Considerations in Relapsed Myeloma
Does this patient need treatment? Are there new high-risk features? What drugs have been used thus far? Response to
previous treatments? (efficacy, duration of response, toxicity)
How fit is the patient (PS, marrow reserve)? What are the patient’s goals/preferences?
PS = performance status.

ASPIRE: KRd vs Rd: Interim OS Analysis
OS results did not meet prespecified statistical boundary (P=0.005) at interim AEs consistent with previous studies; no unexpected toxicities observed
Grade ≥3 cardiac failure and ischemic heart disease: 3.8% and 3.3% in KRd arm vs 1.8% and 2.1% in Rd arm, respectively
NR = not reached.Stewart et al, 2015.
KRd Rd(n=396) (n=396)
Median OS, mo NR NRHR (KRd/Rd) (95% CI) 0.79 (0.63-0.99)P value .04
Median follow-up: 32 mo
1.0
0.8
0.6
0.4
0.2
0
Pro
porti
on S
urvi
ving
KRdRd
0 6 12 18 24 30 36 42 48Months Since Randomization

Pomalidomide + Low-Dose Dexamethasone in Relapsed/Refractory MM
Pom + LoDex approved for relapsed MM following ≥2 lines of therapy
Phase II MM-002 study (N=221): ORR of 33% with Pom + LoDex vs
18% with Pom DoR of 8.3 mo with Pom +
LoDex vs 10.7 mo with Pom Low rates of discontinuations
due to AEs– Grade 3/4 neutropenia occurred in
41% of Pom + LoDex patients, and 48% of Pom patients
– No grade 3/4 peripheral neuropathy reported
LoDex = low dose dexamethasone.Richardson et al, 2014.
PFS
Median PFS, Mo4.22.7
Pom + LoDexPom
100
80
60
40
20
0
Patie
nts
(%)
0 5 2010 15 25 30
PFS (Mo)
HR: 0.68P= 0.003

Phase I/II Study of KPd in Relapsed/Refractory Multiple Myeloma
Relapsed/refractory MM with measurable disease after ≥1 prior therapy MTD: Carfilzomib 27 mg/m2/dose D 1,2,8,9,15,16 every 28 d,
Pomalidomide 4 mg x 21 d, Dexamethasone 40 mg D 1,8,15 Median follow-up 17.9 mo (range 0.3–40.6)
KPd = carfilzomib, pomalidomide, dexamethasone.Rosenbaum et al, 2016.
Outcome PFS (n=56) OS (n=56)Median duration, mo 12.9 NR1-yr rate, % 53 912-yr rate, % 22 78
ITT Response, % All Evaluable Pts Primary Study Population*
Best response (n=55) (n=45)
• CR/nCR 16 13
• ≥VGPR 47 44
• ≥PR 84 84
• ≥MR 93 96

60
100
Bort/Dex ± Panobinostat in RR Myeloma: Pts who Received Prior Bort and IMiDs
Subgroup analysis of patients who received ≥2 previous treatments, including bortezomib and an IMiD FDA approved indication based on subgroup analysis
PFS
Pro
babi
lity,
(%)
RR = relapsed/refractory; IMiD = immunomodulatory drug.Richardson et al, 2016.
Time (months)
80
40
20
00 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Pan/bort/dexPlacebo/bort/dex
Median PFS, Mos (95% CI)
Events, n/N
44/7354/74
12.5 (7.3-14.0)4.7 (3.7-6.1)
HR(95% CI)
0.47 (0.31-0.72)

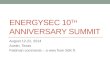
Phase II SIRIUS: Daratumumab Showed Activity in Heavily Pretreated MM
Median PFS: 3.7 mo (95% CI: 2.8-4.6); 1-yr OS: 65% (95% CI: 51.2-75%) Most common grade 3/4 AEs: thrombocytopenia (25%), anemia (24%), and
neutropenia (14%); infusion-related reactions occurred in 43% (most grade 1/2)
Lonial, Weiss et al, 2015.
sCR 3%
VGPR 9%
PR 17%
Overall Pt
Population
0
15
20
25
30
35
Pts
Ach
ievi
ng
Obj
ectiv
e R
espo
nse
(%) 29
Age ≥75
yr
10
5
CrCl ≥
60 m
L/min
>3 Lines
of Tx
Extram
edulla
ry
High-Risk
Cytogen
etics
PIs an
d IMiD
Carfilz
omib
Pomalidomide
Carfilz
omib/
Pomalidomide
Bortezo
mib/
Lenolid
omide
Bortezo
mib/
Lenolid
omide/
Carfilz
omib/
Pomalidomide
33 3330
21 20
30 29 28 28 26
21
ORR by Subgroup ORR by Refractory Status

0.8
CASTOR: Daratumumab Improves PFS
Pro
gres
sion
-Fre
e S
urvi
val (
%)
0
0.2
0.4
0.6
1.0
0 3 6 9 12 15Months
1-Yr PFS*
60.7%
26.9%DVdVd
Median (mo)NR7.2
HR: 0.39 (95% CI: 0.28-0.53; P<0.0001)
DVd = daratumumab/bortezomib/dexamethasone; Vd = bortezomib/dexamethasone;VGPR = very good partial response.Palumbo et al, 2016.

ELOQUENT-2: Anti-SLAMF7 Monoclonal Antibody Elotuzumab + Rd vs Rd
PFS benefit seen with elotuzumab in all predefined subgroups
Lonial, Dimopoulos et al, 2015.
Outcome Elotuzumab + Rd(n=321)
Rd(n=325) HR (95% CI)
PFS Median, mo 1 Yr, % 2 Yrs, % 3 Yrs, %
19.4684126
14.9572718
0.73 (0.60-0.89;P=0.0014)
Median time to next treatment, mo 33 21 0.62 (0.50-0.77)
ORR, % 79 66
Interim OS, mo 43.7 39.6 0.77 (0.61-0.97;P=0.0257)

TOURMALINE-MM1: Ixazomib Efficacy
PFS benefit with ixazomib seen in all prespecified subgroups, including cytogenetic high risk, PI, and IMiD exposed
Grade 3/4 AEs occurred in 74% of the ixazomib group and 69% of the placebo group Thrombocytopenia: 19% in ixazomib group, 9% in placebo group Rash: 36% in ixazomib group, 23% of placebo group Peripheral neuropathy: 27% in ixazomib group, 22% in placebo group
aHR: 0.742; bHR: 0.712.PI = proteasome inhibitor.Moreau et al, 2016.
Characteristic Ixazomib + Rd(n=360)
Placebo + Rd(n=362) P Value
Median PFS, mos 20.6 14.7 0.012a
ORR, % CR VGPR PR
78.311.736.466.7
71.56.6
32.364.9
0.0350.019
Median time to response, mos 1.1 1.9
Median DoR, mos 20.5 15.0
Median TTP, mos 21.4 15.7 0.007b

Case Presentation
72-year-old man diagnosed with ISS stage III MM in 2010. At presentation, FISH showed hyperdiploid MM Enrolled in a clinical trial and received RVd x 8 cycles followed
by ASCT Achieved CR (MRD testing was not performed) and began
lenalidomide maintenance (10 mg) Is 5.5 years post-SCT with evidence of relapsed disease based
on emergent M spike of 0.5 g/dL What would you do next?

Case Presentation: Next Steps
Repeat staging including: Bone marrow aspirate and genetic testing Skeletal imaging Serum and urine assessment of disease
Treatment considerations: Genetic changes Prior therapy Comorbid illnesses Patient preference

Case Presentation
52-year-old man diagnosed with ISS stage III MM in 2015. At presentation, FISH showed 1q+, t(4;14) and del(17p) Enrolled in a clinical trial and received KRd x 8 cycles followed
by ASCT Achieved CR and began lenalidomide maintenance (10 mg) Is 1 year post-SCT with evidence of relapsed disease based on
emergent M spike of 0.5 g/dL What would you do next?

Case Presentation: Next Steps
Repeat staging including: BM aspirate and genetic testing Skeletal imaging Serum and urine assessment of disease
Treatment Considerations: Genetic changes Prior therapy Comorbid illnesses Patient preference

Key Takeaways
Treatment landscape in myeloma is rapidly evolving with many emerging therapies that have translated into improved survival
Patients should be risk stratified based on clinical and genetic features that can help guide therapeutic decisions
Depth of response matters and is generally associated with superior outcomes
MRD testing is rapidly moving to clinical application offering the potential of recognizing deeper remissions, raising questions as to what to do for those who remain MRD positive

References
Attal M, Palumbo A, Holstein SA, et al (2016). Lenalidomide (LEN) maintenance (MNTC) after high-dose melphalan and autologous stem cell transplant (ASCT) in multiple myeloma (MM): a meta-analysis (MA) or overall survival (OS). J Clin Oncol (ASCO Annual Meeting Abstracts), 34, Abstract 8001.
Attal M, Lauwers-Cances V, Hulin C, et al (2015). Autologous transplantation for multiple myeloma in the era of new drugs: a phase III study of the Intergroupe Francophone du Myélome (IFM/DFCI 2009 Trial). Blood, 126(23):391.
Attal M, Lauwers-Cances V, Marit G, et al (2012). Lenalidomide maintenance after stem-cell transplantation for multiple myeloma. N Engl J Med, 366(19):1782-1791. DOI: 10.1056/NEJMoa1114138
Avet-Loiseau H, Corre J, Lauwers-Cances V, et al (2015). Evaluation of minimal residual disease (MRD) by next generation sequencing (NGS) is highly predictive of progression free survival in the IFM/DFCI 2009 trial. Blood, 126(23):191.
Avet-Loiseau H, Leleu X, Roussel M, et al (2010). Bortezomib plus dexamethasone induction improves outcome of patients with t(4;14) myeloma but not outcome of patients with del(17p). J Clin Oncol, 28(30):4630-4634. DOI:10.1200/JCO.2010.28.3945
Benboubker L, Dimopoulos MA, Dispenzieri A, et al (2014). Lenalidomide and dexamethasone in transplant-ineligible patients with myeloma. N Engl J Med, 371(10):906-917. DOI:10.1056/NEJMoa1402551
Cavo M, Tacchetti P, Patriarca F, et al (2010). Bortezomib with thalidomide plus dexamethasone compared with thalidomide plus dexamethasone as induction therapy before, and consolidation therapy after, double autologous stem-cell transplantation in newly diagnosed multiple myeloma: a randomised phase 3 study. Lancet, 376(9758):2075-2085. DOI:10.1016/S0140-6736(10)61424-9
Cytoxan® (cyclophosphamide) prescribing information (2013). Baxter Healthcare Corporation. Available at: http://www.accessdata.fda.gov
Dimopoulos MA, Weisel KC, Song KW, et al (2015). Cytogenetics and long-term survival of patients with refractory or relapsed and refractory multiple myeloma treated with pomalidomide and low-dose dexamethasone. Haematologica, 100(10):1327-1333. DOI:10.3324/haematol.2014.1177077
Dispenzieri A, Rajkumar SV, Gertz MA, et al (2007). Treatment of newly diagnosed multiple myeloma based on Mayo Stratification of Myeloma and Risk-adapted Therapy (mSMART): consensus statement. Mayo Clin Proc, 82(3):323-341.
Gay F, Larocca A, Wijermans P, et al (2011). Complete response correlates with long-term progression-free and overall survival in elderly myeloma treated with novel agents: analysis of 1175 patients. Blood, 117(11):3025-3031. DOI:10.1182/blood-2010-09-307645
Harousseau JL, Avet-Loiseau H, Attal M, et al (2009). Achievement of at least very good partial response is a simple and robust prognostic factor in patients with multiple myeloma treated with high-dose therapy: long-term analysis of the IFM 99-02 and 99-04 Trials. J Clin Oncol, 27(34):5720-5726. DOI:10.1200/JCO.2008.21.1060

References
Jakubowiak AJ, Dytfeld D, Griffith KA, et al (2012). A phase 1/2 study of carfilzomib in combination with lenalidomide and low-dose dexamethasone as a frontline treatment for multiple myeloma. Blood, 120(9):1801-1809. DOI:10.1182/blood-2012-04-422683
Jasielec JK & Jakubowiak AJ (2013). Current approaches to the initial treatment of symptomatic multiple myeloma. Int J Hematol Oncol, 2(1). DOI:10.2217/ijh.13.3
Kapoor P, Kumar SK, Dispenzieri A, et al (2013). Importance of achieving stringent complete response after autologous stem-cell transplantation in multiple myeloma. J Clin Oncol, 31(36):4529-4535. DOI:10.1200/JCO.2013.49.0086
Kumar SK, Berdeja J, Niesvizky R, et al (2014). Safety and tolerability of ixazomib, an oral proteasome inhibitor, in combination with lenalidomide and dexamethasone in patients with previously untreated multiple myeloma: an open-label phase 1/2 study. Lancet Oncol, 15(13):1503-1512.
Kumar SK, Dispenzieri A, Lacy MQ, et al (2014). Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients. Leukemia, 28(5):1122-1128. DOI:10.1038/leu.2013.313
Kumar SK, Flinn I, Richardson PG, et al (2012). Randomized, multicenter, phase 2 study (EVOLUTION) of combinations of bortezomib, dexamethasone, cyclophosphamide, and lenalidomide in previously untreated multiple myeloma. Blood, 119:4375-4382.
Kumar SK, Lee JH, Lahuerta JJ, et al (2012). Risk of progression and survival in multiple myeloma relapsing after therapy with IMiDs and bortezomib: a multicenter international myeloma working group study. Leukemia, 26(1):149-157. DOI:10.1038/leu.2011.196
Kumar SK, Mikhael JR, Buadi FK, et al (2009). Management of newly diagnosed symptomatic multiple myeloma: updated Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) consensus guidelines. Mayo Clin Proc, 84(12):1095-1110. DOI:10.4065/mcp.2009.0603
Kumar SK, Rajkumar SV, Dispenzieri A, et al (2008). Improved survival in multiple myeloma and the impact of novel therapies. Blood, 111(5):2516-2520.
Kumar SK, Therneau TM, Gertz MA, et al (2004). Clinical course of patients with relapsed multiple myeloma. Mayo Clin Proc, 79(7):867-874.
Leleu X, Karlin L, Macro M, et al (2015). Pomalidomide plus low-dose dexamethasone in multiple myeloma with deletion 17p and/or translocation (4;14): IFM 2010-02 trial results. Blood, 125(9):1411-1417. DOI:10.1182/blood-2014-11-612069
Lonial S, Dimopoulos MA, Palumbo A, et al (2015). ELOQUENT-2: a phase III, randomized, open-label study of lenalidomide (len)/dexamethasone (dex) with/without elotuzumab (elo) in patients (pts) with relapsed/refractory multiple myeloma (RMM). J Clin Oncol (ASCO Annual Meeting Abstracts), 33. Abstract LBA8512.

References
Lonial S, Weiss BM, Usmani SZ, et al (2015). Phase II study of daratumumab (DARA) monotherapy in patients with ≥ 3 lines of prior therapy or double refractory multiple myeloma (MM):54767414MMY2002 (Sirius). J Clin Oncol (ASCO Annual Meeting Abstracts), 33. Abstract LBA8512.
Martinez-Lopez J, Lahuerta JJ, Pepin F, et al (2014). Prognostic value of deep sequencing method for minimal residual disease detection in multiple myeloma. Blood, 123(20):3073-3079. DOI:10.1182/blood-2014-01-550020
McCarthy PL, Owzar K, Hofmeister CC, et al (2012). Lenalidomide after stem-cell transplantation for multiple myeloma. N Engl J Med, 366(19):1770-1781. DOI:10.1056/NEJMoa1114083
Mikhael JR, Dingli D, Roy V, et al (2013). Management of newly diagnosed asymptomatic multiple myeloma: updated Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) consensus guidelines 2013. Mayo Clin Proc, 88(4):360-376. DOI:10.1016/j.mayocp.2013.01.019
Moreau P, Masszi T, Grzasko N, et al (2016). Oral ixazomib, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med, 374(17):1621-1634. DOI:10.1056/NEJMoa1516282
Ninlaro® (ixazomib) prescribing information (2015). Millennium Pharmaceuticals. Available at: http://www.ninlaro.com O’Donnell EK, Laubach JP, Yee AJ, et al (2015). A phase II study of modified lenalidomide, bortezomib, and dexamethasone (RVD-
lite) for transplant-ineligible patients with newly diagnosed multiple myeloma. Blood, 126(23):4217. Palumbo A, Avet-Loiseau H, Oliva S, et al (2015). Revised International Staging System for multiple myeloma: a report from
International Myeloma Working Group. J Clin Oncol, 33(26):2863-2869. DOI:10.1200/JCO.2015.61.2267Palumbo A, Bringhen S, Kumar SK, et al (2014). Second primary malignancies with lenalidomide therapy for newly diagnosed
myeloma: a meta-analysis of individual patient data. Lancet Oncol, 15(3):333-342. DOI:10.1016/S1470-2045(13)70609-0Palumbo A, Cavallo F, Gay F, et al (2014). Autologous transplantation and maintenance therapy in multiple myeloma. N Engl J
Med, 371(10):895-905. DOI:10.1056/NEJMoa1402888Palumbo A, Chanan-Khan A, Weisel K, et al (2016). Daratumumab, bortezomib, and dexamethasone for Multiple myeloma. N Engl
J Med,375(8):754-766. DOI:10.1056/NEJMoa1606038Palumbo A, Hajek R, Delforge M, et al (2012). Continuous lenalidomide treatment for newly diagnosed multiple myeloma. N Engl
J Med, 366(19):1759-1769. DOI:10.1056NEJMoa1112704Palumbo A, Bringhen S, Ludwig H, et al (2011). Personalized therapy in multiple myeloma according to patient age and
vulnerability: a report of the European Myeloma Network (EMN). Blood, 118(17):4519-4529. DOI:10.1182/blood-2011-06-358812
Pomalyst® prescribing information (2013). Celgene Corporation. Available at: http://www.pomalyst.com Rajkumar SV, Dimopoulos MA, Palumbo A, et al (2014). International Myeloma Working Group updated criteria for the diagnosis
of multiple myeloma. Lancel Oncol, 15(12):e538-548. DOI:10.1016/S1470-2045(14)70442-5

References
Reeder CB, Reece DE, Kukreti V, et al (2014). Long-term survival with cyclophosphamide, bortezomib and dexamethasone induction therapy in patients with newly diagnosed multiple myeloma. Br J Haematol, 167(4):563-565.
Revlimid® (lenalidomide) prescribing information (2015). Celgene Corporation. Available at: www.revlimid.com Richardson PG, Hungria VTM, Yoon S-S, et al (2016). Panobinostat plus bortezomib and dexamethasone in previously treated
multiple myeloma: outcomes by prior treatment. Blood, 127:713-721.Richardson PG, Siegel DS, Vij R, et al (2014). Pomalidomide alone or in combination with low-dose dexamethasone in relapsed
and refractory multiple myeloma: a randomized phase 2 study. Blood, 123(12):1826-1832. DOI:10.1182/blood-2013-11-538835
Richardson PG, Weller E, Lonial S, et al (2010). Lenalidomide, bortezomib, and dexamethasone combination therapy in patients with newly diagnosed multiple myeloma. Blood, 116(5):679-686. DOI:10.1182/blood-2010-02-268862
Rosenbaum CA, Stephens LA, Kukreti V, et al (2016). Phase 1/2 study of carfilzomib, pomalidomide, and dexamethasone (KPd) in patients (Pts) with relapsed/refractory multiple myeloma (RRMM): a Multiple Myeloma Research Consortium multicenter study. J Clin Oncol (ASCO Annual Meeting Abstracts), 34. Abstract 8007.
Roussel M, Lauwers-Cances V, Robillard N, et al (2014). Front-line transplantation program with lenalidomide, bortezomib, and dexamethasone combination as induction and consolidation followed by lenalidomide maintenance in patients with multiple myeloma: a phase II study by the Intergroupe Francophone du Myélome. J Clin Oncol, 32(25):2712-2717. DOI:10.1200/JCO.2013.54.8164
San Miguel JF, Schlag R, Khuageva NK, et al (2008). Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. N Engl J Med, 359(9):906-917. DOI:10.1056/NEJMoa0801479
Sonneveld P, Asselbergs E, Zweegman S, et al (2015). Phase 2 study of carfilzomib, thalidomide, an dexamethasone as induction/consolidation therapy for newly diagnosed multiple myeloma. Blood, 125(3):449-456. DOI:10.1182/blood-2014-05-576256
Sonneveld P, Goldschmidt H, Rosiñol L, et al (2013). Bortezomib-based versus nonbortezomib-based induction treatment before autologous stem-cell transplantation in patients with previously untreated multiple myeloma: a meta-analysis of phase III randomized, controlled trials. J Clin Oncol, 31(26):3279-3287. DOI:10.1200/JCO.2012.48.4626
Stewart AK, Rajkumar SV, Dimopoulos MA, et al (2015). Carfilzomib, lenalidomide, an dexamethasone for relapsed multiple myeloma. N Engl J Med, 372(2):142-152. DOI:10.1056/NEJMoa1411321
Thalomid® (thalidomide) prescribing information (2015). Celgene Corporation. Available at: http://www.thalomid.com Velcade® (bortezomib) prescribing information (2014). Millennium Pharmaceuticals, Inc. Available at: http://www.velcade.com

References
Zamagni E, Nanni C, Pezzi A, et al (2013). PET/CT is a useful tool for both refining the definition of complete response (CR) in multiple myeloma (MM) and detecting otherwise unrevealed progression during the follow-up of the disease: a single centre experience on 282 patients. ASH Annual Meeting Abstracts. Abstract 1936.
Zamagni E, Patriarca F, Nanni C, et al (2011). Prognostic relevance of 18-F FDG PET/CT in newly diagnosed multiple myeloma patients treated with up-front autologous transplantation. Blood, 118(23):5989-5995. DOI:10.1182/blood-2011-06-361386
Zimmerman TM, Griffith K, Jasielec JK, et al (2016). Carfilzomib (CFZ, Kyprolis®), lenalidomide (LEN, Revlimid®), and dexamethasone (DEX) (KRd) combined with autologous stem cell transplant (ASCT) shows improved efficacy compared with KRd without ASCT in newly diagnosed multiple myeloma (NDMM). Biol Blood Marrow Transplant, 22(3):S40. DOI:10.1016/j.bbmt.2015.11.320