Embed Size (px)
Citation preview

Myeloma Perspectives 2017
DR. BRIAN DURIE DR. MARIA-VICTORIA MATEOS
Brian GM DurieJanuary 12th, 2017

International Myeloma Foundation
Key Topics
Who should be treated?
Frontline options 2017
Role of autotransplant
MRD - / MRD: Testing and management
Current relapse options?
New agents/ combos?
2

International Myeloma Foundation
When Should Treatment Be Started?
Potential New Myeloma or Smoldering Myeloma
Observation
Any Myeloma Defining Events?• CRAB,
• >60% PC,
• FLC > 100,
• MRI > 1 focal
No Myeloma Defining Events (SMM)
Treat as Myeloma
High Risk SMM(Median TTP ~2 years)
Low Risk SMM(~5% per year PD)
Consider Treating as Myeloma
Evolving, or many high risk factors
Clinical Trials
Rajkumar SV, Landgren O, Mateos MV. Blood 2015;125:3069-75.
3

International Myeloma Foundation
How should HR SMM be treated?
4
Gently RdDaraElo Rd
For Cure Cesar: KRd + ASCT ASCENT: KRd + dara + ASCTiStopMM: Dara + Rd
International Myeloma Foundation
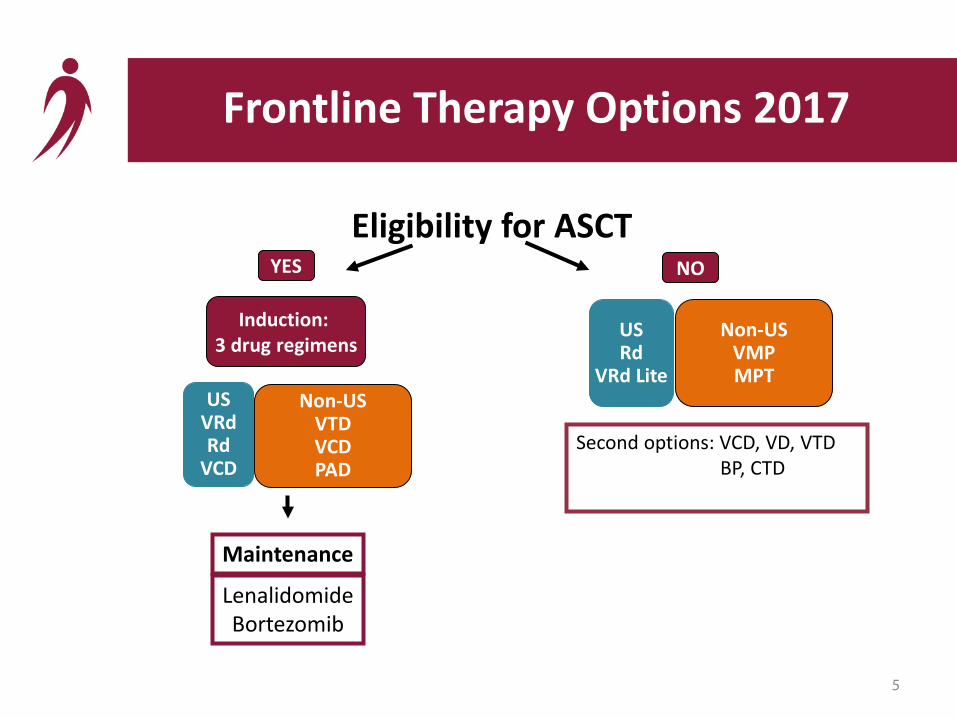
Eligibility for ASCT
Second options: VCD, VD, VTDBP, CTD
Frontline Therapy Options 2017
Induction: 3 drug regimens
YES
Maintenance
USVRdRd
VCD
Non-USVTDVCDPAD
NO
5
USRd
VRd Lite
Non-USVMPMPT
LenalidomideBortezomib

International Myeloma Foundation
Eight 21-day Cycles of VRd
Bortezomib 1.3/mg2 IVDays 1, 4, 8, and 11Lenalidomide 25 mg/day PODays 1-14Dexamethasone 20 mg/day PODays 1, 2, 4, 5, 8, 9, 11, 12
Six 28-day Cycles of Rd
Lenalidomide 25 mg/day PODays 1-21Dexamethasone 40 mg/day PODays 1, 8, 15, 22
RandomizationN = 525
Stratification:• ISS (I, II, III)• Intent to
transplant @ progression (yes/no)
SWOG S0777 Study Design
6
Lancet Dec 2016

International Myeloma Foundation
SWOG S0777 Outcome Measures
OutcomeMeasures VRd RdORR, % 82% 72%≥ VGPR, % 16% 8%Median PFS, mo 46 mo 30 moMedian OS, mo 75 mo 64 mo
7
Lancet Dec 2016

International Myeloma Foundation
SWOG S0777 Progression Free Survival by Treatment Arm
8Lancet Dec 2016
VRd

International Myeloma Foundation
Progression Free Survival (PFS) If VGPR Achieved
9
VGPR

International Myeloma Foundation
SWOG S0777Overall Survival By Treatment Arm
10Lancet (in press) 2016
VRd
International Myeloma Foundation
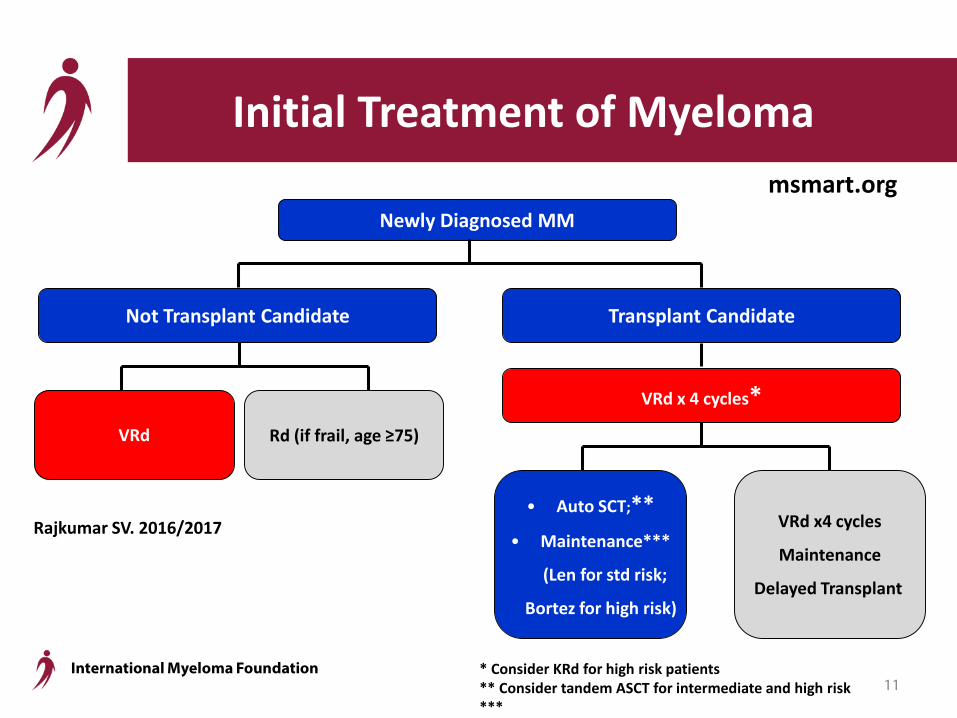
Rajkumar SV. 2016/2017
Initial Treatment of Myeloma
Not Transplant Candidate
VRd
Newly Diagnosed MM
Transplant Candidate
VRd x 4 cycles*
• Auto SCT;**• Maintenance***
(Len for std risk;
Bortez for high risk)
VRd x4 cycles
Maintenance
Delayed Transplant
Rd (if frail, age ≥75)
* Consider KRd for high risk patients** Consider tandem ASCT for intermediate and high risk***
msmart.org
11

International Myeloma Foundation
Role of Autotransplant (ASCT/HDT) Progression Free Surivival
P < 0 .0 01
0
10
20
30
40
50
60
70
80
90
10 0
Pa
tie
nts
(%
)
3 5 0 296 2 28 12 8 24no H D T35 0 309 2 61 15 3 27H D T
N a t risk
0 12 24 36 48
M o n th s o f f o l lo w -u p
H D T
no H D T
Attal M. ASH 2015 12
IFM 2009 Trial

International Myeloma Foundation
P N S
0
10
20
30
40
50
60
70
80
90
10 0P
ati
en
ts (
%)
3 5 0 33 8 3 20 24 4 56no H D T35 0 32 8 3 09 22 6 55H D T
N a t risk
0 12 24 36 48
M o n th s o f f o l lo w -u p
H D T
no H D T
Overall Survival (OS)
Attal M. ASH 201513
IFM 2009 Trial
International Myeloma Foundation
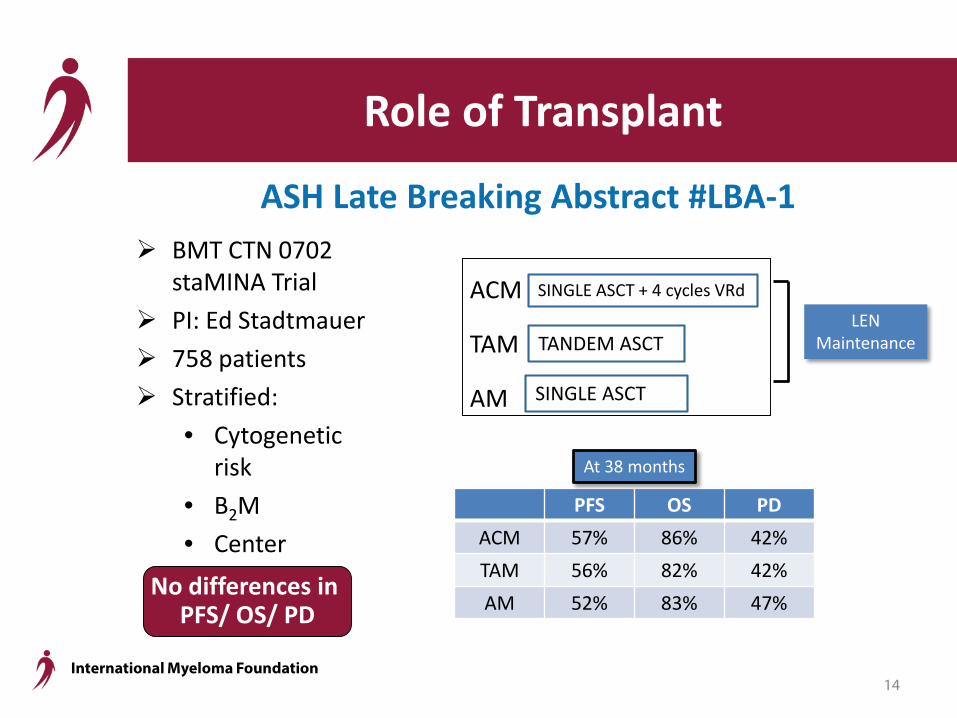
Role of Transplant
ASH Late Breaking Abstract #LBA-1 BMT CTN 0702
staMINA Trial PI: Ed Stadtmauer 758 patients Stratified:
• Cytogenetic risk
• B2M• Center
PFS OS PDACM 57% 86% 42%TAM 56% 82% 42%AM 52% 83% 47%
At 38 months
ACM
TAM
AM
TANDEM ASCTLEN
Maintenance
SINGLE ASCT + 4 cycles VRd
SINGLE ASCT
No differences in PFS/ OS/ PD
14

International Myeloma Foundation
Prog
ress
ion-
free
sur
viva
l (%
)
Time from response assessment (months)
MRD- (n=316) median PFS: 58 monthsCR (n=128) median PFS: 24 monthsnCR (n=96) median PFS: 21 monthsPR (n=199) median PFS: 26 months<PR (38) median PFS: 9 months
MRD- vs CR: P <.001CR vs nCR: P =.127
Ove
rall
surv
ival
(%)
Time from response assessment (months)
MRD- (n=316) median OS: 145 monthsCR (n=128) median OS: 59 monthsnCR (n=96) median OS: 63 monthsPR (n=199) median OS: 59 months<PR (38) median OS: 32 months
MRD- vs CR: P <.001CR vs nCR: P =.657
P <.001 P <.001
GEM2000, GEM2005MENOS65, GEM2005MAS65, GEM2010MAS65 (n=777)Lahuerta JJ, et al. manuscript under review
The true value of CR relies on the MRD status
15
MRD Negative
MRD Negative
PFS OS
International Myeloma Foundation
Need for integrated next-generation immunophenotypic and sequencingtechniques for new concepts in risk
stratification towards precision medicine
16

International Myeloma Foundation
Unsustained CR
Sustained CR
MRD-positive
Maintenance?
Which maintenance strategies are effective in patients with persistent MRD?
17
CR
MRD Negative

International Myeloma Foundation
15 cell populations
clonal PCs
normal PCsB-cell precursors
Memory B-cells
Naïve B-cells
T-&NK-cells
Cytotoxic T-&NK-cells
CD117+ Myeloid precursors
CD117+ Erythroidprecursors
Mast cellsMonocytes
Basophils
Whole BM cellularity
Eosinophils
Neutrophils
Nucleated red cells
NEXT GENERATION FLOW-MRD monitoring in MM- immediate and simultaneous sample QC -
7.5% of samples not suited for MRD in multicenter (international) trials
18
International Myeloma Foundation
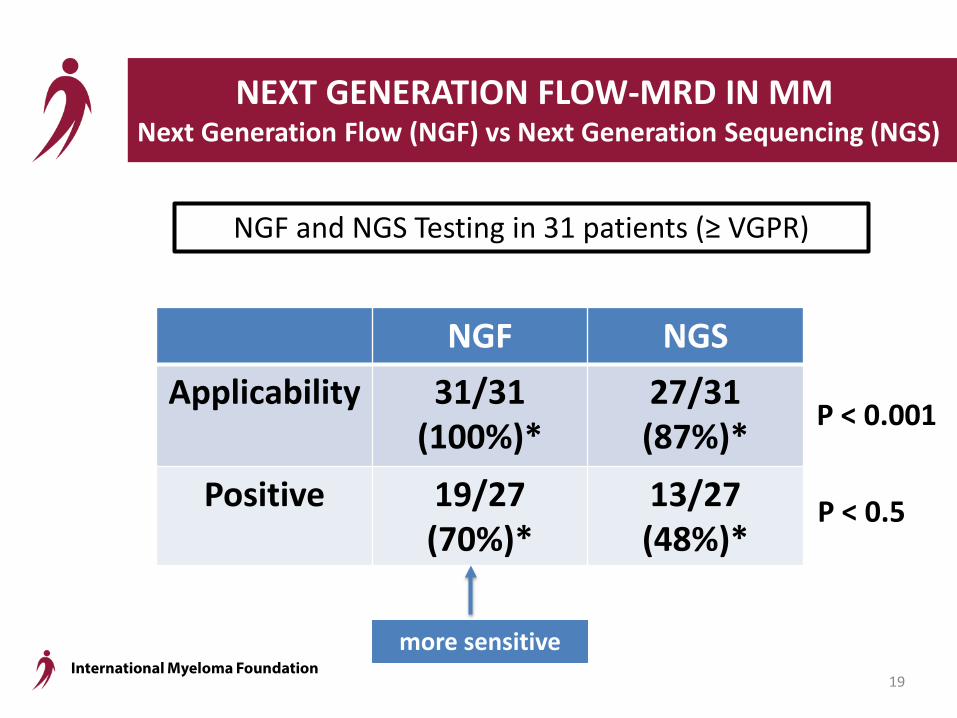
NEXT GENERATION FLOW-MRD IN MM Next Generation Flow (NGF) vs Next Generation Sequencing (NGS)
19
NGF and NGS Testing in 31 patients (≥ VGPR)
P < 0.001
P < 0.5
NGF NGSApplicability 31/31
(100%)*27/31 (87%)*
Positive 19/27 (70%)*
13/27 (48%)*
more sensitive
International Myeloma Foundation
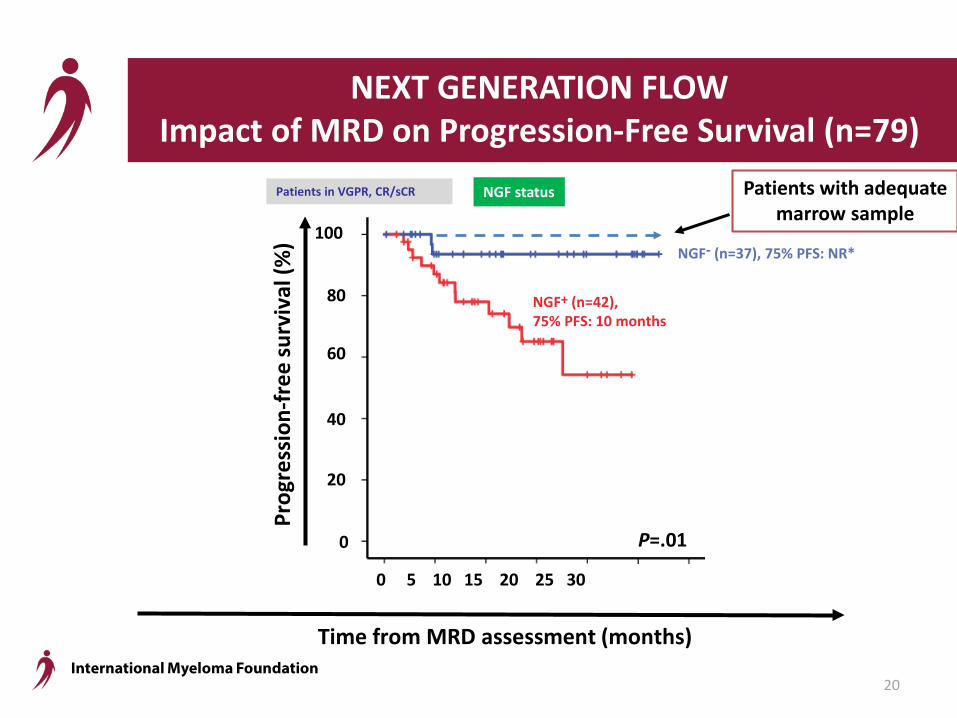
NEXT GENERATION FLOW Impact of MRD on Progression-Free Survival (n=79)
80
100
60
20
40
0
Prog
ress
ion-
free
surv
ival
(%)
Time from MRD assessment (months)
P=.01
NGF- (n=37), 75% PFS: NR*
NGF+ (n=42),75% PFS: 10 months
0 5 10 15 20 25 30
Patients in VGPR, CR/sCR NGF status
20
Patients with adequate marrow sample

International Myeloma Foundation
Induction Consolidation Maintenance
GEM 2017: New protocol to evaluate MRD
(except Dara arm)
DR
DR
21
VMP/ Rd
KRd +/- Dara
International Myeloma Foundation
How should MRD testing be used?
Y• To assess MRD –• To study and further treat MRD +
W• Is it too soon?
or• Can be used with careful patient
education?
22
In clinical trials: throughout the disease
In clinical practice
International Myeloma Foundation
POLLUX and CASTOR lead the way!
23
Dara combinations
Game Changer?

International Myeloma Foundation
Early Relapse: Lenalidomide-based StudiesPOLLUX
DRd vs Rd
PFS HR (95% CI)
0.37 (0.27-0.52)
ORR 93%
≥VGPR 76%
≥CR 43%
Duration of response, mo NE
OS HR (95% CI)
0.64(0.40-1.01)
ASPIREKRd vs Rd1
ELOQUENT-2ERd vs Rd2,3
TOURMALINE-MM1NRd vs Rd4
0.69 (0.57-0.83)
0.73 (0.60-0.89)
0.74 (0.59-0.94)
87% 79% 78%
70% 33% 48%
32% 4% 14%
28.6 20.7 20.5
0.79(0.63-0.99)
0.77 (0.61-0.97) NE
1. Stewart AK, et al. N Engl J Med. 2015;372(2):142-152.2. Lonial S, et al. N Engl J Med. 2015;373(7):621-631.3. Dimopoulos MA, et al. Blood. 2015;126(23):Abstract 28. 4. Moreau P, et al. N Engl J Med. 2016;374(17):1621-1634.
Dimopoulos M, et al. EHA 2013. Abstract LB2238.
24

International Myeloma Foundation
Early Relapse: PI-Based Studies
1. Dimopoulos MA, et al. Lancet Oncol. 2016;17(1):27-38.2. San-Miguel JF, et al. Lancet Oncol. 2014;15(11):1195-1206.3. San-Miguel JF, et al. Blood. 2015;126(23):Abstract 3026.4. Jakubowiak A, et al. Blood. 2016. Epub ahead of print.
Palumbo et al. Presented at ASCO 2016 (Abstract LBA4), oral presentation
DaratumumabDVd vs Vd
PFS HR (95% CI) 0.39 (0.28-0.53)
PFS Median mo NE
>VGPR 59%
>CR 19%
Duration of response, mo NE
OS HR (95% CI) 0.77 (0.47, 1.26)
CarfilzomibKd vs Vd1
PanobinostatPVd vs Vd2,3
ElotuzumabEVd vs Vd4
0.53 (0.44-0.65)
0.63 (0.52-0.76)
0.72 (0.59-0.88)
18.7 12.0 9.7
54% 28% 36%
13% 11% 4%
21.3 13.1 11.4
0.79 (0.58-1.08)
0.94 (0.78-1.14)
0.61 (0.32-1.15)
25

International Myeloma Foundation
Daratumumab-Revlimid-Dex(DRd)
Not refractory to Lenalidomide* Refractory to Lenalidomide
*Relapse occurring while off all therapy, or while on small doses of single-agent lenalidomide, or on bortezomibmaintenance
*Consider salvage auto transplant in eligible patients
Treatment of First Relapse*
Daratumumab-Velcade-Dex (DVd), orCyBorD
Derived from: msmart.org; Rajkumar SV, Kyle RA. Progress in Myeloma: A Monoclonal Breakthrough. N Engl J Med 2016;375:1390-1392
msmart.org
26

International Myeloma Foundation
CyBorDDRd, DVd
First Relapse Options
Ixazomib-RdElotuzumab-Rd
Other Dara-based regimensPanobinostat-Bortez-Dex
Additional Options
Derived from: msmart.org
Second or higher relapse
27
International Myeloma Foundation
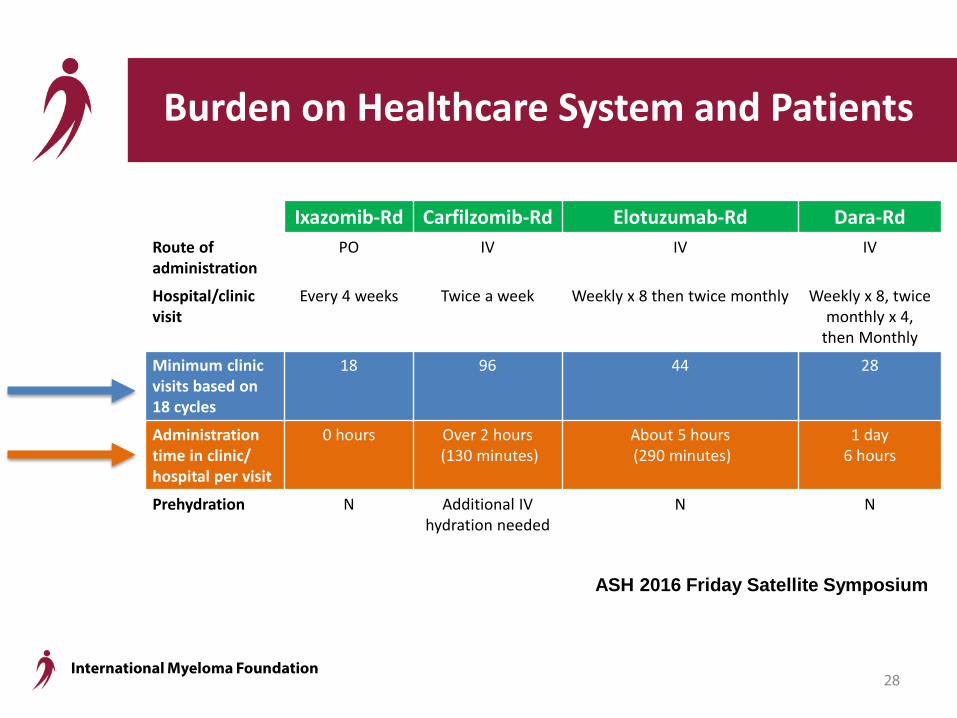
Burden on Healthcare System and Patients
Ixazomib-Rd Carfilzomib-Rd Elotuzumab-Rd Dara-Rd Route of administration
PO IV IV IV
Hospital/clinic visit
Every 4 weeks Twice a week Weekly x 8 then twice monthly Weekly x 8, twice monthly x 4,
then Monthly
Minimum clinic visits based on 18 cycles
18 96 44 28
Administration time in clinic/ hospital per visit
0 hours Over 2 hours(130 minutes)
About 5 hours(290 minutes)
1 day6 hours
Prehydration N Additional IV hydration needed
N N
ASH 2016 Friday Satellite Symposium
28

International Myeloma Foundation
How do you prioritize choices at first relapse?
• Efficacy• Toxicity• Ease of administration• Costs/ Reimbursement• To achieve MAXIMUM RESPONSE
29

International Myeloma Foundation
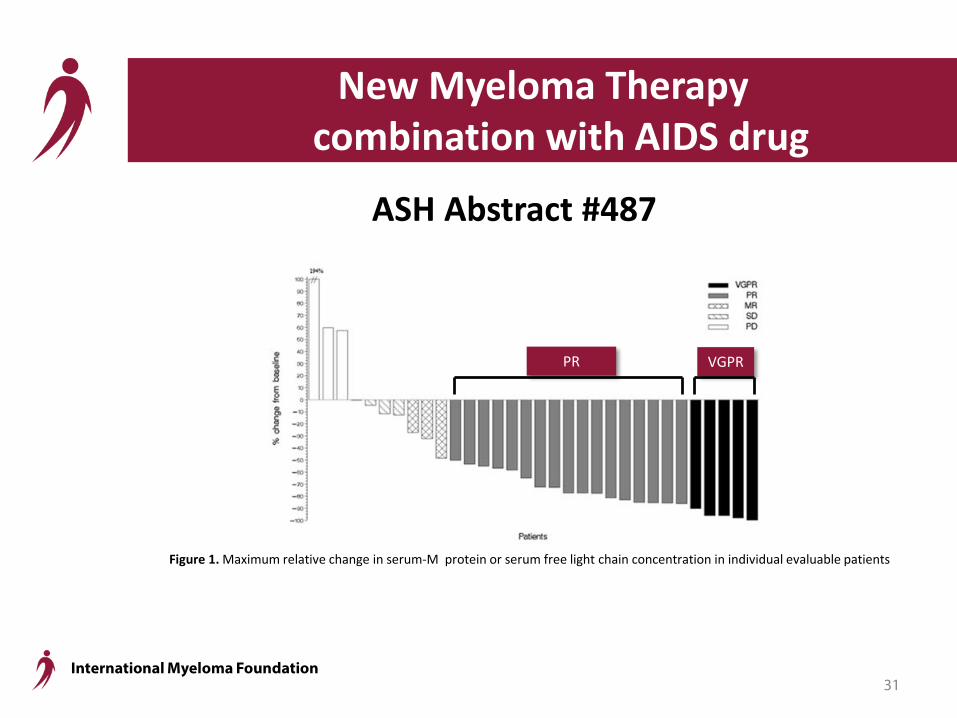
New Myeloma Therapy combination with AIDS drug
St. Gallen, Switzerland team 34 patients; resistant to Velcade® Nelfinavir (NFV) ; oral; overcomes Velcade® resistance Combo = NFV + Velcade/ Dex; well tolerated Relapse/ Refractory patients ORR (PR or better) = 65%
ASH Abstract #487: AIDS Drug
30
International Myeloma Foundation
New Myeloma Therapy combination with AIDS drug
ASH Abstract #487
Figure 1. Maximum relative change in serum-M protein or serum free light chain concentration in individual evaluable patients
PR VGPR
31

International Myeloma Foundation
Venetoclax: BCL-2 Inhibitor Therapy
Shaji Kumar; AbbVie Inc. (Genentech) study 66 patients; relapse/ refractory disease Acceptable safety profile
ASH Abstract #488: BCL-2 Inhibitor
t(11;14)
40%
32

International Myeloma Foundation
Venetoclax + bortezomib/ dex in Relapse/ Refractory Myeloma
Philippe Moreau; AbbVie Inc. (Genentech) study 66 patients; relapse/ refractory disease
ASH Abstract #975: BCL-2 Inhibitor Combo
33

International Myeloma Foundation
Selinexor/ Dex in Relapse/ Refractory Myeloma
Dan Vogl: Karyopharm 79 patients: 48 – quad (4) refractory: Rev/ Pom/ Velcade/ Kyprolis 31 – penta (5) refractory: + dara “unmet need group”
ORR (≥ partial response) = 21% (quad); 20% (penta) Median DOR = 5 months
OS = 9.3 months Main toxicities: platelets ; GI ; fatigue
ASH Abstract #491: Anti-oncogene “export” inhibitor
“STORM” Trial
34

International Myeloma Foundation
Selinexor/ Velcade/ Dex Combo
Bahlis; Karyopharm 22 patients; PI refractory; well tolerated
ASH Abstract #977
Table 1: Best Response by Prior Proteasome Inhibitor (PI) Treatment Status
7 (58%)
“STOMP” Trial
Also, Abstract #330: Selinexor/ Pom/ dexAbstract #973: Selinexor/ Car/ dex
35

International Myeloma Foundation
Anti-CD19 CAR-T Cell Therapy
U Penn Team 10 patients treated; post-ASCT; safe
ASH Abstract #974
3long
VGPRs
36
International Myeloma Foundation
What are the most exciting new/evolving therapies?
• NFV combo• Venetoclax• Selinexor• CAR-T: CD19/ BCMA• Checkpoint inhibitors• Virotherapy• Other
37

International Myeloma Foundation
OPEN DISCUSSION
FINAL THOUGHTS
What are the most exciting new/evolving therapies?
38

International Myeloma Foundation
Thank you to our sponsors!
39





























