Embed Size (px)
Citation preview

By samir ali2014_2015

Surgical Incisions and Flaps
2
The following fundamental rules apply to every surgicalprocedure, concerning the incision and flap:
1_The incision must be carried out with a firm,
continuousstroke, not interrupted strokes. During theincision, the scalpel should be in constant contactwith bone. Repeated strokes at the same place, manytimes, impair wound healing
2_Flap design and incision should be carried out in
such a way that injury of anatomic structures isavoided

3
3_Vertical releasing incisions should begin approximatelyat the buccal vestibule and end at the interdentalpapillae of the gingiva.
4_Envelope incisions and semilunar incisions, whichare used in apicoectomies and removal of root tips,must be at least 0.5 cm from the gingival sulcus.
5_The elliptic incision, which is used for the excision of various soft tissue lesions, comprises two convex
incisions joined at an acute angle at each end, whilethe depth of the incision is such that there is no tensionwhen the wound margins are coapted and sutured.

4
6_ The width of the flap must be adequate, so that theoperative field is easily accessible, without creatingtension and trauma during manipulation
7_The base of the flap must be broader than the free gingival margin, to ensure adequate blood supply and to promote healing.
8_ The flap itself must be larger than the bone deficitso that the flap margins, when sutured, are restingon intact, healthy bone and not over missing or unhealthybone, thus preventing flap dehiscence andtearing
5
9_The mucosa and periosteum must be reflected together.This is achieved (after a deep incision) whenthe elevator is continuously kept and pressed firmlyagainst the bone.
10_When the incision is not made along the gingival
sulcus, for esthetic reasons, and especially in peoplewith broad smiles,
11_During the surgical procedure, excessive pulling
and crushing or folding of the flap must be avoided,because the blood supply is compromised and healingis delayed.

Types of Flapsbased mainly upon shape
1_Trapezoidal FlapThe trapezoidal flap is created after a _ ∏shaped incision,which is formed by a horizontal incision alongthe gingivae, and two oblique vertical releasing incisionsextending to the buccal vestibule. The verticalreleasing incisions always extend to the interdental papillaand never to the center of the labial or buccal surface
of the tooth
6

This ensures the integrity of the gingivaproper, because if the incision were to begin at thecenter of the tooth, contraction after healing wouldleave the cervical area of the tooth exposed
7

The trapezoidal flap is suitable forextensive surgical procedures, especially when the triangularflap would not provide adequate access.
8

.
The fact that the base of the
resulting flap is broader than its free gingival margin
ensures the necessary adequate blood supply for the
healing process
9

.
Trapezoidal flap. a Diagrammatic illustration
b. Clinical photograph
10
.
Advantages.
Provides excellent access, allows surgery
to be performed on more than one or two teeth,
produces no tension in the tissues, allows easy reapproximation
of the flap to its original position and
hastens the healing process.
Disadvantages.
Produces a defect in the attached
gingiva (recession of gingiva).
11
2_Triangular FlapThis flap is the result of an L-shaped incision
with a horizontal incision made along
the gingival sulcus and a vertical or oblique incision.
The vertical incision begins approximately at the vestibular
fold and extends to the interdental papilla of the
gingiva.
12

Triangular flap
a Diagrammatic illustration b Clinical photograph.
Triangular flap
13

The triangular flap is performed labially orbuccally on both jaws and is indicated in the surgicalremoval of root tips, small cysts, and apicoectomies.
#apicoectomies.a surgical procedure to remove the end of a tooth root in endodontic therapy.
14
Advantages.Ensures an adequate blood supply, satisfactory
visualization, very good stability and reapproximation;it is easily modified with a small releasingincision, or an additional vertical incision, or evenlengthening of the horizontal incision.
Disadvantages.Limited access to long roots, tension
is created when the flap is held with a retractor, and itcauses a defect in the attached gingiva.
15

3_Envelope Flap
This type of flap is the result of an extended horizontal incision along the cervical lines of the teeth. The incision is made in the gingival sulcus and extends along four or five teeth. The tissue connected to the cervical lines of these teeth and the interdental papillae is thus freed. T
16

Single-sided (envelope) flap created by a single
horizontal incision along the cervical lines of the teeth.
a Diagrammatic illustration (buccal). b Clinical photograph
17

The envelope flap is usedfor surgery of incisors, premolars and molars, onthe labial or buccal and palatal or lingual surfaceand is usually indicated when the surgicalprocedure involves the cervical lines of the teeth
labially (or buccally) and palatally (or lingually), apicoectomy(palatal root), removal of impacted teeth,cysts,
18

Advantages. Avoidance of vertical incision and easy reapproximation to original position.
Disadvantages. Difficult reflection (mainly palatally), great tension with a risk of the ends tearing, limited visualization in apicoectomies, limited access, possibility of injury of palatal vessels and nerves, defect of attached gingiva.
19

4_Semilunar FlapThis flap is the result of a curved incision, which beginsjust beneath the vestibular fold and has a bowshapedcourse with the convex part towards the attachedgingiva The lowest point of theincision must be at least 0.5 cm from the gingival margin,so that the blood supply is not compromised. Eachend of the incision must extend at least one tooth overon each side of the area of bone removal.
20

Semilunar flap. a Diagrammatic illustration. b Clinical photograph
21

The semilunarflap is used in apicoectomies and removal of smallcysts and root tips.
22

Advantages. Small incision and easy reflection, norecession of gingivae around the prosthetic restoration,no intervention at the periodontium, easier oralhygiene compared to other types of flaps.
Disadvantages.Possibility of the incision being performedright over the bone lesion due to miscalculation,scarring mainly in the anterior area, difficulty of
reapproximation and suturing due to absence of specific reference points, limited access and visualization tendency to tear 23

4_Pedicle Flaps
The three main types of pedicle flaps used for closureof an oroantral communication are: buccal, palatal,and bridge flaps.
A_Buccal FlapThis is a typical trapezoidal flap createdbuccally, corresponding to the area which is to be covered,and is usually used on dentulous patients. It isthe result of two oblique incisions that diverge upwards,and extend as far as the tooth socket
24

After creating the flap, the periosteum is incised transversally,making it more elastic so that it may coverthe orifice that results from the tooth extraction. Theoblique buccal flap is a variation of the buccal flap. It isthe result of an anteroposterior incision, so that its baseis perpendicular to the buccal area, posterior to thewound. The flap is rotated about 70°–80° and is placedover the socket. Both cases require that, before placingthe flap, the wound margins must be debrided.
25

Pedicle flaps. a Buccal. b Palatal. These techniquesare suitable for closure of oroantral communication
26

B_ Palatal Flap. This type of flap is used in edentulouspatients so that the vestibular depth is maintained
The resulting palatal mucoperiosteal flap is rotatedposteriorly and buccally, always including the vesselsthat emerge from the corresponding greater palatineforamen After rotation, the flap is placedover the orifice of the socket, the wound margins aredebrided, and the flap is sutured with the buccal tissues.A gingival dressing is applied for a few days atthe void created and healing is achieved by secondaryintention.
27

C_Pedicle Bridge Flap. This flap is palatobuccal and is perpendicular to the alveolar ridge After creation, the flap is rotated posteriorly or anteriorly, to cover the orifice of the oroantral communication,without compromising the vestibular fold. This typeof flap is used only on edentulous parts of the alveolarridge.
28

. Pedicle bridge flap, used for closure of oroantralcommunication 29

Other Types of FlapsOther types of flaps are the result of a - shaped andAn - shaped incision. These flaps are used in surgicalprocedures of the palate, mainly for the removal ofexostoses (torus palatinus).
Flap Resulting from - shaped Incision. An incisionis made along the midline of the palate, as well as twoanterolateral incisions, which are anterior to the caninesThis type of flap is indicated insurgical procedures involving the removal of smallexostoses.
30
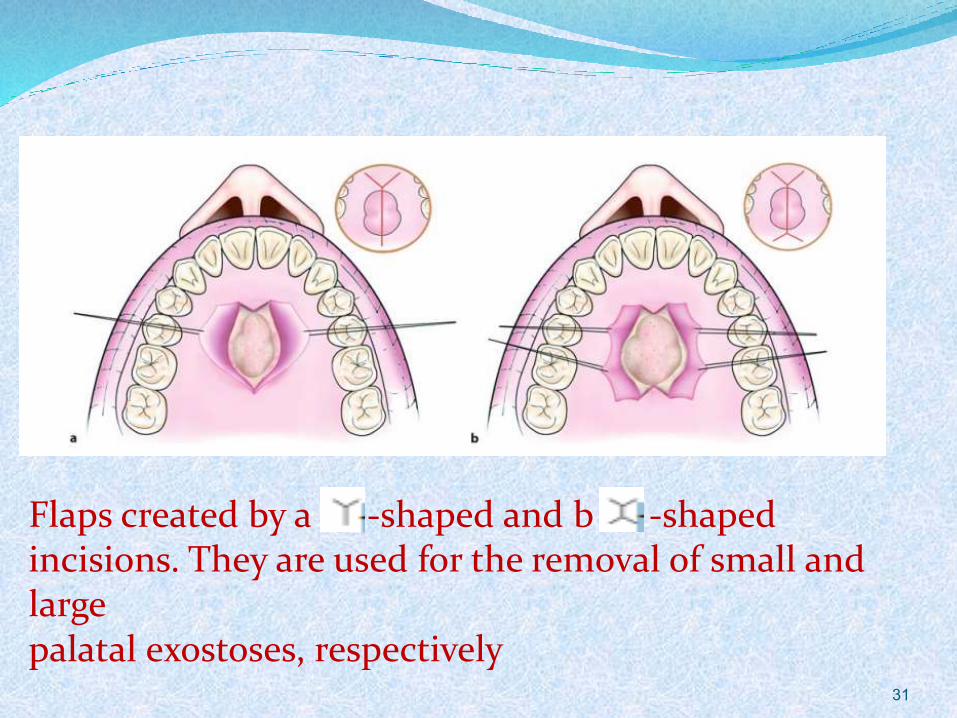
Flaps created by a -shaped and b -shaped incisions. They are used for the removal of small and largepalatal exostoses, respectively
31

Flap Resulting from -shaped Incision.
This type of flap is used in larger exostoses, and is basically an extension of the -shaped incision (Fig. 3.13 b). The difference is that two more posterolateral incisions aremade, which are necessary for adequate access to thesurgical field. This flap is designed such that majorbranches of the greater palatine artery are not severed
32

33
Reflection of the MucoperiosteumReflection is performed to separate the mucoperiostealflap from the underlying bone. The elevator is indirect contact with bone and reflection starts at theincision, usually at an angle and is completedwith gentle, steady strokes towards the labial orbuccal vestibule, without damaging the tissues. Whenthe attachment between bone and periosteum is strongor if symphysis occurs, then scissors or surgical bladesmay be used.

34
Reflection of the mucoperiosteal flap after incision,with a periosteal elevator, which usually starts fromthe corner of the horizontal-vertical flap