Embed Size (px)
Citation preview

Dr PS Deb, DM
Hyperacute Management of Stroke

Normal flow, normal function
Synaptic transmission failure
Membrane pump failure
20
50
10
0
Time in hours
CB
F (
ml/1
00g
brai
n)
Low flow, raised O2 extraction, normal function
1 2 3 4 5

NA, Dopamine
Ca2+ i é
Ischaemia - 02 ê glucose ê
Anoxic depolarisation
é lactate
Glutamate
Hi é Free Fe2+
Free radicals
Lipolysis NO synthase
Proteolysis
Ischaemic Brain Injury

Aim of Rx: Ischemic Stroke
1. ReperfusionA. Thrombolysis
B. Mechanical disruption of clot
2. Reducing the size of infarctA. Antiplatelate
B. Anticoagulant
C. Neuro-protection
D. Blood pressure control
3. Treat associated complicationA. Raised ICT
B. Seizure

Thrombolysis in acute stroke
Within 3-4.5 hour of Stroke No occlusion
Medium Vessel
IV rTPA/URK
Large Vessel
IA rTPA/URK
Stop
C-D/ D-P mismatch

Challenge of thrombolysis
Lack of awareness: – Patient – Physician
Out of scope Operational issue
– Emergency team – Imaging team
Failure of medical thrombolysis Re-closure of opened vessel: (Stenting) Reperfusion injury with toxic edema and
hemorrhage

Overcoming challange
Education– Patient– Physician
Alternative approach in failed cases– Mechanical disruption of clot: Primary
angioplasty– Transcranial doppler and thrombolysis– Surgical emergency endarterectomy
Stenting to prevent reclosure

Blood pressure control
Systolic BP < 220 or diastolic < 120 – Observe unless other end-organ
involvement
Systolic BP > 220 or diastolic >120 – Labetalol 10-20 mg IV over 1-2 mins.
May repeat or double every 10 mins. (300 mg/d)
Diastolic BP > 140 – Nitroprusside 0.5mcg/kg/min IV infusion– *Aim for 10-15% reduction of BP
Systolic BP > 185 or diastolic > 110 For thrombolysis – Labetalol 10-20 mg IV over 1-2
mins. May repeat x 1
CBF
Mean systemic BP
60 160

Aspirin in Acute Stroke
Aspirin 325mg
Clopidogrel 75-150mg if Aspirin CI– Early recurrent ischemic stroke – 7 fewer per 1,000 treated
(p< 0.0001)– Death from any cause – 4 fewer per 1,000 treated (p=0.05)– Death or early recurrence of non-fatal stroke – 9 fewer per
1,000 treated (p=0.001)– Death or dependency at discharge or six months – 13 fewer
per 1,000 treated (p=0.007)– Hazard : Hemorrhagic stroke or transformation – 2 more
per 1,000 in ASA treated (p=0.06)
Bath, 2001b [A];
Chinese Acute Stroke Trial Collaborative Group, 1997 [A];
International Stroke Trial Collaborative Group, 1997 [A];
Sandercock, 1993 [M]).

Anticoagulant in Acute Stroke
Early use (<3Hr) may reduce mortality and morbidity. Hemorrhagic transformation is high Arterial dissection Cardioembolic infarct with or without AF
– Immediate for small infarct if re-embolization risk is high
– Delayed 2 weeks for all cases Heparin - 1000 units/hr. PTT 1.5 avoid bolus Enaoxaparin – 40mg SC BD Low dose Enoxaparin 40mg SC OD prophylactic for DVT

Other measures
Statins– Use after 2 days of onset
(AHA)– Continue in those already
taking (NHS)
Neuroprotection– Citicolin– Magnesium

Spontaneous Intra-cerebral Hemorrhage

Copyright ©1997 American Heart Association
Brott, T. et al. Sroke 1997;28:1-5
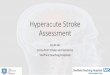
Early hemorrhage growth in patients with intracerebral hemorrhage.
• This 66-year-old white man with a baseline GCS score of 14 and NIH Stroke Scale score of 20 had a putaminal hemorrhage with a baseline ICH volume of 10 mL (top row)
• The ICH volume on the 1-hour CT was 27 mL (bottom row). However, the 17-mL increase in ICH volume was not accompanied by any change in the 1-hour GCS (14) and NIH Stroke Scale (20) scores.

Hematoma volume 30d outcome
Type ICH Vol. mL GCS Prognosis
I < 30 >9 Good
II <30 <8Fair30-60 >9
III 30-60 <8Poor>60 <8
(Joseph P. Broderick et al Stroke 1993;24:987-993)

Approach to Treatment of ICH
1.Stopping or slowing the initial bleedingA. Factor VIIa
B. Blood pressure control
2.Reducing raised ICT due to Hematoma and EdemaA. Evacuation of hematoma
B. Osmotherapy
C. Neuroprotection
3.Control of Seizure and other associated complication

A. Factor VIIa Trial
Useful in Hemophilia with Ab to factor VII or IX Produce clotting by stimulating coagulation cascade in
normal Used in cased of ICH secondary to coagulopathy There is mild reduction in progression of hematoma,
morbidity and mortality (Phase II, III trial) INR may return to normal transiently it require repeated
dose Routine use in Primary ICH remains investigational

B. Blood Pressure control
Hypertension is common during early states of ICH -> Expansion, Peri-hematoma edema and re-bleeding
A systolic BP above 140 to 150 mm Hg within 12 hours of ICH is associated with more than double the risk of subsequent death or dependency.
Association of low BP and deterioration is not consistent like ischemic stroke.
Blood pressure
Antihypertensive Treatment in Acute Cerebral Hemorrhage (ATACH- I)INTensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT- I)

Recommendation: AHA 2010
In patients presenting with a systolic BP of 150 to 220 mm Hg, acute lowering of systolic BP to 140 mm Hg is probably safe
Class IIa; Level of Evidence: B

Raised ICT
The Monro-Kellie doctrine

Problem secondary to raised ICT
1. Early hematoma expansion and secondary edema-induced brain compression and consequent neuronal death;
2. Cytotoxic (intracellular) and vasogenic (extracellular) edema resulting from disruption of the blood–brain barrier;
3. Reductions in cerebral perfusion pressure (CPP) from mass effect and raised intracranial pressure (ICP);
4. Brain herniation

Approach to raised ICT
Head end elevation Surgical evacuation of
hematoma Osmotherapy Hyperventilation Analgesia and
sedation Neuromuscular block
Barbiturate coma Hypothermia Corticosteroid CSF drainage Defroxamin

Head-of-Bed Elevation
Elevation of the head of the bed to 30° improves jugular venous outflow and lowers ICP.
The head should be midline, and head turning to either side should be avoided.
In patients who are hypovolemic, elevation of the head of the bed may be associated with a fall in blood pressure and an overall fall in CPP.

Principals of Osmo-therapy
1. Brain volume falls as long as there is an osmotic gradient between blood and brain.
2. Short lived action few hours.
3. Normal brain shrink (White/ Gray)
4. Rebound edema.
5. Dose not clear: 10 mOsm/L change in osmolality may be effective
6. Chronic use not recommended as brain adapt

Mannitol
Wise and Chater in 1962 Cleared from brain and CSF due to large molecular wt
(182Dalton), less rebound phenomenon. Rebound phenomenon with increasing dose to sustain
hyperosmolality of brain, as serum osmolality falls Dose:
– 1g/kg increases serum osmolality 20-30 mOsm/L for 3-4 hours.– Higher dose 1.5-2gm/kg lower CSF pressure for longer time with
increased rebound phenomenon. – Lower dose 0.5gm/kg has less rebound

Mannitol Use in Acute Stroke Case Fatality at 30 Days and 1 Year
In a tricenter, prospective study, 809 patient with ICH within 72 hours were analyzed 30-day and 1-year case fatality with respect to mannitol treatment in 2/3rd cases
No recommendations can be made on the use of mannitol in acute stroke. Stroke. 2003;34:1730-1735.

Mannitol in ICH
Mannitol 20% 100ml q6h within 6 days of ictus for 5 days, tapered in next 2 days Mannitol did not seem to be beneficial in patients with ICH
J Neurol Sci. 2005 Jul 15;234(1-2):41-5.
Died
Disabl
ed
Recov
ered
0
5
10
15
20
25
MannitolControl
MannitolControl
Randomized, controlled, double-blind study.

Effect of single mannitol bolus in intracerebral hemorrhage
CT scan >3cm midline shift in ICH Randomized with bolus dose of Mannitol /Saline. Superior sagittal sinus to pontomesencephalic junction
(SSS-PMJ) distance and edema hematoma complex were measured.
Mannitol led to transient clinical improvement in five patients without significant reduction in superior sagittal sinus to pontomesencephalic junction (SSS-PMJ) distance at 30 and 60 min.
U. K. Misra et al Department of Neurology, Sanjay Ghandi PGIMS, Lucknow, IndiaEur J Neurol. 2007 Oct;14(10):1118-23. Epub 2007 Aug 28.

Effect of mannitol on early enlargement of hematoma following hypertensive cerebral hemorrhage
Hypertensive cerebral hemorrhage cases were randomized – Group A 36 – Mannitol – Group B 35 – furosemide
Two follow-up CT were done Result: Enlargement of hematoma
– Group A : 33 3% patients(12 cases)– Group B: 17 1% patients(6 cases)
The inapt use of mannitol may be one reason of the early enlargement of hematoma following hyperten-sive cerebral hemorrhage
Wang Minzhong,Pang Zaiying,Feng Yabo,et al Manni-tol
Control0
2
4
6
8
10
12
14
Enlargement of Hematoma

Hypertonic Saline
Used in head injury and when Mannitol or Hyperventilation failed
No trial on stroke patient Abrupt change in serum osmolality may leads
– Coma,– Seizure and – Subdural hematoma– Pontine myelinolysis
Volume expansion– Cardiac failure
Altered coagulation parameters -> bleeding– Prolongation of PT, TT– Decreased platelet aggregation
Rebound phenomenon

Recommendation: Raised ICT
Conservative– An elevation of the head of the bed – Analgesia and sedation
Aggressive therapies – Osmotic diuretics (mannitol and hypertonic saline solution), – Drainage of CSF via ventricular catheter, – Neuromuscular blockade, – Hyperventilation, generally require concomitant monitoring of ICP and
blood pressure with a goal to maintain CPP >70 mm Hg
Class IIa, Level of Evidence B

Seizure and Antiepileptic drugs
Incidence at onset -> 2 weeks: 3-17% Electrographic seizure 28-31% (on AET) One study prophylactic AE reduce clinical Sz. after Lobar
hematoma Prospective population based studies did not show clinical
Sz and worsened neurological outcome or mortality. Subclinical Sz.: one study showed prophylactic PHY
increased disability and death at 90 days.

Recommendation: Seizure control
Clinical seizures should be treated with antiepileptic drugs Class I; Level of Evidence: A
Continuous EEG monitoring in patients with depressed mental status out of proportion to the degree of brain injury
Class IIa; Level of Evidence: B
Patients with a change in mental status who are found to have electrographic seizures on EEG should be treated with antiepileptic drugs
Class I; Level of Evidence: C
Prophylactic anticonvulsant medication should not be used Class III; Level of Evidence:B

Summary - ICH Rx
Blood pressure control remains the mainstay of management in hemorrhagic stroke
Osmotherapy has doubtful role and routine use is not indicated in minor bleed.
Clinical and subclinical seizure with EEG abnormality should be treated.
Surgical evacuation of hematoma and Supportive and critical care of patient during acute state is
most important to reduce morbidity and mortality