Embed Size (px)
Citation preview

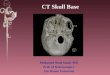
Skull Base Imaging
24-5-20169.21 pm

Great teachers – All this is their work . I am just the reader of their
books .Prof. Paolo castelnuovo
Prof. Aldo Stamm Prof. Mario Sanna
Prof. Magnan

For Other powerpoint presentatioins of
“ Skull base 360° ”I will update continuosly with date tag at the end as
I am getting more & more information
click
www.skullbase360.in - you have to login to slideshare.net with
Facebook account after clicking www.skullbase360.in

Dr.Prahlad sir https://www.facebook.com/prahlada?fref=tsskull base imaging lecture
Click link for skull base imaging video = https://www.youtube.com/watch?v=HYYB-8pv7k4&feature=youtu.be

Popular videos of skull base imaging in youtube
https://www.youtube.com/playlist?list=PLxfT3LHUjLuJD3JsWQU4vL
h4X5f_5OD0g

• In book of Mario sanna – “Microsurgery of paragangliomas” given – “ Radiological Anatomy ” in 3rd chapter – click https://books.google.co.in/books?id=7k_jwKyT6d0C&lpg=PP1&dq=mario%20sanna%20paraganglioma&pg=PP101#v=snippet&q=Radiological%20Anatomy&f=false


Content
• Normal skull base anatomy
• Pathology intrinsic to skull base – some case examples
• Pathology affecting skull base from below – some case examples
• A few hints and tips!

Anatomy
Five Bones:
• Ethmoid - CP• Sphenoid-
GW+LW• Occipital• Temporal- paired• Frontal-paired

Cranial Fossae
• Anterior
• Middle
• Posterior

Anterior Cranial Fossa• Anterior
• Frontal bone: frontal sinus,supra-orbital foramen
• Posterior• Post. edge of lesser
wing sphenoid and its ant. Clinoid processes
– Intracranial landmarks: foramen ceacum, crista galli, cribiform plate, planum sphenoidal
– Extracranial landmarks: nasal cavity, ethmoid and sphenoid sinuses, orbits

Middle Cranial Fossa
• Anterior• Posterior edge of lesser
wing of sphenoid
• Posterior• Post-sup edge of
petrous temporal bone

Posterior Cranial Fossa• Anteriorly
– Post-sup edge of petrous temporal bone
• Posteriorly– it is enclosed by the
occipital bone.• Laterally
– portions of the squamous temporal and mastoid part of the temporal bone form its walls.
• It contains the brainstem and cerebellum.

Skull Base Anatomy
Temporal Bone
Temporal bone- petrous portion
Sphenoid Bone
Occipital Bone
Key Fissures
• Petro-sphenoidal fissure
• Petro-occipital fissure
Key Sutures
• Sphenosquamous Suture
• Occipitomastoid Suture

Skull base foramina

FORAMEN OVALE
FORAMEN SPINOSUM

CAROTID CANAL
JUGULAR FORAMEN

IACINTERNAL AUDITORY CANAL
CAROTID CANAL
OSSICLES
MALLEUS
INCUS

Skull Base Anatomy

Skull Base Anatomy
Foramen spinosum
Sphenoid spine- lower level
Foramen rotundum- higher level
Pterygopalatine fossa
Foramen ovale
Petro-occipital fissure
Pterygoid canal
f. lacerum

Skull Base AnatomyForamen Spinosum• Middle meningeal artery/vein
• CV V3, recurrent branch
• Lesser superficial petrosal nerve
Foramen Ovale• CN V3
• Lesser petrosal nerve
• Accessory meningeal artery
• Emissary veins

Skull Base Anatomy
Foramen Lacerum• Ascending pharyngeal artery- meningeal branch
• Nerve of pterygoid canal
Vidian Canal • aka pterygoid canal
• Pterygopalatine fossa - foramen lacerum
• Vidian nerve
• Vidian artery

Skull Base Anatomy
Foramen rotundum• CN V2
• Artery of foramen rotundum
• Emissary veins

*
Skull Base Anatomy
Foramen magnum• Medulla oblongata
• Vertebral arteries
• Anterior/Posterior spinal arteries
Hypoglossal canal• CN XII
• Hypoglossal artery*

Skull Base Anatomy
Jugular Foramen• Pars nervosa: CN IX, inferior petrosal sinus
• Pars vascularis: CN X, XI, jugular bulb
*
* Carotid canal

Skull Base Anatomy
Pterygopalatine Fossa• Pterygopalatine ganglia V2
• Pterygopalatine plexus
• Communicates with:Inferior orbital fissure
Orbital apex
Sphenopalatine foramen
Pterygomaxilary fissure
Foramen rotundum
Vidian canal
Greater/lesser palatine canals and foramina

Receives: Superior opthalmic vein Inferior opthalmic vein Sphenoparietal sinus
Drains via: Petrosal sinuses Basilar plexus
Pterygoid plexus
Connection: Circular sinus
Contains: CN III, IV, V1, V2, VI
Skull Base Anatomy
Cavernous Sinus
Meckel’s Cave• Posterior aspect of cavernous sinus
• Gasserian ganglion (sensory root ganglion of CN V)

Skull Base AnatomySuperior Orbital Fissure• CN III, IV, V1, VI
• Middle meningeal artery- orbital branch
• Recurrent meningeal artery
• Superior opthalmic vein
Inferior Orbital Fissure• Infraorbital artery, vein, and nerve (V2 branch)
Optic Canal• Optic nerve
• Opthalmic artery

Orbital landmarks• Superior orbital fissure
• Optic canal
• Inferior orbital fissure – other end of foramen rotundum
• Ant. And Post. Ethmoidal foramina
• Anterior & Posterior ethmoidal arteries
• Foramina = constant guide to level of ethmoid roof as position of fronto-ethmoid suture.

Skull base Pathology
• Intra-axial – brain lesions/tumours
• Extra-axial – lesions from adjacent structures, usually from below skull base
• Metastatic eg breast, lung, prostate ca

Extra- axial pathology of anterior and middle cranial fossae
• Paranasal sinus Lesions
• Malignant: SCC, adenocarcinoma, sarcoma, melanoma, olfactory neuroblastoma, adenoid cystic, distant mets.
• Benign: mengioma juvenille nasopharyngeal angiofibroma, fibrous dysplasia, Inverting papilloma, fibro osseous disease

Paranasal sinus malignancy• Maxillary sinus carcinoma
• SCC commonest
• T4b- involvement of dura, brain, clivus, nasopharynx (inoperable)
• Multiplanar CT with contrast and MRI to fully assess – unilateral sinus mass with bony wall destruction (sinus wall is rarely expanded).
• MRI good for perineural, dural and intra cranial spread

Extra-axial pathology of posterior cranial fossa
• CPA lesions• Acoustic neuromas, meningioma’s, other
neuromas (rare eg VII nerve neuroma), epidermoids, glomus tumours, arachnoid cysts, haemangiomas
• Rare – mets, chordomas, chondrosarcoma, lipoma, dermoids, teratomas
• Petrous apex lesions• Cholesterol granuloma, cholesteatoma,
meningioma, asymmetric petrous( extra bone marrow – can be mistaken for neoplasm!), mucocele, petrous ICA aneurysm, giant cell tumour.

Intra-axial Pathology of skull base
• Brainstem – gliomas (commonest CPA tumour in children)
• Cerebellum/ brain – medulloblastomas, astrocytomas, haemangioblastomas
• Fourth ventricle – choroid plexus papillomas, ependymomas
Brainstem Glioma

Case 1

Chondrosarcoma
CT Findings:• Irregular, destructive mass
• Centered off midline
• Petro-occipital fissure
• Calcifications, 70%; “rings/arcs”
MRI Findings:• Low T1 signal, high T2 signal
• Enhance with contrast
• Scalloped, well circumscribed margins

ChondrosarcomaOrigin:• Preexisting cartilaginous lesion, synchondroses, cartilage endplates
Location:• Paranasal sinuses, skull base, parasellar region
• Long bones, pelvis, sternum, ribs
Clinical:• 45 yo, median age
• Classic, mesenchymal, or undifferentiated

Case 2

CT/MRI Findings:• Expansile lytic lesion, midline
• Well delineated mass arising from bone
• Large soft tissue component
• Variable calcification
• Anteroposterior extension
• Heterogeneous enhancement on T1, T2
• Dark on T1, bright on T2
Chordoma
Diff. Dx:• Chondroma
• Chondrosarcoma
• Clivus meningioma

ChordomaOrigin• Notochord remnants
Location• Clivus 35%
• Sacrum 50%, Vertebral bodies 15%
Clinical• age 30-70
• Slow growing, locally aggressive
• CN VI- CN deficits
• Mets late
• Tx: surgery, radiation

Case 3

Glomus Tumor
Glomus jugulare CT/MRI Findings:• Center: jugular foramen
• Limit: hyoid bone
• Enhance w/ contrast
• Salt and pepper appearance on MRI
• Bone erosion

Glomus Tumor
Origin:• Chemoreceptor cells
Location:• 10% multiple
• glomus jugulare: jugular bulb
• glomus tympanicum: cochlear promontory;
Clinical:• Pulsatile tinnitus
• Hearing loss
• arrythmia, BP fluctuation

Hints and tips!• MRI-Talk about signal intensity (low vs high)
• Marrow=hyper intense• Bone=hypointense• High flow blood vessels – black on MR
• MRI T1weighted• water=black• Fat=white• Look for CSF around spinal cord to see
• MRI T2 weighted• Water=white• Fat=black• Nodes show up brighter on T2 as cystic necrosis

Hints and tips - MRI• Lipomas signal suppresion on STIR
• Adenoid cystics – peri neural spread seen only after gadolinium contrast on T1 – makes them shine!
• Parapharyngeal space –Schwannomas and paragangliomas are behind carotid so push carotid antero-medially and up to skull base. Best seen on T1 after gadolinium
• Paragangliomas – look shaggy, light up quickly with contrast then wash out
• Schwannomas – look smooth and have delayed enhancement after contrast
Paraganglioma on T2
Lipoma at petrous apex

Hints and tips - MRI• Glomus Jugulare – slow
growing, shows irregular bone destruction
• Fibrous dysplasia – inhomogenous enhancement
• Meningioma – bright on T1 and light up with gadolinium, broad based and dural tail


For Other powerpoint presentatioins of
“ Skull base 360° ”I will update continuosly with date tag at the end as
I am getting more & more information
click
www.skullbase360.in - you have to login to slideshare.net with
Facebook account after clicking www.skullbase360.in