Embed Size (px)
Citation preview

Skull base for FESS surgeons
26-4- 20168.40 am
The purpose of this PPT is to have knowledge of skull base for FESS surgeons who wants to limit for FESS surgery
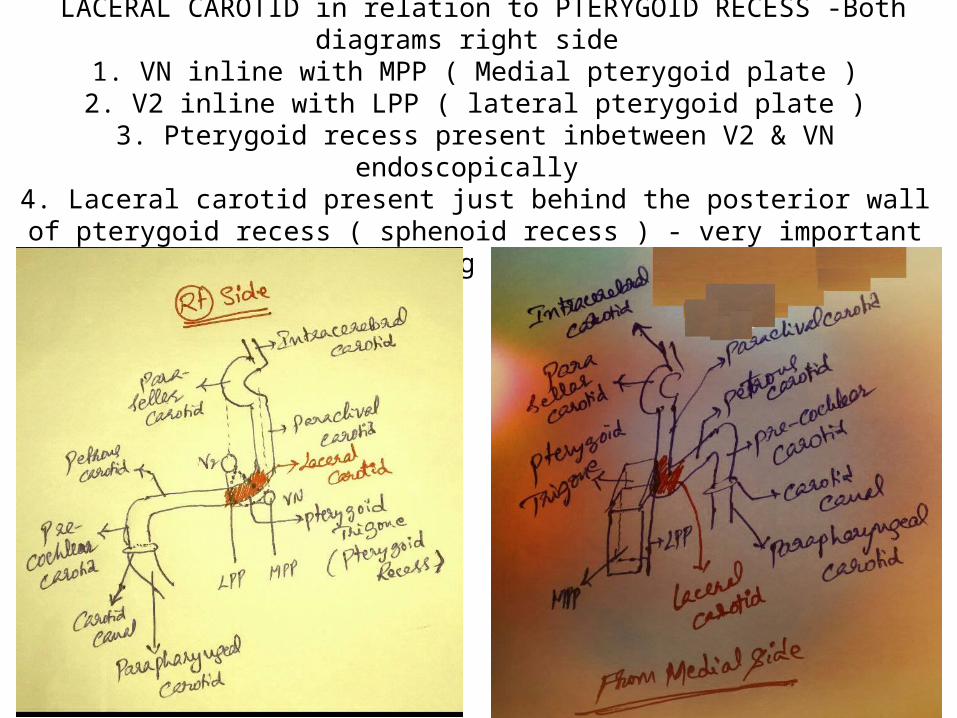
LACERAL CAROTID in relation to PTERYGOID RECESS -Both diagrams right side 1. VN inline with MPP ( Medial pterygoid plate )2. V2 inline with LPP ( lateral pterygoid plate )
3. Pterygoid recess present inbetween V2 & VN endoscopically 4. Laceral carotid present just behind the posterior wall of pterygoid recess
( sphenoid recess ) - very important vital structure in clearing pterygoid recess pathology
Pterygo-palatine fossa
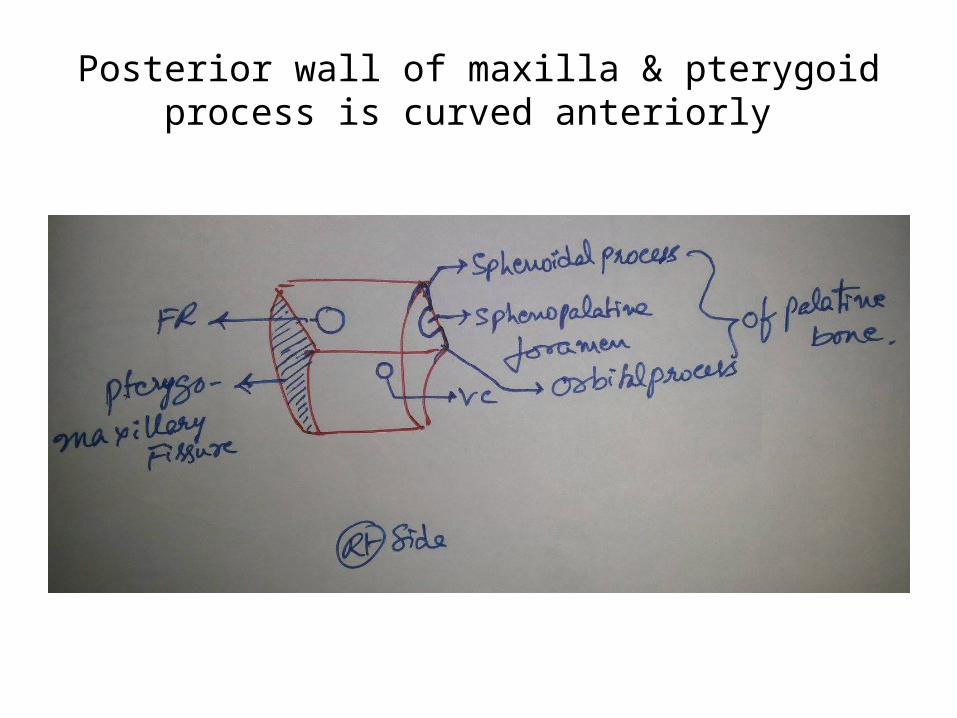
Posterior wall of maxilla & pterygoid process is curved anteriorly
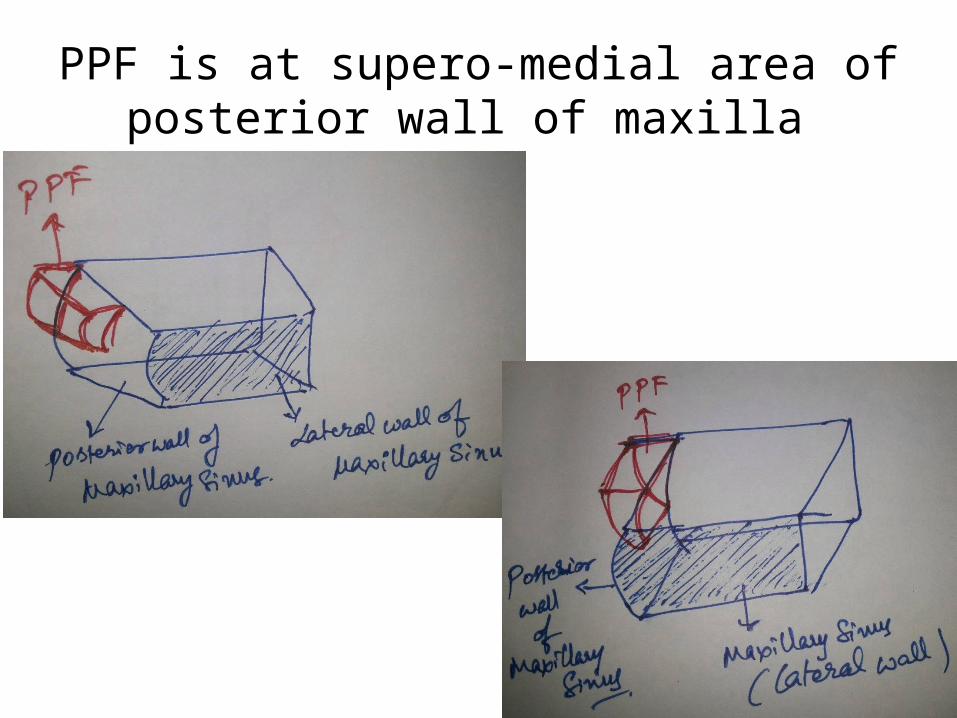
PPF is at supero-medial area of posterior wall of maxilla
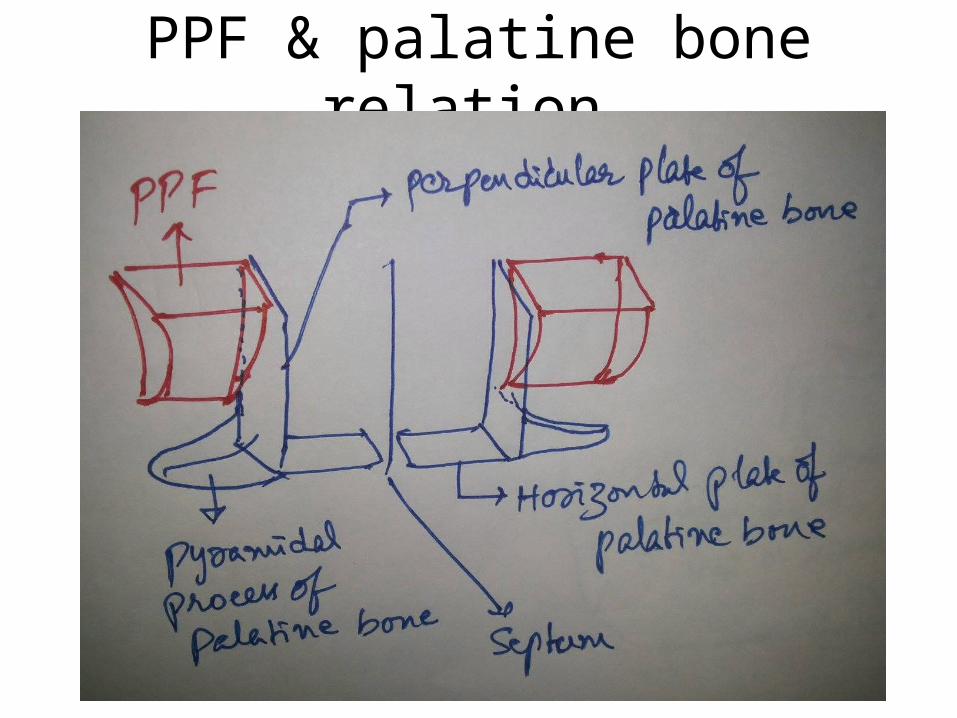
PPF & palatine bone relation
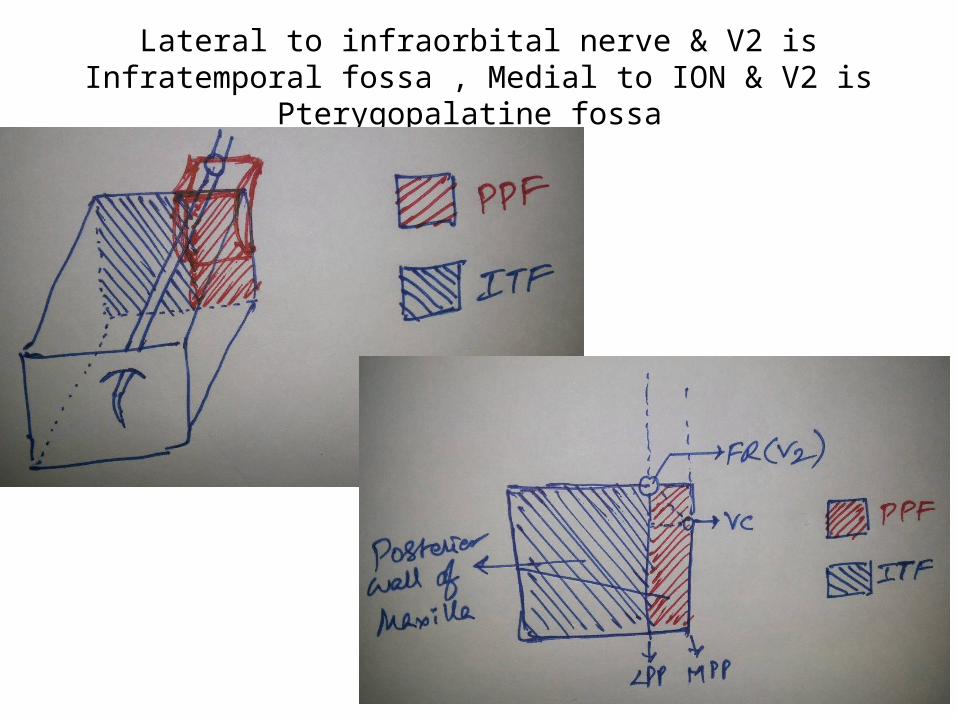
Lateral to infraorbital nerve & V2 is Infratemporal fossa , Medial to ION & V2 is Pterygopalatine fossa
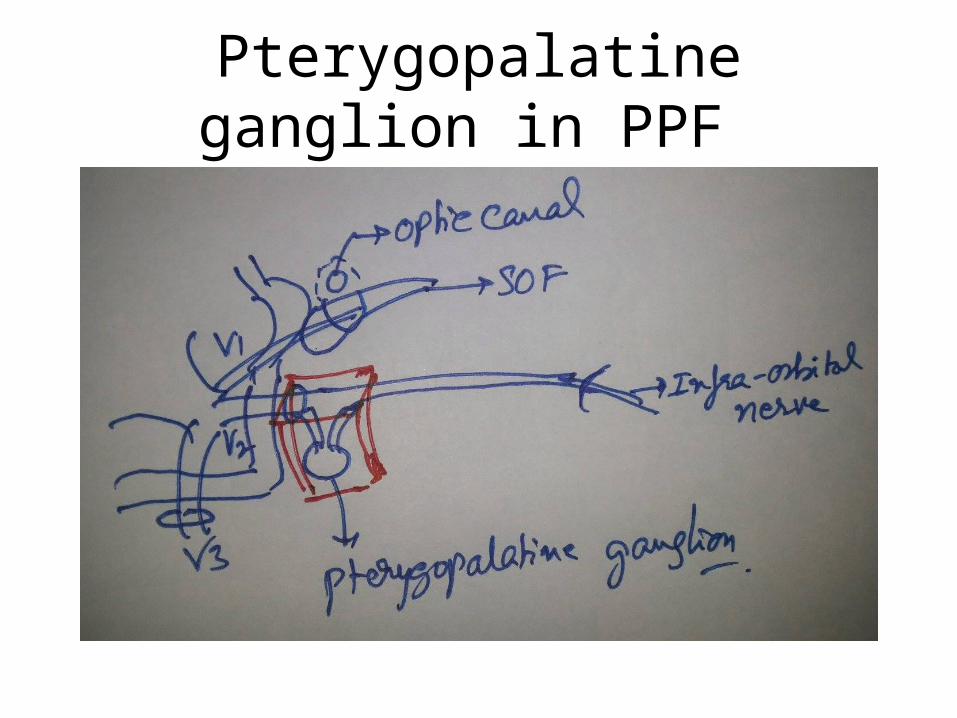
Pterygopalatine ganglion in PPF
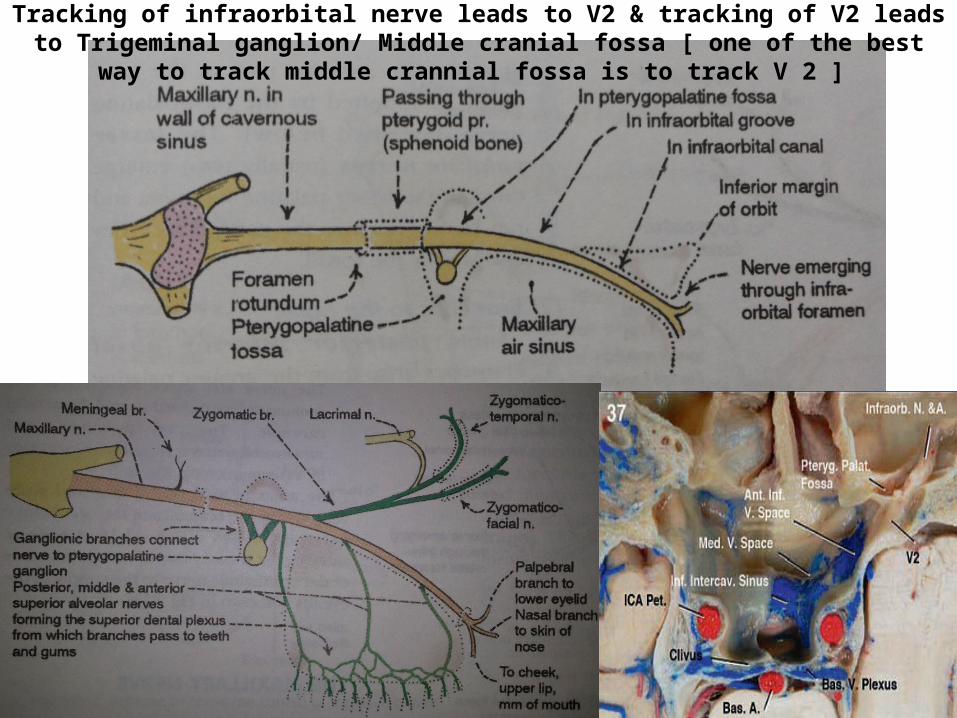
Tracking of infraorbital nerve leads to V2 & tracking of V2 leads to Trigeminal ganglion/ Middle cranial fossa [ one of the best way to track middle crannial fossa is to track V 2 ]
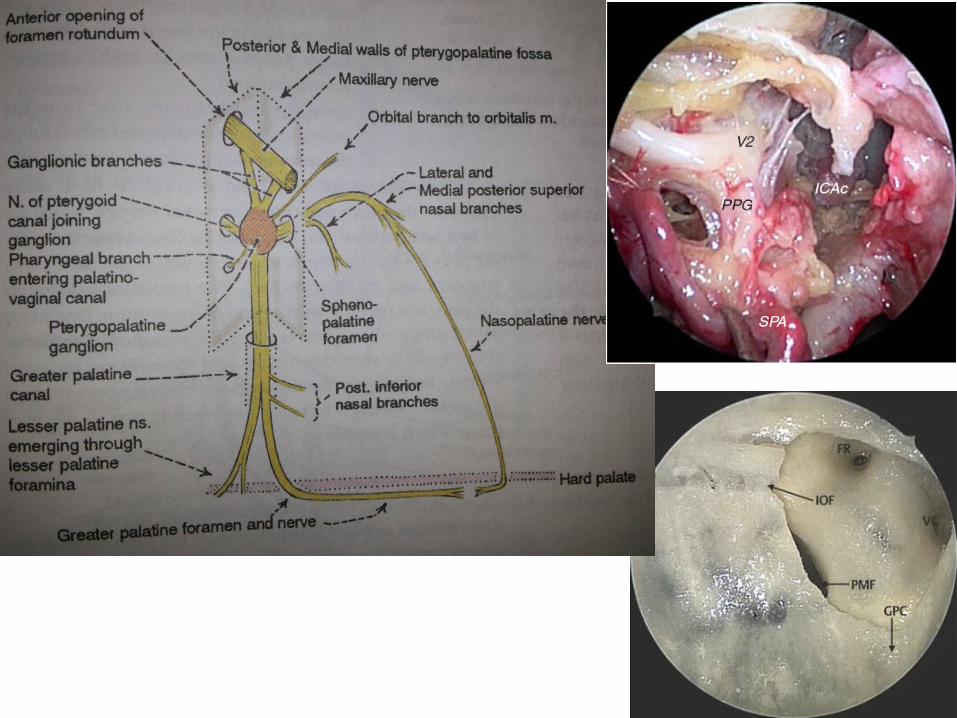
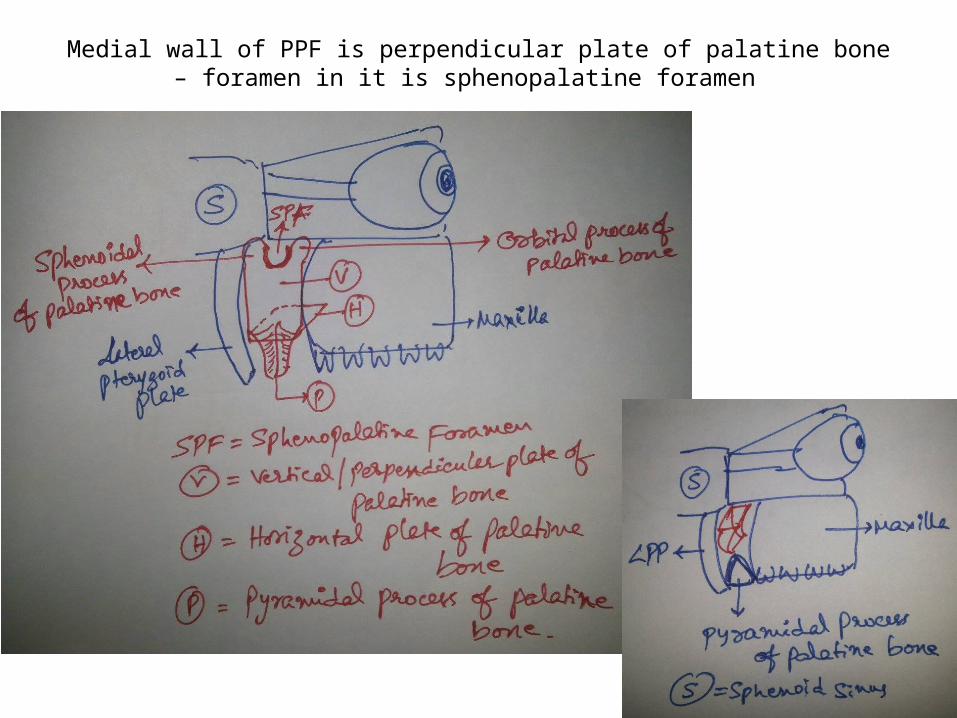
Medial wall of PPF is perpendicular plate of palatine bone – foramen in it is sphenopalatine foramen
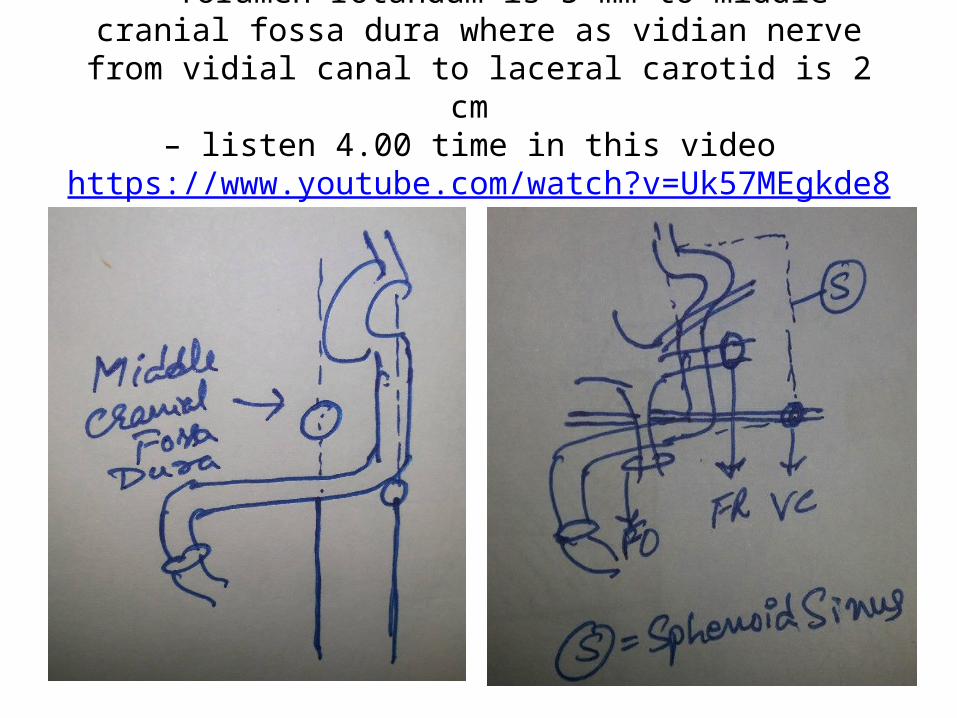
foramen rotandum is 5 mm to middle cranial fossa dura where as vidian nerve from vidial canal to laceral carotid is 2 cm
– listen 4.00 time in this video https://www.youtube.com/watch?v=Uk57MEgkde8
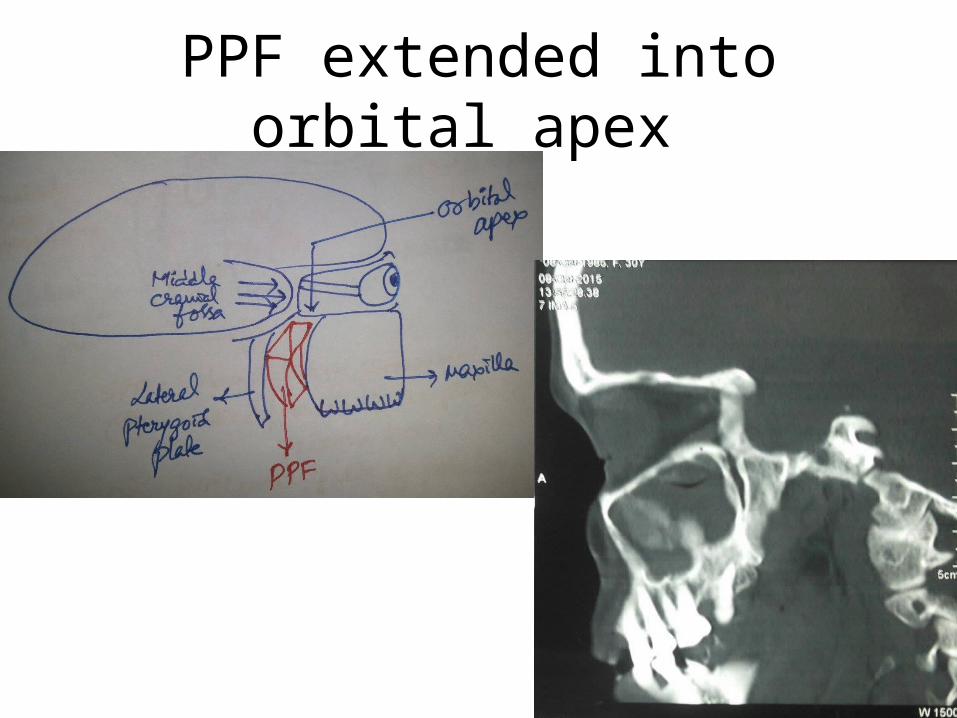
PPF extended into orbital apex
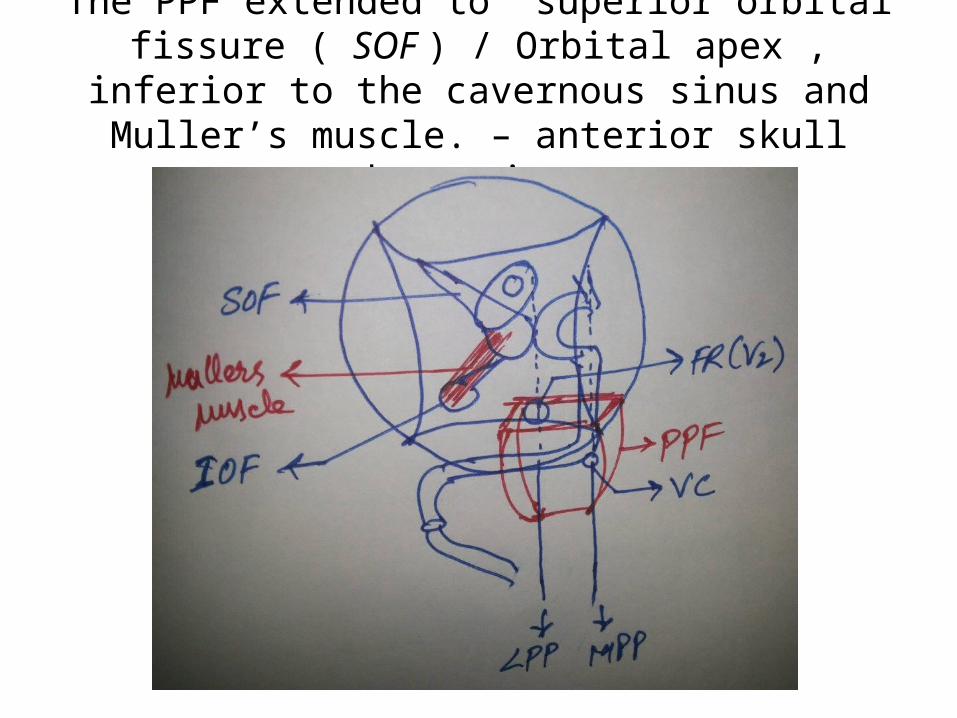
The PPF extended to superior orbital fissure ( SOF ) / Orbital apex , inferior to the cavernous sinus and
Muller’s muscle. – anterior skull base view
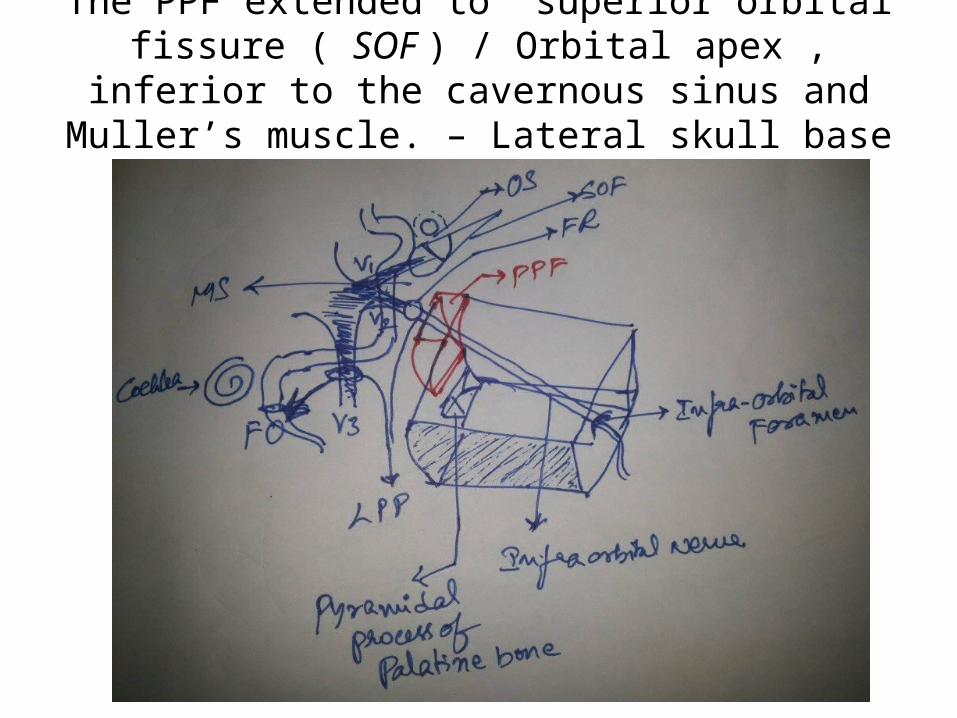
The PPF extended to superior orbital fissure ( SOF ) / Orbital apex , inferior to the cavernous sinus and
Muller’s muscle. – Lateral skull base view
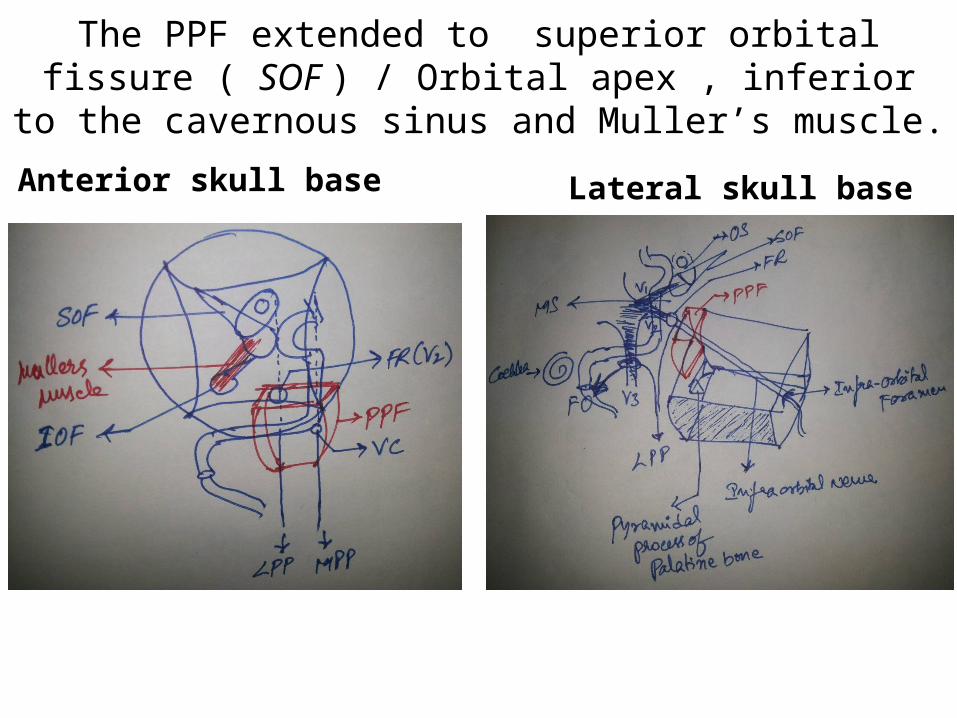
The PPF extended to superior orbital fissure ( SOF ) / Orbital apex , inferior to the cavernous sinus and Muller’s muscle.
Anterior skull base Lateral skull base

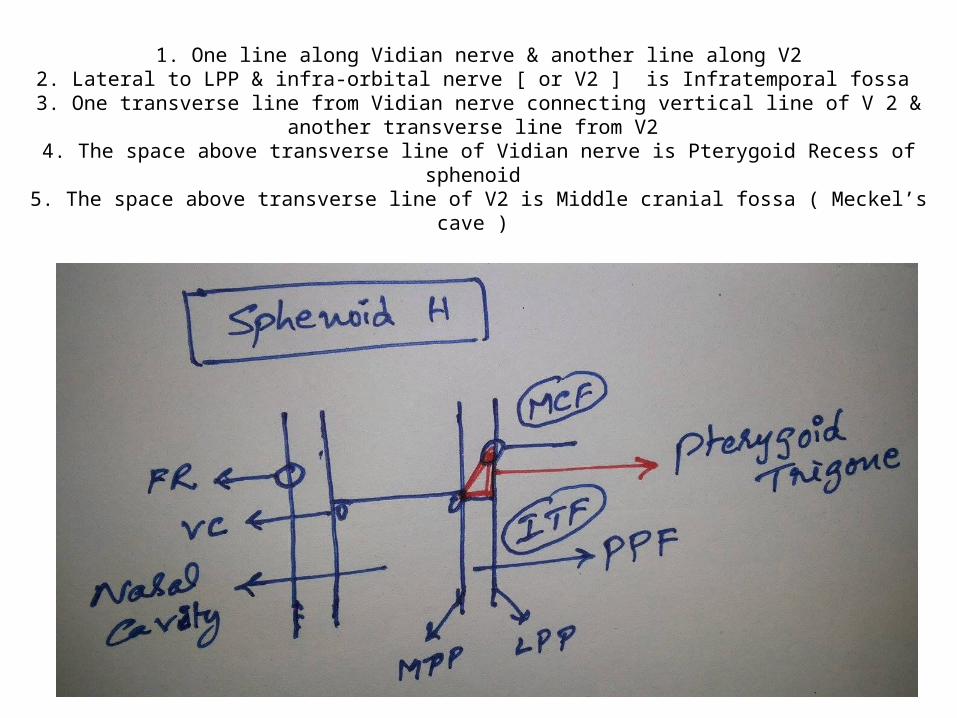
1. One line along Vidian nerve & another line along V22. Lateral to LPP & infra-orbital nerve [ or V2 ] is Infratemporal fossa
3. One transverse line from Vidian nerve connecting vertical line of V 2 & another transverse line from V2
4. The space above transverse line of Vidian nerve is Pterygoid Recess of sphenoid 5. The space above transverse line of V2 is Middle cranial fossa ( Meckel’s cave )
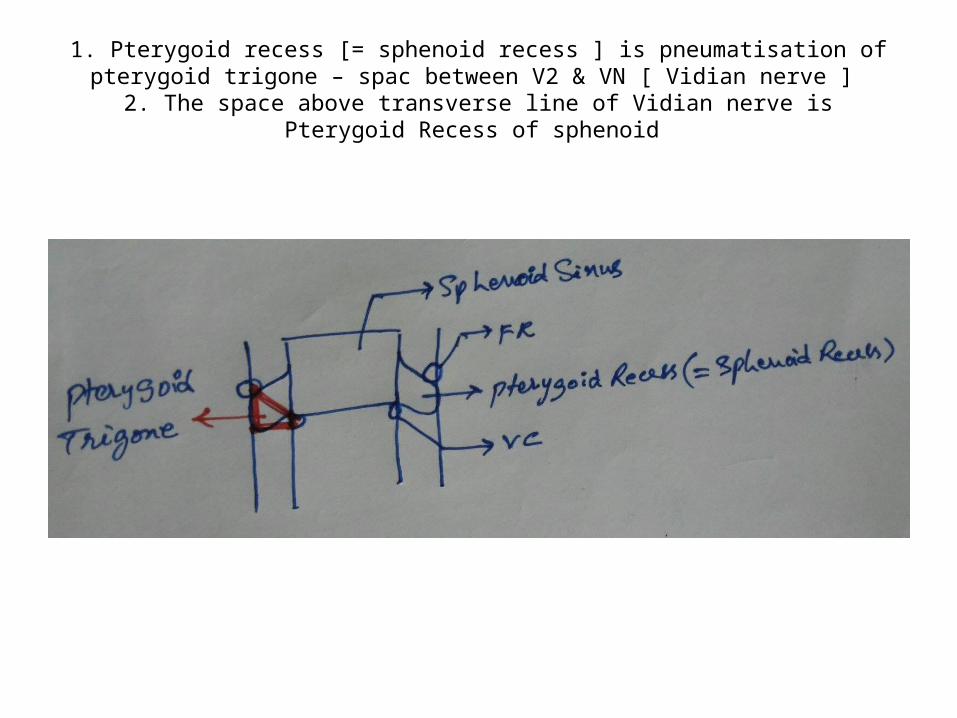
1. Pterygoid recess [= sphenoid recess ] is pneumatisation of pterygoid trigone – spac between V2 & VN [ Vidian nerve ]
2. The space above transverse line of Vidian nerve is Pterygoid Recess of sphenoid
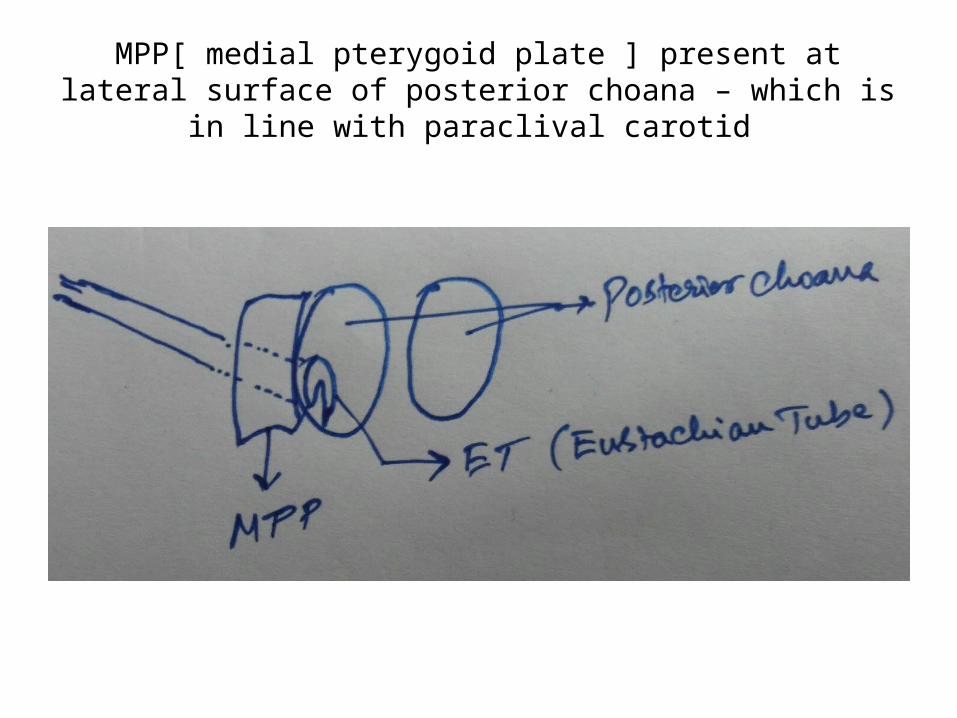
MPP[ medial pterygoid plate ] present at lateral surface of posterior choana – which is in line with paraclival carotid
Vidian canal is funnel shaped
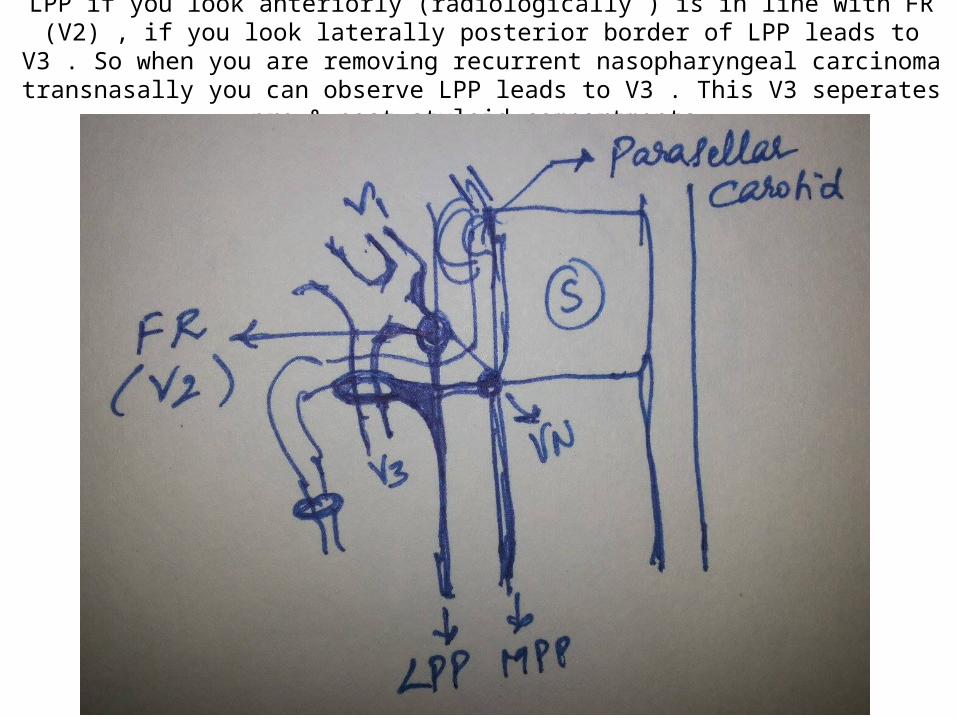
LPP if you look anteriorly (radiologically ) is in line with FR (V2) , if you look laterally posterior border of LPP leads to V3 . So when you are removing recurrent nasopharyngeal carcinoma
transnasally you can observe LPP leads to V3 . This V3 seperates pre & post styloid compartments.
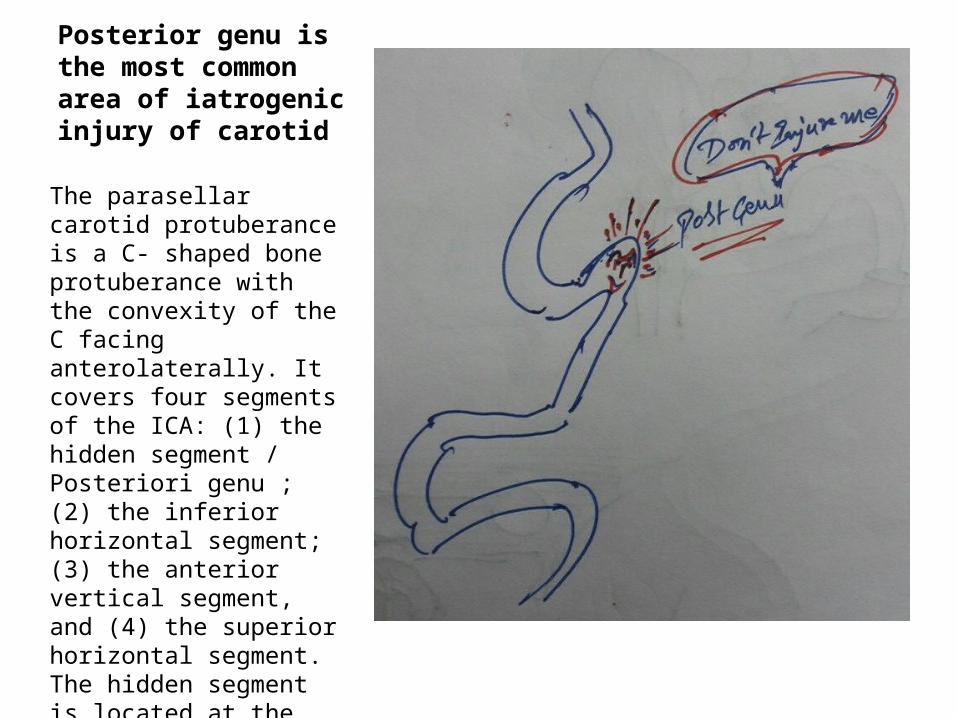
Posterior genu is the most common area of iatrogenic injury of carotid
The parasellar carotid protuberance is a C- shaped bone protuberance with the convexity of the C facing anterolaterally. It covers four segments of the ICA: (1) the hidden segment / Posteriori genu ; (2) the inferior horizontal segment; (3) the anterior vertical segment, and (4) the superior horizontal segment. The hidden segment is located at the level of the posterior sellar floor and includes the posterior bend of the ICA.
IATROGENIC CAROTID INJURE AREAS -
1. Upper & Lower point of C-shape of parasellar carotid - mnemonic
2. Upper point is m-OCR ( optico - carotid recess ) - junction of para seller & intra-cerebral carotid
3. Lower point is posterior genu - junction of paraclival & parasellar carotid
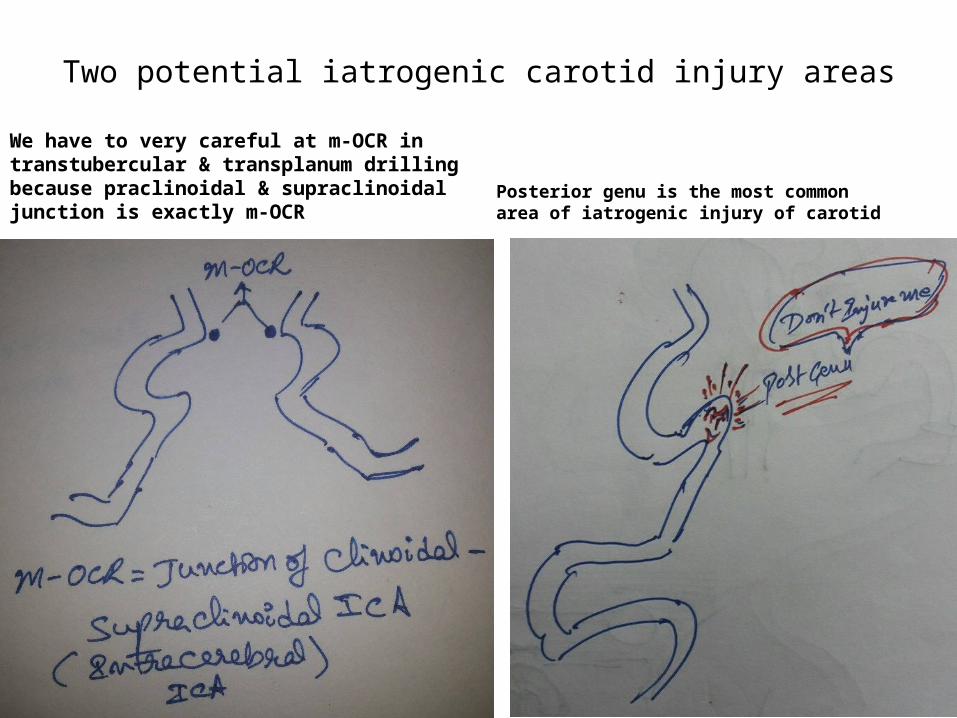
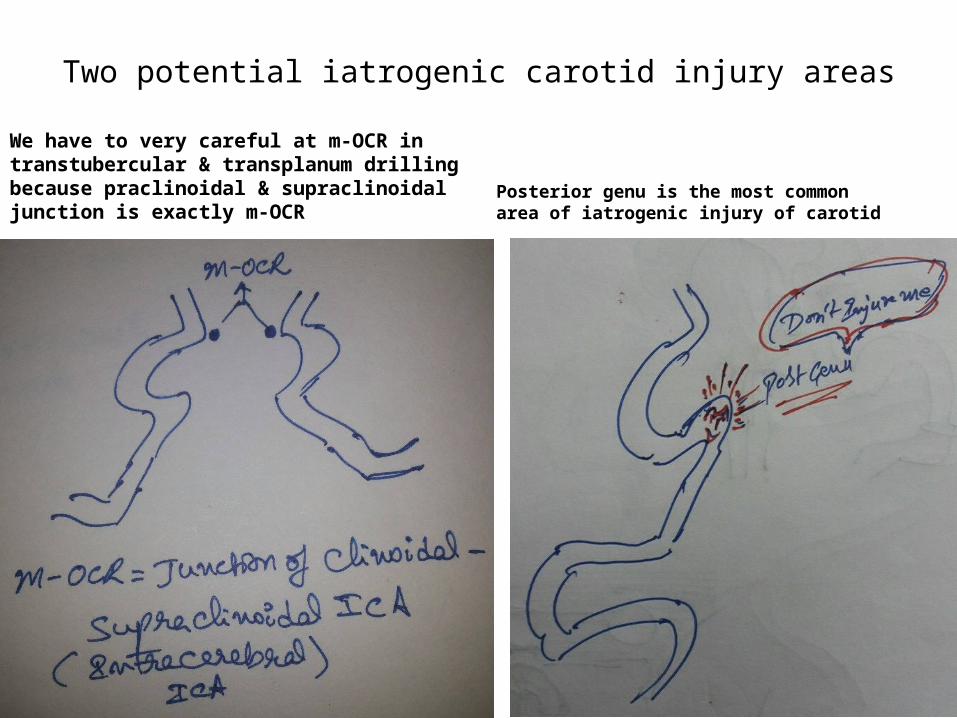
Two potential iatrogenic carotid injury areas
We have to very careful at m-OCR in transtubercular & transplanum drilling because praclinoidal & supraclinoidal junction is exactly m-OCR
Posterior genu is the most common area of iatrogenic injury of carotid
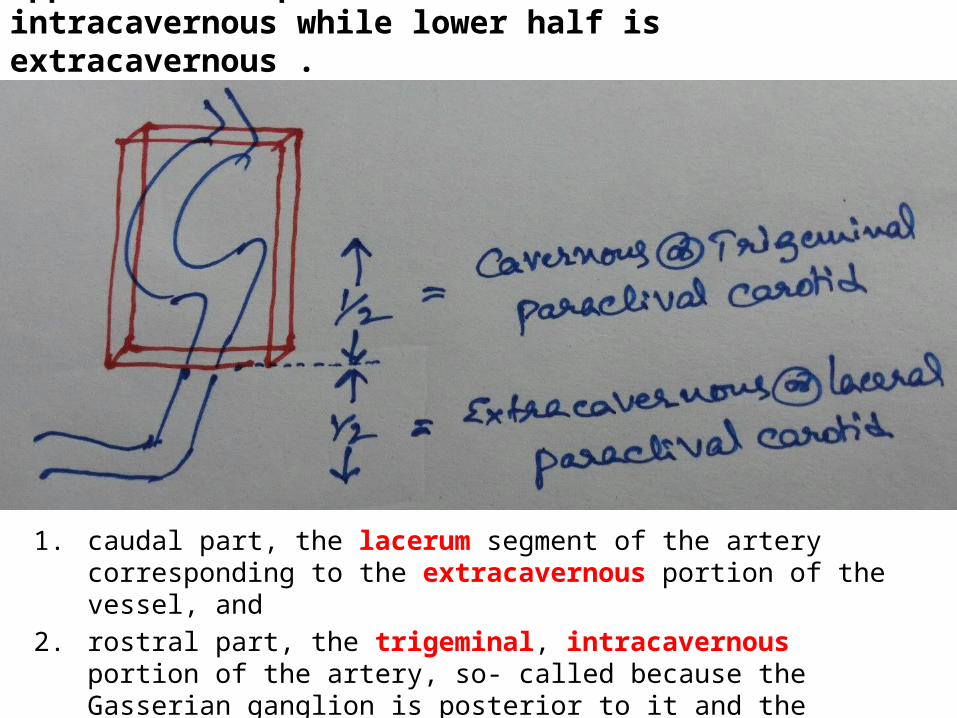
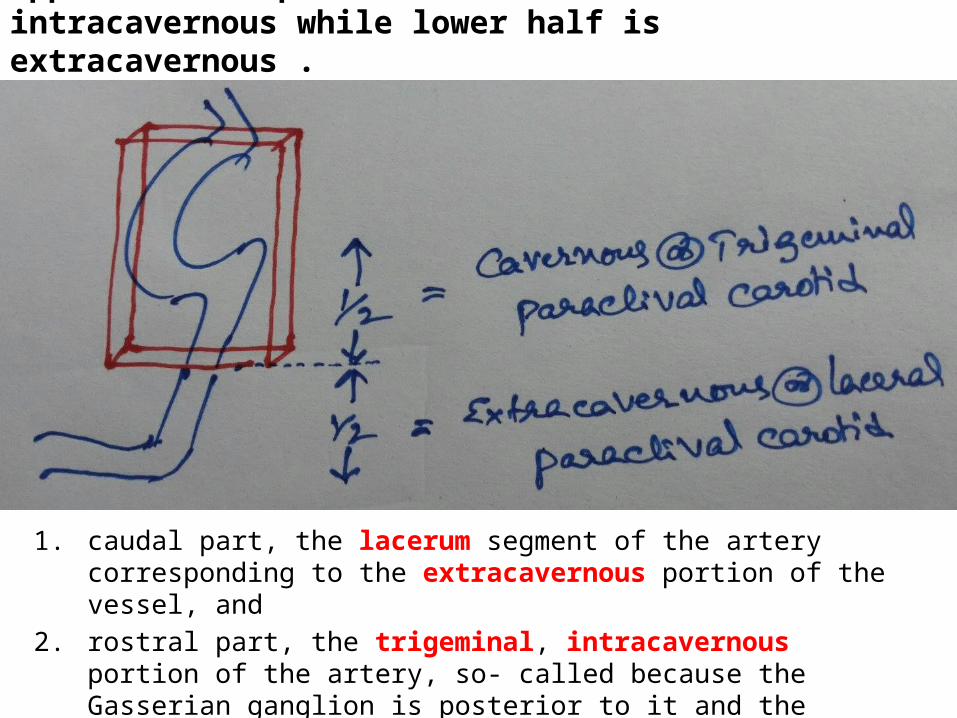
Upper half of paraclival carotid is intracavernous while lower half is extracavernous .
1. caudal part, the lacerum segment of the artery corresponding to the extracavernous portion of the vessel, and
2. rostral part, the trigeminal, intracavernous portion of the artery, so- called because the Gasserian ganglion is posterior to it and the trigeminal divisions are lateral to it.
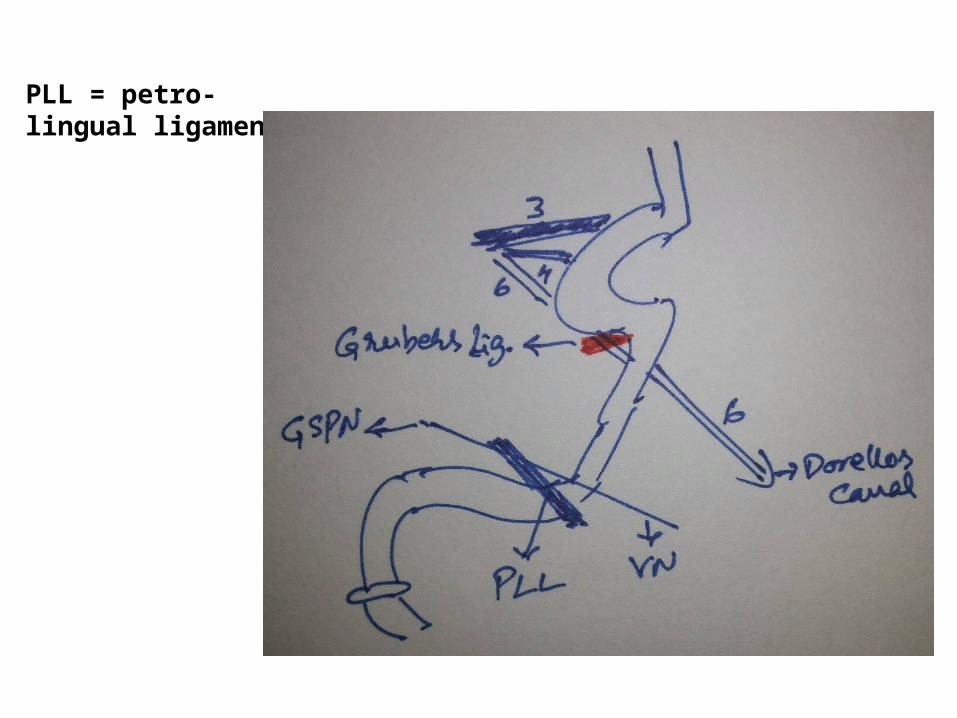
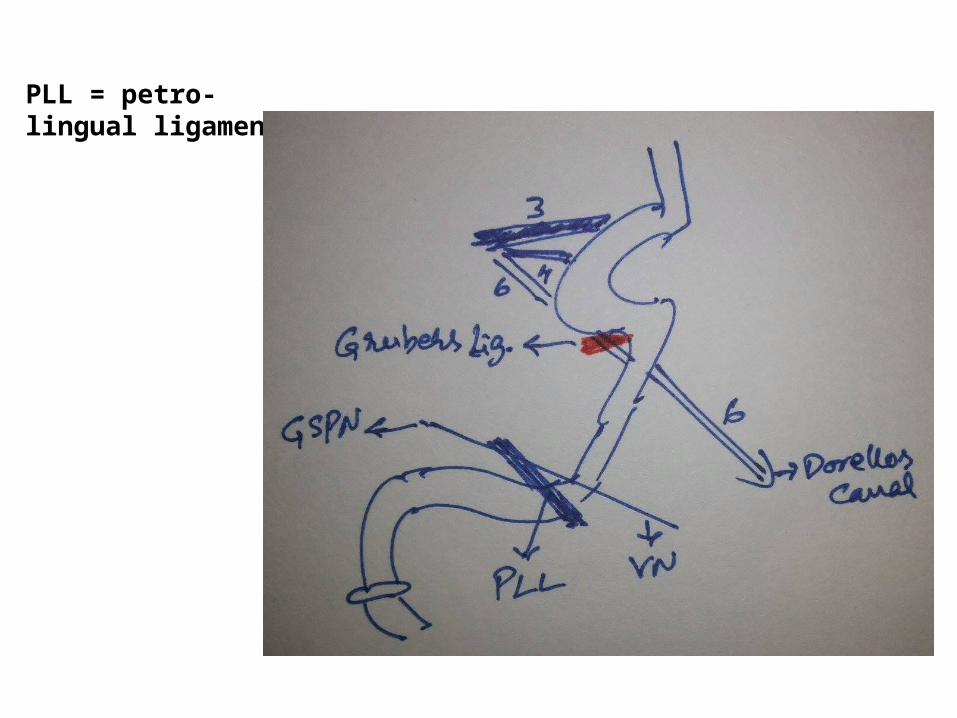
PLL = petro-lingual ligament
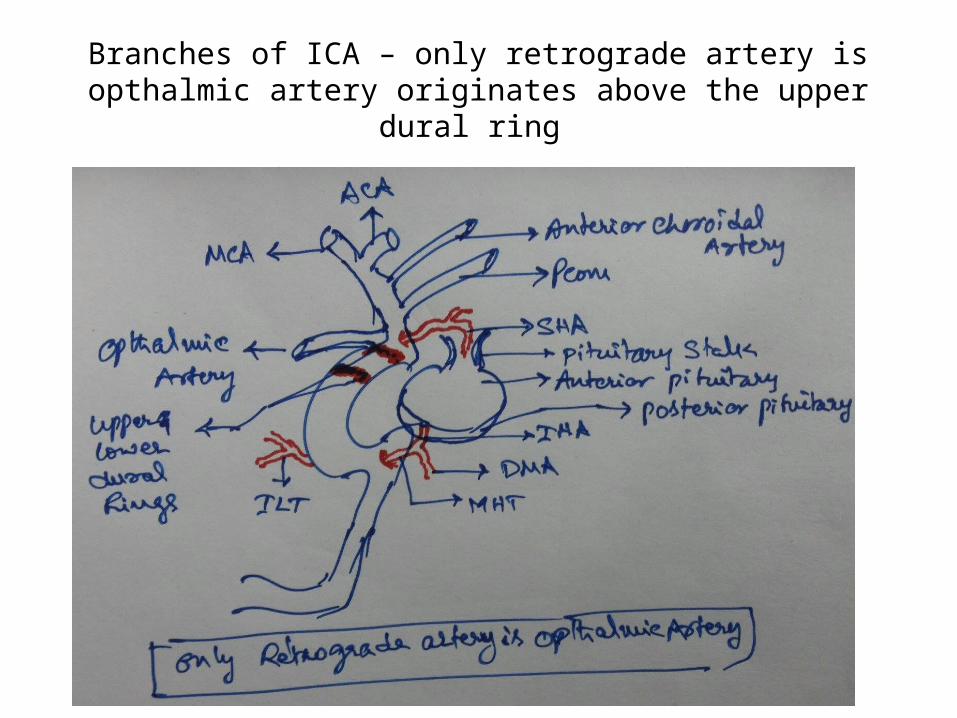
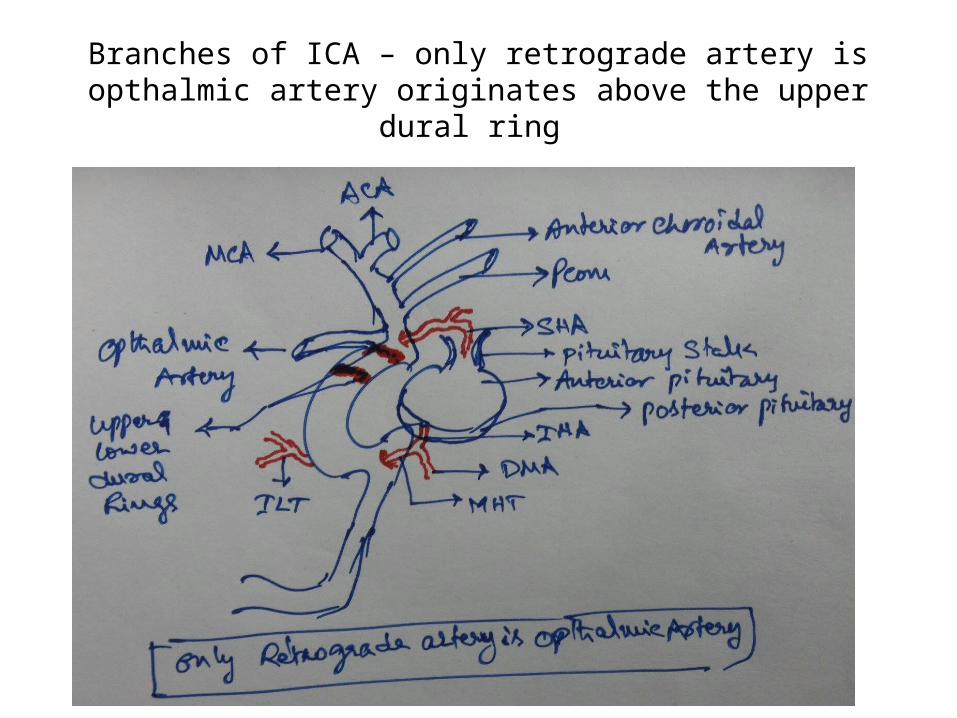
Branches of ICA – only retrograde artery is opthalmic artery originates above the upper dural ring
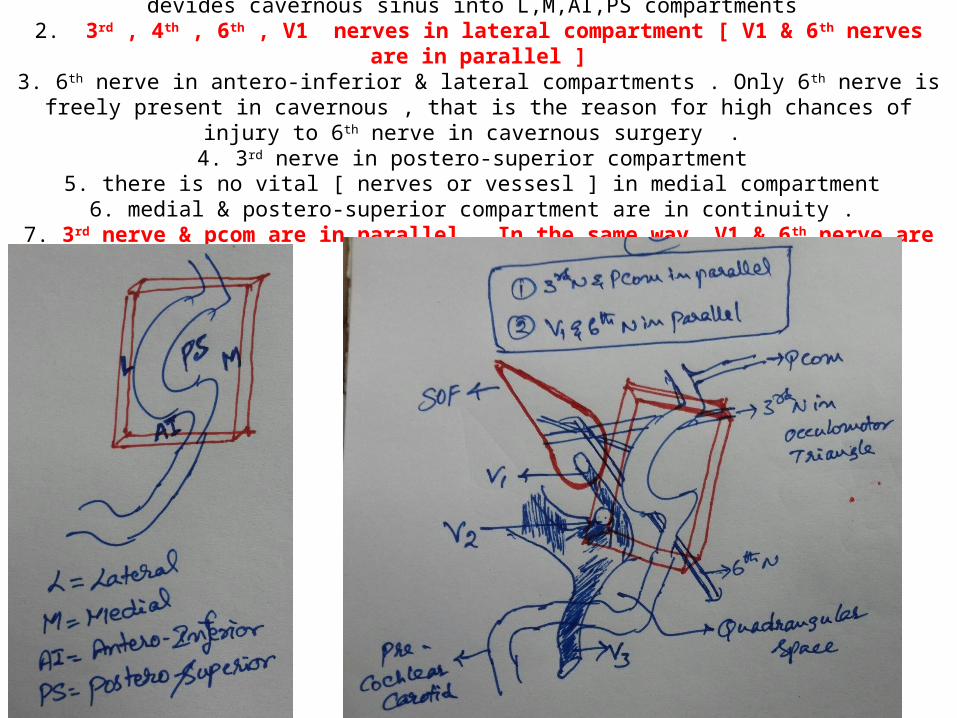
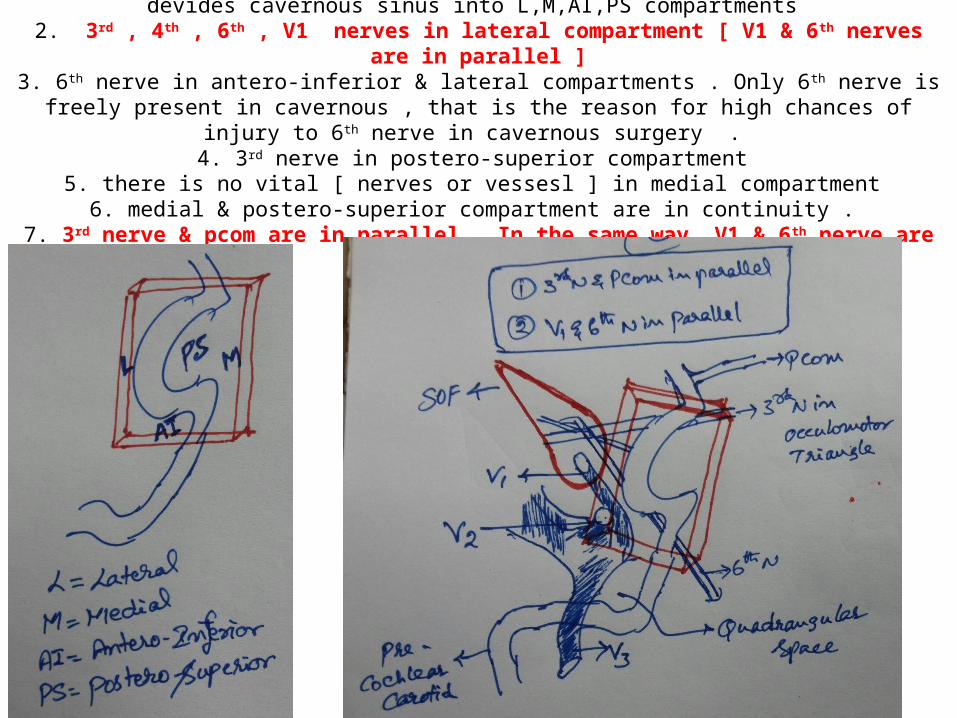
1. Virtual compartments of cavernous sinus – parasellar carotid virtually devides cavernous sinus into L,M,AI,PS compartments
2. 3rd , 4th , 6th , V1 nerves in lateral compartment [ V1 & 6th nerves are in parallel ]3. 6th nerve in antero-inferior & lateral compartments . Only 6th nerve is freely present in cavernous , that is
the reason for high chances of injury to 6th nerve in cavernous surgery . 4. 3rd nerve in postero-superior compartment
5. there is no vital [ nerves or vessesl ] in medial compartment 6. medial & postero-superior compartment are in continuity .
7. 3rd nerve & pcom are in parallel. In the same way V1 & 6th nerve are in parallel
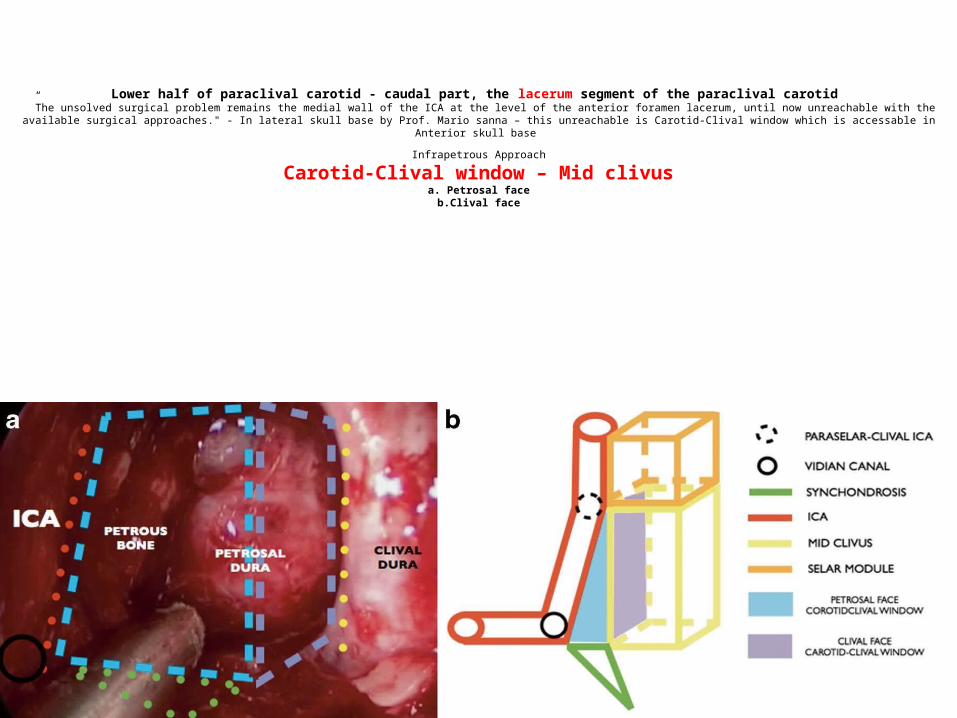
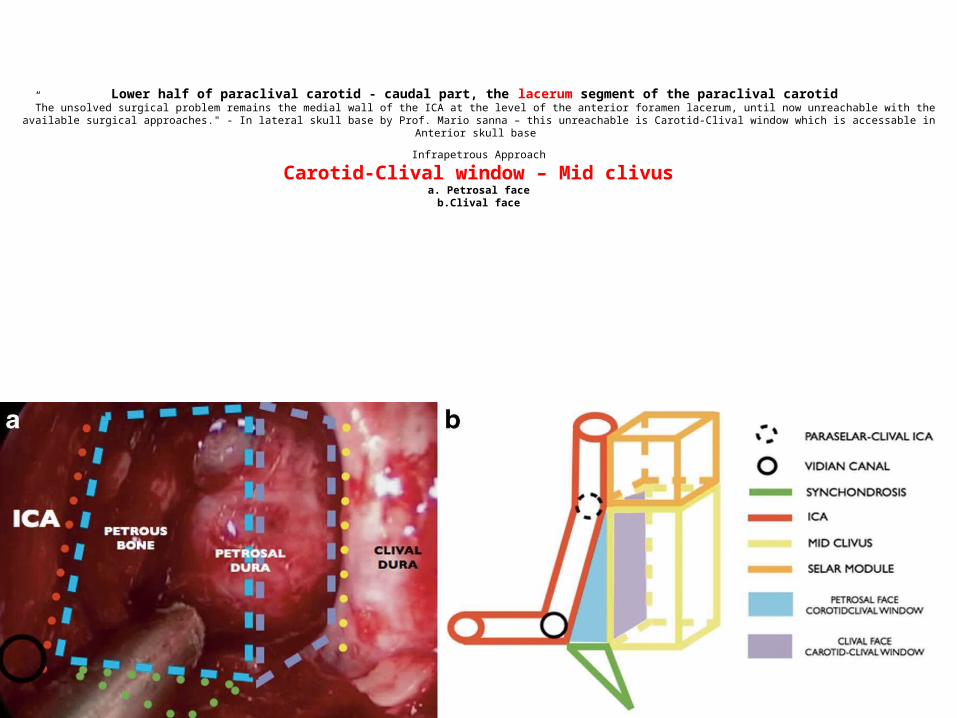
Lower half of paraclival carotid - caudal part, the lacerum segment of the paraclival carotid ”The unsolved surgical problem remains the medial wall of the ICA at the level of the anterior foramen lacerum, until now unreachable with the available surgical approaches." - In lateral skull base by Prof.
Mario sanna – this unreachable is Carotid-Clival window which is accessable in Anterior skull base
Infrapetrous Approach
Carotid-Clival window – Mid clivusa. Petrosal face
b.Clival face
Upper half of paraclival carotid is intracavernous while lower half is extracavernous .
1. caudal part, the lacerum segment of the artery corresponding to the extracavernous portion of the vessel, and
2. rostral part, the trigeminal, intracavernous portion of the artery, so- called because the Gasserian ganglion is posterior to it and the trigeminal divisions are lateral to it.
PLL = petro-lingual ligament
Branches of ICA – only retrograde artery is opthalmic artery originates above the upper dural ring
1. Virtual compartments of cavernous sinus – parasellar carotid virtually devides cavernous sinus into L,M,AI,PS compartments
2. 3rd , 4th , 6th , V1 nerves in lateral compartment [ V1 & 6th nerves are in parallel ]3. 6th nerve in antero-inferior & lateral compartments . Only 6th nerve is freely present in cavernous , that is
the reason for high chances of injury to 6th nerve in cavernous surgery . 4. 3rd nerve in postero-superior compartment
5. there is no vital [ nerves or vessesl ] in medial compartment 6. medial & postero-superior compartment are in continuity .
7. 3rd nerve & pcom are in parallel. In the same way V1 & 6th nerve are in parallel
Lower half of paraclival carotid - caudal part, the lacerum segment of the paraclival carotid ”The unsolved surgical problem remains the medial wall of the ICA at the level of the anterior foramen lacerum, until now unreachable with the available surgical approaches." - In lateral skull base by Prof.
Mario sanna – this unreachable is Carotid-Clival window which is accessable in Anterior skull base
Infrapetrous Approach
Carotid-Clival window – Mid clivusa. Petrosal face
b.Clival face
Superior & inferior orbital fissure
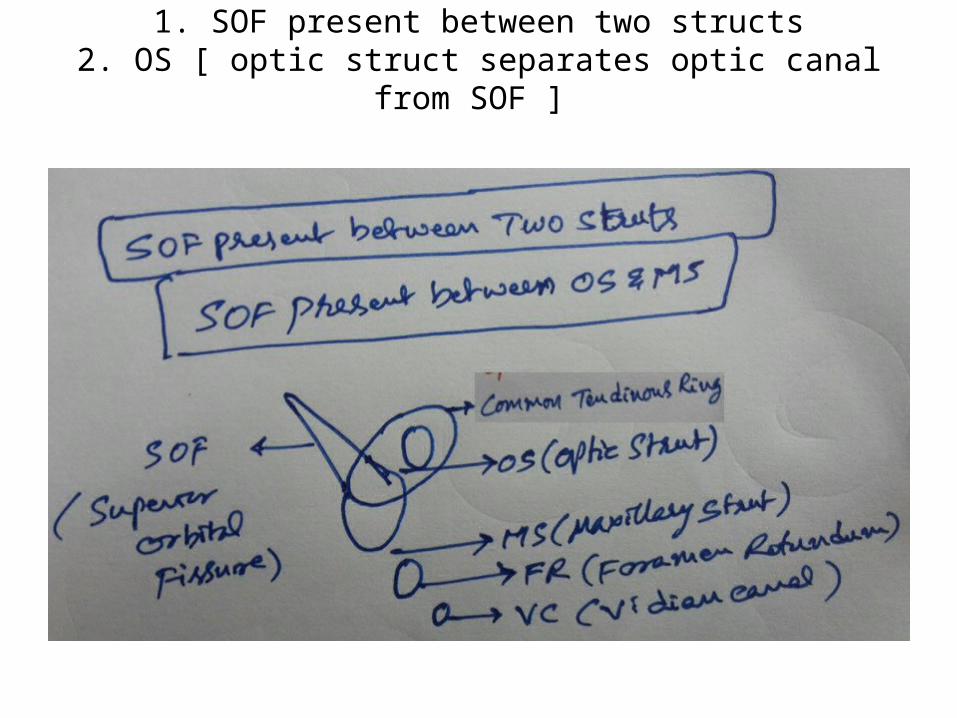
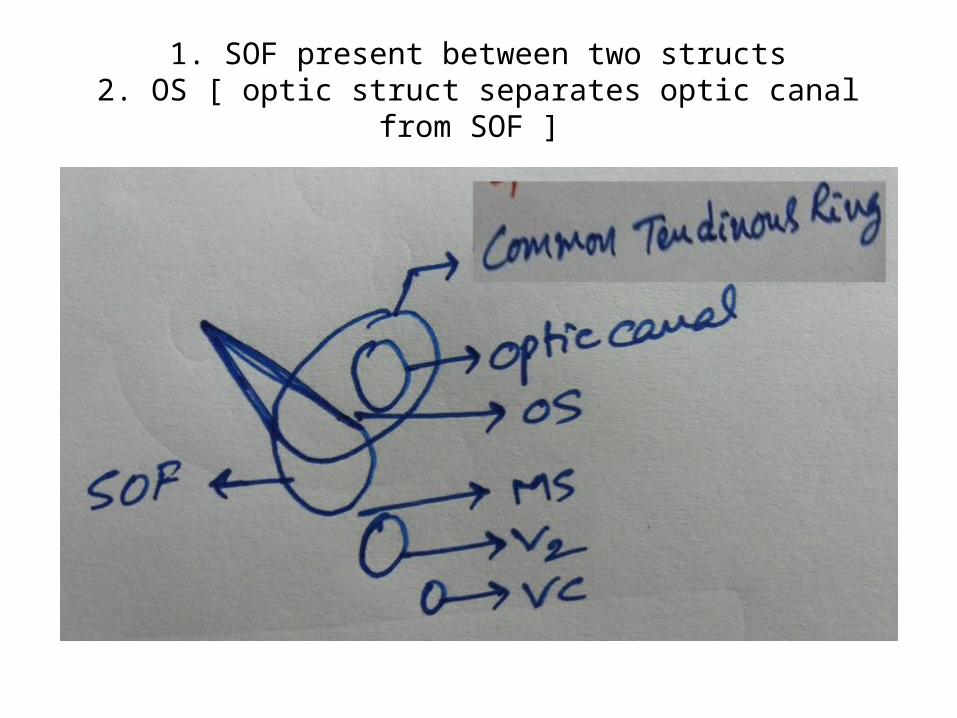
1. SOF present between two structs2. OS [ optic struct separates optic canal from SOF ]
1. SOF present between two structs2. OS [ optic struct separates optic canal from SOF ]
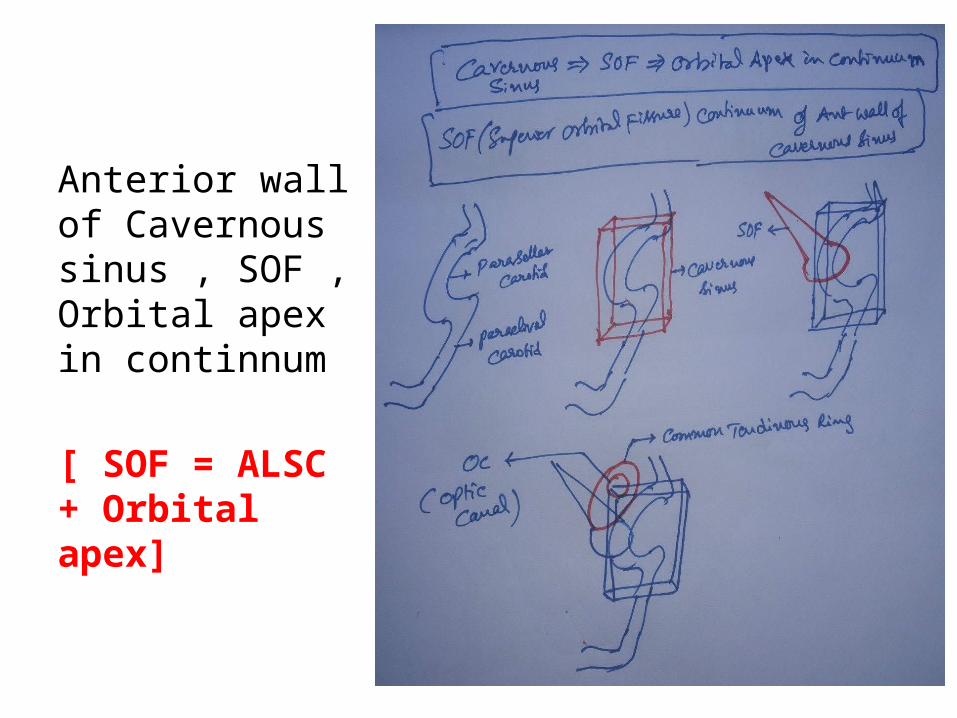
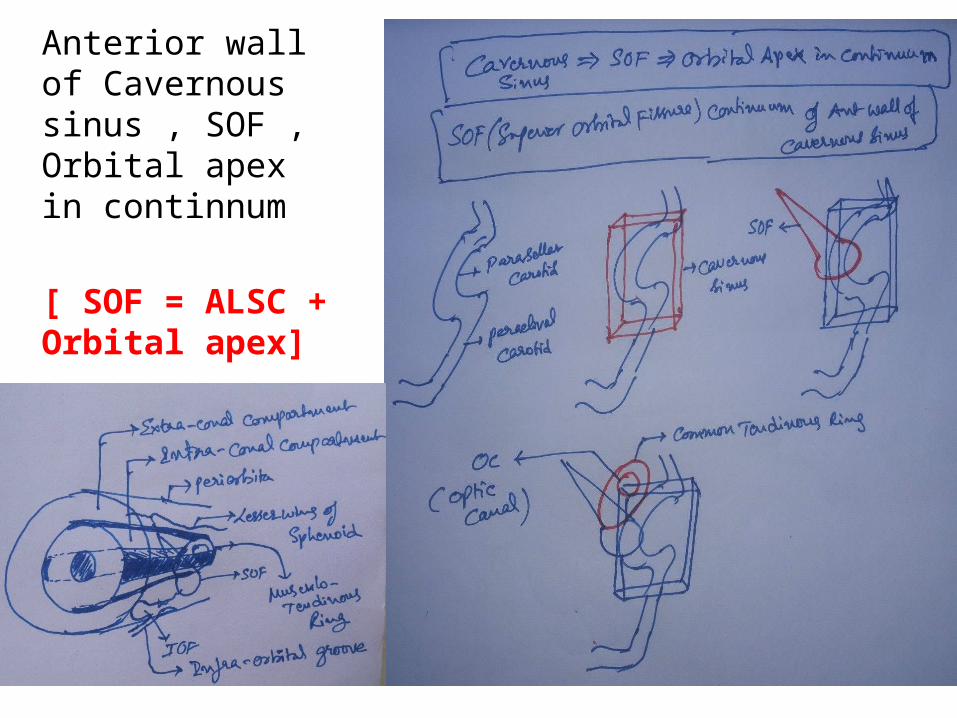
Anterior wall of Cavernous sinus , SOF , Orbital apex in continnum
[ SOF = ALSC + Orbital apex]
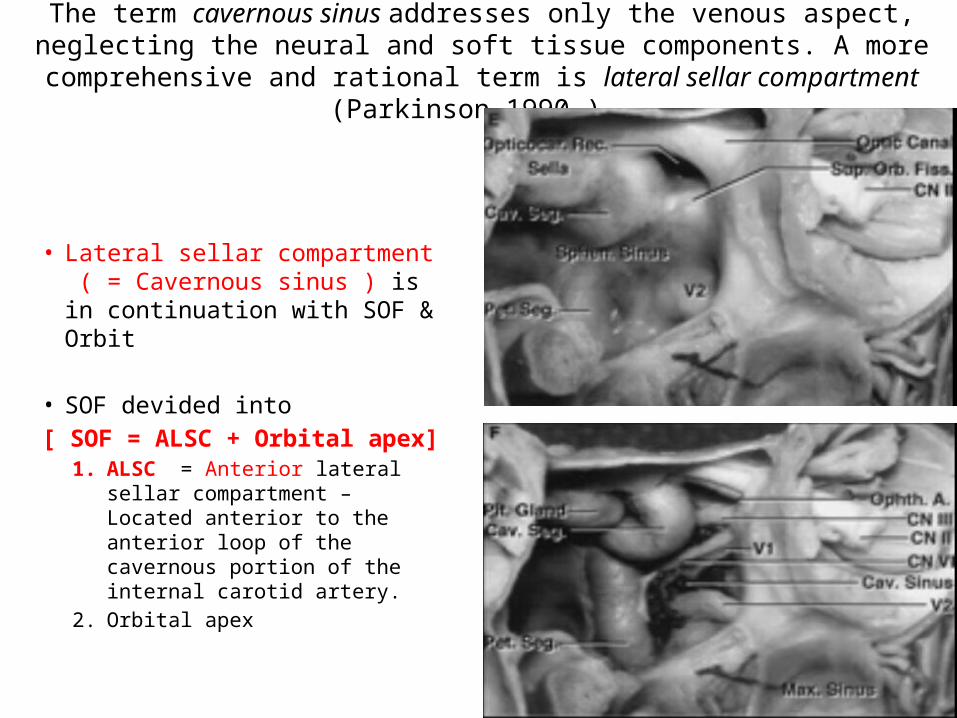
The term cavernous sinus addresses only the venous aspect, neglecting the neural and soft tissue components. A more comprehensive and rational term is lateral sellar
compartment (Parkinson 1990 ) .
• Lateral sellar compartment ( = Cavernous sinus ) is in continuation with SOF & Orbit
• SOF devided into [ SOF = ALSC + Orbital apex]
1. ALSC = Anterior lateral sellar compartment – Located anterior to the anterior loop of the cavernous portion of the internal carotid artery.
2. Orbital apex
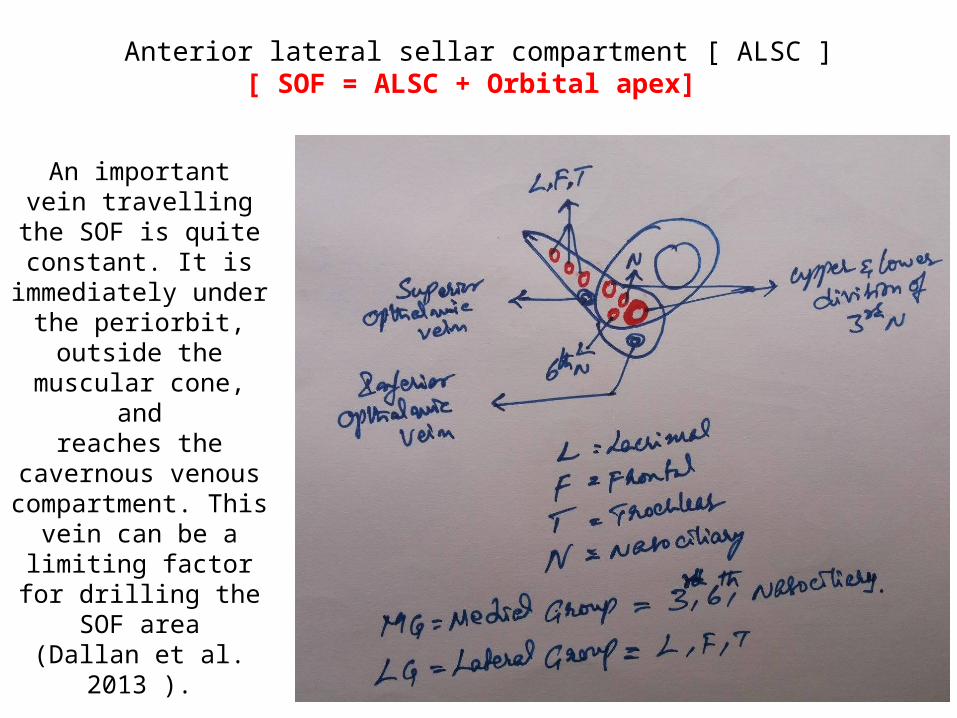
Anterior lateral sellar compartment [ ALSC ] [ SOF = ALSC + Orbital apex]
An importantvein travelling the
SOF is quite constant. It is
immediately under the periorbit, outside the
muscular cone, andreaches the
cavernous venous compartment. This
vein can be a limiting factor for
drilling the SOF area(Dallan et al. 2013 ).
Parts of ALSC ( Anterior lateral sellar compartment )
1. Superior Part – Nervous compartment
a. Lateral Group of nerves - from lateral to medial - LFT[ Liver functional tests ] Menumonic – Lacrimal N., Frontal N.,TrochlearN.
b. Middle Group of nerves - 3rd , 6th , Nasocilliary N.
2. Inferior part – Venous compartment - Inferior Opthalmic vein – The inferior venous compartment is given by the confluence of the superior ophthalmic vein ( SOV ) and inferior ophthalmic vein ( IOV ), which drain into the cavernous sinus (Froelich et al. 2009 ) .
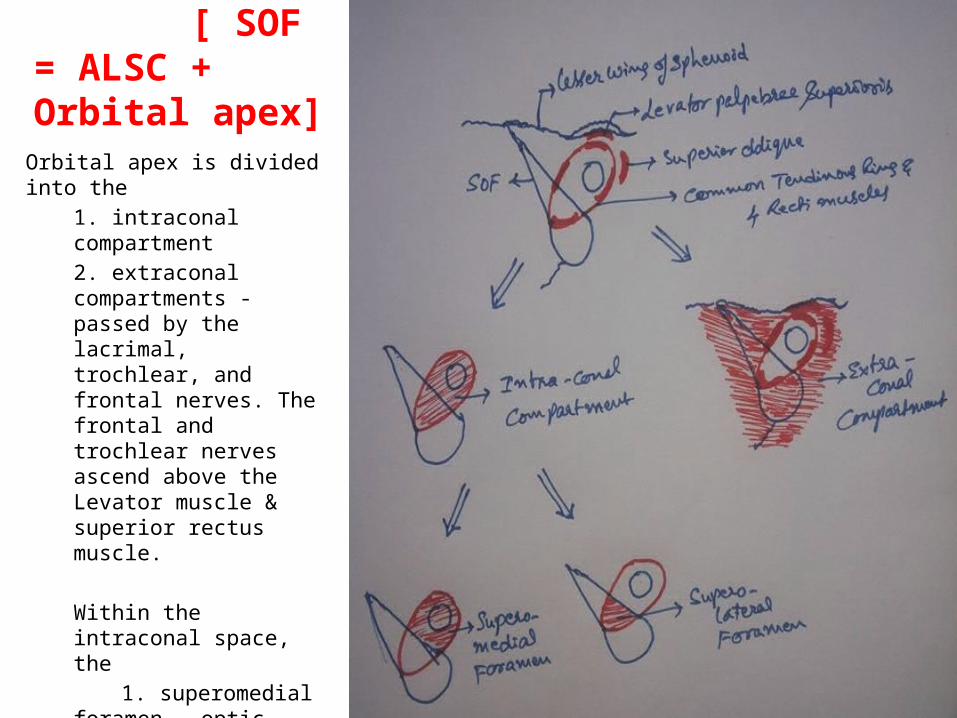
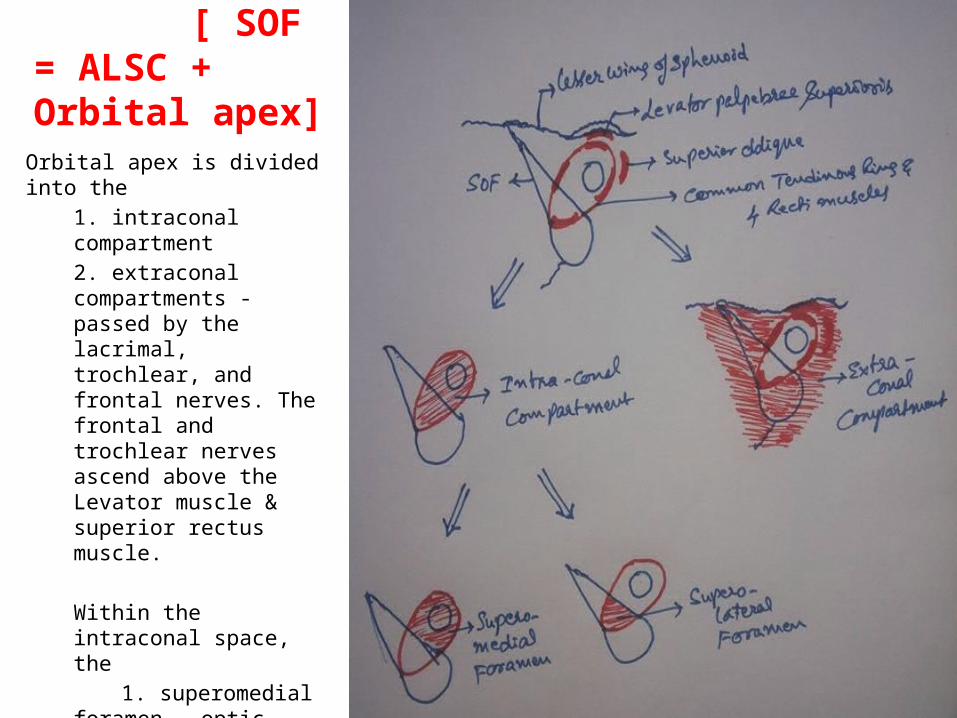
ORBITAL APEX [ SOF = ALSC + Orbital apex]
Orbital apex is divided into the 1. intraconal compartment2. extraconal compartments - passed by the lacrimal, trochlear, and frontal nerves. The frontal and trochlear nerves ascend above the Levator muscle & superior rectus muscle.
Within the intraconal space, the
1. superomedial foramen - optic nerve and the ophthalmic artery pass.
2. superolateral foramen - oculomotor, nasociliary, and abducens nerves pass.
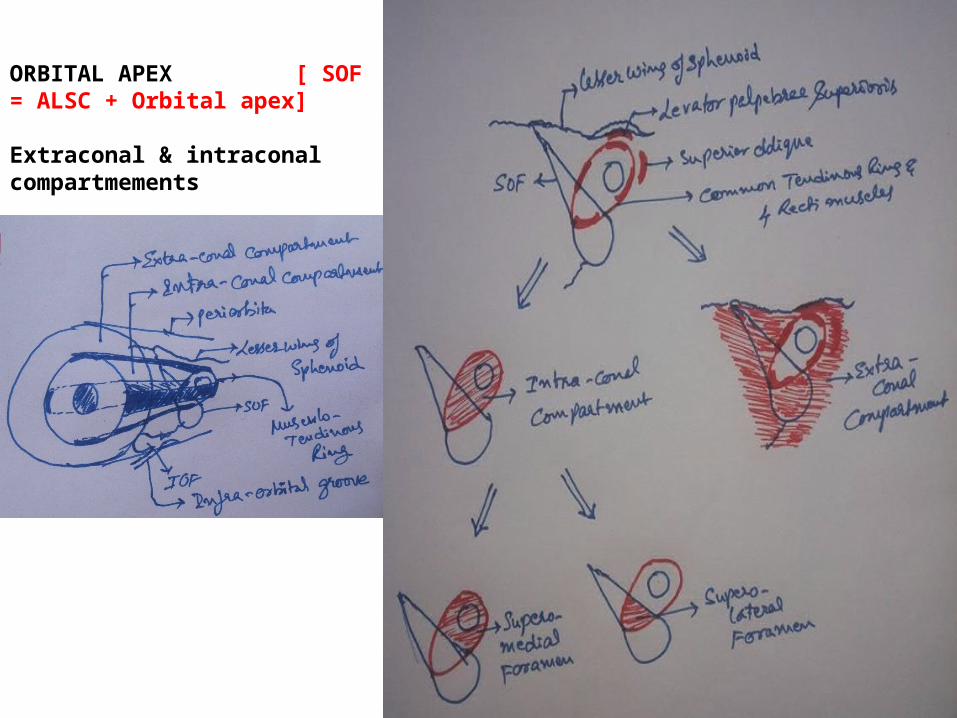
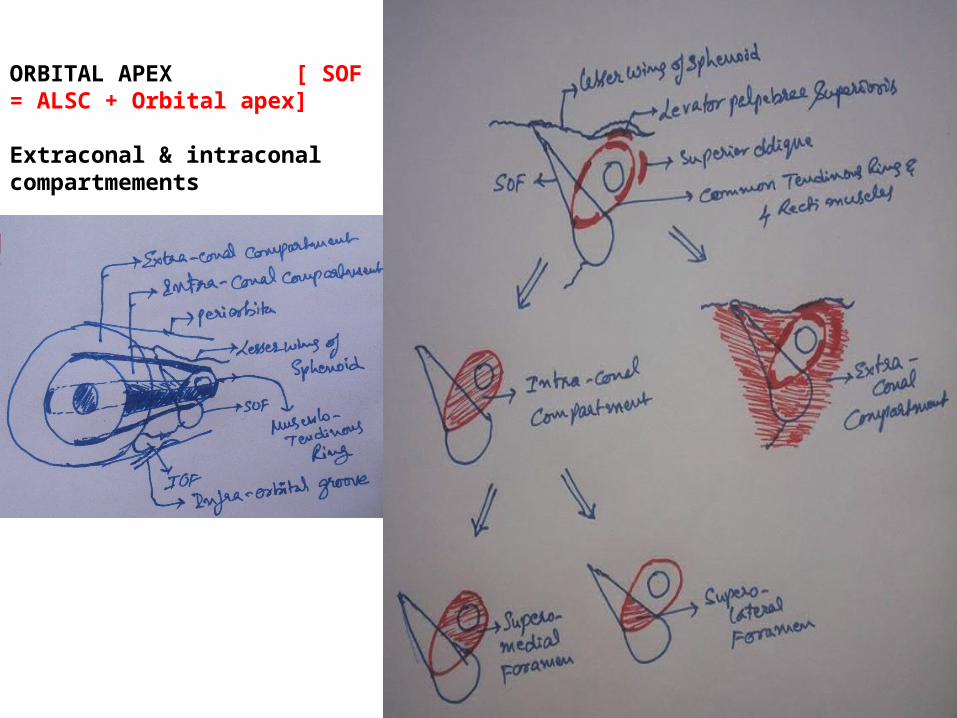
ORBITAL APEX [ SOF = ALSC + Orbital apex]
Extraconal & intraconal compartmements
Parts of Orbital Apex
Orbital apex is divided into the – intraconal compartment– extraconal compartments - passed by the lacrimal, trochlear,
and frontal nerves. The frontal and trochlear nerves ascend above the Levator muscle & superior rectus muscle.
Within the intraconal space, the 1. superomedial foramen - optic nerve and the ophthalmic artery pass.
2. superolateral foramen - oculomotor, nasociliary, and abducens nerves pass.
Anterior wall of Cavernous sinus , SOF , Orbital apex in continnum
[ SOF = ALSC + Orbital apex]
ORBITAL APEX [ SOF = ALSC + Orbital apex]
Orbital apex is divided into the 1. intraconal compartment2. extraconal compartments - passed by the lacrimal, trochlear, and frontal nerves. The frontal and trochlear nerves ascend above the Levator muscle & superior rectus muscle.
Within the intraconal space, the
1. superomedial foramen - optic nerve and the ophthalmic artery pass.
2. superolateral foramen - oculomotor, nasociliary, and abducens nerves pass.
ORBITAL APEX [ SOF = ALSC + Orbital apex]
Extraconal & intraconal compartmements
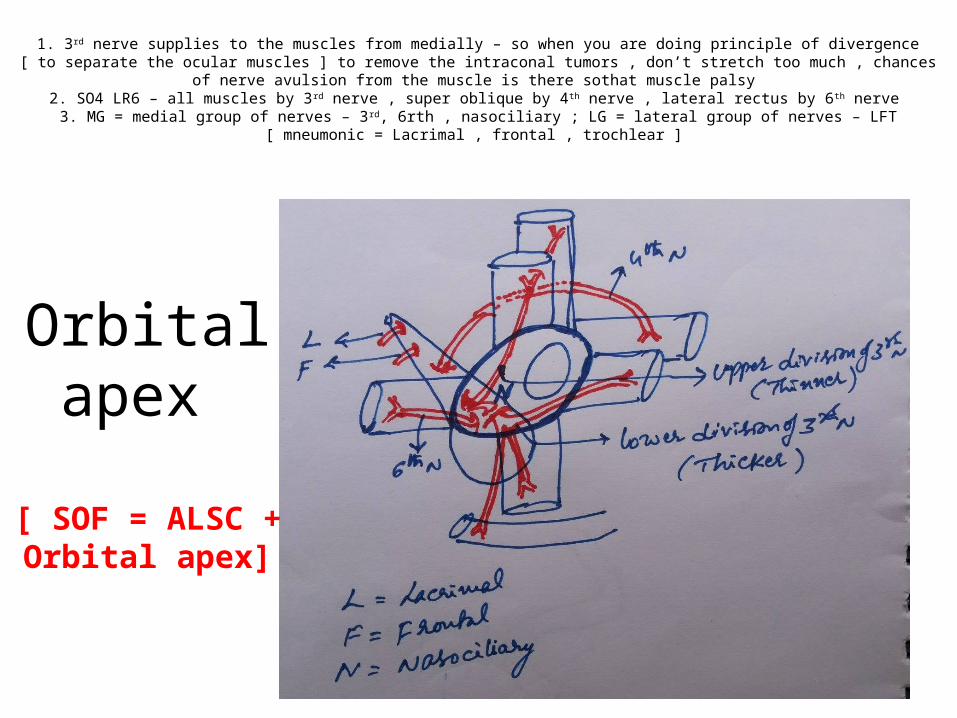
1. 3rd nerve supplies to the muscles from medially – so when you are doing principle of divergence [ to separate the ocular muscles ] to remove the intraconal tumors , don’t stretch too much , chances of nerve avulsion from the muscle is there sothat muscle palsy
2. SO4 LR6 – all muscles by 3rd nerve , super oblique by 4th nerve , lateral rectus by 6th nerve 3. MG = medial group of nerves – 3rd, 6rth , nasociliary ; LG = lateral group of nerves – LFT [ mneumonic = Lacrimal , frontal ,
trochlear ]
Orbital apex
[ SOF = ALSC + Orbital apex]
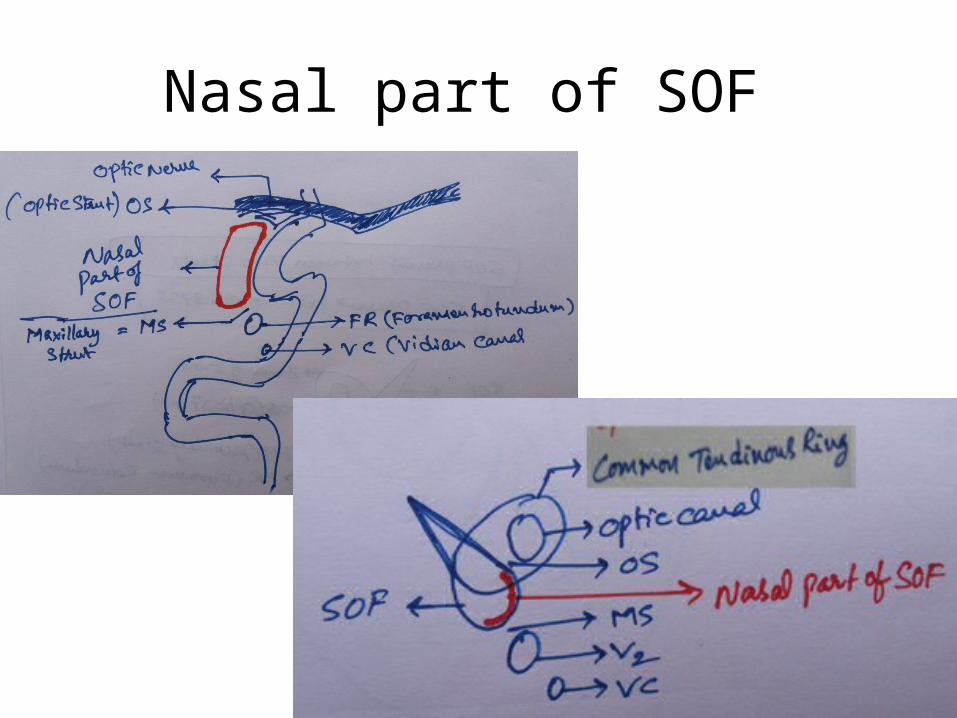
Nasal part of SOF

1. 3rd nerve supplies to the muscles from medially – so when you are doing principle of divergence [ to separate the ocular muscles ] to remove the intraconal tumors , don’t stretch too much , chances of nerve avulsion from the muscle is there sothat muscle palsy
2. SO4 LR6 – all muscles by 3rd nerve , super oblique by 4th nerve , lateral rectus by 6th nerve 3. MG = medial group of nerves – 3rd, 6rth , nasociliary ; LG = lateral group of nerves – LFT [ mneumonic = Lacrimal , frontal , trochlear ]
4. 6th nerve is lateral to nasociliary nerve in between two divisions of 3rd nerve because it has to supply lateral rectus .
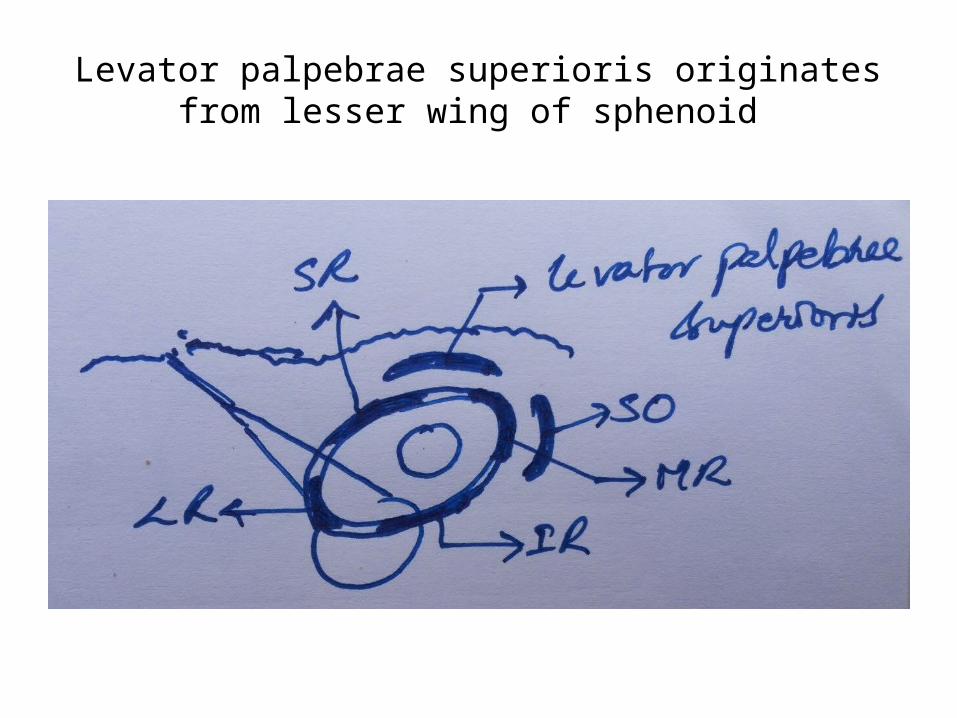
Levator palpebrae superioris originates from lesser wing of sphenoid
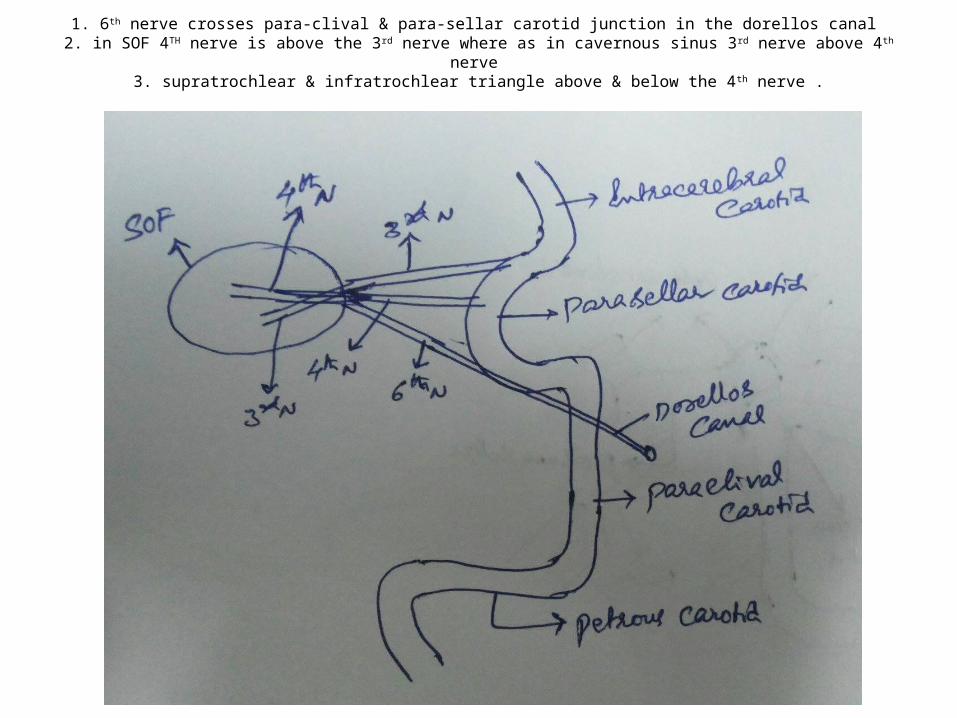
1. 6th nerve crosses para-clival & para-sellar carotid junction in the dorellos canal 2. in SOF 4TH nerve is above the 3rd nerve where as in cavernous sinus 3rd nerve above 4th nerve
3. supratrochlear & infratrochlear triangle above & below the 4th nerve .
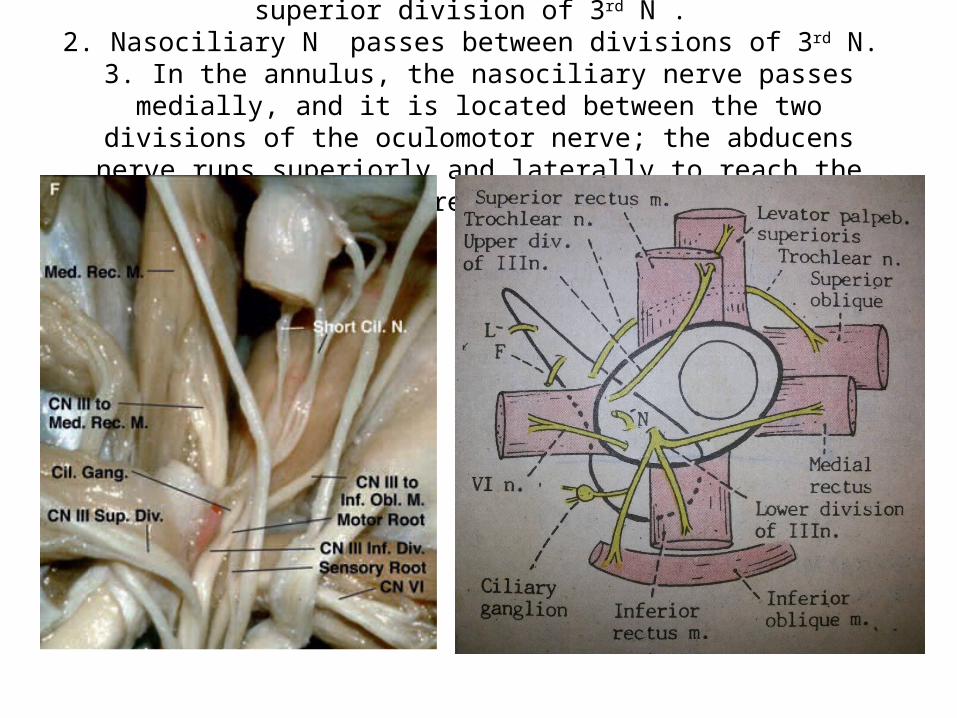
1. Thicker inferior division of 3rd N. & thinner superior division of 3rd N . 2. Nasociliary N passes between divisions of 3rd N.
3. In the annulus, the nasociliary nerve passes medially, and it is located between the two divisions of the oculomotor nerve; the abducens nerve runs
superiorly and laterally to reach the lateral rectus muscle.
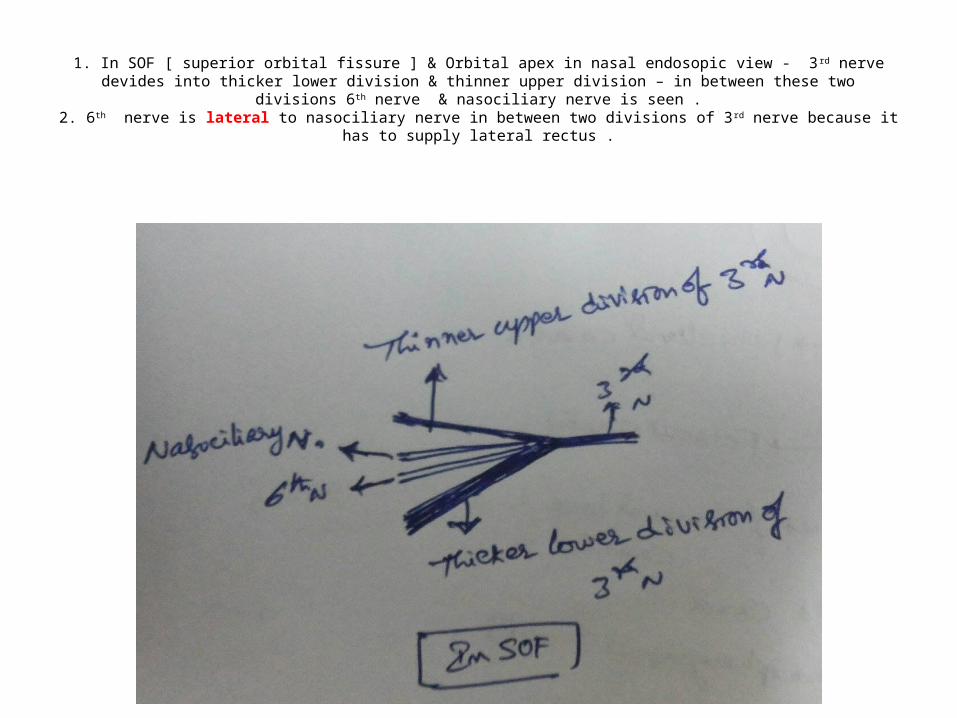
1. In SOF [ superior orbital fissure ] & Orbital apex in nasal endosopic view - 3rd nerve devides into thicker lower division & thinner upper division – in between these two divisions 6th nerve & nasociliary nerve is seen .
2. 6th nerve is lateral to nasociliary nerve in between two divisions of 3rd nerve because it has to supply lateral rectus .
M-OCR
Two potential iatrogenic carotid injury areas
We have to very careful at m-OCR in transtubercular & transplanum drilling because praclinoidal & supraclinoidal junction is exactly m-OCR
Posterior genu is the most common area of iatrogenic injury of carotid
Opthalmic artery
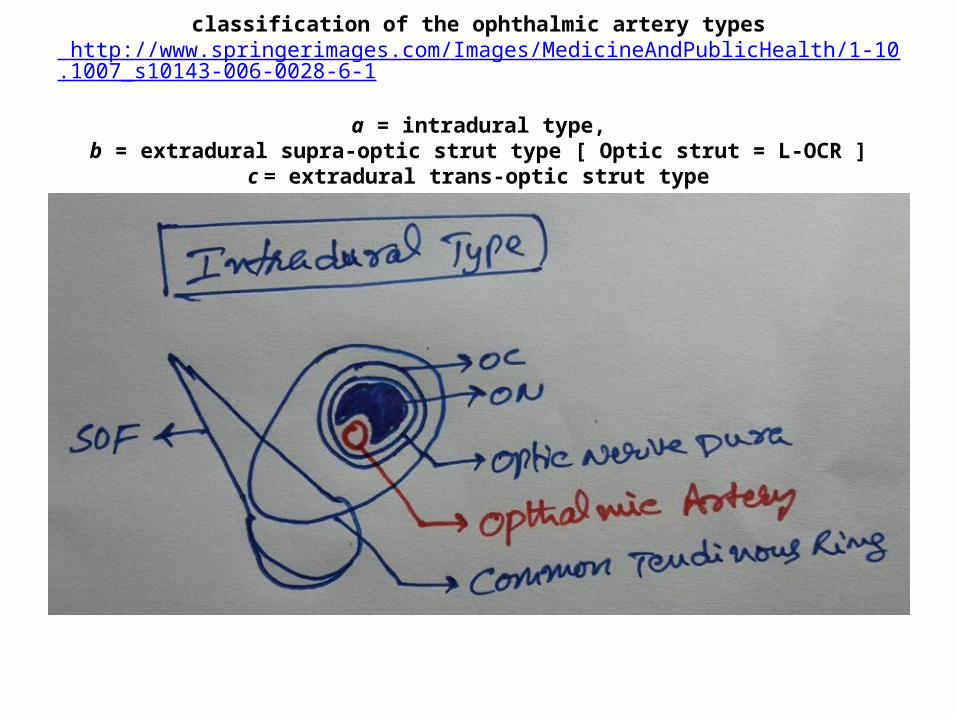
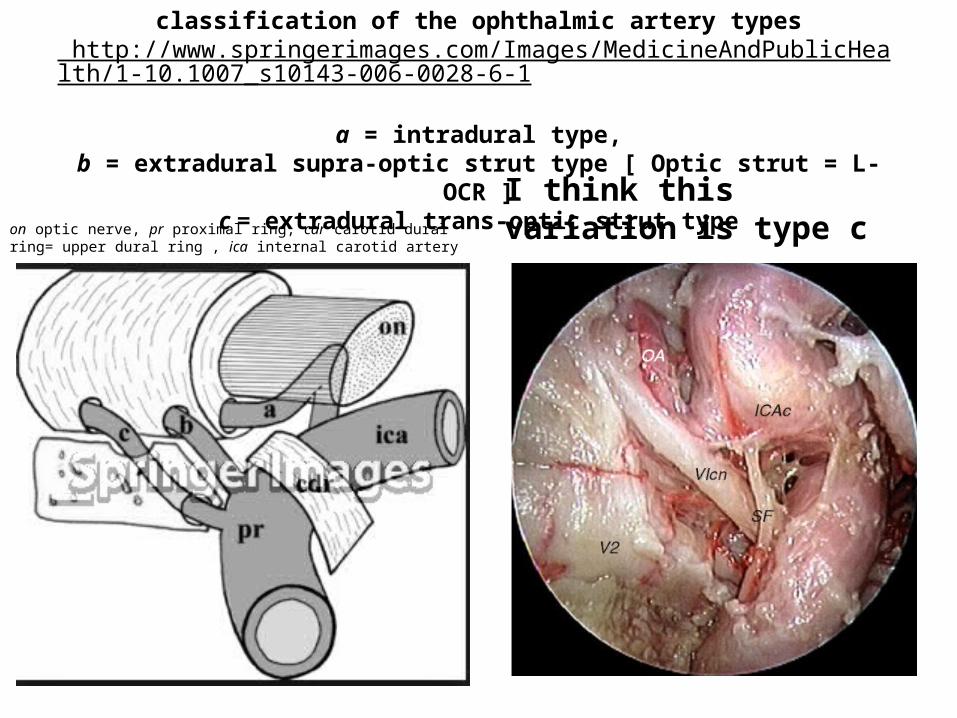
classification of the ophthalmic artery types http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s10143-006-0028-6-1
a = intradural type,
b = extradural supra-optic strut type [ Optic strut = L-OCR ]c = extradural trans-optic strut type
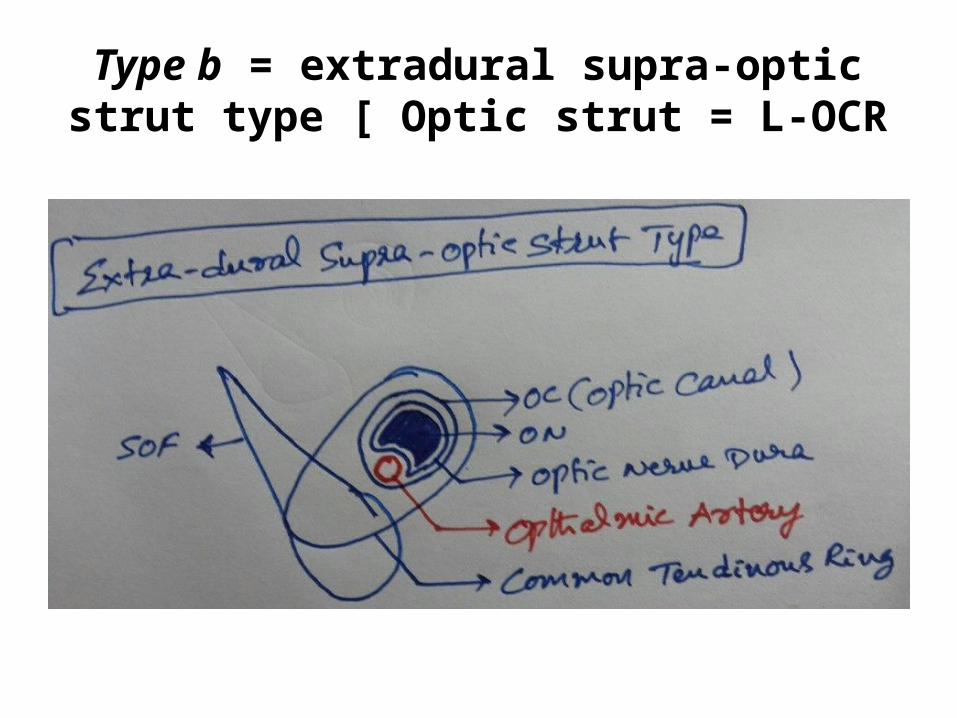
Type b = extradural supra-optic strut type [ Optic strut = L-OCR
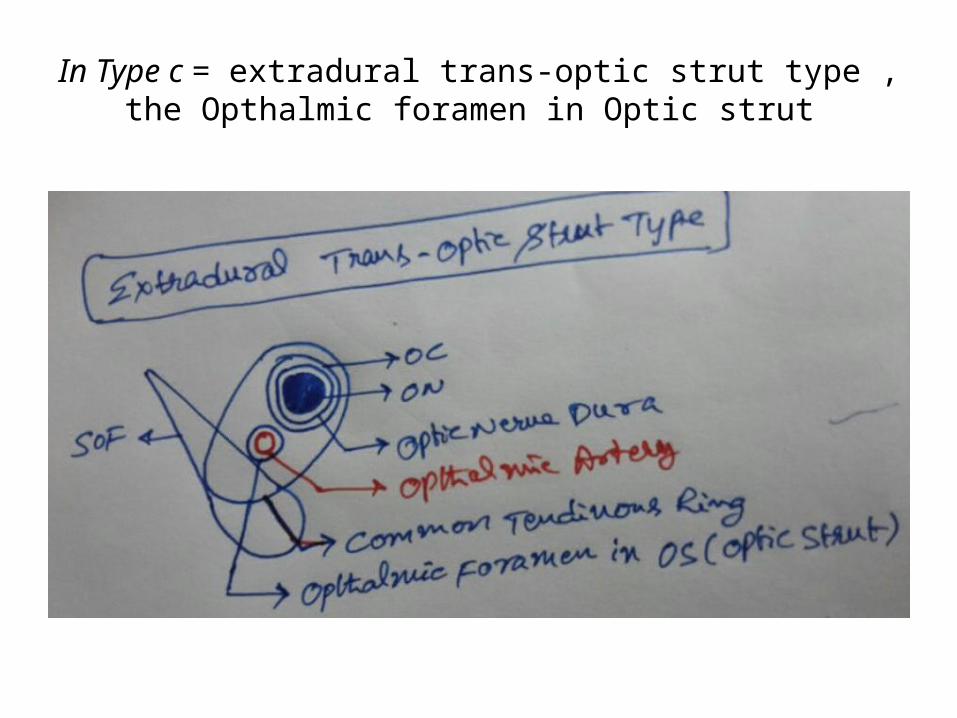
In Type c = extradural trans-optic strut type , the Opthalmic foramen in Optic strut
classification of the ophthalmic artery types http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s10143-006-0028-6-1
a = intradural type,
b = extradural supra-optic strut type [ Optic strut = L-OCR ]c = extradural trans-optic strut typeon optic nerve, pr proximal ring, cdr carotid dural
ring= upper dural ring , ica internal carotid artery I think this variation is type c
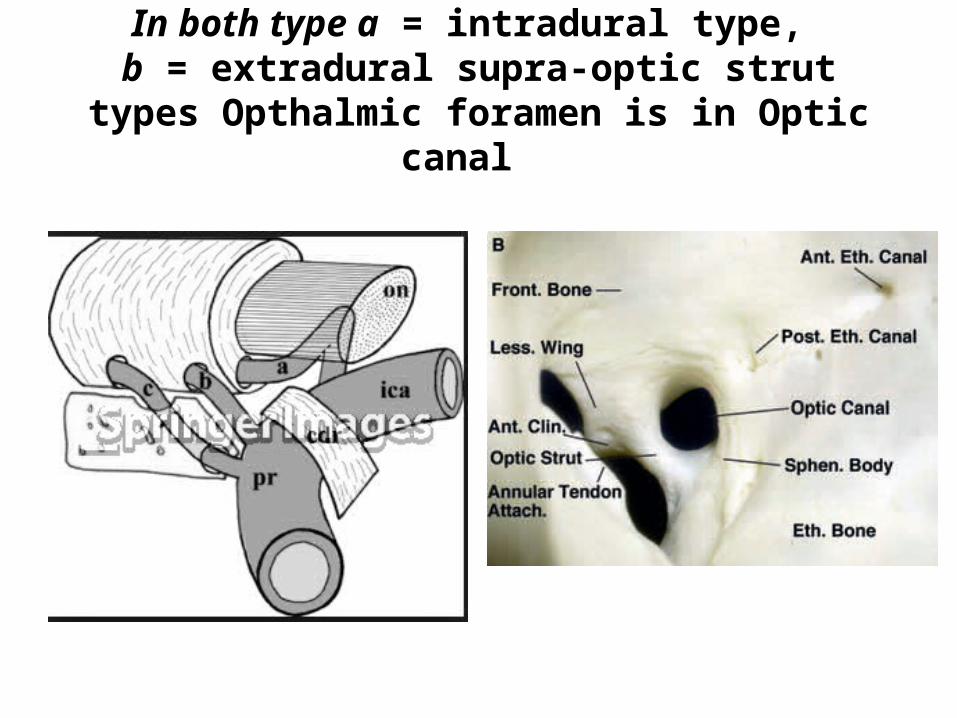
In both type a = intradural type, b = extradural supra-optic strut types Opthalmic
foramen is in Optic canal
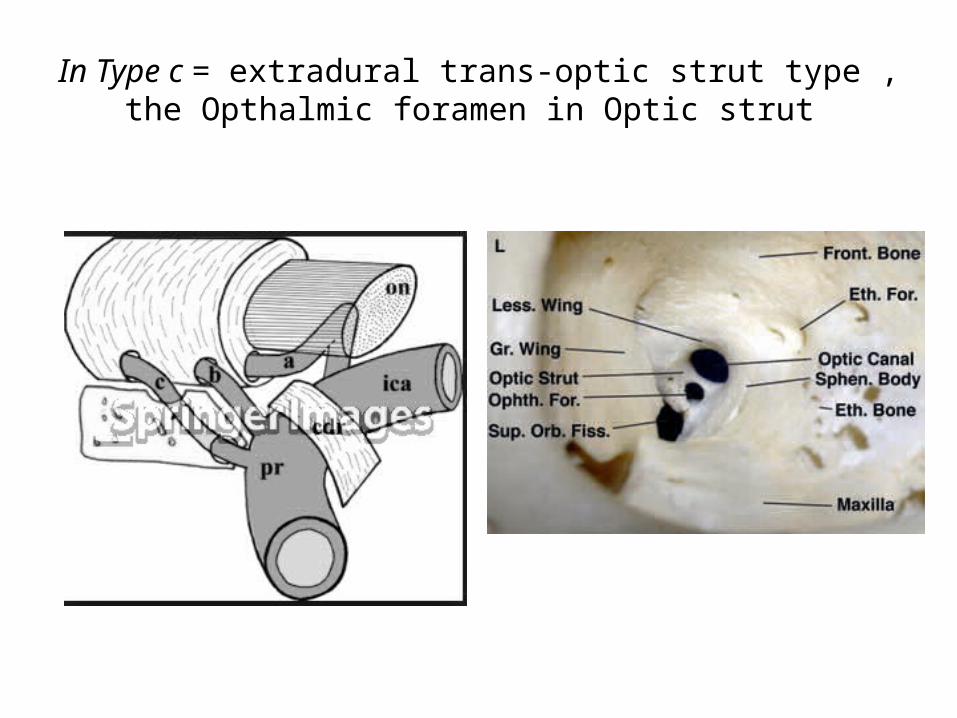
In Type c = extradural trans-optic strut type , the Opthalmic foramen in Optic strut
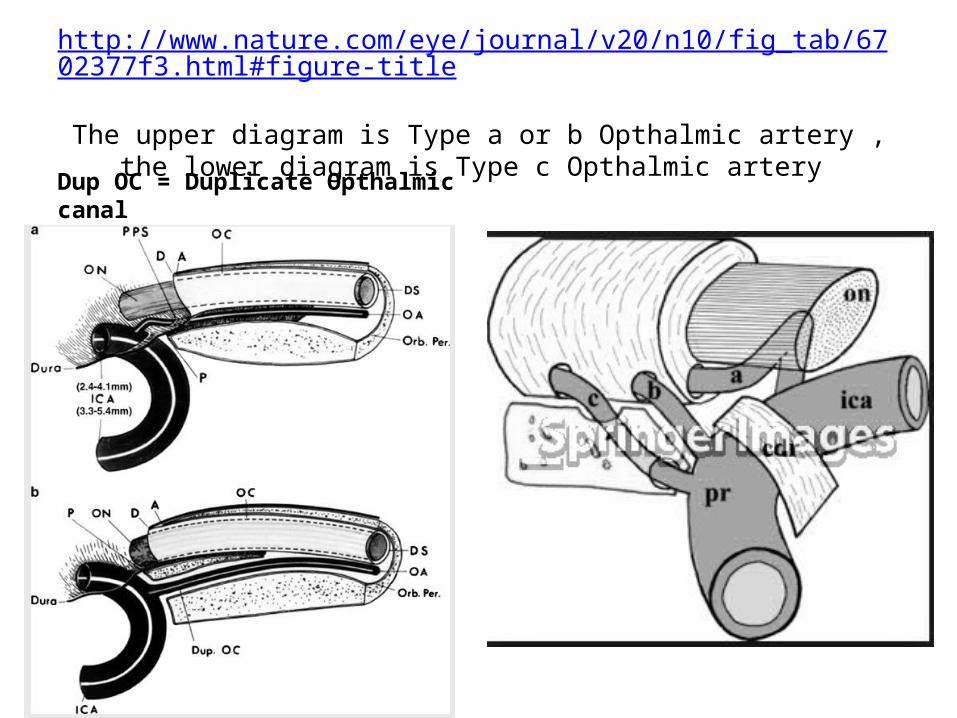
http://www.nature.com/eye/journal/v20/n10/fig_tab/6702377f3.html#figure-title
The upper diagram is Type a or b Opthalmic artery , the lower diagram is Type c Opthalmic artery
Dup OC = Duplicate Opthalmic canal
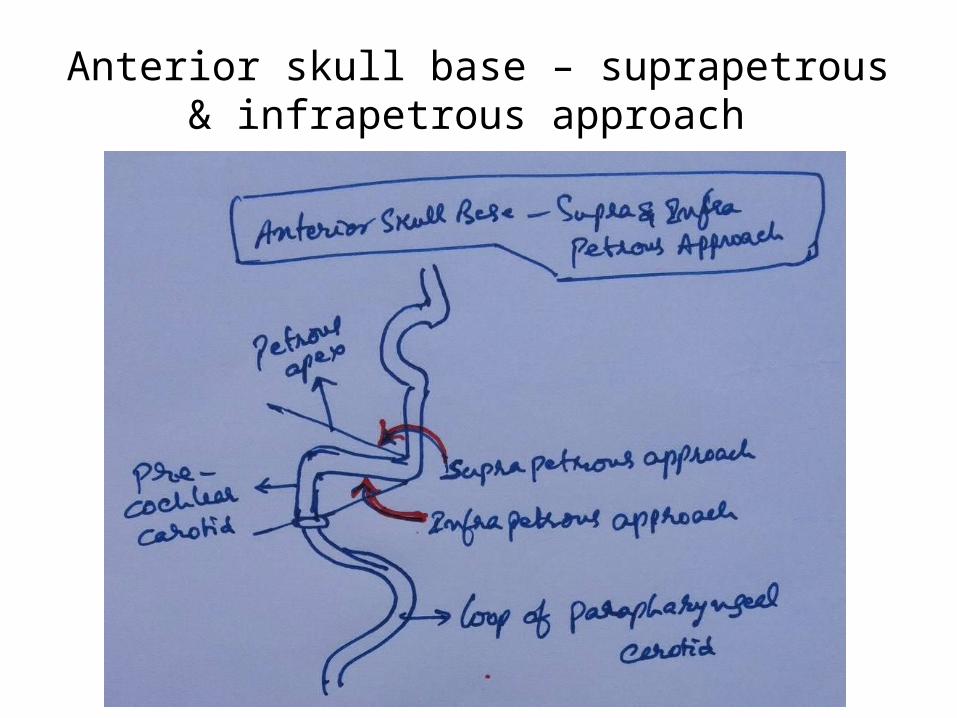
Anterior skull base – suprapetrous & infrapetrous approach
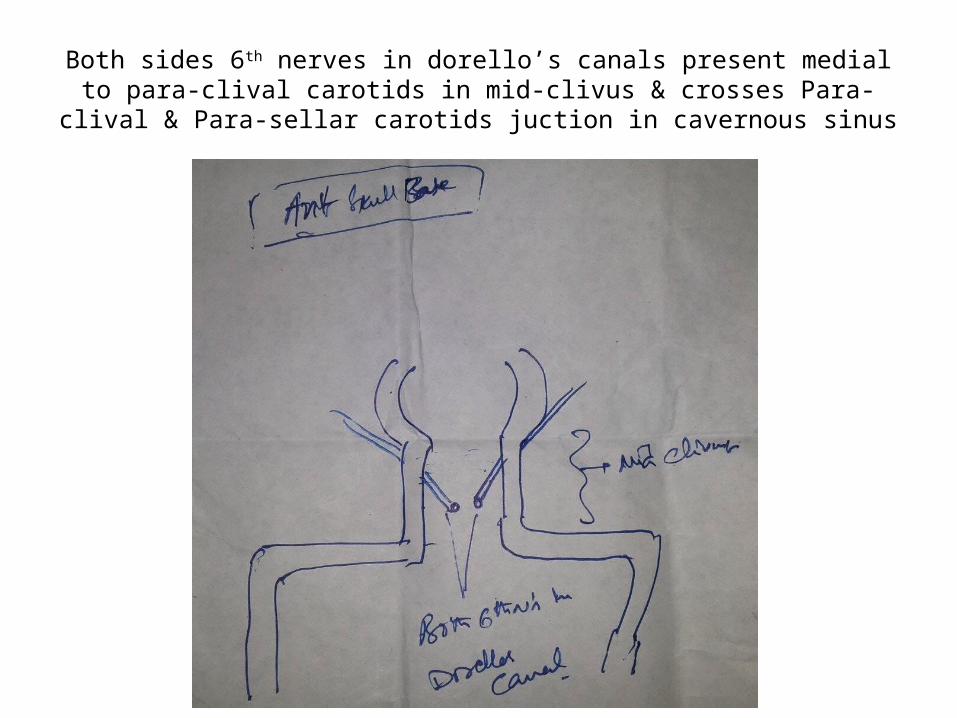
Both sides 6th nerves in dorello’s canals present medial to para-clival carotids in mid-clivus & crosses Para-clival & Para-sellar carotids
juction in cavernous sinus
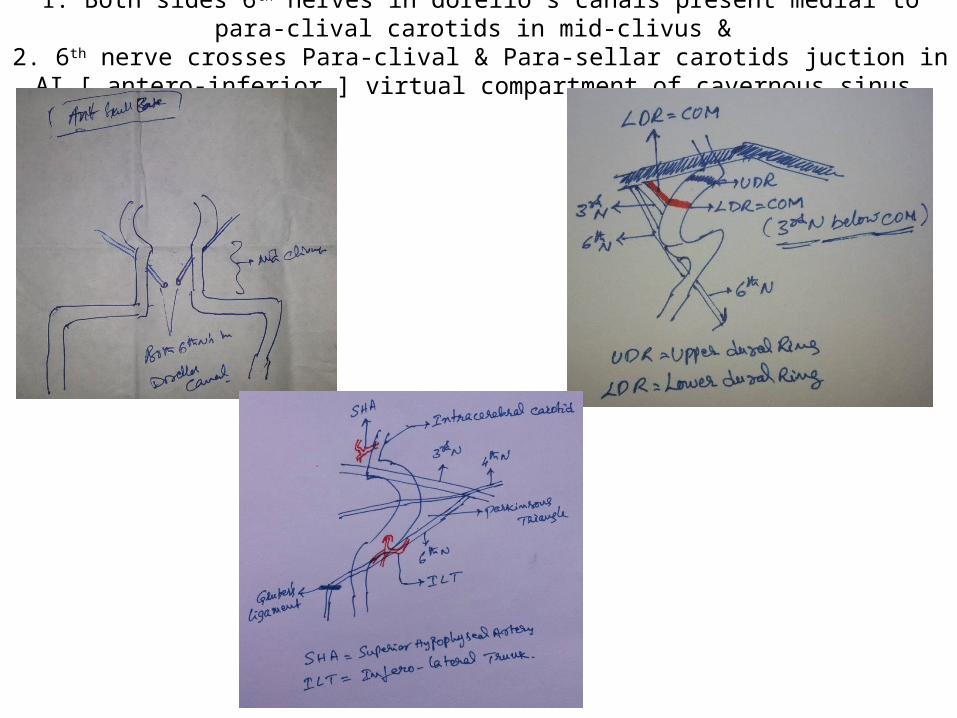
1. Both sides 6th nerves in dorello’s canals present medial to para-clival carotids in mid-clivus & 2. 6th nerve crosses Para-clival & Para-sellar carotids juction in AI [ antero-inferior ] virtual
compartment of cavernous sinus
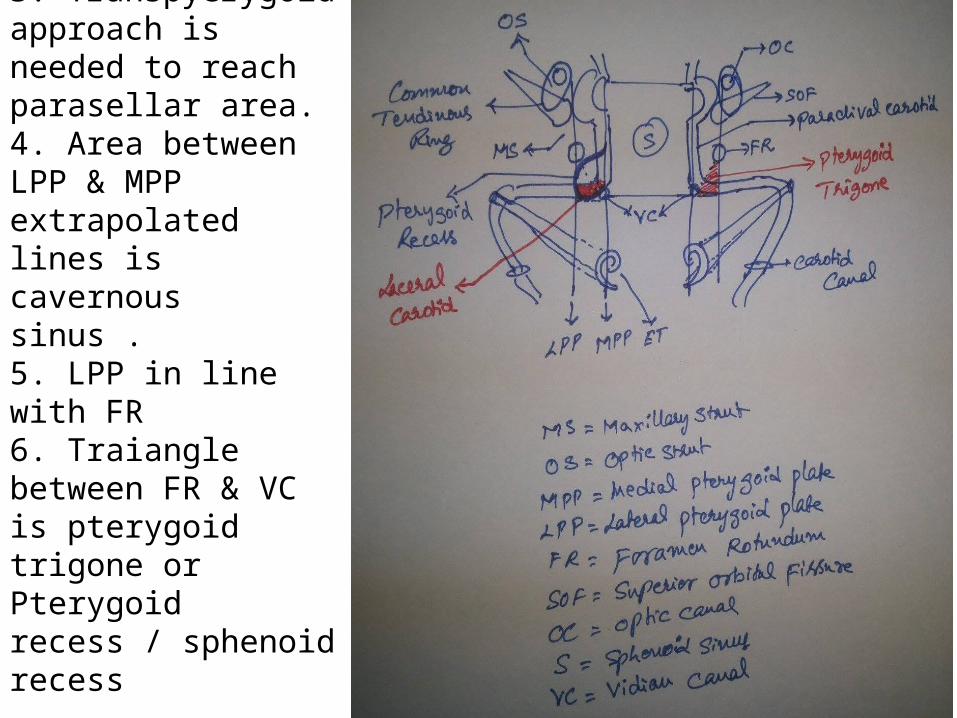
1. MPP & ET opening is in line with paraclival carotid . 2. Laceral carotid is in posterior wall of pterygoid recess / sphenoid recess. 3. Transpyerygoid approach is needed to reach parasellar area.4. Area between LPP & MPP extrapolated lines is cavernous sinus . 5. LPP in line with FR 6. Traiangle between FR & VC is pterygoid trigone or Pterygoid recess / sphenoid recess
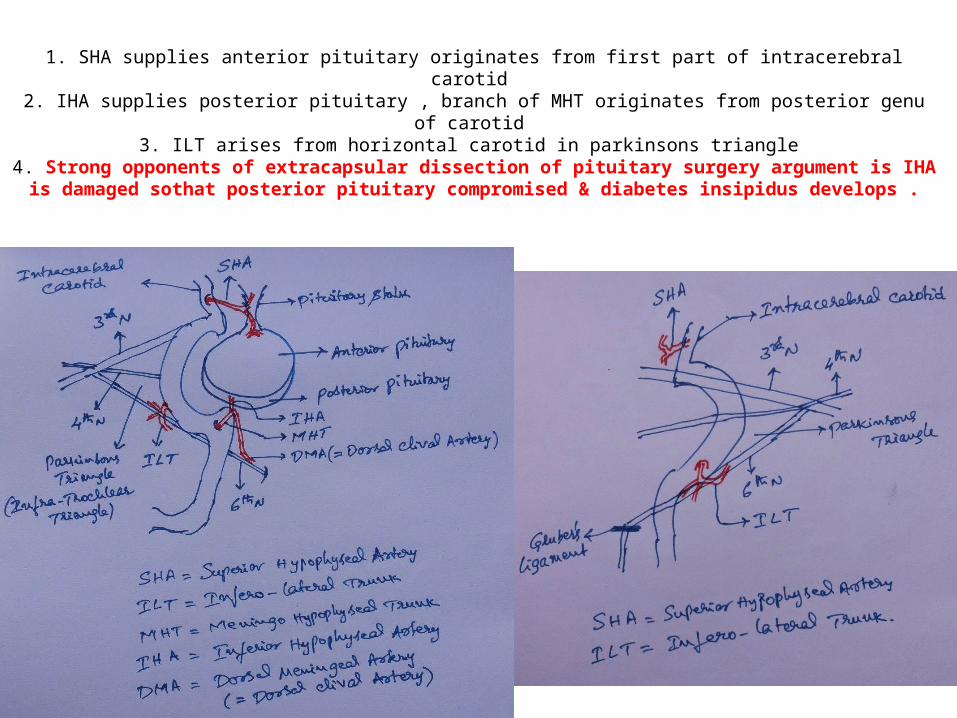
1. SHA supplies anterior pituitary originates from first part of intracerebral carotid 2. IHA supplies posterior pituitary , branch of MHT originates from posterior genu of carotid
3. ILT arises from horizontal carotid in parkinsons triangle 4. Strong opponents of extracapsular dissection of pituitary surgery argument is IHA is
damaged sothat posterior pituitary compromised & diabetes insipidus develops .