Embed Size (px)
Citation preview

Rivermead Assessment of Somatosensory
PerformanceRaiza Belarmino, Andy Phung,
Jessica Hoang, & Jasmine Vassel

Raiza Belarmino,
OTSCalifornia State University San
Marcos
BA Communication
Stanbridge University
MS Occupational Therapy

Andy Phung, OTS
California State University Fullerton
BA Health Science
Stanbridge University
MS Occupational Therapy

Jessica Hoang, OTS
California State University Long Beach
BA Psychology
Stanbridge UniversityMS Occupational Therapy

Jasmine Vassel, OTS
Azusa Pacific UniversityBA in Psychology w/
concentration in Health Psychology
Stanbridge UniversityMS in Occupational Therapy

IntroductionWhat is the somatosensory system?
Concerned with conscious perception of touch, pressure, pain, temperature, position, movement, and vibration which arises from the muscles, joints, and skin.
Who would have somatosensory impairments?
Stroke
Multiple Sclerosis
Head Injury
Spinal Cord Injury

What is the RASP?Standardized battery test designed to provide an quantifiable and
reliable assessment of somatosensory functioning
Includes standardized instruments that provide comprehensive measures of various somatosensory functions to inform and monitor rehabilitation and recovery

What is the RASP?Comprised of Seven Subtests
5 Primary Subtests
Sharp/dull discrimination
Surface pressure touch
Surface localization
Temperature discrimination
Movement and direction proprioceptive discrimination
2 Secondary SubtestsSensory extinction
Two point discrimination

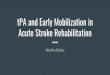
RASP Instrument: NeurometerUsed to test
Sharp/dull discrimination
Surface pressure touch
Surface localization
Sensory extinction
2 parts
Top = sharp/ dull discrimination
Lower = surface pressure touch, surface localization and sensory extinction

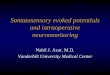
RASP Instrument: NeurotempRed and blue colored instruments with liquid crystal displays
Blue instrument displays temperatures from 6-10°C
Red instrument displays temperatures from 44-49°C

RASP Instrument: NeurodiscFour-pointed, fixed-distance, two-point discriminator
Used to establish extent of two-point discrimination on finger pads
Applied perpendicular to skin surface and parallel to the finder axis and depressed approximately 1 mm briefly
Three fixed distances: 3, 4, and 5 mm

Patient and Control SampleReliability and validity for RASP established
Inclusion Criteria: Patients with diagnosis of first ever unilateral stroke
Exclusion Criteria:Evidence of bilateral signs, noncompliance, severe visual/hearing impairment,
cognitive impairments
The presence of another neurological condition
100 patients used in standardization
Control Group:50 non brain damaged subjects

Test ReliabilityReliability established by comparing 15 different patients scored
independently by 2 different raters and the original research therapist

Patient ReliabilityAssumes that sometimes information provided can be inaccurate
Controls possible sources of unreliabilitySeries of sham trials on 2 of the 5 primary subjects
Sharp/dull discrimination
Surface pressure touch
Sham trials, also known as “non-touch” trials, are performed to control patient reliability

Sham TrialThe examiner pretends to give a stimulus when in fact none is applied
Six sham trials are conducted for each side
Helps identify patients whose performance demonstrates unreliability
Improves patient reliability by enabling the examiner to exclude those that are consistently reporting sensations on sham trials

Who uses the RASP?Medical doctors
Neurologists
General Practitioners
Physiotherapists
Occupational therapists
Speech and language pathologists
Nurses
Research Psychologists
Other clinically qualified staff
Used when health care practitioners wish to document sensory loss in a patient for clinical or research purposes
Provides a comprehensive picture of the patient’s performance
Findings can be used to inform and monitor rehabilitation and recovery.

The Patient Should BeAppropriately dressed so the examiner is able to assess all 10 areas of
the body
Have the purpose of each assessment explained to them
Always shown what the test involves prior to administration
Made aware they will first be assessed on the unaffected side
Informed they will need to keep their eyes closed for all tests
Discouraged from guessing
Reassured not to be surprised if sometimes they cannot feel anything

The Tester ShouldBe aware that altered body functions may affect test procedures and
limit access to certain test regions
Always allow for a few practice trials
Carry out testing in a quiet setting and ensure the participant is comfortable
Record relevant participant details on the score sheet
Use clinical judgment in deciding the number and types of subtests to employ

Scoring10 anatomically referenced test regions
Alternating pattern from unaffected side → affected side; head → feet
Each test region is approximately 25mm squared● Scoring is recorded on specific table/body chart
● Total score represents patient’s ability to detect and discriminate sensory stimulation
● Sham trials scored separately
False positives = 1
Maximum sham score = 2

Anatomical Reference

LimitationsAll tests require verbal responses
Subjects with speech or language difficulties will need accommodations
Examiner has 2 options for verbally impaired patients:
1. Point to pictures, objects, or words on designated cards
2. Use hand signals

Test Sequence1.Sharp/dull discrimination
2.Surface pressure touch
3.Surface localization
4.Sensory extinction
5.Two point discrimination
6.Temperature discrimination
7.Proprioception
a. Movement
b. Direction

Sharp/Dull DiscriminationEquipment needed:
2 neurometers, 2 neurotips, scoring sheet
Regions on the body to be tested:
Face (1 and 2), hand (3-6), foot (7-10)
Procedure:
Subtest administered with patient’s eyes closed
Work from unaffected to affected side, neurometer is applied to test area pseudo-randomized order (designated trial sequence)
Neurometer is applied to the subject’s skin
60 trials (30 left, 30 right) and 20 shams (10 left and 10 right)
10 test regions → 6 stimuli presented: 3 dull, 3 sharp, 2 sham in following order: S § D D S S § D

Sharp/Dull Discrimination●Explanation to patient:
○ Patient is shown two neurometers with sharp and dull ends pointed out
○ Examiner tells patient that he/she is going to test whether patient can feel sharp or dull
●Scoring:
○ Only correct detections are noted
○ Record each response for stimulus on scoring sheet
○ Test provides single score representing patient’s ability to detect sharp/dull discrimination

Sharp/Dull Scoring

Surface Pressure TouchTest equipment needed:
1 neurometer, scoring sheet
Regions on the body to be tested:
Face (1 and 2), hand (3-6), foot (7-10)
Procedure:
Subtest is administered with patient’s eyes closed
Neurometer is set to level one throughout testing
Neurometer applied to designated testing area briefly (until thick white filament tip disappears before releasing
60 trials (30 left and 30 right) and 20 shams (10 left and 10 right)
10 test regions → 6 touch (T) stimuli and 2 (§) sham trials are presented in following order: T § T T T T § T

Surface Pressure TouchExplanation to Patient:
Patients are informed that Neurpen will be used to touch areas of face, arms and legs
Examiner will say, “I want to see if you can feel this light touch. Before each trial I’m going to say “Do you feel this?”
Scoring:
Only correct discriminations are noted
Record each response on scoring sheet

Surface Pressure Touch Scoring

Surface LocalizationTest equipment needed:
1 neurometer, scoring sheet
Regions on the body to be tested:
Face (1 and 2), hand (3-6), foot (7-10)
Explanation to Patient:
Patient is requested to identify where on their body they have been touched
Responses can be verbal or on the body chart
If the patient indicates they have not felt the stimulus, it can be repeated once

Surface LocalizationProcedure:
Test is administered with the patient’s eyes closed
Neurometer is set to level one
Total of 60 trials (30 left and 30 right) are administered
Sequence of touches: 1 (unaffected side), 2 (affected side), 3 (unaffected side), 9 (affected side), 2 (unaffected side), 3 (affected side)
No sham trials

Surface Localization ScoringOnly correct localizations are recorded

Sensory ExtinctionTest equipment needed:
2 neurometers, scoring sheet
Regions on the body to be tested:
Face and hand
Explantation:
Explain to the patients that they may feel one or two touches on similar area either by itself or at the same time (e.g. hands and face)
Procedure:
Examiner sets the neurometer to level two and see if the patient can feel the stimulus on the affected side. If not, the test is discontinued.
When testing only affected arm, the individual closes their eyes and the examiner apply the neurometer until the tip just disappears before releasing.
When testing both arms, the examiner apply both neurometers simultaneously with the same testing condition.

Sensory Extinction ScoringScores are obtained for left and right brain damaged patients and are
divided into face and hand

Two-point DiscriminationTest equipment needed:
Discriminator, scoring sheet
Regions on the body to be tested:
Fingertip of index finger on both hands
Explantation:
Show the patient the discriminator and explain how it will be used to find out whether they can feel one or two points on the tip of their index finger
Procedure:
Test is administered with patient closing their eyes and other parts of the hand does not come in contact with the discriminator
Discriminator is applied to the fingertip either a single point or one of the two points within the range of 3mm - 5mm
Testing starts on the unaffected side first
Testing is discontinued if the patient fails between one and two points between the three distances

Two-point Discrimination ScoringPatients that failed to detect within 3-5 mm range are considered to
show impairment.

Temperature DiscriminationTest equipment needed: 2 Neurotemps, scoring sheet
Regions on the body to be tested: face (1 and 2), hand (3-6), foot (7-10)

Temperature Discrimination Procedure●Explanation to patient: “I am going to use these Nuerotemps to test whether
you can feel warm or cold. Just before the trial I am going to say “What’s this?” Don’t worry if you don’t feel all the trials and remember to indicate only warm or cold”
●Procedure:○ Ensure Nuerotemps are at the end of the temp window (Warm = 44-49°C, Cold =
6-10°C) prior to administering the test
○ Place Neurometer for up to 1 second on patient
○ For each of the 10 test regions 6 stimuli are presented (for a total of 60 trials)
■ 3 warm and 3 cold in the following order - WCCWWC
○ Each of the patient’s response are recorded in the corresponding box

Temperature Discrimination Scoring

Proprioception Movement/Direction Discrimination
Test equipment needed:
Scoring sheet
Joints to be tested:
Elbow (L/R), wrist (L/R), thumb or finger (L/R), ankle, toe (L/R)
Explanation to patient:
Say: “I am going to move your [elbow, etc] up and down and I want you to tell me whether you can feel me moving this joint and in which direction. Up is towards your head and down is towards your feet. Before each trial I am going to say ‘What’s this?’ Don’t worry if you don’t feel all the trials and remember only to indicate when you’re actually feel something.

Proprioception Movement/Direction Discrimination
Procedure:
Patient is given several practice trials and instructed to close their eyes
Each joint should be held by lateral surfaces
Starting position may be up to 20° either side of the mid-joint
Only move each joint approximately 20°
Each joint is moved 6 times in the following order: up, down, down, up, up down
Wait 1-2 seconds between movements
No sham trials

Proprioceptive Movement Discrimination ScoringScoring depends on the detection of movement
Movement or no movement

Proprioceptive Direction Discrimination Scoring Scoring depends on the detection of direction of movement
Up or down

References Busse, M. & Tyson, S.F. (2009). How many body locations need to be tested when assessing sensation after stroke? An investigation of redundancy in the Rivermead Assessment of Somatosensory Performance. Clinical rehabilitation, 23, 91-95. doi: 10.1177/0269215508097296Connell, L.A., Lincoln, N.B., & Radford, K.A. (2008). Somatosensory impairment after stroke: frequency of different deficits and their recovery. Clinical Rehabilitation, 22, 758-767. doi: http://dx.doi.org/10.1177/0269215508090674Helliwall, S. (2009). Does the use of a sensory re-education programme improve the somatosensory and motor function of the upper limb in subacute stroke? A single case experimental design. The British Journal of Occupational Therapy, 72(12), p. 551-558. doi: https://doi.org/10.4276/030802209X12601857794853Winward, C.E., Halligan, P.W., & Wade D.T. (2002). The Rivermead Assessment of Somatosensory Performance (RASP): standardization and reliability data. Clinical Rehabilitation, 16, 523-533. doi: http://dx.doi.org/10.1191/0269215502cr522oaWinward, C.E., Halligan, P.W., & Wade D.T. (2007). Somatosensory recovery: A longitudinal study of the first 6 months after unilateral stroke. Disability and Rehabilitation, 29(4), 293-299. doi: 10.1080/09638280600756489
Wu, C., Chuang, I., Ma, H., Lin, K., & Chen, C. (2016). Validity and responsiveness of the revised nottingham sensation assessment for outcome evaluation in stroke rehabilitation. The American Journal of Occupational Therapy, 70(2). doi:10.5014/ajot.2016.018390

QUESTIONS?

THANK YOU