Embed Size (px)
DESCRIPTION
Radiology, X-ray Contrast Exams Image Review
Citation preview
Contrast Exam~~~~~~~
Image Review
1
The following information is only a personal suggested guideline to
follow when positioning for Contrast exams.
For additional information on positioning of these exams, please
reference your Radiographic Positioning and Related Anatomy
Textbook. 2
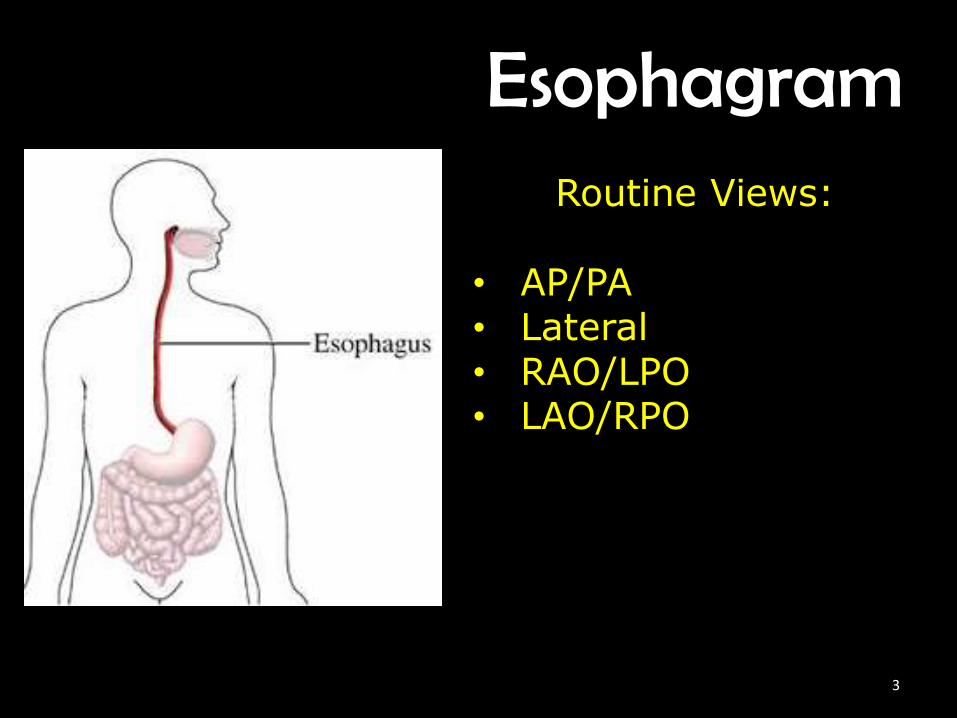
EsophagramRoutine Views:
• AP/PA• Lateral• RAO/LPO• LAO/RPO
3

AP/PA Esophagram• Body is supine or prone• Align MS to midline• Ensure no rotation• CR ┴ to IR
• CP is to T5-T6(3”inferior to jugular notch)
• Collimate a hand width• Instruct patient to swallow
barium/expose
4
5
Lateral Esophagram• Body is in lateral recumbent• Midcoronal plane to midline• Ensure no rotation• CR ┴ to IR
• CP is to T5-T6(3”inferior to jugular notch)
• Collimate a hand width• Instruct patient to swallow
barium/expose
6
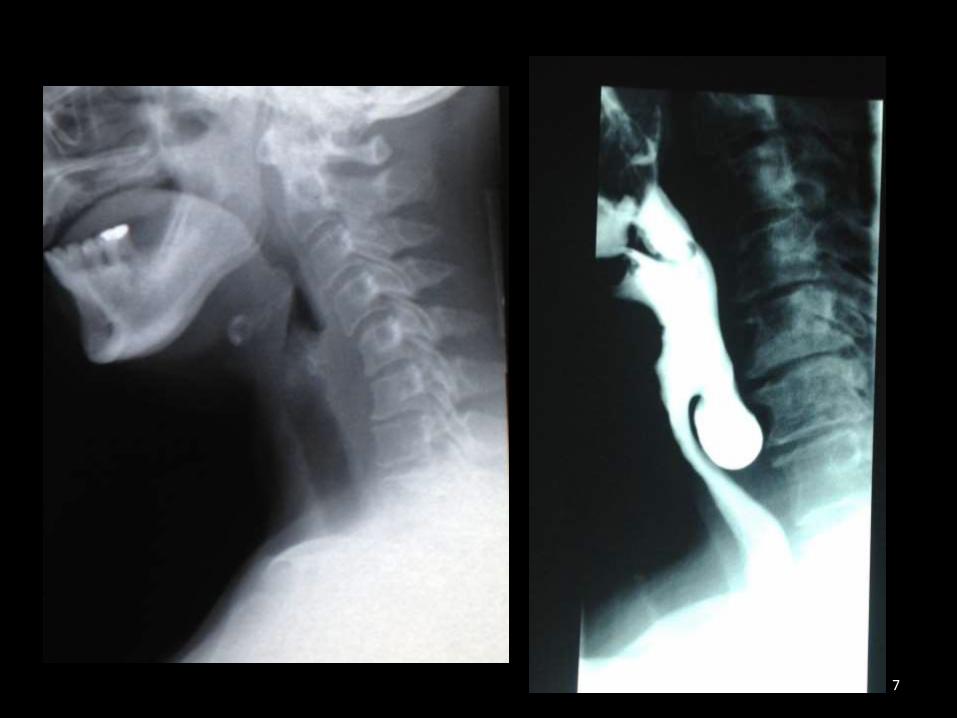
7
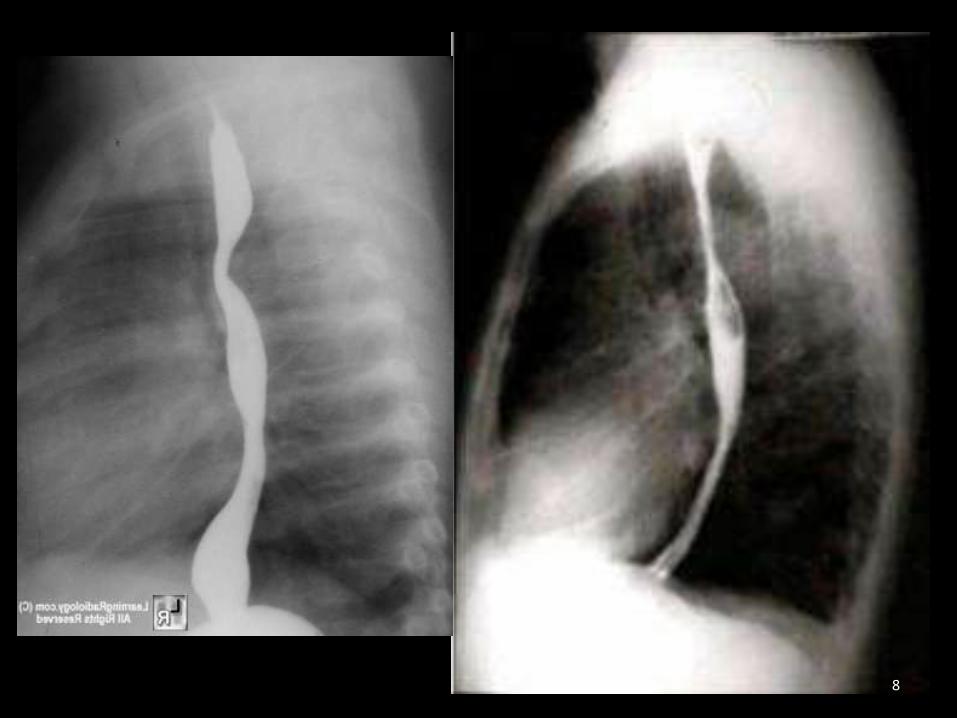
8
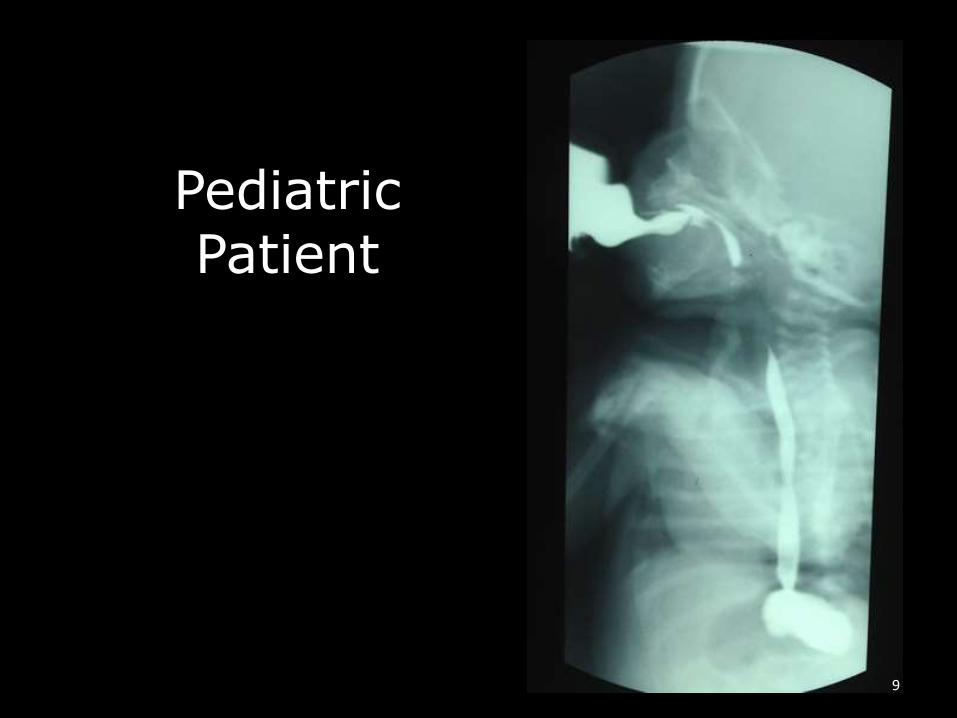
Pediatric Patient
9
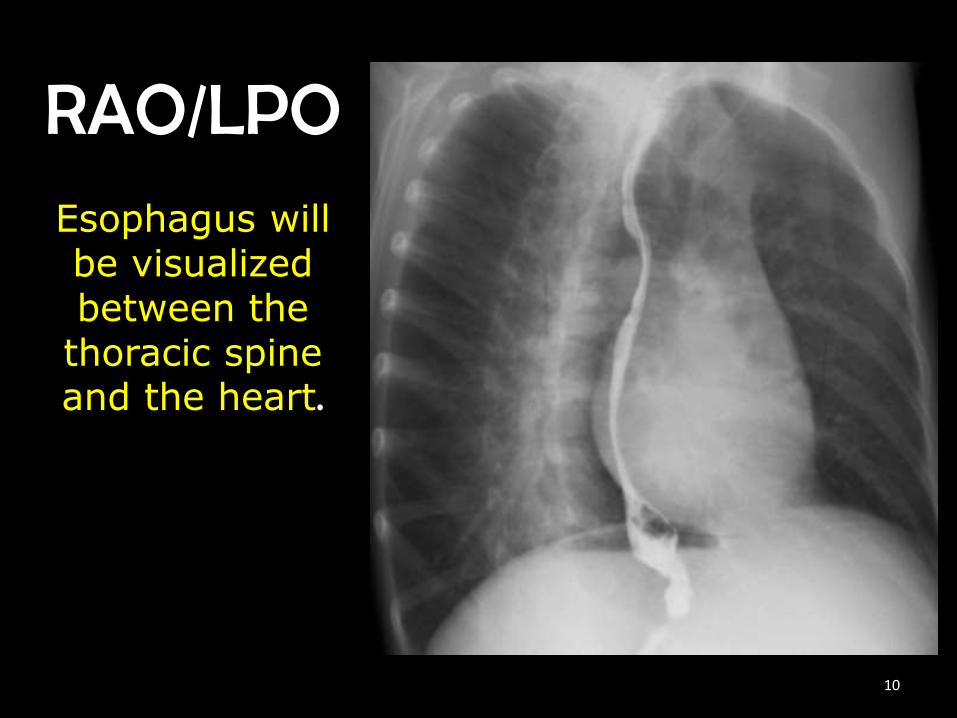
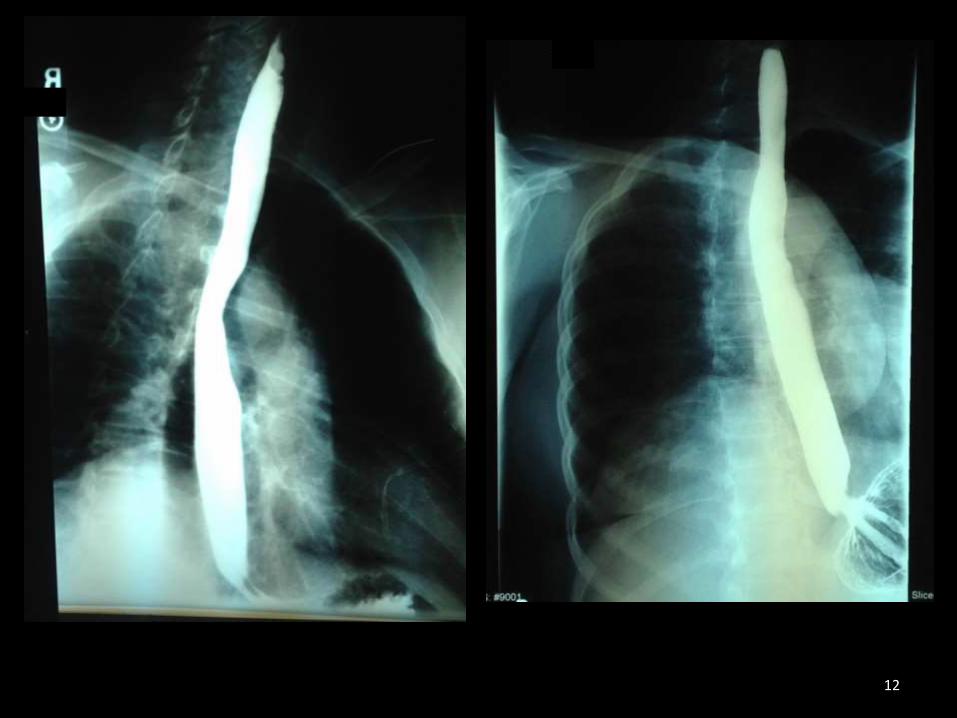
RAO/LPOEsophagus will be visualized between the
thoracic spine and the heart.
10
RAO/LPO Esophagram• Body is rotated 35°-40°
• CR ┴ to IR
• CP is to T5-T6(3”inferior to jugular notch)
• Collimate to hand width
• Instruct patient to swallow barium/expose
11
12

13
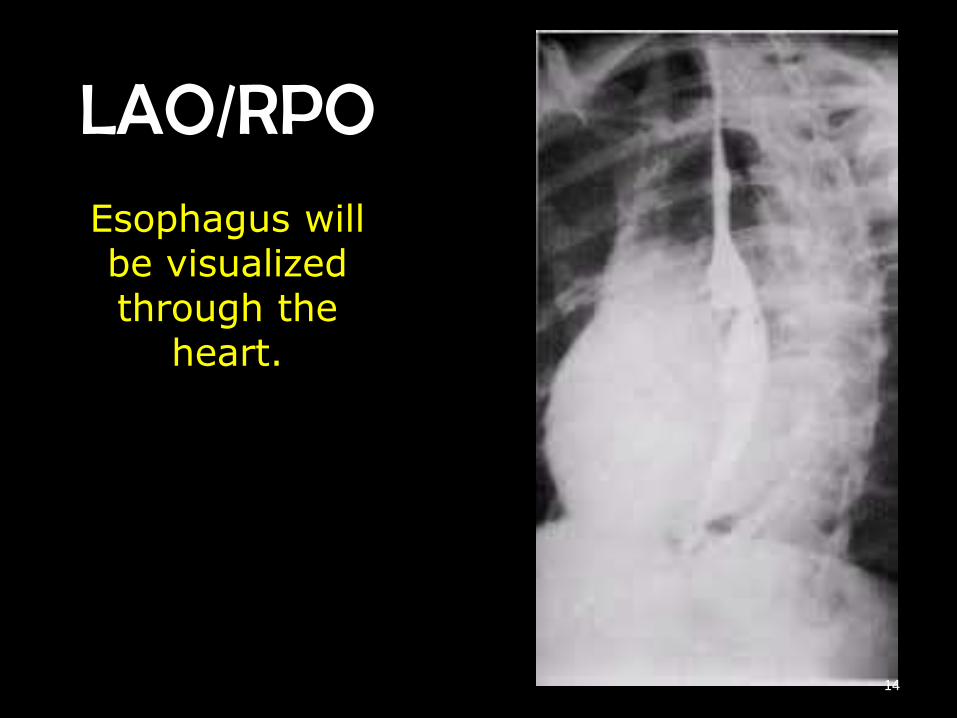
LAO/RPOEsophagus will be visualized through the
heart.
14
LAO/RPO Esophagram• Body is rotated 35°-40°
• CR ┴ to IR
• CP is to T5-T6(3”inferior to jugular notch)
• Collimate to hand width
• Instruct patient to swallow barium/expose
15
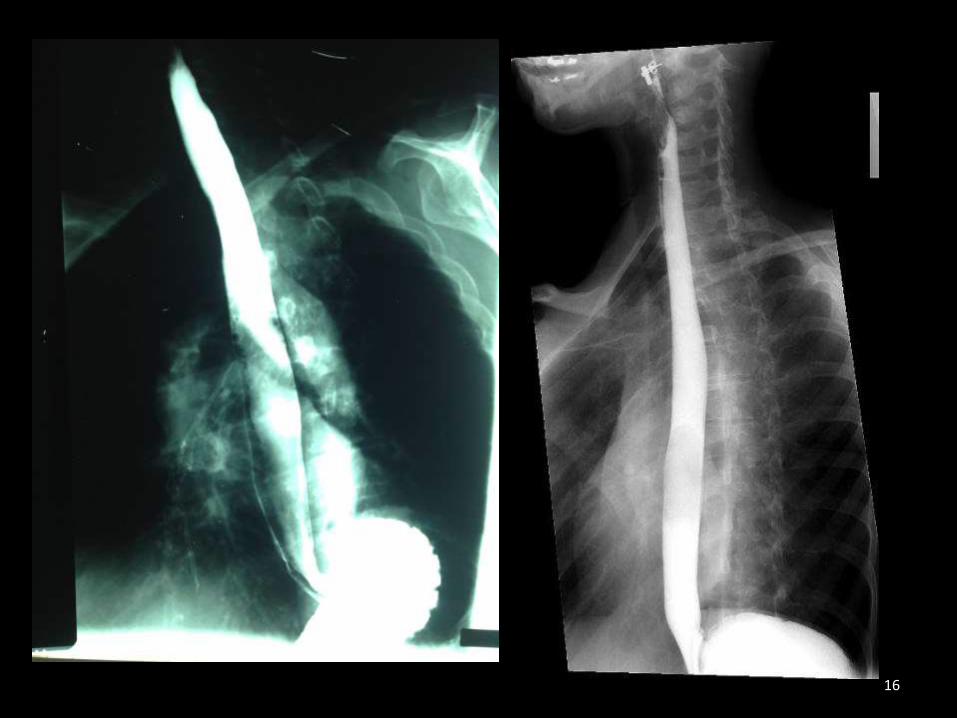
16
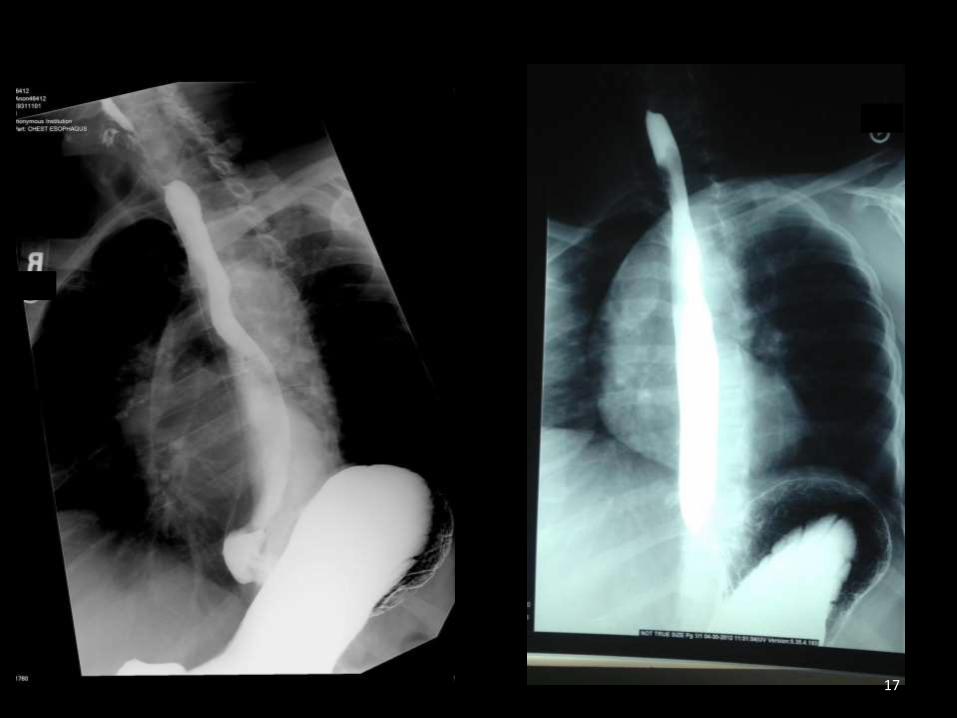
17
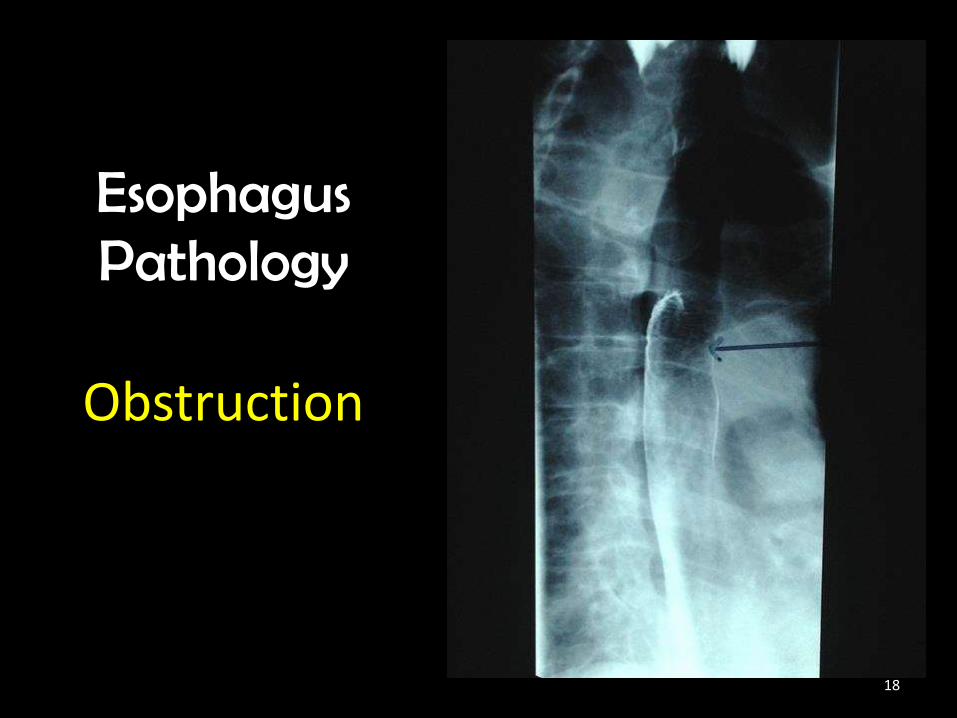
EsophagusPathology
Obstruction
18
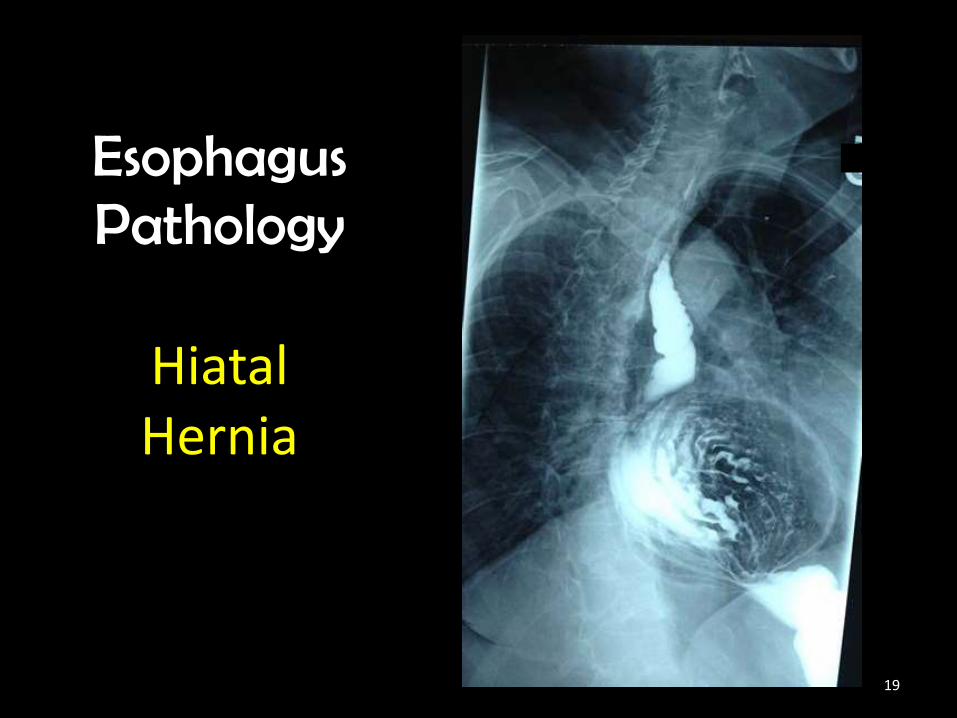
EsophagusPathology
Hiatal Hernia
19
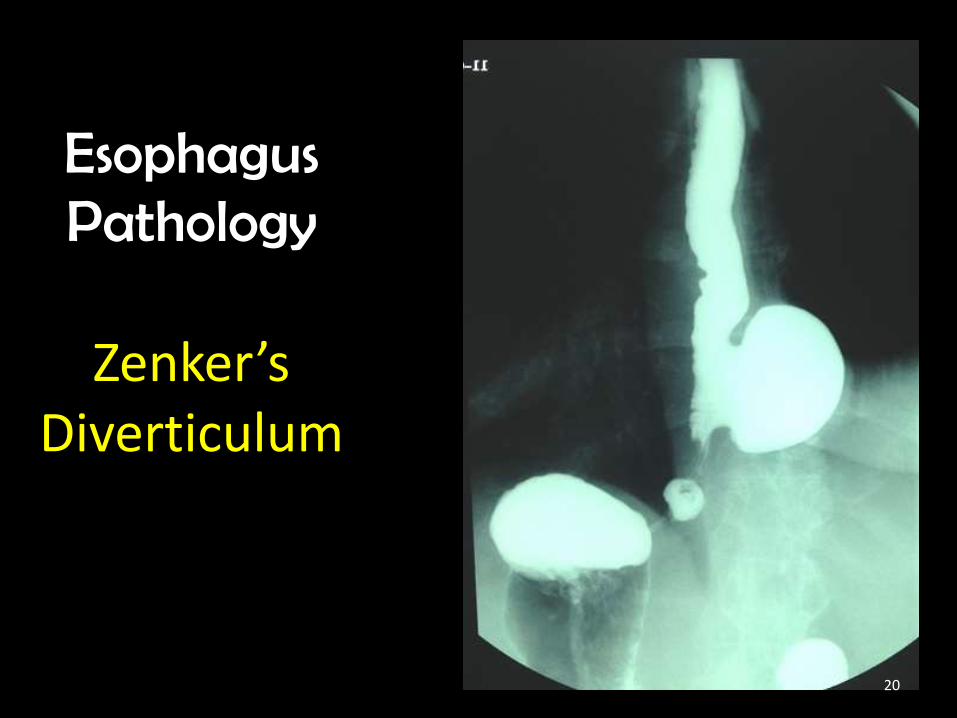
EsophagusPathology
Zenker’sDiverticulum
20
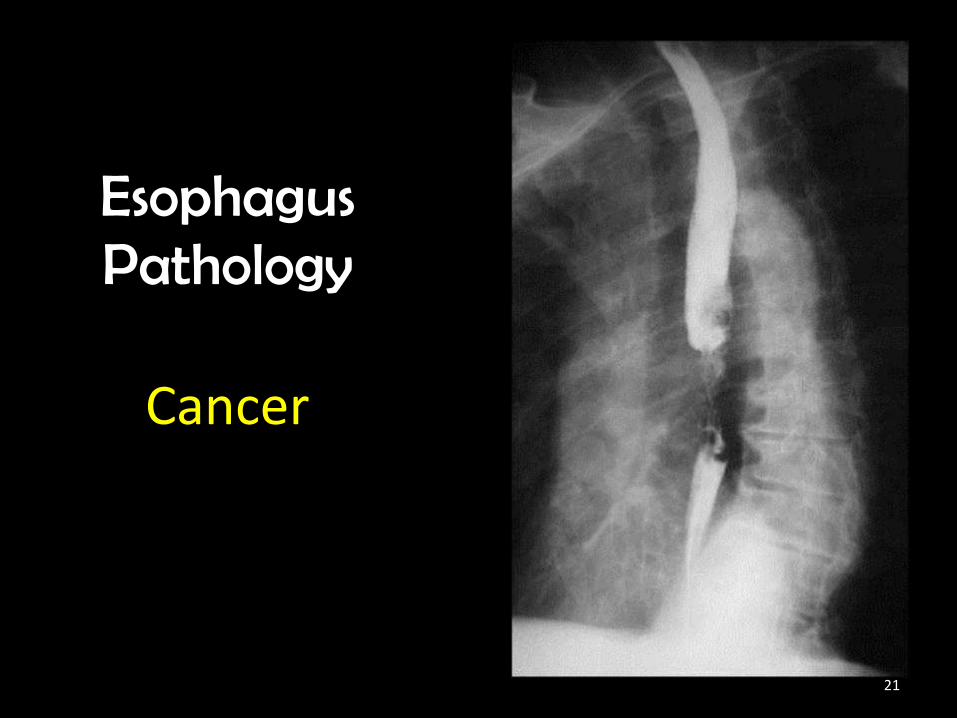
EsophagusPathology
Cancer
21
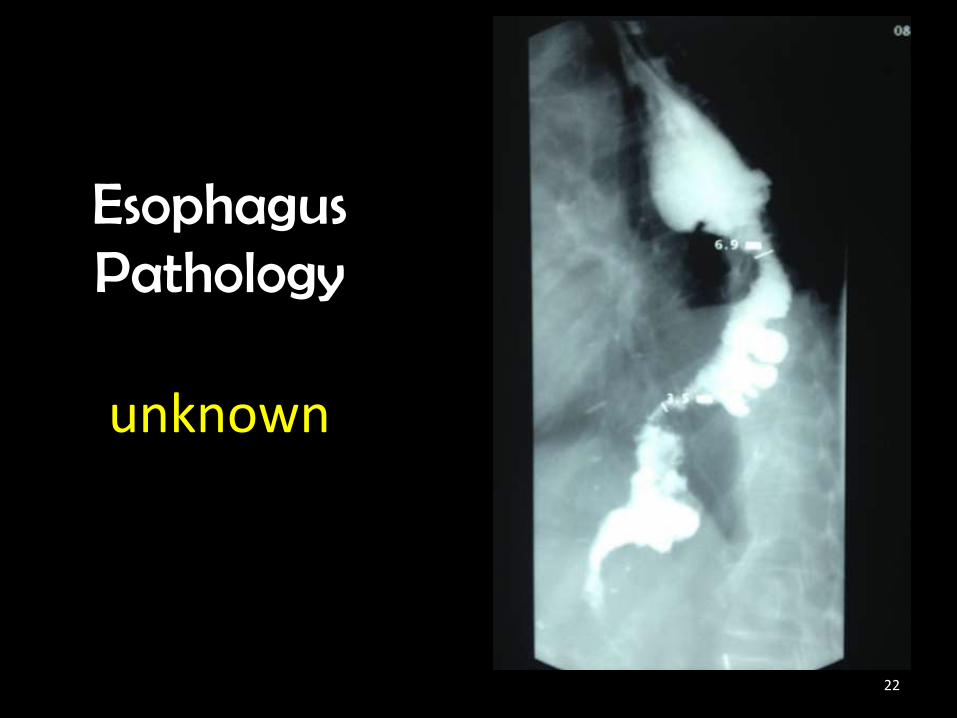
EsophagusPathology
unknown
22
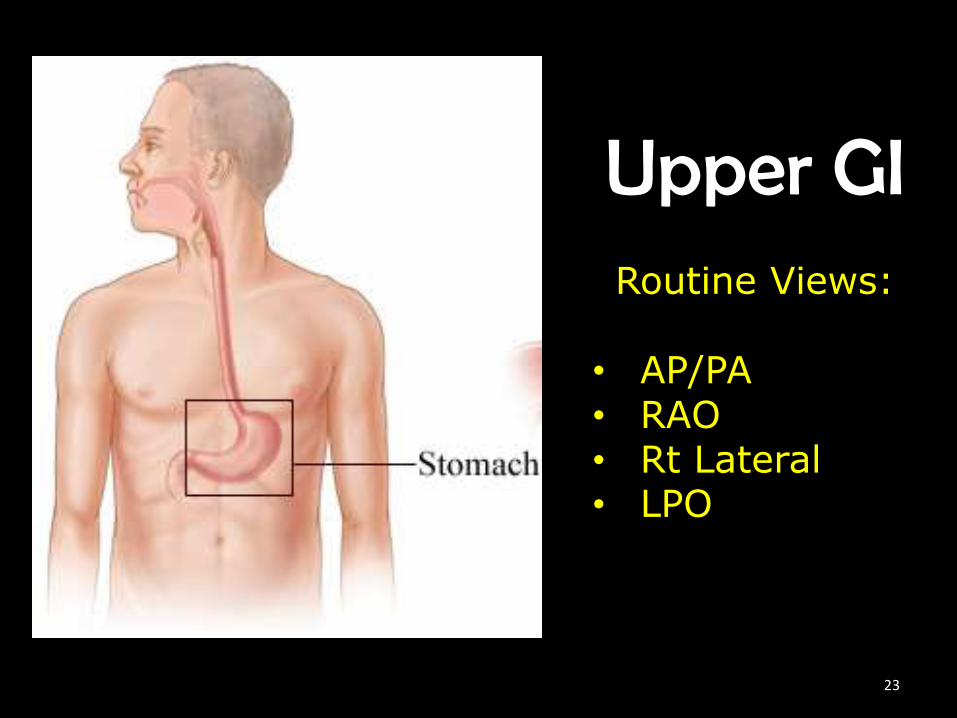
Upper GIRoutine Views:
• AP/PA• RAO• Rt Lateral• LPO
23

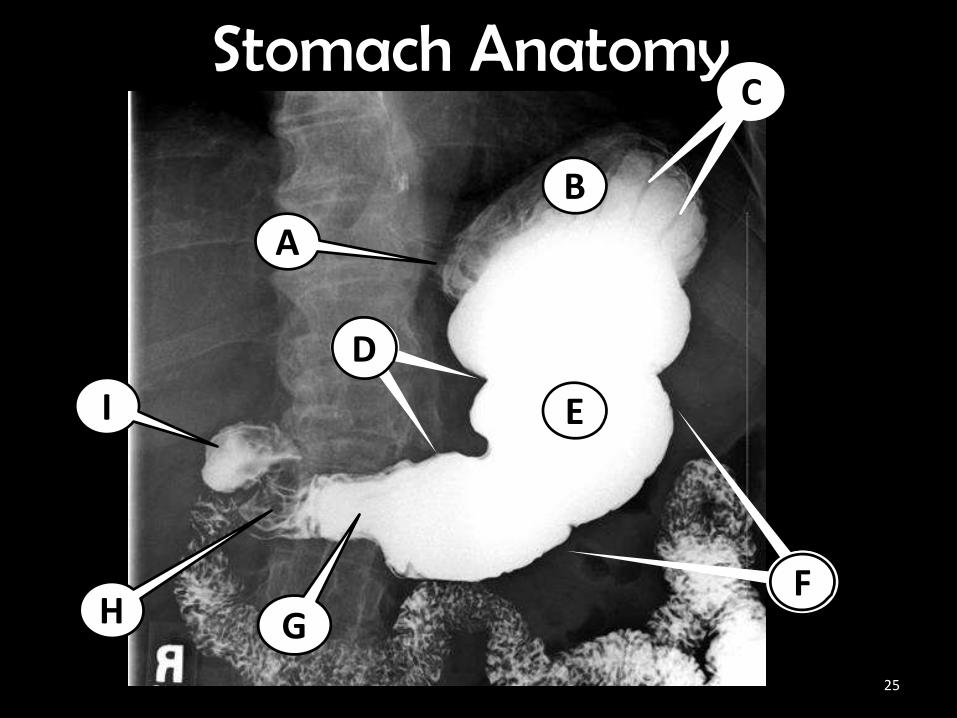
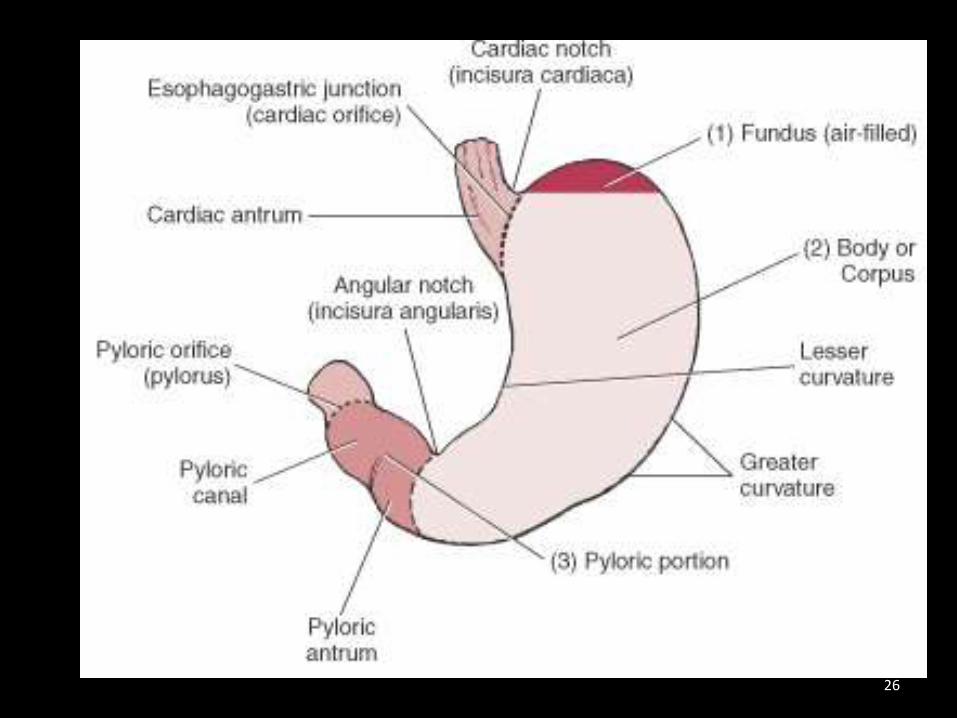
Upper Gastrointestinal System
24
I E
A
C
A
H
E
G
Stomach AnatomyC
F
D
B
25
26
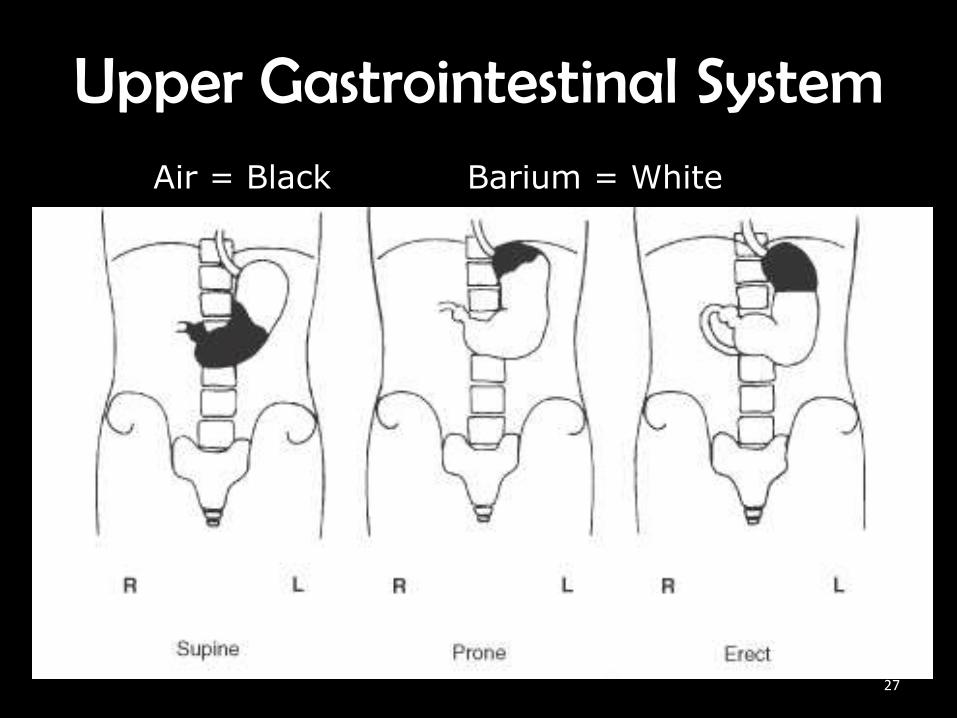
Upper Gastrointestinal SystemAir = Black Barium = White
27

For all stomach images…Ask yourself:
What is in the fundus?What is the spine doing?
28
AP/PA UGI• Body is recumbent
• Ensure no rotation
• CR ┴ to IR
• CP for Sthenic is to L1* & 1” left of midline
• CP for Hypersthenic is 2” above L1 & near midline
• *one hand width above crest29
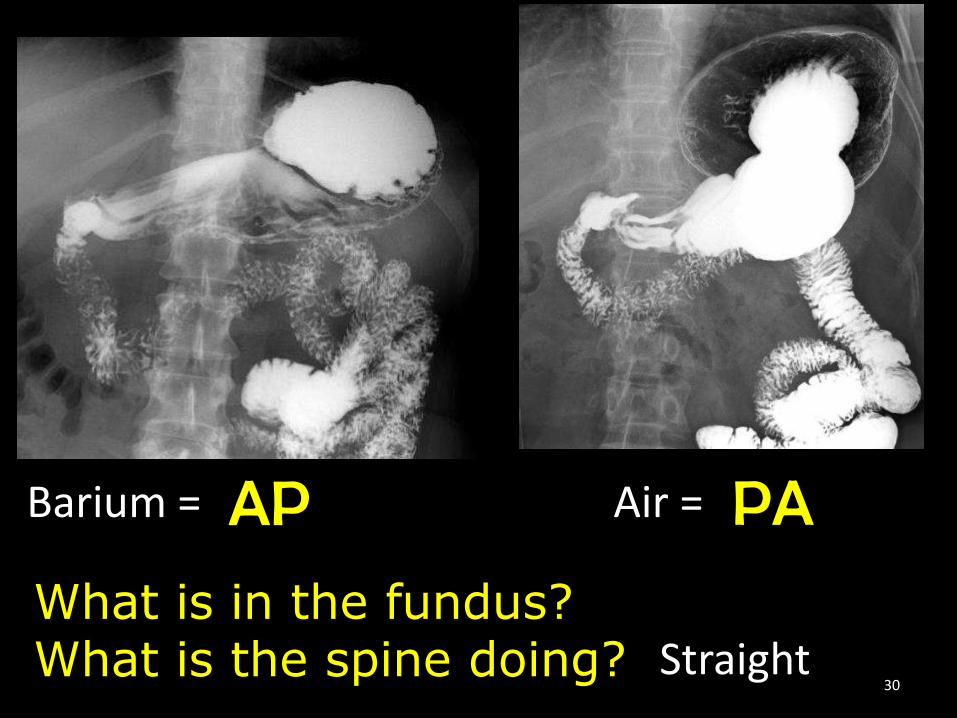
AP PA
What is in the fundus?What is the spine doing? Straight
Barium = Air =
30
RAO UGI• Body is rotated 40°-70°
• CR ┴ to IR
• CP for Sthenic is to L1* -w/45°-55° Oblique
• CP for Hypersthenic is 2” above L1 - w/70° Oblique
• And midway between spine & upside lateral abdomen
• *one hand width above crest31
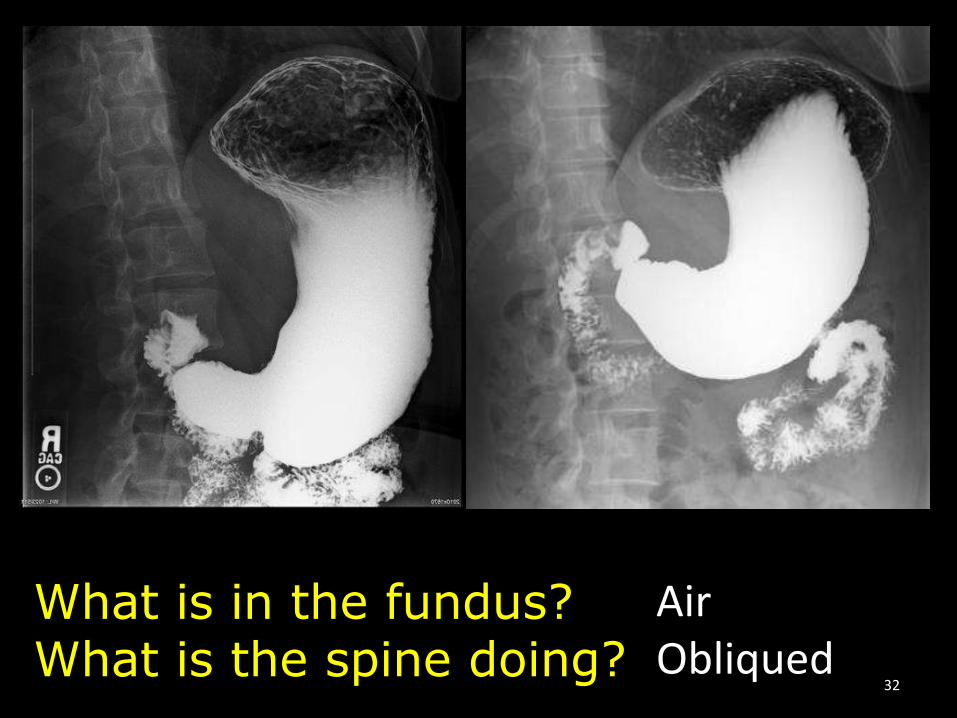
What is in the fundus?What is the spine doing?
AirObliqued
32
Lateral UGI• Body is in lateral recumbent• Midcoronal plane to midline• Ensure no rotation• CR ┴ to IR
• CP for Sthenic is to L1* & 1-2” anterior to MC plane
• CP for hypersthenic is 2” above L1
• * one hand width above crest
33
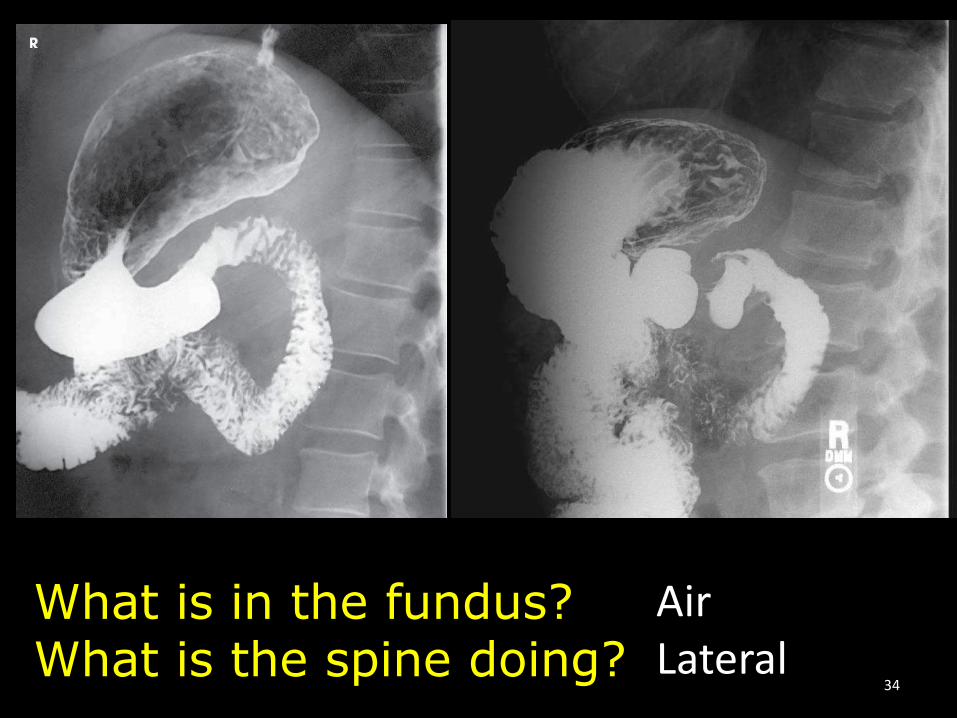
What is in the fundus?What is the spine doing?
AirLateral
34
LPO UGI• Body is rotated 30°-60°
• CR ┴ to IR
• CP for Sthenic is to L1* w/45° Oblique
• CP for hypersthenic is 2” above L1 - w/60° Oblique
• And midway between MS & left lateral abdomen
• * one hand width above crest35
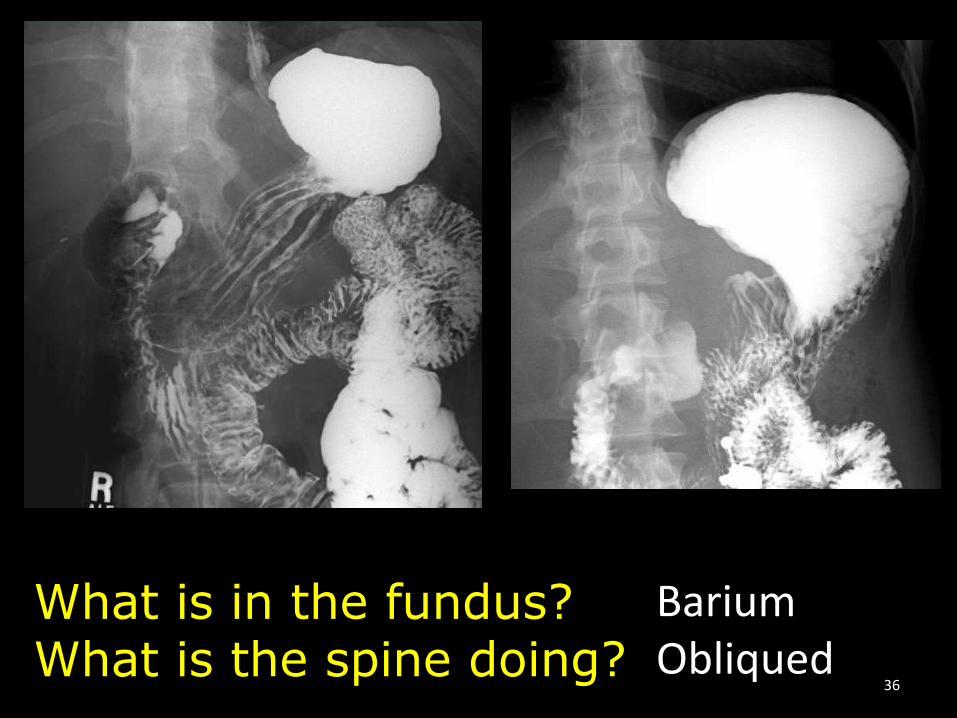
What is in the fundus?What is the spine doing?
BariumObliqued
36
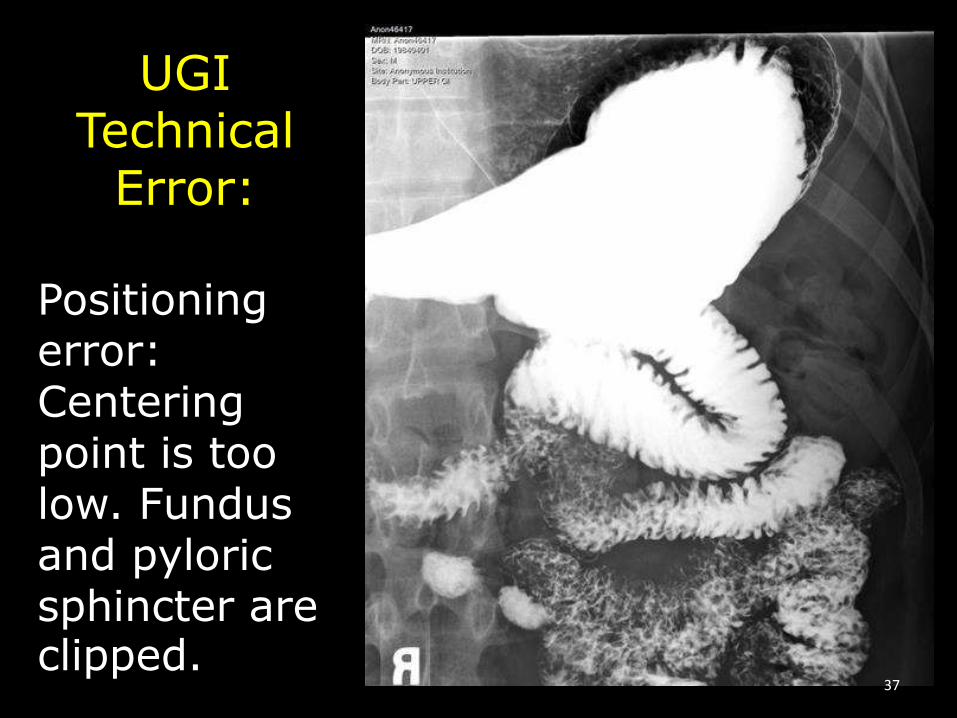
UGITechnical
Error:
Positioning error:Centering point is too low. Fundus and pyloric sphincter are clipped.
37

UGITechnical
Error:
Positioning error:Centering point is too low. Fundus is clipped.
38
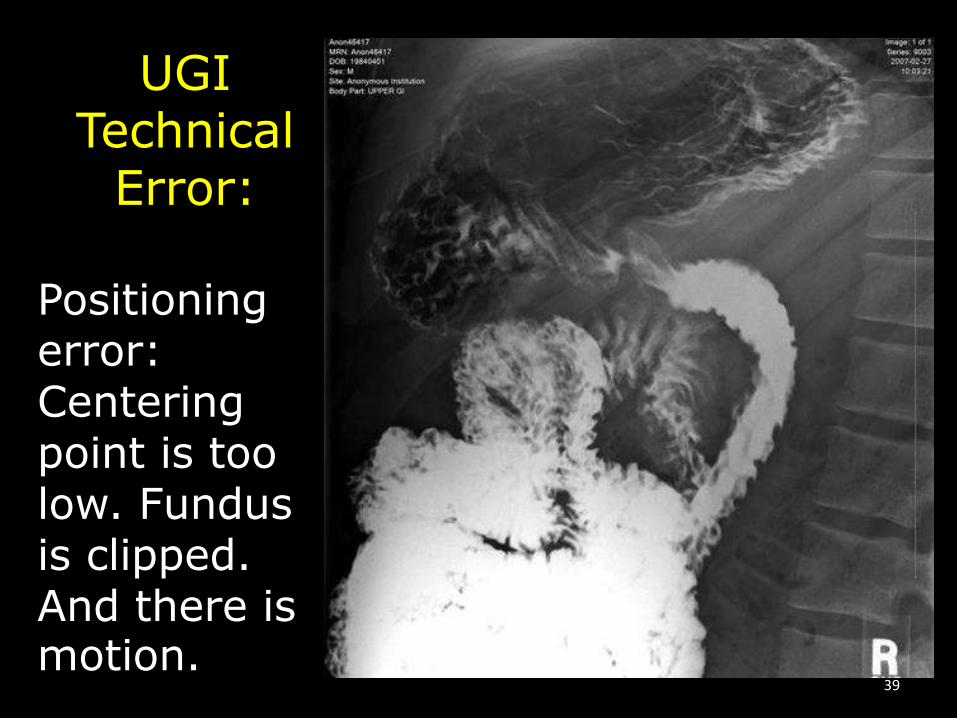
UGITechnical
Error:
Positioning error:Centering point is too low. Fundus is clipped. And there is motion.
39
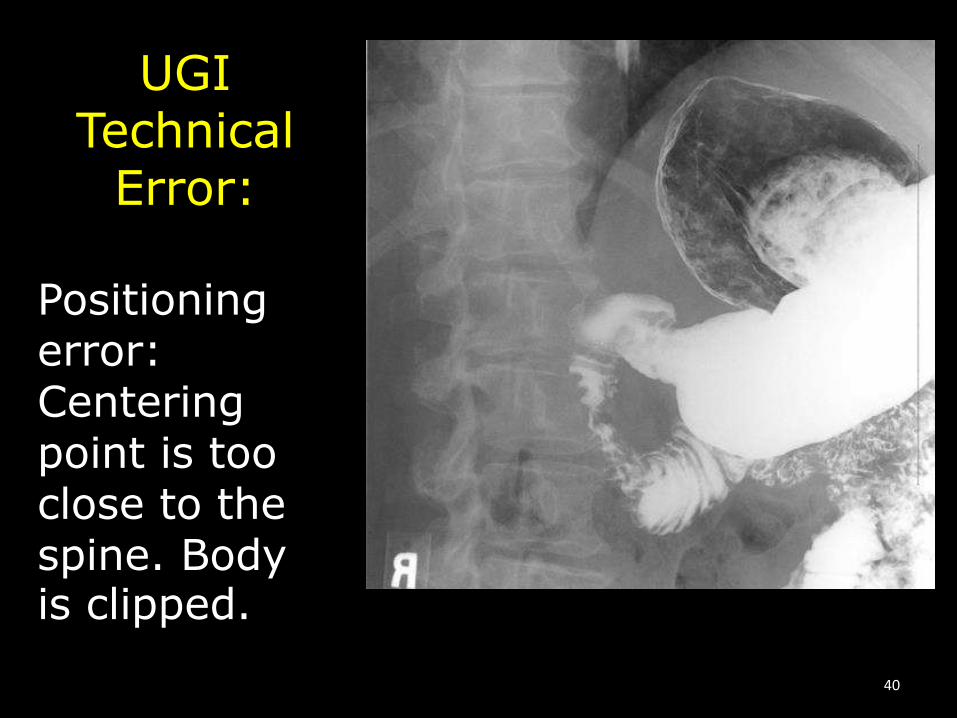
UGITechnical
Error:
Positioning error:Centering point is too close to the spine. Body is clipped.
40
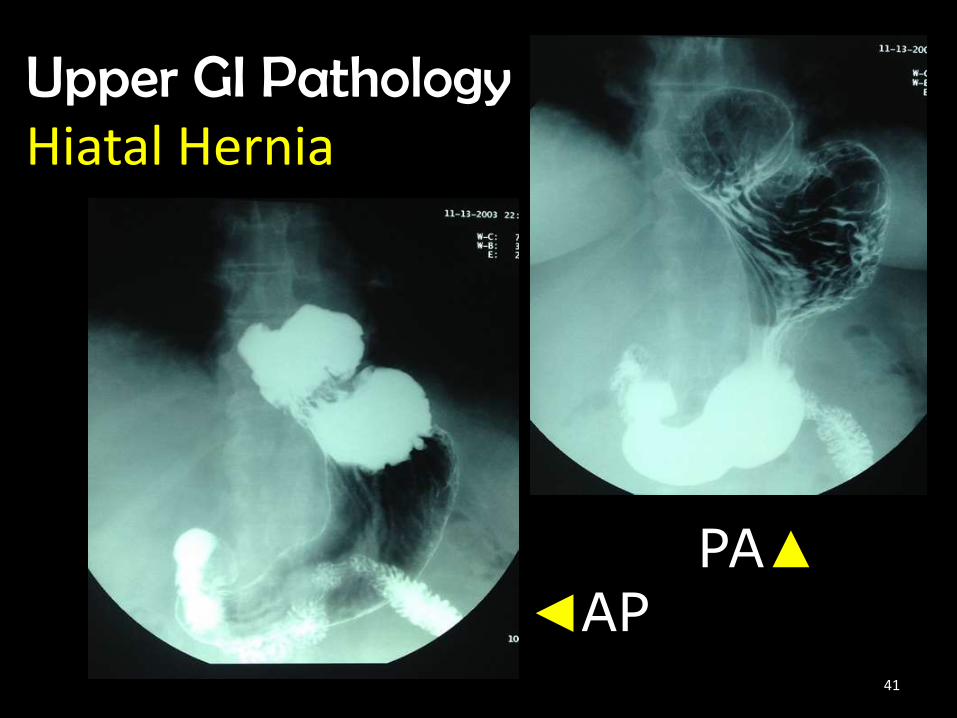
Upper GI PathologyHiatal Hernia
PA▲
◄AP41

Upper GIPathology
J-peg tube
42
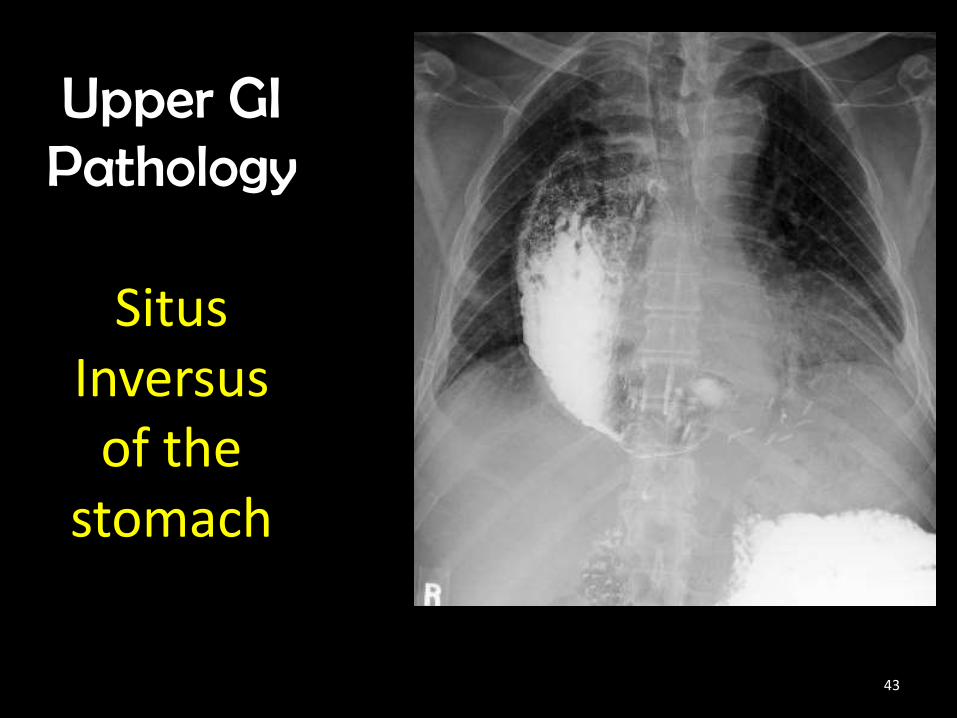
Upper GIPathology
SitusInversus
of the stomach
43
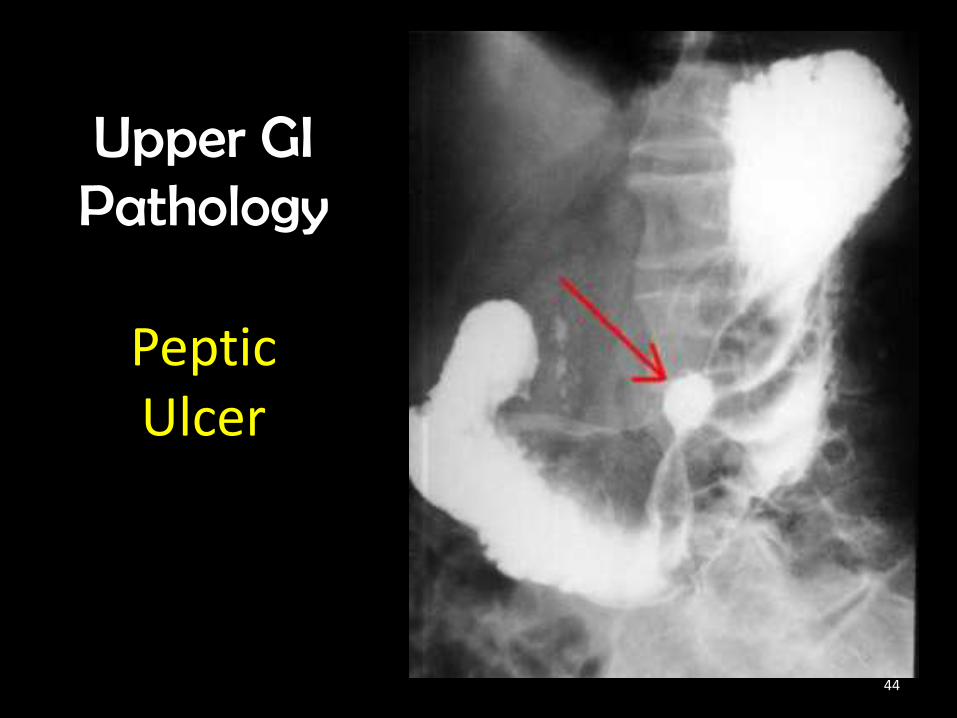
Upper GIPathology
Peptic Ulcer
44

Upper GIPathology
Pyloric Stenosis
45

Upper GIPathology
Bezoar
46
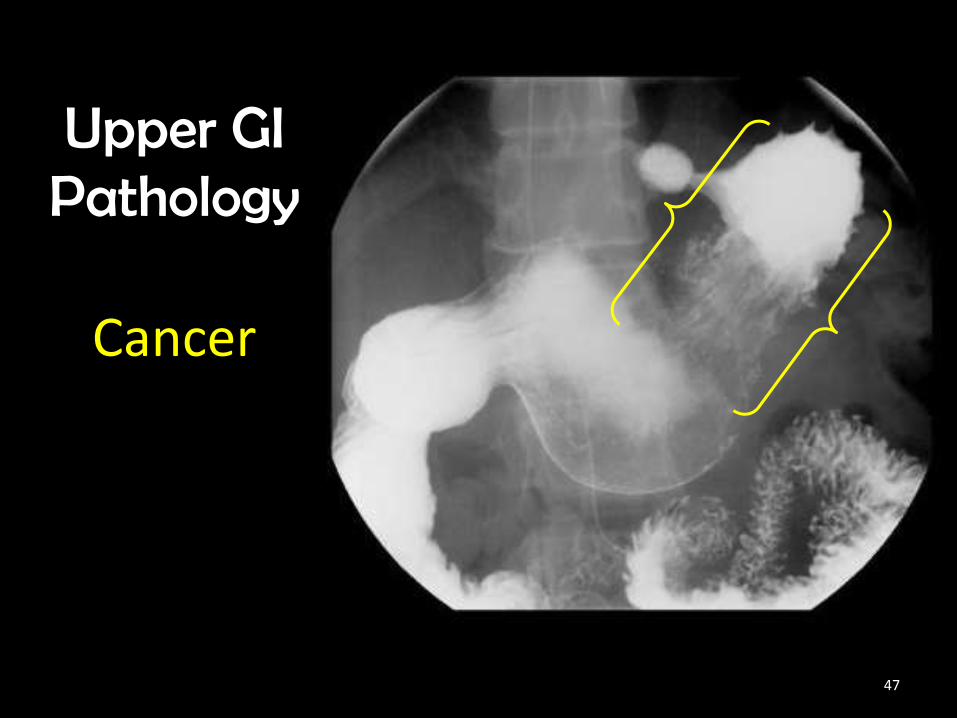
Upper GIPathology
Cancer
47

Upper GIPathology
Cancer
48
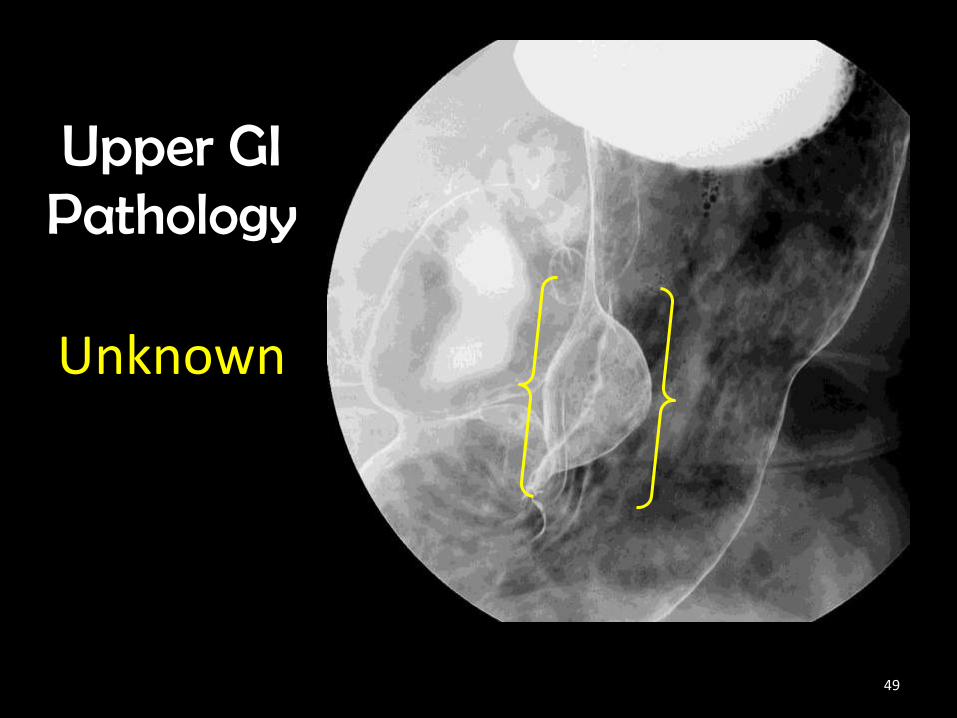
Upper GIPathology
Unknown
49
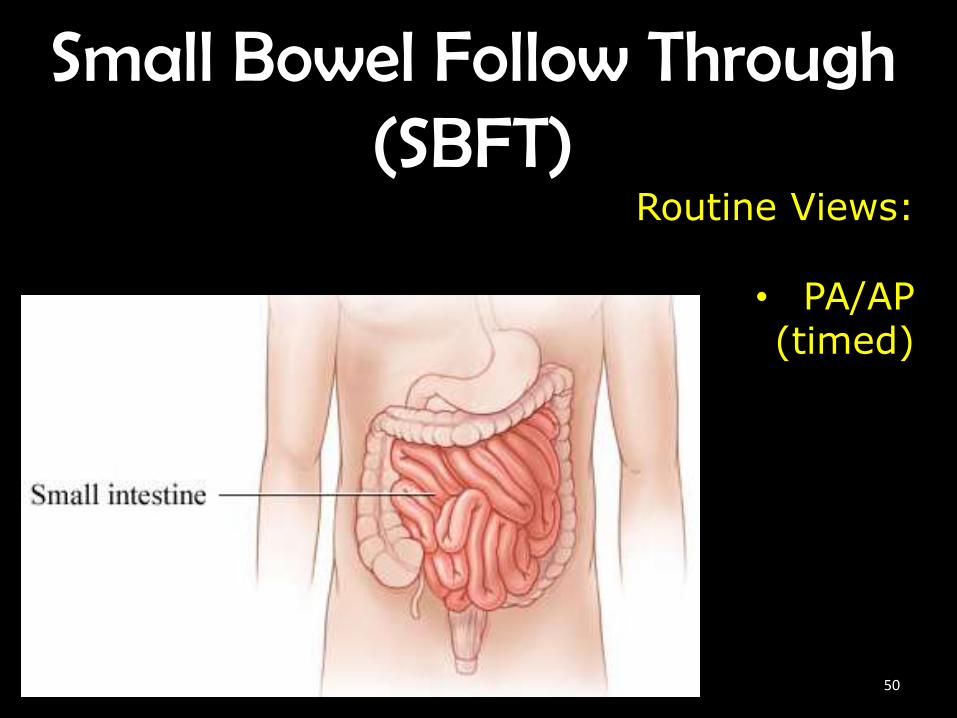
Small Bowel Follow Through (SBFT)
Routine Views:
• PA/AP(timed)
50

(SBFT)Small Bowel Follow Through• The prone position allows
abdominal compression to separate the various loops of bowel, creating a higher degree of visibility. However follow departmental protocols
51
(SBFT)Small Bowel Follow Through
• Depending on departmental protocol, the Immediate, 15 & 30 min. images are generally centered at least 2” above crest. Additional timed images thereafter are centered at the crest to include pubic bone.
52

(SBFT)Small Bowel Follow Through
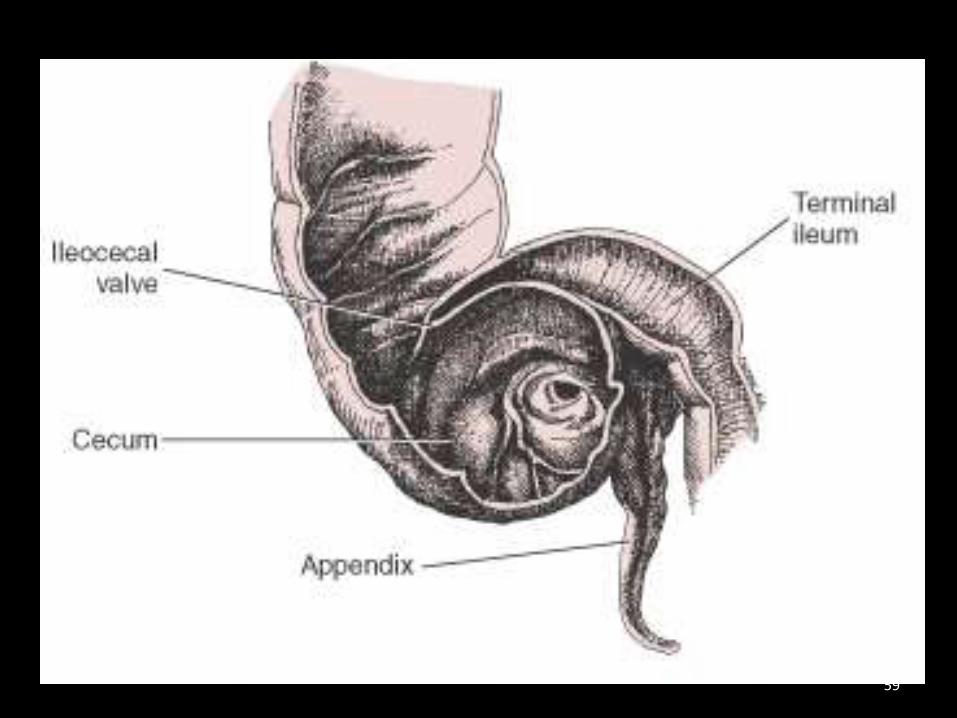
• SBFT is complete when the barium enters through the ileocecal valve into the cecum.
53
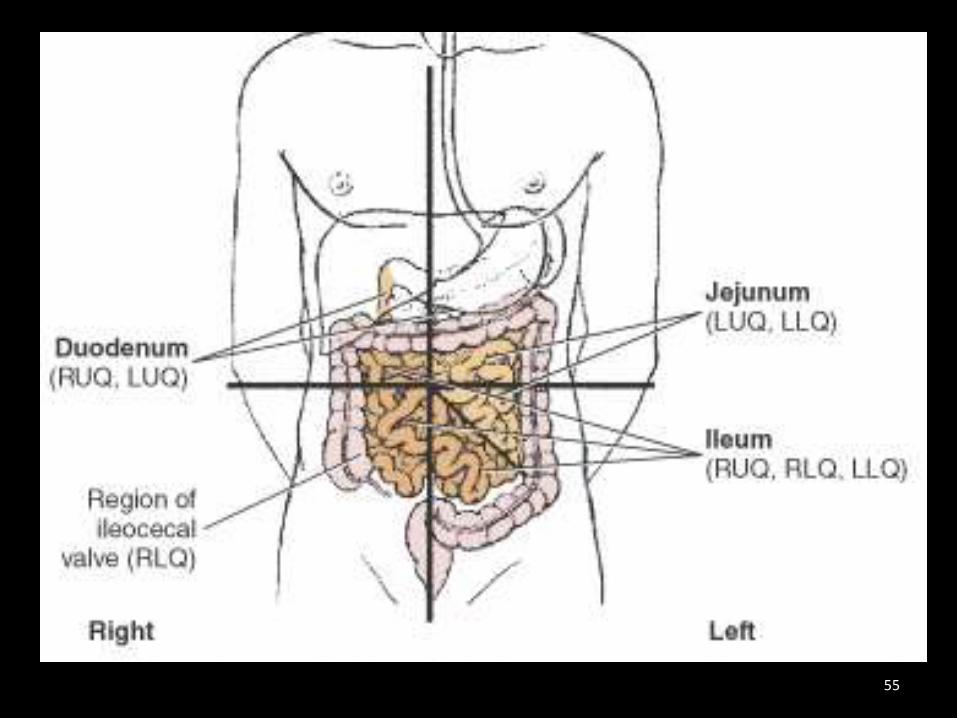
What quadrant(s) is the:1. Duodenum located? Length?2. Jejunum location? Length?3. Ileum location? Length?4. Ileocecal Valve location?
1. RUQ & LUQ – 10”
2. LUQ & LLQ – 2/5
3. RUQ, RLQ & LLQ – 3/5
4. RLQ54
55

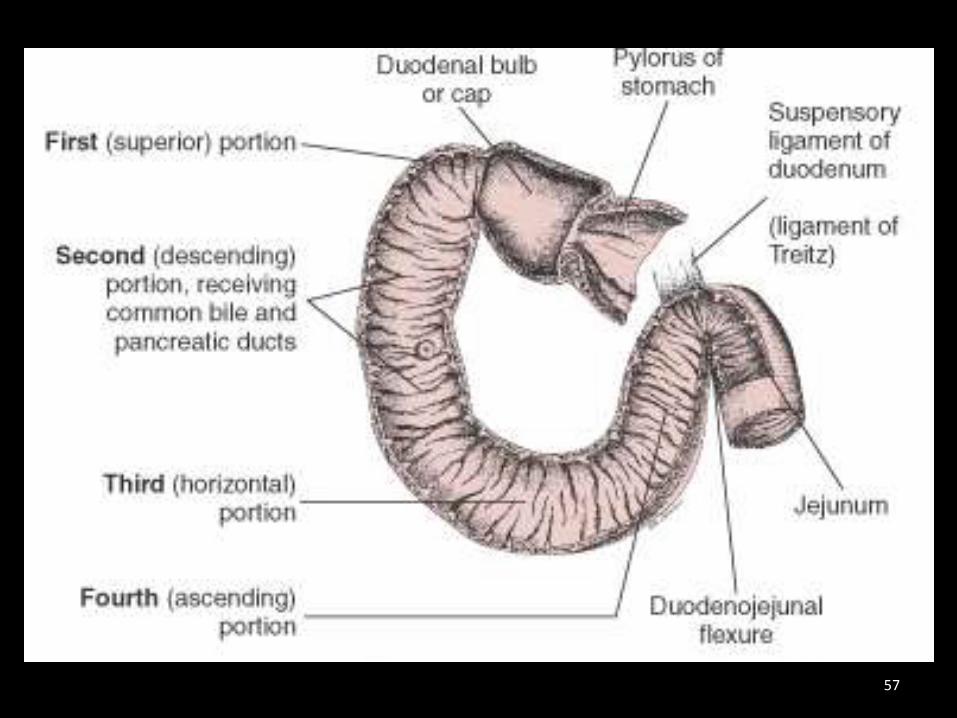
Proximal Stomach & Duodenum Anatomy
56
57

Terminal Ileum & Proximal Colon Anatomy
A
B
C
D
E58
59
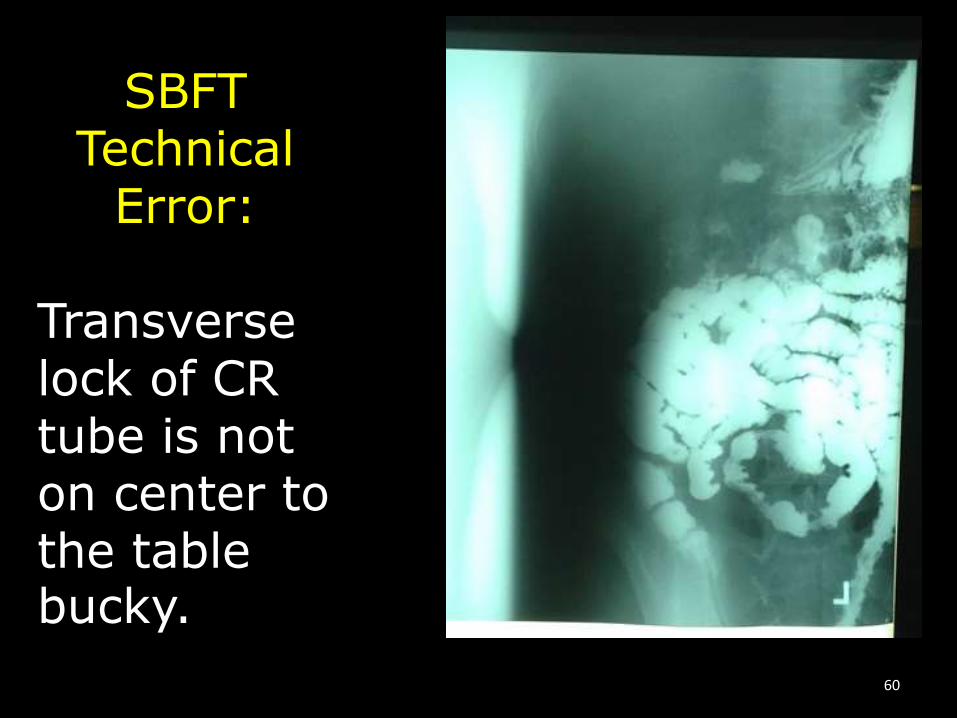
SBFTTechnical
Error:
Transverse lock of CR tube is not on center to the table bucky.
60

SBFTTechnical
Error:
Wrong centering.Anatomy is clipped for the appropriately timed image.Wrong
45 min61
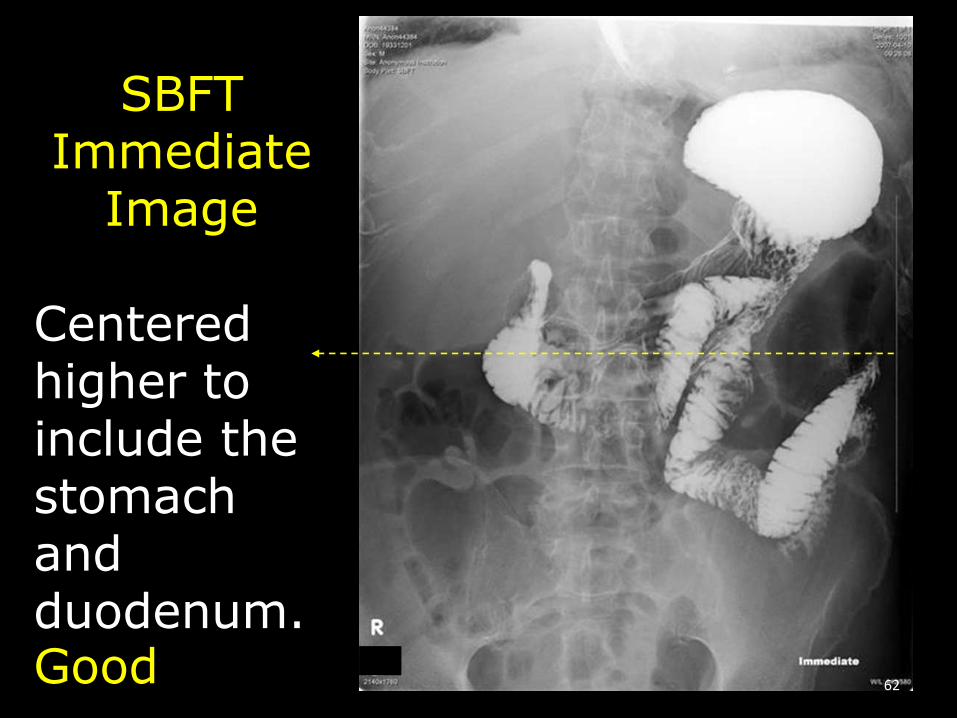
SBFTImmediate
Image
Centered higher to include the stomach and duodenum.Good 62
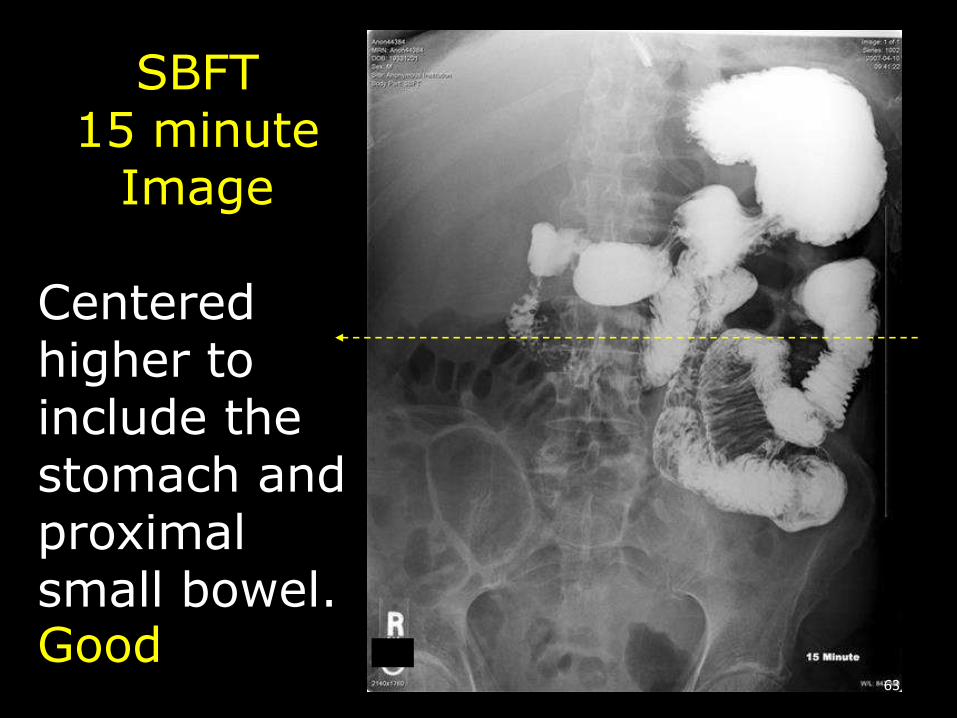
SBFT15 minute
Image
Centered higher to include the stomach and proximal small bowel.Good
63
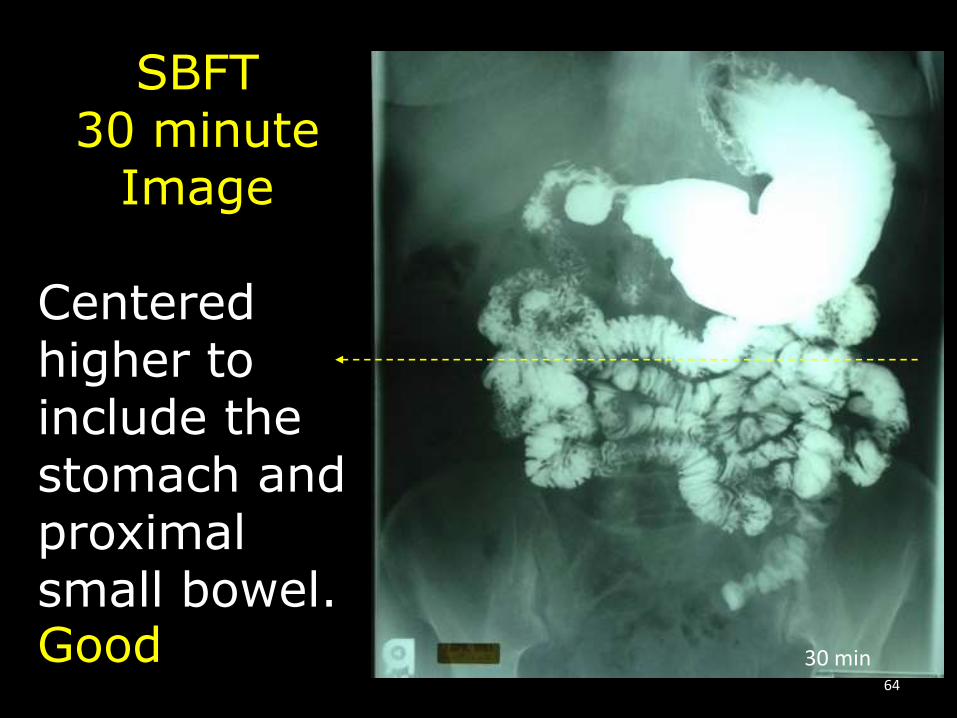
SBFT30 minute
Image
Centered higher to include the stomach and proximal small bowel.Good 30 min
64

45 min
SBFT45 minute
Image
Centered at the crest to include distal small bowel.Good
65
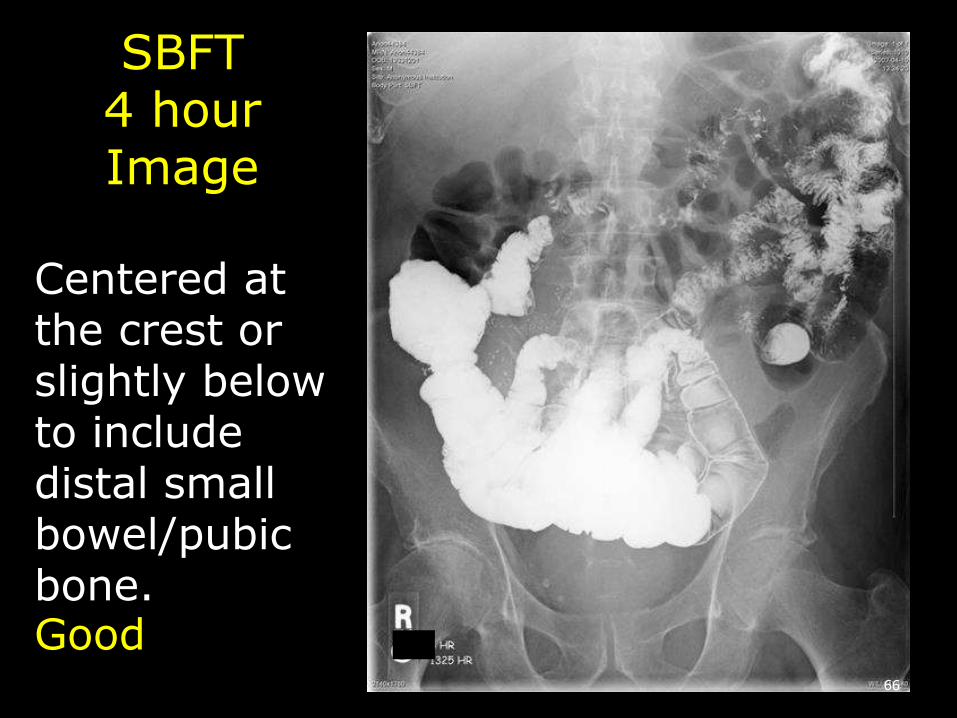
SBFT4 hourImage
Centered at the crest or slightly below to include distal small bowel/pubic bone.Good
66

Pathology
HiatalHernia
67
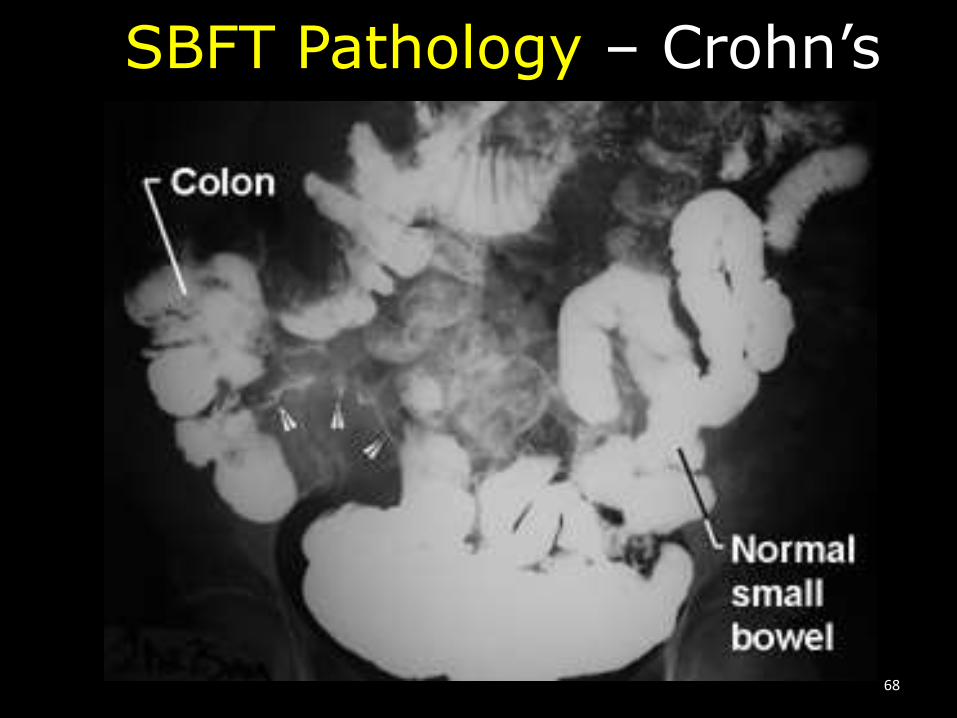
SBFT Pathology – Crohn’s
68

SBFTPathology
GastricBypass
69

SBFT Pathology Volvulus
70
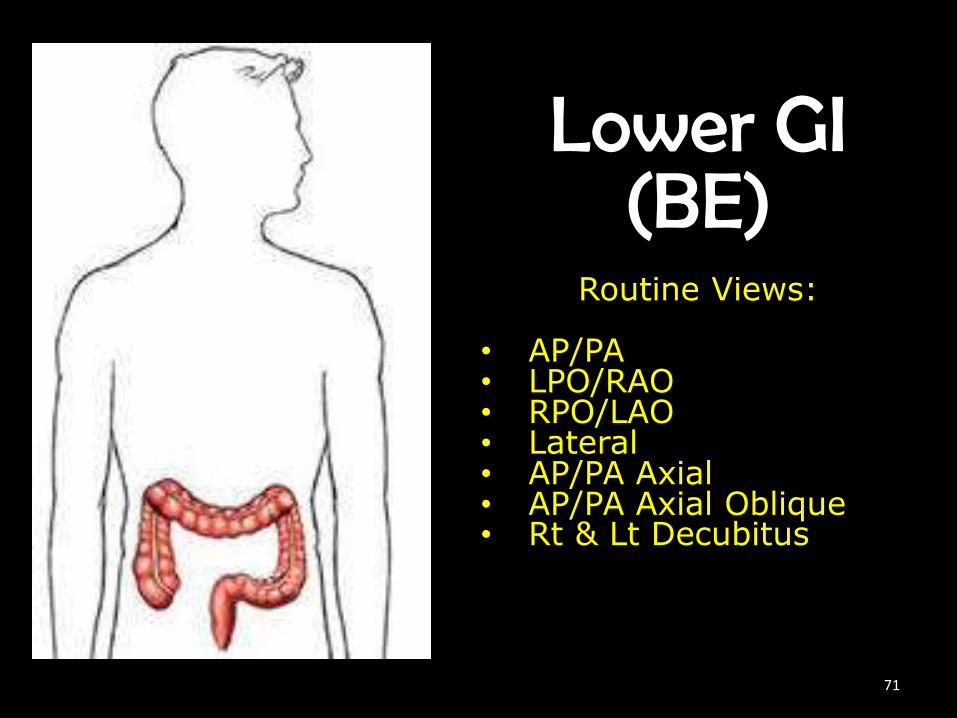
Lower GI(BE)
Routine Views:
• AP/PA• LPO/RAO• RPO/LAO• Lateral• AP/PA Axial• AP/PA Axial Oblique• Rt & Lt Decubitus
71

Lower Gastrointestinal System
• Barium Enema - Single Contrast
• Barium Enema - Iodinated, Water-soluble Contrast
• Barium Enema - Double Contrast
• Defecogram – Barium mixed with potato starch
72
Lower GI (Colon) Exams
• Single Contrast - 100-125kV• Iodinated Contrast - 80-90kV• Double Contrast - 90-100kV• Barium/potato starch - 100-125kV
73
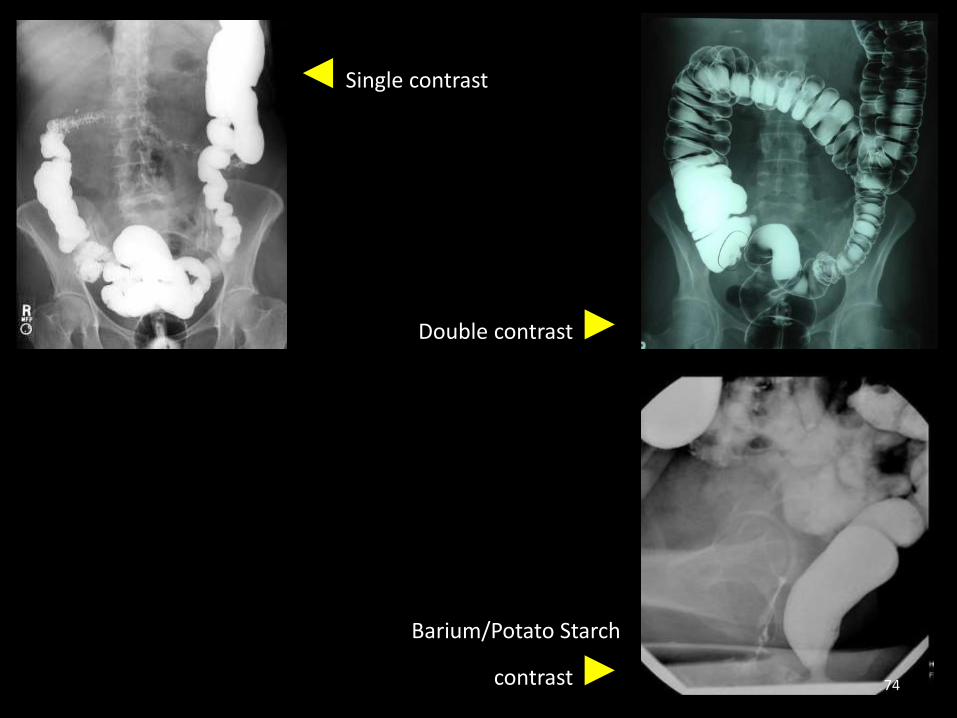
◄ Single contrast
Double contrast ►
Barium/Potato Starch
contrast ► 74
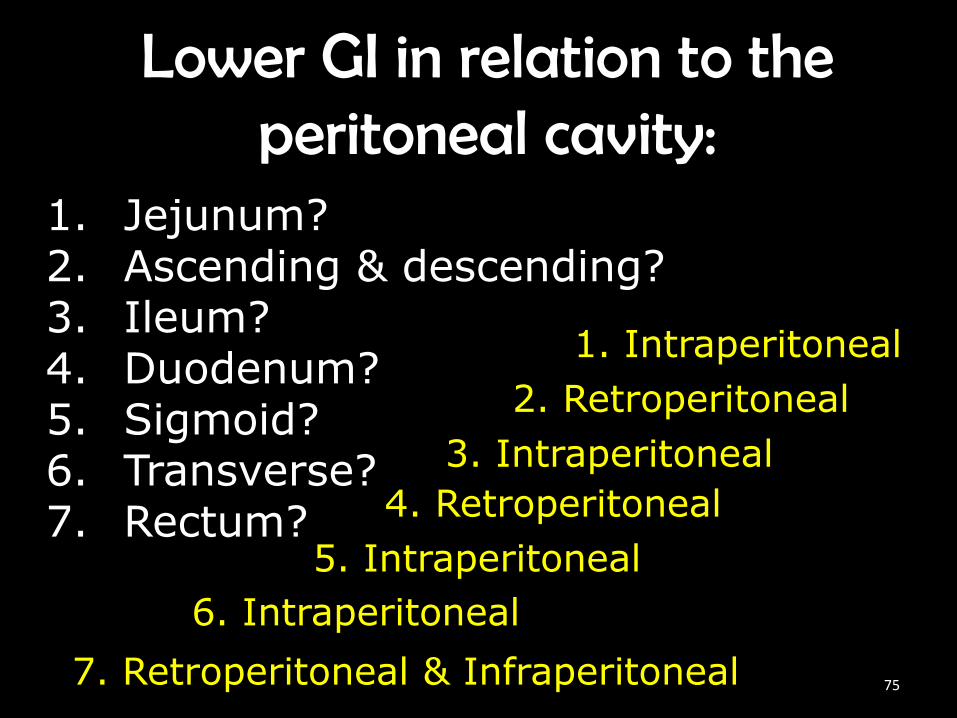
Lower GI in relation to the peritoneal cavity:
1. Jejunum?2. Ascending & descending?3. Ileum?4. Duodenum?5. Sigmoid?6. Transverse?7. Rectum?
1. Intraperitoneal
2. Retroperitoneal
3. Intraperitoneal
4. Retroperitoneal
5. Intraperitoneal
6. Intraperitoneal
7. Retroperitoneal & Infraperitoneal 75
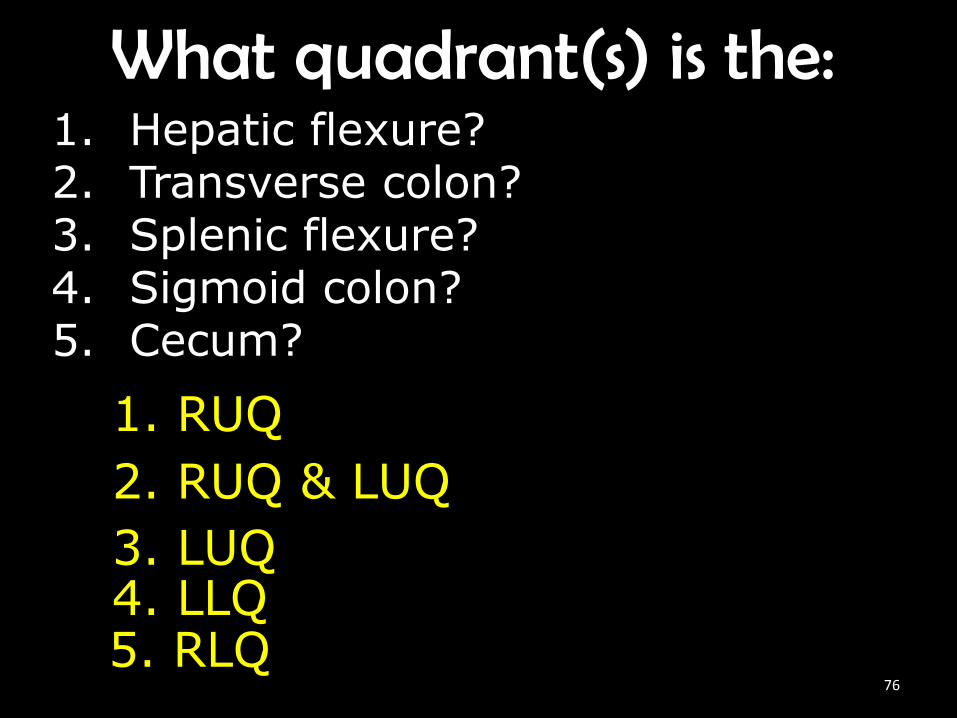
What quadrant(s) is the:1. Hepatic flexure?2. Transverse colon?3. Splenic flexure?4. Sigmoid colon?5. Cecum?
1. RUQ
2. RUQ & LUQ
3. LUQ4. LLQ5. RLQ
76
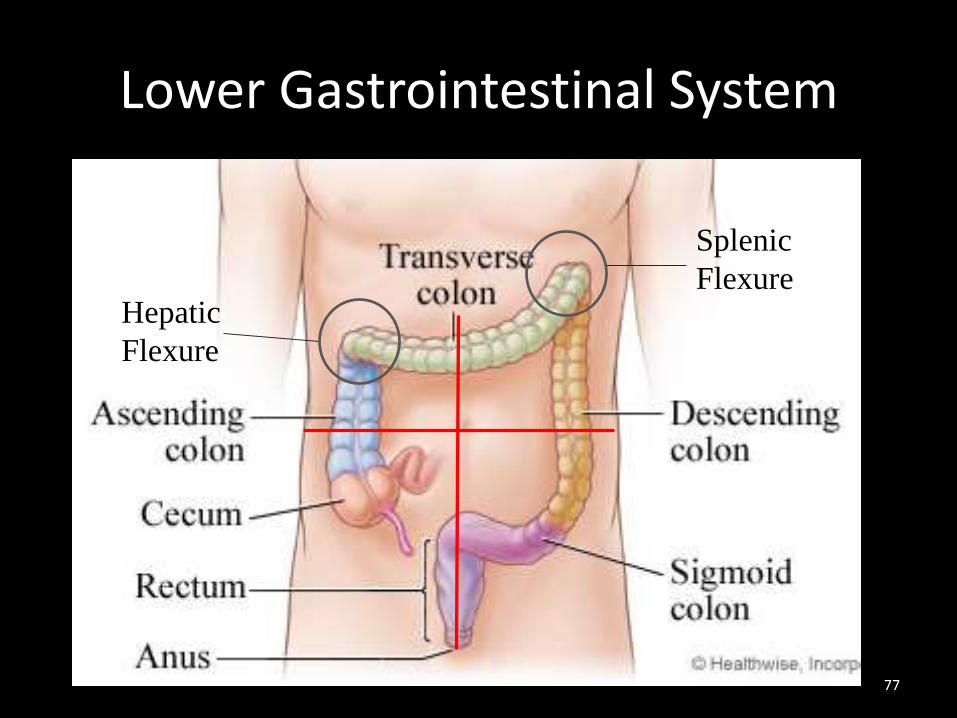
Lower Gastrointestinal System
Hepatic
Flexure
Splenic
Flexure
77

Barium vs Air in Large Intestine
78

PA BE• Body is prone
• Align MSP to Midline
• Ensure no rotation
• CR ┴ to IR
• CP to iliac crest
79

80
RAO/LPO BE• Body is rotated 35°-45°
• CR ┴ to IR
• CP at the iliac crest & 1” to the left of MSP
• Right colic/hepatic flexure
81

82

LAO/RPO BE• Body is rotated 35°-45°
• CR ┴ to IR
• CP 1-2” ABOVE iliac crest & 1” to the upside of MSP
• Left colic/splenic flexure
83
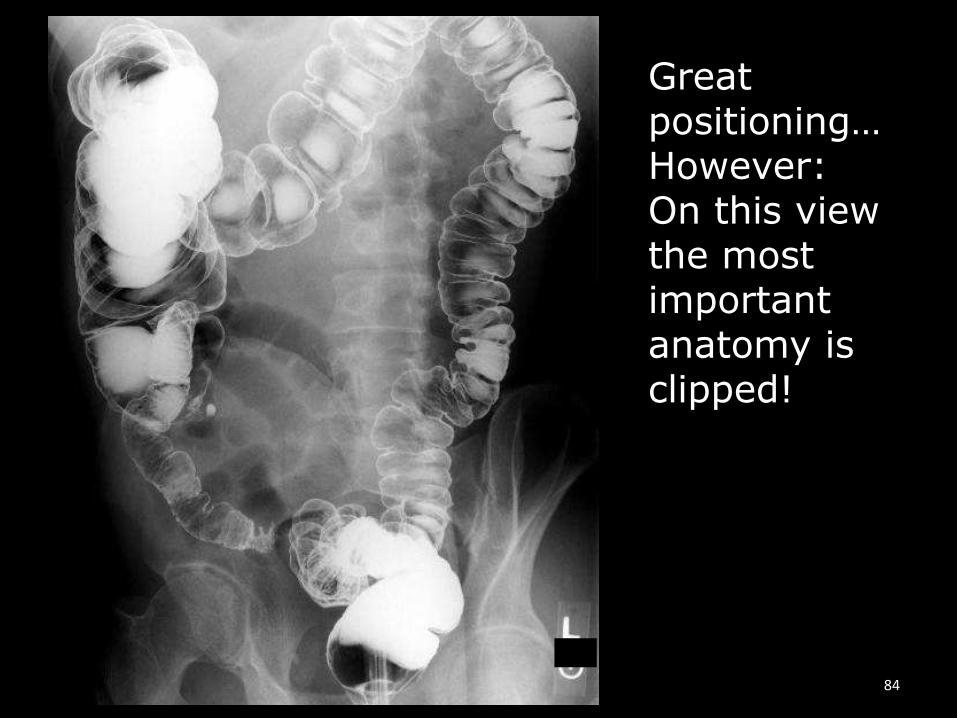
Great positioning… However:On this view the most important anatomy is clipped!
84

Lateral Rectum BE
• Body is in lateral recumbent
• Midcoronal plane to midline
• Ensure no rotation
• CR ┴ to IR
• CP at level of ASIS & Midcoronal Plane
85

86

Lateral Decubitus BE
• Body is in lateral recumbent
• Ensure no rotation with IR
• CR is horizontal to IR
• CP at iliac crest*
• *possibly center higher for when Left colis/splenic flexure is up.
87

88
AP Axial BE• Body is supine
• Align MSP to Midline
• Ensure no rotation
• CR 30°-40° cephalad to IR
• CP 2” inferior to ASIS
89

90

AP Axial Oblique LPO (Butterfly) BE
• Body is rotated 30°-40° LPO
• CR 30°-40° cephalad to IR
• CP 2” inferior and 2” medial to right ASIS
• Elongates sigmoid colon91
92

93
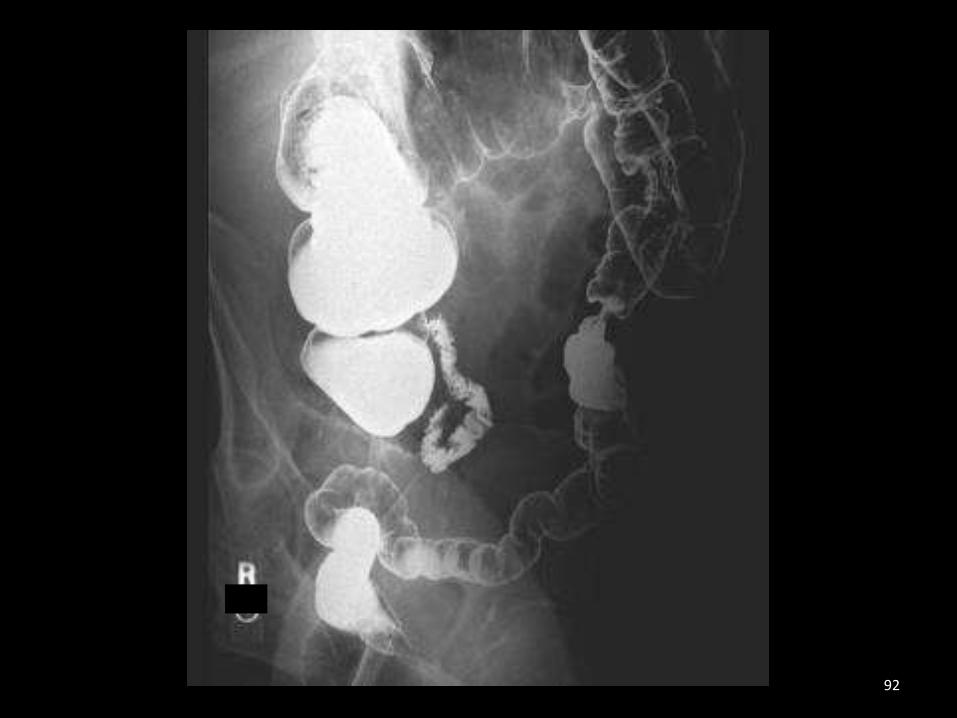
PA Axial Oblique RAO (Butterfly) BE
• Body is rotated 35°-45° LPO
• CR 30°-40° caudad to IR
• CP at the level of the ASIS and 2” to the left of the lumbar spinous processes
• Elongates sigmoid colon94
AP Post Evac BE• Body is supine
• Align MSP to Midline
• Ensure no rotation
• CR ┴ to IR
• CP to iliac crest
95

96
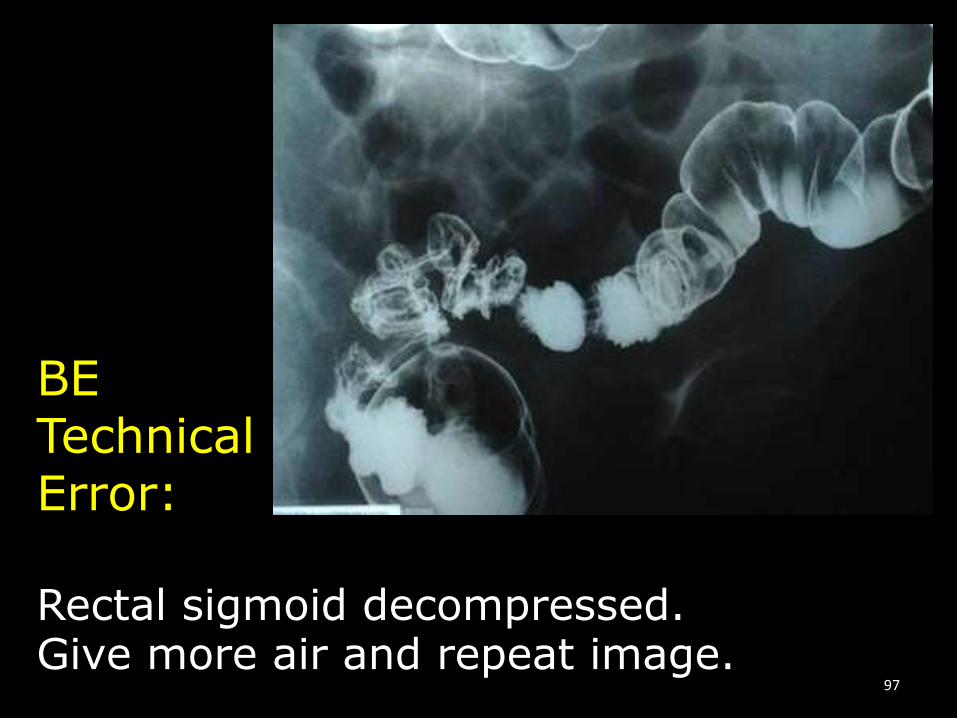
BETechnical Error:
Rectal sigmoid decompressed. Give more air and repeat image.
97

Lower GI Pathology:Ulcerative Colitis
Normal Hustra
98
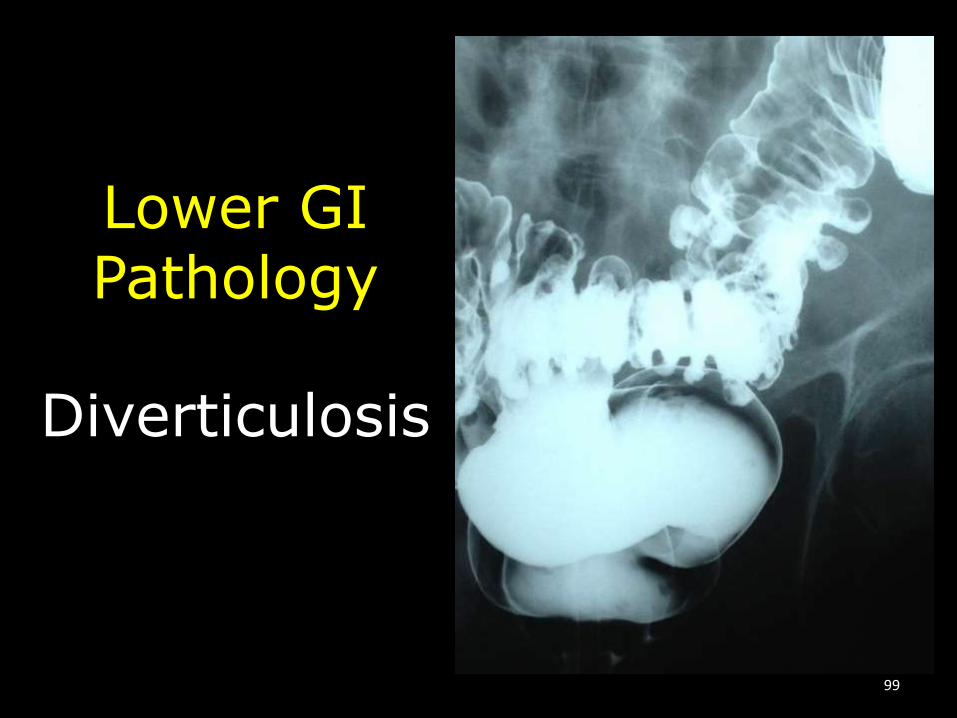
Lower GIPathology
Diverticulosis
99
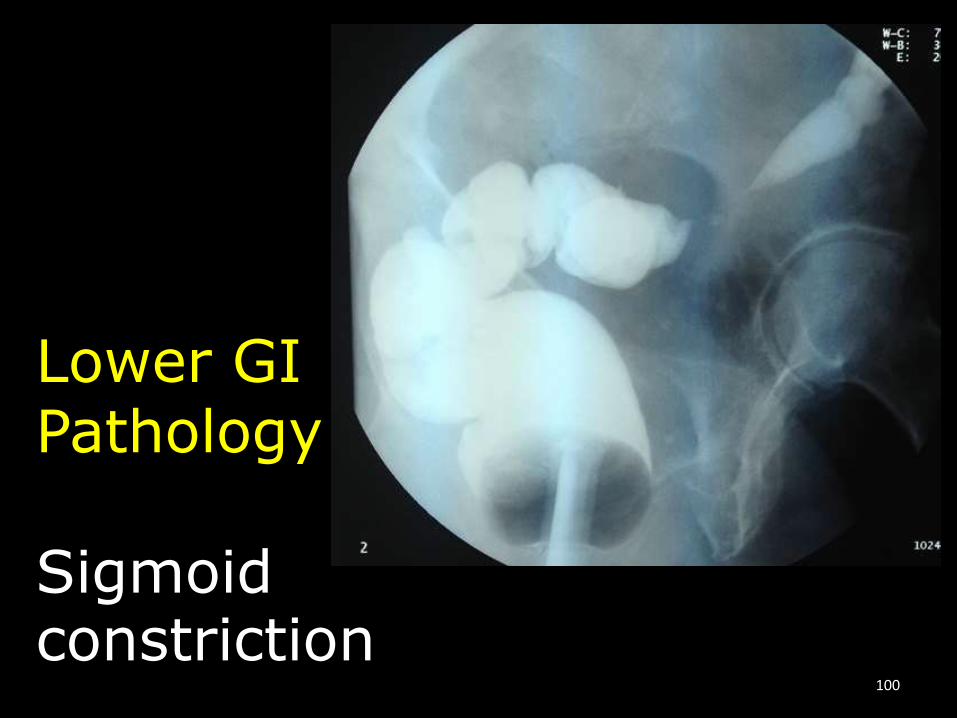
Lower GIPathology
Sigmoid constriction
100

Lower GIPathology
Colon Herniated into the chest
101

Lower GIPathology
Herniawith constrictions
102
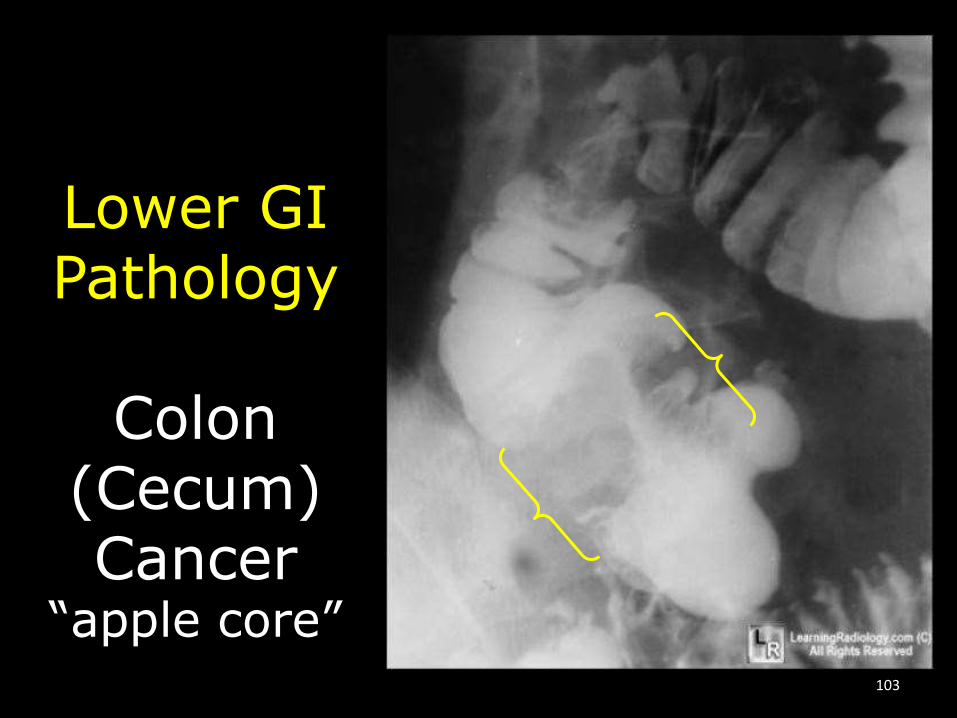
Lower GIPathology
Colon(Cecum)Cancer
“apple core”103
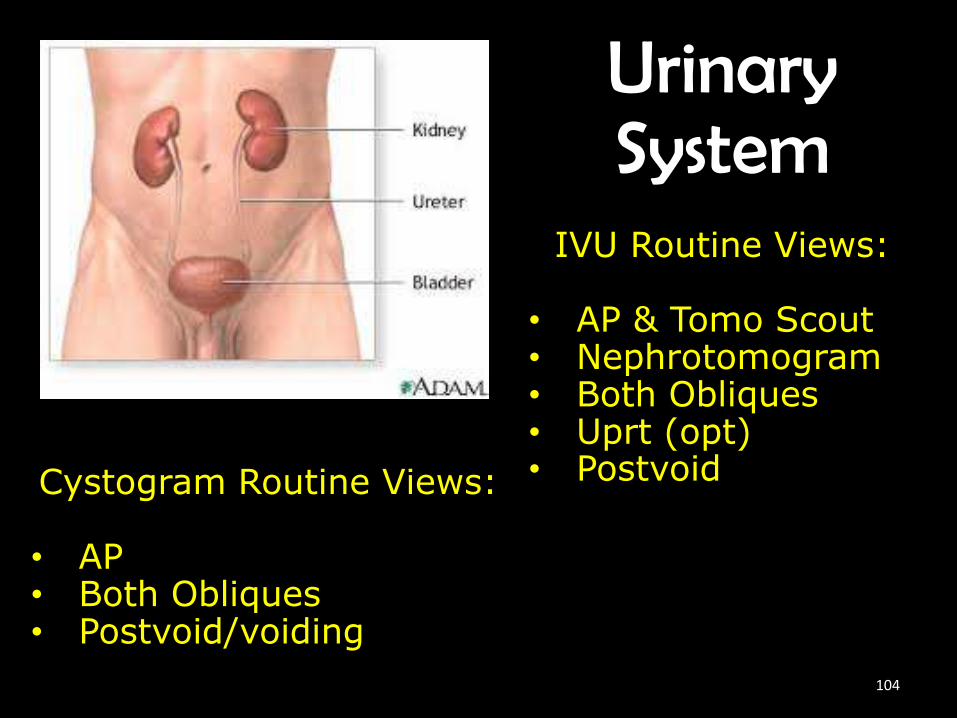
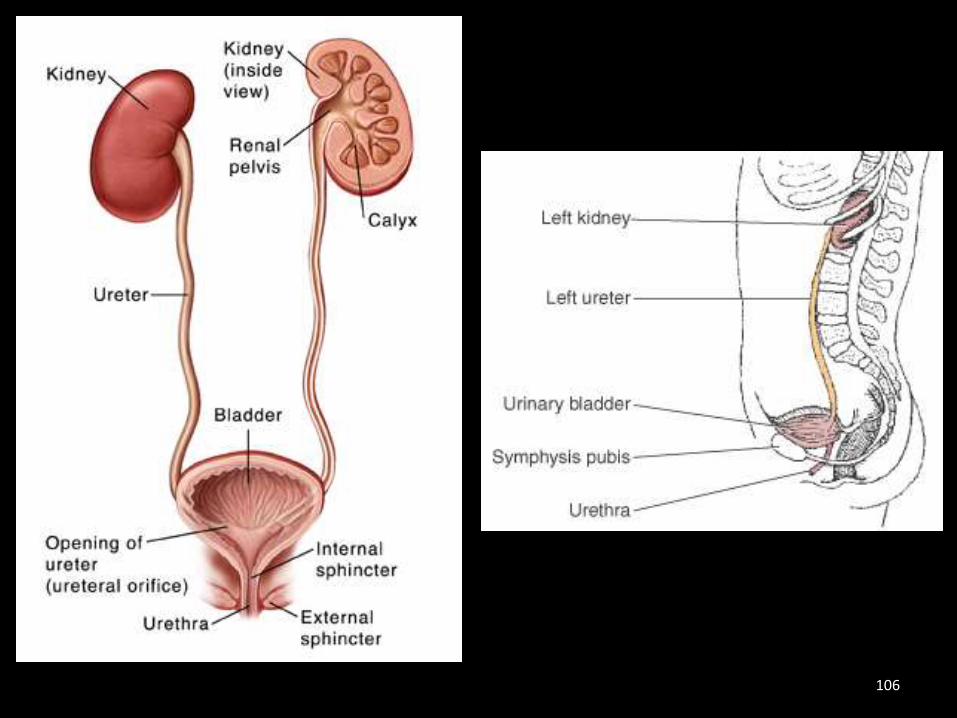
Urinary System
IVU Routine Views:
• AP & Tomo Scout• Nephrotomogram• Both Obliques• Uprt (opt)• PostvoidCystogram Routine Views:
• AP • Both Obliques• Postvoid/voiding
104
Urinary organs in relation to the peritoneal cavity:
1. Kidneys?2. Ureters?3. Adrenal glands?4. Bladder?5. Reproductive organs?
1. Retroperitoneal
2. Retroperitoneal
3. Retroperitoneal
4. Infraperitoneal
5. Infraperitoneal 105
106

AP Intravenous Urography
• Body is supine
• MS to midline
• Ensure no rotation
• CR ┴ to IR
• CP to level of iliac crest
• At timed intervals
107

108
AP Nephrogram Urography
• Body is supine
• MS to midline
• Ensure no rotation
• 10°-20° angle tomogram
• CR ┴ to IR
• CP midway between xiphoid & iliac crest
109
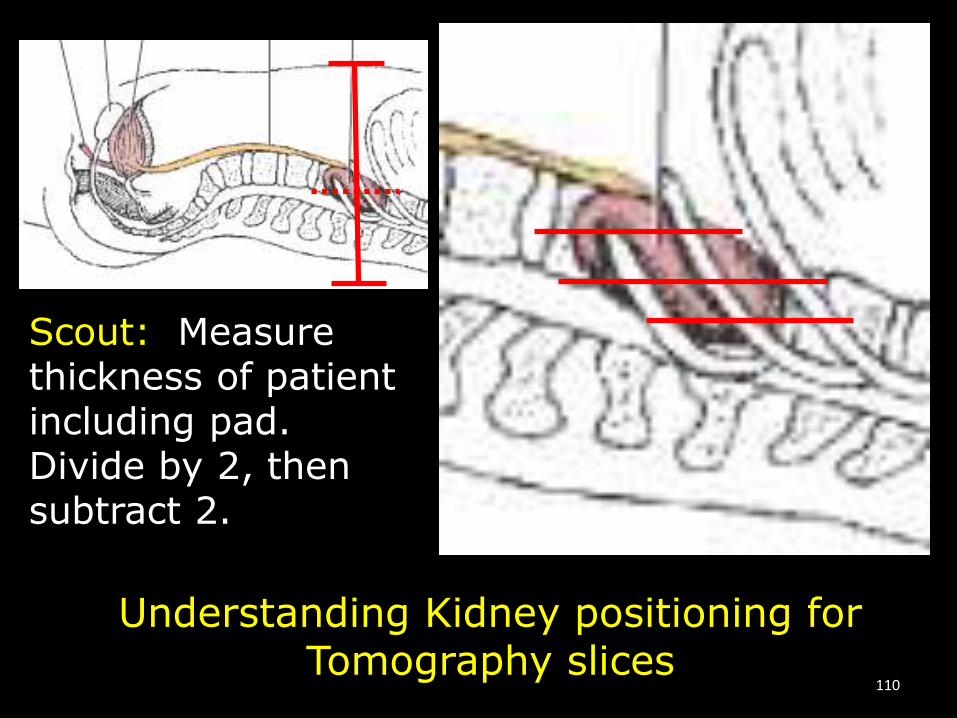
Understanding Kidney positioning for Tomography slices
Scout: Measure thickness of patient including pad. Divide by 2, then subtract 2.
110
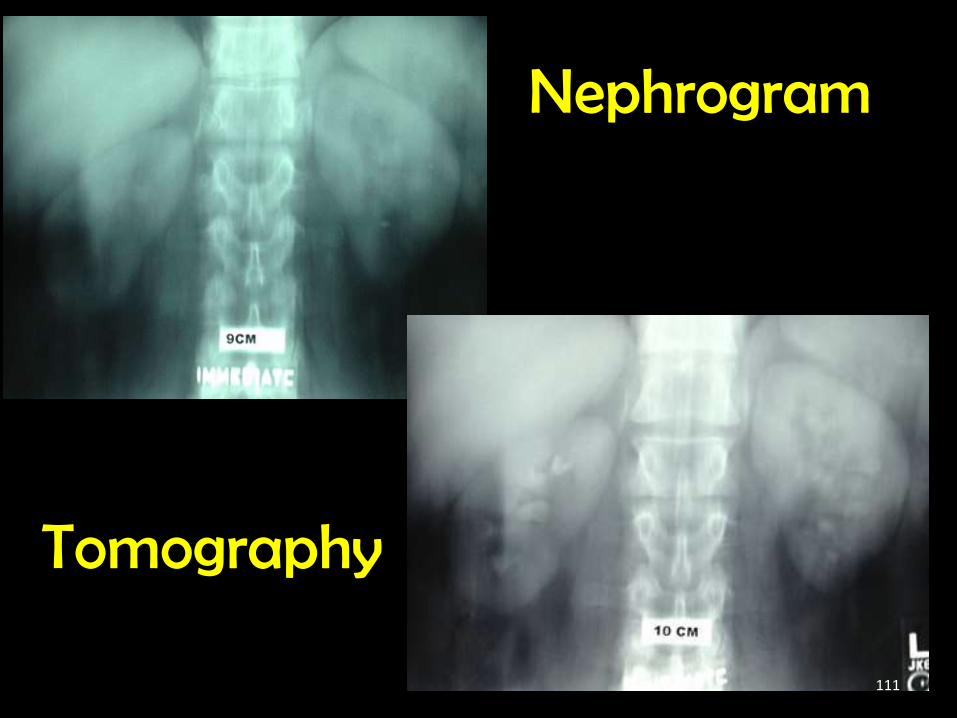
Nephrogram
Tomography
111

LPO/RPO Intravenous Urography
• Body is rotated 30°
• CR ┴ to IR
• CP at the iliac crest
• LPO = Right kidney in profile, proximal left ureter & distal right ureter.
• RPO = Left kidney in profile; proximal right ureter & distal left ureter.
112
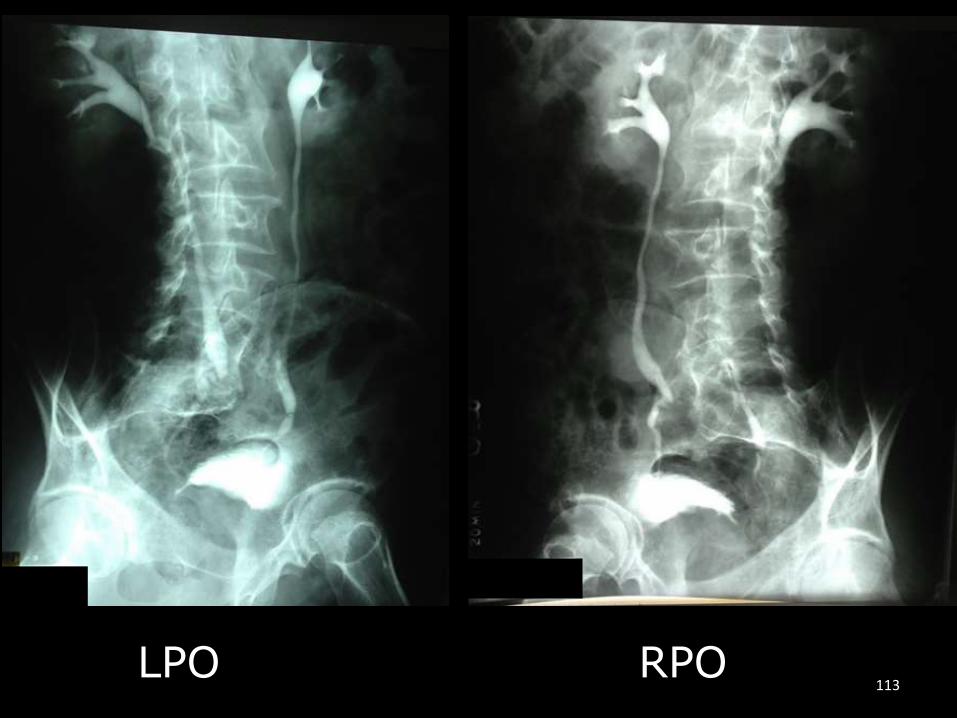
LPO RPO113
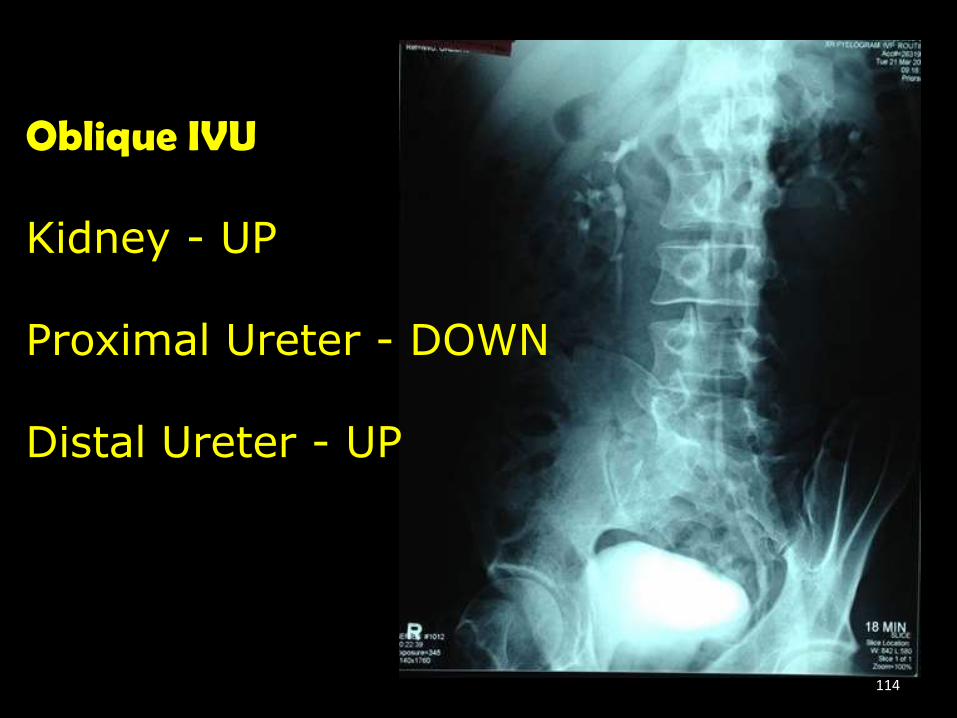
Oblique IVU
Kidney - UP
Proximal Ureter - DOWN
Distal Ureter - UP
114

AP Uprt/PA Post Void Intravenous Urography
• Body is AP Uprt or prone
• Align MSP to Midline
• Ensure no rotation
• CR ┴ to IR
• CP to iliac crest *MUST include bladder
115

116
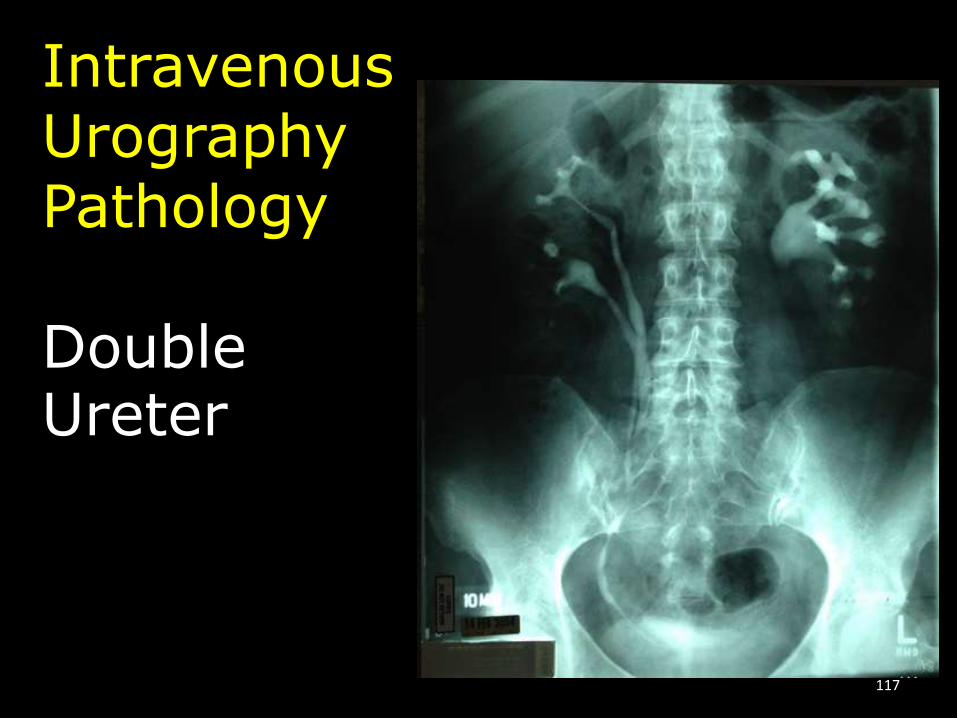
IntravenousUrographyPathology
DoubleUreter
117

IntravenousUrographyPathology
StaghornCalculi
118
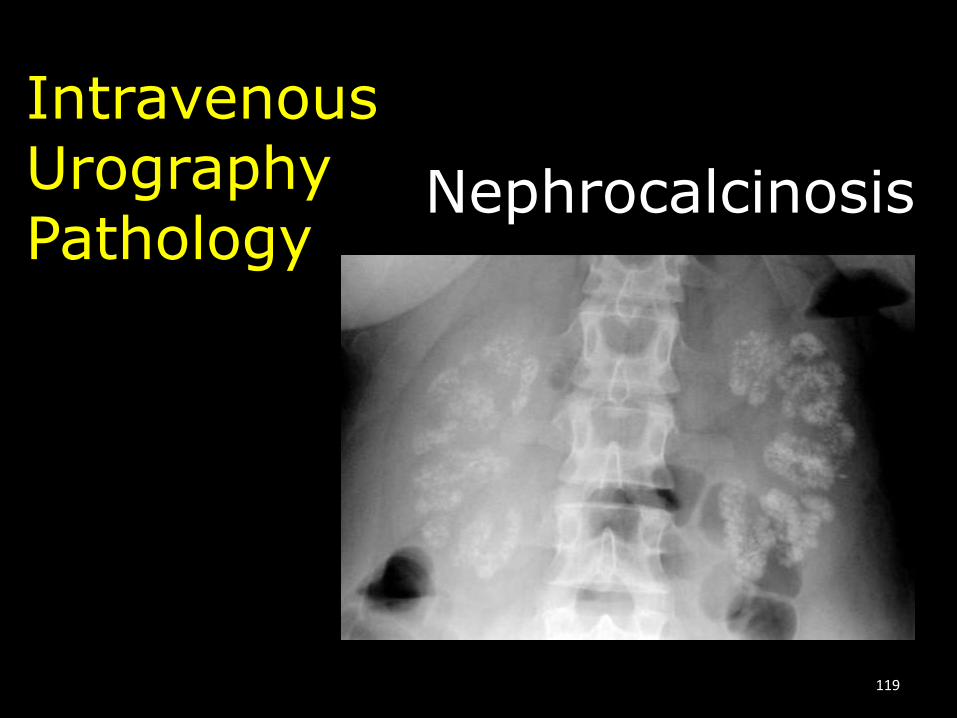
IntravenousUrographyPathology
Nephrocalcinosis
119
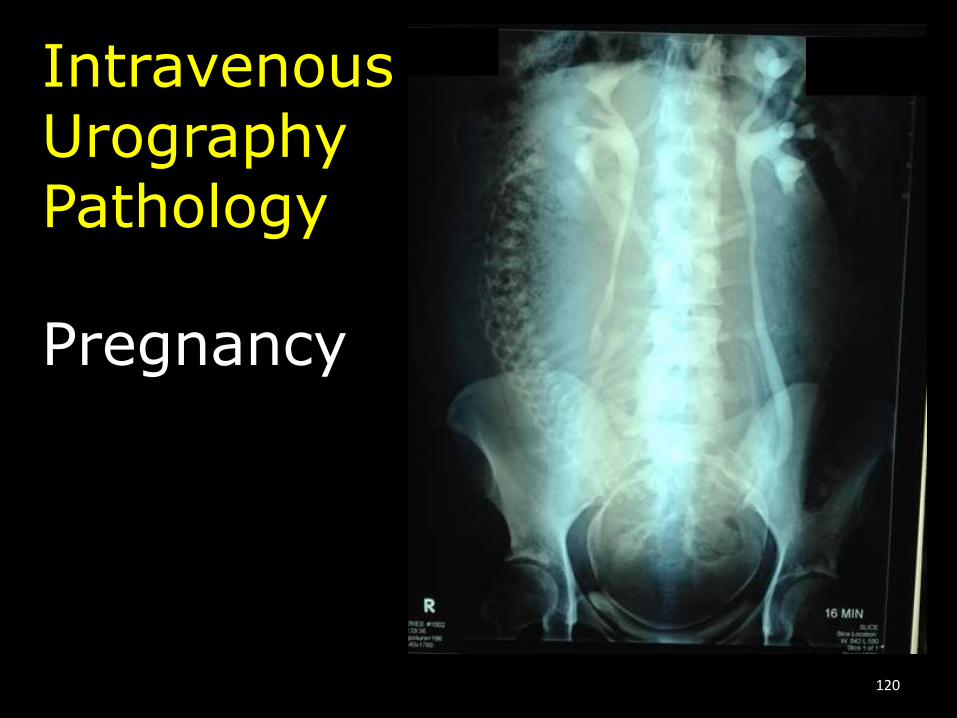
IntravenousUrographyPathology
Pregnancy
120
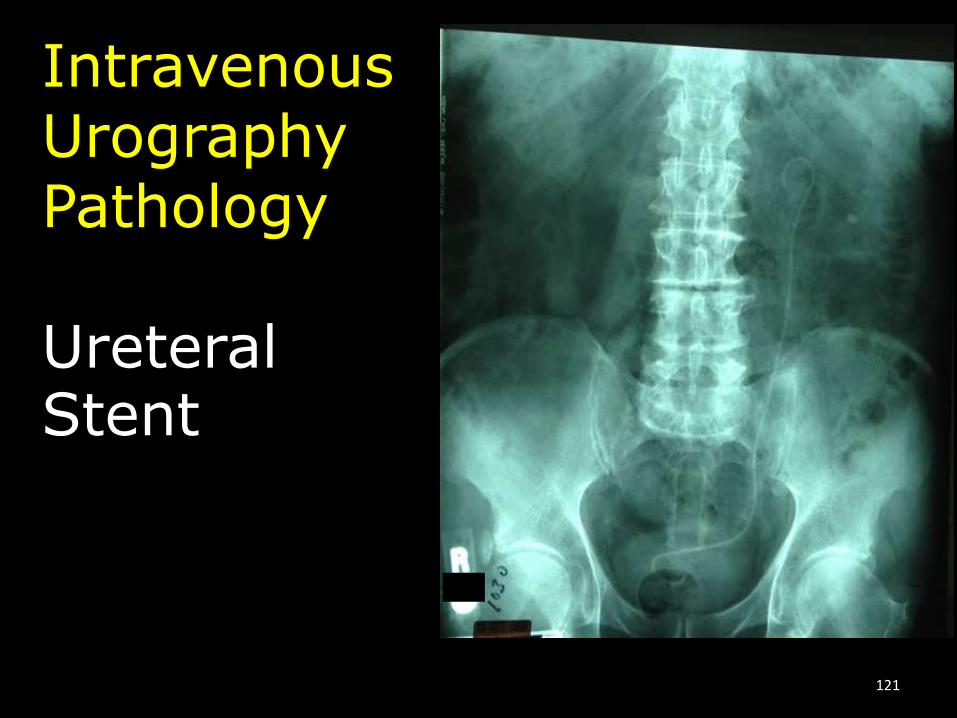
IntravenousUrographyPathology
Ureteral Stent
121
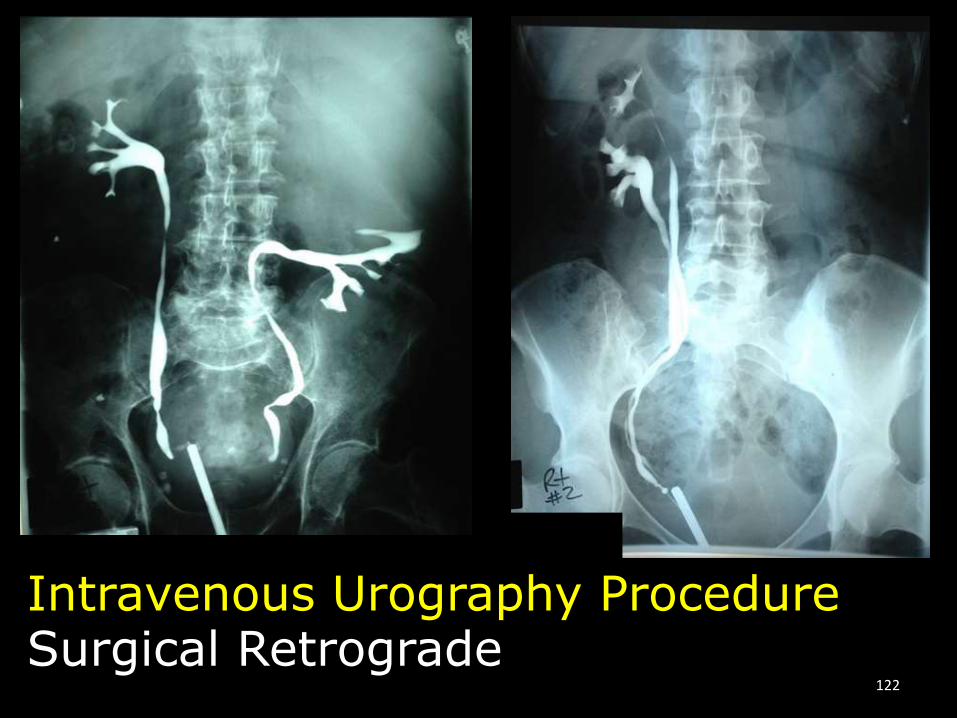
Intravenous Urography ProcedureSurgical Retrograde
122

AP Cystography
• Body is supine
• MS to midline
• CR 10°-15° caudad to IR
• CP 2” superior to pubic symphysis
123
LPO & RPO Cystography• Body is rotated 45°-60°
• CR 10°-15° caudad to IR
• CP 2” superior to pubic symphysis & 2” medial to upside ASIS
124
Lateral Cystography
• Body is lateral recumbent
• Midcoronal is ┴ to IR
• CR ┴ to IR
• CP 2” superior to and posterior to pubic symphysis
125

◄LPO
RPO►
◄ Lateral
CystographyName the view:
AP/Voiding►126
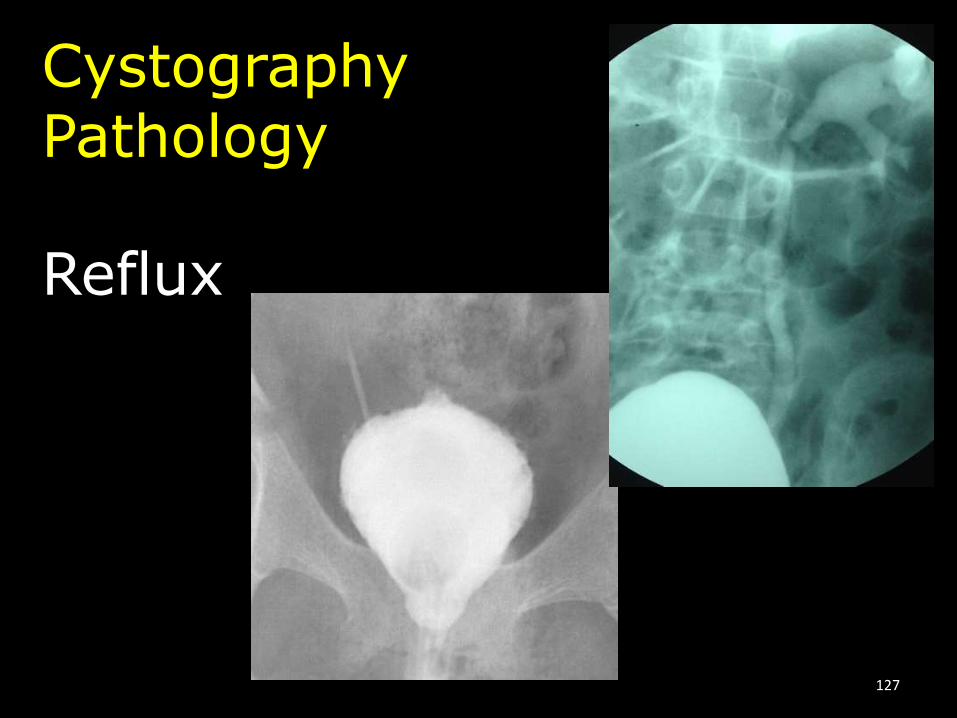
CystographyPathology
Reflux
127
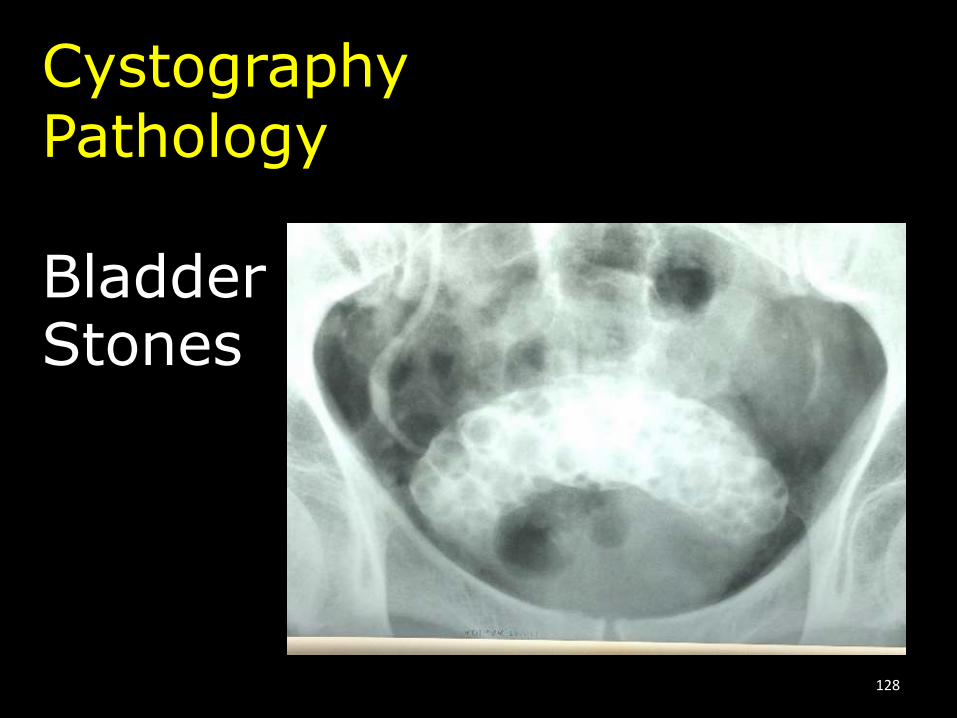
CystographyPathology
BladderStones
128

Biliary Tract
SystemExams:
• Oral Chole• Surg Chole• Surg T-tube
• ERCP
129
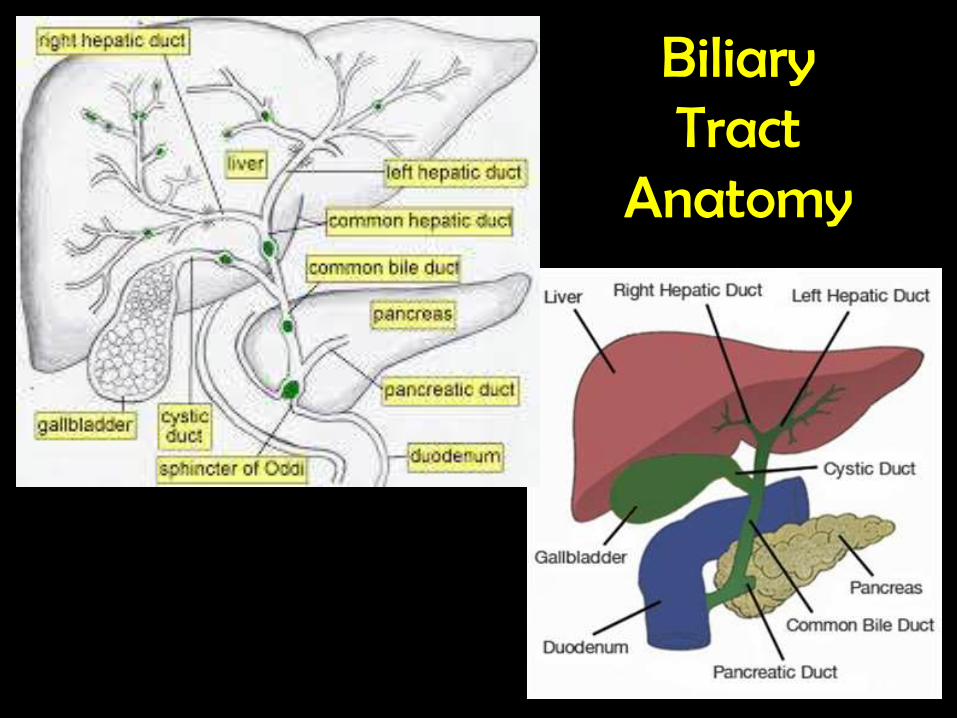
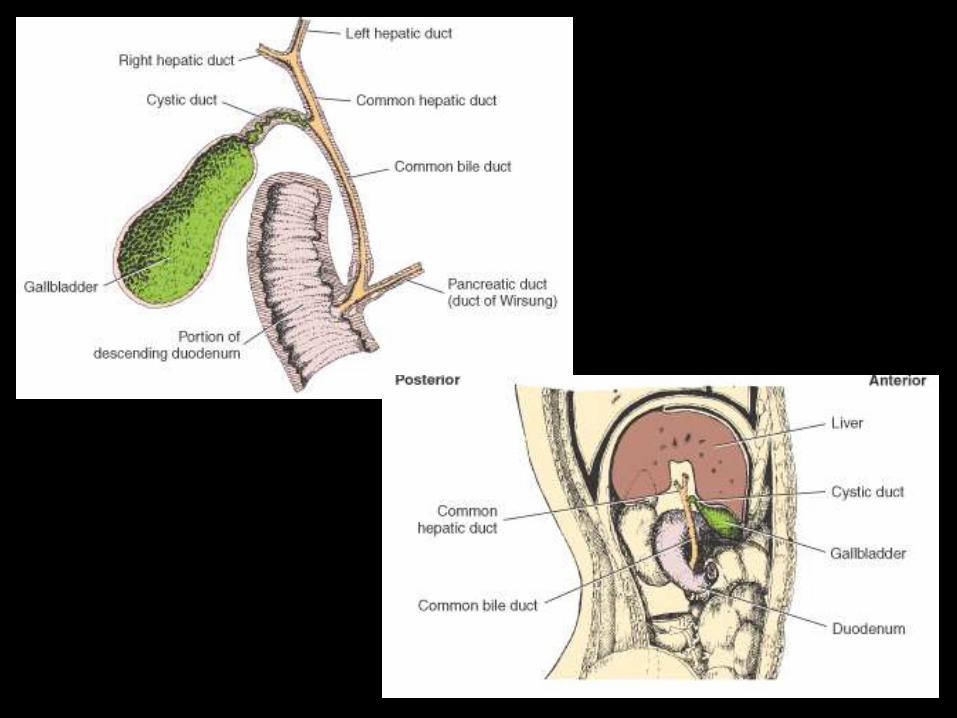
Biliary Tract
Anatomy
130
131

Biliary Tract ProcedureOral Cholecystogram
132

Biliary Tract ProcedureSurgical Cholangiogram w/C-Arm
133
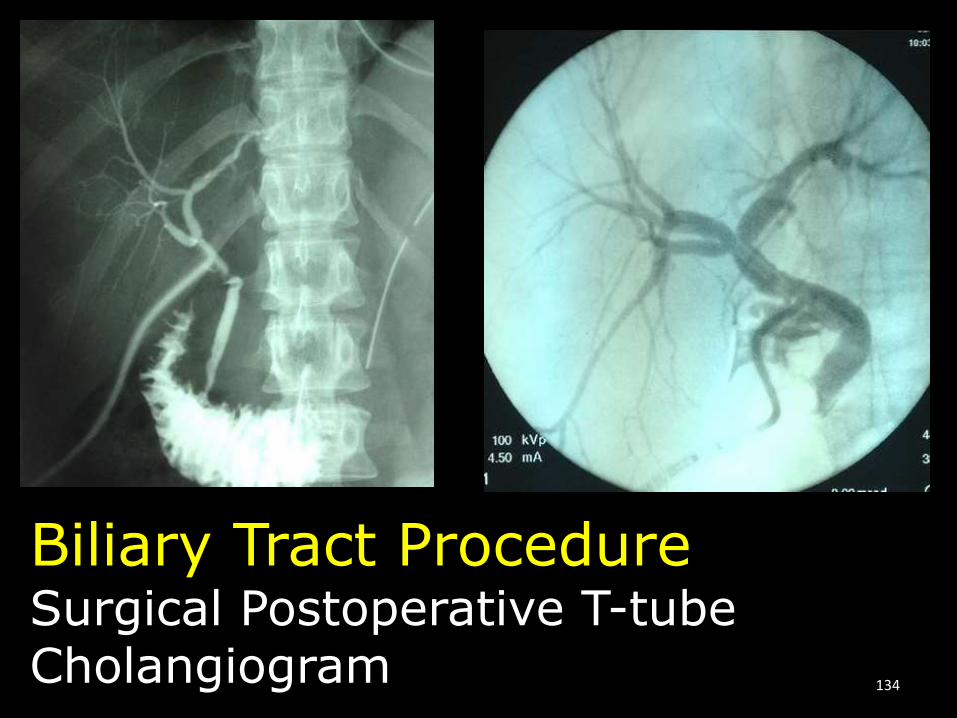
Biliary Tract ProcedureSurgical Postoperative T-tube Cholangiogram 134
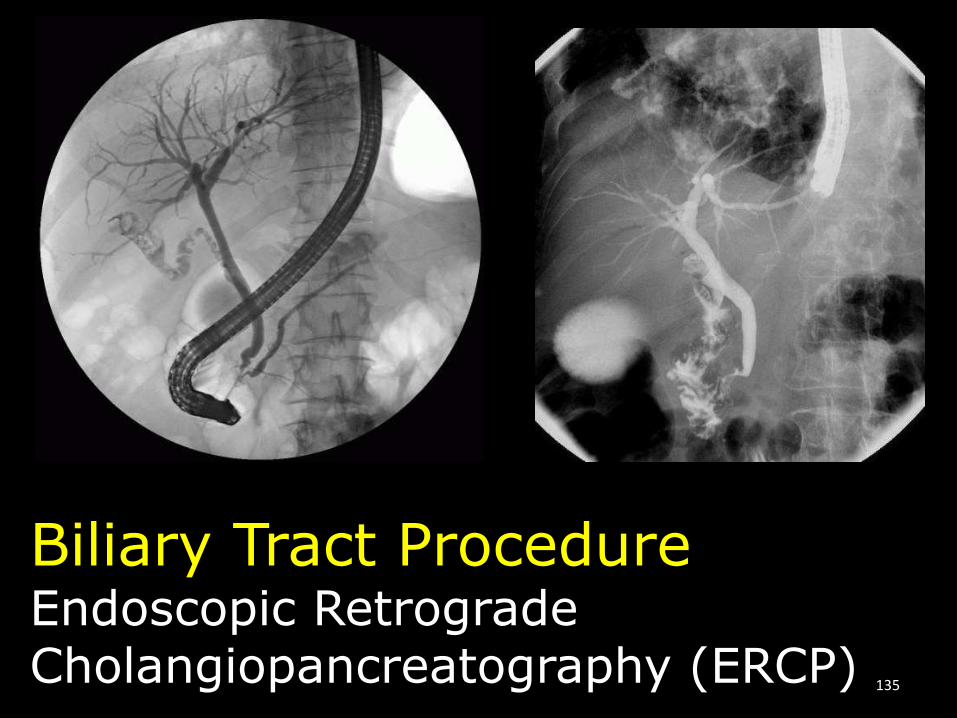
Biliary Tract ProcedureEndoscopic Retrograde Cholangiopancreatography (ERCP) 135

~ The End ~
136
![Açai Juice as Contrast Agent in MRCP Exams: Qualitative and … · 2020-01-31 · been used in MRCP exams including orange, lemon, pineapple, blueberry and, açai juices [3,4,7,8]](https://img.pdfslide.us/doc/110x75/5f09f78d7e708231d4295e34/aai-juice-as-contrast-agent-in-mrcp-exams-qualitative-and-2020-01-31-been-used.jpg)