Embed Size (px)
Citation preview
ODONTOGENIC INFECTIONS
Prepared by:Dr. Rea Corpuz

(1) Cellulitis
(2) Ludwig’s Angina
(3) Cavernous Sinus Thrombosis
(4) Osteomyelitis
Odontogenic Infections

if abscess is NOT able to establish drainage through the surface of skin or into oral cavity
may spread diffusely through facial planes of soft tissue
acute + edematous spread of acute inflammatory process
(1) Cellulitis

two dangerous forms:
Ludwig’s Angina
Cavernous Sinus Thrombosis
(1) Cellulitis

named after German physician who described the seriousness of disorder in 1836
Angina comes from Latin word angere
strangle
(2) Ludwig’s Angina

70% of cases, develop from spread of an acute infection from lower molar teeth
prevalence in patients who are immunocompromised secondary to disorders such as:
diabetes mellitus organ transplantation acquired immunodeficiency syndrome (AIDS) aplastic anemia
(2) Ludwig’s Angina

Clinical Features
massive swelling on neck
often extends close to clavicle
involvement of sublingual space results in
• elevation Woody Tongue• posterior enlargement can compromise• protrusion of tongue airway
(2) Ludwig’s Angina

(2) Ludwig’s Angina
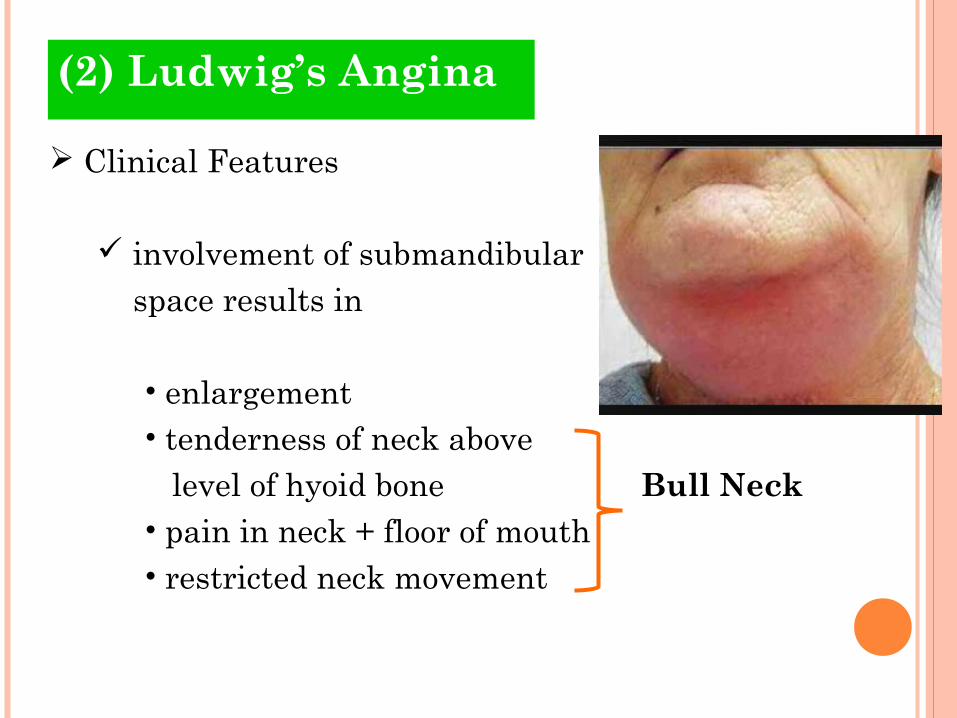
Clinical Features
involvement of submandibular space results in
• enlargement• tenderness of neck above level of hyoid bone Bull Neck• pain in neck + floor of mouth• restricted neck movement
(2) Ludwig’s Angina

Clinical Features
involvement of submandibular space results in
• dysphagia• dysphonia• dysarthria• drooling• sore throat
(2) Ludwig’s Angina

Clinical Features
involvement of lateral pharyngeal space
• respiratory obstruction secondary to laryngeal edema
• tachypnea• dyspnea• tachycardia• patient needs to maintain erect position
(2) Ludwig’s Angina

Treatment & Prognosis
centers around 4 activities
• maintenance of airway• incision + drainage• antibiotic therapy• elimination of original focus
of inflammation
(2) Ludwig’s Angina

Treatment & Prognosis
initial observation many clinicians administer
• systemic corticosteroid medications such as intravenous (IV) dexamethasone
attempt to reduce cellulitis
(2) Ludwig’s Angina

Treatment & Prognosis
if signs or symptoms of impending airway obstruction:
• fiber-optic nasotracheal intubation
• tracheostomy
• cricothyroidotomy
(2) Ludwig’s Angina

Treatment & Prognosis
if signs or symptoms of impending airway obstruction:
• cricothyroidotomy
sometimes performed instead of tracheostomy
perceived lower risk of spreading infection to mediastinum
(2) Ludwig’s Angina

Treatment & Prognosis
• cricothyroidotomy
(2) Ludwig’s Angina

Treatment & Prognosis
high dose of penicillin penicillin-
Clindamycin OR sensitive Choramphenicol patients
anitbiotic medication is adjusted according to patient’s response + culture result from aspirates of fluid from enlargement
(2) Ludwig’s Angina

Treatment & Prognosis
if infection remains:
diffuse surgical intervention indurated is at discretion of clinician brawny + often governed by patient’s
response to noninvasive therapy
(2) Ludwig’s Angina

Treatment & Prognosis
complications:
• Pericarditis• Pneumonia• Mediastinitis• Sepsis• Empyema• Respiratory Obstruction
(2) Ludwig’s Angina

edematous periorbital enlargement
with involvement of eyelids + conjunctiva
(3) Cavernous Sinus Thrombosis

in cases, involving canine space
swelling along lateral border of nose
may extend up to medial aspect of eye + periorbital area
protrusion + fixation of eyeball
(3) Cavernous Sinus Thrombosis

in cases, involving canine space
induration + swelling of adjacent forehead + nose
pupil dilation lacrimation may also photophobia occur loss of vision
(3) Cavernous Sinus Thrombosis

in cases, involving canine space
pain over eye + along distribution of:
• opthalmic Trigeminal • maxillary branches Nerve
(3) Cavernous Sinus Thrombosis

Treatment & Prognosis
surgical drainage + high-dose antibiotic medication similar to those administered for patient’s with Ludwig’s Angina
(3) Cavernous Sinus Thrombosis
an acute or chronic inflammatory process in extends
medullary spaces OR away from cortical surfaces of bone initial site of
involvement
(4) Osteomyelitis

caused by bacterial infections
result in expanding lytic destruction of involved bone
with suppuration sequestra formation
(4) Osteomyelitis

patients of all ages can be affected
strong male predominance
most cases involves mandible
(4) Osteomyelitis

Acute Supporative Osteomyelitis
Chronic Suppporative Osteomyelitis
(4) Osteomyelitis

acute inflammatory process spreads through medullary spaces of bone
insufficient time has passed for body to react to presence of inflammatory infiltrate
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Clinical Features
symptoms of acute inflammatory process less than1 month in duration
fever
leukocytosis
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Clinical Features
lymphadenopathy
soft tissue swelling of affected area
on occasion, paresthesia of lower lip
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Histopathologic Features
biopsy material from patients
• liquid content• lack of soft tissue component• consist predominantly of necrotic bone
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Histopathologic Features
necrotic bone
• loss of osteocytes• peripheral resorption• bacterial colonization• acute inflammatory infiltrate
consists of polymorphonuclear leukocytes
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Radiographic Features
ill- defined radioluscency
periosteal new bone formation may be seen
• response to subperiosteal spread of infection
• proliferations more common in young patients
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Radiographic Features
periosteal new bone formation may be seen
• single-layered radioopaque line
• separated from normal cortex by an intervening radiolucent band
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Radiographic Features
on occasion, exfoliation of fragments of necrotic bone
fragment of necrotic bone that has separated from adjacent vital bone is teremed sequestrum
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Radiographic Features
on occasion, fragments of necrotic bone may become surrounded by new vital bone, known as involucrum
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

Treatment
if obvious abscess formation,
• antibiotics penicillin clindamycin cephalexin cefotaxime gentamicin
• drainage
(4) Osteomyelitis (Acute Supporative Osteomyelitis)

defensive response leads to production of granulation tissue
subsequent forms dense scar tissue
• attempt to wall off infected area
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

subsequent forms dense scar tissue
• encircled dead space acts as reservoir for bacteria
• antibiotic medications have great difficulty reaching the site
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

Clinical Features
if acute osteomyelitis is not resolved expeditiously
entrenchment of chronic osteomyelitis occurs
sometimes may arise without previous acute episode
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

Clinical Features
swelling pain sinus formation purulent discharge sequestrum formation tooth loss pathologic fracture
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)
Clinical Features
may experience acute exacerbations or periods of decreased pain associated with chronic smoldering progression
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

Histophathologic Features
biopsy material from patient
• soft tissue component• consists of chronically or subacutely inflammed connective tissue filling the intertrabecular areas of bone• scattered sequestra + pockets of abscess formation
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)
Radiographic Features
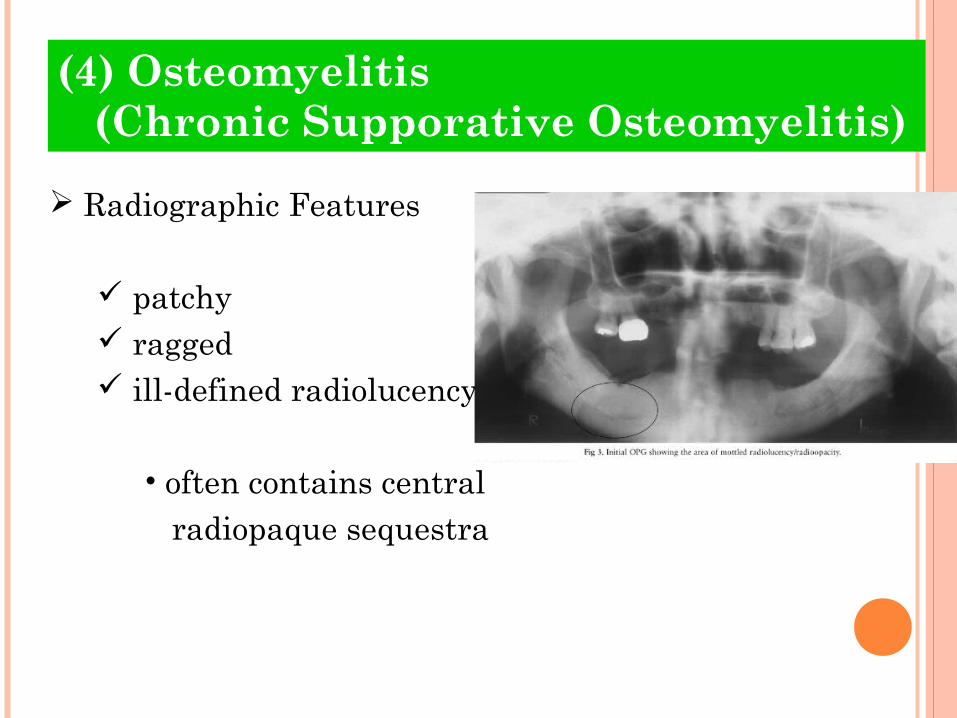
patchy ragged ill-defined radiolucency
• often contains central radiopaque sequestra
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

Radiographic Features
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

Treatment
difficult to manage medically
• pockets of dead bone• organisms are protected from antibiotic drugs
due to surrounding wall of fibrous connective tissue
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

Treatment
surgical intervention is mandatory
antibiotic medications are similar to those used in acute form
• but must be given intravenously in high doses
(4) Osteomyelitis (Chronic Supporative Osteomyelitis)

References:References:
BooksBooks
Neville, et. al: Oral and Maxillofacial PathologyNeville, et. al: Oral and Maxillofacial Pathology 33rdrd Edition Edition
• (pages 138-144) (pages 138-144)