Embed Size (px)
Citation preview
ASSIGNMENT: OCCLUSION
By Dr.Sukhia
Student: Uzma Jan
Roll # 48
BDS Batch III
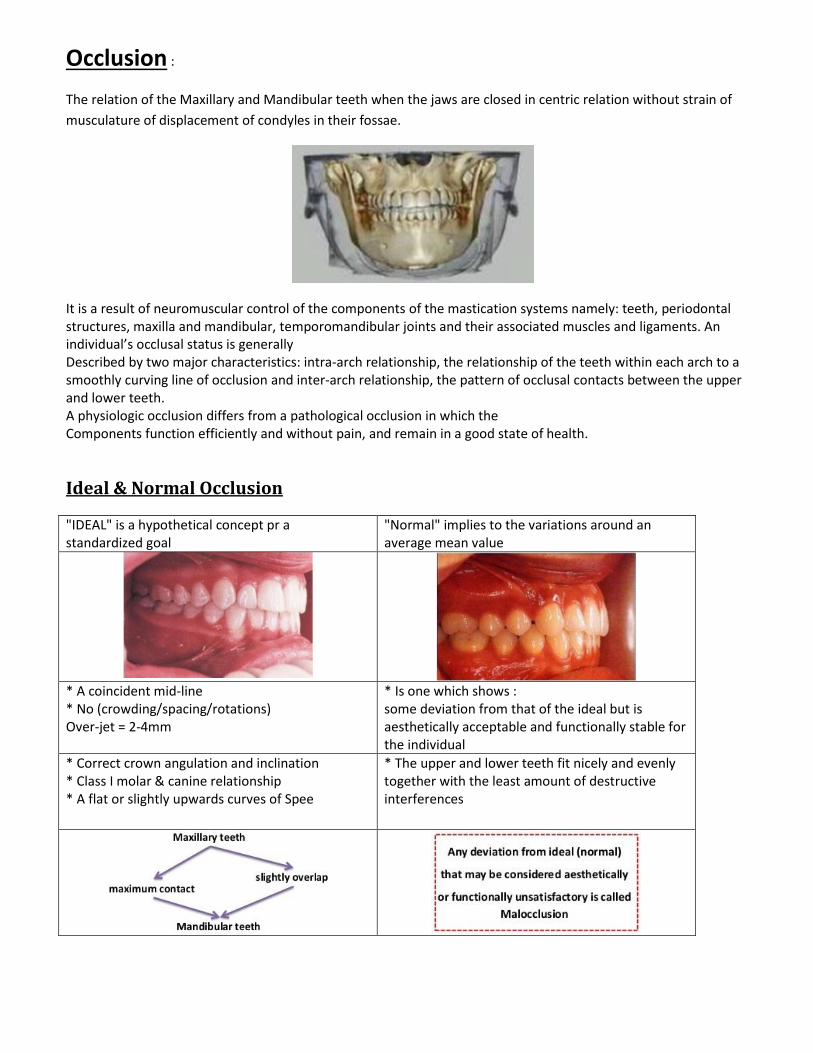
Occlusion :
The relation of the Maxillary and Mandibular teeth when the jaws are closed in centric relation without strain of
musculature of displacement of condyles in their fossae.
It is a result of neuromuscular control of the components of the mastication systems namely: teeth, periodontal structures, maxilla and mandibular, temporomandibular joints and their associated muscles and ligaments. An individual’s occlusal status is generally Described by two major characteristics: intra-arch relationship, the relationship of the teeth within each arch to a smoothly curving line of occlusion and inter-arch relationship, the pattern of occlusal contacts between the upper and lower teeth. A physiologic occlusion differs from a pathological occlusion in which the Components function efficiently and without pain, and remain in a good state of health.
Ideal & Normal Occlusion
"IDEAL" is a hypothetical concept pr a standardized goal
"Normal" implies to the variations around an average mean value
* A coincident mid-line * No (crowding/spacing/rotations) Over-jet = 2-4mm
* Is one which shows : some deviation from that of the ideal but is aesthetically acceptable and functionally stable for the individual
* Correct crown angulation and inclination * Class I molar & canine relationship * A flat or slightly upwards curves of Spee
* The upper and lower teeth fit nicely and evenly together with the least amount of destructive interferences

CENTRIC OCCLUSION
* The maxillary teeth OVERLAP the mandibular ones
* The mesial surfaces of the upper & lower central incisors are in one line at the median plane

CURVE OF SPEE
The Curve of Spee (called also von Spee's curve or Spee's curvature) is defined as the curvature of the mandibular
occlusal plane beginning at the tip of the lower cuspid and following the buccal cusps of the posterior teeth,
continuing to the terminal molar.
CURVE OF WILSON
The curvature of the cusps of the teeth as projected on the frontal plane. That of the mandibular dental arch is
concave and that of the maxillary dental arch is convex.
LEEWAY SPACE
The amount by which the space occupied by the primary canine and first and second primary molars exceeds that
occupied by the canine and premolar teeth of the secondary dentition, usually averaging 1.7 mm on each side of the
dental arch.
OVERBITE
Overbite describes the amount by which the upper anterior teeth overlap the lower anterior teeth in the vertical
plane. A normal overbite exists when the upper anterior teeth overlap the lower anterior teeth by approximately 2
mm when the posterior teeth are in contact.

In some cases, the anterior teeth contact with no overbite at all, and this is called an edge-to-edge relationship.
When the overbite exceeds 2 mm we speak of a deep overbite or deep bite. In extreme cases, the incisal edges of
the anterior teeth may contact the gingiva in the opposing arch (e.g. lower anterior biting directly into the palate).
Deep overbites may limit mandibular movements, and are considered to be potentially destructive
Normal overbite, no overbite and deep overbite.
Over jet is the amount by which the upper anterior teeth protrude beyond the lower incisors in the horizontal plane. An over jet of about 2 mm is considered normal. Severe over jets are regarded as unattractive-we refer to them as protruding or buck teeth.
Normal overjet, no overjet, severe overjet.
Open bite exists if there is no contact between the upper and lower anterior teeth when the posterior teeth are in contact. This condition often occurs due to thumb or finger sucking, or a tongue-thrusting habit.

OPEN BITE
Normal occlusion is when the buccal cusps of the lower posterior teeth occlude in the central fissures of the upper posterior teeth. The incisal edges of the lower anterior teeth normally occlude lingually to the incisal edges of the upper anterior teeth. Cross-bite exists if the upper teeth occlude lingually to the lower. Cross-bite may occur anteriorly or posteriorly, bilaterally or unilaterally, and may involve one or more teeth.
Anterior cross bite exists if an upper anterior tooth occludes lingually to the lower anterior teeth
ANTERIOR CROSSBITE
Posterior cross bite exists if the buccal cusp of an upper posterior tooth occludes in the central fissure of the lower posterior tooth, that is, lingually to its normal position.
Normal posterior relationship, unilateral, right-sided posterior cross bite and bilateral posterior cross bite.

Malocclusion
Malocclusion may be defined as a condition where there is departure from the normal relation of the teeth to other
teeth in the same dental arch and / or to teeth in the opposing arch.
In Normal Occlusion the line of occlusion passes through
Classification based on intra-arch and inter-arch problems
1. Malposition’s of individual or group of teeth in the same arch i. Sagittal Problems - Labioversion - Linguoversion - Mesioversion - Distoversion ii. Transverse problems - Crowding - Spacing - Linguoversion - Buccoversion iii. Vertical problems - Supraversion - Infraversion iv. Rotated teeth v. Transposition of teeth
2. Mal-relation b/w upper & lower dental arches Sagittal * Class II malocclusion * Class III malocclusion II. Transverse * Cross bites, scissor bite * Midline shift III. Vertical * Deep Bite * Open Bite
Malposition of individual teeth:
The direction of the deviation of a tooth from the line of normal occlusion is identified by adding the suffix- version
to the direction of deviation, as follows:
Mesioversion:- Mesial to the normal position Distoversion:- Distal to the normal position Labioversion:-Towards the lip-Maxillary and mandibular anterior teeth. Buccoversion:- Towards the cheeks-Maxillary and Mandibular posterior teeth Palatoversion:- Towards the palate-Maxillary Teeth Linguoversion:- Towards The Tongue-Mandibular teeth Supraversion:- Erupted past the line of occlusion-Over erupted Infraversion:- Short of the line of occlusion-Submerged Torsiversion:- Rotated of its long axis

Labioversion A tooth that has assumed a position labial to normal
Lingoversion Position lingual to normal
Palatoversion Position palatal to normal
Buccoversion Position buccal to normal
Supraversion Over-Erupted beyond the level of occlusion
Infraversion Depressed below the line of occlusion, for example, primary tooth that is submerged or ankylosed
Torsiversion Turned or rotated

Malrelation of the upper and lower dental arch is
Analyzed in the three planes of space:
2. Malrelation b/w upper & lower dental arches Sagittal * Class II malocclusion * Class III malocclusion III. Transverse * Crossbites, Scissor Bite * Midline Shift III. Vertical * Deep Bite * Open Bite
Malocclusions are classified numerically according to Angle's classification as follows:
Class I malocclusion
Class II Division 1 malocclusion
Class II Division 2 malocclusion
Class III malocclusion.

Class 1 malocclusion
The maxilla is in normal relationship to the mandible and the first molar relationship is also normal. Class I malocclusions are common and include crowding problems (tooth size greater than the arch size), rotated or malpositioned teeth, cross bite, open bites or deep bites.
Class I malocclusion — normal relationship of first molars. Maxilla and mandible in normal relationship
Class II malocclusion
In a Class II malocclusion, the mandible is distal in its relationship to the maxilla, and therefore the lower first molar is distal in its relationship to the upper first molar. Compare this with the normal relationships found in graphics above. The subdivisions of Class II malocclusion are based on the inclination and positioning of the upper anterior teeth.
Class II malocclusion — the lower first molar is distal in its relationship to the upper first molar.

Class II Division 1 malocclusion
The lower first molar is distal to its normal relationship to the upper first molar, and the lower jaw is distal to its normal relationship to the upper jaw. The upper incisors protrude labially. Overjet is always greater than normal. Typically prominent or ‘buck teeth’.
Class II Division 2 malocclusion
The lower first molar is distal to its normal relationship to the upper first molar. The lower jaw is distal to its normal relationship to the upper jaw. The upper central incisors incline lingually, and the upper lateral incisors appear to flare labially. There may also be a severe overbite, with the upper anterior teeth covering all or nearly all of the lower interiors.
Class III malocclusion
The lower first molar is mesial to its normal relationship to the upper first molar, and the mandible is mesial in relationship to the maxilla. There will be a cross bite affecting all the anterior teeth, and the appearance is that of a prominent lower jaw.
Class III malocclusion — anterior frostbite and mesial relationship of the lower first molar
Question 2:- What are the disadvantages of bad occlusion?
Answer- There are five main muscles that control your ability to open and close your mouth. Together these muscles
can generate tremendous forces when chewing, clenching and grinding your teeth. If a misalignment of the teeth is
present, these large forces can be translated form the misaligned teeth as destructive forces to the ligaments and
bone that hold the teeth in place, the muscles of the head and neck and the jaw joint.
If left untreated, malocclusion could lead to:
Chronic headaches
Temporomandibular joint disorder (TMJ)
Muscle pain
Tooth movement
Tooth loss
Injuries to the teeth
Tooth wear
Tooth sensitivity.
Abnormal alignment of teeth
Abnormal appearance of the face
Difficulty or discomfort when biting or chewing
Speech difficulties (rare), including lisp
Mouth breathing (breathing through the mouth without closing the lips)
Question 3:- What is wrong with your malocclusion?
Answer - I have Class 1 malocclusion (spacing between teeth)
Question 4:- Why do you have malocclusion?
Answer- It is inherited and runs in our family





























