Embed Size (px)
Citation preview

CASE REPORTS
Blood, Vol. 55, No. 2 (February), 1980 253
“Microgranular” Acute Promyelocytic Leukemia: A Distinct
Clinical, Ultrastructural, and Cytogenetic Entity
By Harvey M. Golomb, Janet D. Rowley, James W. Vardiman, Joseph R. TeSta, and Ann Butler
Three patients with acute leukemia, disseminated intravascular coagulation, and a specific acquired chromosome
abnormality [t (1 5;1 7)] were found by transmission electron microscopy to have the typical distribution of granules seen in
promyelocytes. However, the average granule sizes were 1 20. 1 70, and 1 80 nm, respectively, for the three patients,
significantly less than the 250-nm resolution of light microscopy. We regard the leukemia in these three patients as
comprising a distinct clinical, ultrastructural, and cytogenetic entity that we have chosen to call � ‘microgranular’ acute
promyelocytic leukemia.
A CCORDING to the criteria of the French-Amen-
can-British (FAB) cooperative study group, the
diagnosis of acute promyelocytic leukemia (APL)
should be made only when the “great majority” of
cells are abnormal promyelocytes whose cytoplasm is
packed with coarse granules and which have promi-
nent Auer-like bodies. Clinically, APL is a form of
acute leukemia characterized by episodes of hemor-
rhage and by disseminated intravascular coagulation
(DIC).2 Cytogenetically, a specific chromosome
abnormality [t (15;I7)J has been identified in patients
with APL;35 this translocation has not been reported
in any of the other acute leukemias of the FAB
classi fication 6
In 1978, we reported on a patient whose bone
marrow appeared, by light microscopy, to be similar
morphologically to that in acute mycloblastic
leukemia with maturation. In addition to DIC, the
patient was found on cytogenetic analysis to have the
I 5; 17 translocation. The characteristic distribution
and morphology of granules seen in APL were
observed only when transmission electron microscopy
(TEM) was used.7 More recently, in reviewing our
experience from 1973 to l’i18,� we briefly alluded to a
similar case. The present report was prompted by a
third identical patient who was first examined in early
1979. We now describe in detail three patients with
DIC, a t(l5;l7), and a typical distribution of granules
in promyelocytes, which, in most cells, could be
observed only with TEM.
MATERIALS AND METHODS
Wright-stained peripheral blood (PB) and bone marrow (BM)
aspirates obtained from the 3 patients were examined, and 500-cell
differential counts were done. The PB and BM specimens were
studies with peroxidase, periodic acid-Schifi, a-naphthyl acetate
esterase (ANAE) with and without sodium fluoride, a-naphthyl
butyrate, naphthol AS-D-chloroacetate esterase, and acid phospha-
tase reactions.
Spicules from BM aspirates were prepared for TEM by conven-
tional methods. Preparation and analysis of chromosomes from BM
and PB were as previously described.9 All samples were analyzed
with Q banding.tm#{176}G banding” and reverse (R) banding’2 were each
used in the analysis of one sample from patient I to allow precise
identification of the I 5; 17 rearrangement.
Case 1
A detailed case report was presented previously.1
Case 2
The patient, a 27-yr-old black woman, was admitted to the
Obstetrics Service in June 1978, at approximately 15 wk into her
first pregnancy, because of bleeding gums and hematuria. One week
prior to admission, the patient experienced dull lower abdominal
pain that caused fl() distress. At the same time, she had bleeding
gums. She saw her dentist, who cleaned her teeth and started her on
penicillin tablets. Her gums continued to be painful, and I day prior
to admission she noticed blood-tinged urine. On the day of admis-
sion. gross hematuria had developed. The patient also had bruised
easily for several days, but she denied having rectal or vaginal
bleeding. No fever or cough was present. The past medical history
included a previous admission 5 yr earlier for repair of an umbilical
hernia.
Physical examination revealed a blood pressure of I 20/60 mm
Hg. a regular pulse of 90/mm, and regular respirations of I 6/mm;
the patient was afebrile, The skin contained multiple ecchymoses.
The ocular fundi showed no evidence of hemorrhage or exudate. The
gums were swollen and bleeding and were covered with petechiae.
The chest was clear, and the abdomen was protuberant without a
palpable liver or spleen. The findings in the remainder of the
examination were unremarkable; no localized neurologic signs were
discovered.
The initial laboratory examination revealed a white blood cell
(WBC) count of 10.9 x 109/liter with l7 bands. 5� lymphocytes,
4% monocytes, and 9#{216}(3�,myeloblasts. The hematocrit (H) was
29.3% and the platelet count I I x l09/liter. The patient was
immediately transferred to the Hematology Service. Routine chem-
istry laboratory values on the day of admission were within normal
limits. However, the plasma fibrinogen was 0.07 g/liter (normal,
0.1-0.4 g/liter). The prothrombin time (PT) was 20.3 see, with a
control of 12.4 see, and the partial thromboplastin time (PTT) was
From the Departments of Medicine and Pathology, Univer.sitt’ of
(‘hicago, and the Franklin McLean Memorial Research Institute
(operated b�v the University of Chicago for the Department of
Energy under Contract EY-76-C-02-0069), (‘hicago, Ill.
Supported in part by the Hematology Research Foundation, the
Thomas Moore Fund, the Cancer Research Foundation, and Grant
CA lo9lOfrom the National Institutes of Health.
Submitted July 18, 1979; accepted October 10, 1979.
Address reprint requests to Harvey M. Golomb, M.D., Box 420,
950 East 59th Street, Chicago, Ill. 60637.i(� 1980 by Grune & Stratton, Inc.
0006-4971/80/5502-OOl ISOl.00/0
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

254 GOLOMB ET AL.
Table 1 . Clinical Characteristics
Survival
Patient
Age(yr) Sex Race Initial Therapy Response
From
Diagnosis
(mo) DIC
PreviouslyReported
(Ref)
1 20 M B Ara-C, TG CR 8 + 7
2 27 F B Ara-C, TG, Daun CR 7 + + 8
3 25 F W Ara-C, TG, Daun PR 2 + + -
M, male; F, female; B. bI ack; W, whit e; Ara-C, cytosine arabinoside; TG, 6 thioguanine; Daun, daunorubicin; CR, complete re sponse; PR, partial
response; DIC. disseminated intravascular coagulation.
38.5 sec with a control of 26.2 sec. Fibrin degradation products
(FDP) were reported between 40 and 80 �g/ml (normal, less than
20 �zg/ml).
The patient was diagnosed as having acute myelogenous or
myelomonocytic leukemia at the time of admission, underwent a
therapeutic abortion, and was begun on chemotherapy I day later.
Chemotherapy consisted of our TAD regime, which included 6-
thioguanine (100 mg/sqm every 12 hr for 5 days), cytosine arabino-
side (200 mg/sqm with continuous 24-hr infusion for 5 days), and
daunorubicin (60 mg/sqm iv. push daily for 3 days). A BM biopsy
done approximately I mo after the initiation of therapy showed a
cellularity of 1 5% with clusters of blasts. A second cycle of chemo-
therapy was started 5 wk after the initial one; at the start the
hematocrit was 27.9%, the WBC count 3.7 x 109/liter, and the
platelet count 200 x l09/Iiter. A BM specimen obtained I mo later
showed residual acute leukemia; at that time, the Hct was 31.9%,
WBC count 22.3 x 109/liter, and the platelet count 367 x lOt/liter.
The patient now refused any further inpatient therapy and was
begun on 6-thioguanine. 40 mg bid., as an outpatient. One month
later, a repeat BM specimen was 80% cellular. No evidence of
residual disease was found; 6-thioguanine was stopped. The patient
developed HAA-positive hepatitis 2 mo later (i.e., 5 mo after her
initial diagnosis and treatment). A BM specimen obtained in
December 1978 appeared normal, with less than 5% blasts. The
patient was placed on maintenance therapy with only hydroxyurea
and BCNU. She was last seen 9 mo after initial diagnosis and
treatment, was doing well, had no complaints, and showed a steady
weight gain. Blood samples at that time showed a WBC count of 5.1
x l09/liter, Hct of 37.9%, and a platelet count of 165 x 109/liter.
Case 3
The patient, a 25-year-old white woman, was in excellent health
and studying at a college in California until approximately 4 days
prior to admission when she noted multiple ecchymoses as well as
petechiae on her thighs and lower legs. About 2 days prior to
admission, she felt feverish without specific complaints. She was
referred to a school physician, who noted a WBC count of 4.35 x
109/liter, Hct of 30.5%, and a platelet count of 14 x l09/liter. The
differential WBC count showed 1% eosinophils, 1% bands, 14%
neutrophils, 83% lymphocytes, and I % monocytes. She was referred
to a hematologist, who obtained a sternal BM aspirate and made a
diagnosis of acute leukemia, probably myeloblastic. She was re-
ferred to the University of Chicago for further evaluation and
therapy.
The patient, who was mildly anxious but in no acute distress,
admitted to a weight loss of approximately 1 5 lb during the previous
6 mo. Her menstrual period approximately 1 wk earlier had been
heavy and longer than usual by 3 days. She had had no epistaxis,
melena, hematemesis, or hematuria, but complained of persistent
oozing from the BM aspiration site in the sternum.
During physical examination, her temperature was 37.8#{176}C,the
pulse 100/mm and regular, respirations 14/mm and regular, and
the blood pressure I 30/80 mm Hg. The patient was slightly pale,
with multiple ecchymoses on her extremities and on her soft palate.
There was oozing from the sternal marrow site. The remainder of
the findings in the examination were unremarkable; no adenopathy,
hepatosplenomegaly, or abnormal neurologic findings were
observed. Admission laboratory values included a WBC count of 2.1x l09/liter, with 18% neutrophils, 76% small Iymphoctyes, 4%
monocytes, 1% blasts, and 1% metamyelocytes. The platelet count
was 5 x lO9/liter and Hct 18%. Electrolyte levels and other blood
chemistry tests at the time of admission were normal. Fibrinogen
was 0. 1 g/liter (normal, 0. 1-0.4 g/Iiter). The initial PT was I 8.5 sec
(control, 1 1 .9 see), and the PTT was 23.8 sec (control, 25. 1 see). An
admission cardiogram showed a sinus tachycardia with a rate of
120/mm and borderline left ventricular hypertrophy. Nonspecific
T-wave inversion was also seen. A chest x-ray showed no abnormali-
ty.
A BM aspirate obtained at the time of admission revealed a
hypercellular marrow, with numerous blasts replacing the normal
marrow elements. Many blasts had convoluted nuclei and very fine
cytoplasmic granules. A bone core biopsy done at the same time
showed an overall cellularity of 99%; no megakaryocytes and few
erythroid precursors were detected. The abnormal cells had folded,
Table 2. Light and El ectron M icroscopic Characte ristics (Bone Marrow)
Light MicroscopyCytochemistry
Ultrastructure
Average
GranulePercent
Hyper-
Percent
Faintly Percent Percent�‘anuIar Granulated Auer Px Positive ANAE Size Auer
Patient Promyeiocytes “Promyelocytes” FAB Bodies Nucleus Cells Cells RER (nm( Bodies
1 9 22 M2 Rare Irregular, folded,
bibbed
40 <5 Dilated 120 Rare
2 5 45 M2 Rare Irregular, folded,
bibbed
90 <5 Dilated 1 70 Rare
3 10 62 M� Rare Irregular, folded,
bibbed
99 40 Dilated 180 Rare
Px, peroxidase; ANAE. abpha-naptyl acetate esterase; RER, rough endoplasmic reticulum.
The presence of NaF-inhibited ANAE activity in 40% of the cells could indicate an M4 classification for this case if cytochemistry alone were
considered.
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

,.. . ‘:. � ,,il
�
I . �
� � �
‘ ‘I
MICROGRANULAR APL 255
irregular nuclei with large nucleoli. Approximately 60% of the cells
contained fine cytoplasmic granules; large, dark azurphilic granules
were seen in only 10% of the cells. One day after admission, FDP
were between I 280 and 2560 big/mI (normal, less than 20 jzg/ml).
Within 24 hr of admission and upon return of the FDP results, the
patient was begun on combination chemotherapy for her acute
leukemia. The treatment consisted of TAD, as for case 2. In
addition, continuous-infusion heparin was begun at 2000 U intrave-
nous push, to be followed by 600 U every hour continuously.
A repeat BM aspirate obtained I 3 days after the start of
treatment, when the hemtocrit was 35% (posttransfusion), WBC
count 0.4 x l09/liter, and the platelet count 69 x lOt/Iiter, showed
5% cellularity, with the majority ofcells consisting of promyelocytes
and blasts. At this time, the second course ofTAD was begun at the
same dosages and completed 5 days later. A BM specimen obtained
approximately 3 wk after the start of the second cycle of TAD
showed an overall cellularity of less than I %, with very few hemato-
poietic elements. No clusters of immature myeloid cells were noted.
A repeat BM aspirate 2 wk later, at a time when the WBC count
was 0.1 x 109/liter, showed little cellularity. Two weeks later, or
approximately 2 mo after the initial admission, the patient had a
WBC count of 2.4 x 109/liter with 52T neutrophils, 40 lympho-
cytes, 7% monocytes, and no blasts. The platelet count was 44 x
lOt/liter and the hematocrit 32%. Evaulation I I wk after initiation
ofTAD demonstrated normal blood counts, however, a BM aspirate
showed residual leukemia.
Clinical
RESULTS
The clinical characteristics of all patients are
summarized briefly in Table 1. All three patients
presented with bleeding complaints; the first two had
bleeding gums, the third had multiple ecchymoses as
well as a prolonged menstrual cycle. All three had
laboratory evidence of DIC with increased FDP.
Light and Electron Microscopy
Light-microscopic evaluation showed all three
patients to have less than 50% hypengranular promyel-
ocytes in their BM, but to have a significant percent-
age of promyelocytes with fine, dust-like granules,
often concentrated in one area of the cytoplasm (Table
2). In each case, more than 50% of the cells had
irregular, folded, and bibbed nuclei that resembled
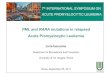
monocytic nuclei (Fig. I ). Cytochemically, cells from
Fig. 1 . Representative cells from each of the three casesshow only faint cytoplasmic granulations by light microscopy.Similarities of nuclear irregularities are obvious (Wright Giemsa,*750).
.�#{149}�U%,5:�
. ,‘, i�:�
� .�,,
..; .
:� ,� � � �
;&. � �
� - %%‘�,It �
., ..%.. “.�‘:p�� ..k�::
‘a :..1�#{216}�; . ,� ‘ .‘� ,,�.
�t* � . : ‘. %,W.�.‘ c...,. ..
� :�‘. , .‘
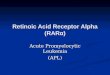
Fig. 2. (A) Low magnification transmission electron micro-graph of a bone marrow spicube from patient 3. Note the large
folded nuclei and the primary granules scattered throughout thecytoplasm (*4700). (B) Higher magnification of a cell from thesame patient. Many primary granules and dilated rough endoplas-
mic reticulum are visible (x18,200).
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

30
2
5,
0
3
�-A
401
T� B
0 � 200 300 400
256 GOLOMB ET AL.
patients 1 and 2 were positive for peroxidase and
naphthol AS-D-chloroacetate esterase, and fewer than
5% of the cells showed any positivity with the nonspe-
cific esterase reaction. For patient 3, more than 95% of
the abnormal cells had an intense peroxidase and
naphthol AS-D-chloroacetate esterase reaction. How-
ever, 40% of the cells showed a moderate reaction with
alpha-naphthyl acetate, and this esterase activity was
inhibited with sodium fluoride.
Ultrastructural examination demonstrated a dilated
endoplasmic reticulum in all three cases (Fig. 2). The
average granule sizes were I 20, 1 70, and I 80 nm for
patients I , 2, and 3 respectively. (The limit of resolu-
tion of light microscopy is approximately 250 nm.’3)
All granules were dense; those in case 3 were not
typical of monocytic differentiation despite the cyto-
chemical reactions observed. A histogram showing the
distribution of granules, according to size, of each of
the three patients is given in Fig. 3. Granules larger
than 250 nm comprised only 2%, 1 5� and 9� of the
total population of granules in patients I , 2, and 3
respectively. In addition to the data from these three
patients, the distribution of granule size is included for
two previously reported cases of classical hypengranu-
lan promyelocytic leukemia from our institution (Fig.
3, A and B). One of these patients3 had granules of an
average size of 640 nm, and all were larger than 250
nm; the second patient4 had granules of an average
size of 270 nm, approximately 50% being larger than
250 nm.
Cytogenetic
In each of the three patients, a I 5; 1 7 rearrangement
was present in a high percentage (799�-l00%) of the
metaphases from the initial sample (Table 3). The
structural rearrangement seemed to be identical in all
of the abnormal metaphases from patients I and 2 and
in one of the metaphases from patient 3 [t (15:17)
(q25?; q22?)]. All of the other abnormal metaphase
cells in patient 3, however, had another rearrange-
ment; whereas the translocation between nos. I 5 and
17 appeared to involve the breakpoints mentioned
above, the 17q- chromosome had additional uniden-
tified bands on the short arm (Fig. 4). The I7p+ q-
chromosome was submetacentnic with conventional
stain and did not appear to be an isochromosome of the
long arm of the deleted no. I 7 when it was examined
with quinarcrine fluorescence.
All three patients had one or more cytogenetic
analyses during the period of response, and each had a
normal karyotype during this time. Patient I showed
clonal evolution of the karyotype to further complexity
during relapse.7 Patients 2 and 3 continued to have
normal karyotypes as of May I 979.
Diameter of granules (nm)
Fig. 3. Histograms 1 . 2 and 3 illustrate the distribution ofprimary granules in the cells of three patients with microgranular
acute promyebocytic leukemia (API). The majority of granuleshave a diameter less than 250 nm. the limit of resolution of lightmicroscopy. Histograms A and B show the distribution of primarygranule size in the cells of two previously reported patients with
typical API, diagnosed by light microscopy. Although there is aheterogeneity of granule size, many granules with a diametergreater than 250 nm exist.
DISCUSSION
It seems clear that these three patients belong to a
subgroup of ANLL that has only recently been identi-
fled 7,8.14,15 There is disagreement as to the correct
classification of these patientst”5 It is our contention
that the clinical syndrome of DIC, the ultrastructural
determination of numerous primary granules, and the
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

MICROGRANULAR APL 257
Table 3. Summary o f Cyto genetic Findings
Patient
Sample
Date
Sample
Source’
No. of Metaphases
PercentWith
t) 1 5; 1 �)t Karyotype
No. of Chromosomes
Totalt<44 44 45 46 >46
1 12-01-76 BM, PB 5 0 4 22 0 31(14) 79 46,XY/46,XY,t)15;17)(q25?;q22?(�1
2 6-12-78 BC 3 2 7 10 0 22(14) 93 46,XX�/46.XX,t(15;17)(q25?;q22?)
3 2-6-79 BM 1 6 10 18 0 35(21) 100 46,XX,t)15;17)(q25?;q22?)�
‘BC. bone core biopsy; BM, bone marrow aspirate; PB, peripheral blood (without PHA).
tNumber in parentheses indicates number of informative metaphases examined in detail with fluorescence.
�Ca(culated as percent informative metaphases examined with fluorescence.
§Only one metaphase seen in this sample showed a normal karyotype.
#{182}Subsequent samples at the time of relapse showed clonal evolution to a more complex karyotype.
�ln 20 of 2 1 banded metaphases, the 1 7q - had additional unidentified bands on the short arm.
cytogenetic findings of the t(15:17) combine to iden-
tify this subgroup as a variant of acute promyclocytic
leukemia, which we have chosen to call the “micro-
granular” type.
All 3 patients had DIC, which is consistent with the
observation of Sultan et al.16 that, of 140 consecutive
patients who had ANLL, 17 of 18 patients with
abnormal coagulation tests had APL.
Although our three patients had less than 10%
hypergranular cells, with a larger percentage of cells
containing only dust-like granules by light micro-
scopy, TEM showed that the majority of cells in these
patients contained many granules that were less than
250 nm in size and thus smaller than the limit of
resolution of light microscopy. By light microscopy,
however, similarities were observed in the nuclear
configuration in the cells of these three patients and in
four of our patients with the more classic variety of
Fig. 4. Karyotype of a Q-banded metaphase cell obtained from a BM sample from patient 3. The metaphase has a transbocationbetween the long arms of one no. 15 and one no. 17 [t(15;17)(q25?;q22?)]. The abnormal 17 also has additional unidentified bands on theshort arm. Inset: partial karyotype of pairs 15 and 17 from another metaphase from the same BM sample; there is a t(15;17)(q25?;q22?).but without any alteration of the short arm of the abnormal 17.
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

I1��50 00 50 200250 300 350400430 500
D,omeie� oi g�o,,iiies nm)
Fig. 5. Histogram represents the distribution of primarygranule size in the cells of a patient with acute myelogenousleukemia with maturation (M2). The distribution is similar to thatseen in the cases of microgranular acute promyebocytic leukemia.
258 GOLOMB ET AL.
APL; reniform, folded, and bibbed monocyte-like
nuclei were numerous in each. Cells from all three
patients contained extremely dilated rough endoplas-
mic reticulum (RER), although one patient also had
cells with nondilated RER. Dilated RER in the
promyelocytes of APL patients was recently reported
by Parkin and Brunning.’7
The specificity of the 15;17 translocation for APL
has been suggested by our group in a study of 90
ANLL patients, 4 of whom (including one from the
present study) had the t(l5;17); all 4 had APL.’8
Recently Van Den Berghe et al.5 reported a t(l5;l7)
(q26;q22) in 1 1 of 16 APL patients. A l5;17 translo-
cation has also been reported for APL patients seen by
several other investigators.92’ This rearrangement
was observed in 9 of I 7 APL patients reviewed at the
First International Workshop on Chromosomes in
Leukemia;6 in contrast, it was not seen in any of the
224 patients who had other forms of AN LL.
The 15;17 structural rearrangement in patients I
and 2 was identical to that seen in four of our
previously reported patients with classic hypergranu-
lan promyelocytic leukemia.8 The breakpoints in the
long arm of nos. I 5 and 1 7 in patient 3 also appeared
to be identical to those in these other patients; howev-
er, in patient 3 the 17q- chromosome had additional
unidentified material on the short arm in all but one of
the abnormal cells. The metaphase with the usual
t(15;l7) in patient 3 probably represents the original
abnormal clone, whereas the metaphases with the
I 7p + q - represent a subsequent structural rearrange-
ment in this clone.
Although the diagnosis of “microgranular” APL
seems warranted from the data presented, the positive
ANAE reaction in case 3 remains to be explained.
Analysis of case 3 by TEM showed only primary
granules; there was no evidence of monocytic granules.
Although the positive ANAE reaction is more in
keeping with a monocytic origin of some of the cells, a
similar pattern has been described previously for the
cytochemistry of APL22’23 Thus, the positive ANAE
reaction in case 3 would suggest a FAB classification
of M4 yet TEM evaluation would demand an M3
designation. Cases I and 2 would have been classified
as an M2 by light microscopy and cytochemistry, but
TEM analysis would require an M3 designation.
Recently, Bergen et al.14iS reported on three pa-
tients with a t(15;I7) who showed a type of ANLL
similar to that of the patients in this report. They
classified their patients as AML, although they
acknowledged that they were atypical. Their cases
were characterized by a high WBC count, monocyte-
like myeloblasts, DIC, and a t(I5;17) in the majority
of leukemic cell mitoses. Light microscopy showed
reniform folded nuclei, as described in our three cases;
cytochemistry yielded positive peroxidase, but essen-
tially negative napthal AS-D-chloracetate esterase and
ANAE. Transmission electron micrographs were not
labeled by cases; most cells had reniform nuclei and
sparse primary granules; there was one example of a
cell with multiple Auer rods.
We recently used TEM to analyze the cell ultra-
structure of 25 patients with ANLL (Butler A, et al.,
unpublished observations). One patient, a 37-year-old
white woman, had no DIC, had a normal karyotype,
and was classified by the FAB system as M2 (i.e.,
acute myelogenous leukemia with some maturation).
By TEM analysis, the majority of cells were found to
contain numerous granules that averaged 190 nm in
size and were similar in distribution to those in our 3
patients with microgranular APL (Fig. 5).
It seems to us, therefore, that there are patients with
ANLL that form a distinct subgroup, although there
is some variability in the morphology and cytochemis-
try of the leukemic cells. This group is characterized
by a hematologic history and laboratory evidence of
DIC; by cytochemical findings that are predominantly
myelocytic, but with an occasional case with mono-cytic staining characteristics; by ultrastructural find-
ings of few to many cytoplasmic primary granules that
are usually smaller than the resolution of light micro-
scopy; and by the presence of the t(15;17). In view of
the number of features that are typical of classical
APL, we prefer to classify these patients as APL,
“microgranular” variant. It is apparent, however, that
there is a spectrum of morphological forms from
myeloblastic through promyelocytic to monocytic; the
precise position within this continuum of the patients
presented in this report must await the careful cyto-
genetic, cytochemical, and TEM analysis of additional
patients.
It is important clinically to make the correct diagno-
sis of APL as early as possible in order to initiate
appropriate therapy. Bernard et al.24 showed that
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

MICROGRANULAR APL 259
15. Berger R, Bernheim A, Daniel, M-T, Valensi R, Flandrin G,
daunorubicin can induce remission in about 50% of
APL patients with a median survival of 26 mo.
Drapkin et al.25 suggested that prophylactic hepanin
along with chemotherapy may allow a better chance of
induction remission. Thus, it is important that possible
cases of APL be studied cytochemically, ultrastructu-
rally, and cytogenetically; the determination of the
diagnosis of APL has therapeutic importance.
REFERENCES
I . Bennett J, Catovsky D, Daniel MT. Flandrin G, Galton DAG.
Gralnick NR, Sultan C: IFrench-American-British (FAB) Cooper-
ative groupl. Proposals for the classification of the acute leukemias.
Br J Haematol 33:451-458, 1976
2. Jones ME, Suleem A: Acute promyelocytic leukemia. Am J
Med 65:673-677, 1978
3. Golomb HM, Rowley JD, Vardiman JW, Baron JM, Locker
G, Krasnow S: Partial deletion of long arm of chromosome I 7: A
specific abnormality in acute promyelocytic leukemia’� Arch Intern
Med 136:825-828, 1976
4. Rowley JD, Golomb HM, Vardiman JW, Fukuhara 5, Dough-
erty 5, Potter D; Further evidence for a consistent chromosomal
abnormality in acute promyelocytic leukemia. Int J Cancer 20:869-
872, 1977
5. Van Den Berghe H, Louwagie A, Broeckaert-Van Orshoven
A, David G, Verwilghen R, Michaux JL, Ferrant A, Sokal G;
Chromosome abnormalities in acute promyelocytic leukemia
(APL). Cancer 43:558-562, 1979
6. First International Workshop on Chromosomes in Leukemia,
Chromosomes in Acute Non-lymphocytic Leukemia. Br J l-laematol
39:311-316, 1978
7. Testa JR. Golomb HM, Rowley JD, Vardiman JW, Sweet
DL: Hypergranular promyelocytic leukemia (APL): Cytogenetic
and ultrastructural specificity. Blood 52:272-280, 1978
8. Golomb HM, Testa JR. Vardiman JW, Butler A, Rowley JD;
Cytogenetic and ultrastructural features of de novo acute promyebo-
cytic leukemia, the University of Chicago experience (1973-78).
Cancer Genet Cytogenet I :69-78, 1979
9. Rowley JD; Nonrandom chromosomal abnormalities in hema-
tologic disorders of man. Proc NatI Acad Sci USA 72;152-l56,
I975
10. Caspersson T, Zech L, Johansson C, Modes EJ; Identifica-
tion of human chromosomes by DNA-binding fluorescent agents.
Chromooma 30:215-227, 1970
I 1 . Sun NC, Chu EHY, Chang CC; Staining method of the
banding patterns of human mitotic chromosomes. Caryologia
27:315-324, 1974
12. Verma RS, Lubs HA; A simple R banding technic. Am J
Human Genet 27:1 10-I 17, 1975
13. Raphael 5; Lynch’s Medical Laboratory Technology, Phila-
delphia Saunders, 1976, p 585
14. Berger R, Bernheim A, Daniel M-T, Valensi F, Flandrin G;
Une nouvelle variete de leu#{225}emie aigu#{235}non promy#{233}locytaire auer
translocation t(15;17). Compt Rend Acad Sci Paris 288:1 17-1 19,
I 979
Bernard J; Translocation t(I5;17). leuc#{233}mieaigu#{235}promy#{233}locytaire
et non promy#{233}locytaire. Nouv Rev Fr H#{233}matol 2l;l 17-131, 1979
16. Sultan C, Heilmann-Govault M, Tulliez M: Relationship
between blast-cell morphology and occurrence of a syndrome of
disseminated intravascular coagulation. Br J Haematol 24:255-259,
I 973
17. Parkin JL, Brunning RD; Unusual configurations of endo-
plasmic reticulum in cell of acute promyelocytic leukemia, J NatI
Cancer Inst 61:341-347, 1978
18. Golomb JM, Vardiman JW, Rowley JD, Testa JR. Mintz U;
Correlation of clinical findings with quinacrine-banded chromo-
somes in 90 adults with acute nonlymphocytic leukemia. N EngI J
Med 299:613-619, 1978
19. Okada M, Miyazaki T, Kumota K; 15/17 Translocation in
acute promyelocytic leukaemia. Lancet; 961, 1978
20. Kaneko Y, Sakurai M; 15/17 Translocation in acute
promyelocytic leukaemia Lancet 1 961 , 1978
21. Scheres JMJC, Hustinx TWJ, de Vaan GAM, Rutten FJ;
15/17 Translocation in acute promyelocytic leukemia. Human
Genet43; 115-117, 1978
22. Liso V, Troccoli G, Graude M; Cytochemical study of acute
promyelocytic leukemia. Blut 30:261-268, 1975
23. Shaw MT; Cytochemistry of acute leukemia: A diagnostic
and prognostic evaluation. Semin Oncol 3;219-228, 1976
24. Bernard J, Weil M, Boiron M; Acute promyelocytic leuke-
mia; results of treatment by daunorubicin. Blood 41 489-496, 1973
25. Drapkin RL, Gee TS, Dowling MD; Prophylactic heparin
therapy in acute promyelocytic leukemia. Cancer 41:2484-2490,
1978
ADDENDUM
Since acceptance of this manuscript, the French-
American-British (FAB) Group have suggested recog-
nition of a variant form of hypergranular promyelo-
cytic leukemia (M3) in which the cells are character-
ized by bibbed, multilobed, or reniform nuclei, and
cytoplasm with minimal or no granulation. A few cells
with the features of typical M3 will be present in such
instances. The cases in this report correspond to this
variant group. [Bennet JM, Catovsky D, Daniel MT.
Flandrin G, Galton DAG, Gralnick HR, Sultan C: A
variant form of hypergranular promyelocytic leukemia
(M3). Br J Haem (in press)].
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom

1980 55: 253-259
HM Golomb, JD Rowley, JW Vardiman, JR Testa and A Butler ultrastructural, and cytogenetic entity"Microgranular" acute promyelocytic leukemia: a distinct clinical,
http://www.bloodjournal.org/content/55/2/253.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
For personal use only.on April 3, 2019. by guest www.bloodjournal.orgFrom