Embed Size (px)
Citation preview

19th & 20th November 2016
Fairmont Hotel, Jakarta
www.isicam.org
INDONESIAN SOCIETY OF INTERVENTIONAL CARDIOLOGY ANNUAL MEETING
PCI in High Bleeding Risk
Isman Firdaus
Interventional Cardiologist Consultant
Pusat Jantung Nasional Harapan Kita, Indonesia
19th & 20th November 2016
Fairmont Hotel, Jakarta
www.isicam.org
INDONESIAN SOCIETY OF INTERVENTIONAL CARDIOLOGY ANNUAL MEETING
I have the following potential conflicts of interest to report: Research contracts
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Others
I do not have any potential conflict of interest
Speaker name: Isman Firdaus, MD, FIHA, FAPSIC, FAsCC, FESC, FSCAI
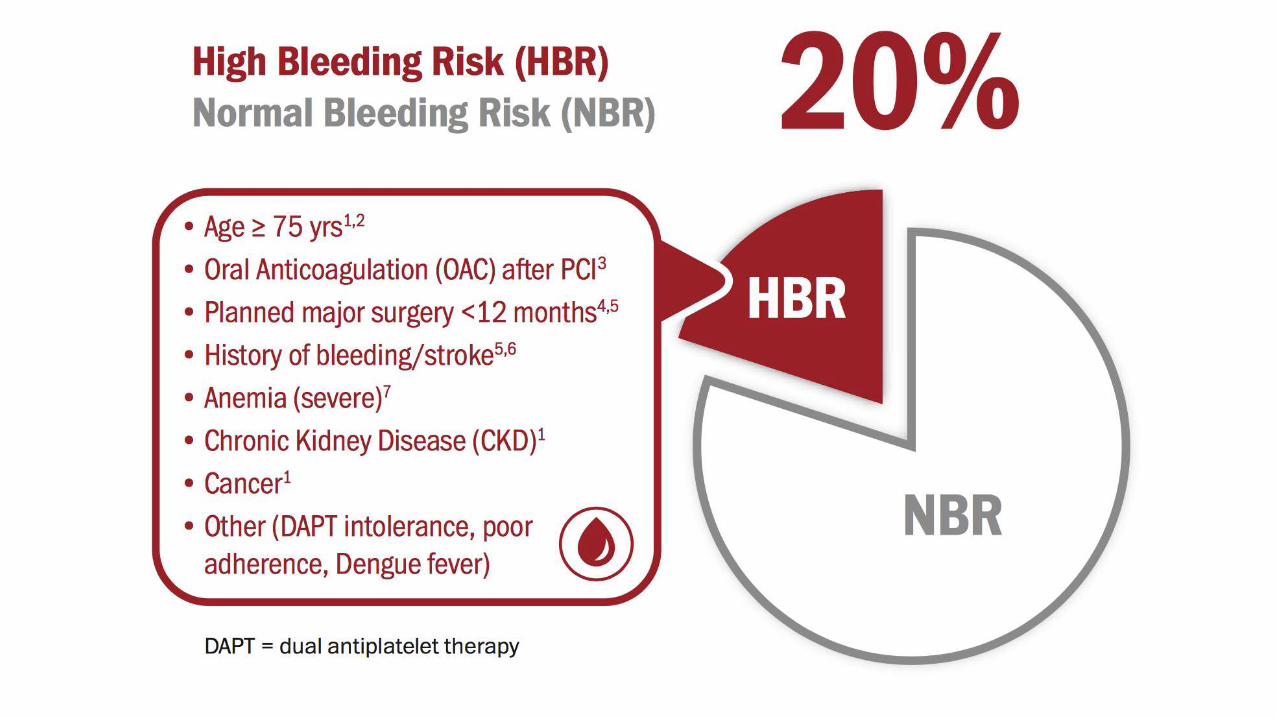
•At Least 20% of PCI patients are High Bleeding Risk
Rao et al. AHJ 2013;166:273-281.e4 Rittger H et al. Herz 2014;39(2):212-8 Faxon et al. Circ Cardiovasc Interv 2011;4:522-34 De Biase et al. Transl Med 2015;11(3):14-23 To et al. Circ Cardiovasc Interv-2009;2:213-21 Wiviott et al. NEJM 2007;357:2001-15 Pilgrim et al. Circ Cardiovasc Interv. 2012;5:202-210 Shanmugam VB et al. Journal of Geriatric Cardiology 2015;12:174−184 Urban P. et al. Am Heart J 2013;165:704-9
CASE 1:
• Male, 48 yo
• History of PCI 4 DES in 2008
• Hospitalized for ORIF surgery due to fibula and tibial fractures in Jakarta Private Hospital
• Aspilet was stopped for 7 days by Orthopedist

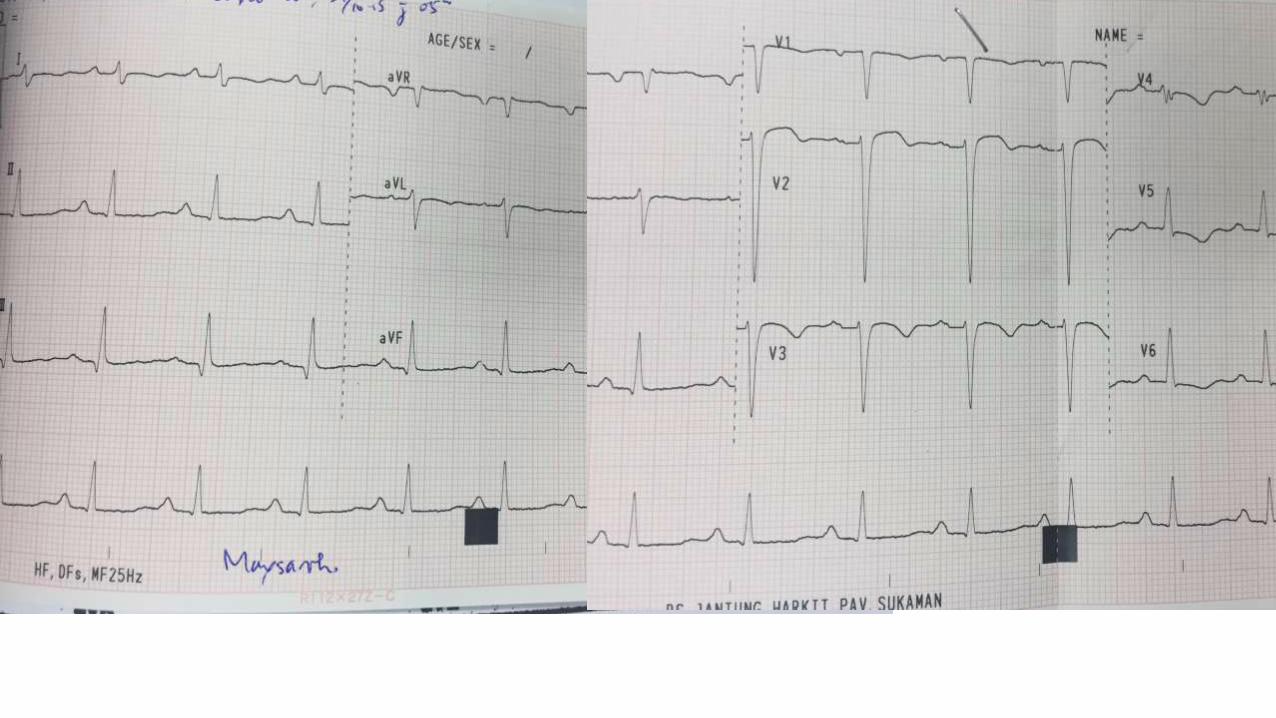
• 2 days before surgery, patient was sufferred refractory progressive angina
• Refractory heart failure
• Orthophedist and Cardiologist preffered for early PCI
• Refferred to PJN Harapan Kita
PJN Harapan Kita
• Planned for Early PCI
• Angiogram showed• LM : Irregularities
• LAD : Irregularities with severe In stent, difuse and long stenosis from proximal to mid part. Distal part was total occlusion due to stent failure
• LCx : Irregularities with difuse and subtotal occlusion at prox-distal part
• RCA : Irregularities with severe and diffuse stenosi, Chronic total occlusion at proximal part
Dx/• NSTEMI (very high risk profile)
• CAD 3 VD , RCA and LAD CTO
• Fibula-tibial Fracture planned for non cardiac surgery

RCA ANGIOGRAM LCA ANGIOGRAM
•Operator incharge decided to suspend PCI and planned for CABG
•Heart Team Conference (intervensional Cardiologist, Cardiac surgeaon, Orthopedist, and Cardiac Intensivist)
preffered for PCI than CABG
Difficulties in Decision and Technique
• Cardiac Surgeon reffused for CABG
• Complex and advance PCI
• Culprite or target vessel in dual CTO lession
• DAPT consideration, required non cardiac surgery (ORIF)
Strategy and Technique
• Single vs Dual Guide JR 3.5/6F and XB 3.5/6F
• Antegrade vs retrograde XTA wire
• Femoral vs radial
• 1st line wire selection : Fielder (XT-A vs XT-R) vs non-Fielder family
• Stent selection : BMS vs DES vs DCS
• Stent selection was very important to Reduced the duration of DAPT after PCI
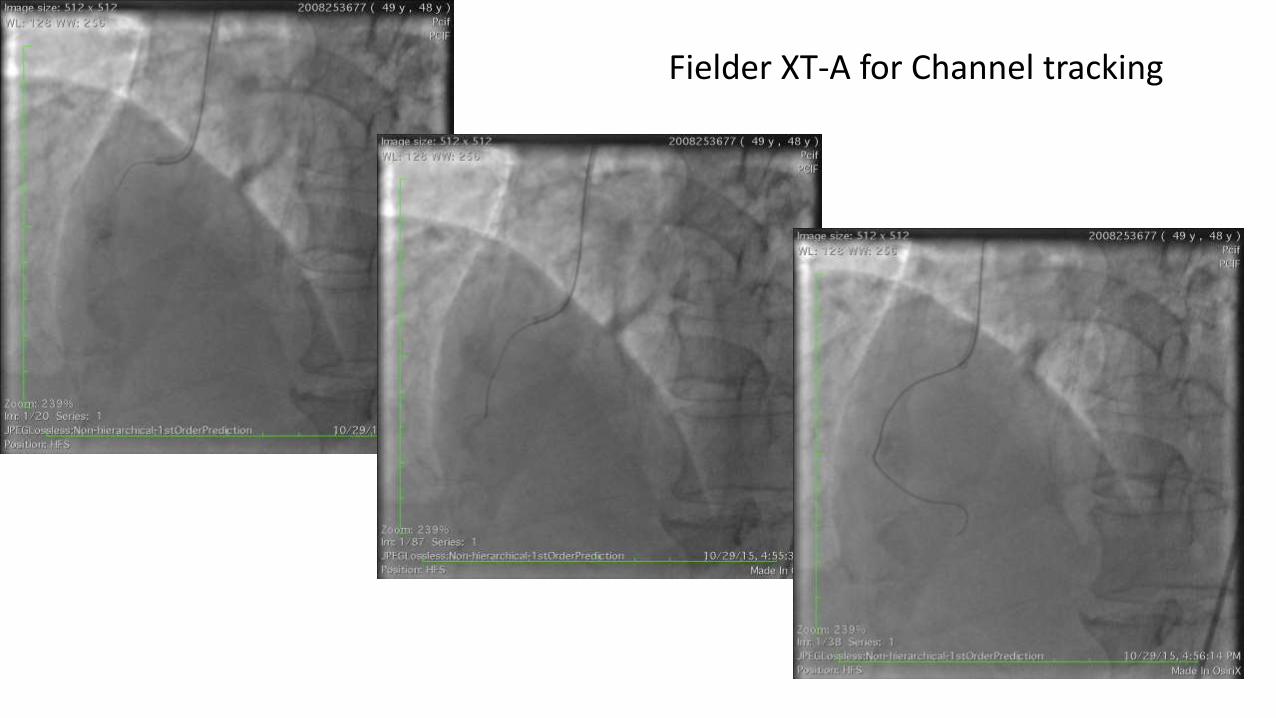
Fielder XT-A for Channel tracking
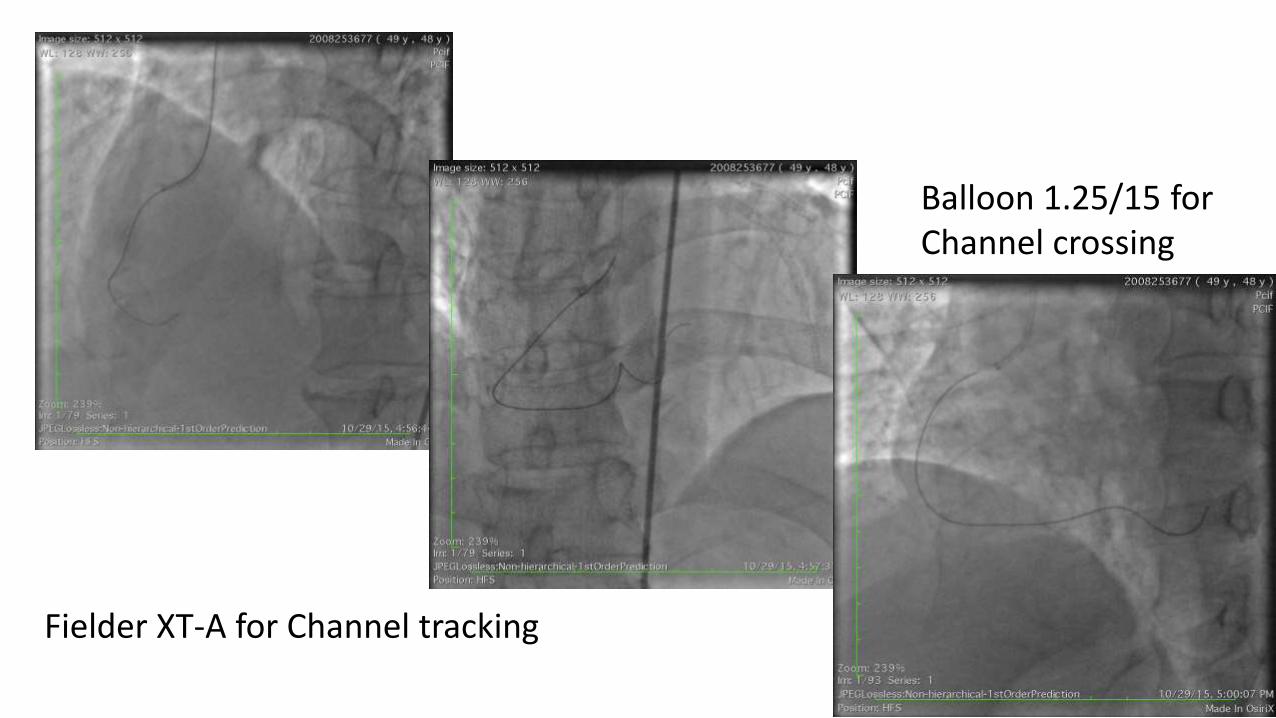
Fielder XT-A for Channel tracking
Balloon 1.25/15 for Channel crossing
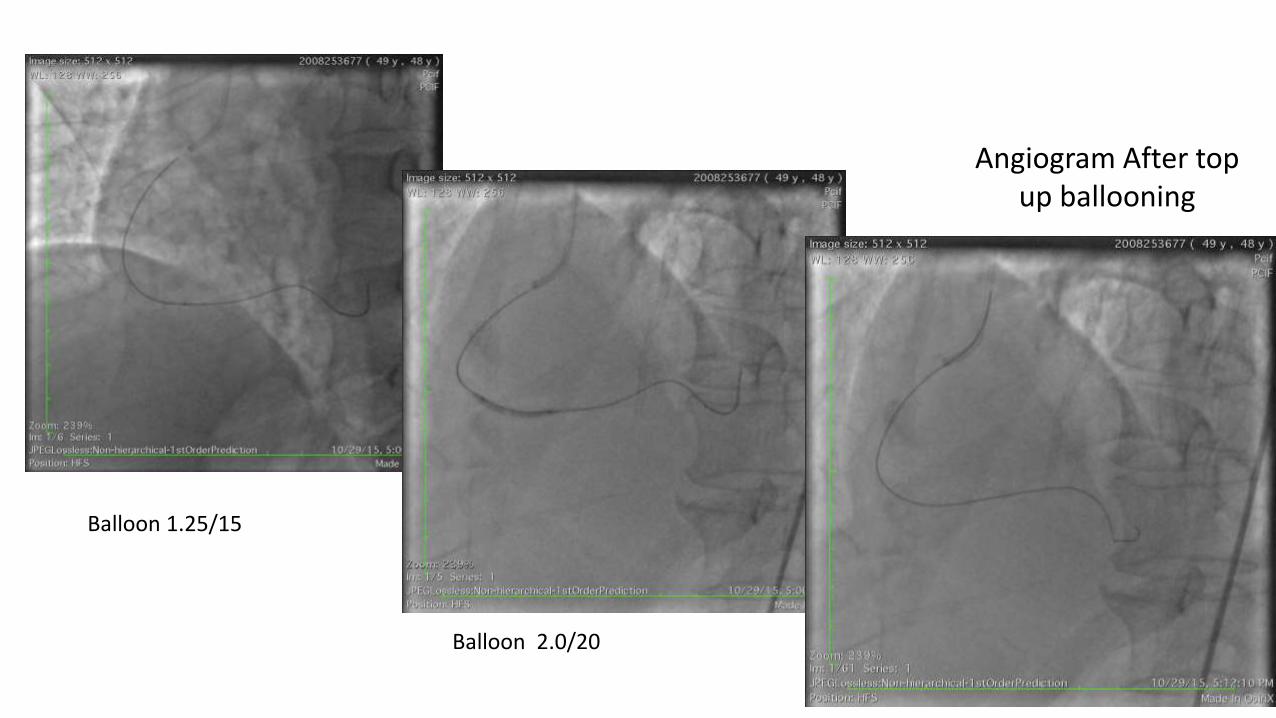
Balloon 1.25/15
Balloon 2.0/20
Angiogram After top up ballooning
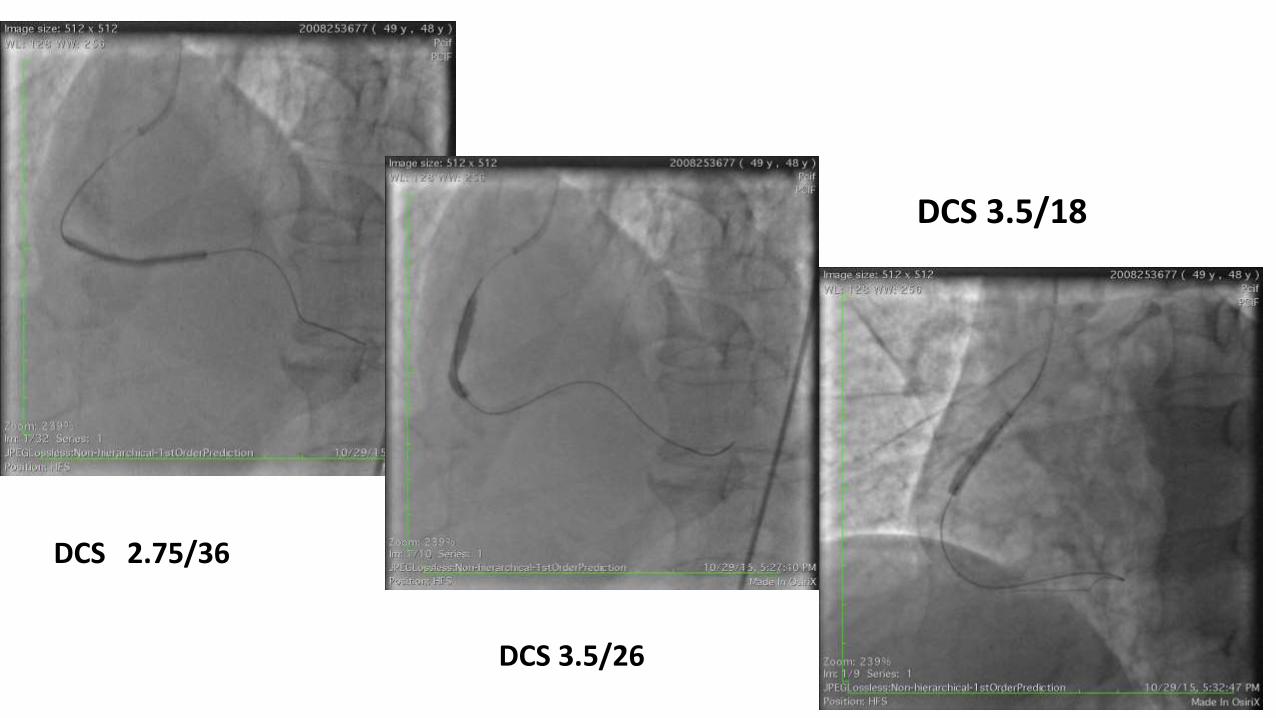
DCS 2.75/36
DCS 3.5/26
DCS 3.5/18
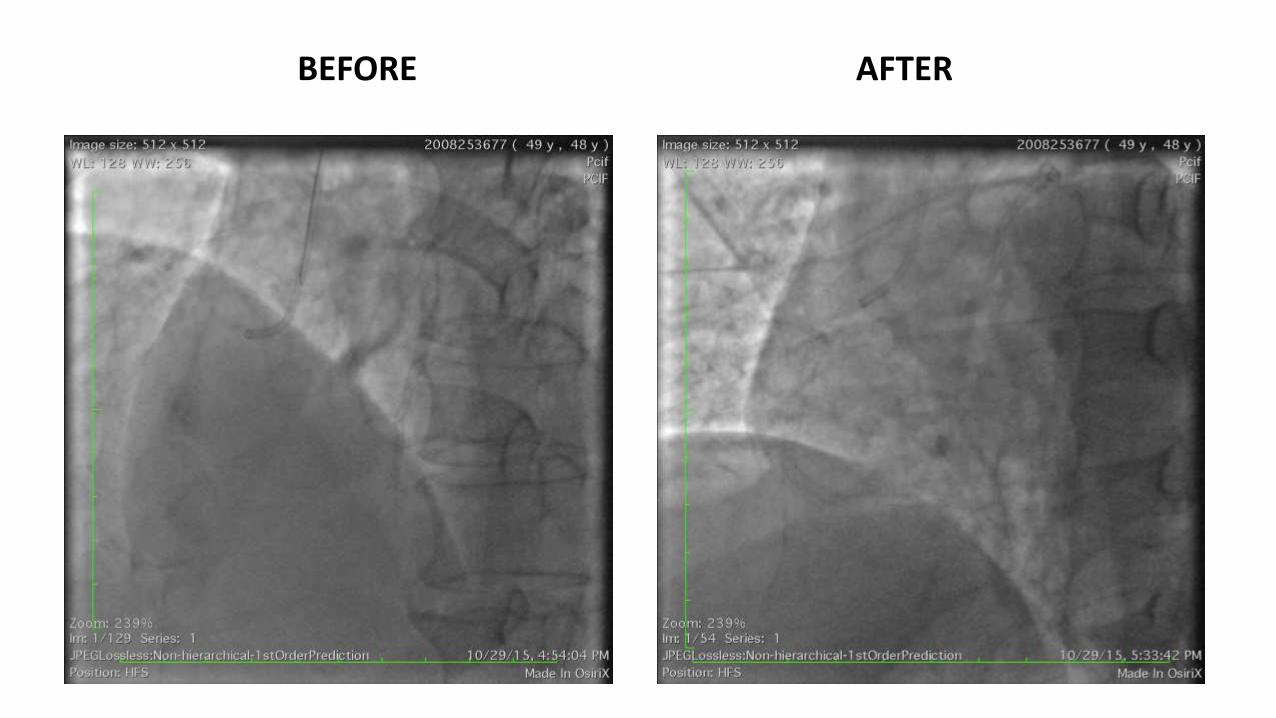
BEFORE AFTER
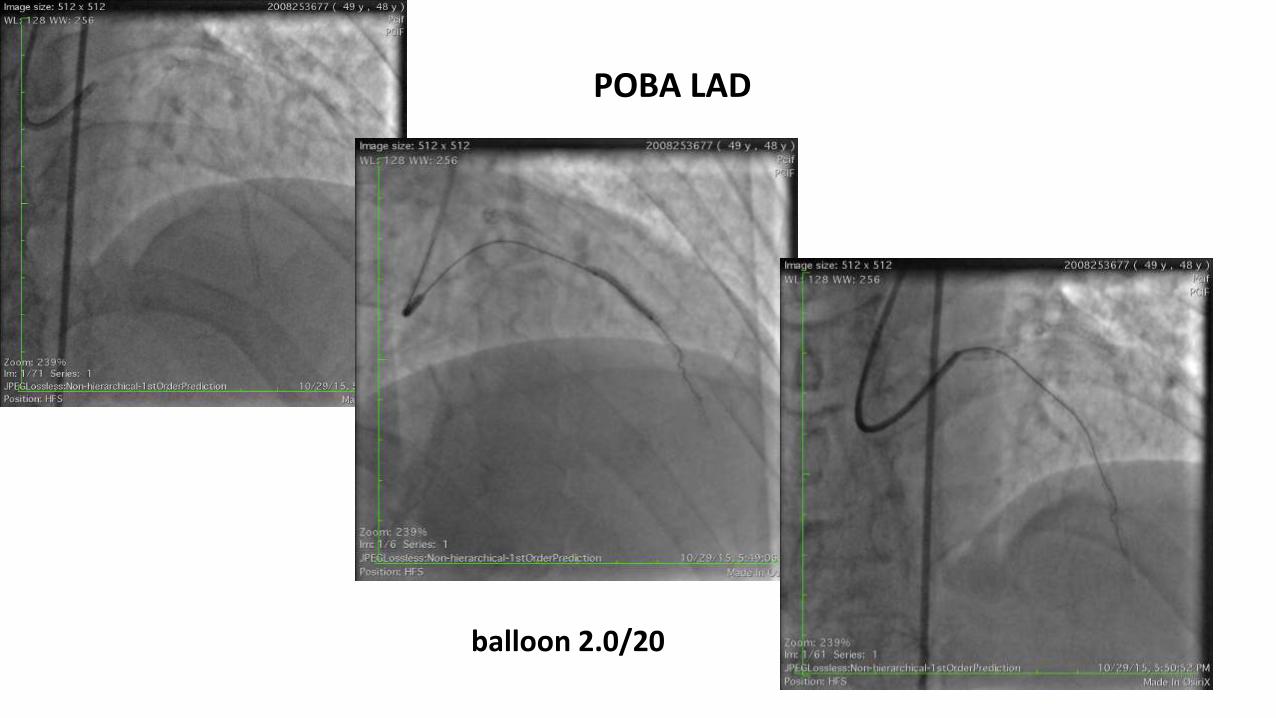
balloon 2.0/20
POBA LAD

LCx PCI : DCS 2.75/36
After PCI
• Refractory angina and heart failure was relieved
• He required 1 mo duration of DAPT : Ticagrelor 2 x 90 mg and Aspilet 1 x 80 mg
• Underwent successful major surgery ORIF without any complication
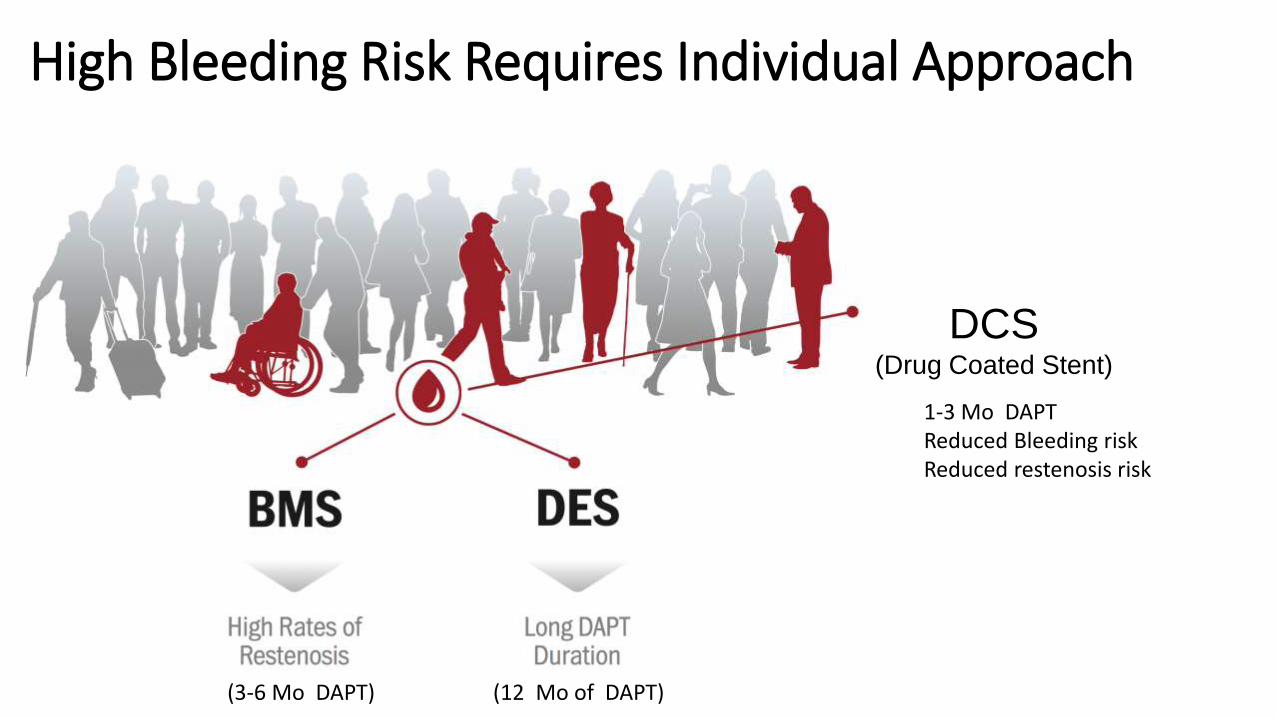
High Bleeding Risk Requires Individual Approach
DCS(Drug Coated Stent)
(3-6 Mo DAPT) (12 Mo of DAPT)
1-3 Mo DAPTReduced Bleeding riskReduced restenosis risk


































