Embed Size (px)
Citation preview

Imaging in ENT
Muhammad Bin Zulfiqar PGR II SIMS/SHL New Radiology Department

BASIC ANATOMY• EAR
1) External2) Middle3) Inner
• NOSE AND PARANASAL SINUSES
• THROAT1) Oral cavity and mouth2) Pharynx• Nasopharynx• Oropharynx• Pharynx
3) Larynx

Imaging modalities
• Plain Radiography(main)• Computerized tomography(main)• Magnetic resonance Imaging• Ultrasound• Barium swallow

Anatomy of EAR
• External• Middle• Inner


Tympanic Membrane
Separates external ear from middle ear.

Middle Ear

Middle Ear
Stapes

Middle Ear

Middle Ear

Internal Ear

Internal Ear
Semicircular Canals

Internal Ear
Cochlea

Internal Ear
Facial nerve canal
The incus is seen connecting to the stapes

Internal EarGeniculate ganglion
The incus is seen connecting to the stapes

Nose and Para nasal Sinuses
• Nasal Bones• Nasal Soft Tissue• Nasopharynx

Nasal Anatomy

NASAL ANATOMY

Nasopharynx


Para Nasal Sinuses•Frontal sinuses
•Maxillary sinuses
•Sphenoid Sinuses
•Ethmoid air cells
oAnterior
oMiddle
oposterior

Para Nasal Sinuses

A. Frontal SinusB. Sphenoid SinusC. NostrilD. Posterior Nasopharyngeal wallE. Posterior esophageal wallF. Nasal turbinate
Para Nasal Sinuses

Osteomeatal Complex

Throat
1) Oral cavity and mouth2) Pharynx• Nasopharynx• Pharynx• Oropharynx
3) Larynx

• Nasopharynx• Oropharynx• Pharynx• Larynx

Nasopharynx

Nasopharynx

Nasopharynx

Oropharynx

Pharynx

Pharynx

Oropharynx

Larynx

Larynx

Larynx

Larynx

Larynx

Larynx

Diseases of Ear
• Chronic Suppurative Otitis Media• Cholesteatoma• Otosclerosis
– CHOCHLEAR IMPLANT

Chronic Suppurative Otitis Media
• Poorly pneumatized mastoid air cells.• Ear drum is thickened.• Soft tissue seen around ossicles without
erosion.• Calcification of ear drum, tendon of stapedius.• Almost complete opacification of middle ear
cavity.

Chronic Suppurative Otitis Media
Stapes calcification
Eardrum calcification
Eardrum calcification
Normal
Loss of pneumatization

Chronic Suppurative Otitis Media
Opacification of tympanic cavity

Cholesteatoma
• Present as soft tissue mass with associated erosions.
• Auditory ossicles, especially the long process and lenticular processes of the incus as well as the head of the stapes
• Wall of the lateral semicircular canal • Lateral epitympanic wall (the scutum)

Cholesteatoma
Cholesteatoma: 20-year old woman with recurrent Otitis. Granulations on left ear drum. Soft tissue mass between ossicular chain and lateral tympanic wall, which is eroded. Right side for comparison.
Granulations on left ear drum. Soft tissue mass between ossicular chain and lateral tympanic wall, which is eroded. Right side for comparison.

Cholesteatoma
Cholesteatoma with erosion of the wall of the lateral semicircular canal
There is a soft tissue mass with erosion of the long process of the incus.
Automastoidectomy due to a large cholesteatoma

Cholesteatoma
The examination shows a mass with mixed intensity on sagittal T1 and high intensity on transverse T2 weighted images. It has a high intensity on diffusion weighted images, which indicates restricted diffusion. (arrows)

Otosclerosis
• Otosclerosis is a genetically mediated metabolic bone disease of unknown etiology.
• conductive hearing loss and is considered to be the hallmark of the disease.
• The process starts in the region of the oval window, classically at the fistula ante fenestram, i.e. in front of the oval window (fenestral otosclerosis).
• It can also occur around the cochlea (retrofenestral otosclerosis).

Otosclerosis
There is a lucency anterior to the oval window (arrow) and between the cochlea and the internal auditory canal. This is combined fenestral and retrofenestral otosclerosis.
Otosclerosis anteriorly to the oval window (arrow)

Otosclerosis
Bilateral otosclerosis

Cochlear Implant
• Cochlear implantation is performed in patients with sensorineural deafness due to degeneration of the organ of Corti.
• The electrode is inserted into the scala tympani of the cochlea via the round window or via a drill hole directly into the basal turn.
• Post-operatively its position can be evaluated with plain films or with CT.

Cochlear Implant
Status after cochlear implantation

Nose And Para Nasal Sinuses
• Deviated Nasal Septum• Nasal Bone Fracture• Enlarged Adenoids• Sino nasal Polyposis• Angiofibroma

Deviated Nasal Septum
• Nasal septum deviation is a common physical disorder of nose involving a displacement of nasal septum.
• Trauma is a frequent cause.• Can be congenital.• Poor drainage of sinuses.

Deviated Nasal Septum
Waters view (close-up view of the patient in the previous image) shows a deviated nasal septum, quadrangular cartilage displaced from the maxillary crest, and a nasal root deviated to the right

Fracture of Nasal bone

Fracture of Nasal bone

Enlarged Adenoids
• The adenoids are sections of soft tissue found at the back of the nasal cavities where they meet the pharynx.
• Like tonsils, adenoids help to stop harmful bacteria and airborne pathogens from entering the airways and causing infections.
• Multiple sinus infections, snoring and worsened breathing esp. in children.

Enlarged Adenoids

Sinonasal Polyposis• Polyps are soft tissue pedunculated masses of edematous
hyper plastic mucosa lining the upper respiratory tract…..nasal cavity and sinuses.
• These are benign mucosal lesions.• Commonest sites in order of frequency are;
1. Ethmoids2. Maxillary antra3. sphenoids

Causes of Sinonasal Polyposis
1. Allergic rhinitis2. Asthma3. Cystic fibrosis(child)4. Kartagener syndrome5. Nickel exposure6. Nonneoplastic hyperplastic hyperplasia of
inflammed mucous membranes.

Sinonasal Polyposis

Juvenile Nasopharyngeal Angiofibroma
• Benign highly vascular tumor• Locally invasive, submucosal spread• Vascular supply most commonly from internal maxillary
artery– Also: internal carotid, external carotid, common
carotid, ascending pharyngeal• Occurring almost exclusively in males• Peak age of onset = 13-15 years old• Intracranial Extension between 10-20%• Recurrence Rates as high as 50%

Juvenile Nasopharyngeal Angiofibroma
Origen considered to be posterlateral nasal wall at sphenopalatine foramen.
Medial growthNasal cavityNasopharynx
Lateral growthPterygopalatine fossa
Vertical expansion through inferior orbital fissure to orbit possible
Infratemporal fossa Superior expansion through pterygoid process may involve middle cranial fossa
Lateral and posterior walls of sphenoid sinus can be eroded Cavernous sinus may be involved Pituitary may involve.

Coronal CT: Bone Window
• Widening of left sphenopalatine foramen
• Lesion fills left choanae
• Extends into sphenoid sinus

Axial CT: Soft Tissue Window with Contrast
• Homogenous enhancement
• Widening of left sphenopalatine foramen
• Extension into– Nasopharynx– Pterygopalatine fossa

Axial CT: Soft Tissue Window with Contrast
• Homogenous enhancement
• Widening of right sphenopalatine foramen
• Extension into– Nasopharynx– Pterygopalatine fossa

Axial MRI: T1
• Heterogeneous intermediate signal
• Flow voids represent enlarged vessels
• Extension into– Nasopharynx– Masticator space

Coronal MRI: T1 with Contrast• Diffuse intense
enhancement
• Multiple flow voids within hypervascular mass
• Extension into– Nasopharynx– Pterygopalatine fossa

Axial MRI: T2• Heterogeneous
intermediate to high signal enhancement
• Multiple flow voids within hypervascular mass
• Extension into– Nasopharynx– Pterygopalatine fossa

THROAT Diseases
• Enlarged adenoids• Pharyngitis• CROUP(Laryngotracheobronchitis)

Pharyngitis and Tonsillitis
• Bacterial• Viral • Fungal

Croup (acute laryngotracheobronchitis)
• Croup, also called acute laryngotracheobronchitis is caused by viral infection of the upper airway usually parainfluenza virus or respiratory syncytial virus (RSV).
• It is common and has a peak incidence before the age of 1 year (typically between 3 and 6 months of age).
• It is presented Clinically by protracted barking cough and inspiratory strider due to tracheal narrowing that is caused by mucosal edema .

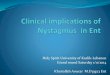
Croup (acute laryngotracheobronchitis)
steeple signdistension of the hypopharynx due to the patient's attempt at decreasing airway resistance

Croup (acute laryngotracheobronchitis)
Steeple Sign

QUESTIONS ?

THANK YOU