Embed Size (px)
Citation preview

HYDATID DISEASE
OF LIVER
Akriti Sah7th Semester
North DMC Medical College & Hindu Rao Hospital
Malka Ganj, Delhi 110007
Dated: 01/09/17

Among many liver infections, is
Hydatid disease which will be our
topic of discussion today.
Akriti Sah

WHY DO WE NEED TO DISCUSS IT?
BURDEN
Globally distributed and found in every
continent except Antarctica. Very common
in countries around the Mediterranean
Sea.
More than 1 million people are affected at
any one time. (WHO)
AND IN INDIA
High incidence reported from Tamil Nadu,
Andhra Pradesh. Akriti Sah
Let me draw your
attention to the term:
ECHINOCOCCOSIS
Akriti Sah
1.Human echinococcosis is a zoonotic disease that is
caused by parasites, namely tapeworms of the genus
Echinococcus.
2.Echinococcosis occurs in 4 forms:
3.The two most important forms, which are of medical and
public health relevance in humans are
4.Cystic echinococcosis (CE): also known as hydatid
disease or hydatidosis, caused by infection with the larval
stage of Echinococcus granulosus.
(most frequently observed form.)
5.Alveolar echinococcosis (AE): caused by infection with the
larval stage of E. multilocularis. (rare)
ETIOLOGY
Akriti Sah

`
Common name of E. Granulosus:
Dog Tapeworm or Hydatid worm
Akriti Sah

Echinococcus granulosus adult, stained
with carmine. Close-up of the scolex of
E. granulosus.
Akriti Sah
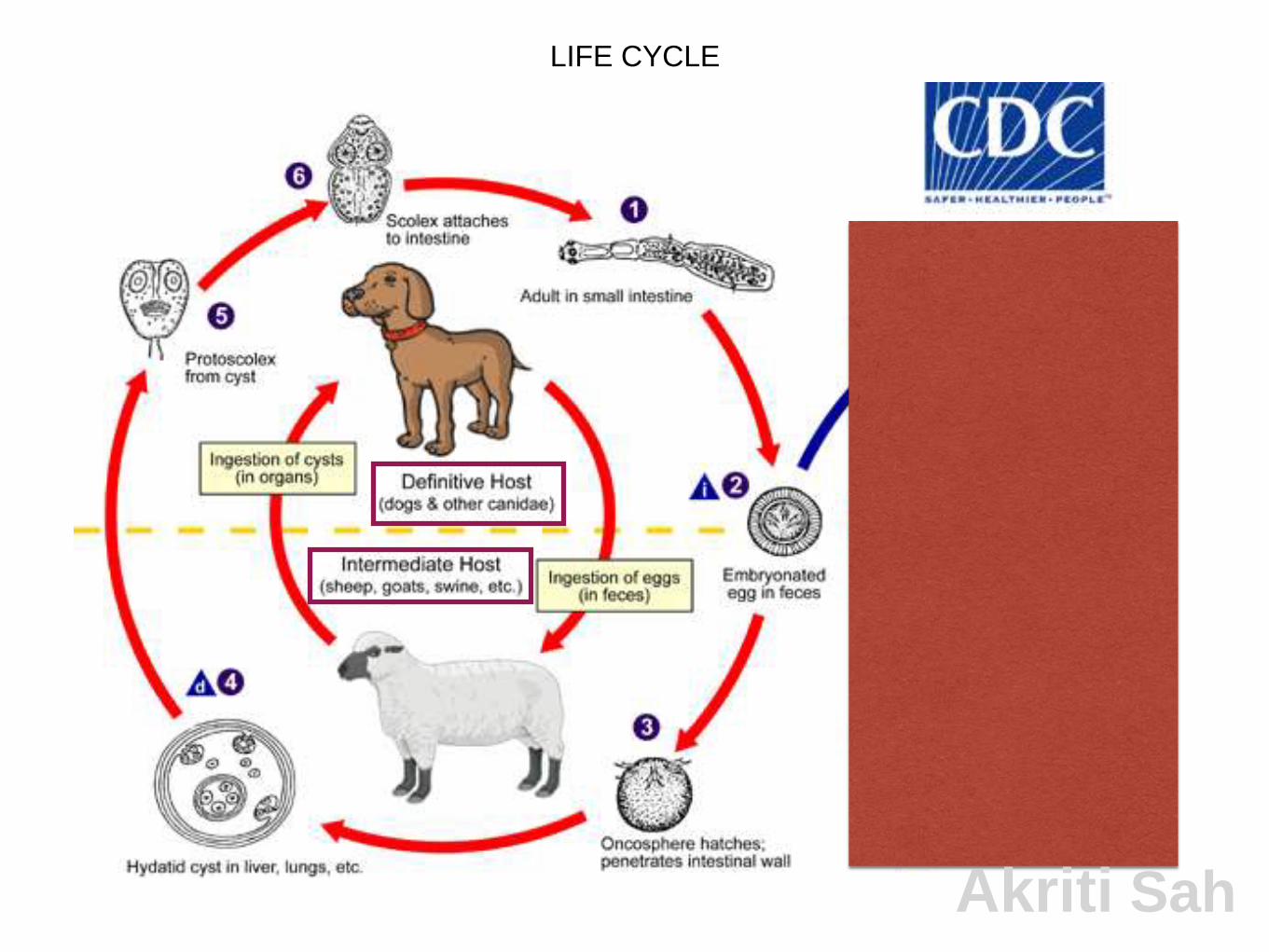
LIFE CYCLE
Akriti Sah

MODE OF INFECTION:
2. The most common mode of transmission to humans is
by the accidental consumption of soil, water, or food
that has been contaminated by the fecal matter of an
infected dog or by direct contact with an infected dog
(handling/ playing with infected dogs.)
3. Humans act as so-called accidental intermediate
hosts in the sense that they acquire infection in the
same way as other intermediate hosts, but are not
involved in transmitting the infection to the
definitive host.
Akriti Sah

PATHOGENESIS
1. The ingested eggs release oncospheres that are able to
penetrate the human intestinal wall.
2. These oncospheres enter the radicles of portal vein and
are carried to the liver. The liver acts as the first filter where
60-70% of human infections are located.
3. Some embryos may pass through the hepatic capillaries
and enter the pulmonary circulation. Lungs act as the
second filter.
4. A few of these embryos may pass pulmonary circulation
and enter general circulation and may lodge in various
organs
Akriti Sah
1. Wherever the embryos settle, an active cellular reaction consisting of
monocytes, giant cells and eosinophils takes place around the parasite.
2. A large no of parasites are thus destroyed by this host defence
mechanism.
3. Some however escape and develop into cysts. The cellular reaction in
the cases gradually disappears, followed by the appearance of fibroblasts
and the formation of new blood vessels.
4. Fibroblasts lay fibrous tissue, which envelops the growing embryo. This
is known as pericyst.
5. This pericyst merges with the surrounding normal tissue to provide
nutrition to the growing parasite.
6. In old cysts the pericyst may become sclerosed or calcified and parasite
within it may die.
Development of hydatid cyst in the organ
Akriti Sah
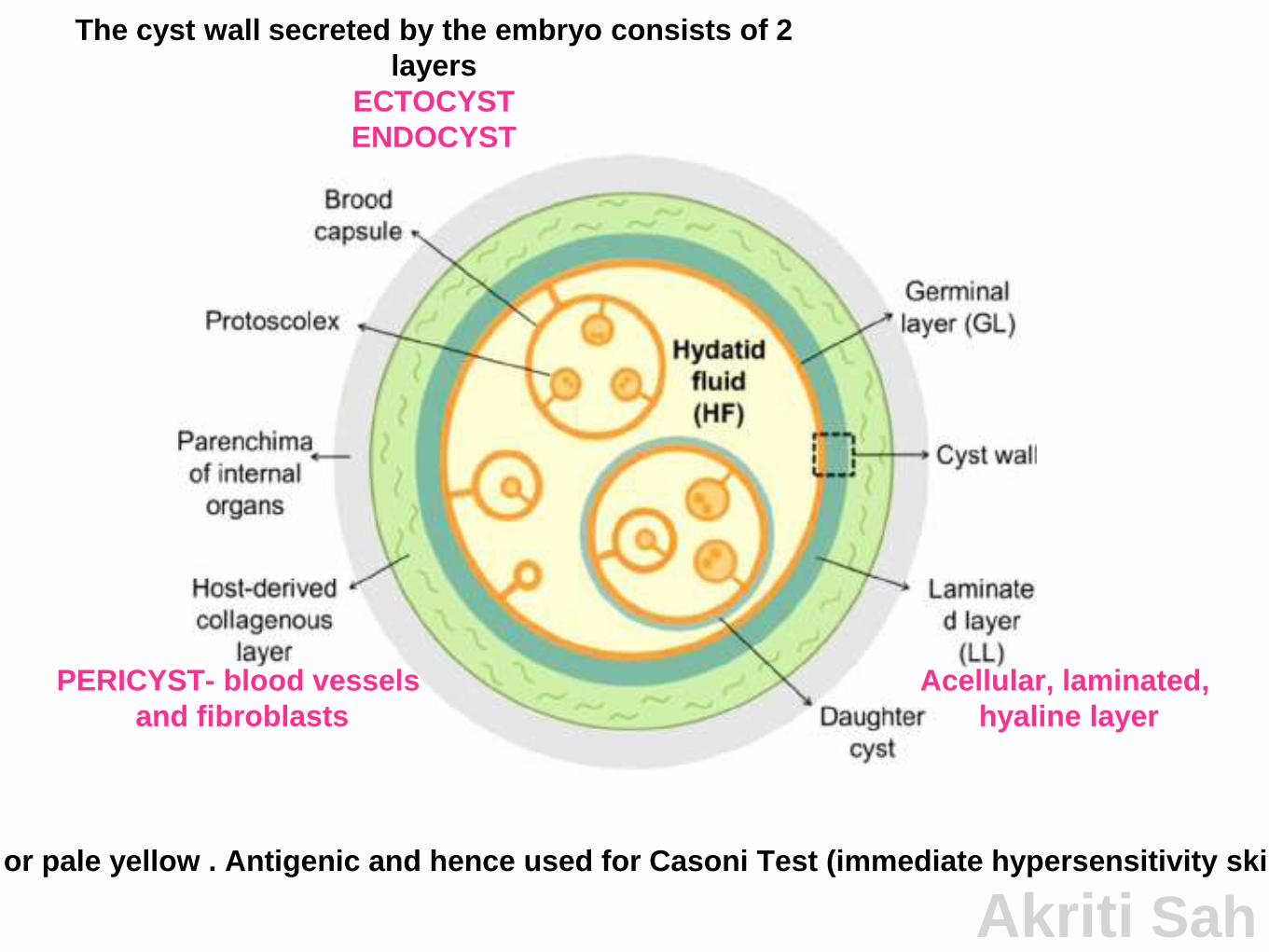
The cyst wall secreted by the embryo consists of 2
layers
ECTOCYST
ENDOCYST
PERICYST- blood vessels
and fibroblasts
clear colorless or pale yellow . Antigenic and hence used for Casoni Test (immediate hypersensitivity skin test, many false p
Acellular, laminated,
hyaline layer
Akriti Sah
1. Cysts most often occur in the liver (70%) or
lungs (20%). However, 10% of cysts can be
found anywhere in the body, including the spleen
(6%), heart (2%), kidney (2%), and brain (< 2%).
2. Cysts are usually unilocular, and can range
anywhere from 1 cm to 15 cm in diameter. They
also tend to affect the right lobe more frequently
than the left lobe due to the nature of portal
blood flow.
Akriti Sah
SYMPTOMS
1. It can go undetected for many years due to
i. the slow growth and development of cysts and
ii.the response of the host’s immune system.
2. Depending on the size and location, cysts can eventually exert pressure
on nearby structures, producing discomfort, pain, nausea and vomiting.
3. Cysts in the liver can compress bile ducts, causing obstruction that can
manifest as obstructive jaundice,
abdominal pain,
anorexia, and
pruritus.
4.When in the lungs, cysts can irritate the membranes leading to chronic
cough, dyspnea, pleuritic chest pain, and hemoptysis.
Akriti Sah
COMPLICATIONS
1.Liver cysts can also rupture
• through the diaphragm producing an empyema,
• into the biliary tract producing obstructive jaundice, or
• into the stomach.
2.Cyst rupture or leakage can cause immunologic symptoms from the
initiation of an immunoglobulin (Ig)E response, leading to allergic reactions
most frequently characterized by hives, flushing, and mucous membrane
swelling.
3.A major rupture can cause a life-threatening anaphylactic reaction.
4.Ruptured cysts can release viable cystic contents and protoscolices into
the peritoneum, resulting in secondary hydatidosis (implanting and growing
within the peritoneal cavity).
Akriti Sah

Akriti Sah

DIAGNOSIS
Akriti Sah
CLINICAL
1. Signs and symptoms may include
hepatic enlargement with or without a palpable mass in the
right upper quadrant,
right epigastric pain,
nausea, and
vomiting.
2. On per abdominal examination,
3. When the cyst involves the lower margin of the liver
i. A palpable spherical and smooth swelling may be felt in
the right hypochondrium
ii. Hydatid thrill positive (rarely demonstrated)
4. When the cyst involves the superior margin,
5. Upper limit of liver dullness is found to be raisedAkriti Sah
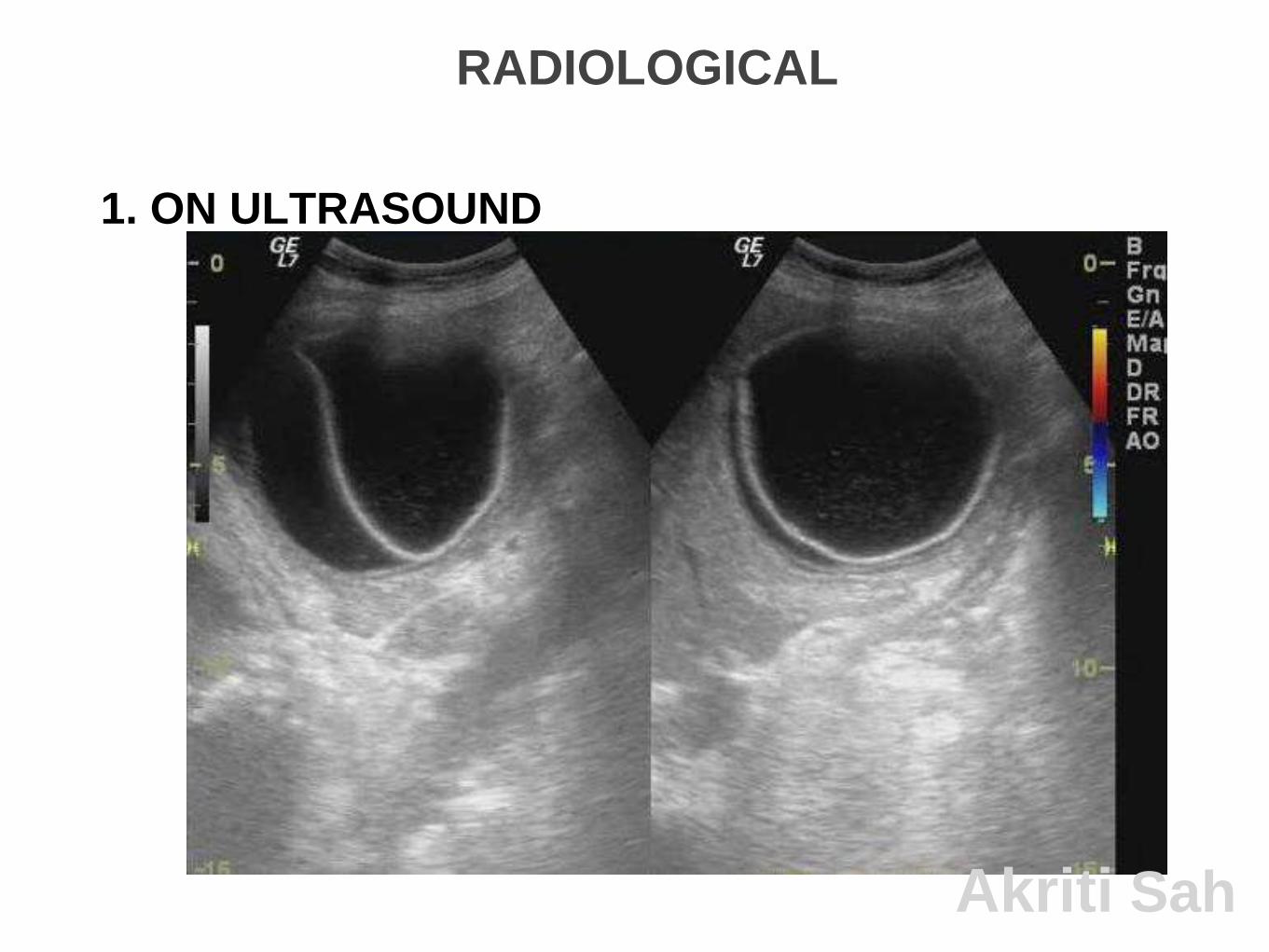
RADIOLOGICAL
1. ON ULTRASOUND
Akriti Sah
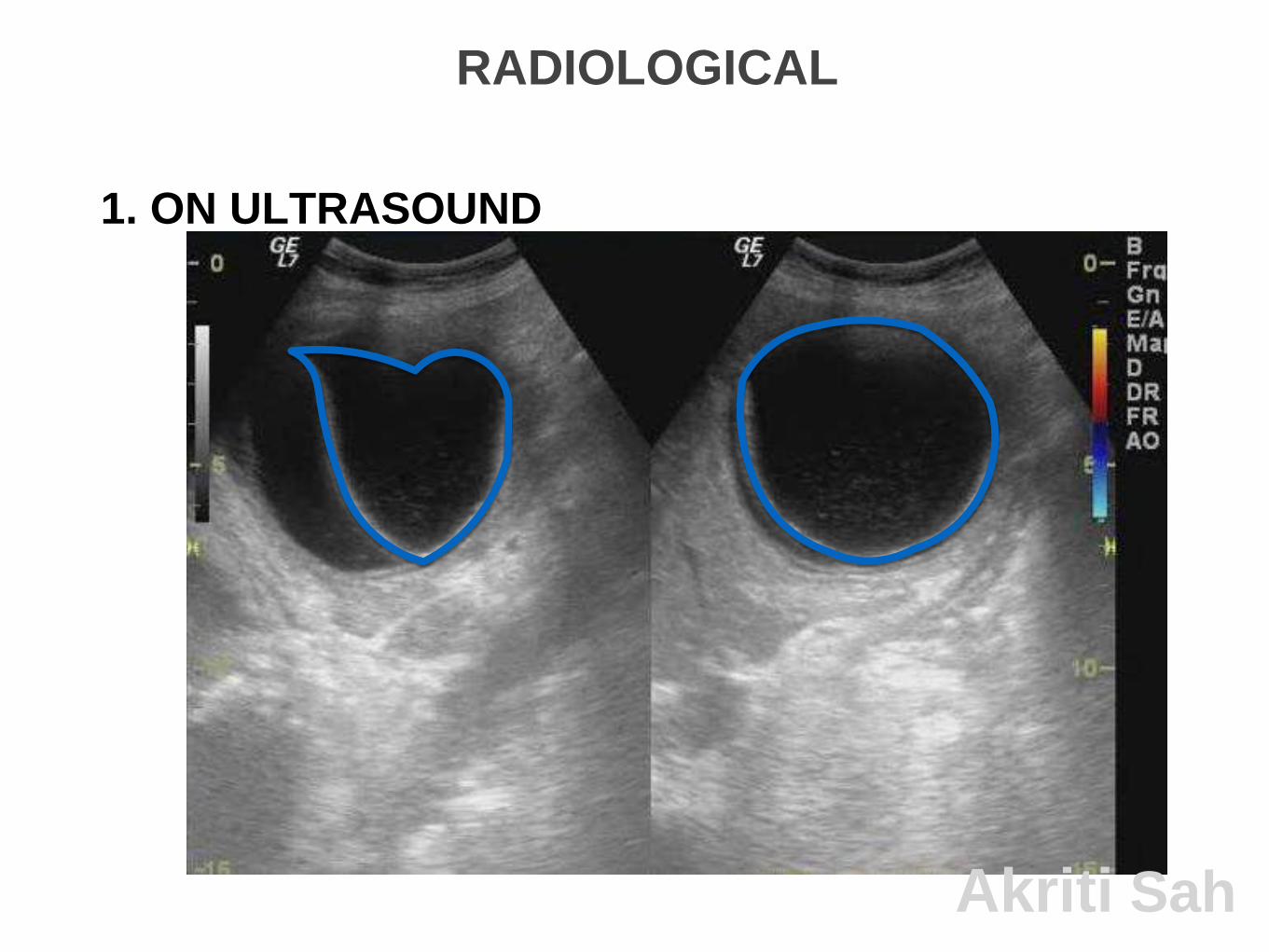
RADIOLOGICAL
1. ON ULTRASOUND
Akriti Sah

Akriti Sah

Akriti Sah

Akriti Sah

Akriti Sah

1. Shows a well-defined cystic lesion.
2. The cyst wall usually has a hypoechoic layer, flanked by an
echogenic line on either side.
3. At times the endocyst can also detach from the pericyst. This
detachment may appear as a localized split in the wall and “floating
membranes” within the cystic cavity;
4. Complete detachment the endocyst observed by ultrasonography is
referred to as the water lily sign.
5. Multivesicular cysts may also be seen which are fluid collections
that often appear in a honeycomb pattern with multiple septa. These
septa represent the walls of the daughter cysts, which appear as
cysts within a cyst.
6. Multiple punctate echogenic foci are often present within the cyst,
appearing grain-like. These foci represent hydatid sand, a
combination of fluid and protoscolices. Akriti Sah

The findings on imaging vary
depending on the stage of the cyst.
A classification system originally developed
by Gharbi and colleagues in 1981, was revised
by the WHO-Informal Working Group
Classification on Echinococcus (IWGE).
Akriti Sah

Akriti Sah
Ultrasound has become a widely used modality for
CE detection.
This is currently the screening method of choice,
due in part to
• accessibility even in small, rural medical centers,
• cost containments, and
• portability of the device.
Ultrasound is not only helpful for diagnosis, but in
post-treatment monitoring.
Akriti Sah

2. ON CT
Akriti Sah

1.CT plays a crucial role during the peri-
operative period for detection of complications,
such as
•biliary and vascular involvement,
•cyst ruptures, and
•underlying infection.
2.In addition, CT can reveal many of the same
findings that can be seen by ultrasonography.
Akriti Sah

SEROLOGY1.Infection with Echinococcus induces an antibody
response, most commonly IgG (predominantly IgG1 and
IgG4), followed by IgM, IgA, and IgE.
2.A number of detection assays for IgG, IgM, and IgE
antibodies to hydatid antigens are in use.
3.Serologic tests, such as enzyme-linked immunosorbent
assay (ELISA) and indirect hemagglutination test, are
highly sensitive methods for detecting infection.
4.Specific confirmation can be obtained by demonstrating
echinococcal antigens by immunodiffusion (arc 5)
procedures or immunoblot assays (8-, 21 –kD bands).
Akriti Sah

1.Although antibody detection assays tend to have higher
sensitivities (up to 97%) when compared to antigen assays,
they do not distinguish between active and past infections.
Therefore, assays for antigens are preferred, as they are not
only more specific, but levels have been shown to reflect
improvement in surgically treated patients
2.A disadvantage of these assays is the variability in sensitivity
rates, which range from 33% to 85%. This variability may be
due to the structure of calcified cysts, concealment of cysts
by surrounding normal tissue, or the fact that antigen–
antibody complexes are not easily detected by assays.
3.However, in approximately 30–40% of patients, no
antibodies of any kind are detectable, even in individuals who
have circulating parasitic antigens. These data suggest that
the infection may be associated with an inhibition of the host
immune response. Akriti Sah

In conclusion,
1.Ultrasonography imaging is the technique of
choice for the diagnosis .This technique is
usually complemented or validated by
computed tomography (CT) and/or magnetic
resonance imaging (MRI) scans.
2.After a cyst has been detected, serologic
tests may be used to confirm the diagnosis.
Akriti Sah

REFERENCES
1.Bailey & Love's Short Practice of Surgery,
26E
2.Park’s preventive and social medicine,26E
3.Medical Parasitology by Arora, 4E
4.www.who.int/
5.www.cdc.gov/
6.www.ncbi.nlm.nih.gov/
Akriti Sah
WHAT’S NEW?
Vaccination of lambs is currently being evaluated as an additional intervention.
WHO is working towards the validation of effective cystic echinococcosis control
strategies by 2020.
Akriti Sah