MANAGEMENT OF PENETRATING LIVER TRAUMA Andrew Lee PGY4 SUNY Downstate Grand Rounds Thursday February 16, 2017
www.downstatesurgery.org
CASE PRESENTATION
17 year old male GSW to right paraspinal back below scapula, GSW left forearm through and through, GSW left hip below ASIS, bullet palpated,
Primary survey - tachycardic to 120s, peritoneal abdomen
Secondary survey - no hard signs of vascular injury, distal radial pulse, motor and sensation intact
www.downstatesurgery.org
Presenter
Presentation Notes
17 year old male with multiple GSW. It appeared he was shot twice one through and through the left forearm with a corresponding wound in the left hip where the bullet could be palpated and right back beneath the scapula with bullet lodged in right upper abdomen. His primary survey was significant for peritoneal abdomen and hemodynamically unstable with HR in the 120s. On secondary survey palpable left radial pulse, and motor sensation in tact in left hand.
www.downstatesurgery.org
Presenter
Presentation Notes
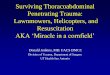
What do you see on chest X-ray? no pneumothorax, no hemothorax - small hemothorax, and bullet in RUQ
www.downstatesurgery.org
Presenter
Presentation Notes
We got X-rays to determine trajectory of bullet
INTRA-OP
Rushed to OR as level 1 for crash laparotomy
Evacuated 1L dark blood clots
Hole in right diaphragm, repaired primarily
Placed right chest tube
Grade 4 liver injury, posterior right lobe blast injury
www.downstatesurgery.org
Presenter
Presentation Notes
He was taken emergently as a level 1 for crash laparotomy Upon entry into abdomen 1000cc of dark blood clots were evacuated with more exanguinating. We temporarily packed all quadrants while anesthesia resuscitated. Billowing of the right diaphragm showed a hole in the diaphragm and was repaired primarily along with chest tube placement. We noted the majority of bleeding coming from a right grade 4 posterolateral lobe blast injury
INTRA-OP CONTINUED
Eviscerated and ran the bowel
Mobilized and divided the falciform ligament
Packed liver with lap pads and Nu-Knit over injured area
Temporary abdominal closure
Received: 6 RBC 6 FFP 2 Platelets
www.downstatesurgery.org
Presenter
Presentation Notes
Small bowel was eviscerated and run not revealing any injuries Falciform was divided up to diaphragm Temporary lap pads placed at injured site along with Nu-knit temporary abdominal closure placed in all received 6 PRBC 6 FFP 2 platelets
POST-OP COURSE
Transferred to SICU
Hypertensive - systolic 150s
Intermittently tachycardic to 130-140s
Transiently responded to 2 PRBC and 2 FFP
Continued output from Barker vac approaching 100-200cc/hr
Concern for ongoing hepatic bleeding
www.downstatesurgery.org
Presenter
Presentation Notes
Postoperatively transferred to SICU He was hypertensive and intermittently tachycardic to 130-140s and transiently responded to 2 more units RBC, and FFP. Output from the Barker vac was 100-200cc/hr. Concern for ongoing hepatic bleed. What do you do next? PGY 2 resident
www.downstatesurgery.org
Presenter
Presentation Notes
Angiogram performed which showed multiple contrast blushes scattered in the right hepatic lobe. Performed angioembolization with gel foam and resolution of extravasation
ANGIOGRAM
Contrast blush in segment 7 or 8 represents extravasation
Other small focal collections of contrast seen scattered through right lobe
Angioembolization performed of right hepatic artery with gel-foam
www.downstatesurgery.org
HOSPITAL COURSE
Planned take back POD3, removal of hepatic packs, Blake drain and JP drain placed, abdomen closed
POD4 patient extubated, chest tube d/c’ed
Blake drain approximately 100-200cc/24hr bilious fluid
POD 9 JP less than 20cc/24hr serosanguinous JP d/c’ed
POD14 CT scan showed a small necrotic patch of liver. HIDA scan showed active extravasation of bile
www.downstatesurgery.org
Presenter
Presentation Notes
The rest of his hospital course, he was taken back on POD3 for removal of hepatic packs, Blake drain placed on raw surface of posterior liver bed and JP drain placed in Morrison’s pouch, abdomen closed POD4 patient was extubated and chest tube d/c’ed Blake drain was approximately 100-200cc/24hour bilious fluid POD 9 JP drain in Morrison’s pouch was d/c’ed POD 14 continued output from drain, he received a CT a/p that showed a perihepatic collection and HIDA scan performed that showed active extravasation of bile
HOSPITAL COURSE
POD 15 underwent ERCP, unable to stent or perform sphincterotomy
POD 21 drain continued output ~100cc/24hr, afebrile, benign abdomen, wbc and liver enzymes normalized - d/c’ed home with follow up in clinic
www.downstatesurgery.org
Presenter
Presentation Notes
POD 15 underwent ERCP and unable to place stent or perform sphincterotomy with difficulty cannulating the papilla POD 21 drain continued output of 100cc/24hr, afebrile, benign abdomen, WBC and liver enzymes normalized and he was d/c’ed home
www.downstatesurgery.org
“IF TRAUMA SURGERY IS A CONTACT SPORT, THE BADLY INJURED LIVER IS THE NINJA MASTER: A VICIOUS, CUNNING AND LETHAL ADVERSARY.” -TOP KNIFE
www.downstatesurgery.org
PENETRATING LIVER TRAUMA
Liver anatomy
Grading
Background
Decision making
Management
www.downstatesurgery.org
Presenter
Presentation Notes
we will be talking about anatomy, background of liver trauma, grading of injury, clinical decision making, and intraoperative management. and hopefully come away from this able to feel more comfortable with high grade liver injury.
ANATOMY www.downstatesurgery.org
Presenter
Presentation Notes
the coronary ligaments attach the diaphragm to the parietal surface of the liver. The triangular ligaments are at the lateral extensions of the right and left coronary ligaments. The falciform ligament with the underlying ligamentum teres attaches to the anterior peritoneal cavity.
ANATOMY www.downstatesurgery.org
Presenter
Presentation Notes
This is a blowout view of the liver segments. Cantlie’s line divides the liver into right and left hepatic lobes which is an imaginary line from the ivc to the gallbladder fossa. The Couinaud segments are divided based on the hepatic veins. The right hepatic vein runs between right posterolateral 6, 7 and anteromedial 5 and 8. On the left, the left hepatic vein delineates the anterior 3 and 4 and posterior segment 2. Middle hepatic vein derived from segments 4 and 5. In 90% the middle hepatic vein joins the left hepatic vein before joining IVC. Retrohepatic IVC receives the blood of the hepatic veins. The portal vein is formed from the confluence of the splenic and SMV behind the pancreatic head. We see it posterior to the bile duct and proper hepatic artery within the porta hepatis. The portal vein provides about 75% of the blood flow and 50% of the oxygen to the liver. CHA branches from the celiac artery. Then branches into GDA, right gastric and proper hepatic. What is important to remember is anatomic variances, and most frequently 11% there is an aberrant right hepatic artery originating from the SMA that goes behind the duodenum. Also left hepatic artery from the left gastric artery.
GRADING www.downstatesurgery.org
HISTORICAL PERSPECTIVE Change in paradigm over last 30 years
Decline in operative liver trauma and decline in mortality
1960 Shaftan Kings County - Landmark study on penetrating abdominal trauma and unnecessary laparotomies
1986 Kings County - utility of CT scan in hemodynamically stable penetrating trauma to flank and back
1986 Demetriades et al. documented nonoperative management of liver injuries
www.downstatesurgery.org
Presenter
Presentation Notes
As I was preparing this talk, reading the early literature, Kings County was at the forefront of some landmark papers influencing how we deal with abdominal trauma. And what we saw was a paradigm shift over the last 30 years where penetrating trauma to the abdomen mandated exploration it has now become accepted practice for isolated liver trauma to undergo nonoperative management. So how did we get there? We saw a decline in operative liver trauma as well as a decline in mortality - this is likely multifactorial, with less penetrating trauma, and less severe injury. 1960 Shaftan from Kings county first documented complications stemming from unnecessary laparotomies. He concluded the application surgical judgment rather than dogma is the more rational and intelligent approach to the management of abdominal injury. In 1986 County first documented the utility and safety of scanning patients with penetrating trauma to flank and back allowing better diagnostic, and clinical decision making In 1986 Demetriades documented the efficacy and safety of nonoperative management of liver injuries. Now the mainstay of treatment in the hemodynamically stable liver trauma patient is nonoperative management.
BACKGROUND
Incidence of penetrating trauma decreasing from 75% in 2000 to 20% in 2010
The liver is most frequently injured intraabdominal organ
Now only 13.7% of liver injuries are managed operatively
Zago TM, Pereira BM, Nascimento B, Alves MSC, Rodrigues T, Calderan A, et al. Hepatic trauma: a 21-year experience. Rev Col Bras Cir. 2013;40(4):318–22.
www.downstatesurgery.org
Presenter
Presentation Notes
As we said before the incidence of penetrating trauma decreasing overall from 75% in 2001 to 20% in 2010 for admissions. And while the liver is the most frequently injured intraabdominal organ only 13.7% of liver injuries are managed operatively
THE SITUATION
Non op vs. operative management
Low numbers of operative management and less high grade injuries
High grade liver injury - how do you manage?
www.downstatesurgery.org
Presenter
Presentation Notes
So you have non op vs operative management however there are low numbers of operative management. So the situation is with the low numbers of operative management and high grade injuries, you have a high grade liver injury - how do you manage it?
Literature review from 1960 to 2007
Recommendations
Hemodynamically unstable or peritonitis should be taken for laparotomy (level 1)
Hemodynamically stable with unreliable clinical exam warrants further investigation or laparotomy (level 1)
Laparotomy not indicated in stable patients with stab wounds without signs of peritonitis (level 2)
Laparotomy not indicated in stable patients with GSW if wounds are tangential and without signs of peritonitis (level 2)
Patients selected for NOM, abdominopelvic CT should be strongly considered as a diagnostic tool (level 2)
Patients with penetrating injury isolated to RUQ may be managed without laparotomy in presence of stable vital signs, reliable exam, and minimal to no abdominal tenderness (level3)
www.downstatesurgery.org
Presenter
Presentation Notes
Recent literature review article published in 2010 and the basis for EAST guidelines broke it down simply for management of penetrating abdominal trauma. There is pretty much no argument for a patient who is hemodynamically unstable or with peritonitis to be taken to the operating room. Patient that has an unreliable clinical exam (i.e. traumatic brain injury, seizure, ect.) warrants investigation or laparotomy Level 2 evidence for no laparotomy in stable patients with stab wounds without signs of peritonitis Level 2 evidence for no laparotomy in stable patients with GSW if wounds are tangential and without signs of peritonitis Patients that are selected for nonoperative management CT scan should be performed Level 3 evidence with penetrating trauma to RUQ may be managed without laparotomy in presence of stable vital signs, reliable exam, and minimal to no tenderness
You’ve made the decision to operate on a patient with a liver injury
Staring at a high grade IV injury to right hepatic lobe after a gun shot wound… How do you proceed?
www.downstatesurgery.org
Presenter
Presentation Notes
So you’ve made the rare decision to operate on a patient with a liver injury. While management has shifted, there haven't been many major advances in surgical technique. You’re staring at a high grade 4 injury to right hepatic lobe after a gun shot wound…. how would you proceed?
Lesser omentum is opened, enter the foramen of Winslow and the hepatoduodenal ligament encircled
www.downstatesurgery.org
Presenter
Presentation Notes
Obtain temporary control of bleeding. We can do this by manual compression, temporary packing, Pringle Maneuver. How do you perform a pringle maneuver? PGY 2 resident By opening the lesser omentum, enter the foramen of Winslow and then encircle the hepatoduodenal ligament. Encircle with either manually, vascular clamp, or with a Rommel tourniquet which is the picture here with a vessel loop and a red rubber catheter
INTRAOP MANAGEMENT
Continued arterial bleeding despite Pringle
What is next step?
Supraceliac aortic clamping
Dark blood from posterior liver - retrohepatic venous injury
www.downstatesurgery.org
Presenter
Presentation Notes
If there is continued arterial bleeding despite Pringle maneuver What is next step? PGY 3 resident Supraceliac aortic clamping likely due to anomalous right or left hepatic artery If you see continued dark blood from posterior liver you’re likely dealing with a retrohepatic venous injury
FOR CONTROL OF INFRA HEPATIC IVC - EXTENDED KOCHER MANEUVER
MAY MOBILIZE KIDNEY FOR POSTERIOR UPPER IVC
ADRENAL VEIN
TOTAL VASCULAR CONTROL
www.downstatesurgery.org
Presenter
Presentation Notes
If you get retrohepatic IVC injury, and packing is ineffective, you may have to get total vascular control of the liver. You can perform this by first doing a Pringle. Then you do an extended Kocher where you incise the lateral attachments of the duodenum and carry out the incision caudally to the white line of Toldt. This will expose the infrahepatic IVC, renal hilum and right kidney. You can achieve more exposure if you mobilize the right kidney to gain access to posterior IVC. You may need to ligate the adrenal vein if there is no room for a clamp above the renal vein.
SUPRAHEPATIC IVC CONTROL
www.downstatesurgery.org
Presenter
Presentation Notes
For supra hepatic control it may be hard to do it intraabdominally without mobilizing the liver, so you can extend you midline into sternotomy, open the pericardium and put a vascularr clamp on the IVC just before it enters the right atrium
MOBILIZE THE INJURED LOBE Unless dealing with anterior laceration, the injured lobe must be delivered to midline
To mobile left lobe, divide the falciform, divide the left triangular ligament
To mobilize the right lobe, incise the right triangular ligament up to the anterior coronary ligament
Any suspicion for retrohepatic venous injury, don't mobilize the liver
www.downstatesurgery.org
Presenter
Presentation Notes
After you get temporary control you need to mobilize the injured lobe. So unless you’re dealing with a laceration anteriorly the injured lobe needs to be delivered to midline. In order to mobilize the left lobe, you divide the falci, and the left triangular ligament The right lobe similarly you divide the falci and incise right triangular ligament up to anterior coronary ligament. If there is any suspicion for a retrohepatic injury, do not mobilize the liver as it can release your tamponade and cause massive exsanguination
MORE EXPOSURE?
If needed for added exposure, convert midline laparotomy into Chevron, or Kocher
Thompson retractor or Omni retractor
www.downstatesurgery.org
Presenter
Presentation Notes
In case more exposure is needed you can always convert your midline laparotomy into some subcostal with the aid of thompson or Omni retractors for adequate exposure.
SMALL PROBLEM OR BIG PROBLEM?
Small problems - liver injuries may be fixed with a simple maneuver
electrocautery, liver stitch, local hemostatic agent
Big problem
Damage control mode
Focus is on rapid control of hemorrhage
Preservation of the patient’s physiology
www.downstatesurgery.org
Presenter
Presentation Notes
Once you have the problem in your face, you need to decide whether as Top knife puts it, small problem or big problem. Small problems have easy solutions with either electrocautery, argon beam, liver stitch or local hemostatic agent. With a Big problem you’re looking at damage control mode and focusing on rapid control of hemorrhage, truncating the laparotomy, and preserving the patient’s physiology and preventing from circling down the deadly triad.
OPTIONS FOR HEMOSTASIS
Liver packing
Immediate postoperative angiography
Deep liver sutures
Total vascular exclusion
Balloon tamponade
www.downstatesurgery.org
Presenter
Presentation Notes
Options for hemostasis include liver packing careful placement in Morrison’s pouch, and anterior to liver capsule creating a liver sandwich Postoperatively you can perform angiography and embolization Deep liver sutures with 0 chromic with a blunt needle tip or like this picture shows balloon tamponade with a foley balloon, or with a penrose and a red rubber catheter tied on either end and filled with saline
HEPATOTOMY WITH SELECTIVE VASCULAR LIGATION
Pringle
Extend laceration with cautery
Open parenchyma
Deaver retractors to facilitate exposure
Finger fracture leaves ductal structures
Hemoclip, suture ligate bleeders
www.downstatesurgery.org
Presenter
Presentation Notes
Another technique as part of your arsenal when you see arterial bleeding from a deep laceration is hepatotomy with selective vascular ligation. To perform this you can start out with a pringle, extended the laceration with cautery turned on high. Open the parenchyma in the direction of the injury. Use narrow Deavers into laceration to help with exposure. Using finger fractures or crushing the parenchyma disintegrates between your fingers while the ductal structures remain intact and can be ligated. You can suture ligate the bleeding vessel or apply 2 hemostatic clips.
RESECTIONAL DEBRIDEMENT
Evaluation of lobe - if destroyed and bleeding profusely - debridement
Mobilize, and encircle the injured area
Resect immediately outside the injured area, never resect within injured tissue
Don’t attempt in a patient rapidly dying on operating table
www.downstatesurgery.org
BILE DUCT INJURY
Damage control solution - external drainage
Cannulate proximal duct to abdominal wall
Drain in Morrison’s pouch
Definitive repair - simple repair and t tube or Roux-en-Y hepaticojejunostomy
www.downstatesurgery.org
ROLE OF ANGIOEMBOLIZATION
Ability to diagnose vascular lesions deep in parenchyma.
Can achieve hemostasis without need for lapaorotomy and blood loss
Generally accepted guidelines
Higher grade of hepatic injury
Part of multidisciplinary strategy when using damage control
After perihepatic packing tamponades nonsurgical bleeding, AE can be key for final hemostasis and prevent re bleeding at time of unpacking
Scalea, T. Angioembolization, Hepatic. Shock Trauma Center, University of Maryland School of Medicine, Baltimore, MD,
www.downstatesurgery.org
Presenter
Presentation Notes
Part of what has really improved mortality in high grade liver trauma is interventional radiology. After the operating room, some adjuncts for hemostasis is angioembolization. Often times during an operation you’re unable to see deep parenchymal bleeding, angiography is able to diagnose deep parenchyma vascular bleeding. It can achieve hemostasis without subjecting the patient to laparotomy and further blood loss While there is no clearcut guidelines there are generally accepted guidelines that include high grade hepatic injury, it can be used in multidisciplinary strategy when using damage control, and after perihepatic packing tamponades nonsurgical bleeding, embolization can be key for final hemostasis and prevent re bleeding when patient is unpacked.
3 year retrospective review
37 DC patients
Compared 8 DC laparotomy and angio to 11 DC laparotomy alone
All DC/angio survived while 10/11 DC alone survived to second operation
Integration of AE represents a logical extension of modern damage control technique, and can be safely performed in select patients in damage control scenario
www.downstatesurgery.org
Presenter
Presentation Notes
Finally I will end on a paper from university of Pennsylvania in a 3 year retrospective review looked at a series of 37 damage control patients. Compared 8 damage control laparotomy patients and angiography to 11 damage control laparotomy alone. They looked at death, intraabdominal processes, respiratory and kidney failure. All damage control with angio survived while 10/11 damage control alone survived to second operation. In all there were 4 deaths with one in the damage control and angio. And what they concluded was the integration of angioembolization is a logical extension of damage control technique and can be safely performed in select patients in the damage control scenario
TAKE HOME POINTS
PENETRATING TRAUMA TO ABDOMEN - HEMODYNAMIC INSTABILITY OR PERITONITIS WARRANTS LAPAROTOMY
OBTAIN INFLOW CONTROL WITH PRINGLE MANEUVER AND OUTFLOW CONTROL WITH SUPRA AND INFRA HEPATIC IVC CLAMPING
AWARENESS OF ABERRANT ARTERIAL ANATOMY KEY FOR VASCULAR CONTROL
HIGH GRADE LIVER TRAUMA THAT REQUIRES OPERATIVE INTERVENTION, LIVER PACKING IS AN EFFECTIVE OPTION
DO NOT DIVIDE ALREADY INJURED LIVER WHEN PERFORMING SELECTIVE VASCULAR LIGATION
ANGIOEMBOLIZATION IS A USEFUL ADJUNCT FOR DAMAGE CONTROL
www.downstatesurgery.org
www.downstatesurgery.org
REFERENCES Como, John J. MD; et al Journal of Trauma- Practice Management Guidelines for Selective Nonoperative Management of Penetrating Abdominal Trauma. Injury Infection & Critical Care. March 2010 - Volume 68 - Issue 3 - pp 721-733
Hirshberg, A. Mattox, K., Top Knife: the Art and Craft of Trauma Surgery. EXTENT P/H 234 p, paperback Shrewsbury 2005.
Kozar, R., Westn Trauma Association/Critical Decisions in Trauma: Operative Management of Adult Blunt Hepatic Trauma. J Trauma. 2011; 71: 1-5
Scalea, T. Penetrating Liver Injuries. Current Trauma Report 2015 1:69-75
AAST Organ Injury Scale Liver/spleen • The American College of Surgeons. Committee on Trauma. • American Association for the. Surgery of Trauma