Embed Size (px)
DESCRIPTION
e-book ini menjelaskan teknik fertilisasi in vitro berdasarkan pendekatan genetika
Citation preview


In-Vitro Fertilization Third Edition hird Edition


In-Vitro Fertilization Third Edition Kay Elder Senior Research Scientist, Bourn Hall Clinic, Bourn, Cambridge, UK and Honorary Senior Lecturer in Clinical Embryology, University of Leeds, UK
Brian Dale Director of the Centre for Assisted Fertilization, Clinica Villa del Sole, Naples, Italy
with contributions from: Yves Ménézo Scientific Advisor, Unilabs, Paris, France and Geneva, Switzerland
Joyce Harper Reader in Human Genetics and Embryology, UCL Centre for PG & D, University College London, London, UK
and John Huntriss Reproduction and Early Development Research Group, Leeds Institute of Genetics, Health and Therapeutics, University of Leeds, UK

cambrid ge universit y press Cambridge, New York, Melbourne, Madrid, Cape Town, Singapore, São Paulo, Delhi, Dubai, Tokyo, Mexico City
Cambridge University Press Th e Edinburgh Building, Cambridge CB2 8RU, UK
Published in the United States of America by Cambridge University Press, New York
www.cambridge.org Information on this title: www.cambridge.org/9780521730723
© K. Elder and B. Dale 1997, 2000, 2011
Th is publication is in copyright. Subject to statutory exception and to the provisions of relevant collective licensing agreements, no reproduction of any part may take place without the written permission of Cambridge University Press.
Th is edition published by Cambridge University Press 2011 Second edition published by Cambridge University Press 2000 First edition published by Cambridge University Press 1997
Printed in the United Kingdom at the University Press, Cambridge
A catalogue record for this publication is available from the British Library
Library of Congress Cataloguing in Publication data Elder, Kay, 1946–
In-vitro fertilization / Kay Elder, Brian Dale ; with contributions from Joyce Harper, John Huntriss. – 3rd ed. p. ; cm.
Includes bibliographical references and index. ISBN 978-0-521-73072-3 (pbk.) 1. Fertilization in vitro, Human. I. Dale, Brian. II. Title. [DNLM: 1. Fertilization in Vitro–methods. 2. Germ Cells–growth & development. 3. Reproductive Techniques, Assisted. WQ 208] RG135.D34 2011 618.1′78059–dc22 2010040403
ISBN 978-0-521-73072-3 Paperback
Cambridge University Press has no responsibility for the persistence or accuracy of URLs for external or third-party internet websites referred to in this publication, and does not guarantee that any content on such websites is, or will remain, accurate or appropriate.
Every eff ort has been made in preparing this book to provide accurate and up-to-date information which is in accord with accepted standards and practice at the time of publication. Although case histories are drawn from actual cases, every eff ort has been made to disguise the identities of the individuals involved. Nevertheless, the authors, editors and publishers can make no warranties that the information contained herein is totally free from error, not least because clinical standards are constantly changing through research and regulation. Th e authors, editors and publishers therefore disclaim all liability for direct or consequential damages resulting from the use of material contained in this book. Readers are strongly advised to pay careful attention to information provided by the manufacturer of any drugs or equipment that they plan to use.

v
Contents
1 Review of cell and molecular biology 1 2 Endocrine control of reproduction: Controlled
ovarian hyperstimulation for ART 19 3 Gametes and gametogenesis 28 4 Sperm–oocyte interaction 50 5 First stages of development 64 6 Implantation and early stages of fetal
development 82 7 Stem cell biology 93 8 The clinical in-vitro fertilization
laboratory 109 9 Quality management in the IVF
laboratory 127 10 Sperm and ART 139
11 Oocyte retrieval and embryo culture 157 12 Cryopreservation of gametes and
embryos 191 13 Micromanipulation techniques 216 14 Preimplantation genetic diagnosis 238
Joyce Harper
15 Epigenetics and assisted reproduction 252 John Huntriss
Index 268 Th e color plates appear between pages 150 and 151
Preface vii Acknowledgements x


vii
of a human life” in formulating legislation surrounding assisted reproductive technologies (ART). Not surpris-ingly, these defi nitions vary from country to country and oft en refl ect the theological beliefs of the nations involved. Scientifi cally, a number of basic facts regard-ing fertilization and embryo development must be con-sidered in defi ning the “Beginning of Life”. Both in vivo and in vitro, gametes and preimplantation embryos are produced in great excess, with only a tiny proportion surviving to implant and produce off spring; human gametes are certainly error-prone, and the majority are never destined to begin a new life. Some female gam-etes may undergo fertilization, but subsequently fail to support further development due to defi ciencies in the process of oogenesis . Once gametes are selected, their successful interaction is probably one of the most dif-fi cult steps on the way to the formation of a new life. At this stage the two genomes have not yet mixed, and numerous developmental errors can still occur, with failures in oocyte activation , sperm decondensation, or in the patterns of signals that are necessary for the transition to early stages of embryo development. A fertilized ovum is a totipotent cell that initially divides into a few cells that are equally totipotent, but for a brief period of time these cells can give rise to one (a normal pregnancy), none (a blighted ovum or anem-bryonic vesicular mole), or even several (monozy-gotic twinning) individuals. Although fertilization is necessary for the life of a being, it is not the only critical event, as preimplantation embryo development can be interrupted at any stage by lethal processes or simple mistakes in the developmental program. A series of elegantly programmed events begins at gametogen-esis and continues through to parturition, involving a myriad of synchronized interdependent mechanisms, choreographed such that each must function at the right time during embryogenesis. Combinations of both physiological and chromosomal factors result in a continuous reduction, or “selection” of concep-tion products throughout the stages that lead to the
Th e union of male and female gametes during the pro-cess of fertilization marks the creation of a completely new individual, a unique event that ensures genetic immortality by transferring information from one generation to the next. It also creates variation, which introduces the eff ects of evolutionary forces. During the fi rst half of the nineteenth century, fertilization and the creation of early embryos was studied in a variety of marine, amphibian and mammalian species, and by the early 1960s had been successfully achieved in rab-bits (Chang, 1959 ), the golden hamster (Yanagimachi and Chang, 1964 ) and mice (Whittingham, 1968 ). Following a decade of extensive research in mouse, rat and rabbit reproductive biology and genetics, Robert Edwards began to study in-vitro maturation of human oocytes in the early 1960s (Edwards, 1965 ). On February 15, 1969, the journal Nature published a paper authored by R.G. Edwards, B.D. Bavister and P.C. Steptoe: “Early stages of fertilization in vitro of human oocytes matured in vitro” (Edwards et al ., 1969 ). Th e paper scandalized the international community – reporters and camera crews from all around the world fought to gain entry to the Physiological Laboratory in Cambridge, where Edwards and his team were based. It drew fi erce criticism from Nobel Laureates and much of the scientifi c, medical and religious establishment of the UK and elsewhere, being regarded as tampering with the beginning of a human life: religious, ethical and moral implications were numerous. IVF is now accepted completely as a clinical procedure; in the quest for improvements via new technology we should not be disheartened or surprised by irrational criti-cism, but draw courage from the pioneering work of Bob Edwards and his colleagues, whose brave perse-verance opened up an entirely new fi eld of interdiscip-linary study, embracing science, medicine, ethics, the law and social anthropology.
Half a century later, the creation of new life via human IVF continues to attract debate and discussion, prompting many governments to defi ne “the beginning
Preface

Preface
viii
potential implantation of an embryo in the uterus. Preimplantation embryogenesis might be described as a type of Darwinian fi lter where only the fi ttest embryos survive, and the survival of these is initially determined during gametogenesis.
It may be argued that the task of elaborating and defi ning the concept of a “new individual” belongs to philosophers and moralists. For some, the begin-ning of human life coincides with the formation of a diploid body in which the male and female chromo-somes are brought together. For others, true human life only occurs aft er implantation of the embryo in the uterine mucosa. Many believe that a new individ-ual is formed only aft er diff erentiation of the neural tube , whilst others believe that life begins when a fetus can live outside the uterus. In its most extreme form, some philosophers consider the acquisition of self-awareness of the newborn to defi ne a new life. Most scientists would probably agree that life is a continu-ous cyclical process, with the gametes merely bridging the gap between adult stages. Science, one of the bases of human intellect and curiosity, is generally impartial and oft en embraces international and religious bound-aries; ethicists, philosophers and theologians cannot proceed without taking into account the new informa-tion and realities that are continuously generated in the fi elds of biology and embryology. Advances in the expanding range and sensitivity of molecular biology techniques, in particular genomics, epigenomics and proteomics continue to further our understanding of reproductive biology, at the same time adding further levels of complexity to this remarkable process of cre-ating a new life.
In the decade since the previous edition of this book was published, the fi eld of human IVF has under-gone signifi cant transformation in many diff erent ways. Further scientifi c knowledge gained from use of sophisticated technology is one of them; management of patients and treatment cycles has also been infl u-enced by commercial pressures as well as legislative issues. Th e rapid expansion in both numbers of cycles and range of treatments off ered has introduced a need for more rigorous control and discipline in the IVF laboratory routine, and it is especially important that IVF laboratory personnel have a good basic under-standing of the science that underpins our attempts to create the potential beginning of a new life.
IVF is practiced in most countries of the world, and the number of babies born is estimated to be in the order of at least 10 million; a vast and comprehensive
collection of published literature covers clinical and sci-entifi c procedures and protocols, as well as information gained from modern molecular biology techniques. Many books are now available that cover every chapter (and in some cases individual paragraphs) of this edi-tion. Unlike 10 years ago, a wide range and variety of media, equipment and supplies is available specifi cally for use in human IVF, each with its own instructions and protocols for use. IVF is successfully carried out with numerous adaptations in individual labs, and spe-cifi c detailed protocols are no longer appropriate. Our aim in preparing this third edition was to try to dis-till large bodies of information relevant to human IVF into a comprehensive background of physiological, biochemical and physical principles that provide the scientifi c foundation for well-established protocols in current use.
Th is book is dedicated to Bob Edwards, who embraces and inspires all who are blessed with the experience of knowing him … we salute and honor his infi nite vision and endless optimism:
Th ere wasn’t any limit, no boundary at all to the future … and it would be so that a man wouldn’t have room to store such happiness… .
(James Dickey, American poet and novelist, 1923–1997 )
Further reading Braude P , Bolton V , Moore S ( 1988 ) Human gene expression
fi rst occurs between the four- and eight-cell stages of preimplantation development . Nature 333 : 459 –461.
Carp H , Toder V , Aviram A , Daniely M , Mashiach S , Barkai G ( 2001 ) Karyotype of the abortus in recurrent miscarriages . Fertility and Sterility 75 : 678 –682.
Chang MC ( 1959 ) Fertilization of rabbit ova in vitro . Nature (London ) 184 : 406 .
Edwards RG ( 1965 ) Maturation in vitro of human ovarian oocytes . Lancet ii : 926 –929.
Edwards RG ( 1965 ) Meiosis in ovarian oocytes of adult mammals . Nature 196 : 446 –450.
Edwards RG ( 1965 ) Maturation in vitro of mouse, sheep, cow, pig, rhesus monkey and human ovarian oocytes . Nature 208 : 349 –351.
Edwards RG ( 1972 ) Control of human development. In: Austin CR , Short RV (eds.) Artifi cial Control of Reproduction, Reproduction in Mammals , Book 5, Cambridge University Press , pp. 87–113.
Edwards RG ( 1989 ) Life Before Birth: Refl ections on the Embryo Debate . Hutchinson, London.
Edwards RG , Hansis C ( 2005 ) Initial diff erentiation of blastomeres in 4-cell human embryos and its signifi cance

Preface
ix
for early embryogenesis and implantation . Reproductive Biomedicine Online 2 : 206 –218.
Edwards RG , Bavister BD , Steptoe PC ( 1969 ) Early stages of fertilization in vitro of human oocytes matured in vitro . Nature 221 : 632 –635.
Hassold T , Chiu D ( 1985 ) Maternal age-specifi c rates of numerical chromosome abnormalities with special reference to trisomy . Human Genetics 70 : 11 –17.
Hassold T , Chen N , Funkhouser J , Jooss T , Manuel B , Matsuura J , Matsuyama A , Wilson C , Yamane JA , Jacobs PA ( 1980 ) A cytogenetic study of 1000 spontaneous abortuses . Annals of Human Genetics London 44 : 151 –178.
Jacobs PA , Hassold TJ ( 1987 ) Chromosome abnormalities: origin and etiology in abortions and live births. In: Vogal F , Sperling K (eds.) Human Genetics , Springer-Verlag , Berlin , pp. 233–244.
Márquez C , Sandalinas M , Bahçe M , Alikani M , Munné S ( 2000 ) Chromosome abnormalities in 1255 cleavage-
stage human embryos . Reproductive Biomedicine Online 1 : 17 –27.
Munné S , Cohen J ( 1998 ) Chromosome abnormalities in human embryos . Human Reproduction Update 4 : 842 –855.
Nothias JY , Majumder S , Kaneko KJ , et al . ( 1995 ) Regulation of gene expression at the beginning of mammalian development . Journal of Biological Chemistry 270 : 22077 –22080.
Steptoe PC , Edwards RG ( 1978 ) Birth aft er the re-implantation of a human embryo (letter) . Lancet 2 : 366 .
Warner C ( 2007 ) Immunological aspects of embryo development. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Informa Healthcare , London , pp. 155–168.
Whittingham DG ( 1968 ) Fertilization of mouse eggs in vitro . Nature 200 : 281 –282.
Yanagimachi R , Chang MC ( 1964 ) IVF of golden hamster ova . Journal of Experimental Zoology 156 : 361 –376.

x
and Mila Roode for help with stem cell biology; to Gianfraco Coppola for his help with drawings, and to Oleksii Barash, Marc van den Bergh, Th omas Ebner and Agnese Fiorentino for generously contributing original images of oocytes and embryos.
Special and very sincere thanks to Mike Macnamee and all of the friends and colleagues at Bourn Hall Clinic who continue to off er endless encouragement and support.
Acknowledgements
We are immensely grateful to Helen Picton, David Miller, John Huntriss, Jan Hogg and Allan Pacey for kindly allowing the current course material for the University of Leeds MSc in Clinical Embryology to be adapted for this book. We are also deeply indebted to numerous colleagues who patiently reviewed and revised each emerging chapter; particular thanks to Yves Ménézo, Bryan Woodward, Marc van den Bergh, Darja Kastelic, to Kathy Niakan, Jenny Nicholson

Chapter
1
Review of cell and molecular biology
Gametogenesis , embryo development , implantation and in-vitro culture involve numerous complex path-ways and interactions at the cellular and molecular level; a true understanding of their signifi cance requires secure fundamental knowledge of the underlying prin-ciples. Th is chapter therefore provides a condensed overview and review of basic terminology and defi ni-tions, with particular emphasis on aspects relevant to reproductive biology and in-vitro fertilization.
Mammalian cell biology In 1839, two German scientists, Matthias Jakob Schleiden and Th eodor Schwann, introduced the “cell theory,” the proposal that all higher organisms are made up of a single fundamental unit as a building block. In 1855, Rudolf Virchow extended this cell the-ory with a suggestion that was highly controversial at the time: “Omnis cellulae e celula” (all living cells arise from pre-existing cells). Th is statement has become known as the “biogenic law.” Th e cell theory is now accepted to include a number of principles: 1. All known living things are made up of cells. 2. Th e cell is the structural and functional unit of all
living things. 3. All cells come from pre-existing cells by division
(spontaneous generation does not occur). 4. Cells contain hereditary information that is
transmitted from cell to cell during cell division. 5. Th e chemical composition of all cells is basically
the same. 6. Th e energy fl ow (metabolism and biochemistry) of
life occurs within cells.
Although these features are common to all cells, the expression and repression of genes dictates individ-ual variation, resulting in a large number of diff erent types of variegated but highly organized cells, with
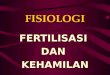
convoluted intracellular structures and interconnected elements. Th e average size of a somatic cell is around 20 µm; the oocyte is the largest cell in the body, with a diameter of approximately 120 µm in its fi nal stages of growth ( Figure 1.1 ). Th e basic elements and organelles in an individual cell vary in distribution and number according to the cell type. Bacterial cells diff er from mammalian cells in that they have no distinct nucleus, mitochondria or endoplasmic reticulum. Th eir cell membrane has numerous attachments, and their ribos-omes are scattered throughout the cytoplasm.
Cell membranes are made up of a bimolecular layer of polar lipids, coated on both sides with protein fi lms. Some proteins are buried in the matrix, others fl oat inde-pendently of each other in or on the membrane surface,
1
MV
SP
G
TZP
PVS ZP
rER
FCGJ
N
MCG
ChMT
PB1
Figure 1.1 Schematic diagram of oocyte ultrastructure showing the zona pellucida (ZP) and the perivitelline space (PVS), fi rst polar body (PB1), microvilli (MV), rough endoplasmic reticulum (rER), chromosomes (Ch) on the spindle (SP), Golgi complex (G), cortical granules (CG), two follicle cells (FC) attached to the oocyte and to each other via gap junctions (GJ). TZP = transzonal process, MT = Microtubules, M= Mitochondria.
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 1: Review of cell and molecular biology
2
forming a fl uid mosaic of diff erent functional units that are highly selective and specialized in diff erent cells. Cells contain many diff erent types of membrane, and each one encloses a space that defi nes an organelle, or a part of an organelle. Th e function of each organelle is determined largely by the types of protein in the membranes and the contents of the enclosed space. Membranes are important in the control of selective permeability, active and passive transport of ions and nutrients, contractile properties of the cell, and recognition of/association with other cells.
Cellular membranes always arise from pre-existing membranes, and the process of assembling new mem-branes is carried out by the endoplasmic reticulum (ER, see below). Th e synthesis and metabolism of fatty acids and cholesterol is important in membrane com-position, and fatty acid oxidation (e.g., by the action of reactive oxygen species, ROS) can cause the mem-branes to lose their fl uidity, as well as have an eff ect on transport mechanisms.
Microvilli are extensions of the plasma membrane that increase the cell surface area; they are abundant in cells with a highly absorptive capacity, such as the brush border of the intestinal lumen. Microvilli are present on the surface of oocytes, zygotes and early cleavage stage embryos in many species, and in some species (but not humans) their distribution is thought to be important in determining the site of sperm entry.
Cell cytoplasm is a fl uid space, containing water, enzymes, nutrients and macromolecules; the cyto-plasm is permeated by the cell’s architectural support, the cytoskeleton.
Microtubules are hollow polymer tubes made up of alpha-beta dimers of the protein tubulin. Th ey are part of the cytoskeletal structure, and are involved in intracellular transport, for example, the movement of mitochondria. Specialized structures such as cen-trioles, basal bodies, cilia and fl agella are made up of microtubules. During prophase of mitosis or meio-sis, microtubules form the spindle for chromosome attachment and movement.
Microfi laments are threads of actin protein, usually found in bundles just beneath the cell surface; they play a role in cell motility, and in endo- and exocytosis.
Centrioles are a pair of hollow tubes at right angles to each other, just outside the nucleus. Th ese struc-tures organize the nuclear spindle in preparation for the separation of chromatids during nuclear division. When the cell is about to divide, one of the centrioles migrates to the other side of the nucleus so that one lies at each end. Th e microtubule fi bers in the spindle are
contractile, and they pull the chromosomes apart dur-ing cell division.
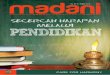
Th e nucleus of each cell is surrounded by a layered membrane, with a thickness of 7.5 nm. Th e outer layer of this membrane is connected to the ER, and the outer and inner layers are connected by “press studs,” creat-ing pores in the nuclear membrane that allow the pas-sage of ions, RNA and other macromolecules between the nucleus and the cell cytoplasm. Th ese pores have an active role in the regulation of DNA synthesis, since they control the passage of DNA precursors and thus allow only a single duplication of the pre-existing DNA during each cell cycle . Th e inner surface of the mem-brane has nuclear lamina, a regular network of three proteins that separate the membrane from peripheral chromatin. DNA is distributed throughout the nucleo-plasm wound around spherical clusters of histones to form nucleosomes, which are strung along the DNA like beads. Th ese are then further aggregated into the chromatin fi bers of approximately 30 nm diameter. Th e nucleosomes are supercoiled within the fi bers in a cylindrical or solenoidal structure to form chromatin, and the nuclear lamina provide anchoring points for chromosomes during interphase ( Figure 1.2 ):
Active chromatin = euchromatin – less condensed • Inactive (turned off ) = heterochromatin – more • condensed Before and during cell division, chromatin • becomes organized into chromosomes.
Th ree types of cell lose their nuclei as part of normal diff erentiation, and their nuclear contents are broken down and recycled:
Red blood cells (RBCs) • Squamous epithelial cells • Platelets. •
Other cells may be multinuclear: syncytia in muscle and giant cells (macrophages), syncytiotrophoblast.
Nuclear RNA is concentrated in nucleoli , which form dense, spherical particles within the nucleoplasm ( Figure 1.3 ); these are the sites where ribosome subu-nits, ribosomal RNA and transfer RNA are manufac-tured. RNA polymerase I rapidly transcribes the genes for ribosomal RNA from large loops of DNA, and the product is packed in situ with ribosomal proteins to generate new ribosomes (RNP: ribonucleoprotein particles).
Mitochondria are the site of aerobic respiration. Each cell contains 40–1000 mitochondria, and they are

Chapter 1: Review of cell and molecular biology
3
most abundant in cells that are physically and metabol-ically active. Th ey are elliptical, 0.5–1 µm in size, with a smooth outer membrane, an intermembranous space, and a highly organized inner membrane which forms cristae (crests) with elementary particles attached to them, “F1-F0 lollipops,” which act as molecular dyna-mos. Th e cristae are packed with proteins, some in large complexes: the more active the tissue, the more cristae in the mitochondria. Cristae are the site of intracellu-lar energy production and transduction, via the Krebs (TCA) cycle, as well as processes of oxidation, dehydro-genation, fatty acid oxidation, peroxidation, electron transport chains and oxidative phosphorylation. Th ey
also act as a Ca 2+ store, and are important in calcium regulation. Mitochondria contain their own double-stranded DNA that can replicate independently of the cell, but the information for their assembly is coded for by nuclear genes that direct the synthesis of mitochon-drial constituents in the cytoplasm. Th ese are trans-ported into the mitochondria for integration into its structures.
A number of rare diseases are caused by muta-tions in mitochondrial DNA, and the tissues primarily aff ected are those that most rely on respiration, i.e., the brain and nervous system, muscles, kidneys and the liver. All the mitochondria in the developing human embryo come from the oocyte, and therefore all mito-chondrial diseases are maternally inherited, transmit-ted exclusively from mother to child. In the sperm, mitochondria are located in the midpiece, providing the metabolic energy required for motility; there are no mitochondria in the sperm head.
Oocytes contain 100 000–1 000 000 mitochondria. • Sperm contain 70–100 mitochondria, in the • midpiece of each sperm. Th ese are incorporated into the oocyte cytoplasm, but do not contribute to the zygote mitochondrial population – they are eliminated at the four- to eight-cell stage. All of the mitochondria of an individual are • descendants of the mitochondria of the zygote, which contains mainly oocyte mitochondria.
The human mitochondrial genome
The sequence of human mitochondrial DNA was pub-lished by Fred Sanger in 1981, who shared the 1980 Nobel Prize in Chemistry with Paul Berg and Walter
The sequence of human mitochondrial DNA was pub-lished by Fred Sanger in 1981, who shared the 1980Nobel Prize in Chemistry with Paul Berg and Walter
2 nm
11 nm
30 nm
300 nm
700 nm
Centromere
Sister chromatids
1400 nm
Figure 1.2 Levels of chromatin packaging. From the top: DNA double helix, nucleosome “beads on a string,” chromatin fi ber of packed nucleosomes, section of extended chromosome, condensed chromosome and fi nally the entire chromosome.
Figure 1.3 Human oocyte at germinal vesicle stage, showing prominent nucleolus.

Chapter 1: Review of cell and molecular biology
4
Gilbert, “for their contributions concerning the deter-mination of base sequences in nucleic acids.” The mitochondrial genome has:
Small double-stranded circular DNA molecule • (mtDNA) 16 568 bp in length 37 genes that code for: •
2 ribosomal RNAs 22–23 tRNAs 10–13 proteins associated with the inner mito-chondrial membrane, involved in energy production
Other mitochondrial proteins are encoded by • nuclear DNA and specifi cally transported to the mitochondria. Mitochondrial DNA is much less tightly packed • and protected than nuclear DNA, and is therefore more susceptible to ROS damage that can cause mutations. As it is inherited only through the maternal line, • mutations can be clearly followed through gener-ations and are used as “markers” in forensic science and archaeology, as well as in tracking diff erent human populations and ethnic groups.
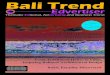
Mitochondria can be seen in diff erent distribu-tions during early development ( Figure 1.4 ); they do not begin to replicate until the blastocyst stage, and therefore an adequate store of active mitochon-dria in the mature oocyte is a prerequisite for early development.
Germinal vesicle oocyte: homogeneous clusters • associated with endoplasmic reticulum (ER) Metaphase I oocyte: polarized towards the spindle • Metaphase II oocyte: perinuclear ring and polar • body Embryos at 1c, 2c, 4c stages: perinuclear ring • Cytoplasmic fragments in cleavage stage embryos • contain large amounts of active mitochondria
Th e endoplasmic reticulum (ER ) is an intercon-nected lipoprotein membrane network of tubules, vesi-cles and fl attened sacs that extends from the nuclear membrane outwards to the plasma membrane, held together by the cytoskeleton. Th e ER itself is a mem-brane-enclosed organelle that carries out complex biosynthetic processes, producing proteins, lipids and polysaccharides. As new lipids and proteins are made, they are inserted into the existing ER mem-brane and the space enclosed by it. Smooth ER (sER ) is involved in metabolic processes, including synthesis
and metabolism of lipids, steroids and carbohydrates, as well as regulation of calcium levels. Th e surface of rough ER (rER ) is studded with ribosomes, the units of protein synthesis machinery. Membrane-bound vesicles shuttle proteins between the rER and the Golgi apparatus, another part of the membrane system. Th e Golgi apparatus is important in modifying, sorting and packaging macromolecules for secretion from the cell; it is also involved in transporting lipids around the cell, and in making lysosomes.
rER Has attached 80 s ribonucleoprotein particles, the • ribosomes (bacterial ribosomes are 70 s), which
Gilbert, “for their contributions concerning the deter-mination of base sequences in nucleic acids.” Themitochondrial genome has:
Small double-stranded circular DNA molecule•(mtDNA) 16 568 bp in length 37 genes that code for:•
2 ribosomal RNAs 22–23 tRNAs10–13 proteins associated with the inner mito-chondrial membrane, involved in energyproduction
Other mitochondrial proteins are encoded by•nuclear DNA and specifi cally transported to themitochondria. Mitochondrial DNA is much less tightly packed•and protected than nuclear DNA, and is thereforemore susceptible to ROS damage that can causemutations. As it is inherited only through the maternal line,•mutations can be clearly followed through gener-ations and are used as “markers” in forensic scienceand archaeology, as well as in tracking diff erenthuman populations and ethnic groups.
Figure 1.4 Mitochondrial aggregation patterns in a germinal vesicle (GV) oocyte (top), a metaphase I oocyte (center) and a metaphase II oocyte (bottom). Frames to the left are in fl uorescence using the potential sensitive dye JC-1 to show the mitochon-dria, frames on the right are transmitted light images. The two mitochondrial patterns: A (granular-clumped) and B (smooth) are shown. PB = polar body. Scale bars = 50 μm. (With permission from Wilding et al ., 2001, Human Reproduction 16, pp. 909–917.) See color plate section.

Chapter 1: Review of cell and molecular biology
5
are made in the nucleus and then travel out to the cytoplasm through nuclear pores . Ribosomes are composed of two subunits: 40 s • and 60 s (bacteria: 30 s and 50 s); the association between the subunits is controlled by Mg 2+ concentration. Polysomes = several ribosomes which move along • a single strand of mRNA creating several copies of the same protein .
sER A series of fl attened sacs and sheets, site of lipid • and steroid synthesis. Cells that make large amounts of steroids have • extensive sER .
Th e Golgi apparatus was fi rst observed by Camillo Golgi in 1898, using a novel silver staining technique to observe cellular structures under the light microscope; he was awarded the 1906 Nobel Prize in Physiology or Medicine for his studies on the structure of the nervous system. Th e Golgi apparatus consists of a fi ne, compact network of tubules near the cell nucleus, a collection of closely associated compartments with stacked arrays of smooth sacs and variable numbers of cisternae, vesicles or vacuoles. It is connected to rER, linked to vacuoles that can develop into secretory granules, which contain and store the proteins produced by the rER. All of the proteins exported from the ER are funneled through the Golgi apparatus, and every protein passes in a strict sequence through each of the compartments (cis, tubules, trans). Th is process consists of three stages: 1. “Misdirected mail” – sends back misdirected
proteins (cis). 2. “Addressing” – stacks of cisternae that modify
lipid and sugar moieties, giving them “tags” for subsequent sorting.
3. “Sorting and delivering” (trans): proteins and lipids are identifi ed, sorted and sent to their proper destination.
Transport occurs via vesicles, which bud from one com-partment and fuse with the next. Th e Golgi apparatus will move to diff erent parts of the cell according to the ongoing metabolic processes at the time – it is very well developed in secretory cells (e.g., in the pancreas).
Th e Golgi apparatus also makes lysosomes , which contain hydrolytic enzymes that digest worn-out org-an elles and foreign particles, acting as “rubbish bins” and providing a recycling apparatus for intracellular
digestion; they contain at least 50 diff erent enzymes, and “leaky” lysosomes can cause damage and kill cells. Macromolecules inside the cell are transported to lyso-somes, those from outside the cell reach them by pino-cytosis or phagocytosis; phagocytosis only occurs in specialized cells (e.g., white blood cells ).
Peroxisomes are microbody vesicles that contain oxidative enzymes such as catalase; they dispose of toxic hydrogen peroxide, and are important in cell aging .
Metabolism in the mammalian cell Four basic factors infl uence the metabolic activity of a cell: 1. Spatial: compartmentation, permeability,
transport, interactions. 2. Temporal: products become substrates, positive
and negative feedback. 3. Intensity/concentrations: precise amounts of
reactants/substrates/products. 4. Determinants that specify the structure of
enzymes and direct their formation/activation.
Molecules that are important in the biology/metabo-lism of the cell include carbohydrates, fats and lipids, and proteins.
Carbohydrates Carbohydrates are made up of carbon (C), hydro-gen (H) and oxygen (O), with the molecular ratio C x (H 2 O) y .
Monosaccharides : pentose – 5 C’s (ribose, • deoxyribose); hexose – 6 C’s (glucose, fructose) Disaccharides : two monosaccharides (sucrose, • maltose, lactose) Oligosaccharides : combine with proteins and lipids • to form glycoproteins and glycolipids , important in cell–cell recognition and the immune response Polysaccharides : polymers, insoluble, normally • contain 12 to 10 000 monosaccharides (starch, cellulose, glycogen) – Also form complexes with lipids and
phosphate.
Fats and lipids Fatty acids (FAs) have a long hydrocarbon chain end-ing in a carboxyl group :
Saturated FAs have single bonds between carbon • atoms.

Chapter 1: Review of cell and molecular biology
6
Unsaturated FAs have some double bonds between • carbon atoms.
Lipids are made up of FAs plus water : Phospholipids are important in membranes. • Glycolipids are important in receptors. •
Proteins Th e primary structure of a protein is a sequence of amino acids with peptide bonds:
–CONH–
Amino acids have at least one amino and one carboxyl group; they are amphoteric, and form dipolar zwitte-rions in solution. Proteins have secondary structures ; they can be folded into a helix, or form beta sheets that are held together by hydrogen bonds:
Alpha helix – tends to be soluble (most enzymes). • Beta sheets – insoluble – fi brous tissue. •
Proteins also have a three-dimensional tertiary struc-ture , which is formed by folding of the secondary struc-ture, held in place by diff erent types of bond to form a more rigid structure: disulfi de bonds, ionic bonds, intermolecular bonds (van der Waals – non-polar side chains attracted to each other).
High temperatures and extremes of pH denature proteins, destroying their tertiary structure and their functional activity.
Some proteins have a quaternary structure , with several tertiary structures fi tted together; e.g., collagen consists of a triple stranded helix.
Enzymes are proteins that catalyze a large number of biologically important actions, including anabolic and catabolic processes, and transfer of groups (e.g., methylase, kinase, hydroxylase, dehydrogenase). Some enzymes are isolated in organelles, others are free in the cytoplasm; there are more than 5000 enzymes in a typical mammalian cell.
Kinases: add a phosphate group, key enzymes in • many activation pathways. Methylases: add a methyl group. DNA methylation • is important in modifi cations that are involved in imprinting, lipid methylation is important for membrane stability, and proteins are also stabilized by methylation.
Most enzymes are conjugated proteins, with an active site that has a defi nite shape; a substrate fi ts into
the active site, or may induce a change of shape so that it can fi t.
Th e rate of an enzymatic reaction is aff ected by • temperature, pH, substrate concentration, enzyme concentration. Enzymes can be activated by removal of a blocking • peptide, maintaining the S-H groups, or by the presence of a cofactor. Th e active site of an enzyme is oft en linked to the • presence of an amino acid OH – group (serine, threonine). Mutations at this level render the enzymes inactive.
Enzyme inhibitors can be : Competitive – structurally similar • Noncompetitive – no similarity, form an • enzyme/inhibitor complex that changes the shape of the protein so that the active site is distorted Irreversible: heavy metal ions combine with -SH • causing the protein to precipitate. Lead (Pb 2+ ) and cadmium (Cd 2+ ) are the most hazardous; these cations can also replace zinc (Zn 2+ ), which is usually a stabilizer of tertiary structures.
Allosteric enzymes are regulated by compounds that are not their substrate, but which bind to the enzyme away from the active site in order to modify activ-ity. Th e compounds can be activators or inhibitors, increasing or decreasing the affi nity of the enzyme for the substrate. Th ese interactions help to regu-late metabolism by end-product inhibition/feedback mechanisms.
For example, phosphofructokinase (PFK): high ATP inhibits, low ATP activates.
Km is the substrate concentration that sustains half the maximum rate of reaction. Two or more enzymes may catalyze the same substrate, but in diff erent reac-tions; if the reserves of substrate are low, then the enzyme with the lowest Km will claim more of the substrate.
Cytokines
• Cytokines are proteins, peptides or peptidoglycan molecules that are involved in signaling pathways. They represent a large and diverse family of regu-latory molecules that are produced by many diff er-ent types of cell, and are used extensively in cellular communication:
Colony stimulating factors • Growth and diff erentiation factors •
• Cytokines are proteins, peptides or peptidoglycanmolecules that are involved in signaling pathways.They represent a large and diverse family of regu-latory molecules that are produced by many diff er-ent types of cell, and are used extensively in cellularcommunication:
Colony stimulating factors •Growth and diff erentiation factors•

Chapter 1: Review of cell and molecular biology
7
• Immunoregulatory and proinfl ammatory cytokines function in the immune system (inter-feron, interleukins, tumor necrosis factors).
Each cytokine has a unique cell surface receptor • that conducts a cascade of intracellular signaling that may include upregulation and/or downregula-tion of genes and their transcription factors. They can amplify or inhibit their own expression via • feedback mechanisms:
Type 1 cytokines enhance cellular immune • responses:
Interleukin-2 (IL-2), gamma interferon (IFN-γ), • TGF-β, TNF-β, etc.
Type 2 favor antibody responses: • IL-4, IL-5, IL-6, IL-10, IL-13, etc. •
Type 1 and type 2 cytokines can regulate each • other .
Metabolic pathways Each metabolic pathway is a series of reactions, organ-ized such that the products of one reaction become substrates for the next ( Figure 1.5 ). Th e reactants in a pathway may be modifi ed in a series of small steps, so that energy is released in controlled amounts, or minor adjustments can be made to the structure of molecules.
Anabolic pathways require energy to synthesize complex molecules from smaller units.
Catabolic pathways break molecules up into smaller units which can then be used to generate energy.
Each step in a pathway is catalyzed by a specifi c enzyme, and each enzyme represents a point for con-trol of the overall pathway. Th e steps of the pathway
• Immunoregulatory and proinfl ammatory cytokines function in the immune system (inter-feron, interleukins, tumor necrosis factors).
Each cytokine has a unique cell surface receptor •that conducts a cascade of intracellular signaling that may include upregulation and/or downregula-tion of genes and their transcription factors. They can amplify or inhibit their own expression via •feedback mechanisms:
Type 1 cytokines enhance cellular immune •responses:
Interleukin-2 (IL-2), gamma interferon (IFN-γ), •TGF-β, TNF-β, etc.
Type 2 favor antibody responses:•IL-4, IL-5, IL-6, IL-10, IL-13, etc. •
Type 1 and type 2 cytokines can regulate each •other .
Glycoproteins
Glycolipids
Glycosaminoglycans 2 ADP + Pi
2 ATP
Hexosephosphate
Triosephosphate
NADH
Pyruvate
NAD+ + H+
Lactate
H2O
Cytochrome
2 Fe2+
2 Fe3+
FAD+
Electron Transport Chain
Flavoprotein
FADHNAD+
NADH
TCA Cycle
32 ATP
4 ATP
Acetyl-CoAMitochondria
Cytosol
O2
4 ADP + Pi
Glyceraldehyde-3-P
Ribose-5-P
Pentosephosphate
Glucose
1
32Hexosamines
NADPH
Figure 1.5 Pathways that metabolize glucose in a mammalian cell.

Chapter 1: Review of cell and molecular biology
8
may be spatially arranged, so that the product of one reaction is in the right place to become the substrate of the next enzyme. Th is allows high local concen-trations of substrate molecules to build up, and bio-chemical reactions to proceed rapidly. A pathway arranged in this manner may be catalyzed by a multi-enzyme complex.
• Glycolysis , which breaks glucose down into pyruvate, takes place in the cell cytoplasm; pyruvate enters mitochondria to be further metabolized. • Fatty acid oxidation and the Krebs cycle (TCA or Citric acid cycle) take place in the mitochondrial matrix.
Th e Krebs cycle is part of a metabolic pathway that converts carbohydrates, fats and proteins into CO 2 and ATP, which is generated by a process of oxidative phos-phorylation . ATP is exported from the mitochondria for use in protein synthesis, DNA replication, etc.: all energy-requiring processes of life are coupled to the cleavage of ATP:
ATP ⇔ ADP + Phosphate + Energy
ATP is exported from the mitochondria in exchange for ADP arising from the ATP that has been broken down to drive cellular metabolism.
Redox reactions : oxidation and reduction are electron-transfer processes, involving NAD-NADH.
NADP(H) is generally used for anabolic reactions. • NAD(H) is used for catabolic reactions. •
Th ese reactions need ubiquinone and cytochrome C , cytochrome oxidase (inhibited by cyanide).
Oxidation: loss of electrons; reduction: gain of • electrons. An oxidizing agent removes electrons and is itself • reduced. A reducing agent gains electrons and is itself • oxidized.
Reactive oxygen species (ROS, oxygen radicals) ROS are molecules that contain the oxygen ion or peroxide; the presence of unpaired valence electrons makes them highly reactive. They are formed as a by-product of oxygen metabolism, and have an import-ant role in cell signaling mechanisms. However,
high levels of ROS (i.e., oxidative stress) can cause oxidative damage to nucleic acids, proteins and lip-ids, as well as inactivate enzymes by oxidation of cofactors.
Antioxidants such as ascorbic acid (vitamin C) , tocopherol (vitamin E) , glutathione , hypotaurine , pyruvic acid , uric acid and albumin are important in cellular defense mechanisms against ROS damage ( Figure 1.6 ).
Superoxide dismutase (SOD) SOD enzymes catalyze the dismutation of superoxide into oxygen and hydrogen peroxide, an important defense against potential ROS damage. Th ree SOD enzymes are present in mammalian cells:
SOD1: dimer, present in the cytoplasm, contains • Cu 2+ and Zn 2+ SOD2: tetramer, mitochondrial enzyme, contains • Mn 2+ SOD3: tetramer, extracellular, contains Cu • 2+ and Zn 2+
ROS can cause damage to DNA in oocytes, sperm and embryos, with important consequences for fer-tilization and embryo development (Guerin et al ., 2001 ). Oocytes are particularly susceptible during the fi nal stages of follicular growth, and ROS damage to sperm DNA has been strongly linked to male infertility (Sakkas et al ., 1998 ).
Fundamental principles of molecular biology Th e nucleic acids, DNA (deoxyribose nucleic acid; Figure 1.7 ) and RNA (ribose nucleic acid), are made up of: 1. Nucleotides: organic compounds containing a
nitrogenous base 2. Sugar: deoxyribose in DNA, ribose in RNA 3. Phosphate group.
Nucleotides are purines and pyrimidines, determined by the structure of the nitrogenous base.
DNA RNA
Purines Adenine (A) Adenine (A)
(double ring) Guanine (G) Guanine (G)
Pyrimidines Cytosine (C) Cytosine (C)
(single ring) Thymine (T = methylated U)
Uracil (U)

Chapter 1: Review of cell and molecular biology
9
Methylation of cytosine is important in gene silen-cing and imprinting processes .
Nucleotides also function as important cofactors in cell signaling and metabolism: coenzyme A (CoA), flavin adenine dinucleotide (FAD), flavin mononucleotide, adenosine triphosphate (ATP), nicotinamide adenine dinucleotide phosphate (NADP).
DNA Double-stranded helix with paired bases to form • complementary strands G=C or A=T • Pentose deoxyribose – phosphate backbone • Stabilized by H bonds between purines and • pyrimidines, on the inside of the helix Each pitch of the double helix has 10 base pairs . •
DNA replication DNA copies itself by semi-conservative replica-tion: each strand acts as a template for synthesis of a complementary strand. 1. Free nucleotides are made in the cytoplasm, and
are present in the nucleoplasm before replication begins.
2. Th e double helix unwinds, and hydrogen bonds, holding the two DNA strands together, break. Th is leaves unpaired bases exposed on each strand.
3. Th e sequence of unpaired bases serves as a template on which to arrange the free nucleotides from the nucleoplasm.
4. DNA polymerase moves along the unwound parts of the DNA, pairing complementary nucleotides from the nucleoplasm with each exposed base.
Follicular fluid
Storage of
transcriptsCuZnSOD
SOD, GPX
Oocyte
Vit.C
Hypotaurine
MnSOD
CuZnSOD
GPX
Catalase
+
GSH Tubal fluid
transcript
CSD: Cysteine sulfinate decarboxylase
MnSOD: Manganese superoxide dismutase
CuZnSOD: Copper zinc superoxide dismutase
GPX: Glutathione peroxidase
GSH: reduced glutathione
SOD GPX
CuZnSODMnSOD GPX
H2O2
O2
OHº
OHºº– O2º–
Embryo
Methionine Tubal epithelial cells
MnSOD GPX
CSD:
Figure 1.6 Mechanisms that protect oocytes and embryos from ROS damage (with thanks to Y. Ménézo).

Chapter 1: Review of cell and molecular biology
10
5. Th e same enzyme connects the nucleotides together to form a new strand of DNA, hydrogen bonded to the old strand:
DNA polymerase forms new hydrogen bonds • on the 5′3′ strand DNA ligase acts on the 3• ′5′ strand Several replication points appear along the • strand, which eventually join.
6. DNA is then mounted on “scaff olding proteins,” histones – and this is then wrapped around non-histones to form chromatin. Histones are basic proteins that bind to nuclear DNA and package it into nucleosomes; the regulation of gene expression involves histone acetylation and deacetylation. Th ere are two ATP-dependent remodeling complexes and acetyltransferases that preferentially bind activated states and fi x chromatin confi gurations:
Histone acetyltransferase coactivator complex • Histone deacetylase corepressor complex. •
Methylation of protamines and histones is a crucial component of imprinting processes: an association has been found between Beckwith–Wiedemann syn-drome and epigenetic alterations of LitI and H19 dur-ing in-vitro fertilization (DeBaum et al ., 2003 ).
Each mammalian cell contains around 1.8 m of DNA, of which only 10% is converted into specifi c pro-teins; the noncoding part of the DNA still carries gen-etic information, and probably functions in regulatory control mechanisms.
Genes = chief functional unit of DNA • Exons – contain information for the amino • acid sequence of a protein (coding sequence) Introns = non-coding regions in between exons • Codon = a group of three nucleotide bases • which code for one amino acid.
Nucleotides
CytosineP
P
P
P
P
P
P
P
P
P
S
S
S
S
SS
S
S
S
S
A
Deoxyribonucleic Acid (DNA)
G
T
TA
C G
A
C
T
NH2
N
N
H
Thymine
NHH3C
N
H
O
O
Guanine C
T
G
O
O
N
NH2N
Adenine
NH2
N
N
N
A
NH
NH
HN
Figure 1.7 Structure of DNA. Complementary base pairs form the DNA double helix; two hydrogen bonds form between A and T, three hydrogen bonds form between G and C. The two polynucleotide chains must be antiparallel to each other to allow pairing. S = sugar, P = phosphate group.

Chapter 1: Review of cell and molecular biology
11
The genetic code: the biochemical basis of heredity
In 1968, the Nobel Prize in Physiology or Medicine was awarded to Robert Holland, Ghobind Khorana and Marshall Nirenberg “for their interpretation of the genetic code and its function in protein synthesis”:
DNA transfers information to mRNA in the form of a • code defi ned by a sequence of nucleotides bases. The code is triplet, unpunctuated and non-• overlapping. Three bases are required to specify each amino acid, • there are no gaps between codons , and codons do not overlap. • Since RNA is made up of four types of nucleotides (A, C, G, U), the number of triplet sequences (codons) that are possible = 4 × 4 × 4 = 64; three of these are “stop codons” that signal the termination of a poly-peptide chain. The remaining 61 codons can specify 20 diff erent • amino acids, and more than one codon can specify the same amino acid (only Met and Trp are specifi ed by a single codon).
Since the genetic code thus has more information • than it needs, it is said to be “degenerate.”
A mutation in a single base can alter the coding for • an amino acid, resulting in an error in protein synthe-sis: translated RNA will incorporate a diff erent amino acid into the protein, which may then be defective in function (sickle cell anemia , phenylketonuria are examples of single gene defects).
Regulation of transcription
• A homeobox is a DNA sequence that codes for a 60 amino acid protein domain known as the homeodomain . A • homeodomain acts as a switch that controls gene transcription. • Homeobox genes , fi rst discovered in 1983, are a highly conserved family of transcription factors that switch on cascades of other genes:
Involved in the regulation of embryonic develop-• ment of virtually all multicellular animals, playing a crucial role from the earliest steps in embryogen-esis to the latest stages of diff erentiation Are arranged in clusters in the genome. •
• POU factors are a class of transcriptional regula-tors, required for high affi nity DNA binding, that are important in tissue-specifi c gene regulation; they are named after three proteins in the group: P it-l (also known as GHF-1), O ct-l and U nc-86 .
RNA Paired bases are G–C and A–U. • Pentose sugar = ribose. • Basic structure in mammalian cells is single-• stranded, but most biologically active forms contain self-complementary sequences that allow parts of the RNA to fold and pair with itself to form double helices, creating a specifi c tertiary structure. RNA molecules have a negative charge, and metal • ions such as Mg 2+ and Zn 2+ are needed to stabilize many secondary and tertiary structures. Hydroxyl groups on the deoxyribose ring make • RNA less stable than DNA because it is more prone to hydrolysis.
Th ere are many diff erent types of RNA, each with a dif-ferent function:
Transcription, translation/protein • synthesis: mRNA, rRNA, tRNA Post-transcriptional modifi cation or DNA • replication: small nuclear RNA (snRNA) , small nucleolar RNA (snoRNA) , guide RNA (gRNA) , ribonuclease P , ribonuclease MRP , etc. Gene regulation: microRNA (miRNA) , small • interfering RNA (siRNA), etc.
microRNAs are increasingly recognized • as “master regulators” of gene expression, regulating large networks of genes by chopping up or inhibiting the expression of protein coding transcripts.
Ribosomal RNA: 80% of total RNA Made in the nucleolus, then moved out into the • nucleoplasm and then to the cytoplasm to be incorporated into ribosomes .
Transfer RNA (4S RNA): 10-15% of total RNA Single strand, 75–90 nucleotides wound into a • clover leaf shape; each tRNA molecule transfers an amino acid to a growing polypeptide chain during translation .
A three-base anticodon sequence on the “tail” is com-plementary to a codon on mRNA; an amino acid is attached at the 3′ terminal site of the molecule, via a covalent link that is catalyzed by an aminoacyl tRNA synthetase. Each type of tRNA molecule can be attached to only one type of amino acid; however, multiple
In 1968, the Nobel Prize in Physiology or Medicine was awarded to Robert Holland, Ghobind Khorana and Marshall Nirenberg “for their interpretation of the genetic code and its function in protein synthesis”:
DNA transfers information to mRNA in the form of a •code defi ned by a sequence of nucleotides bases. The code is triplet, unpunctuated and non-•overlapping. Three bases are required to specify each amino acid, •there are no gaps between codons , and codons do not overlap.
• Since RNA is made up of four types of nucleotides (A, C, G, U), the number of triplet sequences (codons) that are possible = 4 × 4 × 4 = 64; three of these are “stop codons” that signal the termination of a poly-peptide chain. The remaining 61 codons can specify 20 diff erent •amino acids, and more than one codon can specify the same amino acid (only Met and Trp are specifi ed by a single codon).
Since the genetic code thus has more information •than it needs, it is said to be “degenerate.”
A mutation in a single base can alter the coding for •an amino acid, resulting in an error in protein synthe-sis: translated RNA will incorporate a diff erent amino acid into the protein, which may then be defective in function (sickle cell anemia , phenylketonuria are examples of single gene defects).
• A homeobox is a DNA sequence that codes for a 60 amino acid protein domain known as the homeodomain .A• homeodomain acts as a switch that controls gene transcription.
• Homeobox genes, fi rst discovered in 1983, are a highly conserved family of transcription factors that switch on cascades of other genes:
Involved in the regulation of embryonic develop-•ment of virtually all multicellular animals, playing a crucial role from the earliest steps in embryogen-esis to the latest stages of diff erentiation Are arranged in clusters in the genome. •
• POU factors are a class of transcriptional regula-tors, required for high affi nity DNA binding, that are important in tissue-specifi c gene regulation; they are named after three proteins in the group: Pit-l (also known as GHF-1), Oct-l and Unc-86 .

Chapter 1: Review of cell and molecular biology
12
codons in DNA can specify the same amino acid, and therefore the same amino acid can be carried by tRNA molecules that have diff erent three-base anticodons.
Methioninyl tRNA has a critical function, required • for the initiation of protein synthesis.
Messenger RNA: 3-5% of total cellular RNA (exception: sperm cells contain approx. 40% mRNA, and very little rRNA) mRNA molecules are single-stranded, complementary to one strand of DNA (coding strand) and identical to the other. DNA is transcribed into mRNA molecules, which carry coding information to the ribosomes for translation into proteins.
Transcription DNA information is transcribed to mRNA in the • nucleus, starting from a promoter sequence on the DNA at the 5′ end, and fi nishing at the 3′ end. All of the exons and introns in the DNA are • transcribed – stop and start sequences are encoded in the gene. Th e product, nuclear mRNA precursor (HnRNA, • heterogeneous nuclear RNA) is processed into mature cytoplasmic mRNA by splicing at defi ned base pairs to remove the introns and join the exons together. A cap of 7-methylG is added at the 5• ′ end. A string of polyA is added at 3• ′ end = polyA tail, 50–300 residues. Polyadenylated mRNA molecules are very • susceptible to degradation by ribonuclease (RNAse) aft er their release from the nucleolus
A promoter is a specifi c DNA sequence that signals the site for RNA polymerase to initiate transcription; this process needs an orchestrated interaction between pro-teins binding to specifi c DNA sequences, as well as pro-tein–protein interactions. DNA methylation is involved in the regulation of transcription. Gene sequences that lie 5′ to the promoter sequence bind specifi c proteins that infl uence the rate of transcription from a promoter:
A • TATA box aligns RNA polymerase II with DNA by interacting with transcription initiation factors (TFs). Proteins that bind to a CAAT box determine the • rate at which transcription is initiated, bringing RNA polymerase II into the area of the start site in order to assemble the transcriptional machinery.
Th e tertiary structure of the DNA (bends and folds) is important in making sure that all components are correctly aligned. Enhancers, silencers, hormone response elements • (steroid receptors) are important in determining the tissue-specifi c expression or physiological regulation of a gene; these factors respond to signals such as cAMP levels.
Transcription in oocytes
• Transcription takes place during oocyte growth, and stops before ovulation. mRNA turnover begins before ovulation: mRNA • molecules must be protected from premature translation. Oocytes contain mechanisms that remove histone • H1 from condensed chromatin. Diff erential acetylation profi les of core histone H4 • and H3 for parental genomes during the fi rst G1 phase may be important in establishing early zyg-otic “memory.” The timing of transcriptional events during the fi rst • zygotic cell cycle will have an eff ect on further devel-opmental potential.
Translation (protein synthesis) During protein synthesis, ribosomes move along the mRNA molecule and “read” its sequence three nucle-otides at a time, from the 5′ end to the 3′ end. Each amino acid is specifi ed by the mRNA’s codon , and then pairs with a sequence of three complementary nucle-otides carried by a particular tRNA (anticodon). Th e translation of mRNA into polypeptide chains involves three phases: initiation, elongation and termination. Messenger RNA binds to the small (40 s) subunit of the ribosome on rER in the cytoplasm, and six bases at a time are exposed to the large (60 s) subunit. Th e endpoint is specifi ed by a “stop” codon : UAA, UAG or UGA. 1. Initiation : Th e fi rst three bases (codon ) are
always AUG, and the initiation complex locates this codon at the 5′ end of the mRNA molecule. A methionyl-tRNA molecule with UAC on its coding site forms hydrogen bonds with AUG, and the complex associates with the small ribosome subunit (methionine is oft en removed aft er translation, so that not every protein has methionine as its fi rst amino acid). Some mRNAs contain a supernumerary AUG and associated short coding region upstream and independent
• Transcription takes place during oocyte growth, andstops before ovulation. mRNA turnover begins before ovulation: mRNA• molecules must be protected from prematuretranslation. Oocytes contain mechanisms that remove histone• H1 from condensed chromatin. Diff erential acetylation profi les of core histone H4• and H3 for parental genomes during the fi rst G1phase may be important in establishing early zyg-otic “memory.” The timing of transcriptional events during the fi rst• zygotic cell cycle will have an eff ect on further devel-opmental potential.

Chapter 1: Review of cell and molecular biology
13
of the main AUG coding region; these upstream open reading frames (uORFs) can regulate the translation of the downstream gene.
Th e large ribosome subunit has a P site which binds to the growing peptide chain, and an A site which binds to the incoming aa-tRNA.
2. Elongation : the unbound tRNA may now leave the P site, and the ribosome moves along the mRNA by one codon .
A peptide bond is formed, and the aa-tRNA • bond is hydrolyzed to release the free tRNA. A second tRNA molecule, bringing another • amino acid, bonds with the next three exposed bases. Th e two amino acids are held closely together, and peptidyl transferase in the small ribosomal subunit forms a peptide bond between them. Th e ribosome moves along the mRNA, • exposing the next three bases on the ribosome, and a third tRNA molecule brings a third amino acid, which joins to the second one.
3. Termination : Th e polypeptide chain continues to grow until a stop codon (UAA, UAC or UGA) is exposed on the ribosome. Th e stop codon codes for a releasing factor instead of another aa-tRNA; the completed peptide is released, and components of the translation complex are disassembled .
Cellular replication Replication of individual cells is the fundamen-tal basis of growth and reproduction for all living
organisms: each cell grows and then divides to prod-uce daughter cells. Cells can divide by using one of two diff erent mechanisms – mitosis or meiosis. During mitosis, the cellular DNA that represents the cell’s entire diploid genome is replicated into two copies, and the two cells produced aft er division each contain this same diploid genome. Meiosis, or “reduction div-ision,” splits the DNA in the diploid genome in half, so that the daughter cells are haploid, with a single copy of each gene. Th is is the process that leads to the gener-ation of the germ cells, sperm and oocyte.
Th e sequence of growth, replication and division that produces a new cell is known as the cell cycle ; in human cells, the mitotic cell cycle takes from 8 to 24 hours to complete. Th e cell cycle is divided into phases: G1, S, G2 (interphase) and M ( Figure 1.8 ):
G1: cell growth, a period of high metabolic activity • when new proteins are synthesized; rRNA, mRNA, tRNA are produced in the nucleolus, and new organelles are formed . S: synthesis of DNA and duplication of the • centrosome . Each new DNA double helix is surrounded by histones to form chromatids , which are held together at the centromere . G2: centrioles replicate, and the cell prepares for • mitosis . M: mitosis has four phases, during which the • replicated DNA is distributed to the two new daughter cells:
prophase, metaphase, anaphase, telophase . •
(i) Early prophase : the two replicated chromosomes condense, the nuclear
M – Mitosis(cell division)
2n:2c during G12n:4c during S
2n:4c during G2G2 (second growthphase and preparationfor mitosis)
G1 (growth and preparation
for DNA synthesis)
S – Synthesis(replication of DNA)
InterphaseG0 (resting,
non-dividing cells)
Figure 1.8 Phases of the cell cycle. n = chromosome number c = chromatid (DNA copy) number

Chapter 1: Review of cell and molecular biology
14
membrane dissociates, centrioles divide and migrate to diff erent poles, microtubules form an aster shape around the centrioles, and form the spindle. Spindle fi bers attach to the centromeres at the kinetochore.
(ii) Metaphase : chromosomes are lined up on the equatorial spindle plate; centromeres start to divide at the end of metaphase.
(iii) Anaphase : chromatids separate and are pulled by the spindle fi bers to opposite poles.
(iv) Telophase : chromatids have reached opposite poles, and a nuclear membrane forms around them. Th e chromosomes uncoil to become indistinct, spindle fi bers disintegrate, and the nucleolus reforms.
During cytokinesis , the cytoplasm divides to form two daughter cells. A ring of microfi laments develops around the cell, usually near the equator. Th ese micro-fi laments are attached to the cell membrane and con-tract when division takes place to pull the cell in (like a drawstring), creating a division furrow.
G0 : a cell can leave the cell cycle, temporarily or per-manently during G1, and enter a “resting” phase known as G0, where they will continue to carry out their des-ignated function (e.g., secretion, immune functions). Some G0 cells may be terminally diff erentiated, and will never re-enter the cell cycle to continue dividing. Others can be stimulated to re-enter at G1 and proceed to new rounds of cell division (e.g., lymphocytes encountering a new antigen). A G0 phase requires active repression of the genes required for mitosis – cancer cells cannot enter G0 and continue to divide indefi nitely.
Th e cell cycle is regulated by a sophisticated and carefully orchestrated series of control mechanisms, involving a number of proteins and cofactors whose levels fl uctuate according to the phase/stage: the major regulatory proteins include cyclins, cyclin-dependent kinases (CdKs) and anaphase-promoting complex (APC, or cyclosome).
Defi nitions
Chromosomes : the repository of genetic information, molecules of DNA complexed with specifi c proteins . Chromatin : the protein/DNA complex that makes up the chromosome. Chromatids : pairs of identical DNA molecules formed after DNA replication, joined at the centromere.
Centromere : constricted region in a chromosome, which divides it into two “arms.” It serves as an attach-ment site for sister chromatids and spindle fi bers, allowing chromosomes to be pulled to diff erent poles. Normally located centrally, but in some species found near the end (pericentric), at the end (telocentric) or spread all over the chromosomes (holocentric) . Kinetochore : structure that forms at the centromere to bind microtubules during mitosis . Diploid : two pairs of each chromosome in a cell . Haploid : one of each pair of chromosomes in a cell . Aneuploid : incorrect number of chromosomes; e.g., trisomy (three copies), monosomy (one copy).
Reproduction is based upon transmission of half of each parent’s chromosomes to the next gen-eration. Th is is carried out by setting aside a special population of germ cells that are destined to form the gametes, i.e., spermatozoa and oocytes . Successful completion of meiosis , a specialized form of cell div-ision, is a fundamental part of gametogenesis , and a detailed understanding of this process is a crucial background.
Mitosis and meiosis Meiosis diff ers from mitosis in a number of ways, as summarized below (see also Figure 1.9 ).
Mitosis Occurs in all tissues . • Involves one round of DNA replication for each • cell division. Produces genetically identical diploid somatic • (body) cells. Is a rapid process. • Th e daughter cells are genetically identical to • the parent cell and have the same number of chromosomes. Th is type of cell division takes place during • growth of an organism (e.g., embryonic growth), healing, the development of new cells, and is also important for maintaining populations of cells, replacing those that die.
Meiosis Occurs only in the ovary (oocytes) and the testis • (spermatozoa) . Involves one round of DNA replication and two • cell divisions, thus generating haploid products .
Chromosomes : the repository of genetic information,molecules of DNA complexed with specifi c proteins .Chromatin : the protein/DNA complex that makes upthe chromosome. Chromatids : pairs of identical DNA molecules formedafter DNA replication, joined at the centromere.
Centromere: constricted region in a chromosome,which divides it into two “arms.” It serves as an attach-ment site for sister chromatids and spindle fi bers,allowing chromosomes to be pulled to diff erent poles.Normally located centrally, but in some species foundnear the end (pericentric), at the end (telocentric) orspread all over the chromosomes (holocentric) . Kinetochore: structure that forms at the centromereto bind microtubules during mitosis .Diploid: two pairs of each chromosome in a cell .Haploid: one of each pair of chromosomes in a cell . Aneuploid: incorrect number of chromosomes; e.g.,trisomy (three copies), monosomy (one copy).

Chapter 1: Review of cell and molecular biology
15
Involves pairing of specifi c chromosome • homologues that then exchange pieces of DNA (genetic recombination), which results in daughter cells that are genetically diff erent from the original germ cells. Completion of this cell division may take years. •
Principles of meiosis In humans, meiosis is initiated during the fi rst trimester of gestation in females, and following puberty in males. Meiosis allows the exchange of DNA between overlap-ping sister chromatids, with subsequent recombination into two “new” chromatids – new, but related, gene
combinations can be created, facilitating genetic diver-sity. Th is occurs during the pachytene/diplotene stages of meiotic prophase, as illustrated in Figure 1.10 . In the middle diagram, the sister chromatids cross over at a sin-gle crossover point. In the diagram on the bottom, this leads to an equal and reciprocal exchange of chromatin.
Th e crossover point occurs between two DNA duplexes that contain four DNA strands (see Figure 1.10 ). Th e strands in fact switch their pairing at the joining point to form a crossed-strand junction, a mechanism that was fi rst proposed by Robin Holliday in 1964 and is known as a Holliday structure/junc-tion . Heteroduplexes are regions on recombinant DNA molecules where the two strands are not exactly
Mitosis
DNA replication
Diploid parent cell2n:2c
Prophase2n:4c
2n:4c
Diploid parent cell2n:2c
METAPHASE2n:4c
ANAPHASETELOPHASE4n:4c
CELL DIVISION
Haploid daughter cells1n:1c
Diploid daughter cells2n:2c
FIRST MEIOTIC DIVISION 1
METAPHASE 1
ANAPHASE ITELOPHASE IPROPHASE II
METAPHASE II
CROSSINGOVER
PROPHASE 1 Pairing of homologouschromosomes
DNA replication
Meiosis
SECONDMEIOTIC
DIVISION 2
1n:2c1n:2c
2n:4c
2n:4c
Figure 1.9 Comparison of mitosis and meiosis; mitosis generates two identical diploid daughter cells, and meiosis generates four chromosomally unique haploid cells from each diploid cell.

Chapter 1: Review of cell and molecular biology
16
complementary, and Holliday carried out experiments that detected heteroduplex regions in both strands of recombining DNA. In Figure 1.10 , the junction is mag-nifi ed to reveal its structure.
Meiosis diff ers from mitosis in terms of : 1. Checkpoint controls 2. DNA replication 3. Dependence on external stimuli 4. Regulation of cell cycle control proteins.
Cell cycle checkpoints control the order and timing of cell cycle transition, ensuring that critical events such as DNA replication and chromosome separation are com-pleted correctly – one process must be completed before another starts. During meiotic division , recombination must be completed before the beginning of cell division so that a correct segregation of homologous chromo-somes is obtained. Several genes have been identifi ed in yeast that are responsible for blocking meiosis when dou-ble-strand DNA breaks are not repaired. A checkpoint specifi c to meiotic cells ensures that anaphase I does not begin until paired chromosomes are correctly attached to the spindle. Th is control resembles the spindle-assembly checkpoint of mitotic cells. Fulka et al . ( 1998 ) carried out a series of experiments to test DNA-responsive cell cycle checkpoints in bovine and mouse oocytes, using ultra-violet (UV) irradiation to induce DNA damage or chem-ical treatment to prevent chromosome condensation. Th eir results suggest that replication-dependent check-points may be either inactive or highly attenuated in fully grown mammalian oocytes ; this should be borne in mind when considering the eff ects of endocrine or in-vitro manipulations carried out during assisted reproduction cycles, or the in-vitro maturation of oocytes. Although resumption of meiosis apparently has no cell cycle check-point, the fi rst cell cycle does, as does each embryonic cell cycle. Micromanipulation experiments in sperma-tocytes show that tension on the spindle generated by
attached homologues acts as a checkpoint. If this tension is eliminated by experimental manipulation, anaphase is prevented. A major diff erence between the mitotic and meiotic cell cycles lies in the fact that during mei-osis the oocyte can be blocked at precise phases of the cell cycle, until a specifi c stimulus (e.g., hormone or sperm) removes the block. In somatic cells , a state of quiescence or cell cycle block in response to a specifi c physiological state of the cell is described as the G0 phase of the cell cycle . However, G0 diff ers from meiotic blocks in terms of cell cycle regulation and the activity of the key kinases that maintain the arrest.
In oocytes, progression from the fi rst to the second meiotic arrest is usually referred to as oocyte matur-ation , and the oocyte is now ready to be ovulated, i.e., expelled from the ovary. Shortly aft er ovulation, fertil-ization occurs; removal of the second meiotic block at fertilization is called oocyte activation .
In the female, only one functional cell is produced • from the two meiotic divisions . Th e three remaining smaller cells are called polar bodies . In the male, four functional spermatozoa are • produced from each primary cell ( Figure 1.11 ).
Errors in meiosis Th e process of crossing over at diplotene in the female lasts for many years (from birth until ovulation), and the chromosomes may become sticky, become knot-ted together at diakinesis , and fail to separate correctly. Failure of chromosomes to separate during fi rst or second meiotic divisions results in aneuploidy. With autosomes this is usually lethal; sex chromosome aneu-ploidy can lead to anomalies of sexual development .
Sometimes pairs of chromosomes fail to rejoin aft er crossing over at diplotene and are lost from the gamete – they may become attached to another chromosome to produce a partial trisomy, or a balanced translocation.
Sister chromatids alignHolliday junction
Sister chromatids cross over at twolocations
An equal and reciprocal exchange ofchromatin occurs
Figure 1.10 Exchange of genetic material during chromosomal crossing over; a cross-over point is magnifi ed to illustrate the Holliday junction.

Chapter 1: Review of cell and molecular biology
17
HeLa cells
The majority of our knowledge about fundamen-tal principles of cell and molecular biology has been gained from model systems, particularly in yeast and bacteria, as well as human cell lines maintained in tis-sue culture. The fi rst human cell line to be propagated and grown continuously in culture as a permanent cell line is the HeLa cell, an immortal epithelial line: know-ledge of almost every process that takes place in human cells has been obtained through the use of HeLa cells , and the many other cell lines that have since been isolated.
The cells were cultured from biopsy of a cervical cancer taken from Henrietta Lacks, a 31-year-old African American woman from Baltimore, in 1951. George Gey, the head of the cell culture laboratory at Johns Hopkins Hospital, cultivated and propagated the cells; Henrietta died from her cancer 8 months later. Gey and his wife Margaret continued to propa-gate the cells, and sent them to colleagues in other laboratories. In 1954, Jonas Salk used HeLa cells to develop the fi rst vaccine for polio, and they have been used continually since then for research into cancer, AIDS, gene mapping, toxicity testing, and numerous other research areas – they even went up in the fi rst space missions to see what would happen to cells in zero gravity.
HeLa cells attained “immortality” because they have an active version of the enzyme telomerase, which prevents telomere shortening that is associ-ated with aging and eventual cell death. They adapt readily to diff erent growth conditions in culture, and
can be diffi cult to control: their growth is so aggres-sive that slight contamination by these cells can take over and overwhelm other cell cultures. Many other in-vitro cell lines used in research (estimates range from 1-10% of established cell lines) have been shown to have HeLa cell contamination . Twenty-fi ve years after Henrietta’s death, many cell cultures thought to be from other tissue types, including breast and pros-tate cells, were discovered to be in fact HeLa cells, a fi nding that unleashed a huge controversy and led to questions about published research fi ndings. Further investigation revealed that HeLa cells could fl oat on dust particles in the air and travel on unwashed hands to contaminate other cultures.
The cells were established in culture without the knowledge of her family, who discovered their “fame” accidentally 24 years after her death – they were con-tacted for DNA samples that could be used to map Henrietta’s genes in order to resolve the contamin-ation problem (Skoot, 2010 ).
Further reading Website information Basic concepts in molecular cell biology; based on
information at the National Health Museum : http://www.accessexcellence.org/RC/VL/GG/index.html
Books Berg JM , Tymoczko JL , Stryer L (eds.) ( 2002 ) Biochemistry ,
5th edn. W H Freeman & Co. , New York .
The majority of our knowledge about fundamen-tal principles of cell and molecular biology has been gained from model systems, particularly in yeast and bacteria, as well as human cell lines maintained in tis-sue culture. The fi rst human cell line to be propagated and grown continuously in culture as a permanent cell line is the HeLa cell, an immortal epithelial line: know-ledge of almost every process that takes place in human cells has been obtained through the use of HeLa cells , and the many other cell lines that have since been isolated.
The cells were cultured from biopsy of a cervical cancer taken from Henrietta Lacks, a 31-year-old African American woman from Baltimore, in 1951. George Gey, the head of the cell culture laboratory at Johns Hopkins Hospital, cultivated and propagated the cells; Henrietta died from her cancer 8 months later. Gey and his wife Margaret continued to propa-gate the cells, and sent them to colleagues in other laboratories. In 1954, Jonas Salk used HeLa cells to develop the fi rst vaccine for polio, and they have been used continually since then for research into cancer, AIDS, gene mapping, toxicity testing, and numerous other research areas – they even went up in the fi rst space missions to see what would happen to cells in zero gravity.
HeLa cells attained “immortality” because they have an active version of the enzyme telomerase, which prevents telomere shortening that is associ-ated with aging and eventual cell death. They adaptreadily to diff erent growth conditions in culture, and
can be diffi cult to control: their growth is so aggres-sive that slight contamination by these cells can takeover and overwhelm other cell cultures. Many otherin-vitro cell lines used in research (estimates rangefrom 1-10% of established cell lines) have been shownto have HeLa cell contamination . Twenty-fi ve yearsafter Henrietta’s death, many cell cultures thought tobe from other tissue types, including breast and pros-tate cells, were discovered to be in fact HeLa cells, afi nding that unleashed a huge controversy and led toquestions about published research fi ndings. Furtherinvestigation revealed that HeLa cells could fl oat ondust particles in the air and travel on unwashed handsto contaminate other cultures.
The cells were established in culture without theknowledge of her family, who discovered their “fame” accidentally 24 years after her death – they were con-tacted for DNA samples that could be used to mapHenrietta’s genes in order to resolve the contamin-ation problem (Skoot, 2010 ).
Spermatogonia
MITOSES
Oogonia
MEIOTICDIVISIONS
MEIOTICDIVISION
Primary spermatocytes
Secondaryspermatocytes
Spermatids
1st polar body
2nd polarbody
1 Oocyte Polar bodies4 Spermatozoa
Figure 1.11 Gametogenesis . Gametogenesis in the male gives rise to four functional spermatozoa; in the female only one of the four daughter cells becomes a functional oocyte. Modifi ed from Dale ( 1983 ).

Chapter 1: Review of cell and molecular biology
18
Dale B ( 1983 ) Fertilization in Animals . Edward Arnold , London .
Johnson MH ( 2007 ) Essential Reproduction , 6th edn. Blackwell Publishing , Oxford .
Lodish H , Berk A , Zipursky SL , Matsudaira P , Baltimore D , Darnell J (eds.) ( 2000 ) Molecular Cell Biology , 4th edn. W H Freeman & Co. , New York .
Skoot R ( 2010 ) Th e Immortal Life of Henrietta Lacks . Crown Publishing Group , New York .
Publications Barrit J , Kokot T , Cohen J , et al . ( 2002 ) Quantifi cation
of human ooplasmic mitochondria . Reproductive BioMedicine Online 4 : 243 –237.
Cummins JM ( 2002 ) Th e role of maternal mitochondria during oogenesis, fertilization and embryogenesis . Reproductive BioMedicine Online 4 : 176 –182.
DeBaum M , Niemitz E , Feinberg A ( 2003 ) Association of in vitro fertilization with Beckwith-Wiedemann syndrome and epigenetic alterations of LitI and H19 . American Journal of Human Genetics 72 : 156 –160.
Fulka J Jr., First N , Moor RM ( 1998 ) Nuclear and cytoplasmic determinants involved in the regulation of mammalian oocyte maturation . Molecular Human Reproduction 4 (1): 41 –49.
Guerin P , El Mouatassim S , Ménézo Y ( 2001 ) Oxidative stress and protection against reactive oxygen species in the pre-implantation embryo and its surroundings . Human Reproduction Update 7 : 175 –189.
Hays FA , Watson J , Shing Ho ( 2003 ) Caution! DNA crossing: crystal structures of Holliday junctions . Journal of Biological Chemistry 278 (50): 49663 –49666.
Huarte J , Stutz A , O’Connell ML , et al . ( 1992 ) Transient translational silencing by reversible mRNA deadenylation . Cell 69 : 1021 –1030.
Sakkas D , Urner F , Bizzaro D , et al . ( 1998 ) Sperm nuclear DNA damage and altered chromatin structure: eff ect on fertilization and embryo development . Human Reproduction 13 (Suppl. 4): 11 –19.
Sutovsky P , Navara CS , Schatten G ( 1996 ) Fate of the sperm mitochondria, and the incorporation, conversion, and disassembly of the sperm tail structures during bovine fertilization . Biology of Reproduction 55 : 1195 –1205.
Van Blerkom J ( 2004 ) Mitochondria in human oogenesis and preimplantation embryogenesis: engines of metabolism, ionic regulation and developmental competence . Reproduction 128 : 269 –280.
Ward WS ( 1993 ) Deoxyribonucleic acid loop domain tertiary structure in mammalian spermatozoa . Biology of Reproduction 48 (6): 1193 –1201.

Chapter
19
Endocrine control of reproduction : Controlled ovarian hyperstimulation for ART
Introduction Synchrony is essential for gametogenesis and correct embryo development, and a basic knowledge of repro-ductive endocrinology is fundamental to understand-ing synchrony in reproductive physiology. Although sexual arousal , erection and ejaculation in the male are obviously under cerebral control, it is less obvious that the ovarian and testicular cycles are also coordinated by the brain. For many years aft er the discovery of the gonadotropic hormones follicle stimulating hormone (FSH) and luteinizing hormone (LH) , the anterior pituitary gland was considered to be an autonomous organ, until animal experiments in which lesions were induced in the hypothalamus clearly demonstrated that reproductive processes were mediated by the nervous system. Th e hypothalamus is a small inconspicuous part of the brain lying between the midbrain and the forebrain; unlike any other region of the brain, it not only receives sensory inputs from almost every other part of the central nervous system (CNS) , but also sends nervous impulses to several endocrine glands and to pathways governing the activity of skeletal muscle, the heart and smooth muscle ( Figure 2.1 ). Via a sophisti-cated network of neural signals and hormone release, the hypothalamus controls sexual cycles, growth, preg-nancy, lactation and a wide range of other basic and emotional reactions. Each hypothalamic function is associated with one or more small areas that consist of aggregations of neurons called hypothalamic nuclei . In the context of reproduction, several groups of hypo-thalamic nuclei are connected to the underlying pituit-ary gland by neural and vascular connections.
Functions of the hypothalamus in reproduction
The hypothalamus links the nervous system to the pituitary gland by receiving signals from:
The central nervous system (CNS) •
The hypothalamus links the nervous system to the pituitary gland by receiving signals from:
The central nervous system (CNS) •
• Neurons from other parts of the brain, including the amygdala (involved in emotional response), the vis-ual cortex, and the olfactory cortex Endocrine factors from the testis, ovary, and other • endocrine glands.
It then releases factors into the hypothalamic-hypo-physeal portal veins that stimulate or inhibit synthe-sis and release of hormones by the pituitary, including (but not only):
GnRH: FSH and LH • TRH: Thyroid stimulating hormone (TSH) • CRF: (CRH) Adrenocorticotropic hormone (ACTH) • GHRH: Growth hormone (GH) . •
Gonadotropin hormone releasing hormone (GnRH) is secreted by groups of hypothal-amic nuclei and transported to the anterior pituitary through the portal vessels. GnRH, a decapeptide with the structure (Pyr)-Glu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH 2 , is the most important mediator of reproduction by the CNS. Any abnormality in its synthesis, storage, release or action will cause partial or complete failure of gonadal function. GnRH is secreted in pulses, and binds to spe-cifi c receptors on the plasma membrane of the gona-dotroph cells in the pituitary, triggering the inositol triphosphate second messenger system within these cells. Th is signal induces the movement of secretory granules towards the plasma membrane and even-tually stimulates the pulsatile secretion of LH and FSH. Alterations in the output of LH and FSH may be achieved by changing the amplitude or frequency of GnRH, or by modulating the response of the gonado-troph cells.
Th e anterior pituitary secretes LH, FSH and TSH, which are heterodimeric glycoprotein molecules that share a common alpha-subunit (also shared by human
• Neurons from other parts of the brain, including theamygdala (involved in emotional response), the vis-ual cortex, and the olfactory cortex Endocrine factors from the testis, ovary, and other• endocrine glands.
It then releases factors into the hypothalamic-hypo-physeal portal veins that stimulate or inhibit synthe-sis and release of hormones by the pituitary, including(but not only):
GnRH: FSH and LH • TRH: Thyroid stimulating hormone (TSH)• CRF: (CRH) Adrenocorticotropic hormone (ACTH) • GHRH: Growth hormone (GH) . •
2
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 2: Endocrine control of reproduction
20
chorionic gonadotropin: hCG), and diff er by their unique beta-subunit. Only the heterodimers have biological activity. Th e specifi c functions of FSH have been studied with targeted deletions in “knock-out” mice: FSH-defi cient male mice have a decrease in tes-ticular size and epididymal sperm count, but remain fertile. In contrast, homozygous females with the mutation are infertile: their ovaries show normal prim-ordial and primary follicles, with no abnormalities in oocytes, granulosa or theca cells, but the follicles fail to develop beyond the preantral stage. Th e ovaries also lack corpora lutea, and serum progesterone levels were
decreased by 50% compared with normal mice. Th ese studies indicate that, in mice, whereas spermatogenesis can continue in the absence of FSH, follicle maturation beyond the preantral stage is FSH-dependent.
At the onset of puberty, increased activity of the GnRH pulse generator induces maturation of the pituitary-gonadal axis. A progressive increase in the release of gonadotropins from the pituitary stimulates a subsequent rise in gonadal steroid hormones. In males, FSH released in response to the GnRH pulses acts on Sertoli–Leydig cells to initiate spermatogenesis, and LH acts on the Leydig cells to stimulate testosterone
HYPOTHALAMUS
PORTALVESSEL
ANTERIORPITUITARY
Inhibin: negative feedback
OVARIANFOLLICLE
Granulosa cell
Estradiol
Estradiol
Androgens
Capillary network
Theca interna cell
Gonadotroph
FSHLH
GnR
H
Figure 2.1 HPG axis. Schematic summary of the endocrine control of reproduction in mammals. From Johnson ( 2007 ).

Chapter 2: Endocrine control of reproduction
21
production. In females, FSH initiates follicular mat-uration and estrogen production, and LH stimulates theca cell steroidogenesis and triggers ovulation.
Male reproductive endocrinology Th e neuroendocrine mechanisms that regulate tes-ticular function are fundamentally similar to those that regulate ovarian activity. Th e male hypothalamo–pituitary unit is responsible for the secretion of gonado-tropins that regulate the endocrine and spermatogenic activities of the testis, and this gonadotropin secretion is subject to feedback regulation. A major diff erence between male and female reproductive endocrinology is the fact that gamete and steroid hormone production in the male is a continuous process aft er puberty, and not cyclical as in the female. Th is is refl ected in the absence of a cyclical positive feedback control of gonadotropin release by testicular hormones. Th e hypothalamus inte-grates all of these signals, and relays a response via the release of the peptide hormone GnRH. Th e hormone is released in pulses, with peaks every 90–120 minutes, and travels to the anterior pituitary gland, where it stimulates the synthesis and episodic release of gonado-tropic hormones to regulate sperm production in the testes. Interestingly and paradoxically, aft er the pituit-ary is initially stimulated to produce these gonadotro-pins, exposure to constant GnRH (or a GnRH agonist ) occupies the receptors so that the signaling pathway is disrupted, and inhibits gonadotropin release.
Th e process of spermatogenesis is a “two-cell” process, dependent on cross-talk between the Leydig (equivalent to ovarian theca) and Sertoli (equivalent to granulosa) cells via their respective gonadotropin receptors, LH and FSH. Sertoli cells respond to pituitary FSH, and secrete androgen binding proteins (ABPs) . Pituitary LH stimulates the interstitial cells of Leydig to produce testosterone, which combines with ABP in the seminiferous tubules, and testosterone controls LH secretion by negative feedback to the hypothalamus , maintaining the high intratesticular testosterone that is appropriate for normal spermatogenesis. Sertoli cells also produce inhibin, which exerts a negative feedback eff ect on pituitary FSH secretion. It probably also has a minor controlling infl uence on the secretion of LH.
Although less clearly than in the female, inhibin-like molecules in the male have also been found in tes-ticular extracts, which presumably also regulate FSH secretion. In humans, failure of spermatogenesis is correlated with elevated serum FSH levels, perhaps
through reduced inhibin secretion by the testis. In the testis, LH acts on Leydig cells, and FSH on Sertoli cells; males are very sensitive to changes in activity of LH and are relatively resistant to changes in FSH activity.
Gonadotropins in the male
1. Follicle stimulating hormone (FSH) : acts on the germinal epithelium to initiate spermatogenesis; receptors are found on Sertoli cells .
Sertoli cells secrete inhibin, which regulates FSH • secretion.
2. Luteinizing hormone (LH): stimulates the Leydig (interstitial) cells to produce testosterone.
Gonadotropic stimulation of the testes regulates the release of hormones (androgens) that are required for the development of puberty, and then to initiate and maintain male reproductive function and spermatogen-esis. Testosterone is the major secretory product of the testes, responsible for male sexual characteristics such as facial hair growth, distribution of body fat/muscle and other “masculine” features. Testosterone is metabolized in peripheral tissue to the potent androgen dihydro-testosterone, or to the potent estrogen estradiol. Th ese androgens and estrogens act independently to modu-late LH secretion. In the testis, the androgen receptor (AR) is found on Sertoli cells, Leydig and peritubular myoid cells. AR ablation inhibits spermatogenesis.
Feedback mechanisms are an important part of the reproductive axis; testosterone inhibits LH secretion, while inhibin (secreted by Sertoli cells in the testes) reg-ulates FSH secretion. If negative feedback is reduced, the pituitary responds by increasing its FSH secretion, similar to the situation in women reaching the meno-pause. Serum FSH levels in the male therefore act as an indicator of testicular germinal epithelial function – i.e., they are broadly correlated with spermatogenesis. Testosterone levels indicate Leydig cell function, and refl ect the presence of “masculine” characteristics :
Low levels in boys and castrates (4 nm/L). • Varies throughout the day in adult males – highest • in the morning. Levels decrease in older men. •
Serum LH level is diffi cult to assess, because it is released in pulses. Prolactin also interacts with LH and FSH in a complex manner, via inhibition of GnRH release from the hypothalamus . In males with hyperprolactinemia, inhibition of GnRH decreases LH secretion and testos-terone production; elevated prolactin levels may also have a direct eff ect on the CNS.
1. Follicle stimulating hormone (FSH) : acts on thegerminal epithelium to initiate spermatogenesis;receptors are found on Sertoli cells .
Sertoli cells secrete inhibin, which regulates FSH•secretion.
2. Luteinizing hormone (LH): stimulates the Leydig(interstitial) cells to produce testosterone.

Chapter 2: Endocrine control of reproduction
22
Male sexual maturity and reproductive function depends upon appropriate secretion of hormones:
• Gonadotropin releasing hormone (GnRH) Luteinizing hormone (LH) • Follicle stimulating hormone (FSH) • Testosterone (T) • Inhibin •
Serum endocrinology in the male
An endocrine profi le should be performed in men with oligospermia , or if there are signs or symptoms to sug-gest androgen defi ciency or endocrine disease .
1. Testosterone: normal range is 10–35 nmol/L, but serum levels undergo diurnal variation, with highest levels in the morning. Therefore the time of the test is important, and borderline levels should be compared with other measurements taken on diff erent days.
2. FSH and LH: normal serum levels of both are <10 IU/L (but normal ranges for specifi c laboratories should be noted).
Azoospermia with normal T, FSH and LH indicates • mechanical obstruction to the passage of sperm. Elevated FSH indicates germinal cell insuffi ciency. • Elevated FSH and LH, low T indicates primary tes-• ticular failure. Low FSH, LH and T indicates hypothalamic or pitu-• itary insuffi ciency .
Female reproductive endocrinology In females, gonadotropin output is regulated by the ovary. 1. Low circulating levels of estradiol exert a negative
feedback control on LH and FSH secretion, and high maintained levels of estradiol exert a positive feedback eff ect.
2. High plasma levels of progesterone enhance the negative feedback eff ects of estradiol and keep FSH and LH secretion down to a low level.
3. Th e secretion of FSH, but not LH, is also regulated by nonsteroidal high molecular weight (around 30 000 kDa) proteins called inhibins found in follicular fl uid : inhibin is found at high levels in late follicular phase plasma of fertile women, and although it has been used as a relative marker of ovarian reserve, the direct correlation is not clear.
In an ovulatory cycle, FSH stimulates the growth of fol-licles and increases the rate of granulosa cell produc-tion, the aromatization of androgenic precursors, and
the appearance of receptors for LH/hCG on granulosa cells. Estrogens enhance the action of LH on the fol-licle, and also exert a negative feedback eff ect on the hypothalamus and pituitary to inhibit further release of gonadotropins. Th e levels of estrogen produced by the granulosa cells increase throughout the follicu-lar phase until a threshold is reached where a separ-ate positive feedback mechanism elicits the LH surge and overrides the negative feedback on gonadotropin secretion – this is the trigger for ovulation.
Inhibin is also secreted by the ovary, and reduces pituitary FSH secretion.
LH stimulates theca cells to secrete androgens, which are converted to estrogens by the granulosa cells, and also infl uences granulosa cell diff erentiation , i.e., limits their replication and causes luteinization . LH stimulates the formation of progesterone directly from cholesterol in both granulosa and theca cells, and aft er ovulation the follicle changes rapidly from estrogen to progesterone dominance within a short period of time.
Two-cell two-gonadotropin theory
The “two-cell two-gonadotropin” theory suggests that both FSH and LH are required for estrogen biosyn-thesis, and this requires the cooperation of both theca and granulosa cells, with coordinated expression of a cytochrome P450 enzyme triad : cholesterol side-chain cleavage cytochrome P450 , 17-alpha hydroxylase cytochrome P450 and aromatase cytochrome P450 .
1. The surface of theca interna cells express LH recep-tors, and LH binding to these receptors initiates a G-protein cell signaling pathway that leads to pro-duction of cAMP . cAMP in turn stimulates the syn-thesis of androgens from acetate and cholesterol precursors.
2. Androstenedione is released from the thecal cell, and enters the mural granulosa cells , where P450 aromatase converts it to estradiol (E2) , which is released into the follicular fl uid and the blood-stream. This reaction is enhanced by FSH.
The secreted estradiol is required for follicle mat-uration and subsequent follicle survival, and these follicles are referred to as “gonadotropin-dependent ,” since they require both LH and FSH in order to carry out their steroid biosynthesis ( Figure 2.2 ).
Serum endocrinology in the female
A baseline endocrine profi le should be performed dur-ing the fi rst 3 days of the menstrual cycle; if the patient has amenorrhea or oligomenorrhea, a random blood sample must be used for the profi le .
• Gonadotropin releasing hormone (GnRH) Luteinizing hormone (LH)• Follicle stimulating hormone (FSH) • Testosterone (T) • Inhibin•
An endocrine profi le should be performed in men witholigospermia , or if there are signs or symptoms to sug-gest androgen defi ciency or endocrine disease .
1. Testosterone: normal range is 10–35 nmol/L, butserum levels undergo diurnal variation, with highestlevels in the morning. Therefore the time of the test isimportant, and borderline levels should be comparedwith other measurements taken on diff erent days.
2. FSH and LH: normal serum levels of both are<10 IU/L (but normal ranges for specifi c laboratoriesshould be noted).
Azoospermia with normal T, FSH and LH indicates•mechanical obstruction to the passage of sperm. Elevated FSH indicates germinal cell insuffi ciency. •Elevated FSH and LH, low T indicates primary tes-•ticular failure.Low FSH, LH and T indicates hypothalamic or pitu-•itary insuffi ciency .
The “two-cell two-gonadotropin” theory suggests thatboth FSH and LH are required for estrogen biosyn-thesis, and this requires the cooperation of both thecaand granulosa cells, with coordinated expression of acytochrome P450 enzyme triad : cholesterol side-chaincleavage cytochrome P450 , 17-alpha hydroxylasecytochrome P450 and aromatase cytochrome P450 .
1. The surface of theca interna cells express LH recep-tors, and LH binding to these receptors initiates aG-protein cell signaling pathway that leads to pro-duction of cAMP . cAMP in turn stimulates the syn-thesis of androgens from acetate and cholesterolprecursors.
2. Androstenedione is released from the thecal cell,and enters the mural granulosa cells , where P450aromatase converts it to estradiol (E2) , which isreleased into the follicular fl uid and the blood-stream. This reaction is enhanced by FSH.
The secreted estradiol is required for follicle mat-uration and subsequent follicle survival, and thesefollicles are referred to as “gonadotropin-dependent ,” since they require both LH and FSH in order to carryout their steroid biosynthesis ( Figure 2.2 ).
A baseline endocrine profi le should be performed dur-ing the fi rst 3 days of the menstrual cycle; if the patienthas amenorrhea or oligomenorrhea, a random bloodsample must be used for the profi le .

Chapter 2: Endocrine control of reproduction
23
• Serum FSH levels >15 IU/L indicates poor ovarian activity, and levels >25 IU/L suggest menopause or premature ovarian failure . Elevated serum LH suggests the presence of poly-• cystic ovarian disease . A serum level of progesterone >30 nmol/L is indica-• tive of ovulation. Amenorrhea with very low levels of FSH and LH • (2 IU/L) suggests pituitary failure or hypogonado-tropic hypogonadism . The most usual cause of elevated serum testoster-• one is polycystic ovary syndrome (PCOS), but levels >5 nmol/L should be investigated to exclude other
causes (congenital adrenal hyperplasia, Cushing’s syndrome , androgen secreting tumors ). Mild elevations in serum prolactin are associated • with stress, and can occur simply as a result of hav-ing blood taken .
Controlled ovarian hyperstimulation (COH) for ART During controlled ovarian hyperstimulation for assisted reproduction , GnRH agonists are used to suppress pituitary release of both LH and FSH. Follicle growth and development can be achieved by the administration of pure FSH alone, in the absence of exogenous LH. However, in women with hypogo-nadotropic hypogonadism , who lack both LH and FSH, administration of FSH alone promotes follicu-lar growth, but the oocytes apparently lack develop-mental competence. Th e diff erence between these two patient populations has been attributed to the fact that downregulation with a GnRH agonist leaves suffi cient residual LH secretion to support FSH-induced follicu-lar development. Th e response to FSH in downregu-lated ART patients is independent of serum LH levels at the time of starting FSH administration. Granulosa cells synthesize estradiol in response to FSH and LH, and estradiol levels per retrieved oocyte appear to
• Serum FSH levels >15 IU/L indicates poor ovarian activity, and levels >25 IU/L suggest menopause or premature ovarian failure . Elevated serum LH suggests the presence of poly-•cystic ovarian disease . A serum level of progesterone >30 nmol/L is indica-•tive of ovulation. Amenorrhea with very low levels of FSH and LH •(2 IU/L) suggests pituitary failure or hypogonado-tropic hypogonadism . The most usual cause of elevated serum testoster-•one is polycystic ovary syndrome (PCOS), but levels >5 nmol/L should be investigated to exclude other
causes (congenital adrenal hyperplasia, Cushing’ssyndrome , androgen secreting tumors ). Mild elevations in serum prolactin are associated•with stress, and can occur simply as a result of hav-ing blood taken .
Cholesterol
THECA CELL
LH
Basementmembrane
FSH
Pregnenolone
Progesterone
Testosterone
Estradiol
Progesterone
Pregnenolone
GRANULOSA CELL
Androgen
Cholesterol
Androstenedione
Hormone Normal rangeFollicle stimulating hormone (FSH) <8 IU/LLuteinizing hormone (LH) <10 IU/LEstradiol: early follicular 50–200 pmol/LMid-cycle 50–1000 pmol/LLuteal 250–1000 pmol/LProgesterone mid-luteal >30 nmol/LTestosterone 0.5–3.0 nmol/LSex hormone binding globulin (SHBG)
16–119 nmol/L
Free androgen index (FAI) (T × 100)/SHBG
<5
TSH 0.5–5.5 mU/LTotal thyroxine 60–160 nmol/LProlactin <600 mIU/L
Figure 2.2 Two-cell two-gonado-tropin hypothesis.

Chapter 2: Endocrine control of reproduction
24
be correlated to developmental competence of the oocytes. Follicular fl uid contains high levels of ster-oids and enzymes, and aspiration of follicles during ART procedures removes this milieu from its natural environment aft er follicle rupture in vivo; in add-ition, follicle fl ushing removes the cells which would have been incorporated in the new corpus luteum. It is possible that this artifi cial separation leads to luteal insuffi ciency or other subtle consequences on ovarian physiology which are not at present evident, and pro-gesterone is usually administered to support the luteal phase in downregulated cycles.
GnRH analogues have been used in COH pro-tocols since the mid-1980s, when high tonic levels of LH during the follicular phase were found to be detrimental to oocyte competence, decreasing fer-tilization and pregnancy rates (Howles et al ., 1986). GnRH agonists were used to suppress and control the LH surge, and thus the timing of ovulation could be regulated. Their use then led to the development of programmed COH protocols, which provide a convenient and effective means of scheduling and organizing a clinical IVF program: oocyte retrievals can be scheduled for specific days of the week, or in “batches.” GnRH analogues have substitutions in their peptide sequence that increase their bioavail-ability over that of native GnRH, and they bind to receptors on the anterior pituitary so that the recep-tors are fully occupied, blocking release of FSH and LH. Two types of analogues are currently used in ART protocols :
1. GnRH agonists : Continuous administration initially causes LH and FSH hypersecretion (fl are-up), and aft er a period of about 10 days the pituitary store of gonadotropins is depleted. Th e pituitary is desensitized so that secretion of LH and FSH is suppressed, preventing ovarian steroidogenesis and follicular growth, creating an artifi cial but reversible menopausal state. Diff erent GnRH agonist preparations can be administered by depot injection (Decapeptyl , Zoladex ), daily subcutaneous injection (buserelin ), or daily intranasal sniff (nafarelin , Synarel ).
2. GnRH antagonists bind to and immediately block receptors on the pituitary; there is no initial hypersecretion of gonadotropins, but their release is instead immediately and rapidly suppressed. A third generation of these compounds (cetrorelix,
ganirelix) is now used to suppress LH secretion aft er follicular growth has been fi rst stimulated by gonadotropin administration on Day 1 or 2 of a menstrual cycle (or withdrawal bleed aft er oral contraceptive pill administration). Th e antagonist is administered by daily subcutaneous injection from approximately Day 6 of stimulation, or when the largest follicle size reaches 14 mm, and continued until the day of hCG administration. Due to the fact that LH suppression is more complete than with agonist administration, some protocols advocate compensating by simultaneously “adding back” recombinant LH (Luveris ) during the period of antagonist treatment.
Several protocols using GnRH analogues have been devised, and individual ART programs apply the same strategy with a variety of diff erent drugs and schedules. Downregulation with a GnRH agonist may begin either in the luteal or the follicular phase (“long protocol’) of the previous menstrual cycle, and can be administered with any preparation of choice. It may also be administered from Day 1 of the treat-ment cycle and continued until ovulation induction with hCG (“short protocol,” sometimes also known as “fl are-up protocol” ). Th e “ultrashort protocol” uses only three doses of the agonist, on Days 2, 3 and 4 of the treatment cycle. Treatment cycles can also be scheduled by programming menstruation using an oral contraceptive preparation such as nore-thisterone 5 mg three times a day, and inducing a withdrawal bleed. Th e “standard” protocols are not always suitable for every patient, and every treat-ment regimen should be tailored according to the patient’s medical history and response to any pre-vious ovarian stimulation. Patients with suspected polycystic ovarian disease (PCO) and those with limited ovarian reserve (“poor responders”) require careful management and individualized treatment regimens.
Th e use of GnRH antagonists is felt to be more physiological (“natural”), since there is no initial sup-pression of pituitary FSH; however, antagonist cycles require more meticulous monitoring of the cycle in order to prevent a premature LH surge.
Original protocols for ovarian stimulation involved oral administration of clomifene citrate (Clomid) , which acts as both an agonist and an antagonist by com-petitively binding to receptors on the hypothalamus

Chapter 2: Endocrine control of reproduction
25
and pituitary. It displaces endogenous estrogen and eliminates feedback inhibition, which stimulates FSH release from the pituitary. Clomid is administered in a dose of 50–100 mg twice daily for 5 days from Days 2–5 of the menstrual cycle, and FSH injections are commenced on Day 3. Th is protocol has the disad-vantage that it does not block the LH surge, and there-fore the cycle must be carefully monitored in order to detect and intercede before an LH surge induces ovula-tion. However, it may sometimes be useful for patients who have failed to respond to agonist or antagonist protocols.
With any of the COH protocols, a baseline assess-ment is normally conducted prior to starting gonado-tropin stimulation, in order to ensure that the ovaries are quiescent and the endometrial lining has been shed, as well as to exclude any pathologies that might jeop-ardize the treatment cycle.
Stimulation protocols for IVF
1. Clomifene citrate (CC)/Gonadotropins
CC 100 mg from Day 2, for 5 days. • Gonadotropin stimulation from Day 4 to day of hCG. •
2. Long GnRH agonist protocols
a. Luteal phase start (7 days after presumed ovulation, approx. Day 21) GnRH agonist from Day 21 until menses. • Start gonadotropins after baseline assessment, con-• tinue to day of hCG. Reduce GnRH agonist dose after start of stimulation, • continue until day of hCG .
b. Follicular phase start Start GnRH agonist Day 2 after menses . • Continue until downregulation, usually at least 14 • days. Start gonadotropin stimulation. • Reduce GnRH dose after start of stimulation, con-• tinue to day of hCG.
3. Short GnRH agonist protocol Start GnRH agonist on Day 2 after menses, continue • to day of hCG. Gonadotropin stimulation from Day 3 to day of hCG. •
4. Ultrashort GnRH agonist protocol Start GnRH agonist on Day 2 after menses, continue • for 3 days. Gonadotropin stimulation from Day 3 to day of hCG . •
5. GnRH antagonist protocol Gonadotropin stimulation from Day 2 until day of • hCG. Start antagonist after 6 days of stimulation, or when • largest follicle size = 14 mm . Continue antagonist until day of hCG . •
Baseline assessment: ultrasound
• Ovaries : size, position Shape, texture • Cysts • Evidence of PCO • Uterus: endometrial size, shape, texture and • thickness Fibroids • Congenital or other anomalies/abnormalities • Hydrosalpinges, loculated fl uid •
Baseline assessment: endocrinology
• Estradiol: < 50 pg/mL LH: < 5 IU/L • Progesterone: < 2 ng/mL •
If any values are elevated: continue GnRH agonist treatment • withhold stimulation • reassess 3–7 days later. •
If LH remains elevated:
withhold stimulation • increase dose of GnRH agonist. •
(FSH: < 10 IU/L without downregulation.)
Ovarian stimulation
Pure FSH (Gonal F, Puregon, Menopur) by subcutane-ous self-injection. Starting dose according to age and/or history:
age 35 or younger: 150 IU/day • age over 35: 225 IU/day • depending on previous response, up to 300–450 IU • daily.
Begin monitoring after 7 days of stimulation (adjusted according to history and baseline assessment ).
Cycle monitoring
Assess follicular growth after 6–8 days of gonado-tropin stimulation .
Ultrasound assessment •
1. Clomifene citrate (CC)/Gonadotropins
CC 100 mg from Day 2, for 5 days. • Gonadotropin stimulation from Day 4 to day of hCG. •
2. Long GnRH agonist protocols
a. Luteal phase start (7 days after presumed ovulation, approx. Day 21) GnRH agonist from Day 21 until menses. • Start gonadotropins after baseline assessment, con-•tinue to day of hCG. Reduce GnRH agonist dose after start of stimulation, •continue until day of hCG .
b. Follicular phase start Start GnRH agonist Day 2 after menses . • Continue until downregulation, usually at least 14 •days. Start gonadotropin stimulation.• Reduce GnRH dose after start of stimulation, con-•tinue to day of hCG.
3. Short GnRH agonist protocol Start GnRH agonist on Day 2 after menses, continue •to day of hCG. Gonadotropin stimulation from Day 3 to day of hCG. •
4. Ultrashort GnRH agonist protocol Start GnRH agonist on Day 2 after menses, continue •for 3 days. Gonadotropin stimulation from Day 3 to day of hCG . •
5. GnRH antagonist protocol Gonadotropin stimulation from Day 2 until day of • hCG. Start antagonist after 6 days of stimulation, or when•largest follicle size = 14 mm . Continue antagonist until day of hCG . •
• Ovaries : size, position Shape, texture • Cysts• Evidence of PCO• Uterus: endometrial size, shape, texture and• thickness Fibroids• Congenital or other anomalies/abnormalities • Hydrosalpinges, loculated fl uid•
• Estradiol: < 50 pg/mL LH: < 5 IU/L • Progesterone: < 2 ng/mL •
If any values are elevated: continue GnRH agonist treatment • withhold stimulation • reassess 3–7 days later. •
If LH remains elevated:
withhold stimulation • increase dose of GnRH agonist.•
(FSH: < 10 IU/L without downregulation.)
Pure FSH (Gonal F, Puregon, Menopur) by subcutane-ous self-injection. Starting dose according to age and/or history:
age 35 or younger: 150 IU/day • age over 35: 225 IU/day• depending on previous response, up to 300–450 IU•daily.
Begin monitoring after 7 days of stimulation (adjusted according to history and baseline assessment). tt
Assess follicular growth after 6–8 days of gonado-tropin stimulation .
Ultrasound assessment •

Chapter 2: Endocrine control of reproduction
26
• Follicle size 14 mm or less: review in 2 or 3 days Follicle size 16 mm or greater: review daily •
Plasma estradiol • Plasma LH •
Review as necessary. •
Induction of ovulation
hCG (Profasi) 10 000 IU or r-hCG (Ovitrelle/Ovidrel 6500 IU) by subcutaneous injection when:
Leading follicle is at least 17–18 mm in diameter • Two or more follicles >14 mm in diameter • Endometrium: at least 8 mm in thickness with tril-• aminar “halo” appearance Estradiol levels approx. 100–150 pg/mL per large • follicle Oocyte retrieval scheduled for 34–36 hours post-• hCG .
Oocyte retrieval (OCR) procedures are performed by vacuum aspirating follicles under vaginal ultra-sound guidance using disposable OCR needles, col-lecting aspirates into heated 15 mL Falcon tubes . Th e procedure can be safely carried out as an outpatient procedure, using either paracervical block for local anesthesia, intravenous sedation or light general anes-thesia. An experienced operator can collect an aver-age number of oocytes (i.e., 8–12) in a 5–10 minute time period, and the patient can usually be discharged within 2–3 hours of a routine oocyte collection
Luteal phase support Hormonal support of the luteal phase is felt to be neces-sary following pituitary downregulation with GnRH agonist treatment, and is usually also used in antagon-ist cycles. Progesterone supplementation may be intro-duced on the evening following oocyte retrieval :
Cyclogest pessaries per vaginam, 200–400 mg • twice a day Utrogestan capsules per vaginam, 100–200 mg • three times a day Crinone gel per vaginam, once daily application • Gestone 50–100 mg daily by intramuscular • injection.
Further reading Books Austin CT , Short RV ( 1972 ) Reproduction in Mammals .
Cambridge University Press , Cambridge .
Balen A , Jacobs H ( 2003 ) Infertility in Practice . Churchill Livingstone , Edinburgh .
Carr BR , Blackwell RE , Azziz R ( 2005 ) Essential Reproductive Medicine . McGraw Hill , New York .
Johnson MH ( 2007 ) Essential Reproduction , 6th edn. Blackwell Publications , Oxford .
Publications Bourgain C , Devroey P ( 2003 ) Th e endometrium in
stimulated cycles for IVF . Human Reproduction Update 9 (6): 515 –522.
Brinsden P ( 2005 ) Superovulation strategies in assisted conception. In: Brinsden P (ed.) A Textbook of In Vitro Fertilization and Assisted Reproduction . Taylor-Francis , London .
Conway , GS ( 1996 ) Clinical manifestations of genetic defects aff ecting gonadotrophins and their receptors . Clinical Endocrinology 45 : 657 –663.
Cortvrindt R , Smitz J , Van Steirteghem AC ( 1997 ) Assessment of the need for follicle stimulating hormone in early preantral mouse follicle culture in vitro . Human Reproduction 12 : 759 –768.
Hillier SG ( 1991 ) Regulatory functions for inhibin and activin in human ovaries . Journal of Endocrinology 131 : 171 –175.
Hillier SG ( 2009 ) Th e science of ovarian ageing – how might knowledge be translated into practice? In: Bewley S , Ledger W , Nikolaou D (eds.) Reproductive Ageing . RCOG Press , London , pp. 75–87.
Howles , CM , Macnamee , MC , Edwards , RG ( 1987 ) Follicular development and early luteal function of conception and non-conceptual cycles aft er human in vitro fertilization . Human Reproduction 2 : 17 –21.
Howles CM , Macnamee MC , Edwards RG , Goswamy R , Steptoe PC ( 1986 ) Eff ect of high tonic levels of luteinizing hormone on outcome of in vitro fertilization . Lancet 2 : 521 –522.
Kumar TR , Wang Y , Lu N , Matzuk MM ( 1997 ) Follicle stimulating hormone is required for ovarian follicle maturation but not male fertility . Nature Genetics 15 : 201 –203.
Loumaye E , Engrand P , Howles CM , O’Dea L ( 1997 ) Assessment of the role of serum luteinizing hormone and estradiol response to follicle-stimulating hormone on in vitro fertilization outcome . Fertility and Sterility 67 : 889 –899.
Macnamee MC , Howles CM , Edwards RG , et al . ( 1989 ) Short term luteinising hormone agonist treatment, prospective trial of a novel ovarian stimulation regimen for in vitro fertilisation . Fertility and Sterility 52 : 264 –269.
• Follicle size 14 mm or less: review in 2 or 3 days Follicle size 16 mm or greater: review daily •
Plasma estradiol • Plasma LH •
Review as necessary. •
hCG (Profasi) 10 000 IU or r-hCG (Ovitrelle/Ovidrel 6500IU) by subcutaneous injection when:
Leading follicle is at least 17–18 mm in diameter • Two or more follicles >14 mm in diameter• Endometrium: at least 8 mm in thickness with tril-•aminar “halo” appearance Estradiol levels approx. 100–150 pg/mL per large•follicle Oocyte retrieval scheduled for 34–36 hours post-•hCG .

Chapter 2: Endocrine control of reproduction
27
Regan L , Owen EJ , Jacobs HS ( 1990 ) Hypersecretion of luteinising hormone, infertility, and miscarriage . Lancet 336 : 1141 –1144.
Shenfi eld F ( 1996 ) FSH: what is its role in infertility treatments, and particularly in IVF? Medical Dialogue 471 : 1 –4.
Tavaniotou A , Smitz J , Bourgain C , Devroey P ( 2001 ) Ovulation induction disrupts luteal phase function . Annals of the New York Academy of Sciences 943 : 55 –63.
Telfer EE ( 1996 ) Th e development of methods for isolation and culture of preantral follicles from bovine and porcine ovaries . Th eriogenology 45 : 101 –110.

Chapter
1
28
Gametes and gametogenesis
Gamete precursor cells: primordial germ cells Aft er a blastocyst has implanted in the uterus and begins to diff erentiate into the three primary germ layers, a special population of cells develop as primor-dial germ cells (PGCs). Th ese are destined to become the gametes of the new individual: future reproduc-tion of the organism is absolutely dependent upon the correct development of these unique populations of cells. Th ey originate immediately behind the primitive streak in the extraembryonic mesoderm of the yolk sac; towards the end of gastrulation they move into the embryo via the allantois, and temporarily settle in mesoderm and endoderm of the primitive streak. In humans, PGCs can be identifi ed at about 3 weeks of gestation, close to the yolk sac endoderm at the root of the allantois. Th ese cells have many special properties in terms of morphology, behavior and gene expres-sion, and undergo a number of unique biological processes:
Lengthy migration through the developing • embryo to the gonadal ridge Erasure of epigenetic information from the • previous generation Reactivation of the X chromosome that has been • silenced (Barr body) in XX cells.
Migration of primordial germ cells PGCs proliferate by mitosis, and begin to migrate through the embryonic tissue, completing approxi-mately six mitotic divisions by the time they colonize the future gonad ( Figure 3.1 ).
Proliferation and migration continue for 3–4 weeks in humans, and during their migration the germ cells and the somatic cells interact together via a number of diff erent types of signals. Th e PGCs
move to the inside of the embryo along with the gut to embed in the connective tissue of the hind-gut, migrate through the dorsal mesentery along the hindgut a few days later, and then fi nally populate the gonadal ridge to form the embryonic gonad. Th e tis-sue of the gonadal ridge makes up the somatic (non-gamete) part of the gonads. In humans, PGCs can be seen in the region of the developing kidneys (the mesonephros) approximately 4 weeks aft er fertiliza-tion (gestational age 5–6 weeks), and their migra-tion is completed by 6 weeks of gestation. Primordial gonads can be identifi ed on either side of the central dorsal aorta between 37 and 42 days aft er fertilization (gestational age 8–9 weeks), as a medial thickening of the mesodermal epithelium that lines the coelom (body cavity).
PGC in the mouse
• During their migration in the mouse, the population of PGCs increases from around 100 cells to 25 000 cells by stage 13.5 of embryonic development (E13.5) . The genital ridges may secrete a chemotactic sub-• stance (probably SDF-1, stromal cell derived factor 1 and its receptor CXCR4) that attracts the PGCs: prim-ordial gonadal tissue grafted into abnormal sites within a mouse embryo attracts germ cells to colon-ize it. Experiments using gene knock-out animal models • have identifi ed a number of genes involved in regu-lating the establishment and migration of PGCs, the signals involved in their movement, and their renewal properties (see MacLaren, 2003 ).
Gonadogenesis: from primordial germ cells to gametes Th e primordial gonadal ridges develop on the poster-ior wall of the lower thoracic and upper lumbar regions, and in both sexes this undiff erentiated mesenchymal
• During their migration in the mouse, the populationof PGCs increases from around 100 cells to 25 000 cellsby stage 13.5 of embryonic development (E13.5) . The genital ridges may secrete a chemotactic sub-•stance (probably SDF-1, stromal cell derived factor 1and its receptor CXCR4) that attracts the PGCs: prim-ordial gonadal tissue grafted into abnormal siteswithin a mouse embryo attracts germ cells to colon-ize it. Experiments using gene knock-out animal models• have identifi ed a number of genes involved in regu-lating the establishment and migration of PGCs,the signals involved in their movement, and theirrenewal properties (see MacLaren, 2003 ).
3
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. (©) K. Elder and B. Dale 2011.

Chapter 3: Gametes and gametogenesis
29
tissue forms the basic matrices of the testes and ovaries . At approximately 6 weeks of gestation the developing gonad appears identical in male and female embryos, and remains sexually undiff erentiated for a period of 7–10 days. During this period, groups of cells derived from the columnar coelomic (germinal) epithelium sur-rounding the genital ridge migrate into the undiff eren-tiated tissue as columns to colonize the gonad – these are known as the primitive sex cords . Key morpho-logical changes then start to take place in the gonads, which depend upon whether or not the Sex determining Region Y (SRY) gene on a Y chromosome is expressed in the cells of the sex cords. Th ese morphological changes result in the formation of:
1. Genital ducts • Wolffi an duct = male, precursor of the vas
deferens and epididymis • Müllerian duct = female, precursor of the
uterus, the upper parts of the vagina and the oviducts.
2. Urogenital sinus .
Knock-out mouse technology has identifi ed a number of genes involved in these early stages of gonadogen-esis, some of which are outlined in Figure 3.2 , and sum-marized here:
1. SRY expression is upregulated by only one isoform of Wilms’ tumor gene product WT1(–KTS).
2. Th e WT1(–KTS) isoform also upregulates DAX1 expression (which antagonizes development of Sertoli cells). Th e WT1(–KTS) isoform is therefore considered essential for development of both the male and the female gonad.
3. Th e WT1(+KTS) isoform increases the number of SRY transcripts, and is required for formation of the male gonad.
4. WNT4 acts to repress migration of mesonephric endothelial and steroidogenic cells in the XX gonad, preventing the formation of a male-specifi c coelomic blood vessel and the production of steroids. WNT4 expression is downregulated aft er sex determination in the XY gonad.
5. DAX1 may inhibit SRY indirectly by inhibiting expression of male-specifi c genes that are activated by SF1.
6. SRY upregulates expression of a related transcription factor, SOX9. SOX9 is required for activation of anti-Müllerian hormone (AMH)/Müllerian inhibitory substance (MIS), which causes regression of the female Müllerian duct.
Allantois
E7.5 E8 E9 E10.5
Germcells
Epiblast
Extraembryonictissue
Neural plate tissue
Developinghindgut
Genital ridges (GR)have formed Germ cells migrate towards
GR via dorsal mesentery
Germ cells incorporatedinto hindgut epithelium
Completion of embryonic turning
Germ cells migratethrough hingdut
Figure 3.1 Migration of primordial germ cells in the mouse. (Adapted diagram courtesy of J. Huntriss, University of Leeds. Modifi ed from Starz-Gaiano, M. and Lehmann, R. 2001. Moving towards the next generation. Mechanisms of Development 105: 1–2, with permission from Elsevier Ltd.) PGCs arise at the start of gastrulation, around embryonic Days 7–7.25 (E7–7.5) at the border of the extraembryonic tissue and the epiblast, at the root of the allantois. The PGCs can be identifi ed and distinguished from the surrounding somatic cells by their positive staining for alkaline phosphatase. Expression of the OCT4 transcription factor becomes restricted to PGCs around day E8 and is used as a PGC marker. See color plate section.

Chapter 3: Gametes and gametogenesis
30
7. Dmrt1 is thought to interfere with the action of SOX9. Dmrt1 is a candidate sex-determining gene in birds, carried on their Z chromosome.
Sex determination
A classic experiment by Alfred Jost in the 1940s dem-onstrated that mammalian embryos castrated prior to diff erentiation of the testis appear to develop pheno-typically as females. This established that the female route of sexual development is the default diff erenti-ation pathway, and led the authors to propose the exist-ence of a testis-determining factor (TDF) . This has now been established by experiments on early embryos, and by molecular experiments. Genetic studies also suggest that ovarian diff erentiation and development may be regulated by certain “anti-testis” factors :
In XY humans who carry a duplication of part of the • small arm of the X chromosome (Xp21) (and in XY mice of certain genetic backgrounds), overexpres-sion of the DAX1 gene causes sex reversal; i.e., these
human or mouse individuals develop as females. Therefore, DAX1 can apparently antagonize SRY in a dosage-sensitive manner to cause sex reversal. Wnt4 is also required for female development. • Genetic studies in the mouse show that:
Wnt4 is initially required for the formation of the • Müllerian duct in both sexes In the developing ovary, Wnt4 suppresses the • development of Leydig cells. In Wnt4 mutants, the Müllerian duct is absent, and • the Wolffi an duct develops further.
Wnt4-mutant females activate testosterone biosyn-thesis and become masculinized.
Knock-outs of SF1, Lim-9 and Wnt1 genes develop as phenotypic females, in support of Jost’s proposal.
Development of the testis Aft er the mesonephros has been populated with prim-ordial germ cells to form the genital ridge, the coelomic
A classic experiment by Alfred Jost in the 1940s dem-onstrated that mammalian embryos castrated prior todiff erentiation of the testis appear to develop pheno-typically as females. This established that the female route of sexual development is the default diff erenti-ation pathway, and led the authors to propose the exist-ence of a testis-determining factor (TDF) . This has nowbeen established by experiments on early embryos,and by molecular experiments. Genetic studies alsosuggest that ovarian diff erentiation and developmentmay be regulated by certain “anti-testis” factors :
In XY humans who carry a duplication of part of the•small arm of the X chromosome (Xp21) (and in XYmice of certain genetic backgrounds), overexpres-sion of the DAX1 gene causes sex reversal; i.e., these
human or mouse individuals develop as females.Therefore, DAX1 can apparently antagonize SRY in adosage-sensitive manner to cause sex reversal. Wnt4 is also required for female development.• Genetic studies in the mouse show that:
Wnt4 is initially required for the formation of the•Müllerian duct in both sexes In the developing ovary, Wnt4 suppresses the• development of Leydig cells.In Wnt4 mutants, the Müllerian duct is absent, and•the Wolffi an duct develops further.
Wnt4-mutant females activate testosterone biosyn-thesis and become masculinized.
Knock-outs of SF1, Lim-9 and Wnt1 genes developas phenotypic females, in support of Jost’s proposal.
Female (XX)
BIPOTENTIAL GONAD
Gonaddevelops
Factors essentialfor development
of bipotential gonad
SF1
LIM1
GATA4
EMX2WT1
WT1(–KTS)
WNT4
AMH/MIS
Sox9
Regression ofMüllerian duct
activationrepression
KEY:
GonaddevelopsSox3?
SRY
Male (XY)
Gonadaldifferentiation
occurs
DAX1
WT1(–KTS)
1
WT1(–KTS)
4
5
6
2
SEX DETERMINATION GONADAL DEVELOPMENT
OVARYDETERMINING
FACTORS
GATA4DAX1
WT13
TESTISDETERMININGFACTORS e.g
DMRT1
Figure 3.2 Genes involved in gonadogenesis; key points are circled, outlining the complex regulatory molecular pathways involved (Adapted from Clarkson MJ, Harley VR, 2002)

Chapter 3: Gametes and gametogenesis
31
epithelium proliferates at a faster rate in male than in female gonads, and the cells penetrate deep into the medullary mesenchyme to form the testis cords. Two dif-ferent testicular compartments are formed: the testicu-lar cords, and the interstitial region. Expression of the SRY gene initiates diff erentiation of Sertoli cells, and the developing Sertoli cells produce a growth factor, fi bro-blast growth factor 9 (FGF-9) that is necessary for forma-tion of the testicular cords. At 7–8 weeks of gestation, the testicular cords (precursor of the seminiferous tubules) can be seen in histological sections as protrusions of the cortical epithelium into the medulla; animal experiments indicate that germ cells are not involved in this process.
Sertoli cells cluster around the germ cells; • peritubular myoid cells surround the clusters, and deposit the basal lamina. Sertoli cells secrete AMH /MIS , which suppresses • the default pathway that would develop Müllerian ducts as precursors of female sexual anatomy. Th e Sertoli cells continue to secrete AMH throughout fetal and postnatal life until the time of puberty, when the levels drop sharply. Leydig cells remain in the interstitial region, close • to blood and lymphatic systems, and they actively secrete androgens from at least 8–10 weeks of gestation. Th is capacity to secrete testosterone is essential for continued testicular development, and, ultimately, for the establishment of the male phenotype. Testosterone causes growth and diff erentiation of • the Wolffi an duct structures (precursor of the male sexual anatomy). Dihydrotestosterone (a metabolite of testosterone) • induces virilization of the urogenital sinus and the external genitalia.
Th e Müllerian duct then regresses, and the Wolffi an duct develops further.
By 16–20 weeks of fetal life, Sertoli cells and rela-tively quiescent prospermatogonial cells lie on a base-ment membrane within seminiferous cords; these are within a vascularized stroma that also contains con-densed Leydig cells, and the entire structure is enclosed within a fi brous capsule, the tunica albuginea. Th e testes gradually increase in size until the time of puberty, and with the onset of puberty they begin to rapidly enlarge:
Th e solid cords canalize to give rise to tubules, • which eventually connect to the rete testis, the vasa eff erentia, and then the epididymis.
Leydig cells signifi cantly increase their endocrine • secretion, and intratubular Sertoli cells also increase in size and activity. Prospermatogonial cells in the cords now line • the seminiferous tubules as spermatogenic epithelium, and begin to divide by mitosis.
Testicular descent Th e testes develop initially in the upper lumbar region of the embryo, and gradually migrate during fetal life through the abdominal cavity and over the pelvic brim. Th is descent is infl uenced by hormones secreted by the Leydig cells, and involves two ligamentous struc-tures: the suspensory ligament at the superior pole, and the gubernaculum at the inferior pole of the testis. As the fetal body grows in size, the suspensory ligament elongates and the gubernaculum does not, so that the position of the testis becomes localized to the pel-vis. Between weeks 25 and 28 of pregnancy, the testes migrate over the pubic bone, and reach the scrotum via the inguinal canal by weeks 35–40. As a result of their external position outside the body cavity, the tempera-ture of the testes is approximately 2°C below body tem-perature, optimal for spermatogenesis.
Genetic control of testis development
• SRY, SOX9, WT1, XH2, SF1, and DAX1 are known to be involved in the control of testis determination. Many of these genes have been identifi ed through analysis of cases of sex reversal. The SRY gene is a key switch in male sexual diff eren-• tiation; it acts only briefl y in male embryos, to initiate diff erentiation of the Sertoli cells in the somatic cells of the genital ridge. SRY may function either : • • As a transcriptional repressor to repress activa-
tion of the genes that cause diff erentiation of the ovary
• As a repressor of the factors that repress testis development
• Synergistically with SF1 to activate SOX9.
Th e adult testes contain approximately 200 m of seminiferous tubule, forming the bulk of the volume of the testis. Th ese tubules are the site of spermato-genesis . Th e round tubules are separated from each other by a small amount of connective tissue that con-tains, in addition to blood vessels, a few lymphocytes, plasma cells and clumps of interstitial Leydig cells. Th e tubules are lined by spermatogenic epithelium, which
• SRY, SOX9, WT1, XH2, SF1, and DAX1 are known tobe involved in the control of testis determination.Many of these genes have been identifi ed throughanalysis of cases of sex reversal. The SRY gene is a key switch in male sexual diff eren-•tiation; it acts only briefl y in male embryos, to initiatediff erentiation of the Sertoli cells in the somatic cellsof the genital ridge. SRY may function either : •• As a transcriptional repressor to repress activa-
tion of the genes that cause diff erentiation of the ovary
• As a repressor of the factors that repress testisdevelopment
• Synergistically with SF1 to activate SOX9.

Chapter 3: Gametes and gametogenesis
32
is made up of spermatogonia at diff erent stages of mat-uration – a cross-section of any normal seminiferous tubule reveals four or fi ve distinct generations of germ cells. Th e younger generation cells are on the basement membrane, and the more diff erentiated cells approach the lumen of the tubule. Th is growth pattern has a wavelike cycle with intermingling of diff erent stages that lie close to each other – any single cross-section of the tubule does not always reveal all generations of spermatogenesis . Th e tubules rest on a delicate anuclear basement membrane that in turn lies on a connective tissue layer, the tunica propria. Th e supporting Sertoli cells, which are believed to nourish the germ cells, form a continuous layer connected by tight junctions. Th ese large polymorphous cells have large, pale nuclei, and abundant cytoplasm that extends from the periphery of the tubule to the lumen, stretching through the lay-ers of developing germ cells. Mature spermatozoa can be seen attached to and surrounding the Sertoli cells prior to their release ( Figure 3.3 ). A wave of sperm-atogenesis passes along the tubule, and the process of development from spermatogonium to spermatozoon takes approximately 65 days. A transverse cross-sec-tion through the human testis shows tubules contain-ing cells at many diff erent stages in spermatogenesis (in contrast to the rat testis, where every tubule has cells at the same stage). In humans, many seminiferous tubules
can be seen that are apparently without spermatocytes and spermatids, a phenomenon that may contribute to the relatively poor effi ciency of spermatogenesis.
Sperm released into the lumen of the seminifer-ous tubules pass via the rete testis through the ductuli eff erentia into the caput epididymis. Th ey traverse the epididymis over a period of 2–14 days, undergoing a number of changes in preparation for fertilization, and are then stored sequentially in the cauda, vas, seminal vesicles and ampullae prior to ejaculation. Th e sem-inal vesicles, prostate and urethral glands add glandu-lar secretions to the sperm at the time of ejaculation. Figure 3.4 illustrates the anatomy of the adult mam-malian testis .
Spermatogenesis Th e process of spermatogenesis can be divided into three phases, and each phase is associated with a spe-cifi c type of germ cell: 1. Proliferation
(spermatocytogenesis): spermatogonia 2. Reduction division (meiosis): spermatocytes 3. Diff erentiation (spermiogenesis): spermatids
In the fetal testis, primordial germ cells diff erentiate into spermatozoal stem cells, type A (A0) spermatogonia.
Adluminalcompartment Spermatozoon
Spermatid(n)
Spermatocyte(2n)
Basal compartment containingspermatogonia
Sertoli cell Figure 3.3 Spermatogenesis in the mammal. Maturation and modeling of the male gamete is regulated by the Sertoli cell. Modifi ed after Johnson ( 2007 ).

Chapter 3: Gametes and gametogenesis
33
Th ese stem cells line the basement membrane of the seminiferous tubules, have large spherical or oval nuclei, and are connected to each other via intercel-lular bridges to form a germ cell syncytium. Th ey are in contact with Sertoli cells, which extend from the epithelium into the lumen of the tubules. At puberty, the spermatogonia start to proliferate by mitoses; this is followed by meiosis and a gradual reorganization of cellular components and a loss of cytoplasm.
Spermatocytogenesis
At intervals aft er puberty, stem cells in the • germinal epithelium of the seminiferous tubules ( type A spermatogonia ) replicate their DNA and divide by mitosis. Each mitotic division produces two cells: another • type A spermatogonium, and a second cell, type B spermatogonia ; these move into the adluminal compartment and start their diff erentiation by entering into meiosis .
Meiosis In the adluminal compartment, the cells undergo two meiotic divisions to form two daughter second-ary spermatocytes initially, and eventually four early spermatids. Th rough a series of diff erent phases, mei-osis (reduction division) converts diploid stem cells (spermatogonia) containing 46 chromosomes into hap-loid gametes, with 23 chromosomes. In the fi rst phase of meiosis, type B spermatogonia (2n:2c) become pri-mary spermatocytes (1n:2c). Th ese cells divide again, to become secondary spermatocytes (1n:1c). Th e cells
go through this stage quickly, and complete the second meiotic division. Aft er the second meiotic division, the cells are known as spermatids. Th ese cells must now go through a process of maturation (spermiogenesis) in order to fi nally emerge as mature spermatozoa (1n:1c).
Spermiogenesis Spermatid diff erentiation occurs in four stages ( Figure 3.5 ): 1. Golgi phase 2. Cap phase 3. Acrosomal phase 4. Maturation phase.
Spermatid nuclei now contain haploid sets of chromo-somes. Th eir autosomes continue to direct the synthe-sis of low levels of rRNA, mRNA and proteins as they enter into their prolonged phase of terminal diff er-entiation, spermiogenesis. During this phase, round spermatid cells are converted into elongated sperm cells with a condensed nucleus and a fl agellum. Th ey do not divide again, either by mitosis or meiosis, but must diff erentiate to acquire functions that will allow them to traverse the female tract and fertilize an oocyte. Th is diff erentiation process takes approximately 2 weeks in most species, and follows well-defi ned stages: 1. Spermatid DNA becomes highly condensed, and
somatic histones are replaced with protamines. 2. Th e acrosome, a sac containing enzymes necessary
for oocyte penetration, is constructed from Golgi membranes.
Efferent ducts
Spermatic chords
Caput epididymis(head)
Blood supply
Septum
Body of epididymis(Corpus epididymis)
Ductus deferens
Rete testis
Seminiferoustubule
Tunica albuginea
Tail of epididymis(Cauda epididymis)
Scrotal cavity
Scrotum
Figure 3.4 Anatomy of the adult mammalian testis. (Drawing adapted from a number of sources.)

Chapter 3: Gametes and gametogenesis
34
3. Cytoplasmic reorganization gives rise to the midpiece, which contains mitochondria and associated control mechanisms necessary for motility.
4. Th e fl agellar apparatus (tail) is formed, which will make the cells motile.
5. A residual body casts off excess cytoplasm.
Sperm modeling is probably regulated by the Sertoli cells, and the cells are moved to the center of the tubu-lar lumen as spermatogenesis proceeds. Th e rate of pro-gression of cells through spermatogenesis is constant, and is not aff ected by external factors such as hormones. Th e timing of stored mRNA translation is a major point of control: for example, the protamine1 gene is tran-scribed in round spermatids, and the resulting mRNA is stored for up to 1 week before it is translated in elongat-ing spermatids. Other mRNAs are stored for only hours or a few days, indicating that there must be a defi ned temporal program of translational control.
Sertoli cells are joined by tight junctions, and act • as nurse cells during spermatogenesis. Tight junctions restrict the passage of substances • from the blood to the lumen of the seminiferous tubules and therefore form a blood–testis barrier. Th is barrier protects sperm from antibodies circulating in the bloodstream.
Molecular features of spermatogenesis
• The trigger that determines which spermatogonia become committed to meiosis is not known. DNA is transcribed from both diploid (proliferative • type A (A0) spermatogonia) and haploid (committed
type B [A1] spermatogonia) genomes throughout the process. Only type B spermatogonia undergo diff erentiation • into spermatozoa, and the vast majority of the germ cell cytoplasm is lost during the terminal stages of diff erentiation, when the spermatids condense into spermatozoa. The reduction process that generates haploid sperm • cells takes at least 65 days in humans, and involves six successive stages over four consecutive sperma-togenic cycles. Note the nomenclature relating to chromosome • complement (n) and DNA copy number (c). 1c is the DNA copy number of a haploid gamete, and no gam-ete is ever tetraploid.
Epididymal maturation Mammalian spermatozoa leaving the testis are not capable of fertilizing oocytes. They gain this abil-ity while passing down the epididymis, a process known as epididymal maturation . The epididymis is divided into different regions: the caput is the upper third, formed by efferent ductules that are lined by pseudostratified columnar ciliated epithelium (such as is found in nasal and bronchial passages – patients with upper epididymal obstruction often have asso-ciated nasal or respiratory problems, as in muco-viscidosis, Young’s syndrome ). The vasa efferentia tubules unite to form the single coiled tubule of the corpus, which has flatter, non-ciliated epithelium and microvilli on the luminal surface. It starts to form a muscular wall towards the cauda, where the lumen is wider, and spermatozoa can be stored prior to ejaculation.
• The trigger that determines which spermatogoniabecome committed to meiosis is not known. DNA is transcribed from both diploid (proliferative•type A (A0) spermatogonia) and haploid (committed
type B [A1] spermatogonia) genomes throughoutthe process. Only type B spermatogonia undergo diff erentiation•into spermatozoa, and the vast majority of the germcell cytoplasm is lost during the terminal stages of diff erentiation, when the spermatids condense intospermatozoa. The reduction process that generates haploid sperm•cells takes at least 65 days in humans, and involvessix successive stages over four consecutive sperma-togenic cycles. Note the nomenclature relating to chromosome•complement (n) and DNA copy number (c). 1c is theDNA copy number of a haploid gamete, and no gam-ete is ever tetraploid.
ROUND
Ax Go
z
z
K
M M
Ak1 2 3 4 5 6 7 8
K
MtStAn
AxAx
SKM
RF
An
Mt
K
K
Ak Ak
F
RF
Mt
SK RF
M
FAn
I
M
CervHeadAk
ELONGATING ELONGATED MATURE
Figure 3.5 Developing sperm. (Courtesy of M. Nijs and P. Vanderzwalmen, Belgium.) A = acrosome; An = annulus; Ax = axoneme; C = centriole; F = fl owerlike structures; Fs = fl agellar substructures; M = mitochondria; Mp = middle piece; Mt = manchette; Ne = neck; PP = principal piece; R = ring fi bers; Sb = spindle-shaped body.

Chapter 3: Gametes and gametogenesis
35
During its journey through the diff erent regions of the epididymis, the head of the spermatozoon acquires the ability to interact with the zona pellucida , with an increase in net negative charge. Many antigens with a demonstrable role in oocyte binding and fusion are synthesized in the testis as precursors, and then activated at some point in the epididymis either through direct biochemical modi-fi cation, through changing their cellular localization, or both. Examples of such antigen processing include a membrane-bound hyaluronidase, fertilin, proacrosin, 1,4-galactosyltransferase (GalTase) and putative zona lig-ands sp56 and p95. Th e terminal saccharide residues of membrane glycoproteins and lipids also undergo changes in their physical and chemical composition.
Although all the necessary morphological structures for fl agellar activity are assembled during spermiogen-esis , testicular spermatozoa are essentially immotile, even when washed and placed in a physiological solu-tion. Spermatozoa from the caput epididymis begin to display motility, and by the time they reach the cauda they are capable of full progressive forward motility. Demembranation and exposure to ATP, cAMP and Mg 2+ triggers movement, which suggests that the ability to move is probably regulated at the level of the plasma membrane. Transfer of a forward motility protein and carnitine from the epididymal fl uid are believed to be important for the development of sperm motility. Since the osmolality and chemical composition of the epididy-mal fl uid varies from one segment to the next, it may be that the sperm plasma membrane is altered stepwise as it progresses down the duct, and motility is controlled by an interplay between cAMP , cytosolic Ca 2+ and pH. During maturation, the spermatozoa use up endogen-ous reserves of metabolic substrates, becoming depend-ent on exogenous sources such as fructose; at this point they shed their cytoplasmic droplet.
Pathology aff ecting spermatogenesis
• A number of diff erent pathologies can disrupt the orderly pattern of spermatogenesis, causing imma-ture forms, especially spermatocytes to slough into the tubular lumen. Less frequently, maturation may proceed to the spermatid stage and be arrested there. Any lesion that causes generalized arrest of matur-• ation, or a mixture of maturation arrest and atrophy to a stage preceding spermiogenesis, will result in azoospermia. The tubular epithelium is very sensitive to toxins and • to ischemia; damage may result in partial, focal or total obliteration of the spermatogenic epithelium,
including the Sertoli cells, while the Leydig cells remain functionally normal. In cases of severe injury, the tubules may be totally • destroyed and become hyalinized, or may be replaced by fi brous tissue. Since the whole tubule is destroyed, this disorder is associated with a much reduced testis size, with absence of Sertoli cells resulting in raised serum FSH. Focal lesions can cause oligospermia of varying • severity, and patients with focal lesions may have normal levels of FSH in their serum.
DNA packaging in sperm The amount of DNA in the sperm nucleus (approxi-mately 1 m in length) has to be packaged into a vol-ume that is typically less than 10% of the volume of a somatic cell nucleus; a different mechanism of pack-aging is required, as illustrated in Figure 3.6 .
Somatic cell DNA is packaged into nucleosomes • by a process of primary compaction that uses histones. A 10 nm fi ber is supercoiled into the 30 nm solenoid, and supercoiled again into loops (A–D). Th ese loops are the major structural form of interphase chromatin. During spermatogenesis, DNA is initially • packaged by histones (as in A–D) but following meiosis, at the secondary spermatocyte stage of spermiogenesis, histones are replaced first by transition proteins and then by protamines (G). The solenoid structure is replaced by torroids (doughnut shapes), which are in turn supercoiled into torroidal loops. This highly compacted structure shuts down transcription during spermiogenesis. The loop domains drawn in E and J represent the chromatin state in the interphase somatic cell nucleus (E) and the sperm nucleus (J). Sperm appear poised for transcription.
Gene expression during spermatogenesis Gene expression during spermatogenesis can be subdi-vided into two distinctive phases: 1. Prior to meiosis, all stages up to and including the
completion of telophase: diploid cells. 2. During spermiogenesis: late secondary
spermatocytes are haploid cells, and the developmental process from this stage onwards is referred to as spermiogenesis.
• A number of diff erent pathologies can disrupt the orderly pattern of spermatogenesis, causing imma-ture forms, especially spermatocytes to slough into the tubular lumen. Less frequently, maturation may proceed to the spermatid stage and be arrested there. Any lesion that causes generalized arrest of matur-•ation, or a mixture of maturation arrest and atrophy to a stage preceding spermiogenesis, will result in azoospermia. The tubular epithelium is very sensitive to toxins and •to ischemia; damage may result in partial, focal or total obliteration of the spermatogenic epithelium,
including the Sertoli cells, while the Leydig cellsremain functionally normal. In cases of severe injury, the tubules may be totally• destroyed and become hyalinized, or may bereplaced by fi brous tissue. Since the whole tubuleis destroyed, this disorder is associated with amuch reduced testis size, with absence of Sertolicells resulting in raised serum FSH. Focal lesions can cause oligospermia of varying•severity, and patients with focal lesions may havenormal levels of FSH in their serum.

Chapter 3: Gametes and gametogenesis
36
Genes are expressed from both the diploid and the haploid genomes. DNA transcription is oft en coordi-nated with mRNA translation into its protein product (e.g., histones, X-linked lactate dehydrogenase). In spermiogenesis, however, transcription may be shut down well before the protein appears, i.e., the mRNA is translated later (e.g., PGK2, acrosin). As spermato-genesis progresses, the transcripts encoding the same protein diff er in size, due to alterations in the length of the mRNA polyA tail (a similar phenomenon occurs in oogenesis , as described later).
Control of gene expression during spermatogenesis
Betw• een primitive spermatogonial and fi nal mature spermatozoa , cellular chromatin is restructured so that certain genes are repressed, potentiated, or potentiated and transcribed. Phosphoglycerokinase 1 gene (PGK1), an essen-• tial glycolytic enzyme, lies on the X chromosome, and this gene is highly expressed, potentiated and transcribed early in spermatogenesis. As the cells progress into meiosis, the X chromosome becomes progressively inactivated, and during spermiogen-esis expression of PGK1 is replaced by expression of an autosomal homologue, PGK2. During spermiogenesis (the haploid stages of • spermatogenesis), cellular histones are replaced fi rst by testis-specifi c histones and then by the transition protein TNP2 and the protamines PRM1 and PRM2. This substitution is a prerequisite for the extremely compact packaging of sperm DNA. These genes are located on chromosome 16.
• Not all histones are replaced. Human sperm retain approximately 15–20% of their chromatin in a nucleosomal confi guration, and we now know that mature sperm cells retain a complex repertoire of mRNAs that may be involved in embryogenesis.
Th e ultimate aim of the male reproductive system is to parcel the male genetic package, a set of 23 chro-mosomes, into the head of a single spermatozoon, and deliver this to the female reproductive tract, in the right place at the right time. However, in order to fertilize the oocyte and initiate embryonic development, the spermatozoon must also contribute two epigenetic fac-tors: an oocyte activating factor and the centrosome or cell division mechanism (see Chapter 4 ).
Development of the ovary In female embryos, primordial germ cells containing two X chromosomes migrate from the genital ridge to the primordial gonad, and these are known as oogo-nia . Th e sex cords, instead of penetrating deeply into the genital ridge as in males, condense as small clus-ters around the PGCs, and these clusters of cells initi-ate the formation of primordial follicles ( Figure 3.7 ). Cells of the cortical sex cords will form the somatic components of the follicle: granulosa, theca, endothe-lial cells and supporting connective tissue. Once they reach the gonadal ridge (approximately Days 25–30), the oogonia start to replicate by mitosis for a limited period. Cells from the mesonephros invade to form the ovarian medulla, forcing the germ cells towards
Betw• een primitive spermatogonial and fi nal maturespermatozoa , cellular chromatin is restructured sothat certain genes are repressed, potentiated, or potentiated and transcribed. Phosphoglycerokinase 1 gene (PGK1), an essen-•tial glycolytic enzyme, lies on the X chromosome,and this gene is highly expressed, potentiated andtranscribed early in spermatogenesis. As the cellsprogress into meiosis, the X chromosome becomesprogressively inactivated, and during spermiogen-esis expression of PGK1 is replaced by expression of an autosomal homologue, PGK2. During spermiogenesis (the haploid stages of •spermatogenesis), cellular histones are replaced fi rstby testis-specifi c histones and then by the transitionprotein TNP2 and the protamines PRM1 and PRM2.This substitution is a prerequisite for the extremelycompact packaging of sperm DNA. These genes arelocated on chromosome 16.
• Not all histones are replaced. Human sperm retainapproximately 15–20% of their chromatin in anucleosomal confi guration, and we now know thatmature sperm cells retain a complex repertoire of mRNAs that may be involved in embryogenesis.
FTransitionproteins
DNA packed byhistones
DNA packed byhistones
Key:-
Histone octamer Solenoid
AG = Active gene Orl = Origin of DNA replication
Solenoid loop Chromatin in somatic nucleus
AGIG
Orl
DNA packed byprotamines Doughnut Doughnut loop Chromatin in sperm nucleus
DNA loopJ
Orl
I
A B C D E
H
H
P= Histone = Protamine IG = Inactive gene
P P P
G
H H H
H H H
Som
atic
cel
lS
perm
Figure 3.6 DNA packaging in somatic cells and spermatozoa. (Image adapted from Ward, 1993.) See color plate section.

Chapter 3: Gametes and gametogenesis
37
the ovarian cortex. Whereas in male embryos sperm-atogonia do not start to enter meiosis until the onset of puberty, in females the oogonia start to enter into their fi rst meiotic division around the twelft h week of gestation, at the end of the fi rst trimester. In humans, the population of oogonia is estimated to increase from a pool of around 600 000 at 8 weeks to a max-imum of 6–8 million at 16–20 weeks. At this stage they become primary oocytes, and do not replicate further by mitosis. Oocytes that are not incorporated into fol-licles degenerate, and thus the number of oocytes is then reduced to around 1–2 million at birth, when the ovary is now populated with its full complement of oocytes.
Aft er the oogonia enter meiosis I, they arrest in the diplotene stage of prophase I, aft er chromatid exchange and crossing-over (diakinesis) have taken place – the last phase of prophase I (see Chapter 1 , Figure 1.9 ). Th ese arrested oocytes are said to be in the dictyate (germinal vesicle) stage. Th e chromosomes disperse, and appear as visible chromosomal threads packaged within a large nucleus, the germinal vesicle (GV). Th e fi rst meiotic prophase stage can be seen at around 9–10 weeks, and diplotene stage chromosomes are apparent around 16 weeks, during the second trimester of preg-nancy. Th e oocytes remain arrested at this stage until the onset of ovulatory cycles at puberty: subsequent developmental stages that lead to the resumption of meiosis are not completed unless the Graafi an (antral) follicle is recruited aft er puberty. Th e process of oogen-esis , from primordial germ cell to pre-ovulatory oocyte,
takes a minimum of 11 years; human oocytes complete meiosis only aft er fertilization.
Th e oogonia within the embryonic ovary are ini-tially arranged into clusters called syncytia , which are connected by intercellular bridges. Organelles, mitochondria and other cellular factors are probably exchanged through these connections. Th ese syncytia are programmed to break down on a large scale dur-ing fetal life, and this is followed by the formation of primordial follicles. A single layer of pre-granulosa cells surrounds a single oogonium; once a complete cell layer has been formed around individual oocytes, the surrounding stromal cells secrete type IV collagen, laminin and fi bronectin. Th ese proteins form a thin basement membrane around each cluster of cells, and a discrete population of primordial follicles is formed. Each follicle has an oocyte arrested in prophase I of meiosis, surrounded by a single layer of fl attened stro-mal pre-granulosa cells that are linked to the oocyte by gap junctions and other cellular connections. Th e primordial follicles become localized to the peripheral region of the ovarian cortex, and remain there in a qui-escent state for many years ( Figure 3.8a ). In this pool of follicles, each will either undergo a phase of growth and development that lasts approximately 6 months, or will become atretic and die. When they resume their growth aft er puberty, usually only one oocyte matures and is ovulated per month for the remaining 35 or so years of the reproductive lifespan ( Figure 3.8b ). Oocytes must complete their growth phase and resume meiosis before they can be fertilized.
A
PGC
G
E F
M M
V
Ad
2
3
1+
+
+ ––
–
–
–
–
–
––
–
4
C
–
Figure 3.7 Development of the human ovary from PGC. (With per-mission from Gosden, R. 1995. Ovulation 1: Oocyte development throughout life, in J.G. Grudzinskas, Jurgis Gediminas Grudzinskas, John Yovich (eds.) Gametes: The Oocyte . Cambridge: Cambridge University Press.)
PGCs travel along the gut (G) mesentery (1) to the gonadal ridge (2), and after proliferation and migration become associated with cortical cords (C, 3). They begin meiosis and become enveloped within follicles (F, 4). Ad = adrenal gland; A = aorta; V = cardinal vein; E = coelomic epithelium; M = mesonephric tubules and duct.

Chapter 3: Gametes and gametogenesis
38
Ovarian reserve
Primordial follicles are the most abundant follicle type within the adult ovary, but there is a high rate of wastage. From around Day 100 of fetal life onwards, oocytes that have arrested in meiotic prophase start to undergo atresia, and this continues throughout fetal and neonatal life. This programmed elimination of germ cells may be associated with a redistribution of organelles (e.g., mitochondria) in order to provide optimal function for the remaining oocytes. Pre-granulosa cells may be involved in this degenerative process. In the mouse, around 70% of oogonia are lost by apoptosis upon entry into meiosis; in humans, the population is reduced to approximately 1–2 million by birth. This pool of oocytes, (the ovarian reserve) was traditionally viewed as the fi nite resource of oocytes that dictates the reproductive lifespan of the indi-vidual ( Figure 3.9 ). However, this dogma has recently been challenged (Johnson et al ., 2005).
Follicle development Formation of primordial follicles In humans, the fi rst primordial follicles can be seen during the fourth month of fetal gestation, and they begin to grow at approximately 20 weeks of fetal life, under the infl uence of gonadotropins. At this stage the oogonia are still active, before their arrest at the dicty-ate stage in prophase 1. Th eir pre-granulosa cells enter a period of quiescence, and cell proliferation will not resume until the primordial follicle begins to grow, oft en months or years aft er it was formed. Th e primor-dial follicles are fi rst established in the medullary region of the ovary, and they continue their development in the more peripheral parts (cortex). During the growth phase, the follicle develops morphologically, acquir-ing a theca interna containing steroidogenic cells, and a theca externa of connective tissue cells forming its
Primordial follicles are the most abundant follicletype within the adult ovary, but there is a high rate of wastage. From around Day 100 of fetal life onwards,oocytes that have arrested in meiotic prophase startto undergo atresia, and this continues throughoutfetal and neonatal life. This programmed eliminationof germ cells may be associated with a redistributionof organelles (e.g., mitochondria) in order to provideoptimal function for the remaining oocytes. Pre-granulosa cells may be involved in this degenerativeprocess. In the mouse, around 70% of oogonia are lostby apoptosis upon entry into meiosis; in humans, thepopulation is reduced to approximately 1–2 million bybirth. This pool of oocytes, (the ovarian reserve) wastraditionally viewed as the fi nite resource of oocytesthat dictates the reproductive lifespan of the indi-vidual ( Figure 3.9 ). However, this dogma has recentlybeen challenged (Johnson et al ., 2005). l
Event
(a)Size
Mitosis
Initiationof
meiosis
35 µm
45–200 µm
200–500 µm
Growth
Meiosis I
>6000 µm
Growth/Maturationof Graafian follicle
Antral cavity forms
1º then 2º follicles
Primordial follicle
Diploid oocyte
Oogonia
PGC
ADULT,POST-PUBERTY
CHILD
FETUS
Mature GV oocyte
MII arrested2º oocyte
Expanded mucifiedcumulus cells
Meiosis IIonly if
fertilized
Ovulation
Primaryoocyte
prophase I arrestedFirst meiotic arrest
Figure 3.8 (a) Schematic diagram of oocyte and follicular development from prenatal through to adult life. (b) Schematic diagram of preo-vulatory antral follicle.
(b)

Chapter 3: Gametes and gametogenesis
39
outer layers. Th e basement membrane around it must either expand or be remodeled to adjust to its increas-ing size, and it becomes a dynamic system that nurtures the oocyte, responding to endogenous and exogenous infl uences via autocrine and paracrine eff ects. Follicular development is regulated by the oocyte itself, in com-bination with numerous cell interactions. A number of key molecules involved in the regulation have been identifi ed, products of genes that are expressed specif-ically in oocytes: FIGalpha/FIGLA, GDF-9, BMP-6 and BMP-15, AMD, cKit, Kit ligand, etc.
Primordial follicles remain in their arrested state for up to 50 years, waiting for a signal to resume development. Aft er puberty, a few primordial folli-cles become recruited to the growth phase every day, and these then go through three phases of develop-ment: primary or preantral, secondary or antral (also known as Graafi an ), and fi nally, preovulatory ( Figure 3.8 ). As described below, the follicular cells produce growth factors and hormones, and also provide phys-ical support, nutrients (such as pyruvate), metabolic precursors (such as amino acids and nucleotides ) and other small molecules that can equilibrate between the two compartments.
Follicular cells
The mass of granulosa cells associated with the oocyte from the antral follicle stage until after fertilization is
known as the cumulus oophorus, a complex tissue that is unique to eutherian mammals.
Cumulus cells contribute to the intrafollicular envir-• onment of the developing oocyte, and the oocyte and its surrounding cells are in close association; electron microscopy shows gap junctions between the apposing membranes. In later stages of growth the oocyte plasma mem-• brane increases in surface area and is organized into long microvilli, presumably required for an increase in transmembrane transport. Under the control of the FIGalpha gene, the oocyte secretes a dense fi brillar material that forms a 5–10 μm layer around the female gamete, called the zona pellucida ( Figure 3.11 ). At this stage, follicle cells remain in contact with the oocyte by means of long interdigitating microvilli, which gives a striated image under the light microscope: this is known as the zona radiata . Cumulus cells express the ganglioside GM3 which • has been implicated in cell recognition, diff eren-tiation and signaling. Blocking the gap junctions interferes with transmission or action of molecules such as 2-deoxyglucose, transforming growth factor alpha (TGF-α) and mitogenic agents on the oocyte. In many species (but not in humans) physically • removing the cumulus cells can inhibit oocyte mat-uration . Signaling between oocyte and cumulus occurs in both directions, and cumulus cells express growth factor receptors and the mRNA for a number of growth factors. They are also a source of prostag-landins , and express angiogenic factors (vascular endothelial growth factor, VEGF) which may have a role in neovascularization of follicles and angiogen-esis at the implantation site of the embryo.
The mass of granulosa cells associated with the oocyte from the antral follicle stage until after fertilization is
known as the cumulus oophorus, a complex tissuethat is unique to eutherian mammals.
Cumulus cells contribute to the intrafollicular envir-•onment of the developing oocyte, and the oocyteand its surrounding cells are in close association;electron microscopy shows gap junctions betweenthe apposing membranes. In later stages of growth the oocyte plasma mem-•brane increases in surface area and is organized intolong microvilli, presumably required for an increasein transmembrane transport. Under the controlof the FIGalpha gene, the oocyte secretes a densefi brillar material that forms a 5–10 μm layer aroundthe female gamete, called the zona pellucida ( Figure3.11 ). At this stage, follicle cells remain in contactwith the oocyte by means of long interdigitatingmicrovilli, which gives a striated image under thelight microscope: this is known as the zona radiata . Cumulus cells express the ganglioside GM3 which• has been implicated in cell recognition, diff eren-tiation and signaling. Blocking the gap junctionsinterferes with transmission or action of moleculessuch as 2-deoxyglucose, transforming growth factoralpha (TGF-α) and mitogenic agents on the oocyte. In many species (but not in humans) physically•removing the cumulus cells can inhibit oocyte mat-uration . Signaling between oocyte and cumulusoccurs in both directions, and cumulus cells expressgrowth factor receptors and the mRNA for a numberof growth factors. They are also a source of prostag-landins , and express angiogenic factors (vascularendothelial growth factor, VEGF) which may have arole in neovascularization of follicles and angiogen-esis at the implantation site of the embryo.
Data (o) and mean from Faddy–Gosden(1996) model (__)
107
106
105
104
103
102
101
0 10 20 30 40 50Age (years)
Num
ber
of fo
llicl
es
Figure 3.9 Variation in total numbers of follicles in human ovaries from neonatal age to 51 (Reproduced from M.J. Faddy et al . 1996 Ovary and ovulation: A model conforming the decline in follicle numbers to the age of menopause in women. Human Reproduction 11.7, with permission from Oxford University Press.)
Figure 3.10 Cumulus–cell interactions. Scanning electron micrograph of the surface of an unfertilized metaphase II human oocyte, with the zona pellucida (zp) and cumulus cells (cc) partially dissected to demonstrate the microvillar organization of the plasma membrane (pm). (From Dale 1996)

Chapter 3: Gametes and gametogenesis
40
• The cumulus cells become polarized during oocyte maturation , and begin to secrete a hyaluronic acid extracellular matrix.
Follicular development after puberty Very small follicles have no independent blood sup-ply; in medium-sized follicles, an anastomotic network of arterioles appears just outside the basement mem-brane. Th is network becomes more extensive as the follicle grows, and each ripe preovulatory follicle has its own rich blood supply. Changes in hormone levels during folliculogenesis aff ect the composition of the follicular fl uid , which is probably the source of energy substrates for the developing oocyte. Th e oocyte plays a fundamental role in follicle development, and controls the diff erentiation of follicular granulosa cells. In order to acquire its necessary developmental competence, there must be communication between the oocyte and granulosa cells.
Follicle recruitment: from primordial to preantral (primary) follicle
In humans the number of follicles recruited into devel-opment at any given time ranges between 2 and 30, related to age. Th e precise mechanisms that regulate the initiation of primordial follicle growth are not well
understood, and two possible mechanisms have been proposed: (a) Growth initiation is a pre-programmed feature
of the ovary: the fi rst primordial follicles to enter the growth phase are those that contain the fi rst oocytes to enter meiosis in the human prenatal ovary (or prenatal/early postnatal mouse ovary (Henderson and Edwards, 1968 ).
(b) Initiation is regulated by certain growth factors or peptides
Primordial follicles that enter the growth phase show two distinct morphological changes: 1. Th e oocyte increases in size. 2. Flattened pre-granulosa cells become cuboidal in
appearance.
However, more subtle biochemical, physiological and molecular changes occur prior to these events; e.g., increased expression of the proliferating cell nuclear antigen (PCNA) has been correlated with the earliest stages of follicle growth (Oktay et al ., 1995 ). A num-ber of other genes that are expressed exclusively in the oocyte or germline have also been identifi ed, includ-ing growth development factor (GDF)-9 , required by the granulosa cells and Oct-4 (also known as Oct-3), a POU factor that is also expressed in pluripotential stem
• The cumulus cells become polarized during oocytematuration , and begin to secrete a hyaluronic acidextracellular matrix.
Figure 3.11 Oogenesis in the human. Modifi ed from Johnson ( 2007 ).

Chapter 3: Gametes and gametogenesis
41
cells of the embryo (Rosner et al ., 1990 ). Follicles that have started the growth phase are referred to as early primary follicles.
Follicular destiny
One of the most intriguing mysteries in ovarian physi-ology is what determines whether one follicle remains quiescent, another begins to develop but later becomes atretic, while still a third matures and ovulates.
Over 99% of follicles are destined to die rather than • ovulate; the degenerative process by which these cells are irrevocably committed to undergo cell death is termed atresia. Atretic oocytes show germinal vesicle breakdown, • followed by fragmentation and disruption of the oocyte–cumulus complex – granulosa cells from an aspirated atretic follicle show clear signs of fragmentation. Despite its critical role during the recruitment of • follicles for ovulation, the mechanisms underlying the onset and progression of atresia remain poorly understood. There are four degenerative stages dur-ing ovarian development which result in a massive loss of ovarian cells: 1. During migration of primordial germ cells from
the yolk sac to the genital ridge – many of these cells undergo degeneration.
2. At the time of entry into the fi rst meiotic stage, some germ cells undergo attrition before follicles are formed.
3. In the later stages of development, early antral follicles either diff erentiate or undergo atresia.
4. If ovulatory signals are absent, the mature follicle also may undergo degeneration.
Ovarian stimulation with FSH during ART cycles res-cues follicles that were destined for atresia; therefore most atretic follicles are evidently normal, or we would have seen more defects from children conceived by ART.
Preantral to antral (secondary) follicle
Th e oocyte continues to increase in size, and the granu-losa cells proliferate and divide; when one to two lay-ers of granulosa cells surround the oocyte, the follicle reaches a transitional stage. Further growth produces a secondary follicle with multiple layers of granulosa cells, and the follicles become associated with small blood vessels. Th is is a signifi cant feature, since the pre-antral development of ovarian follicles depends upon locally acting factors and oocyte–granulosa cell com-munication events , independent of the gonadotropins
that are delivered via the bloodstream. In humans, the theca layer does not form until the follicle contains between three and six layers of granulosa cells.
Antral to preovulatory development
Growth factors and hormones induce further follicular growth, the theca and granulosa cell layers proliferate, and the oocyte expands in size, accumulating water, ions, lipids, RNA and proteins. Follicle stimulating hor-mone (FSH) is required for the formation of follicular fl uid , and several pockets of this fl uid, precursor spaces of the antral cavity, begin to form between the granulosa cells. Th e fl uid is derived from the bloodstream, with added glycoproteins secreted by the granulosa cells. When fi ve to eight layers of granulosa cells surround the oocyte, these pockets of fl uid merge to form the antral cavity (follicular antrum). As the antral cavity extends, the oocyte takes up an acentric position in the follicle, and is surrounded by two or more layers of granulosa cells ( Figure 3.11 ).
Under the infl uence of FSH released from the pitu-itary, the granulosa cells diff erentiate into two distinct populations: 1. Th e oocyte and its surrounding follicular cells
form a network or syncytium, a close association that is essential for follicular growth to continue. Cumulus granulosa cells surround the oocyte; these cells are mitotically inactive, and do not divide further. Th e innermost layers of cells become columnar, forming the corona radiata, and these cells communicate with the oocyte via gap junctions linking them with the oolemma.
2. Mural granulosa cells line the follicle wall; these cells stop dividing and also become columnar in appearance. Under the infl uence of FSH, they express receptors for luteinizing hormone (LH) and steroidogenic enzyme pathways become active within the cells.
Other candidates involved in granulosa cell diff eren-tiation include insulin-like growth factors IGF-I and IGF-II; the oocyte itself may also play an important role.
Preovulatory antral follicles
In humans, the oocyte is 120 µm in size at the time of antral cavity formation. Th e oocyte is now capable of resuming meiosis, but only a limited number of oocytes proceed past the antral stage towards ovulation. Around 20 antral follicles are recruited each month from the total
One of the most intriguing mysteries in ovarian physi-ology is what determines whether one follicle remains quiescent, another begins to develop but later becomes atretic, while still a third matures and ovulates.
Over 99% of follicles are destined to die rather than •ovulate; the degenerative process by which these cells are irrevocably committed to undergo cell death is termed atresia. Atretic oocytes show germinal vesicle breakdown, •followed by fragmentation and disruption of the oocyte–cumulus complex – granulosa cells from an aspirated atretic follicle show clear signs of fragmentation. Despite its critical role during the recruitment of •follicles for ovulation, the mechanisms underlying the onset and progression of atresia remain poorly understood. There are four degenerative stages dur-ing ovarian development which result in a massive loss of ovarian cells:1. During migration of primordial germ cells from
the yolk sac to the genital ridge – many of these cells undergo degeneration.
2. At the time of entry into the fi rst meiotic stage, some germ cells undergo attrition before follicles are formed.
3. In the later stages of development, early antral follicles either diff erentiate or undergo atresia.
4. If ovulatory signals are absent, the mature follicle also may undergo degeneration.
Ovarian stimulation with FSH during ART cycles res-cues follicles that were destined for atresia; therefore most atretic follicles are evidently normal, or we would have seen more defects from children conceived by ART.

Chapter 3: Gametes and gametogenesis
42
number available, and even fewer are selected to ovu-late (this number varies between species). Th e remain-ing follicles degenerate through apoptosis and become atretic. Th e recruited follicles continue to grow, and (in monovular species) one follicle in the cohort is selected to become dominant. Th is preovulatory follicle then grows rapidly. In humans the size increases from 6.9 mm (±0.5) to a size of 18.8 mm (±0.5) over a period of 10–20 days. Th e follicular basement membrane must expand by approximately 400 times its original size to accommo-date this follicular growth. Th e granulosa cell population increases from approximately 2–5 million to 50 million, and the mural granulosa cells diff erentiate further.
Ovulation
1. Within a few hours of the LH surge, the follicle becomes more vascularized and swollen, and expansion of the granulosa/cumulus mass causes the follicle to form a visible bulge on the surface of the ovary. Th e projecting follicle wall becomes thin, forming the stigma.
2. A combination of tension and the action of a collagenase enzyme causes the follicle wall to rupture, and follicular fl uid containing the cumulus–oocyte complex (COC) is released from the antral cavity.
3. Th e fi mbriated mouth of the oviduct scrapes the sticky mass of cumulus-enclosed oocyte off the surface of the ovary; synchronized beating of cilia in the tubal wall move the COC along the oviduct. Th e oocyte remains viable in the oviduct for as long as 24 hours.
Generation of the corpus luteum
Aft er ovulation, the follicular basement membrane degenerates, and blood vessels populate the remaining structure of the follicle to form the corpus luteum . Th is structure contains large luteal cells derived from lutei-nized granulosa cells, and smaller luteal cells derived from the theca interna. Both populations of cells release progesterone . If pregnancy is not established, the cor-pus luteum remains in the ovary for 2–14 days (varying with species), and then degenerates by luteolysis.
Oocyte maturation and ovulation Oocyte growth The environment in the developing follicle provides an essential niche for oocyte survival, nourishment
and development, but oocyte growth does not run strictly in parallel with follicular development (see Figure 3.8 ). The primordial human follicle contains a primary oocyte approximately 35 μm in size, and grows to its final size of 120 μm over a period of around 85 days. During this time, it must acquire competence and the ability to be successfully fer-tilized and then support early embryo develop-ment. This process of oocyte maturation involves the coordination of integrated, but independent nuclear and cytoplasmic events: the nucleus under-goes germinal vesicle breakdown, resumption of meiosis, and completion of the first meiotic div-ision. Cytoplasmic maturation requires relocation of cytoplasmic organelles and establishment of oocyte polarity, with an increase in the number of mitochondria and ribosomes. There are alterations in membrane transport systems, and the developing Golgi apparatus expands and migrates to the periph-ery. Organelles appear in the cytoplasm that reflect storage and export of materials: membrane-bound vesicles, multivesicular and crystalline bodies, fat droplets and glycogen granules.
During its growth phase, the oocyte prepares and stores reserves that will be needed for the fi rst stages of fertilization and initiation of embryo develop-ment: water, lipids, carbohydrates and ions accumu-late, and RNA and proteins are synthesized and stored. As the follicle moves from the primordial to the pri-mary stage, the diameter of the oocyte also increases. Although the distribution of organelles and storage materials do not show a defi nite and obvious polar-ity, spatial patterning cannot be entirely ruled out in mammalian eggs (Gardner, 1999 ). A number of fea-tures can be seen during these stages: 1. Th e numbers of mitochondria increase to
approximately 10 5 , and they become more spherical, with fewer concentrically arched cristae, indicating that they are less active.
2. Under the control of the FIGalpha gene, genes coding for the zona pellucida proteins (ZP1, ZP2, ZP3, ZP4) are expressed coordinately and specifi cally. Th e proteins that will make up the zona pellucida (ZP) are secreted, and this forms a 5–10 μm layer around the oocyte. At this stage, the ZP maintains communication between the oocyte and the granulosa cells; ZP3 is the primary sperm receptor.
3. Cytoplasmic organelles become far more abundant, with the notable exception of centrioles,

Chapter 3: Gametes and gametogenesis
43
which disappear and are not found until aft er fertilization. Th e numbers of ribosomes multiply fourfold to around 10 8 in the mature oocyte.
4. Large amounts of RNA are synthesized and stored: the human oocyte has an estimated 1500 pg of total RNA, in contrast to 14 fg in the spermatozoon.
Oocyte polarity
Polarization represents a diff erential distribution of morphological, biochemical, physiological and func-tional parameters in the cell. The appearance of polar-ization may be associated with triggering the developmental program. The growing oocyte does not have a homogeneous structure; in particular, many cytoplasmic organelles become segregated to various regions of the oocyte and this regional organization determines some of the basic properties of the embryo. In all animal oocytes, the pole where the nuclear divi-sions occur (forming a cleavage furrow), resulting in the formation of the polar bodies, is called the animal pole. The opposite pole (opposite to the extruded polar body) is called the vegetal pole, and often contains a high concentration of nutrient reserves. Scanning elec-tron microscopy shows that mouse oocytes have a microvillus-free area on the plasma membrane, adja-cent to the fi rst polar body and overlying the meiotic spindle. Human oocytes show no polarity in the distri-bution and length of the microvilli, either in the animal or the vegetal pole. Studies with fl uorescent lectins reveal no signs of polarization in membrane sugar dis-tribution. However, Antczak and Van Blerkom ( 1997 ) found that two regulatory proteins involved in signal transduction and transcription activation (leptin and STAT3) are polarized in mouse and human oocytes and preimplantation embryos. They suggest that a subpop-ulation of follicle cells may be partly responsible for the polarized distribution of these proteins in the oocyte, and that they may be involved in determining its animal pole, and in the establishment of the inner cell mass and trophoblast in the preimplantation embryo.
The intracellular location of mRNAs and protein translation machinery is related to cell cytoskeleton regulation. Several lines of evidence suggest that mammalian ooplasm redistributes after sperm entry during fertilization (Edwards and Beard, 1997 ). The meiotic spindle that begins to form just before ovula-tion migrates to the cortex, and its position determines the cleavage plane for extruding the fi rst polar body.
Storing information Th e three main classes of RNA (mRNA, tRNA and rRNA) are all involved in the synthesis of protein. Th e
relative amounts of the three types of RNA present dur-ing oogenesis varies from species to species, in the order of 60–65% rRNA, 20–25% tRNA, 10–15% mRNA. Whereas in species such as Xenopus and Drosophila the embryo retains the vast majority of stored mRNA until the blastula stage to direct protein synthesis later in development, mammalian oocytes contain a fi nite amount of stored RNA, which supports only the very early stages of preimplantation embryo development. Th e dictyate chromosomes in mammalian oocytes actively synthesize ribosomal and mRNA as the follicle starts to grow; there is a dramatic increase in the size of the nucleolus as RNA accumulates in the nucleus, including a signifi cant proportion of translatable polyadenylated mRNA. Nucleosomes contain DNA packaged within chromatin, which also contains struc-tural proteins such as histones, and careful regulation of transcriptional machinery controls the expression of particular genes at specifi c times. When the oocyte is fully grown, transcription of new RNA stops almost completely following germinal vesicle breakdown until the time of zygotic genome activation (ZGA) when the new embryonic genome starts to direct further devel-opment. During the period prior to ZGA, the oocyte is dependent upon its pool of stored mRNA, which has been processed with elegant mechanisms that control its expression. Th e stability of mRNA is related to the length of its polyA tail: a long polyA tail is required for translation, but this long tail also makes the message vulnerable to degradation. Th ere are at least two dif-ferent mechanisms of mRNA adenylation in oocyte cytoplasm – the genes are transcribed with long polyA tails, but some messengers are transcribed and trans-lated during growth, whereas others are “masked” by deadenylation, reducing the tail to less than 40 “A” residues: this prevents their translation, and also pro-tects these messages from degradation. In later stages of maturation, the masked genes can then be activated by selective polyadenylation when their products are required. Both gene types contain a highly conserved specifi c sequence in their 3′ untranslatable regions (UTR) that signals polyadenylation. Th e mRNA for the masked transcripts also contains a further sequence 5′ to the polyadenylation signal, known as the cytoplas-mic polyadenylation element (CPE) or the adenylation control element (ACE). It seems that this sequence con-trols the expression of stored mRNAs: ACE-containing mRNAs are masked and protected from degradation, whilst non-ACE-containing mRNAs, available for immediate translation, have long and relatively stable
Polarization represents a diff erential distribution of morphological, biochemical, physiological and func-tional parameters in the cell. The appearance of polar-ization may be associated with triggering the developmental program. The growing oocyte does not have a homogeneous structure; in particular, many cytoplasmic organelles become segregated to various regions of the oocyte and this regional organization determines some of the basic properties of the embryo. In all animal oocytes, the pole where the nuclear divi-sions occur (forming a cleavage furrow), resulting in the formation of the polar bodies, is called the animal pole. The opposite pole (opposite to the extruded polar body) is called the vegetal pole, and often contains a high concentration of nutrient reserves. Scanning elec-tron microscopy shows that mouse oocytes have a microvillus-free area on the plasma membrane, adja-cent to the fi rst polar body and overlying the meiotic spindle. Human oocytes show no polarity in the distri-bution and length of the microvilli, either in the animal or the vegetal pole. Studies with fl uorescent lectins reveal no signs of polarization in membrane sugar dis-tribution. However, Antczak and Van Blerkom ( 1997 ) found that two regulatory proteins involved in signal transduction and transcription activation (leptin and STAT3) are polarized in mouse and human oocytes and preimplantation embryos. They suggest that a subpop-ulation of follicle cells may be partly responsible for the polarized distribution of these proteins in the oocyte, and that they may be involved in determining its animal pole, and in the establishment of the inner cell mass and trophoblast in the preimplantation embryo.
The intracellular location of mRNAs and protein translation machinery is related to cell cytoskeleton regulation. Several lines of evidence suggest that mammalian ooplasm redistributes after sperm entry during fertilization (Edwards and Beard, 1997 ). The meiotic spindle that begins to form just before ovula-tion migrates to the cortex, and its position determines the cleavage plane for extruding the fi rst polar body.

Chapter 3: Gametes and gametogenesis
44
polyA tails ( Figure 3.12 ). Th e mRNAs are also packaged in association with ribonucleoprotein (RNP) particles, and this may represent another control mechanism as part of the complex regulation of transcription and translation. Packaging with RNPs probably plays a part in controlling the access of ribosomes to regulatory elements within the mRNA.
Oocyte reserves
The growing oocyte contains a large amount of infor-mation that is masked, but the rest of the protein syn-thesizing machinery is functional. Many proteins synthesized during oogenesis are stored in the oocyte cytoplasm for later use; for example, the enzymes necessary for DNA synthesis are present in the growing oocyte and yet DNA replication is switched off . Experiments with interspecies nuclear transfer using nuclei from fi broblast cells transferred into bovine, sheep and monkey enucleated oocytes revealed that the fi rst two cell division cycles were regulated by the oocyte cytoplasm; thereafter, the donor nucleus assumed regulatory control, but development arrested after a limited number of cleavage divisions (Fulka et al ., 1998 ). This again demonstrates that the oocyte itself has a large reserve of functional activity, suffi cient to sustain initial cell division cycles – but diff erentiation events in both cytoplasmic and nuclear compartments are essential for continued development.
Stages of oocyte maturation During the fi nal stages of follicle development, mural granulosa cells increase their estrogen synthesis, and serum estrogen levels are signifi cantly elevated. Th is exerts a positive feedback on the pituitary to increase
its release of gonadotropins, in particular LH, result-ing in the preovulatory LH surge. Binding of LH to its receptors on mural granulosa is enhanced, and this activates the pathways that promote oocyte matur-ation. Th e increased binding eventually downregu-lates the steroidogenic pathway that leads to estradiol synthesis, and the cells switch their steroid synthe-sis to the production of progesterone for the luteal phase. Under the infl uence of LH, the primary oocyte matures via a complex interplay between the follicu-lar cells and the oocyte, involving numerous meta-bolic pathways. Th e fi nal stages that lead to ovulation include:
1. Nuclear maturation to allow resumption of meiosis beyond arrest in prophase I. Th e mid-cycle surge of LH initiates a complex cascade of events, which will be described in detail below.
2. Cytoplasmic maturation . During oocyte growth, the Golgi apparatus enlarges and develops into separate units in the cortex; these export glycoproteins to the zona pellucida and form approximately 5 × 10 3 cortical granules that collect at the surface of the oocyte. Th e cortical granules contain enzymes that are later released to modify the zona pellucida (see Chapter 4 ). A fi ne network of endoplasmic reticulum extends throughout the cytoplasm, with dense patches of membrane that become oriented closer to the periphery of the cortex, where they may be involved in calcium release for cortical granule exocytosis. An important feature of cytoplasmic maturation is the translation of mRNA species that have
The growing oocyte contains a large amount of infor-mation that is masked, but the rest of the protein syn-thesizing machinery is functional. Many proteinssynthesized during oogenesis are stored in the oocytecytoplasm for later use; for example, the enzymesnecessary for DNA synthesis are present in the growingoocyte and yet DNA replication is switched off .Experiments with interspecies nuclear transfer usingnuclei from fi broblast cells transferred into bovine,sheep and monkey enucleated oocytes revealed thatthe fi rst two cell division cycles were regulated by theoocyte cytoplasm; thereafter, the donor nucleusassumed regulatory control, but development arrestedafter a limited number of cleavage divisions (Fulkaet al ., 1998 ). This again demonstrates that the oocytelitself has a large reserve of functional activity, suffi cientto sustain initial cell division cycles – but diff erentiationevents in both cytoplasmic and nuclear compartmentsare essential for continued development.
OOCYTEGROWTH
5′
5′
5′
5′
5′
AAUAAA AAA300-400 AAA300-400
AAA40-100
AAA100-200AAA300-400
mRANdeadenylation
mRANreadenylation
AAUAAA
AAUAAA
AAUAAAAAUAAA
CPE
RNPs storage
CPEMasked
CPE
TranslationTranslation
Translation
GCS & Cu-Zn-SOD GPX & Mn-SOD
OOCYTEMATURATION
?
?
Figure 3.12 mRNA processing during oocyte maturation (with thanks to Y. Ménézo).

Chapter 3: Gametes and gametogenesis
45
accumulated in a stable and dormant form during oogenesis .
(c) Cumulus expansion/mucifi cation . Th e preovulatory hormone surge leads to changes in the morphology of the cumulus granulosa cells, and they secrete hyaluronic acid into the intercellular spaces. Oocytes also produce a soluble factor that initiates production of hyaluronic acid by the cumulus granulosa cells, and the matrix thus formed transforms the granulosa cells from a tightly packed cellular mass to a more diff use and dispersed mucifi ed mass. Th e syncytial relationship between the cumulus cells and the oocyte is lost, intercellular communication via gap junctions between the cumulus cells and the oocyte is terminated, and metabolites and informational molecules can no longer pass. Th ese events may act as the trigger for resumption of meiosis.
Nuclear maturation: resumption of meiosis Nuclear maturation specifi cally refers to the fi rst resumption of meiosis, with transformation of the fully grown primary oocyte in the antral follicle into the unfertilized secondary oocyte; this process follows the preovulatory surge of FSH and LH, just prior to ovula-tion. Th e germinal vesicle membrane breaks down, and the nucleus progresses from the dictyate state of the fi rst meiotic prophase through fi rst meiosis to arrest again at metaphase II. Up to this stage, the primary oocyte has been maintained in meiotic arrest by a com-plex balance of cell cycle protein activity, intracellular levels of cAMP and other intracellular messengers. Th e mid-cycle surge of LH causes the level of cAMP in the oocyte to fall below this threshold level, and a cascade of events is initiated that fi nally leads to break-down of the germinal vesicle (GVBD) and resumption of meiosis. Th is cascade involves intracellular ionic messengers, such as Ca 2+ and H + , and a series of cell cycle complexes that have accumulated within the oocyte, including maturation promoting factor (MPF) and cytostatic factor (CSF). Th e surge levels of LH shift follicular steroidogenesis from predominately estro-gen to progesterone production, and this may actively promote the resumption of meiosis by stimulating the oocyte to produce a signal that induces GVBD. Th e nucleus of the germinal vesicle usually contains only one nucleolus, which enlarges from 2 to almost 10 μm in diameter; this nucleolus disappears when the ger-minal vesicle breaks down. A rim of chromatin forms
around the nucleolus in large oocytes, and this is a sign that they are capable of resuming meiosis.
Nuclear maturation during the development of the Graafi an follicle
1. In response to the preovulatory surge of gonado-tropins, the concentration of cAMP within the oocyte falls.
2. Mitochondria increase in volume, are reduced in number, and move to the perinuclear region, an area that requires high concentrations of ATP dur-ing the formation of the fi rst meiotic spindle.
3. Chromatin forms a dense ring around the nucle-olus; microtubular organizing centers (MTOC) congregate as microtubules in the cytoplasm and reorganize to form a functional spindle apparatus.
4. The chromosomes condense, the germinal vesicle membrane breaks down, and the fi rst meiotic spin-dle forms.
5. The spindle migrates to the animal pole of the oocyte and changes orientation.
6. The fi rst meiotic division proceeds through meta-phase I, and then to telophase I. Asymmetrical cell division gives rise to the large functional oocyte and the smaller fi rst polar body.
7. As soon as meiosis I is complete, the oocyte enters into the second meiotic division, and this second-ary oocyte arrests again at metaphase II – ready for fertilization.
8. The trigger for the resumption of the second mei-otic arrest is supplied by the fertilizing spermato-zoon, and meiosis is completed with the extrusion of the second polar body (in the animal kingdom only coelenterates and echinoderms have com-pleted meiosis before sperm entry).
Timing of events:
Control of nuclear maturation Th e control of nuclear maturation involves a complex interplay between numerous metabolic pathways in both the somatic granulosa cells and the oocyte. Th e follicle cells are in direct physical contact with the oocyte, and they either maintain meiotic arrest, or stimulate resump-tion of meiosis by transferring the appropriate signals. Th e metabolic pathways within the granulosa cells are in turn regulated by the binding of gonadotropins to
1. In response to the preovulatory surge of gonado-tropins, the concentration of cAMP within theoocyte falls.
2. Mitochondria increase in volume, are reduced innumber, and move to the perinuclear region, anarea that requires high concentrations of ATP dur-ing the formation of the fi rst meiotic spindle.
3. Chromatin forms a dense ring around the nucle-olus; microtubular organizing centers (MTOC)congregate as microtubules in the cytoplasm andreorganize to form a functional spindle apparatus.
4. The chromosomes condense, the germinal vesiclemembrane breaks down, and the fi rst meiotic spin-dle forms.
5. The spindle migrates to the animal pole of theoocyte and changes orientation.
6. The fi rst meiotic division proceeds through meta-phase I, and then to telophase I. Asymmetrical celldivision gives rise to the large functional oocyteand the smaller fi rst polar body.
7. As soon as meiosis I is complete, the oocyte entersinto the second meiotic division, and this second-ary oocyte arrests again at metaphase II – ready forfertilization.
8. The trigger for the resumption of the second mei-otic arrest is supplied by the fertilizing spermato-zoon, and meiosis is completed with the extrusionof the second polar body (in the animal kingdomonly coelenterates and echinoderms have com-pleted meiosis before sperm entry).
Timing of events:
LH surge: 0 GV with nucleolus+15 hours GVBD+20 hours fi rst meiotic metaphase+35 hours second meiotic metaphase+38 hours ovulation

Chapter 3: Gametes and gametogenesis
46
their cell surface receptors. Small molecules including adenosine, uridine, hypoxanthine and their metabolites diff use between granulosa cells and the oocyte via gap junctions. Th e precise mechanism for the maintenance of arrest remains to be elucidated, and two mechanisms have been proposed: 1. Adenosine stimulates oocyte adenylate cyclase
via a surface receptor on the oolemma, and hypoxanthine prevents hydrolysis of cAMP : high levels of cAMP sustain meiotic arrest.
2. Adenosine could participate directly in meiotic arrest via its conversion to ATP, a substrate for adenyl cyclase within the oocyte. Purines may also participate in cell signaling via G-proteins on the oolemma and plasma membranes of the cumulus cells.
Production of active maturation promoting fac-tor (MPF) in the oocyte cytoplasm mediates nuclear maturation. 1. MPF consists of two components:
(a) A 34 kDa protein, serine/threonine kinase, that is activated by dephosphorylation; homologous to the product of the cdc2 gene in fi ssion yeast.
(b) Cyclin B: activated by phosphorylation, and is probably a substrate for the product of the Mos proto-oncogene, p39.
MPF activity is low in GV stage oocytes • and increases during GVBD. MPF activity is high aft er the resumption • of meiosis, during both metaphase I and metaphase II.
2. Th e action of phosphokinase A (PKA) prevents GVBD. (a) A decrease in intracellular cAMP reduces
PKA activity, and this allows cyclin B and p34cdc2 to associate and form MPF.
(b) p39mos then participates in the activation of MPF, possibly by cyclin B phosphorylation. Synthesis of p39mos is stimulated by progesterone , and this may be a key event in the induction of meiotic maturation.
(c) By maintaining cyclin B in its phosphorylated (active) form, p39 may stabilize MPF and act as a cytostatic factor (CSF), thereby maintaining metaphase II arrest.
Th e product of the oncogene Mos is expressed early in oocyte maturation and disappears immediately
aft er fertilization. Th e Mos protein has the same eff ects as CSF, arresting mitosis at metaphase with high p34cdc2 activity. It is thought that CSF is, in part or entirely Mos, and that the second meiotic arrest is due to transcription of the Mos oncogene as the oocyte matures.
In summary, the production of a viable oocyte depends on three key processes: 1. Th e fully grown oocyte must recognize regulatory
signals generated by follicular cells. 2. Extensive reprogramming within the oocyte
must be induced – this involves activation of appropriate signal transduction mechanisms.
3. Individual molecular changes must be integrated to drive the two parallel but distinct processes involved in meiotic progression and the acquisition of developmental competence.
Th e oocyte depends on the follicular compartment for direct nutrient support, and for regulatory signals. Aft er the LH surge, new steroid, peptide and protein signals are generated, and alterations to preovulatory steroid profi les can selectively disrupt protein repro-gramming and individual components of the fertiliza-tion process.
Localized short- and long-lived maternal mRNAs regulate the initial stages of development and diff er-entiation both in the oocyte and in the early embryo.
Th ere is no doubt that the process of oocyte growth and maturation is a highly complex process, involv-ing a three-dimensional series and sequence of regu-latory elements at several diff erent molecular levels. Th e fi nal evolution of a mature oocyte which has the potential for fertilization and further development is dependent upon the correct completion and syn-chronization of all processes involved: although an overview is emerging, many aspects still remain to be elucidated. Th us it is impossible to assess and gauge the consequences of manipulations during assisted reproduction practice, and it is essential to maintain an awareness of the complexity and sensitivity of this delicate and highly elegant biological system. Our in-vitro attempts to mimic nature will only succeed if they are carried out within this frame of reference.
Further reading Gametogenesis Antczak M , Van Blerkom J ( 1997 ) Oocyte infl uences on
early development: the regulatory proteins leptin and

Chapter 3: Gametes and gametogenesis
47
STAT3 are polarized in mouse and human oocytes and diff erentially distributed within the cells of the preimplantation stage embryo . Molecular Human Reproduction 3 : 1067 –1086.
Bachvarova R ( 1985 ) Gene expression during oogenesis and oocyte development in mammals. In: Browder LW (ed.) Developmental Biology. A Comprehensive Synthesis , Vol. 1, Oogenesis . Plenum , New York , pp. 453–524.
Bellve A , O’Brien D ( 1983 ) Th e mammalian spermatozoon: structure and temporal assembly. In: Mechanism and Control of Animal Fertilization . Academic Press , New York , pp. 56–140.
Braun RE ( 2000 ) Temporal control of protein synthesis during spermatogenesis . International Journal of Andrology 23 (Suppl. 2): 92 –94.
Briggs D , Miller D , Gosden R ( 1999 ) Molecular biology of female gametogensis. In: Molecular Biology in Reproductive Medicine . Parthenon Press , New York , pp. 251–267.
Buccione R , Schroeder AC , Eppig JJ ( 1990 ) Interactions between somatic cells and germ cells throughout mammalian oogenesis . Biology of Reproduction 43 : 543 –547.
Byskov AG , Andersen CY , Nordholm L , et al . ( 1995 ) Chemical structure of sterols that activate oocyte meiosis . Nature 374 : 559 –562.
Canipari R ( 2000 ) Oocyte-granulosa cell interactions . Human Reproduction Update 6 : 279 –289.
Canipari R , Epifano O , Siracusa G , Salustri A ( 1995 ) Mouse oocytes inhibit plasminogen activator production by ovarian cumulus and granulosa cells . Developmental Biology 167 : 371 –378.
Cho WK , Stern S , Biggers JD ( 1974 ) Inhibitory eff ect of dibutyryl cAMP on mouse oocyte maturation in vitro . Journal of Experimental Zoology 187 : 383 –386.
Choo YK , Chiba K , Tai T , Ogiso M , Hoshi M ( 1995 ) Diff erential distribution of gangliosides in adult rat ovary during the oestrous cycle . Glycobiology 5 : 299 –309.
Clarkson MJ , Harley VR ( 2002 ) Sex with two SOX on: SRY and SOX9 in testis development . Trends in Endocrinology and Metabolism 13 (3): 106 –111.
Dale B ( 1996 ) Fertilization. In: Greger R , Windhorst U (eds.) Comprehensive Human Physiology . Springer Verlag , Heidelberg .
Dekel N ( 1996 ) Protein phosphorylation/dephosphorylation in the meiotic cell cycle of mammalian oocytes . Reviews of Reproduction 1 : 82 –88.
Dong J , Albertini DF , Nishimori K , Kumar TR , Lu N , Matzuk MM ( 1996 ) Growth diff erentiation factor-9 is required during early ovarian folliculogenesis . Nature 383 : 531 –535.
Eddy EM ( 1998 ) Regulation of gene expression during spermatogenesis . Seminars in Cell and Developmental Biology 9 : 451 –457.
Edwards RG , Beard H ( 1997 ) Oocyte polarity and cell determination in early mammalian embryos . Molecular Human Reproduction 3 : 868 –905.
Elder K , Elliott T (eds.) ( 1998 ) Th e use of epididymal and testicular sperm in IVF. Worldwide Conferences in Reproductive Biology 2 , Ladybrook Publications , Australia .
Epifano O , Dean J ( 2002 ) Genetic control of early folliculogenesis in mice . Trends in Endocrinology and Metabolism 13 (4): 169 –173.
Eppig JJ , O’Brien MJ ( 1996 ) Development in vitro of mouse oocytes from primordial follicles . Biology of Reproduction 54 : 197 –207.
Faddy MJ , Gosden RG ( 1995 ) A mathematical model for follicle dynamics in human ovaries . Human Reproduction 10 : 770 –775.
Fulka J Jr., First N , Moor RM ( 1998 ) Nuclear and cytoplasmic determinants involved in the regulation of mammalian oocyte maturation . Molecular Human Reproduction 4 (1): 41 –49.
Gardner R ( 1999 ) Polarity in early mammalian development . Current Opinion in Genetics and Development 9 (4): 417 –421.
Gosden RG , Boland NI , Spears N , et al . ( 1993 ) Th e biology and technology of follicular oocyte development in vitro . Reproductive Medicine Reviews 2 : 129 –152.
Gosden RG , Bownes M ( 1995 ) Cellular and molecular aspects of oocyte development. In: Grudzinskas JG , Yovich JL (eds.) Cambridge Reviews in Human Reproduction, Gametes – Th e Oocyte . Cambridge University Press , Cambridge , pp. 23–53.
Gougeon A ( 1996 ) Regulation of ovarian follicular development in primates – facts and hypotheses . Endocrine Review s 17 : 121 –155.
Gurdon JB ( 1967 ) On the origin and persistence of a cytoplasmic state inducing nuclear DNA synthesis in frog’s eggs . Proceedings of the National Academy of Sciences of the USA 58 : 545 –552.
Henderson SA , Edwards RG ( 1968 ) Chiasma frequency and maternal age in mammals . Nature 217 (136): 22 –28.
Hess RA ( 1999 ) Spermatogenesis, overview. Encyclopedia of Reproduction vol. 4. Academic Press , New York , pp. 539–545.
Hillier SG , Whitelaw PF , Smyth CD ( 1994 ) Follicular oestrogen synthesis: the ‘two-cell, two-gonadotrophin’ model revisited . Molecular and Cellular Endocrinology 100 : 51 –54.
Hirshfi eld AN ( 1991 ) Development of follicles in the mammalian ovary . International Review of Cytology 124 : 43 –100.
Hutt KJ , Albertini DF ( 2007 ) An oocentric view of folliculogenesis and embryogenesis Reproductive Biomedicine Online 14 (6): 758 –764.

Chapter 3: Gametes and gametogenesis
48
Johnson M ( 2007 ) Essential Reproduction , 6th edn. Blackwell Scientifi c Publications , Oxford .
Johnson J , Bagley J , Skaznik-Wikiel M , et al . ( 2005 ) Oocyte generation in adult mammalian ovaries by putative germ cells in bone marrow and peripheral blood . Cell 122 : 303 –315.
Jones R ( 1998 ) Spermiogenesis and sperm maturation in relation to development of fertilizing capacity. In: Lauria A , et al . (eds.) Gametes: Development and Function . Serono Symposia , Rome , pp. 205–218.
Kobayashi M , Nakano R , Ooshima A ( 1990 ) Immunohistochemical localization of pituitary gonadotrophins and gonadal steroids confi rms the ‘two-cell, two-gonadotrophin’ hypothesis of steroidogenesis in the human ovary . Journal of Endocrinology 126 (3): 483 –488.
Kramer JA , McCarrey JR , Djakiew D , Krawetz SA ( 1998 ) Diff erentiation: the selective potentiation of chromatin domains . Development 125 : 4749 –4755.
MacLaren A ( 2003 ) Primordial germ cells in the mouse . Developmental Biology 262 (1): 1 –15.
Masui Y ( 1985 ) Meiotic arrest in animal oocytes. In: Metz CB , Monroy A (eds.) Biology of Fertilization . Academic Press , New York , pp. 189–219.
Matzuk MM , Burns KH , Viveiros MM , Eppig JJ ( 2002 ) Intercellular communication in the mammalian ovary: oocytes carry the conversation . Science 296 (5576): 2178 –2180.
McNatty KP , Fidler AE , Juengel JL , et al . ( 2000 ) Growth and paracrine factors regulating follicular formation and cellular function . Molecular and Cellular Endocrinology 163 : 11 –20.
Merchant-Larios H , Moreno-Mendoza N ( 2001 ) Onset of sex diff erentiation: dialog between genes and cells . Archives of Medical Research 32 (6): 553 –558.
Moore HDM ( 1996 ) Th e infl uence of the epididymis on human and animal sperm maturation and storage . Human Reproduction 11 (Suppl.): 103 –110.
Nurse P ( 1990 ) Universal control mechanisms resulting in the onset of M-phase . Nature 344 : 503 –508.
Oktay K , Schenken RS , Nelson JF ( 1995 ) Proliferating cell nuclear antigen marks the initiation of follicular growth in the rat . Biology of Reproduction 53 (2): 295 –301.
Pereda J , Zorn T , Soto-Suazo M ( 2006 ) Migration of human and mouse primordial germ cells and colonization of the developing ovary: An ultrastructural and cytochemical study . Microscopy Research and Technique 69 (6): 386 –395.
Perez GI , Trbovich AM , Gosden RG , Tilly JL ( 2000 ) Mitochondria and the death of oocytes . Nature 403 (6769): 500 –501.
Picton HM , Briggs D , Gosden RG ( 1998 ) Th e molecular basis of oocyte growth and development . Molecular and Cellular Endocrinology 145 : 27 –37.
Reynard K , Driancourt MA ( 2000 ) Oocyte attrition . Molecular and Cellular Endocrinology 163 : 101 –108.
Rosner MH , Vigano MA , Ozato K , et al . ( 1990 ) A POU-domain transcription factor in early stem cells and germ cells of the mammalian embryo . Nature 345 (6277): 686 –692.
Sagata N ( 1996 ) Meiotic metaphase arrest in animal oocytes: its mechanisms and biological signifi cance . Trends in Cell Biology 6 : 22 –28.
Sagata N ( 1997 ) What does Mos do in oocytes and somatic cells? BioEssays 19 : 13 –21.
Schatten H , Sun QY ( 2009 ) Th e role of centrosomes in mammalian fertilization and its signifi cance for ICSI . Molecular Human Reproduction 15 (9): 531 –538.
Spears N , Boland NI , Murray AA , Gosden RG ( 1994 ) Mouse oocytes derived from in vitro grown primary ovarian follicles are fertile . Human Reproduction 9 : 527 –532.
Starz-Gaiano M , Lehmann R ( 2001 ) Moving towards the next generation . Mechanisms of Development 105 (1–2): 5 –18.
Sutovsky P , Flechon JE , Flechon B , et al . ( 1993 ) Dynamic changes of gap junctions and cytoskeleton in in vitro culture of cattle oocyte cumulus complexes . Biology of Reproductions 49 : 1277 –12787.
Swain A , Lovell-Badge R ( 1999 ) Mammalian sex determination: a molecular drama . Genes and Development 13 (7): 755 –767.
Taylor CT , Johnson PM ( 1996 ) Complement-binding proteins are strongly expressed by human preimplantation blastocysts and cumulus cells as well as gametes . Molecular Human Reproduction 2 : 52 –59.
Telfer EE ( 1996 ) Th e development of methods for isolation and culture of preantral follicles from bovine and porcine ovaries . Th eriogenology 45 : 101 –110.
Telfer EE , McLaughlin M ( 2007 ) Natural history of the mammalian oocyte . Reproductive Biomedicine Online 15 (3): 288 –295.
Van Blerkom J , Motta P ( 1979 ) Th e Cellular Basis of Mammalian Reproduction . Urban and Schwarzenberg , Baltimore .
Ward WS ( 1993 ) Deoxyribonucleic acid loop domain tertiary structure in mammalian spermatozoa . Biology of Reproduction 48 (6): 1193 –1201.
Ward WS , Coff ey DS ( 1991 ) DNA packaging and organization in mammalian spermatozoa: comparison with somatic cells . Biology of Reproduction 44 (4): 569 –574.
Wassarman PM ( 1996 ) Oogenesis. In: Adashi EY , Rock JA , Rosenwaks Z (eds.) Reproductive Endocrinology, Surgery and Technology , vol. 1. Lippincott-Raven Publishers , Philadelphia , pp. 341–359.
Wassarman PM , Liu C , Litscher ES ( 1996 ) Constructing the mammalian egg zona pellucida: some new pieces of an old puzzle . Journal of Cell Science 109 : 2001 –2004.

Chapter 3: Gametes and gametogenesis
49
Whitaker M ( 1996 ) Control of meiotic arrest . Reviews of Reproduction 1 : 127 –135.
Yanagamachi R ( 1994 ) Mammalian fertilization. In: Knobil E , Neill J (eds.) Th e Physiology of Reproduction . Raven Press , New York , pp. 189–317.
Sperm chromatin packaging and RNA carriage Balhorn R ( 1982 ) A model for the structure of chromatin
in mammalian sperm . Journal of Cell Biology 93 : 298 –305.
Balhorn R , Gledhill BL , Wyrobek AJ ( 1977 ) Mouse sperm chromatin proteins: quantitative isolation and partial characterization . Biochemistry 16 : 4074 –4080.
Bench G , Corzett M H , DeYebra L , Oliva R , Balhorn R ( 1998 ) Protein and DNA contents in sperm from an infertile human male possessing protamine defects that vary over time . Molecular Reproduction and Development 50 : 345 –353.
Cho C , Willis WD , Goulding EH , et al . ( 2001 ) Haploinsuffi ciency of protamine-1 or -2 causes infertility in mice Nature Genetics 28 : 82 –86.
Gardiner-Garden M , Ballesteros M , Gordon M , Tam PP ( 1998 ) Histone- and protamine-DNA association: conservation of diff erent patterns within the beta-globin domain in human sperm . Molecular and Cellular Biology 18 : 3350 –3356.
Gatewood JM , Cook GR , Balhorn R , Bradbury EM , Schmid CW ( 1987 ) Sequence-specifi c packaging of DNA in human sperm chromatin Science 236 : 962 –964.
Gatewood JM , Cook GR , Balhorn R , Schmid CW , Bradbury EM ( 1990 ) Isolation of 4 core histones from human sperm chromatin representing a minor subset of somatic histones . Journal of Biological Chemistry 265 : 20662 –20666.
Miller D ( 2000 ) Analysis and signifi cance of messenger RNA in human ejaculated spermatozoa . Molecular Reproduction and Development 56 : 259 –264.
Miller D , Ostermeier GC ( 2006 ) Towards a better understanding of RNA carriage by ejaculate spermatozoa . Human Reproduction Update 12 : 757 –767.
Wykes SM , Krawetz SA ( 2003 ) Th e structural organization of sperm chromatin . Journal of Biological Chemistry 278 : 29471 –29477.
Sex-determining mechanisms Miller D ( 2004 ) Sex determination: insights from the
human and animal models suggest that the mammalian Y chromosome is uniquely specialised for the male’s benefi t . Journal of Men’s Health and Gender 1 : 170 –181.
Morais da Silva S , Hacker A , Harley V , et al . ( 1996 ) Sox9 expression during gonadal development implies a conserved role for the gene in testis diff erentiation in mammals and birds . Nature Genetics 14 : 62 –68.
Sekido R , Bar I , Narvaez V , Penny G , Lovell-Badge R ( 2004 ) SOX9 is up-regulated by the transient expression of SRY specifi cally in Sertoli cell precursors . Developmental Biology 274 : 271 –279.
Sekido R , Lovell-Badge R ( 2008 ) Sex determination involves synergistic action of SRY and SF1 on a specifi c Sox9 enhancer. Nature 453 : 930 –934.

Chapter
1
50
Sperm–oocyte interaction
Gamete interaction In nature, fertilization occurs only aft er both the oocyte and the spermatozoon have completed their fi nal stages of cytoplasmic maturation. Th e male gamete has com-pleted meiosis prior to the moment of fertilization, but fi nal nuclear maturation with the second meiotic div-ision occurs in the female gamete only aft er fertilization has taken place. Sperm–oocyte interaction is a com-plex process of cell–cell interaction that requires spe-cies-specifi c recognition and binding of the two cells. While interacting, each gamete triggers a process of physiological activation in its partner. Controlled, syn-chronous gamete activation is essential for embryonic development; however, the biochemical and cellular processes that ultimately lead to the fusion of the male and female pronuclei are still poorly understood. In human assisted reproductive technology, although the technique of intracytoplasmic injection of spermatozoa (ICSI) essentially bypasses the initial stages of fertiliza-tion, including sperm capacitation and the interaction of the gametes, successful fertilization still requires controlled and correct activation of both sperm and oocyte.
Mammalian fertilization is internal and the male gametes must be introduced into the female tract at coitus. Coitus itself ranges from minutes in humans to hours in camels, but is accompanied by many physio-logical changes. In the human, tactile and psychogenic stimuli can initiate penile erection, caused by decrease in resistance and consequently dilatation in the arteries supplying the penis, with closure of the arterio-venous shunts and venous blood valves. Vasocongestion can increase the volume of the testes by as much as 50%. Sequential contraction of the smooth muscles of the urethra and the striated muscles in the penis results in ejaculation of semen, with mixing of three diff erent components: prostatic liquid rich in acid phosphatase,
the vas deferens fraction containing spermatozoa , and the seminal vesicle fraction containing fructose.
In the woman, tactile stimulation of the glans clitoris and vaginal wall leads to engorgement of the vagina and labia majora, and the vagina expands. Orgasm is accom-panied by frequent vaginal contractions, with uterine contractions beginning in the fundus and spreading to the lower uterine segment. In man, rabbit, sheep, cow and cat, the semen is ejaculated into the vagina. In the pig, dog and horse, it is deposited directly into the cer-vix and uterus. In many species, the semen coagulates rapidly aft er deposition in the female tract, as a result of interaction with an enzyme of prostatic origin. Th e coagulation may serve to retain spermatozoa in the vagina or to protect them from the acid environment.
In the human, this coagulum is dissolved within one hour by progressive action of a second proenzyme, also of prostatic origin. Within minutes of coitus , spermatozoa may be detected in the cervix or uterus; 99% of the spermatozoa are lost from the vagina, but the few that enter the tract may survive for many hours in the cervical crypts of mucus. In the absence of pro-gesterone , cervical mucus permits sperm penetration into the upper female tract. Although data are incon-clusive, it appears that activity of the musculature of the female tract is not required for sperm transport. Spermatozoa probably move through the uterus under their own propulsion, and are transported in currents set up by the action of uterine cilia. Th e cervical crypts may serve as a reservoir regulating fl ow of spermato-zoa into the tract, while the utero-tubal junction may act as a sphincter. In hamster and rabbit, the earliest appearance of spermatozoa in the oviducts is 47 hours. Th erefore, in most animals, although great quantities of spermatozoa are produced, very few reach the oocyte. Th ose that do must then traverse and interact with the cumulus and coronal cells, which reduce the number of
4
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. (©) K. Elder and B. Dale 2011.

Chapter 4: Sperm–oocyte interaction
51
spermatozoa that can reach the oocyte to bind to and penetrate the zona pellucida. Polyspermy , a lethal con-dition where several spermatozoa enter the oocyte, is probably rare in nature.
Sperm–oocyte ratios
In the course of evolution, it seems that great wastage of spermatozoa has been retained as a requirement for the union of one spermatozoon with one oocyte. In most animals, spermatozoa are produced in huge excess, irrespective of whether fertilization occurs externally or internally: in humans, the sperm–oocyte ratio can be as high as 10 9 :1. Of the millions of sperm-atozoa ejaculated and deposited in the female tract, only a few reach the site of fertilization, the ampullae of the fallopian tube in most species. An in-vivo study of fertilization in the mouse showed a 1:1 sperm–oocyte ratio in the ampullae – supernumerary spermatozoa were never observed.
Th e initial stages of fertilization depend princi-pally on two structures: the acrosome of the spermato-zoon and the zona pellucida of the oocyte. Th ree major events are involved in sperm–oocyte interaction: 1. Th e spermatozoon attaches to the zona pellucida
(ZP). 2. Th e spermatozoon undergoes the acrosome
reaction , releasing digestive enzymes, and exposing the inner acrosomal membrane.
3. Th is highly fusogenic sperm membrane makes contact with the oocyte plasma membrane and the two membranes fuse together.
Gamete activation Sperm activation Before the male gamete can initiate the steps required for successfully fertilizing an oocyte, the spermatozoon must itself be fi rst activated, a process that involves sev-eral behavioral, physiological and structural changes. Some of these changes are induced by exposure to environmental signals, and others are induced whilst the spermatozoon is interacting with the oocyte and its extracellular investments. Th e steps include changes in motility, capacitation, acrosome reaction , penetration of the ZP, binding to the oolemma, and membrane fusion.
Motility Spermatozoa are maintained in the testis in a quies-cent state, with a metabolic suppression that may be due to many factors, such as physical restraint, low
pH and low oxygen tension of the seminal fl uid. Th ey acquire motility in the process of epididymal matur-ation, but only become fully motile aft er ejaculation and capacitation.
Capacitation Spermatozoa are not capable of fertilization immedi-ately aft er ejaculation. Th ey develop the capacity to fer-tilize (capacitate) aft er a period of time in the female genital tract; since epididymal maturation and cap-acitation are unique to mammals, this may represent an evolutionary adaptation to internal fertilization. During capacitation, the spermatozoa undergo a series of changes that give them the “capacity” for binding to and penetrating the oocyte. Th ese changes include an increase in membrane fl uidity, cholesterol effl ux, ion fl uxes that alter sperm membrane potential, increased tyrosine phosphorylation of proteins, induction of hyperactive motility, and the acrosome reaction.
Th e time required for capacitation varies from spe-cies to species and ranges from less than 1 hour in the mouse to 6 hours in the human.
Two changes take place: the epididymal and seminal plasma proteins coating the spermatozoa are removed, followed by an alteration in the glycoproteins of the sperm plasma membranes (an antigen on the plasma membrane of the mouse spermatozoon, laid down during epididymal maturation, cannot be removed by repeated washing, but disappears, or is masked dur-ing capacitation). Th e events are regulated by the acti-vation of intracellular signaling pathways, involving cAMP , protein kinase A, receptor tyrosine kinases and non-receptor tyrosine kinases. A number of diff erent molecules regulate these pathways, including calcium, bicarbonate, reactive oxygen species, GABA, proges-terone , angiotensin and cytokines. Phosphorylation of sperm proteins is an important part of capacita-tion, and this has been shown to be associated with the change in the pattern of sperm motility known as hyperactive motility , recognizable by an increase in lat-eral head displacement. Th ere is also some evidence that spermatozoa can translate some mRNA species during capacitation (Gur and Breitbar, 2006 ).
In the human, capacitation in vivo probably starts while the spermatozoa are passing through the cer-vix. Many enzymes and factors from the female tract have been implicated in causing capacitation, such as arylsulfatase, fucosidase and taurine. Th e factors involved are not species specifi c, and capacitation may be induced in vitro in the absence of any signals from
In the course of evolution, it seems that great wastage of spermatozoa has been retained as a requirement for the union of one spermatozoon with one oocyte. In most animals, spermatozoa are produced in huge excess, irrespective of whether fertilization occurs externally or internally: in humans, the sperm–oocyte ratio can be as high as 10 9:1. Of the millions of sperm-atozoa ejaculated and deposited in the female tract, only a few reach the site of fertilization, the ampullae of the fallopian tube in most species. An in-vivo study of fertilization in the mouse showed a 1:1 sperm–oocyte ratio in the ampullae – supernumerary spermatozoa were never observed.

Chapter 4: Sperm–oocyte interaction
52
the female tract. Follicular fl uid can also promote cap-acitation in vitro . A low molecular weight motility fac-tor found in follicular fl uid, ovary, uterus and oviduct may increase sperm metabolism (and hence motility) by lowering ATP and increasing cyclic AMP levels within the sperm. Table 4.1 demonstrates the duration of fertility and motility of mammalian spermatozoa within the oviduct, together with the fertilizable life of oocytes.
Chemically defi ned media with appropriate con-centrations of electrolytes, metabolic energy sources and a protein source (serum albumin) will also induce the acrosome reaction in a population of washed sperm. Th e removal or redistribution of glycoproteins on the sperm cell surface during capacitation exposes receptor sites that can respond to oocyte signals, lead-ing to the acrosome reaction .
Capacitation is temperature dependent and only • occurs at 37–39°C. Sperm surface components are removed or altered • during capacitation. In vitro, the acrosome reaction cannot occur until • capacitation is complete.
Acrosome reaction (AR) Th e acrosome is a membrane-bound cap that covers the anterior portion of the sperm head; it contains a large array of hydrolytic enzymes including hyaluroni-dase, acrosin, proacrosin, phosphatase, arylsulfatase, collagenase, phospholipase C and β-galactosidase. Th e acrosome originates in the Golgi system of the
early spermatid, in a series of concentrically arranged membranes around an aggregation of small vesicles. One of the vesicles increases in size and fi lls with par-ticulate material, and the vesicle grows by fusion of several smaller vesicles. When the future acrosomal vesicle reaches a certain size, it migrates towards the nucleus. Th e nucleus then starts to elongate, the ves-icle loses much of its fl uid content and its membrane wraps around the front of the nucleus to form the typ-ical acrosome.
When the capacitated spermatozoon attaches to the ZP, the permeability of the sperm plasma membrane is altered, causing a transient change in the concentration of several intracellular ions. Th is triggers the acrosome reaction, which is the fi nal prerequisite step in the acti-vation of the spermatozoon before gamete fusion is possible. Th e reaction consists of three stages: 1. Th e outer acrosomal membrane fuses with the
overlying sperm head plasma membrane, allowing the contents to be released; this can be monitored in vitro using a fl uorescent tag in the acrosome reaction to ionophore challenge (ARIC) test .
2. Th e acrosomal granule breaks down, releasing lysins. Th ese enzymes “dissolve” a pathway through the ZP.
3. When the sperm head plasma membrane contacts the oocyte plasma membrane, the two membranes fuse.
It appears that not all of the bound sperm are able to penetrate the egg, and many are not triggered into the acrosome reaction . In order for sperm to attach,
Table 4.1 Survival parameters of mammalian gametes in vitro (with permission from Gwatkin, 1974 )
Time required for capacitation (h)
Duration of sperm motility (h)
Duration of sperm fertility (h)
Fertilizable life of oocytes (h)
Mouse <1 13 6 15
Sheep 1–5 48 30–48 12–15
Rat 2–3 17 14 12
Hamster 2–4 – – 9–12
Pig 3–6 50 24–48 10
Rabbit 5 43–50 28–36 6–8
Rhesus monkey 5–6 – – 23
Man 5–6 48–60 24–48 6–24
Dog – 268 134 24

Chapter 4: Sperm–oocyte interaction
53
a specifi c molecular fi t may be required to induce the acrosome reaction. In the human, the membranes start to fuse near the border between the acrosomal cap and its equatorial segment. Once the correct trigger signals have been received, the acrosome reaction is relatively rapid, taking 2–15 minutes in vitro. Gametes collected from the ampullae of mammals aft er mating show that free-swimming spermatozoa have unreacted acro-somes, and those within the cumulus mass have either reacted acrosomes, or are in the process of reacting. Th e majority of spermatozoa attached to the surface of the zona pellucida surface have reacted acrosomes.
Th e acrosome reaction only occurs in the presence of Ca 2+ : it may be induced artifi cially by adding Ca iono-phore A23187 , a chemical that carries Ca 2+ across cell membranes to the sperm cytoplasm ( Figure 4.1 ), or simply by increasing the external concentration of Ca 2+ . An artifi cially high pH of about 9–9.5 will also induce the AR. It appears that the physiological events lead-ing to the AR parallel those leading to activation of the oocyte, including changes in the ion permeability of the plasma membrane, alterations in the intracellular level of free Ca 2+ and an alkalinization of the cytoplasm. Th e infl ux of calcium triggers the fusion of the acro-somal membranes and the exocytosis of the acrosomal
contents. Th e sequence of events leading to exocytosis may involve potential second messenger pathways, including:
Changes in intracellular calcium • Activation of cAMP and phosphokinase A • pathways Phospholipase C generating InsP3 and • diacylglycerol (DAG) Phospholipase D generating phosphatidic acid • Activation of phospholipase A2 generating • arachidonic acid.
Completion of the acrosome reaction does not neces-sarily ensure successful fertilization in vitro – enor-mous variability can be found in a population of spermatozoa surrounding the cumulus mass. Some will acrosome react too soon, others too late: in some the trigger stimulus will be inadequate, perhaps in others the transduction mechanism will fail at some point. Th e cumulus mass is composed of both cellular and acellular components, and the acellular matrix is made up of proteins and carbohydrates, including hya-luronic acid. In vivo, very few spermatozoa reach the site of fertilization: therefore the idea that large popu-lations of spermatozoa surrounding the oocyte mass dissolve the cumulus matrix, as observed during IVF, is probably incorrect in vivo. Fertilization occurs before the dispersion of the cumulus mass, and in vivo the sperm:oocyte ratio is probably close to 1:1.
Oocyte activation The zona pellucida (ZP) Th e zona pellucida is a glycoprotein sheet several micrometers thick that is secreted by the growing oocyte, providing a protective coat around the oocyte and developing embryo. If we accept the concept that polyspermy prevention is laboratory artifact rather than natural fact, then it probably serves mainly as a protective coat for the developing embryo. Electron microscopy shows the outer surface to have a latticed appearance, and its chemical composition consists of 70% protein, 20% hexose, 3% sialic acid and 2% sulfate. In the mouse oocyte, the zona contains three glyco-proteins, ZP1, ZP2 and ZP3, with apparent molecular weights of 200 000, 120 000 and 83 000, respectively; each is heavily glycosylated. Filaments of ZP2 and ZP3 polymers are crosslinked non-covalently, and ZP1 dimers create bridges between them to form a matrix (Wassarman et al. , 1996 ). In the mouse, ZP2 is
Figure 4.1 Acrosome structure. Transmission electron micro-scope (TEM) section through a human spermatozoon showing the plasma membrane (PM) and outer (OAM) and inner (IAM) acrosomal membranes. To the right is a TEM of a human spermatozoon after exposure to the calcium ionophore A23187 has triggered the acro-some reaction.

Chapter 4: Sperm–oocyte interaction
54
distributed throughout the thickness of the zona, and ZP3 binds to primary receptors on capacitated sperm-atozoa , inducing a cascade of events that lead to the acrosome reaction . Sperm receptors for ZP2, in con-trast, are located on the inner acrosomal membrane and therefore are unmasked only aft er the AR has taken place. Following the AR, ZP2 binds the sperm to the zona, and the sperm penetrate the ZP to fuse with the oocyte plasma membrane.
Th e ZP gene family has an ancient phylogeny, and the coding sequences of the murine and human ZP genes are 74% identical. However, the zona in many species, including humans, contains a fourth zona pro-tein, ZP4, which is absent in mice. Studies carried out in humans have revealed that ZP2 is modifi ed by cleav-age, similar to the mouse model, and sperm penetration through the zona is inhibited aft er fertilization. Aft er sperm penetration the zona undergoes modifi cations consistent with its role as a protective device. However, unlike the mouse, the ZP can still bind spermatozoa and induce the AR. Th us, fertilization does not abol-ish ZP bioactivity. Th is diff erence may be linked to the presence of ZP4 – the precise events that describe the role of the zona proteins in gamete interaction require further study in humans (Lefi evre et al. , 2004 ; Conner et al. , 2005 ; Patrat et al. , 2006 ).
Cytoplasmic maturation Oocytes acquire competence for successful fertilization and the ability to sustain early development via cyto-plasmic maturation, a process that may be considered a parallel to sperm capacitation. Several milestones in development must be reached before it is capable of being fertilized correctly: 1. M-phase promoting factor (MPF) is expressed at a
high level. 2. High levels of other factors are present within
the oocyte, including c-mos, mitogen activated protein kinase (MAPK) and active p34cdc2.
3. Progression to the MII stage of meiosis. Th e fi rst polar body must be extruded to the perivitelline space, between the oolemma and zona pellucida .
4. Virtually all transcription ceases by the time of germinal vesicle breakdown (GBVD) . Th e expression of genes beyond this stage switches to translation of stored mRNA.
Th ese points are summarized in Table 4.2 . Th e fi rst event of activation in oocytes of most spe-
cies is an increase in ionic permeability of the plasma
membrane. In the human, the spermatozoon induces an outward current in the oocyte plasma membrane by activating calcium-gated potassium channels. In vitro, activation competence in oocytes is continually chan-ging, and is not a stable, prolonged feature of ovulated eggs; therefore timing is critical in the handling of in-vitro manipulations.
Sperm–oocyte fusion Th e process of membrane fusion between gametes is temperature, pH and Ca 2+ dependent, and the two membranes must be in close approximation. Fusion appears to be mediated or facilitated by membrane-associated proteins, but terminal saccharides of glyc-oproteins are not directly involved in the process. During penetration of the zona, the spermatozoon loses its acrosomal contents and only the inner acro-somal membrane is in direct contact with the zona. In eutherian mammals, the postacrosomal region of the sperm head plasma membrane only attains fusibility aft er the acrosome reaction ; this area apparently fuses with the oocyte plasma membrane, and the two mem-branes become continuous ( Figure 4.2 ).
Th e surface of the oocyte membrane is organized into evenly spaced short microvilli that seem to facili-tate gamete fusion; these microvilli have a low radius of curvature which may help to overcome opposing electrostatic charges. In mouse and hamster, the area overlying the metaphase spindle is microvillus-free and spermatozoa are not able to, or are less likely to, fuse with this area. Th e human oocyte, however, has microvilli present over the entire surface, with no obvious polarity at this stage – there may be “hotspots” for sperm entry into the oocyte. Th e sperm plasma membrane remains fused with the oocyte plasma membrane and indicates the point of “entry.” Sperm motility is required for pene-tration, but not for gamete fusion; the fertilizing sperm-atozoon continues fl agellar movement for around 20 seconds aft er attachment to the oocyte surface.
In small mammals sperm–oocyte fusion is quite advanced aft er 3 minutes, the entire incorporation of the sperm head takes 15 minutes, and pronucleus formation takes about 60 minutes. In some mammals (e.g., the Chinese hamster) the tail is not incorporated, while in others it is incorporated by the progressive fusion of the oocyte and spermatozoal plasma mem-branes. Aft er incorporation, the midpiece mitochon-dria and axial fi lament of the tail appear to disintegrate. Immediately aft er fusion, the sperm plasma membrane

Chapter 4: Sperm–oocyte interaction
55
remains localized to the point of entry, integrated into the oocyte plasma membrane, but by the time that the pronuclei have formed, sperm surface antigen has spread all over the surface of the zygote.
The cortical reaction Cortical granules (CG) are spherical membrane-bound organelles containing enzymes and mucopolysaccha-rides that lie peripherally in the oocyte ( Figure 4.3 ).
Immediately aft er sperm penetration these granules fuse with the oocyte plasma membrane and release their contents into the perivitelline space by exocyt-osis – this cortical reaction is the fi rst morphological indication of oocyte activation . Th e cortical reaction elicits the zona reaction (zona hardening), changing the characteristics of the zona pellucida , and at the same time the egg plasma membrane becomes a mosaic of cortical granule membrane and original plasma mem-brane. In mammalian oocytes the change is dramatic
Table 4.2 Expression of factors during late stages of oogenesis in preparation for fertilization
G2 →M phase
First meiotic block Second meiotic block
Germinal vesicle
Germinal vesicle breakdown
Metaphase I First polar body
Metaphase II Post fertilization
Phos p34cdc2 ++ – – – – ++
Active p34cdc2 – ++ ++ ++ ++ –
MPF – ++ ++ – ++ –
c-mos + + ++ ++ ++ –
MAPK – ++ ++ ++ ++ –
cAMP ++ – – – – –
(a) (b) Figure 4.2 (a) Transmission electron micrograph showing the point of sperm–oocyte fusion in the sea urchin. Sperm factor must fl ow through this cytoplasmic bridge of 0.1 μm diameter. The large granule (1 μm) below the spermatozoon is a cortical granule (from Dale, 1983). (b) Stages in sperm–oocyte fusion in the mammal. Modifi ed from Yanagimachi ( 1994 ).

Chapter 4: Sperm–oocyte interaction
56
and rapid, does not require any new protein synthesis within the cell, but seems to be related to metabolic de-repression of the oocyte. Th e resulting transient increase in surface area due to CG/oolemma fusion facilitates the necessary increase in metabolic turnover required by the activated oocyte. In the mouse, the action of proteinases or glycosidases results in hydroly-sis of ZP3 receptors, which prevent them from further interaction with sperm – this is known as the vitelline block ; the changes that take place via the cortical reac-tion may have evolved specifi cally as polyspermy-pre-venting mechanisms.
Th e early embryo is a compact mass of cells that are continually dividing, and the embryo is continu-ally changing shape. Such movement would be hin-dered if the cells were attached to a rigid structure, and the fl uid-fi lled perivitelline space (PVS) acts as fl exible boundary that allows movement, while the hardened zona provides a protective structure. Th e PVS may also serve as a microenvironment, buff ering the embryo from changes in its external environment. Th e hardened ZP keeps the dividing blastomeres of the embryo in close contact, and protects them from potential microbial invasion. Th e embryo remains in this protective zona coat until hatching, just prior to implantation.
Aft er penetrating the zona and oolemma, the naked sperm nucleus enters the oocyte cortex, moves laterally, rotates approximately 180 degrees, and during the next 10 minutes starts to develop into the male pronucleus. Th e mitochondria and tail of the spermatozoon also enter the cytoplasm but later degenerate.
Release from meiotic arrest Th e universal messenger that triggers reinitiation of meiosis in oocytes at fertilization is an increase in intracellular Ca 2+ released from intracellular stores in periodic waves or transients ( Figure 4.4 ).
A variety of physical and chemical stimuli can par-thenogenetically cause calcium to be released in a simi-lar fashion, but the kinetics of the calcium transients are diff erent, and do not sustain development. Th ere are two hypotheses as to how the spermatozoon trig-gers intracellular Ca 2+ release:
The G-protein hypothesis Th is model for oocyte activation was extrapolated from the events known about calcium response to hormones in somatic cells . Hormone-receptor binding on the outer surface of the plasma membrane signals through a G-protein in the plasma membrane; this signal trig-gers the activation of phospholipase C, leading to the formation of inositol 1,4,5-trisphosphate (IP3) and hence calcium release. Th is model of oocyte activation suggests that the sperm behaves as an “honorary hor-mone” : the attachment of sperm to a sperm receptor triggers IP3 formation through a G-protein linked to this receptor.
The soluble sperm factor hypothesis Th e sperm factor hypothesis , proposed by Dale and colleagues in the early 1980s, suggests that intracellular calcium release is triggered by a diff usible messenger(s) in the cytoplasm of the spermatozoon, which enters the
Figure 4.3 Transmission electron micrographs of the surface of unfertilized oocytes of the sea urchin (a) and human (b), showing the cortical granules.

Chapter 4: Sperm–oocyte interaction
57
oocyte cytoplasm aft er sperm–oocyte fusion. Th e fi rst direct evidence for a soluble sperm factor was shown by microinjecting the soluble components from sperm-atozoa into sea urchin and ascidian oocytes. Several activation events were triggered, including cortical granule exocytosis and gating of plasma membrane currents. Th e same conclusion was reached when the experiment was repeated in mammals. Th e soluble sperm factor hypothesis gained further support with the advent of ICSI in the 1990s, where the events of oocyte activation, including calcium release, occur when the surface membrane events are bypassed.
Soluble extracts of spermatozoa can activate oocytes from diff erent phyla as well as diff erent species: mam-malian oocytes can be partially activated by microin-jecting sea urchin spermatozoa into the cytoplasm. Th us, sperm factors do not appear to be species specifi c, nor indeed phylum specifi c. Sperm extracts can also trigger calcium oscillations in somatic cells , suggest-ing that they may be common calcium-releasing agents rather than sperm-specifi c molecules. It is possible that both soluble sperm factor and membrane transduction mechanisms interact to trigger oocyte activation .
Spermatozoa contain many calcium-releasing molecules, including adenosine diphosphate ribose (ADPr), IP3, nicotinamide nucleotide metabolites, calcium ions and relatively large proteins. Recently phospholipase C zeta 1, identifi ed in mammalian and human sperm, has been shown to trigger calcium release and lead to oocyte activation. Mammals, together with
sea urchins and ascidians, belong to the deuterostome group of animals that show remarkable similarities in gamete physiology. Since changes in plasma membrane conductance, calcium ion release and MPF inactiva-tion are common to all these oocytes at fertilization, the sperm-borne trigger might also be expected to be common. It remains to be seen if phospholipase C zeta 1 is found in the spermatozoa of these other deuteros-tomes and indeed if this lipase triggers other activation events in the mammalian oocyte such as the ADPr/NO pathway (Dale et al. , 2010 ).
Intracellular calcium release
The pattern of calcium release at fertilization varies from species to species. There are three categories of calcium release mechanisms in oocytes, related to the type of receptor on the intracellular calcium store:
1. Inositol 1,4,5-trisphosphate (IP3)-induced calcium release (IICR) . IP3 is produced by the action of phospholipase C on plasma membrane lipid phos-phatidylinositol bisphosphate, and IICR is triggered by the binding of IP3 to its receptor on the endo-plasmic reticulum.
2. Calcium-induced calcium release (CICR) . CICR is trig-gered by opening the ryanodine receptor on an intracellular store, but can also be triggered in a mechanism involving the IP3 receptor. This can also be triggered by calcium itself, and appears to be modulated by cyclic ADP ribose. Cyclic ADP ribose is, in turn, produced by metabolism of nicotinamide
The pattern of calcium release at fertilization variesfrom species to species. There are three categories of calcium release mechanisms in oocytes, related tothe type of receptor on the intracellular calciumstore:
1. Inositol 1,4,5-trisphosphate (IP3)-induced calciumrelease (IICR) . IP3 is produced by the action of phospholipase C on plasma membrane lipid phos-phatidylinositol bisphosphate, and IICR is triggeredby the binding of IP3 to its receptor on the endo-plasmic reticulum.
2. Calcium-induced calcium release (CICR) . CICR is trig-gered by opening the ryanodine receptor on anintracellular store, but can also be triggered in amechanism involving the IP3 receptor. This can alsobe triggered by calcium itself, and appears to bemodulated by cyclic ADP ribose. Cyclic ADP ribose is, in turn, produced by metabolism of nicotinamide
MPF(active)
MPF(active)
Meiosiscompletion
MPF(inactive)
METAPHASE I METAPHASE II
ER
Ca2
ADPr
NO
DAGPIP2
IP3
Spermfactor(s)
FertilizationChannel(cations)
Figure 4.4 Schematic showing the likely mechanisms involved in ascidian oocyte activation after being triggered by the fertilizing sperm. IP3 = inositol 1,4,5-trisphosphate; NO = nitric oxide; DAG = diacylglycerol; PIP2 = phosphati-dylinositol-4,5-bisphosphate (from Dale et al ., 1999).

Chapter 4: Sperm–oocyte interaction
58
adenine diphosphate (NAD + ) by ADP ribosyl cyclase or NAD + glycohydrolase.
3. NAADP+-induced calcium release . Other calcium-releasing second messengers have been identifi ed, including cATP ribose and NAADP+. Since NAD+, NADH, NADP+ and NADPH can be metabolized to calcium-releasing second messengers in sea urchin microsomes, it is possible that other calcium-re-leasing second messengers may be discovered in the nicotinamide nucleotide family.
In mammalian oocytes there is a large increase in the sensitivity to CICR at fertilization, together with a series of repetitive calcium spikes. This again suggests that both CICR and IICR are activated at fertilization.
Centrosomes and centrioles Th e centrosome provides the “division center” for the new zygote, forming the basis for the mitotic spindle that guides the chromosomes through their process of duplication and division. In studies on sea urchins and roundworms at the turn of the century, Boveri at the Stazione Zoologica in Naples showed that the male gamete provided this “division center” for the zygote, and predicted that the structure is a cyclical reprodu-cing organ of the cell. Th e centrosome is paternal in origin, contributed by the sperm – two notable excep-tions to this are the mouse and hamster, where it is apparently maternal in origin, lending support to the observation that these rodents are poor model systems for human fertilization. In frogs, however, although the centrosome is contributed by the sperm, it lacks tubulin, which is needed for microtubule nucleation. Tubulin is provided by the oocyte cytoplasm, and therefore the functional frog centrosome is a mosaic of paternal and maternal components.
In somatic cells the centrosome is composed of two structures known as centrioles ( Figure 4.5 ), which are made up of nine triplets of microtubules arranged in a pinwheel shape. Th ese centrioles are placed at right angles to each other, and are surrounded by dense peri-centriolar material. During interphase, the cent rosome divides to form the poles of the mitotic spindle; aft er division, this segregates with the chromosomes to each of the daughter cells. In contrast, during oogenesis the centrosome degenerates aft er meiosis, leaving the oocyte without a “division center” – this is then con-tributed by the sperm during fertilization. Th e sperm centrosome has a functional proximal centriole , close to the nucleus, and a degenerate distal centriole.
Aft er the sperm enters the oocyte a small “aster” of microtubules grows out from the centriole, and this aster directs the migration of the sperm pronucleus to the center of the oocyte to make contact with the decondensing maternal pronucleus. Th is initiates the migration of the maternal pronucleus towards the for-ming male pronucleus. Microtubules extend from a point in between the now juxtaposed male and female pronuclei, and the centrioles duplicate and migrate to opposite poles during mitotic prophase to set up the fi rst mitotic spindle of the zygote. Th e zygotic centrosome duplicates and then splits apart during interphase.
Although the centrioles are the main organelles associated with cell division, it is now thought that the pericentriolar material may be principally responsible for organizing the microtubules. In cases of polyspermy, when the oocyte is fertilized by more than one sperm, human oocytes develop multiple asters, each associ-ated with a sperm.
Parthenogenetically activated cattle and human oocytes can organize their microtubules without sperm entry, but this takes place later, and less completely than it does aft er sperm entry. Defective centrosome func-tion can result in fertilization failure – microtubules are present in the second meiotic spindle of unfertil-ized oocytes that are arrested in metaphase. During parthenogenesis , where there is no sperm to contribute a centrosome, there is no aster of nucleated microtu-bules, and the microtubules are found in the cytoplasm throughout the oocyte. In this case, the female centro-some becomes functional, duplicating and forming the mitotic spindle poles.
Six hours post insemination, a small microtubule sperm aster extends from the sperm centrosome , and the activated egg extrudes the second polar body.
Pronucleus formation During spermatogenesis , gene expression is repressed, DNA replication ceases, and sperm chromatin is tightly packed into a nuclear envelope that lacks pores. Th e mammalian sperm nucleus is packed with pro-teins that contain highly charged basic amino acids (protamines) that condense the DNA and repress tran-scription. Extensive disulfi de linking in the protamines make the sperm head rigid, a property that is necessary for penetration of the zona. Protamine crosslinking in the human spermatozoon is regulated by Zn 2+ present in prostatic gland secretions. When the sperm nucleus enters the oocyte cytoplasm, the process is reversed,
adenine diphosphate (NAD+) by ADP ribosyl cyclaseor NAD + glycohydrolase.
3. NAADP+-induced calcium release . Other calcium-releasing second messengers have been identifi ed,including cATP ribose and NAADP+. Since NAD+,NADH, NADP+ and NADPH can be metabolized tocalcium-releasing second messengers in sea urchinmicrosomes, it is possible that other calcium-re-leasing second messengers may be discovered inthe nicotinamide nucleotide family.
In mammalian oocytes there is a large increase inthe sensitivity to CICR at fertilization, together with aseries of repetitive calcium spikes. This again suggeststhat both CICR and IICR are activated at fertilization.

Chapter 4: Sperm–oocyte interaction
59
with changes in morphology and biochemical proc-esses. Th e sperm nuclear membrane breaks down, and under the infl uence of factors in the oocyte cyto-plasm , the highly condensed chromatin starts to swell and become dispersed, so that fi laments of chromatin are released into the cytoplasm. Th e factors that cause decondensation are apparently not species-specifi c, since human sperm can decondense when microin-jected into an amphibian oocyte – a reduced form of glutathione is probably responsible for facilitating the process, by reducing disulfi de bonds in sperm nuclear protamines.
Th e mammalian oocyte is in metaphase II stage at the time of sperm entry; the sperm nuclear envelope dissolves and chromatin starts to decondense while the oocyte transits from metaphase II to telophase II. During telophase II, the sperm chromatin completes its decondensation as the female pronucleus develops. Sperm protamines are replaced by histones, and the male and female pronuclear envelopes then develop synchronously. Recent research, however, suggests that paternal histones delivered to the egg are retained in the male pronucleus and contribute to zygotic chro-matin (van der Heijdn et al. , 2008 ). Between 4 and 7 hours aft er fusion, a new nuclear membrane forms around the decondensed male and female chromatin, creating pronuclei that contain the two sets of haploid chromosomes. Oocyte cytoplasm contains factors that are necessary for the development of the male pro-nucleus; these factors are again not species-specifi c, since human spermatozoa can develop into normal pronuclei in hamster oocytes, and form a normal
chromosome complement. In hamster oocytes, a max-imum of fi ve pronuclei will decondense at any time, indicating that the factors may be present in limited quantities.
In the bovine system, sperm tagged with a mitochon-drion-specifi c vital dye have been used to follow sperm incorporation and the conversion of sperm-derived components within the zygote. Th e zygotes were then fi xed at various times aft er fertilization for immuno-chemistry and ultrastructural studies. Th ese experi-ments showed that complete incorporation of the sperm can be inhibited by the microfi lament disrupter cyto-chalasin B, and therefore this process depends upon the integrity of oocyte microfi laments. Aft er sperm incorp-oration, the mitochondria were displaced from the sperm midpiece, and the sperm centriole was exposed to egg cytoplasm. Th e microtubule-based sperm aster then formed, initiating union of male and female pronuclei. Th e disassembly of the sperm tail occurred as a series of precisely orchestrated events, involving the destruction and transformation of particular sperm structures into zygotic and embryonic components.
Nucleolar precursor bodies and nucleoli When the two pronuclei are formed in the zygote, they contain structures known as nucleolar precursor bod-ies (NPBs) ; the number and pattern displayed by their arrangement became popular as criteria for evaluating the embryonic potential of individual zygotes (Tesarik and Greco, 1999 ; Scott et al ., 2000 ). Spermatozoal nucleoli are destroyed during spermatogenesis (Schulz
Microtubule Centromere Chromosomes Centrioles Figure 4.5 Schematic representation of the spindle apparatus, showing centrioles, microtubules and chromosomes with centromeres.

Chapter 4: Sperm–oocyte interaction
60
and Leblond, 1990 ), and recent evidence has shown that oocyte nucleolar material is required for the reassembly of nucleoli in both female and male pro-nuclei (Ogushi et al. , 2008 ).
Tesarik and colleagues ( 1986 , 1988 ) described the mechanism of NPB and nucleolar formation in human embryos, a scheme that diff ers from the process that takes place during the diff erentiation of adult somatic cells . In somatic cells, nucleoli are periodically recon-stituted during mitotic telophase, with fi rst a dense fi brillar component and then a granular component appearing around specifi c loci on chromosomes bear-ing rRNA genes , usually located at or close to a second-ary constriction. In contrast, rDNA of the mammalian zygote and embryo appears to be incapable of starting transcription and thus triggering the nucleogenetic process unless it is associated with nuclear precursors.
Th e sequence of events described by Tesarik and colleagues for human embryos involves four stages: 1. Transcriptionally inactive rDNA has not yet
penetrated into the homogeneous nuclear precursor (pre-nucleoli).
2. rDNA penetrates into the heterogeneous nuclear precursor and turns on the synthesis of pre-rRNA, whose processing is still inactive.
3. Processing of pre-rRNA is progressively activated in compact fi bro-granular nucleoli.
4. Active pre-rRNA synthesis and processing occur in reticulated nucleoli.
Th is scheme, however, did not include information about the paternal or maternal origin of the compo-nents. Th e oocyte nucleolus is derived from material that is present in the germinal vesicle, and its content may change during the process of oocyte maturation . It is composed of approximately 700 proteins, with roles in many cellular processes, including cell cycle regu-lation and apoptosis . Ogushi et al. ( 2008 ) conducted a series of experiments leading to the conclusion that the nucleoli of both male and female pronuclei are maternal in origin, derived exclusively from maternal nucleolar remnants retained at the time of GVBD. Microsurgical removal of murine and pig oocyte nucleoli during pro-phase I indicated that the nucleoli did not contain the factors necessary for oocyte maturation. However, aft er fertilization of mature oocytes without nucleoli, no nucleoli were then visible in the resulting zygote pronuclei, and these zygotes could not complete devel-opment to blastocyst stage . Transfer of GVs to recipient cytoplasts indicated that material(s) within the mature
oocyte GV, showing a ring of condensed chromatin around the nucleolus just prior to GVBD, is essential for full-term development. Although the oocyte nucle-olus is clearly involved, the factors have not been iden-tifi ed, and may include precursor molecules required for the assembly of fully functional nucleoli at a later stage in the development of the embryo.
Lefèvre ( 2008 ) described and summarized these experiments: “Th e nucleoli of the two pronuclei are exclusively of maternal origin, and the oocyte nucle-olar material is essential for the reassembly of nucleoli in both male and female pronuclei.”
Syngamy Aft er the male and female pronuclei are formed, over the next few hours they gradually migrate to the cen-ter of the oocyte, until they are adjacent to each other. During this period DNA is synthesized, in preparation for the fi rst mitotic division. Th e process of migration has been studied extensively in the sea urchin and the mouse. In the mouse, fl uorescein conjugated probes for cytoskeletal elements show a thickened area of micro-fi laments below the cortex of the polar body region. In addition to the spindle microtubules there are 16 cyto-plasmic microtubule organizing centers (MTOCs) or foci, and each centrosomal focus organizes an aster. Th ese foci condense on the surface of the envelope just before the pronuclear membranes disintegrate. Th e mitotic metaphase spindle then forms, which involves duplication of the proximal centriole contributed by the sperm centrosome to form a pair of polar centri-oles, and the chromosomes are aligned along the spin-dle equator. Th e plane of cell division is mediated by astral microtubules that extend from the mitotic spin-dle to the plasma membrane. Between 18 and 24 hours aft er gamete fusion, the two sets of chromosomes come together in syngamy ( Figure 4.6 ), a cleavage furrow forms as soon as the fi rst mitotic anaphase and telo-phase are completed, and the zygote becomes a two-cell embryo.
“The sun in the egg” Leopold Auerbach of Breslau, Germany (1828–1897) described two protoplasmic vacuoles in a newly ferti-lized egg, as well as a radiating fi gure between them. In 1876, Oscar Hertwig identifi ed these vacuoles as the male and female pronuclei ( Figure 4.7 ), and he observed their fusion. When the two nuclei merged together in syngamy, he described the fi gure:

Chapter 4: Sperm–oocyte interaction
61
Es entsteht so vollstandig das Bild einer Sonner im Ei. It arises to completion like a sun within the egg.
In an analysis of Hertwig’s paper, Paul Weindling ( 1991 ) proposed, “Th is vivid image conveyed the dis-covery of the moment at which a new life was formed. Th e metaphor expressed awareness that the force of natural powers was greater than the sum of two cells.”
Further reading Auerbach L ( 1874 ) Organologische Studien . Breslau . Boveri T ( 1902 ) Über mehrpolige Mitosen als Mittel zur
Analyse des Zellkerns . Verhandlungen der physicalisch-medizinischen Gesselschaft zu Würzburg N.F. 35 : 67 –90.
Breitbart H , Spungin B ( 1997 ) Th e biochemistry of the acrosome reaction . Molecular Human Reproduction 3 (3): 195 –202.
Cohen-Dayag A , Tur-Kaspa I , Dor J , Mashiach S , Eisenbach M ( 1995 ) Sperm capacitation in humans is transient and correlates with chemotactic responsivness to follicular factors . Proceedings of the National Academy of Sciences 92 : 11039 –11043.
Collas P ( 1998 ) Cytoplasmic control of nuclear assembly . Reproduction, Fertility, and Development 10 : 581 –592.
Collas P , Poccia D ( 1998 ) Remodeling the sperm nucleus into a male pronucleus at fertilization . Th eriogenology 49 (1): 67 –81.
Conner SJ , Lefi evre L , Hughes DC , Barratt CL ( 2005 ) Cracking the egg: increased complexity in the zona pellucida . Human Reproduction 20 : 1148 –1152.
Dale B (1983) Fertilization in animals . Edward Arnold, London.
Dale B , DeFelice LJ ( 1990 ) Soluble sperm factors, electrical events and egg activation. In: Dale B. (ed.) Mechanism of Fertilization: Plants to Humans . Springer , Berlin (NATO ASI cell biology ser H 45).
Dale B, Di Matteo L, Marino M, Russo G, Wilding M (1999) Soluble sperm activating factor. In “Th e Male Gamete: from basic knowledge to clinical applications”. Cache Rover Press, Il, USA.
Dale B , Monroy A ( 1981 ) How is polyspermy prevented? Gamete Research 4 : 151 –169.
Dale B , Marino M , Wilding M ( 1998 ) Soluble sperm factor, factors or receptors . Molecular Human Reproduction 5 : 1 –4.
Dale B , Tosti E , Iaccarino M ( 1995 ) Is the plasma membrane of the human oocyte reorganized following fertilisation and early cleavage? Zygote 3 (1): 31 –36.
Figure 4.6 A drawing from Wilson ( 1900 ) showing (left) the fusion of male (m) and female (f) pronuclei to form the zygote nucleus as in sea urchins. In the majority of animals (and usually in mammals) the pronuclear membranes break down without fusing, allowing the chromosomes to interact in the cytoplasm (frames on the right). pb = polar body.
Figure 4.7 Fertilized oocyte with two pronuclei and two polar bodies clearly visible; nucleolar precursor bodies are aligned in the pronuclei.

Chapter 4: Sperm–oocyte interaction
62
Dale B , Wilding M , Coppola G , Tosti E ( 2010 ) How do spermatozoa activate oocytes . Reproductive Biomedicine Online 21 : 1 –3.
Davidson EH ( 1990 ) How embryos work: a comparative view of diverse modes of cell fate specifi cation . Development 108 : 365 –389.
Edwards RG ( 1982 ) Conception in the Human Female . Academic Press , New York .
Eisenbach M , Ralt D ( 1992 ) Precontact mammalian sperm-egg communication and role in fertilization . American Journal of Physiology 262 : 1095 –1101.
Fleming TA , Johnson MH ( 1988 ) From egg to epithelium . Annual Review of Cell Biology 4 : 459 –485.
Foltz KR , Lennarz WJ ( 1993 ) Th e molecular basis of sea urchin gamete interactions at the egg plasma membrane . Developmental Biology 158 : 46 –61.
Gianaroli L , Tosti E , Magli C , Ferrarreti A , Dale B ( 1994 ) Th e fertilization current in the human oocyte . Molecular Reproduction and Development 38 : 209 –214.
Gur Y , Breitbart H ( 2006 ) Mammalian sperm translate nuclear-encoded proteins by mitochondrial-type ribosomes . Genes and Development 20 (4): 411 –416.
Gwatkin R ( 1974 ) Fertilization Mechanisms in Man and Mammals . Plenum Press , New York .
Hertwig O ( 1876 ) Beiträge zur Kenntniss der Bildung, Befruchtung und Th eilung des thierischen Eies . Morphologische Jahrbuch 1 : 347 –434.
Hewitson L , Simerley C , Schatten G ( 1999 ) ICSI: Unravelling the mysteries . Alpha Newsletter vol. 17 (May 1999), and Nature Medicine 5 (4): 431 –433.
Holy J , Schatten G ( 1991 ) Spindle pole centrosomes of sea urchin embryos are partially composed of material recruited from maternal stores . Developmental Biology 147 : 343 –53.
Jaff e L ( 1980 ) Calcium explosions as triggers of development . Annals of the New York Academy of Sciences 339 : 86 –101.
Lanzafame F , Chapman M , Guglielmino A , Gearon CM , Forman RG ( 1994 ) Pharmacological stimulation of sperm motility . Human Reproduction 9 (2): 192 –194.
Lauria A , Gandolfi E , Enne G , Gianaroli L (eds.) ( 1998 ) Gametes: Development and Function . Serono Symposia , Rome .
Lefèvre B ( 2008 ) Th e nucleolus of the maternal gamete is essential for life . Bioassays 30 : 613 –616.
Lefi evre L , Conner SJ , Salpekar A , et al . ( 2004 ) Four zona pellucida glycoproteins are expressed in the human . Human Reproduction 19 : 1580 –1586.
Lennarz WJ ( 1994 ) Fertilization in sea urchins: how many diff erent molecules are involved in gamete interaction and fusion? Zygote 2 (1): 1 –4.
Maro B , Gueth-Hallonet C , Aghion J , Antony C ( 1991 ) Cell polarity and microtubule organization during mouse early embryogenesis . Development Supplement 10 : 17 –25.
Myles DG ( 1992 ) Molecular mechanism of sperm-egg membrane binding and fusion in mammals . Developmental Biology 158 : 35 –45.
Nasr-Esfahani MH , Razavi S , Mardani M , Shirazi R , Javanmardi S ( 2007 ) Eff ects of failed oocyte activation and sperm protamine defi ciency on fertilization post-ICSI . Reproductive Biomedicine Online 14 (4): 422 –429.
Nuccitelli R , Cherr G , Clark A ( 1989 ) Mechanisms of Egg Activation . Plenum Press , New York .
Ogushi S , Palmieri C , Fulka H , et al. ( 2008 ) Th e maternal nucleolus is essential for early embryonic development in mammals . Science 319 : 613 –616.
Patrat C , Auer J , Fauque P , et al . ( 2006 ) Zona pellucida from fertilised human oocytes induces a voltage-dependent calcium infl ux and the acrosome reaction in spermatozoa, but cannot be penetrated by sperm . BMC Developmental Biology 6 : 59 .
Ralt D , Goldenber M , Fetterolf P , et al . ( 1991 ) Sperm attraction to follicular factors correlates with human egg fertilizability . Proceedings of the National Academy of Sciences of the USA 88 : 2840 –2844.
Santella L , Alikani M , Talansky B. , Cohen J , Dale B ( 1992 ) Is the human oocyte plasma membrane polarized? Human Reproduction 7 : 999 –1003.
Schatten G ( 1994 ) Th e centrosome and its mode of inheritance: the reduction of the centrosome during gametogenesis and its restoration during fertilization . Developmental Biology 165 (2): 299 –335.
Schatten G , Simerly C , Schatten H ( 1991 ) Maternal inheritance of centrosomes in mammals; studies on parthenogenesis and polyspermy in mice . Proceedings of the National Academy of Sciences of the USA 88 (15): 6785 –6789.
Schulz MC , Leblond CP ( 1990 ) Nucleolar structure and synthetic activity during meiotic prophase and spermiogenesis in the rat . American Journal of Anatomy 189 : 1 –10.
Scott L , Alvero R , Leondires M , et al . ( 2000 ) Th e morphology of human pronuclear embryos is positively related to blastocyst development and implantation . Human Reproduction 15 : 2394 –2403.
Shapiro S ( 1987 ) Th e existential decision of a sperm . Cell 49 : 293 –294.
Simerly C , Wu G , Zoran S , et al. ( 1995 ) Th e paternal inheritance of the centrosome, the cell’s microtubule-organising center, in humans and the implications of infertility . Nature Medicine 1 : 47 –53.
Sutovsky P , Navara CS , Schatten G ( 1996 ) Fate of the sperm mitochondria, and the incorporation, conversion, and disassembly of the sperm tail structures during

Chapter 4: Sperm–oocyte interaction
63
bovine fertilization . Biology of Reproduction 55 : 1195 –1205.
Tesarik J , Greco E ( 1999 ) Th e probability of abnormal preimplantation development can be predicted by a single static observation on pronuclear stage morphology . Human Reproduction 14 : 1318 –1323.
Tesarik J , Kopecny V ( 1989a ) Developmental control of the human male pronucleus by ooplasmic factors . Human Reproduction 4 : 962 –968.
Tesarik J , Kopecny V ( 1989b ) Nucleic acid synthesis and development of human male pronucleus . Journal of Reproduction and Fertility 86 : 549 –558.
Tesarik J , Kopecny V ( 1989c ) Development of human male pronucleus: ultrastructure and timing . Gamete Research 24 : 135 –149
Tesarik J , Kopecny V , Plachot M , Mandelbaum J ( 1988 ) Early morphological signs of embryonic genome expression in human preimplantation development as revealed by quantitative electron microscopy . Developmental Biology 128 : 15 –20.
Tesarik J , Kopecny V , Plachot M , Mandelbaum J , Da Lage C , Fléchon J-E ( 1986 ) Nucleologenesis in the human embryo developing in vitro: ultrastructural and autoradiographic analysis . Developmental Biology 115 , 193 –203
Tesarik I , Sousa M , Testart J ( 1994 ) Human oocyte activation aft er intracytoplasmic sperm injection . Human Reproduction 9 : 511 –514.
Tosti E ( 1994 ) Sperm activation in species with external fertilization . Zygote 2 (4): 359 –361.
Van der Heijdn GW , Ramos L , Baart EB , van den Berg IM , et al . ( 2008 ) Sperm derived histones contribute to zygotic chromatin in humans . BMC Developmental Biology 8 : 34 .
Ward CR , Kopf GS ( 1993 ) Molecular events mediating sperm activation . Developmental Biology 158 : 9 –34.
Wassarman PM ( 1990 ) Profi le of a mammalian sperm receptor . Development 108 : 1 –17.
Wassarman PM , Florman HM , Greve IM ( 1985 ) Receptor-mediated sperm-egg interactions in mammals. In: Metz CB , Monroy A (eds.) Fertilization , vol. 2. Academic Press , New York , pp. 341–360.
Wassarman PM , Liu C , Litscher ES ( 1996 ) Constructing the mammalian egg zona pellucida: some new pieces of an old puzzle . Journal of Cell Science 109 : 2001 –2004.
Weindling PJ ( 1991 ) Darwinism and Social Darwinism in Imperial Germany: Th e Contribution of the Cell Biologist Oscar Hertwig (1849–1922) . G. Fischer Verlag, Stuttgart, p. 71.
Wilson EB ( 1900 ) Th e Cell in Development and Inheritance . Macmillan , London .
Yanagimachi R ( 1981 ) Mechanisms of fertilization in mammals. In: Mastroianni L , Biggers , JD (eds.) Fertilization and Embryonic Development In Vitro . Plenum Press , New York , pp. 81–182.
Yanagimachi R ( 1994 ) Mammalian fertilization. In: Knobil E , Neill J (eds.) Th e Physiology of Reproduction . Raven Press , New York .

Chapter
1
64
First stages of development
Preimplantation development Aft er completing fertilization with fusion of the pro-nuclei during syngamy , the zygote now has a dip-loid complement of chromosomes, undergoes its fi rst mitotic division and then continues to divide by mitosis into a number of smaller cells known as blast-omeres . In humans, the fi rst few cleavage divisions take place in the oviduct, before the embryo reaches its site of implantation in the uterus ( Figure 5.1 ).
In contrast to oogenesis , where the cell undergoes a period of growth without replication or division, early embryo cleavage involves intense DNA replica-tion and cell division in the absence of growth – the overall size of the embryo does not change as a result of the early cleavage divisions. As cleavage progresses, the embryo polarizes, and diff erences arise between the blastomeres; this process of diff erentiation may be regulated by unequal distributions of cytoplasmic components previously laid down in the oocyte during oogenesis , or by changes occurring in the blastomeres as a result of new embryonic gene transcription dur-ing development ( Figure 5.2 ). Each blastomere nucleus will be subjected to a diff erent cytoplasmic environment, which, in turn, may diff erentially infl u-ence activity of the genome. As a result, aft er the onset of zygote gene activation and subsequent diff erenti-ation, eventually the blastomeres set off on their own specifi c program of development. Maternal mRNA encoding developmental information is essential in early diff erentiation, and has been found to per-sist during specifi c patterns of gene expression until gastrulation in some species; embryos in some bats and marsupials can remain in a state of diapause (dor-mancy) within the uterine cavity for many months. In mammals, maternal mRNA rapidly disappears aft er the major activation of the genome, i.e., at the two-cell stage in the mouse, four- to six-cell in humans, and
eight-cell in sheep and cattle. Localized short- and long-lived maternal mRNAs probably regulate the initial stages of diff erentiation; there is some evidence to suggest that stores of maternal RNA in the oocytes of older women may be depleted, perhaps due to dys-function or disruption of the mechanisms that con-trol its storage.
Genome activation As described in Chapter 3 , the developing oocyte accu-mulates reserves of mRNA, proteins, organelles, etc. which are required to support and direct early devel-opment. In vitro, the early embryo shows very little metabolic activity during its fi rst few cleavage divi-sions. Th e zygote initially depends on stored maternal mRNA to direct the fi rst two cleavage divisions, and then activation of the new embryonic genome provides novel transcripts and reprograms the pattern of gene expression to direct further development. Aft er the long period of gene suppression in both gametes, the new embryonic cell cycle must be precisely timed and regulated, with a correct timing of DNA synthesis dur-ing S-phase . Without appropriate zygotic genome acti-vation (ZGA), the mammalian embryo fails to develop further. Th is critical transition takes place during the four- to eight-cell stage in humans, and maternal mRNA rapidly disappears whilst the zygote genome gradually increases its expression. However, the transition is not absolute, and a small amount of maternal message is needed almost up until the blastocyst stage – therefore previous failures at any stage of oocyte development, maturation, and handling can aff ect development even aft er ZGA. Gene expression involves conformational changes in nucleosome organization (like uncoiling a spring), regulated by interactions between DNA methylation , histone acetylation and messenger RNA polyadenylation patterns . Activation of the embryonic
5
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. (©) K. Elder and B. Dale 2011.

Chapter 5: First stages of development
65
genome follows a series of progressive steps; the timing and coordination of gene expression can be regulated at the level of maternal mRNA translation. 1. Maternal RNA transcripts are depleted, and
new embryonic mRNA is transcribed. Th e replacement of maternal transcripts by those of the zygote occurs at diff erent rates for diff erent genes (Temeles et al ., 1994 ); this may be due to the relative importance of diff erent transcripts for immediate developmental events, or because the protein products diff er in their stability, or both.
2. Th ere is a qualitative shift in protein synthesis, and in post-translational modifi cation.
3. A functional nucleosomal structure develops, the nuclear organizing region (NOR) . Establishing the precise timing of genome activation is related to the sensitivity of methods available for its detection; new protein synthesis activity has been detected at diff erent stages in diff erent species:
Th ere is evidence to suggest that a minor degree of tran-scriptional activity does take place prior to the major activation of the genome, with a period of minor gene activation from the paternal pronucleus in the one-cell embryo, followed by a period of gene activation in the two-cell embryo when maternal mRNA and zyg-otic gene transcripts are handled diff erently, so that transcription and translation of nascent transcripts is delayed (Wiekowski et al ., 1991 ; Nothias et al ., 1995 ;
Figure 5.1 Development of the mammalian embryo. The oocytes released from the ovary (OV) enter the ampulla where they are fertilized (F) and then are transported along the fallopian tube, cleaving to generate the morula stage (M). The blastocyst expands, hatches and then implants in the endometrium (E) of the uterus. From Sathananthan et al . ( 1993 ).
Rabbit 1–2 cells
Mouse 2 cells
Cow 4–8 cells
Human 4 cells
Sheep 8–16 cells
Drosophila 4000 cells
Xenopus 5000 cells

Chapter 5: First stages of development
66
Schultz, 2002 ). In human preimplantation embryos, reverse transcriptase-polymerase chain reaction (RT-PCR) detected early transcripts for two paternal Y chromosome genes, ZFY and SRY . ZFY transcripts were detected at the pronucleate stage, 20–24 hours aft er in-vitro insemination, and at intermediate stages up to the blastocyst stage. SRY transcripts were also detected at two-cell to blastocyst stages (Ao et al ., 1994 ).
Cleavage increases the number of nuclei, which amplifi es the number of templates that will facilitate the production of specialized proteins needed for the later processes of compaction and diff erentiation to the blastocyst stage. Changes in chromatin structure, rather than changes in the activity of the transcrip-tional apparatus, may underlie the timing and basis for ZGA. Transcription factors must be available that can bind to the DNA, and a functional physical structure, the nuclear organizing region (NOR) develops, pro-ducing conformational changes in the DNA structure that will allow the binding of promoters and enhanc-ers of transcription. In the mouse and rabbit, there is a general chromatin-mediated repression of promoter
activity. Repression factors are inherited by the mater-nal pronucleus from the oocyte, but are absent in the paternal pronucleus; they become available sometime during the transition from a late one-cell to a two-cell embryo (Henery et al ., 1995 ). Th is means that pater-nally inherited genes are exposed to a diff erent envir-onment in fertilized eggs than are maternally inherited genes, a situation that could contribute to genomic imprinting.
Th e formation of the NOR is related to the nuclear:cytoplasmic ratio. A titratable factor in the cytoplasm, possibly related to cdc25, may be diluted with the increase in nuclear:cytoplasmic ratio, driv-ing maturation promoting factor (MPF) and a kinase cascade that triggers mitosis . Th e gradual depletion of cdc25 causes a pause in cleavage, which allows time for the nuclear organizing region to develop, and mitosis induces a general repression of promoters prior to ini-tiation of zygotic gene expression. Enhancers then spe-cifi cally release this repression. A biological clock may delay transcription until both paternal and maternal genomes are replicated; they must then be remodeled from a postmeiotic state to one in which transcription
Figure 5.2 Timescale of early human embryo development up to the blastocyst stage, correlating morphological changes with developmental events. Time is in hours.

Chapter 5: First stages of development
67
is repressed by chromatin structure. Th e chromatin structure must have a confi guration that allows specifi c transcription enhancers to relieve/reverse repression at appropriate times during development. Diff erential hyperacetylation of histone H4 (particularly on DNA in the male pronucleus) has been implicated in the remodeling of maternal and paternal chromatin, and depletion of maternally derived histones has also been suggested as one of the mechanisms involved in ZGA (Adenot et al ., 1997 ).
Chromatin-mediated repression of promoter activity prior to ZGA is similar to that observed during Xenopus embryogenesis ; this mechanism ensures that genes are not expressed until the appropriate time in development. When the time is right, positive factors such as enhancers can begin their activity. Th e mech-anism by which enhancers communicate with promot-ers seems to change during development, and may depend upon the presence of specifi c co-activators. In the mouse, ZGA occurs during the second cell division cycle (two-cell stage) and seems to be regulated by a “zygotic clock” that measures the time following fer-tilization rather than progression through the fi rst cell cycle . Th ere is evidence that circadian clock genes may be involved in programming an appropriate timing, so that development is synchronized with endocrine and other local factors to ensure successful implantation. In support of this concept, expression of circadian clock genes has been found in the reproductive tract and conceptus of the mouse during the fi rst four days of pregnancy (Johnson et al ., 2002 ). It may be that in vivo, mammalian ZGA is a time-dependent mechan-ism that must interact in synchrony with the cell cycle and other physiological events.
Imprinting During oogenesis and spermatogenesis , the maternal and paternal chromosomes are packaged in a manner that aff ects subsequent transcription of some of the genes during development. Th e DNA sequence that specifi es the parental genes is not altered, but the way in which it is chemically modifi ed and packaged in chro-matin aff ects the expression of the genes. Because the genetic code itself remains the same, this modifi cation is referred to as an epigenetic change , and the phenom-enon is known as imprinting . Th e pattern of epigen-etic change is parentally specifi c, i.e., the genes aff ected (imprinted) in oocytes diff er from those imprinted in sperm – there is diff erential expression of the two par-ental alleles of a gene. In terms of function, this means
that although the oocyte and the sperm each contribute a complete set of genes, each set on its own is not com-petent to direct a complete program of development; a fully functional genome requires the combination of both paternal and maternal genes. Th e process of gen-omic imprinting is established during gametogenesis , and the nucleus of the zygote has an imprint memory that is retained by the embryo into both prenatal and postnatal life. Imprinting is highly regulated during preimplantation development; the topic is thus highly signifi cant and relevant to in-vitro manipulations and culture, and will be discussed in detail in Chapter 15 .
Compaction Th e fi rst event that determines the directed develop-ment of previously undiff erentiated blastomeres is compaction . During the fi rst few cleavage divisions to reach the four- to eight-cell stage, individual blast-omeres can be clearly seen in the developing embryo. At about the third cleavage division there is a signifi -cant increase in RNA and protein synthesis, a marked change in the patterns of phospholipid synthesis, and the embryo undergoes compaction to form a morula. Th is process is calcium-dependent, and requires prior transcription of the zygote genome. With compaction, the blastomeres fl atten against each other and begin to form junctions between them, so that the boundaries between blastomeres can no longer be distinguished. Th e cells of the compacted embryo become highly polarized and tightly associated, with redistribution of surface microvilli and other plasma membrane components.
Coordination of these complex developmen-tal processes requires communication between the cells; two types of intercellular junction have been described: 1. Structural tight junctions and desmosomes anchor
the cells together and form an impermeable epithelial barrier between cells. Tight junctions are composed of several integral and peripheral proteins, including occludin and cingulin (ZO-1).
2. Low resistance junctions such as gap junctions allow the fl ow of electrical current and the direct transfer of small molecules, including metabolites and second messengers (cAMP ) between blastomeres.
Compaction has been extensively studied in the mouse: the distribution of dense microvillar and amicrovillar regions indicates surface polarity, and

Chapter 5: First stages of development
68
the distribution of endocytotic vesicles and actin fi laments, and the location of the cell nucleus dem-onstrates polarity in the cytoplasm. In the mouse, isolated blastomeres that are decompacted experi-mentally maintain their polarity, and compaction does not require either a prior round of DNA repli-cation, or protein synthesis (Kidder and McLachlin, 1985 ). Th erefore, the four-cell embryo probably contains some of the proteins required for compac-tion . Although the factors that trigger the timing of its onset are not known, experimental evidence sug-gests that this may be regulated by post-translational modifi cation of specifi c proteins such as E-cadherin . E-cadherin protein (uvomorulin) is expressed in the oocyte, and during all stages of preimplantation development. It is uniformly distributed on the sur-face of blastomeres and accumulates in the regions of intercellular contact during compaction. E-cadherin phosphorylation can be observed in the mouse eight-cell embryo. Culturing embryos in calcium-free medium inhibits E-cadherin phosphorylation and prevents compaction, but the situation is complex, and precise mechanisms behind the molecular basis for compaction and its timing remain unclear.
In human embryos, tight junctions begin to appear on Day 3, at the 6–10-cell stage, heralding the onset of compaction. Th e surface morphology of human oocytes and embryos has been studied with scanning electron microscopy (Santella et al ., 1992 ; Dale et al ., 1995 ; Nikas et al ., 1996 ), and this showed that unfer-tilized oocytes one day aft er insemination were evenly and densely covered with long microvilli. Th e length and density of microvilli appeared to decrease in fer-tilized oocytes, and a further decrease was observed in Day 2 and Day 3 embryos with 2–12 cells. Th ere was no evidence of surface polarity until Day 4, when it was evident in the majority of embryos with 10 or more cells. Th e microvilli appeared dense again with a polar-ized distribution over the free surface of the compacted blastomeres.
In the mouse, gap junctions are expressed at the 8-cell stage, and their de novo assembly during compaction is a time-dependent event. Inhibition of DNA synthesis during the third and fourth cell cycles has no eff ect on the establishment of gap junctional coupling during compaction (Valdimarsson and Kidder, 1995 ), but a delay of 10 hours in DNA synthe-sis during the second cell cycle results in the failure of gap junctional coupling at the time of compaction.
In human embryos, gap junctions are not apparently well developed until the early blastocyst stage, when intercellular communication is clearly seen between inner cell mass (ICM) cells (Figures 5.3 and 5.4; Dale et al ., 1991 ).
Following compaction, the developing embryo is described as a morula, seen in the human normally 4 days aft er fertilization. Th e embryo now shows a sig-nifi cant increase and change of pattern in RNA, pro-tein and phospholipid synthesis, and this results in a process of diff erentiation so that cells are now allocated to an ICM , with outer cells forming an epithelial layer of trophectoderm. Whereas early blastomeres are toti-potent (as evidenced by experimental embryo split-ting and chimera formation), at compaction the cells polarize radially, and diff erential division across this axis creates diff erent populations of cells, with unequal distributions of organelles: 1. Outer polar cells with surface microvilli and
redistribution of other plasma membrane components are restricted to the free outer surface of the embryo, and these cells form the trophectoderm .
2. Inner apolar cells with tight junctions containing basal nuclei, which will form the ICM.
Th ese morphological transitions are thought to be brought about by diff erential gene expression with corresponding protein expression profi les, but these have not yet been clearly defi ned at the molecular level. Experimental interference with adhesion between cells during compaction shows that this process is important in determining cell lineages. ICM cells pref-erentially communicate with each other and not with trophectoderm cells via gap junctions, whereas troph-ectoderm cells communicate with each other and not with ICM cells. Th e ratio of trophectoderm to ICM cells can be infl uenced by culture conditions in vitro, and this might have implications for further embry-onic/fetal development.
Cavitation Between the 16- and 32-cell stage, a second morpho-logical change occurs, known as cavitation . Activation of Na + , K + ATP-ase systems in the trophectoderm cells results in energy-dependent active transport of sodium pumped into the central area of the embryo, followed by osmotically driven passive movement of water to form a fl uid-fi lled cavity, the blastocoele. Th e

Chapter 5: First stages of development
69
movement of other ions such as chloride and bicar-bonate also contributes to blastocoele formation. Immunohistochemistry shows that the trophecto-derm cells are sitting on a basement membrane, and tight junctions form a continuous belt between troph-ectoderm cells, preventing leakage of small ions in the blastocoelic fl uid.
Blastocoele formation and expansion is critical for further development, as it is essential for further diff er-entiation of the ICM. Th is is now bathed in a specifi c fl uid medium, which may contain factors and proteins that will infl uence cell proliferation and diff erentiation. Th e position of cells within the ICM in relation to the fl uid cavity might also contribute to the diff erentiation of the outer cells into primitive endodermal cells.
Apoptosis can be seen at the blastocyst stage, local-ized to the inner cell mass: this may represent a mech-anism for the elimination of inappropriate or defective cells.
Th e trophectoderm cells will eventually form the placenta and extra-embryonic tissue. Myxoploidy of trophectoderm cells is a common feature in all animal species, regardless of their implantation mechanisms; mouse and cow, which diff er completely in their mech-anism of implantation, show this feature, with chromo-some complements of 2n, 4n, 8n in their trophectoderm
Figure 5.3 Functional expression of gap junc-tions in the early human embryo shown by micro-injection of the low molecular weight tracer lucifer yellow. There is no dye spread in four cells (a), ten cells (b) or morula (c). However, transfer occurs in the blastocyst stage. icm = inner cell mass. From Dale et al ., 1991.
a
b
Figure 5.4 Transmission electron micrographs showing tight junctions (TJR) and gap junctions (G) in the human morula. (a) is a section at the apical level between two polar cells at a magnifi ca-tion of ×75 500; (b) shows a typical section between a polar and an apolar cell at ×158 000. Arrowheads show sites of tight membrane contact. From Gualteri et al ., 1992.

Chapter 5: First stages of development
70
cells . However, in humans it could possibly be consid-ered as the initiation of syncytiotrophoblast formation. Th e regulation of this process, and apparent lack of div-ision in these cells, remains a mystery – but it seems to be related to the appearance of giant cells in the troph-ectoderm, suggesting that regulation of the nuclear/cytoplasmic ratio is involved. It is interesting to note that there is a counterpart of “giant cells” in the uterus around the time of implantation. A retroviral syncytin envelope gene with cell–cell fusion activity has been identifi ed in mammalian syncytiotrophoblast, and is postulated to be responsible for syncytiotrophoblast formation (Heidmann et al ., 2009 ).
Blastocyst expansion and hatching In humans, the early blastocyst (Day 4/5) initially shows no increase in size, but it subsequently expands over the next one or two days (Day 5/6) by active accumulation of fl uid in the central blastocoelic cavity. Th roughout these early stages the embryo is enclosed in the zona pellucida , which keeps the cells together prior to compaction and acts as a protective barrier. If the ICM divides at this early stage, monozygotic (iden-tical) twins may develop. Before the blastocyst can start the process of implantation, it must free itself from the protective zona pellucida, which becomes visibly thinner as the blastocyst expands; in vitro, initiation of the hatching process can be seen as trophectoderm
cells “escaping” from the zona pellucida ( Figure 5.5 ). Hatching is completed within a few hours, and the freed blastocyst is separated from its empty zona (see also Chapter 11 , Figure 11.8 ).
Cell fate and cell lineages At the earliest stages of development the transcrip-tional machinery that will direct diff erentiation is not switched on, and transcription is under the control of specifi c transcriptional regulators, regulatory RNAs and chromatin remodeling machinery, which are in turn infl uenced by epigenetic marks, cell positional history, cell polarity, and orientation of division. As discussed in Chapter 3 , the mammalian oocyte has evidence of polarity, and this has been confi rmed in human oocytes. Maternal factors are subsequently important in establishing polarities, regulating cleav-age planes, and in allocating specifi c blastomeres to their eventual fate. By the morula stage, cell fate deci-sions have been made, and an axis is established with embryonic (ICM) and abembryonic (trophectoderm ) poles. Cells positioned on the inside of the morula retain pluripotency, and those on the outside develop into extraembryonic trophectoderm which will sup-port the development of the embryo in the uterus and infl uence embryonic patterning before gastrulation via signaling mechanisms. Th e generation of inside cells requires outer cells to divide in an orientation
Figure 5.5 Scanning electron micro-graph of a hatching human embryo. The microvilli on the surface of the trophectoderm cells are bared owing to internal pressure in the blastocoele and dissolution of the zona pellucida.

Chapter 5: First stages of development
71
such that one daughter cell is directed inwards during the 8–16-cell and 16–32-cell stages – these divisions are known as diff erentiative, in contrast to conser-vative divisions in which both daughter cells remain on the outside. Because inside and outside cells will follow diff erent fates, diff erentiative divisions prob-ably distribute cell fate-determining factors asym-metrically between the daughters. Several molecules that infl uence polarization have been identifi ed: the Ca 2+ dependent E-cadherin molecule is implicated in generating blastomere polarity, localized geograph-ically at division together with the actin microfi la-ment stabilizing protein ezrin. Homologues of PAR (partitioning defective proteins) also infl uence the regulation of cell polarization and the control of asymmetric cell divisions via positioning eff ects on the spindle. Th e transcription factor Cdx2 is required for the commitment of outer cells to the trophoblast (see Chapter 7 ).
Th e molecular basis for the generation and stabil-ization of polarity in development is not fully under-stood, but evidence is accumulating to suggest that cell fate may be determined as early as the 4-cell stage in human embryos: mRNAs specifi c for a trophectoderm lineage (beta-hCG) were identifi ed in a single blasto-mere of a 4-cell embryo, and not at the 2-cell stage; a single putative trophectodermal precursor appears to emerge during the second cleavage division (Hansis et al ., 2002 ; Edwards and Hansis, 2005 ). In mouse embryos, lineage tracing experiments using fl uorescent tracers and optional sectioning indicate that diff erences in developmental properties of individual blastomeres may be determined at the 2-cell stage (Piotrowska et al ., 2001 , 2005 ). Th ese experiments showed that the fi rst cell to divide to the 4-cell stage contributed preferentially to the embryonic cell lineage, whereas the later-dividing blastomere contributed to the abembryonic (trophecto-derm) lineage. By the blastocyst stage, the position of cells within regions of the blastocyst has an infl uence on their subsequent fate in postimplantation development (Gardner, 2001 , 2007 ).
Causes of early embryo arrest Cleaved embryos do frequently arrest their devel-opment in culture, and a great deal of research has been carried out in animal systems to elucidate pos-sible causes and mechanisms. Th e longest cell division cycle during development is that during which genome activation takes place, when maternal transcripts are
degraded and massive synthesis of embryonic tran-scripts is initiated. Maternal reserves are normally suf-fi cient until transcription begins, but epigenetic eff ects of defective sperm can lead to accumulation of delays, with resulting arrested development. Antisperm anti-bodies can have deleterious eff ects at this stage, by immunoneutralization of proteins that signal division (CS-1) or regulation (Oct-3). Aft er genome activation, the next critical stage is morula/blastocyst transition. Complex remodeling takes place, and poor sperm quality can compromise this transition (see Ménézo and Janny, 1997 ).
Embryonic arrest is frequently a result of events surrounding maturation, but can be a result of any metabolic problem. In bovine and pig oocytes, insuf-fi cient glutathione inhibits decondensation of the sperm head and polar body formation, and genetic factors regulate the speed of preimplantation develop-ment. Genetic factors implicate enzyme defi ciencies or dysfunctional regulation, which may have deleteri-ous eff ects. In domestic animals, as in humans, there is an age-related maternal eff ect. Maternal age has an eff ect on embryo quality, especially on blastocyst for-mation – this may be related to an ATPase dependent Na + /K + pump mechanism, or to a poor stock of mRNA, poor transcriptional and/or post-transcriptional regu-lation, or accelerated turnover of mRNA.
In clinical IVF, detection of two pronuclei is regarded as evidence that normal fertilization has taken place, and the formation of a normal mitotic spindle following fertilization is critical in order to ensure cor-rect chromosomal alignment. Mistakes at this stage can be lethal, resulting in chromosomal disorders such as aneuploidy. In some cases a fi rst cleavage division takes place when no pronuclei have been detected during the previous 24–28 hours, a phenomenon that has been described as “silent fertilization.” Th e fi rst cell division tends to be asymmetrical, and the embryos arrest during cleavage. Van Blerkom et al . ( 2004 ) undertook a multi-year study of oocytes and embryos in which silent fer-tilization was suspected, using scanning laser confocal fl uorescence microscopy to study chromosomal and microtubular structures. Th ey were able to visualize maternally and paternally derived spindles in embryos that had shown no sign of pronuclear evolution aft er multiple, closely-spaced inspections at the 1-cell stage, with maternal and paternal spindles well separated. Th e authors suggest that the evolution of such embryos may have an unusual pattern of chromosomal segregation, leading to micro- or multinucleation. Th e mechanisms

Chapter 5: First stages of development
72
involved in silent fertilization could be due to defects in normal calcium signaling, inadequate cytoplasmic maturity, or delayed release of sperm-derived factors that also modulate calcium signaling.
Fluorescent in-situ hybridization (FISH) analysis of cleaved human embryos has confi rmed that chromo-somal aberrations are found in a signifi cant proportion of embryos which develop with regular cleavage and morphology; this undoubtedly contributes to the high wastage of embryos in human IVF.
Paternal factors Sperm quality may have an infl uence on embryogen-esis and implantation potential. Increasing pater-nal age is thought to have an infl uence on fertility, possibly through increased nondisjunction in the sperm. Damage during spermatogenesis may be induced by reactive oxygen species and defective oxidative phosphorylation, or via inherited dysfunc-tional mitochondrial DNA. Fertilization by a sperm that is diploid, with incomplete decondensation and DNA activation or inadequate chromatin packaging, may cause aneuploidy or lack of genome compe-tence in the embryo. Th e quality of condensation and packaging of sperm DNA are important factors for the initiation of human embryo development, even aft er intracytoplasmic sperm injection (ICSI) . Th e centrosome, involved in microtubular organization, is the fi rst epigenetic contribution of the sperm, and correct and harmonious microtubule arrangement is necessary for chromosome segregation and pro-nuclear migration. An abnormal sperm carrying an imperfect centrosome can disrupt mitosis, pro-voking problems at the beginning of embryogenesis with the formation of fragments, abnormal chromo-some distribution, and early cleavage arrest. Up to 25% of apparently unfertilized eggs may show signs of having initiated fertilization, but then have anom-alies that prevent cell division. In bulls, there is a positive correlation between sperm aster formation at the time of fertilization and the bull’s fertility. In the human, paternal Y-linked genes are transcribed as early as the zygote stage, and compromised pater-nal genetic material could be transcribed at even this early stage, causing fertilization failure or embryonic arrest. Finally, as discussed in Chapter 3 , spermato-zoa lacking in, or with defective oocyte activating factor may only partially activate oocytes and lead to abortive development.
Metabolic requirements of the early mammalian embryo in vitro Yves Ménézo When the oocyte is fertilized and starts the process of transcription, the new embryo must maintain equilib-rium between many diff erent parameters: 1. Th e endogenous pool of metabolites, largely the
result of fi nal stages of oocyte maturation 2. Metabolic turnover of RNA messengers and
proteins 3. Active uptake of sugars, amino acids and nucleic
acid precursors 4. Passive transport, especially of lipids 5. Incorporation of proteins such as albumin, which
can bind lipids, peptides and catecholamines.
ATP as an energy source is a basic requirement, and mammalian cells can generate ATP either by aerobic oxidation of substrates to carbon dioxide and water, or by anaerobic glycolysis of glucose to lactic acid. Under in-vitro conditions, oocytes and embryos generate ATP by aerobic oxidative metabolism of pyruvate, lac-tate, amino acids and possibly lipids. Th ese metabolites have been shown to be important prior to genomic activation; pyruvate can also remove toxic ammonium ions via transamination to alanine.
Pentose phosphate pathway, NADPH and glutathione An important feature of early embryo metabolism is linked to the activation process that is induced by sperm entry, which increases glycolysis and glucose uptake through transporters. Th ese may provide energy by generating ATP, but upregulation of the pentose phosphate pathway (PPP) is a more signifi -cant metabolic parameter during this period. Th e PPP generates ribose 5-phosphate, a nucleotide pre-cursor for subsequent DNA synthesis and replica-tion. Upregulation of glucose metabolism via the PPP requires a fully grown pronucleus; the activity of the PPP infl uences the onset of the fi rst S-phase in both male and female pronuclei, and continues to infl u-ence embryo development up to the blastocyst stage. Th e PPP also generates NADPH, which is involved in the majority of anabolic pathways: 1 mole of glucose 6-phosphate generates 1 mole of ribose 5-phosphate plus 2 moles of NADPH. NADPH further allows

Chapter 5: First stages of development
73
methionine to be recycled from homocysteine, with the formation of folic acid via methylene tetrahydro-folate reductase. Th is pathway infl uences imprinting processes in the oocyte, and is also involved in thy-midine synthesis (5-methyl-uracyl, see section on vitamins, p. 75). NADPH is also required to reduce oxidized glutathione (GSSG). Th e synthesis of gluta-thione from cysteine is energy consuming (ATP), and therefore recycling of GSSG is important, redu-cing energy consumption and decreasing the need for available cysteine.
Glutathione is necessary for sperm head swelling, and the impact of glutathione mobilization on further embryonic development is immediate: an increased blastocyst formation rate is observed, with increased cell number per blastocyst formed. Th is is probably due to the universal role of glutathione in protection against oxidative stress.
Glucose It has been suggested that glucose is toxic during in-vitro culture before genomic activation, and that glucose and phosphate together may inhibit early embryo development. Th e mechanisms proposed include induction of glycolysis at the expense of sub-strate oxidation, through disrupted mitochondrial function. High levels of glucose can lead to excessive free radical formation, but the toxic eff ect is depend-ent upon the overall composition of the media; in some systems the negative eff ect of glucose may be counterbalanced by the presence of a correct amino acid balance, but not by removing “essential amino acids” (Lane and Gardner, 1997 ). Amino acids and EDTA suppress glycolysis through diff erent combin-ations, and act in combination to further suppress glycolysis. Aft er genome activation, glucose becomes a key metabolite, required for lipid, amino acid and nucleic acid synthesis. It is also essential for blasto-cyst hatching.
Lipids Lipids can be synthesized (through C-2 condensa-tion reactions), accumulated from the surrounding medium or carried with albumin. Cholesterol syn-thesis is possible, but slow: there is a rate-limiting step at the level of hMG (3-hydroxy-3-methyl- glutaryl) CoA reductase. If synthesis of cholesterol is experi-mentally inhibited by chetosterol, the embryos arrest and die.
Electrolytes Th e correct balance of electrolytes is always an essen-tial basis for biochemical processes that lead to energy production and cAMP -based regulatory mechanisms. K + and HCO 3 are involved in sperm capacitation, and intracellular pH regulation is a vital aspect of correct homeostasis. HCO 3 has a particular role in activation, via an increase in sperm cAMP levels. Th e carbon from HCO 3 can be incorporated during anabolic processes in the embryo. Iron and copper cations appear to arrest embryo development, encouraging free radical forma-tion – therefore EDTA (or penicillamine) in early stage culture media is benefi cial as a chelating agent (but not in fertilization medium, as it chelates calcium which is essential for sperm motility, capacitation and the acro-some reaction ). EDTA is also a free radical scavenger. A suggestion that EDTA might be deleterious aft er gen-ome activation and should be removed in the second phase of culture has been shown to be invalid.
Amino acids Amino acids are important regulators of embryo development. The concept of “essential and non- essential” amino acids is not valid for preimplan-tation development, as their role is unlikely to be equivalent to their definition as “essential” in terms of nutrition for the entire individual. The ratio between different amino acids appears to be more important than their actual concentration in cul-ture media, as they compete with each other for membrane transport systems. Differing affinities for transport mechanisms mean that disequilibrium in the external milieu will be reflected in anomalies of the endogenous pool, with potentially deleteri-ous effects on protein synthesis. Active transport mechanisms have been confirmed by the finding that amino acids are found at a higher concentration inside embryos than in the surrounding medium. Sulfur-amino acids play a particularly important role, in that methionine, via S -adenosylmethionine , is used for transmethylation reactions involving pro-teins, phospholipids and nucleic acids, and is prob-ably involved in imprinting through this process. Methylation of nucleic acids is known to modulate gene expression and to participate in the mechan-ism of genomic imprinting ( Figure 5.6 ). S -amino acids also participate in protecting the embryo from free oxygen radicals: cysteine is a precursor

Chapter 5: First stages of development
74
for the synthesis of hypotaurine and taurine, and taurine can neutralize toxic aldehyde by-products of peroxidative reactions. Cysteine is a precursor of cysteamine and glutathione , and redox coup-ling between these amino acids helps the embryo to maintain its redox potential and prevent damage from peroxidative reactions. In the human oocyte, the pathway that recycles homocysteine to methio-nine via the CBS (cystathionine beta synthase path-way) is poorly expressed or nonexistent (Benkhalifa et al ., 2010 ). Ultimately, the initiation of all protein synthesis requires methionyl t-RNA, and the avail-ability of cysteine and methionine is therefore cru-cial during early embryogenesis. A shortage of these compounds, linked to either maternal age or trans-porter deficiency, is detrimental.
Glutamine is also an important source of carbon and energy: in vitro it may be deaminated into glu-tamic acid, but is also converted to pyroglutamic acid (or pyrollidone carboxylic acid, PCA) , which cannot be used for anabolism. However, glutamine is only weakly degraded in slightly alkaline conditions, correspond-ing to culture media. Introducing Gly-glutamine and Ala-glutamine into culture media to prevent degrad-ation does not help, as they are converted to Gly-PCA and Ala-PCA.
Glycine is an energy source, as it can be deaminated immediately to form glycollate and glyoxylate (C-2 metabolites), and also acts as a precursor for peptides, proteins and nucleic acids. It is a chelating agent for toxic divalent cations, has an in-vitro osmoregulatory
role, and is implicated in the regulation of intracellular pH of the embryo.
Deamination reactions are an important part of the biochemical and metabolic processes, and free ammo-nia is immediately recycled by effi cient enzyme systems present in the oviduct ( Figure 5.7 ). In vitro, in the pres-ence of incubator carbon dioxide, free ammonia forms carbonate and ammonium bicarbonate, both unstable compounds. If the embryo cultures are “open,” without oil, ammonia is liberated and eliminated by the car-bon dioxide atmosphere. However, within microdrops under oil, ammonia can accumulate, which is toxic to the embryo – Gardner and Lane ( 1993 ) demonstrated severe teratogenic eff ects in mouse embryos.
Nucleotides At a very early stage, embryos can synthesize purine and pyrimidine bases, precursors of RNA and DNA; these are required for DNA repair processes, which are very important during this period of development (Ménézo et al ., 2010 ). Following DNA damage caused by reactive oxygen species (ROS), the oxidized deoxy-nucleoside triphosphate pool is a signifi cant contribu-tor to genetic instability. Th ese oxidized bases must be removed in order to avoid their reintroduction into DNA. Th e nucleotide pool sanitization enzymes are the fi rst defenses against mutagenesis, and the human oocyte is well equipped with NUDT (nucleo-side diphosphate linked moiety X ), the major enzyme involved. However, there is a requirement for ATP,
Ammonia detoxification
Transsulfurationpathway
Methionyl mRNA
GLUCOSE
Glutathione
Oxidative stress
DNA, Lipid Peroxides
APOPTOSISImprinting DNA methyltransferase
over-methylation (alkylation)
ROS
(starts protein synthesis)
Cysteine
Methionine
HCy3
1
2
4
SAM
NH2
OH
OH
OH
HH H
O
O
s+
Me
N
N N
N
NH2
Figure 5.6 Methionine utilization in the preimplantation embryo (with thanks to Y. Ménézo).

Chapter 5: First stages of development
75
CTP, TTP. For example, GTP must replace oxidized G (8-oxoguanosine, the most common DNA decay linked to ROS) in DNA. Th ese bases can also be actively trans-ported from the surroundings; the embryo probably uses this mechanism, as uptake is generally less energy consuming than full synthesis. Th ere is an exponen-tial increase in the accumulation of these precursors during the transition from morula to blastocyst as the number of cells increases.
Vitamins It is diffi cult to measure vitamin uptake, but indirectly it is clear that folic acid and vitamin B12 , necessary for methylation processes , are mandatory cofactors. Th ymine is also known as 5-methyluracil , a pyrimi-dine nucleobase: inhibition of this methylation pro-cess by methotrexate leads to thymidine starvation and developmental arrest (O’Neill, 1998 ). Other vita-mins such as vitamin C and vitamin E may act as redox regulators.
Growth factors Th e potential role of growth factors (GF) in culture media remains open. Numerous growth factors are present in the oviduct and uterus, and they clearly play a role in vivo. Co-culture systems demonstrated a posi-tive eff ect of growth factors on cell number, embryo quality and freeze–thaw tolerance. However, this positive aspect represents the balanced interaction of several GFs such as leukemia inhibitory factor (LIF),
growth hormone (GH), mitogenic colony stimulat-ing factor (MCSF), rather than the action of a single one. Some may slow down, and several may accelerate embryonic development: the addition of a single GF in vitro remains questionable at this point.
Further reading Adams JM , Cory S ( 1998 ) Th e Bcl-2 protein family: arbiters
of cell survival . Science 281 : 1322 –1326. Adenot PG , Mercier Y , Renard JP , Th ompson EM ( 1997 )
Diff erential H4 acetylation of paternal and maternal chromatin precedes DNA replication and diff erential transcriptional activity in pronuclei of 1-cell mouse embryos . Development 124 (22): 4615 –4625.
Alikani M ( 2007 ) Th e origins and consequences of fragmentation in mammalian oocytes and embryos. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Selection . Taylor-Francis , London , pp. 51–78.
Alikani M , Cohen J , Tomkin G , et al . ( 1999 ) Human embryo fragmentation in vitro and its implications for pregnancy and implantation . Fertility and Sterility 71 : 836 –842.
Antczak M , Van Blerkom J ( 1997 ) Oocyte infl uences on early development: the regulatory proteins leptin and STAT3 are polarized in mouse and human oocytes and diff erentially distributed within the cells of the preimplantation stage embryo . Molecular Human Reproduction 3 : 1067 –1086.
Ao A , Erickson RP , Winston RML , Handyside AH ( 1994 ) Transcription of paternal Y-linked genes in the human zygote as early as the pronucleate stage . Zygote 2 : 281 –287.
Bachvarova R ( 1992 ) A maternal tail of poly(A): the long and short of it . Cell 69 : 895 –897.
Figure 5.7 Nitrogen recycling in the mammalian preimplantation embryo (with thanks to Y. Ménézo).

Chapter 5: First stages of development
76
Balinsky BI ( 1965 ) An Introduction to Embryology . Saunders , London .
Barritt J , Brenner CA , Cohne J , Matt DW ( 1999 ) Mitochondrial DNA rearrangements in oocytes and embryos . Molecular Human Reproduction 5 (10): 927 –933.
Benkhalifa M , Montjean D , Cohen-Bacrie P , Ménézo Y ( 2010 ) Imprinting: RNA expression for homocysteine recycling in the human oocyte . Fertility and Sterility 93 (5): 1585 –1590.
Bonnerot C , Vernet M , Grimber G , Brioand P , Nicolas JF ( 1993 ) Transcriptional selectivity in early mouse embryos: a qualitative study . Bioessays 15 (8): 531 –538.
Bouniol-Baly C , Nguyen E , Besombes D , Debey P ( 1997 ) Dynamic organization of DNA replication in one-cell mouse embryos: relationship to transcriptional activation . Experimental Cell Research 236 : 201 –211.
Braude P , Bolton V , Moore S ( 1988 ) Human gene expression fi rst occurs between the four- and eight-cell stages of preimplantation development . Nature 332 : 459 –461.
Brenner CA , Wolny YM , Barritt JA , et al . ( 1998 ) Mitochondrial DNA deletion in human oocytes and embryos . Molecular Human Reproduction 4 (9): 887 –892.
Brenner C , Wolny YM , Adler RR , Cohen J ( 1999 ) Altenative splicing of the telomerase catalytic submit in human oocytes and embryos . Molecular Human Reproduction 5 (9): 845 –850.
Brison DR , Schulz RM ( 1997 ) Apoptosis during mouse blastocyst formation: evidence for a role for survival factors including transforming growth factor alpha . Biology of Reproduction 56 : 1088 –1096.
Brison DR , Schulz RM ( 1998 ) Increased incidence of apoptosis in TGF-alpha defi cient mouse blastocysts . Biology of Reproduction 59 : 136 –144.
Calarco PG ( 1995 ) Polarization of mitochondria in the unfertilized mouse oocyte . Developmental Genetics 16 : 36 –43.
Chen C , Sathanantan AH ( 1986 ) Early penetration of human sperm through the vestments of human eggs in vitro . Archives of Andrology 16 : 183 –197.
Cho WK , Stern S , Biggers JD ( 1974 ) Inhibitory eff ect of dibutyryl cAMP on mouse oocyte maturation in vitro . Journal of Experimental Zoology 187 : 383 –386.
Clayton L , McConnell JM , Johnson MH ( 1995 ) Control of the surface expression of uvomorulin aft er activation of mouse oocytes . Zygote 3 (2): 177 –189.
Conaghan J , Handyside AH , Winston RM , Leese HJ ( 1993 ) Eff ects of pyruvate and glucose on the development of human preimplantation embryos in vitro . Journal of Reproduction and Fertility 99 (1): 87 –95.
Coticchio G , Fleming S ( 1998 ) Inhibition of phosphoinositide metabolism or chelation of intracellular calcium blocks FSH-induced but not
spontaneous meiotic resumption in mouse oocytes . Developmental Biology 203 : 201 –209.
Cummins JM , Jequier AM , Kan R ( 1994 ) Molecular biology of human male infertility: links with ageing, mitochondrial genetics, and oxidative stress? Molecular Reproduction and Development 37 : 345 –362.
Dale B , Gualtieri R , Talevi R , et al . ( 1991 ) Intercellular communication in the early human embryo . Molecular Reproduction and Development 29 : 22 –28.
Dale B , Marino M , Wilding M ( 1998 ) Sperm-induced calcium oscillations: soluble factor, factors or receptors? Molecular Human Reproduction 5 : 1 –4.
Dale B , Tosti E , Iaccarino M ( 1995 ) Is the plasma membrane of the human oocyte re-organized following fertilization and early cleavage? Zygote 3 : 31 –37.
Dekel N ( 1996 ) Protein phosphorylation/dephosphorylation in the meiotic cell cycle of mammalian oocytes . Reviews of Reproduction 1 : 82 –88.
Delhanty JDA , Harper JC , Ao A , Handyside AH , Winston RML ( 1997 ) Multicolour FISH detects frequent chromosomal mosaicism and chaotic division in normal preimplantation embryos from fertile patients . Human Genetics 99 : 755 –760.
De Sousa PA , Caveney A , Westhusin ME , Watson AJ ( 1998 ) Temporal patterns of embryonic gene expression and their dependence on oogenetic factors . Th eriogenology 49 : 115 –128.
Dominko T , First N ( 1997 ) Timing of meiotic progression in bovine oocytes and its eff ect on early embryo development . Molecular Reproduction and Development 47 : 456 –467.
Dulcibella T ( 1996 ) Th e cortical reaction and development of activation competence in mammalian oocytes . Human Reproduction Update 2 (1): 29 –42.
Eddy EM ( 1998 ) Regulation of gene expression during spermatogenesis . Seminars in Cell and Developmental Biology 19 : 451 –457.
Edwards RG , Beard H ( 1997 ) Oocyte polarity and cell determination in early mammalian embryos . Molecular Human Reproduction 3 : 868 –905.
Edwards RG , Hansis C ( 2005 ) Initial diff erentiation of blastomeres in 4-cell human embryos and its signifi cance for early embryogenesis and implantation . Reproductive Biomedicine Online 11 (2): 206 –218.
Eichenlaub-Ritter U ( 2002 ) Manipulation of the oocyte: possible damage to the spindle apparatus . Reproductive Biomedicine Online 5 : 117 –124.
Eppig JJ ( 2001 ) Oocyte control of ovarian follicular development and function in mammals . Reproduction 122 : 829 –838.
Eppig JJ , Chesnel F , Hirao Y , et al . (1997) Oocyte control of granulosa cell development: how and why . Human Reproduction 12 (11 Suppl): 127 –132.

Chapter 5: First stages of development
77
Fulka J Jr., First NL , Moor RM ( 1998 ) Nuclear and cytoplasmic determinants involved in the regulation of mammalian oocyte maturation . Molecular Human Reproduction 4 : 41 –49.
Gardner DK ( 1998 ) Changes in requirements and utilization of nutrients during mammalian preimplantation embryo development and their signifi cance in embryo culture . Th eriogenology 49 : 83 –102.
Gardner DK , Lane M ( 1993 ) Amino acids and ammonium regulate mouse embryo development in culture . Biology of Reproduction 48 (2): 377 –385.
Gardner RL ( 2001 ) Specifi cation of embryonic axes begins before cleavage in normal mouse development . Development 128 (6): 839 –847.
Gardner RL ( 2007 ) Th e axis of polarity of the mouse blastocyst is specifi ed before blastulation and independently of the zona pellucida . Human Reproduction 22 : 798 –806.
Gilchrist RB , Lane M , Th ompson JG ( 2008 ) Oocyte-secreted factors: regulators of cumulus cell function and oocyte quality . Human Reproduction Update 14 (2): 159 –177.
Glabowski W , Kurzawa R , Wisniewska B , et al . ( 2005 ) Growth factors eff ects on preimplantation development of mouse embryos exposed to tumour necrosis factor alpha . Reproductive Biology 5 (1): 83 –99.
Gopichandran N , Leese HJ ( 2003 ) Metabolic characterisation of the bovine blastocyst, inner cell mass, trophectoderm and blastocoel fl uid . Reproduction 126 : 299 –308.
Grammont G , Irvine KD ( 2002 ) Organiser activity of the polar cells during Drosophila oogenesis . Development 129 : 5131 –5140.
Gregory L ( 1998 ) Ovarian markers of implantation potential in assisted reproduction Human Reproduction 13 (Suppl. 4): 117 –132.
Grobstein C ( 1988 ) Biological characteristics of the preembryo . Annals of the New York Academy of Sciences 541 : 346 –348.
Gualtieri R , Santella L , Dale B ( 1992 ) Tight junctions and cavitation in the human pre-embryo . Molecular Reproduction and Development 32 : 81 –87.
Guyader-Joly C , Khatchadourian C , Ménézo Y ( 1996 ) Comparative glucose and fructose incorporation and conversion by in vitro produced bovine embryos . Zygote 4 : 85 –91.
Hales BF , Barton TS , Robaire B ( 2005 ) Impact of paternal exposure to chemotherapy on off spring in the rat . Journal of the National Cancer Institute Monograph 34 : 28 –31.
Hales BF , Robaire B ( 2001 ) Paternal exposure to drugs and environmental chemicals: eff ects on progeny outcome . Journal of Andrology 22 (6): 927 –936.
Hamberger L , Nilsson L , Sjögren A ( 1998 ) Microscopic imaging techniques: practical aspects . Human Reproduction 13 : Abstract book 1: 15, L.
Hansis C , Grifo JA , Tang Y , Krey LC ( 2002 ) Assessment of beta-HCG, beta-LH mRNA and ploidy in individual human blastomeres . Reproductive Biomedicine Online 5 (2): 156 –161.
Hardy K ( 1999 ) Apoptosis in the human embryo . Reviews of Reproduction 4 : 125 –134.
Harper JC , Delhanty JDA ( 1997 ) Preimplantation genetic diagnosis. In: Rodeck CH , Whittle MJ (eds.) Fetal Medicine: Basic Science and Clinical Practice . Churchill Livingstone , Edinburgh .
Heidmann O , Vernochet C , Dupressoir A , Heidmann T ( 2009 ) Identifi cation of an endogenous retroviral envelope gene with fusogenic activity and placenta-specifi c expression in the rabbit: a new “syncytin” in a third order of mammals . Retrovirology 6 : 107 .
Heikinheimo O , Gibbons W ( 1998 ) Th e molecular mechanisms of oocyte maturation and early embryonic development are unveiling new insights into reproductive medicine . Molecular Human Reproduction 4 (8): 745 –756.
Henery CC , Miranda M , Wiekowski M , Wilmut I , DePamphilis ML ( 1995 ) Repression of gene expression at the beginning of mouse development . Developmental Biology 169 (2): 448 –460.
Henkel R , Miller C , Miska H , Gips H , Schill WB ( 1993 ) Early embryology: determination of the acrosome reaction in human spermatozoa is predictive of fertilization in vitro . Human Reproduction 8 (12): 2128 –2132.
Hewitson LC , Simerly CR , Dominko T , Schatten G ( 2000 ) Cellular and molecular events aft er in vitro fertilization and intracytoplasmic sperm injection . Th eriogenology 53 : 95 –104.
Hewitson LC , Simerly C , Schatten G ( 1997 ) Inheritance defects of the sperm centrosome in humans and its possible role in male infertility . International Journal of Andrology 20 (Suppl. 3): 35 –43.
Hewitson LC , Simerly CR , Tengowski MW , et al . ( 1996 ) Microtubule and chromatin confi guration during Rhesus intracytoplasmic sperm injection: successes and failures . Biology of Reproduction 55 : 271 –280.
Houghton FD ( 2005 ) Role of gap junctions during early embryo development . Reproduction 129 : 129 –131.
Houghton FD ( 2006 ) Energy metabolism of the inner cell mass and trophectoderm of the mouse blastocyst . Diff erentiation 74 : 11 –18.
Huarte J , Stutz A , O’Connell ML , et al . ( 1992 ) Transient translational silencing by reversible mRNA deadenylation . Cell 69 : 1021 –1030.
Ivanov PL , Wadhams MJ , Roby RK , et al . ( 1996 ) Mitochondrial DNA sequence heteroplasmy in the Grand Duke of Russia Georgij Romanov establishes the authenticity of the remains of Tsar Nicholas II . Nature Genetics 12 : 417 –420.

Chapter 5: First stages of development
78
Janny L , Ménézo YJR ( 1994 ) Evidence for a strong paternal eff ect on human preimplantation embryo development and blastocyst formation . Molecular Reproduction and Development 38 : 36 –42.
Jansen S , Esmaeilpour T , Pantaleon M , Kaye PL ( 2006 ) Glucose aff ects monocarboxylate cotransporter (MCT) 1 expression during mouse preimplantation development . Reproduction and Fertility 131 : 469 –479.
Johnson MH ( 2002 ) Time and development . Reproductive Biomedicine Online 4 (Suppl. 1): 39 –45.
Johnson MH , Day ML ( 2000 ) Egg timers: how is developmental time measured in the early vertebrate embryo? Bioessays 22 : 57 –63.
Johnson MH , Lim A , Fenando D , Day ML ( 2002 ) Circadian clockwork genes are expressed in the reproductive tract and conceptus of the early pregnant mouse . Reproductive Biomedicine Online 4 (12): 140 –145.
Jurisicova A , Acton BM ( 2004 ) Deadly decisions: the roles of genes regulating programmed cell death in human preimplantation embryo development . Reproduction 128 (3): 281 –291.
Kane MT , Morgan PM , Coonan C ( 1997 ) Peptide growth factors and preimplantation development . Human Reproduction Update 3 : 137 –157.
Kaneda H , Hayashi J , Takahama S , et al . ( 1995 ) Elimination of paternal mitochondrial DNA in intraspecifi c crosses during early mouse embryogenesis . Proceedings of the National Academy of Sciences of the USA 92 : 4542 –4546.
Katari S , Turan N , Bibikova M , et al . ( 2009 ) DNA methylation and gene expression diff erences in children conceived in vitro or in vivo . Human Molecular Genetics 18 (20): 3769 –78.
Kawamura K , Fukuda J , Shimizu Y , Kodama H , Tanaka T ( 2005 ) Survivin contributes to the anti-apoptotic activities of transforming growth factor alpha in mouse blastocysts through phosphatidylinositol 3′-kinase pathway . Biology and Reproduction 73 : 1094 –1101.
Kidder GM , McLachlin JR ( 1985 ) Timing of transcription and protein synthesis underlying morphogenesis in preimplantation mouse embryos . Developmental Biology 112 : 265 –275.
Kola I , Trounson A ( 1989 ) Dispermic Human Fertilization: Violation of Expected Cell Behaviour . Academic Press , San Diego .
Krakauer DC , Mira A ( 1999 ) Mitochondria and germ cell death . Nature 400 : 125 –126.
Lane M , Gardner DK ( 1997 ) Nonessential amino acids and glutamine decrease the time of the fi rst three cleavage divisions and increase compaction of mouse zygotes in vitro . Journal of Assisted Reproduction and Genetics 14 (7): 398 –403.
Lane M , Gardner DK ( 2000 ) Lactate regulates pyruvate uptake and metabolism in the preimplantation mouse embryo . Biology and Reproduction 62 : 16 –22.
Lee L , Miyano T , Moor RM ( 2000 ) Localisation of phosophorylated MAP kinase during the transition from meiosis I to meiosis II in pig oocytes . Zygote 8 : 119 –125.
Lefi èvre L , Conner SJ , Salpekar A , et al . ( 2004 ) Four zona pellucida glycoproteins are expressed in the human . Human Reproduction 19 (7): 1580 –1586.
Levy R , Elder K , Ménézo Y ( 2004 ) Cytoplasmic transfer in oocytes: biochemical aspects . Human Reproduction Update 10 (3): 241 –250.
Lightman A , Kol S , Wayner V , et al . ( 1997 ) Th e presence of a sponsoring embryo in a batch of poor quality thawed embryos signifi cantly increases pregnancy and implantation rate . Fertility and Sterility 67 (4): 711 –716.
Lin YC , Chang SY , Lan KC , et al . ( 2003 ) Human oocyte maturity in vivo determines the outcome of blastocyst development in vitro . Journal of Assisted Reproduction and Genetics 20 (12): 506 –512.
Lo H ( 1996 ) Th e role of gap junction membrane channels in development . Journal of Bioenergetics and Biomembranes 8 (4): 399 –409.
Majumder S , DePamphilis ML ( 1994 ) Requirements for DNA transcription and replication at the beginning of mouse development . Journal of Cell Biochemistry 55 (1): 59 –68.
Marangos P , FitzHarris G , Carroll J ( 2003 ) Ca2+ oscillations at fertilization in mammals are regulated by the formation of pronuclei . Development 130 : 1461 –1472.
Maro B , Gueth-Hallonet C , Aghion J , Antony C ( 1991 ) Cell polarity and microtubule organization during mouse early embryogenesis . Development Supplement 1 : 17 –25.
Masui Y ( 2001 ) From oocyte maturation to the in vitro cell cycle: the history of discoveries of Maturation Promoting Factor (MPF) and Cytostatic Factor (CSF) . Diff erentiation 69 : 1 –17.
Mattioli M , Barboni B ( 2000 ) Signal transduction mechanism for LH in the cumulus oocyte complex . Molecular and Cellular Endocrinology 161 : 19 –23.
Memili E , Dominko T , First N ( 1998 ) Onset of transcription in bovine oocytes and embryos . Molecular Reproduction and Development 51 : 36 –41.
Memili E , First NL ( 1999 ) Control of gene expression at the onset of bovine embryonic development . Biology of Reproduction 61 : 1198 –1207.
Ménézo Y , Dale B , Cohen M ( 2010 ) DNA damage and repair in human oocytes and embryos: a review. Zygote (in press).
Ménézo Y , Janny L ( 1997 ) Infl uence of paternal factors in early embryogenesis. In: Barratt C , De Jonge C , Mortimer D , Parinaud J (eds.) Genetics of Human Male Infertility . EDK , Paris , pp. 246–257.

Chapter 5: First stages of development
79
Mio Y ( 2006 ) Morphological analysis of human embryonic development using time-lapse cinematography . Journal of Mammalian Ova Research 23 (1): 27 –35.
Munne S , Alikani M , Tomkin G , Grifo J , Cohen J ( 1995 ) Embryo morphology, developmental rates, and maternal age are correlated with chromosome abnormalities . Fertility and Sterility 64 : 382 –391.
Nargund G , Bourne T , Doyle P , et al . ( 1996 ) Associations between ultrasound indices of follicular blood fl ow, oocyte recovery and preimplantation embryo quality . Human Reproduction 11 (1): 109 –113.
Niemann H , Wrenzycki C ( 1999 ) Alterations of expression of developmentally important genes in preimplantation bovine embryos by in vitro culture condition: implications for subsequent development . Th eriogenology 53 : 21 –34.
Nikas G , Ao A , Winston RM , Handyside AH ( 1996 ) Compaction and surface polarity in the human embryo in vitro . Biology of Reproduction 55 : 32 –37.
Nikas G , Paraschos T , Psychoyos A , Handyside AH ( 1994 ) Th e zona reaction in human oocytes as seen with scanning electron microscopy . Human Reproduction 9 (11): 2135 –2138.
Nothias JY , Majumder S , Kaneko KJ , DePamphilis ML ( 1995 ) Regulation of gene expression at the beginning of mammalian development . Journal of Biological Chemistry 270 : 22077 –22080.
Nothias JY , Miranda M , De Pamphilis ML ( 1996 ) Uncoupling of transcription and translation during zygotic gene activation in the mouse . EMBO Journal 14 : 5715 –5725.
O’Neill C ( 1998 ) Role of autocrine mediators in the regulation of embryo viability: lessons from animal models . Journal of Assisted Reproduction and Genetics 15 (8): 460 –465.
Orsi NM , Leese HJ ( 2004 ) Ammonium exposure and pyruvate aff ect the amino acid metabolism of bovine blastocysts in vitro . Reproduction 127 : 131 –140.
Payne D , Flaherty SP , Barry MF , Matthews CD ( 1997 ) Preliminary observations on polar body extrusion and pronuclear formation in human oocytes using time-lapse video cinematography . Human Reproduction 12 (3): 532 –541.
Payne D , Flaherty SP , Newble CD , Swann NJ , Wang XJ , Matthews CD ( 1994 ) Th e infl uence of sperm morphology and the acrosome reaction on fertilization . Human Reproduction 9 : 1281 –1288.
Picton HM , Briggs D , Gosden RG ( 1998 ) Th e molecular basis of oocyte growth and development . Molecular and Cellular Endocrinology 145 : 27 –37.
Piotrowska K , Wianny F , Pedersen RA , Zernicka-Goetz M ( 2001 ) Blastomeres arising from the fi rst cleavage division have distinguishable fates in normal mouse development . Development 128 : 3739 –3748.
Piotrowska-Nitsche K , Perea-Gomez A , Haraguchi S , et al . ( 2005 ) Four-cell stage mouse blastomeres have diff erent developmental properties . Development 132 : 479 –490.
Piotrowska-Nitsche K , Zernicka-Goetz M ( 2005 ) Spatial arrangement of individual 4-cell stage blastomeres and the order in which they are generated correlate with blastocyst pattern in the mouse embryo . Mechanisms of Development 122 : 487 –500.
Posillico J , and Th e Metabolomics Study Group for Assisted Reproductive Technologies ( 2007 ) Selection of viable embryos and gametes by rapid, noninvasive metabolomic profi ling of oxidative stress biomarkers. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Taylor-Francis , London .
Puissant F , Van Rysselberge M , Barlow P , et al . ( 1987 ) Embryo scoring as a prognostic tool in IVF treatment . Human Reproduction 2 : 705 –708.
Reik W , Dean W , Walter J ( 2001 ) Epigenetic reprogramming in mammalian development (Review) . Science 293 : 1089 –1093.
Robaire B , Hales BF ( 2003 ) Mechanisms of action of cyclophosphamide as a male-mediated developmental toxicant . Advances in Experimental Medicine and Biology 518 : 169 –180.
Rossant J ( 2004 ) Lineage development and polar asymmetries in the peri-implantation mouse blastocyst . Seminars in Cell and Developmental Biology 15 (5): 573 –581.
Sakkas D , Urner F , Bizzaro D , et al . ( 1998 ) Sperm nuclear DNA damage and altered chromatin structure: eff ect on fertilization and embryo development . Human Reproduction 13 (Suppl. 4): 11 –19.
Santella L , Alikani M , Talansky BE , Cohen J , Dale B ( 1992 ) Is the human oocyte plasma membrane polarized? Human Reproduction 7 : 999 –1003.
Sapienza C , Peterson AC , Rossant J , Balling R ( 1987 ) Degree of methylation of transgenes is dependent on gamete of origin . Nature 328 (6127): 251 –254.
Sathanathan AH , Chen C ( 1986 ) Sperm-oocyte membrane fusion in the human during monospermic fertilization . Gamete Research 15 : 177 –186.
Sathananthan AH , Ng SC , Bongo A , Trounson A , Ratnam S ( 1993 ) Visual Atlas of Early Human Development of Assisted Reproduction Technology. Singapore University Press .
Sathananthan AH , Ng SC , Trounson AO , Ratnam SS , Bongso TA ( 1990 ) Human sperm-oocyte fusion. In: Dale B (ed.) Mechanism of Fertilization: Plants to Humans . NATO ASI Series, Vol. h45, Springer-Verlag , Berlin .
Schatten G ( 1994 ) Th e centrosome and its mode of inheritance: the reduction of the centrosome during gametogenesis and its restoration during fertilization . Developmental Biology 165 (2): 299 –335.

Chapter 5: First stages of development
80
Schatten G ( 1999 ) Fertilization. In: Fauser BCJM (ed.) Molecular Biology in Reproductive Medicine . Parthenon Publishing , London , pp. 297–311.
Schatten G , Simerly C , Schatten H ( 1991 ) Maternal inheritance of centrosomes in mammals; studies on parthenogenesis and polyspermy in mice . Proceedings of the National Academy of Sciences of the USA 88 (15): 6785 –6789.
Schultz RM ( 1995 ) Role of chromatin structure in zygotic gene activation in the mammalian embryo . Seminars in Cell Biology 6 (4): 201 –208.
Schultz RM ( 1999 ) Preimplantation embryo development. In: Fauser BCJM (ed.) (1999) Molecular Biology in Reproductive Medicine . Parthenon Publishing , London , pp. 313–331.
Schultz RM ( 2002 ) Th e molecular foundations of the maternal to zygotic transition in the preimplantation embryo . Human Reproduction Update 8 (4): 323 –331.
Simerly C , Navara CS ( 2007 ) Th e sperm centriole: its eff ect on the developing embryo. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Taylor-Francis , London .
Simerly C , Wu G , Zoran S , et al . ( 1995 ) Th e paternal inheritance of the centrosome, the cell’s microtubule-organising center, in humans and the implications of infertility . Nature Medicine 1 : 47 –53.
Spanos S , Becker DL , Winston RM , Hardy K ( 2000 ) Anti-apoptotic action of insulin-like growth factor-1 during human preimplantation embryo development . Biology and Reproduction 63 : 1413 –1420.
Stein P , Worrad DM , Belyaev ND , Turner BM , Schultz RM ( 1997 ) Stage-dependent redistributions of acetylated histones in nuclei of the early preimplantation mouse embryo . Molecular Reproduction and Development 47 (4): 421 –429.
Steuerwald N ( 2007 ) Gene expression analysis in the human oocyte and embryo. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Taylor-Francis , London .
Sun QY ( 2003 ) Cellular and molecular mechanisms leading to cortical reaction and polyspermy block in mammalian eggs . Microscopy Research and Technique 61 (4): 342 –348.
Surani MA , Barton SC , Norris ML ( 1986 ) Nuclear transplantation in the mouse: heritable diff erences between parental genomes aft er activation of the embryonic genome . Cell 45 (1): 127 –136.
Temeles GL , Ram PT , Rothstein JL , Schulz RM ( 1994 ) Expression patterns of novel genes during mouse preimplantation embryogenesis . Molecular Reproduction and Development 37 : 121 –129.
Tesarik J , Greco E ( 1999 ) Th e probability of abnormal preimplantation development can be predicted by a single static observation on pronuclear stage morphology . Human Reproduction 14 : 1318 –1323.
Tesarik J , Kopecny V ( 1989a ) Developmental control of the human male pronucleus by ooplasmic factors . Human Reproduction 4 : 962 –968.
Tesarik J , Kopecny V ( 1989b ) Nucleic acid synthesis and development of human male pronucleus . Journal of Reproduction and Fertility 86 : 549 –558.
Tesarik J , Kopecny V ( 1989c ). Development of human male pronucleus: ultrastructure and timing . Gamete Research 24 : 135 –149.
Tesarik J , Kopecny V , Plachot M , Mandelbaum J ( 1988 ) Early morphological signs of embryonic genome expression in human preimplantation development as revealed by quantitative electron microscopy . Developmental Biology 128 : 15 –20.
Torres-Padilla ME , Zernicka-Goetz M ( 2006 ) Role of TIF1α as a modulator of embryonic transcription in the mouse zygote . Journal of Cell Biology 174 (3): 329 –338.
Tosti E ( 2006 ) Calcium ion currents mediating oocyte maturation events (Review) . Reproductive Biology and Endocrinology 4 : 26 –35.
Valdimarsson G , Kidder GM ( 1995 ) Temporal control of gap junction assembly in preimplantation mouse embryos . Journal of Cell Science 108 (Pt 4): 1715 –1722.
Van Blerkom J , Davis P , Alexander S ( 2004 ) Occurrence of maternal and paternal spindles in unfertilized human oocytes: possible relationship to nucleation defects aft er silent fertilization . Reproductive Biomedicine Online 8 (4): 454 –459.
Warner CM , Cao W , Exley GE et al. ( 1998 ) Genetic regulation of egg and embryo survival . Human Reproduction 13 (Suppl. 3): 178 –190.
Wassarman P ( 1987 ) Th e biology and chemistry of fertilization . Science 235 : 553 –560.
Wassarman P ( 1990 ) Profi le of a mammalian sperm receptor . Development 108 : 1 –17.
Wassarman PM , Florman HM , Greve IM ( 1985 ) Receptor-mediated sperm-egg interactions in mammals. In: Metz CB , Monroy A (eds.) Fertilization , Vol. 2. Academic Press , New York , pp. 341–360.
Wiekowski M , Miranda M , DePamphilis ML ( 1991 ) Regulation of gene expression in preimplantation mouse embryos: eff ects of the zygotic clock and the fi rst mitosis on promoter and enhancer activities . Developmental Biology 147 (2): 403 –414.
Wolff e AP ( 1998 ) Packaging principle: how DNA methylation and histone acetylation control the transcriptional activity of chromatin . Journal of Experimental Zoology 282 : 239 –244.
Woodward BJ , Lenton EA , MacNeil S ( 1993 ) Requirement of preimplantation human embryos for extracellular calmodulin for development . Human Reproduction 8 (2): 272 –276.

Chapter 5: First stages of development
81
Worrad DM , Turner BM , Schultz RM ( 1995 ) Temporally restricted spatial localization of acetylated isoforms of histone H4 and RNA polymerase II in the 2-cell mouse embryo . Development 121 (9): 2949 –2959.
Xu Y , Zhang JJ , Grifo JA , Krey LC ( 2005 ) DNA methylation patterns in human tripronucleate zygotes . Molecular Human Reproduction 11 (3): 167 –171.

Chapter
1
82
Implantation and early stages of fetal development
Implantation During the transition from morula to blastocyst the embryo enters the uterus, where it is sustained by oxy-gen and a rich supply of metabolic substrates in uterine secretions. At the site of implantation the trophecto-derm cells produce proteolytic enzymes that digest a passage through the zona pellucida , as the blastocyst “hatches” free of the zona. Th e uterine environment may also contain proteolytic enzymes, but very little is known about the molecular basis for hatching. Th e exposed cell layers of the hatched blastocyst make fi rm physical contact and implantation starts. Th e process of implantation ( Figure 6.1 ), leading to the success-ful establishment of a pregnancy, must be carefully coordinated in time and in place. Th e embryo and the uterus, both highly complex structures, must interact correctly and at the appropriate time in order for a pregnancy to be established; a multitude of diff erent factors can infl uence their respective unique devel-opmental characteristics. Implantation is initiated via a molecular dialogue between the “free” hatched blastocyst and the endometrium, which allows the embryo to attach to the endometrial epithelium. Th e blastocyst trophectoderm secretes hCG, which provides direct signaling to the epithelial cells of the endometrium; hCG is detectable in maternal circula-tion within 3 days of embryo attachment to the endo-metrial epithelium – i.e., 9–12 days post ovulation. Trophectoderm cells from the blastocyst migrate between the epithelial cells, displace them, and pene-trate up to the basement membrane. Th e process of implantation can be divided into three stages: appos-ition, adhesion and invasion; the three phases must occur during a period when the uterine endometrium is maximally receptive, a period that is known as the “implantation window.”
Apposition: the embryo/endometrial dialogue Th e embryo enters the uterus 3 or 4 days aft er ovulation, and hatches from the zona pellucida as an expanded blastocyst on Day 5–6, so that the hatched blastocyst is “apposed” to the uterine endometrium. Apposition
6 (a)
(c)
(b)
Figure 6.1 Detailed anatomy of implantation in the mammal. (a) Expanded blastocyst showing the fl at layer of trophectoderm cells (T) which will become part of the extra embryonic tissue and the inner cell mass (E) from which the embryo derives. (b) Shows hatching, probably due in part to the production of a proteolytic-like enzyme by some of the trophectoderm cells. (c) Invasion of the epithelium (Ep) of the endometrium (En). St: syncytiotrophoblast.
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. (©) K. Elder and B. Dale 2011.

Chapter 6: Implantation and early stages of fetal development
83
is facilitated by the transient appearance of specialized epithelial cellular membrane protrusions or “pinopo-des,” which surround the pits in endometrial glands and actively reabsorb the uterine secretory phase fl uid. Th eir appearance is progesterone-dependent, they are present for only 2–3 days (between Days 5 and 7 post ovulation) and are a morphological marker of the open-ing of the implantation window (Nikas et al ., 1995 ).
Th e uterine epithelium is coated with a network of glycoproteins (glycocalyx), which acts as a phys-ical barrier to cell–cell interaction. Th e embryo must fi rst overcome this “glycocalyx barrier,” which contains mucins expressed by endometrial cells, via localized (i.e., embryo driven) enzymatic cleavage of the extra-cellular glycoproteins, or via binding of receptors expressed by the embryo and subsequent cleavage of the mucins. When apposition is achieved, the adhesion molecules have access to each other and the embryonic cytotrophoblast cells of the trophectoderm become attached to the endometrial cells.
Adhesion Th e embryo is thought to attach (adhere) to the endo-metrium on Day 6–7 post ovulation. Once the embryo and endometrial adhesion molecules have free access to each other, the embryonic trophoblast cells attach to the endometrial epithelial cells. Several families of adhesion molecules are thought to be involved to a greater or lesser degree in human embryo attachment, including the integrins, tastin/trophinin complexes, heparan sulfate proteoglycans, cadherins, lectin/glycan interactions and glycan/glycan interactions. Th e integ-rin family is one of the key adhesion factors involved in human implantation. Experimental evidence has shown that hCG upregulates the integrin avb3, and interleukins IL-1a and IL-1b from the embryo are also involved. Human oocytes, early embryos and blastocysts express integrins, and they are also widely expressed by the glandular epithelium. Some are synthesized at a constant rate (a2, a3, a6, b1, b4, b5) whereas others vary during stages of the cell cycle (a1, a9, av, b3, b6). Th e av family are the integrins most likely to be involved in attachment; they bind fi bronec-tin, osteopontin, vitronectin and other components of the extracellular matrix.
Invasion Pre-villous trophoblast starts to diff erentiate between Days 7 and 12, and endometrial transformation
(stromal decidualization ) is underway by Day 12 post ovulation (Duc-Goiran et al ., 1999 ). Trophoblast cells extensively invade the uterine tissue to establish an interface between fetus and mother, so that nutrients and waste products can be transferred. Th ey also fulfi ll a mechanical function by stabilizing the placental tis-sue within the uterus. Th e embryonic trophectoderm contains cytotrophoblasts, the mononuclear undiff er-entiated stem cells that are precursors of all trophoblast forms. Th ese diff erentiate into subsets: 1. Invasive intermediate trophoblasts migrate into
the uterine tissue. 2. Villous syncytiotrophoblast makes the majority of
the placental hormones, including hCG. 3. Junctional trophoblast cells mediate the
attachment of the placenta to the uterus.
Invasive trophoblast cells invade the endometrium and upper layers of the myometrium and remodel the extracellular matrix in order to selectively perme-ate uterine spiral arteries. Th e colonized blood vessels are then modifi ed to yield widened, low-resistance channels that can carry an increased maternal blood fl ow to the placenta. Th e mother must protect herself from these invasive trophoblasts migrating toward the uterine spiral arteries, and the endometrial stroma transforms itself into a dense cellular matrix known as the decidua , which will form the maternal part of the placenta. During decidualization, the spindle-shaped stromal fi broblasts enlarge and diff erentiate into plump secretory decidual cells, creating a tough extracellular matrix that is rich in fi bronectin and lam-inin . Th is transformation occurs under the infl uence of progesterone.
Th e reaction is initially localized to cells surround-ing the spiral arteries, but subsequently spreads to neighboring cells. Th e majority of cells of the decidua express leukocyte antigens. Th e largest single popula-tion of white blood cells in the endometrium are large granular lymphocytes (LGLs or NK cells), with smaller numbers of macrophages and T cells also present. Th e abundance of LGLs increases dramatically between ovulation and implantation, infl uenced by steroid hor-mones (King et al ., 1998 ). Th e decidua forms a physical barrier to invasive cell penetration and also gener-ates a local cytokine milieu that promotes trophoblast attachment.
Th e fi rst signs of the decidualization reaction can be seen as early as Day 23 of the normal menstrual cycle (10 days aft er the peak of the luteinizing hormone

Chapter 6: Implantation and early stages of fetal development
84
surge), when the spiral arteries of the endometrium fi rst become prominent. Over the next few days, the eff ect of progesterone causes the stromal cells surrounding the spiral arteries to transform and diff erentiate into predecidual cells. Th is progressive decidualization of the endometrial stroma prepares the uterine lining for the presence of the invasive trophoblasts, but simultan-eously closes the door to implantation. At this stage the embryo fi rst becomes visible to the maternal immune system.
Th e invasion stage requires a very delicate balan-cing of confl icting biological needs between the early fetus and the mother, with a complex regulation of adhesion molecule expression, coordinated in time and in space. Th e invading cells use collagenases, and also express plasminogen activator inhibitor type 1, suggesting that the plasminogen activator system may also be involved. Th ey lose integrins associated with basement membrane interactions (possibly laminin ), and gain integrins that can interact with fi bronectin and type I collagen. Th e outer layer of trophoblast cells fuse to form a multinucleated syncytiotrophob-last layer that covers the columns of invading cells. Th is layer proliferates rapidly, and forms numer-ous processes, the chorionic villi (the chorion is the layer that surrounds the embryo and extraembryonic membranes). Cyclic AMP and its analogues, and more recently hCG itself, have been shown to direct cytotrophoblast diff erentiation toward a syncytiotro-phoblast phenotype that actively secretes the placen-tal hormones.
At the point where chorionic villi make contact with external extracellular matrix (decidual stromal, ECM), another population of trophoblasts prolifer-ates from the cytotrophoblast layer to form the junc-tional trophoblast. Th e junctional trophoblasts make a unique fi bronectin, trophouteronectin (TUN) , which appears to mediate the attachment of the placenta to the uterus. Transforming growth factor-β (TGF-β) and, more recently, leukemia inhibitory factor (LIF) have been shown to downregulate hCG synthesis and upregulate TUN secretion. Th ese cells also make urokinase-type plasminogen activator and type 1 plasminogen activator inhibitor (PAI-1) . Experiments using in-vitro model systems showed that phorbol esters increase trophoblast invasiveness and upregu-late PAI-1 in cultured trophoblasts. Uterine prostag-landins (PGF2 and PGE2) are regulated by steroids, and are involved in regulating the formation of the decidua.
The implantation window Th e existence of a transient implantation window has been well documented for rodent species. In these species, the window is maternally directed and the receptive state is sustained for less than 24 hours. In the human, the window appears to be approximately 5 days long (Day 6 to Day 10 post ovulation in the normalized 28-day menstrual cycle), and the opening of the receptive phase is not as clearly defi ned as its termination. In the mouse, hatched blastocysts read-ily attach and spread in an integrin-dependent pro-cess on any surface that includes ligands found in the stroma during pregnancy (fi bronectin, collagen, lam-inins , vitronectin, thrombospondin, etc.) as well as on artifi cial substrates like Matrigel. However, humans undergo protrusive penetration of trophoblast through the epithelium and the process is likely to be more strongly regulated by complex and multifactor-ial interactions between embryo and endometrium.
Summary Successful implantation requires both a synchronous development and a synchronized interaction between blastocyst and endometrium. Direct signaling from the embryo to the endometrium upregulates mole-cules such as the integrins, and this signaling promotes blastocyst adhesion. Th e blastocyst initially derives nourishment from uterine secretions, but in order to continue growing the conceptus must develop its own vascular system, and, as a fi rst step, induces a highly specialized reaction in the uterine stroma that initi-ates sprouting and growth of capillaries – the primary decidual reaction. Th e decidualized stromal cells make pericellular fi bronectin. Th ere is a dramatic transform-ation of endometrial stromal cells, and a massive leuko-cyte infi ltration by NK cells and macrophages. Maternal hormones infl uence the communication between the embryo and the endometrium, via eff ects on cytokines, adhesion molecules, prostaglandins, metalloproteases and their inhibitors, and angiogenic growth factors.
Th e molecular mechanisms behind this complex and sophisticated process have been studied using animal models, and knock-out (KO) mouse studies have positively identifi ed genes for receptivity (LIF, HMX3), responses to embryo (Cox2), and deciduali-zation (IL-11R). Other factors identifi ed as having a role include immune response gene (IRG1), proges-terone receptor knock-out (PRKO), estrogen receptor knock-out (ERKO), homeobox protein A10 (Hoxa10),

Chapter 6: Implantation and early stages of fetal development
85
IHH (Indian Hedgehog gene ) and immune regulating hormone 1 (IIRH1). Estrogen and progesterone recep-tors and the signaling pathways that interact with them are clearly important, including the IGF-I and epider-mal growth factor (EGF) family and prostaglandins. Research in humans continues, now using microarray technology to look at gene expression in order to iden-tify those factors that determine a receptive endo-metrium, with the hope of elucidating mechanisms that may enhance successful implantation aft er ART (Simon et al ., 2009 ; Sherwin et al ., 2007 ).
Steroid hormones and implantation
Estrogen acts during the proliferative phase of the menstrual cycle to promote the development of the endometrium, and it opens the window of receptivity via several mechanisms:
Causes loss of surface negative charge, shortening • of microvilli and thinning of the mucin coat with changes in its molecular composition Stimulates the synthesis of at least 12–14 endomet-• rial polypeptides, as well as estrogen and progester-one receptors Acts on luminal epithelial cells to make them respon-• sive or sensitive to a blastocyst signal, promoting trophectoderm attachment to the luminal cells Stimulates the release of glandular epithelial secre-• tions that include cytokines, and this activates the implantation process.
Progesterone is secreted by the corpus luteum after ovulation, and stimulates the secretory activity of the uterus:
Produces intense edema in the stroma • Increases blood vessel volume threefold • Stimulates the formation of pinopodes, and primes • the decidua.
Steroids regulate the action of uterine growth factors which are synthesized at various stages of the men-strual cycle: IGF-I and IGF-II, EGF, HB-EGF, FGF, β-FGF, α-FGF, TGF-β1, PDGF-β.
Early postimplantation embryogenesis Most of our knowledge about early postimplantation development was gained from studies in chick, mouse and other mammalian species. Although experimen-tal studies in humans are not possible, information has been gained from fi xed and stained human embryos aft er pregnancy loss at diff erent stages of gestation. Th e Carnegie Collection of Human Development at the National Institute of Child and Human Development
in Washington DC has made a collection of several thousand serial microscopic cross-sections, which are available for study (O’Rahilly and Müller, 1987 ). Human embryos have been classifi ed into 23 devel-opmental stages based on a number of morphological features, known as the Carnegie stages. Th ese stages represent a series of events that occur during devel-opment, with overlap between the diff erent stages. From 1994 onwards the Visible Embryo Project ( www.visembryo.com ) used computer technology to recon-struct accurate 3-D images of human development. A digital image database of serially sectioned human embryos from the Carnegie Collection is available online as Th e Heirloom Collection, supported by the National Library of Medicine in the USA. Beautiful color 3-D reconstructions and animations can be viewed at: http://virtualhumanembryo.lsuhsc.edu/ . Please refer to these images for further details in rela-tion to the brief overview presented here.
7–12 days post ovulation Once the blastocyst has hatched and trophoblast cells have started the process of implantation, the cells of the inner cell mass start to reorganize into distinct lay-ers, each layer destined for a diff erent developmental fate. Cellular morphology changes, and there is active movement of individual cells and groups of cells, set-ting up new relationships between them. In the human embryo, the fi rst 14–18 days of development are con-cerned mainly with the diff erentiation of various extraembryonic tissues, and aft er this time separate tissues can begin to be identifi ed.
Ectopic pregnancy
• A hatched blastocyst can sometimes implant in sites outside the uterus, most commonly in the fal-lopian tube. Other sites include the utero-cervical isthmus (cervical pregnancy) and the utero-tubal junction; more rarely, implantation can take place in the ovary, or in the peritoneal or abdominal cavity. Occasionally two embryos will implant at diff erent • sites: one in each tube (bilateral tubal pregnancy ) or one in the uterus and one at an ectopic site (hetero-topic pregnancy ). An embryo can continue to grow at an ectopic • site for several weeks, with signs and symptoms of early pregnancy in the mother. If undetected, ectopic pregnancy can result in a life-threatening crisis due to tubal rupture or erosion into a blood vessel.
Estrogen acts during the proliferative phase of the menstrual cycle to promote the development of the endometrium, and it opens the window of receptivity via several mechanisms:
Causes loss of surface negative charge, shortening •of microvilli and thinning of the mucin coat with changes in its molecular composition Stimulates the synthesis of at least 12–14 endomet-•rial polypeptides, as well as estrogen and progester-one receptors Acts on luminal epithelial cells to make them respon-•sive or sensitive to a blastocyst signal, promoting trophectoderm attachment to the luminal cells Stimulates the release of glandular epithelial secre-•tions that include cytokines, and this activates the implantation process.
Progesterone is secreted by the corpus luteum after ovulation, and stimulates the secretory activity of the uterus:
Produces intense edema in the stroma• Increases blood vessel volume threefold • Stimulates the formation of pinopodes, and primes •the decidua.
Steroids regulate the action of uterine growth factorswhich are synthesized at various stages of the men-strual cycle: IGF-I and IGF-II, EGF, HB-EGF, FGF, β-FGF, α-FGF, TGF-β1, PDGF-β.
• A hatched blastocyst can sometimes implant insites outside the uterus, most commonly in the fal-lopian tube. Other sites include the utero-cervicalisthmus (cervical pregnancy) and the utero-tubaljunction; more rarely, implantation can take placein the ovary, or in the peritoneal or abdominalcavity. Occasionally two embryos will implant at diff erent•sites: one in each tube (bilateral tubal pregnancy ) orone in the uterus and one at an ectopic site (hetero-topic pregnancy ). An embryo can continue to grow at an ectopic•site for several weeks, with signs and symptomsof early pregnancy in the mother. If undetected,ectopic pregnancy can result in a life-threateningcrisis due to tubal rupture or erosion into a bloodvessel.

Chapter 6: Implantation and early stages of fetal development
86
13–15 days post ovulation (second week of development) Cells of the inner cell mass separate into two diff er-ent sheets of cells to form a bilaminar embryonic disc ( Figure 6.2 ):
Dorsal germinal layer = epiblast Ventral germinal layer = hypoblast.
Th e fl atter hypoblast cells lie on top of the epiblast, and will form the yolk sac; the epiblast contains the cells of the future embryo.
Th e two layers of the embryonic disc divide the blastocyst into two chambers, the amnion and the yolk sac ( Figure 6.3 ); outside the embryo, the extraembry-onic spaces (chorionic, amniotic, yolk sac) continue to develop, the endometrium is being converted into the decidua , and early placentation has begun. Th e amnion fi lls with fl uid that cushions the developing fetus; the yolk sac contributes to the formation of the extra embryonic membranes, chorion and amnion. It is also the site of early blood cell formation, and part of the yolk sac becomes incorporated into the gut later in development. Th e cells of the trophoblast form another chamber, the extraembryonic coelom around the amnion, yolk sac and developing embryo; this will later become the chorionic sac and placenta .
13–15 days post ovulation (end of second week of development) Embryonic epiblast cells move along the surface, begin to pile up near the center to form a node, and then move internally to create a furrowed cell mass, the primitive streak ( Figure 6.4a ). Th is is a visible feature showing that cells are migrating, and the fur-row begins to extend towards the cranial (head) end of the bilaminar disc ( Figure 6.4b ). Cells near the advan-cing edge of the streak begin to pull apart slightly to form an open pit, and cells bordering this pit then migrate between the epiblast and hypoblast to create a
3.5 dpc
4.5 dpc
ICM
Trophectoderm
Epiblast
Hypoblast(primitiveendoderm)
VE
PE
Extraembryonic ectoderm
5.5 dpc
Peri-implantation development Figure 6.2 Diagram of mouse blastocyst showing epiblast layer. ICM = inner cell mass; VE = visceral endoderm; PE = primitive endoderm; dpc = days post conception. With thanks to Cindy Lu and Elizabeth Robertson.
EM AC YS
Figure 6.3 Diagrammatic representation of human embryo trans-verse section on approximately Day 14 post ovulation, indicating extraembryonic mesoblast (EM), amniotic cavity (AC) and yolk sac (YS, also known as umbilical vesicle).

Chapter 6: Implantation and early stages of fetal development
87
new layer, the mesoderm. Cells from the epiblast also displace the hypoblast , creating the endoderm. Th e cells that remain on the surface will form ectoderm, and this formation of a now trilaminar disc is known as gastrulation . During gastrulation , cells from the mesoderm form the notochord, which will defi ne the primitive axis of the embryo and establish cranio-caudal orientation and bilateral symmetry of the fully developed body. Th e three layers of cells form the pri-mary germ cells that will evolve into the specialized cells, tissues and organs of the body:
Endoderm (inner layer): forms the lining of the primitive digestive tract and its associated glandular structures, as well as portions of the liver, pancreas, trachea and lungs . Mesoderm (middle layer): initially forms a loose aggregate of cells, the mesenchyme; this then organizes into regions that evolve into the vertebral column, skeletal muscle, ribs, skull and the dermis of the skin. Mesenchymal cells also form tubular structures: urogenital system, heart, blood vessels, and the lining of the pericardial, pleural and peritoneal cavities. Ectoderm (outer layer): develops into skin epidermis, brain and spinal cord. Sensory receptors for vision, hearing and smell, as well as the future autonomic nervous system and adrenal medulla, also develop from ectoderm.
17–19 days (third week of development) Aft er gastrulation, the mesoderm starts to segment into mesenchymal tissue somites , and the notochord induces rapid growth in the ectoderm. Over the next 2–3 days the ectodermal layer thickens to form a neural plate, which folds to form a neural groove ( Figure 6.4c ): the nervous system is one of the fi rst organs to develop. During this process of neurola-tion, the ectoderm will subdivide into neural tissue and epithelial tissue lineages (pigmented cells of the epidermis, adrenal medullary cells, skeletal and con-nective tissues of the head). Somites continue to form in the mesoderm, the neural groove fuses dorsally to form a tube at the level of the fourth somite, and closes. Th e cranial end of the neural plate is wider, enclosing the region that will form the brain. Th e spi-nal cord will form at the caudal end, which is narrower
(the notochord is eventually replaced by the vertebral column).
Genes signifi cant in early development
• Homeobox genes are a highly conserved family of transcription factors that switch on cascades of other genes that are involved in the regulation of embry-onic development of virtually all multicellular animals. Wnt genes encode short-range secreted proteins • that are involved in cell adhesion and cell–cell signaling. Cellular adhesion molecules such as the integrins • are important for cellular recognition and binding that infl uence cell migration. Laminin and fi bronec-tin are also involved in cell migration . The fate of a migrating cell is apparently determined • largely by its fi nal destination. RhoB and Slug pro-teins, which promote cell migration, are present at the gastrulation stage, and the loss of N-cadherin helps to initiate the migration of neural crest cells. Hedgehog genes encode signaling molecules that • are involved in patterning processes; this family of genes is named after a Drosophila gene whose loss of function produced an embryo covered with pointed denticles, like a hedgehog. Three homologous genes have been found in mammals: Sonic hedgehog , Shh (named after the Sega Genesis video game), Desert hedgehog , Dhh and Indian hedgehog , Ihh.
Shh is secreted by the notochord, and has numer-• ous critical roles in development, involved in the patterning of many systems, including the brain and spinal cord, as well as in establishing left–right axis patterning. Diff erentiation pathways appear to be infl uenced by diff erent levels of Shh, in com-bination with other paracrine factors, including Wnt and FGF. The Shh transcription pathway controls cell div-• ision in adult stem cells, and has been linked to the formation of some cancerous tumors.
19–23 days (third week) Rapid cellular growth elongates the embryo and expands the yolk sac. Primordial germ cells can be identifi ed at the root of the allantois. A head fold rises on either side of the primitive streak, and endocardial cells begin to fuse and form two endocardial tubes which will develop into the heart. Pairs of mesoder-mal somites can be seen on either side of the neural groove ( Figure 6.4d ), appearing fi rst in the caudal region. Th e neural folds rise and fuse along the length of the neural tube ( Figure 6.5a ) , along with budding
• Homeobox genes are a highly conserved family of transcription factors that switch on cascades of othergenes that are involved in the regulation of embry-onic development of virtually all multicellularanimals. Wnt genes encode short-range secreted proteins• that are involved in cell adhesion and cell–cellsignaling. Cellular adhesion molecules such as the integrins•are important for cellular recognition and bindingthat infl uence cell migration. Laminin and fi bronec-tin are also involved in cell migration . The fate of a migrating cell is apparently determined•largely by its fi nal destination. RhoB and Slug pro-teins, which promote cell migration, are present atthe gastrulation stage, and the loss of N-cadherinhelps to initiate the migration of neural crest cells. Hedgehog genes encode signaling molecules that•are involved in patterning processes; this family of genes is named after a Drosophila gene whose loss of function produced an embryo covered with pointeddenticles, like a hedgehog. Three homologous geneshave been found in mammals: Sonic hedgehog , Shh(named after the Sega Genesis video game), Deserthedgehog , Dhh and Indian hedgehog , Ihh.
Shh is secreted by the notochord, and has numer-•ous critical roles in development, involved in thepatterning of many systems, including the brainand spinal cord, as well as in establishing left–rightaxis patterning. Diff erentiation pathways appearto be infl uenced by diff erent levels of Shh, in com-bination with other paracrine factors, includingWnt and FGF. The Shh transcription pathway controls cell div-• ision in adult stem cells, and has been linked to theformation of some cancerous tumors.

Chapter 6: Implantation and early stages of fetal development
88
somites that close the neural tube (like a zipper). Th e neural tube begins to close in the middle of the embryo (cervical area), and then extends in both cra-nial and caudal directions. Failure of the neural tube to close correctly at this stage can lead to anomalies such as spina bifi da (caudal) or anencephaly (cra-nial). Masses of cells detach themselves from the side
of the neural plate and form the neural crest, precur-sor cells of numerous diff erentiated cells of the ner-vous and glandular systems. Th e heart tube becomes S-shaped, with the beginning of cardiac muscle con-traction. Secondary blood vessels appear in the chor-ion/placenta, and hematopoietic cells appear in the yolk sac.
Figure 6.4 Third week of fetal development, dorsal views; dates are approximate, stages overlap. (a) 13 days post ovulation, Carnegie Stage 6; primitive streak and node(bottom) and prechordal plate (top). (b) 16 days post ovulation, Carnegie Stage 7; neurolation. (c) 17–19 days post ovulation, Carnegie Stage 8; primitive pit, notochordal and neurenteric canals. (d) 19–21 days post ovulation, Carnegie Stage 9; appearance of somites. Illustrations by Luke Ebbutt-James, Cambridge, UK.
Actual Size 0.2mm(a) (b)
(c) (d)
Actual Size 0.4mm
Actual Size 1.0 - 1.5mm Actual Size 1.5 - 2.5mm

Chapter 6: Implantation and early stages of fetal development
89
Figure 6.5 Fourth week of fetal development, dorsal views; dates are approximate, stages overlap. (a) 21–23 days post ovulation, Carnegie Stage 10; neural folds/heart folds begin to fuse. (b) 25–27 days post ovulation, Carnegie Stage 12; upper limb buds appear. (c) 26–30 days post ovulation, Carnegie Stage 13; pharyngeal arches and upper limb buds visible. (d) 31–35 days post ovulation, Carnegie Stage 14; esophagus forming, lens vesicle opens to the surface and optic cup develops, upper limb buds elongate and taper. Illustrations by Luke Ebbutt-James, Cambridge, UK.
Actual Size 1.5 - 3.0mm(a) (b)
(c) (d)
Actual Size 3.0 - 5.0mm
Actual Size 4.0 - 6.0mm
Somites
Actual Size 5.0 - 7.0mm
23–27 days (fourth week) A primitive S-shaped tubal heart begins to beat, and the developing neural tube curves the embryo into a C-shape ( Figure 6.5b ). Th e forebrain is closed when 20 somites are present, eyes and ears begin to form, and pharyngeal arches are present. Valves and septa begin to appear in the heart, and a blood circulatory system continues to develop.
28–35 days (fi fth week) Somites organize themselves into myotomes, the groups of tissues that will develop into the musculo-skeletal structure of the body wall, and rudiments of the ribs and limbs begin to appear ( Figure 6.5c and d ). Sclerotomes give rise to the axial skeleton, myotomes to striated muscle, and dermatomes to subcutaneous tissue and skin. Arches that form the face and neck can

Chapter 6: Implantation and early stages of fetal development
90
be seen under the enlarging forebrain. Th e digestive epithelial layer begins to diff erentiate into the future locations of the liver, lung, stomach and pancreas.
35–42 days (sixth week) By Day 35 (fi ft h week of development = 6 weeks from last menstrual period), when clinical pregnancy aft er
IVF can be confi rmed by ultrasound visualization of gestational sac and fetal heartbeat ( Figure 6.6 ), the three primary germ layers have expanded and under-gone a dramatic process of diff erentiation and trans-formation, to form a clearly recognizable fetus. Th e beating heart has chambers, and all limbs and body systems are under development. Medial thickening of
(a) (b)
(c) (d)
(e)
Figure 6.6 Ultrasound scans of early pregnancy. (Images courtesy of Baby Premier, division of Specialist Medical Imaging Ltd.) (a) Six-week scan, showing crown–rump length (crl) = 6.89 mm, = 6 weeks + 4 days. (b) Another view of (a), illustrating fetal pole. (c) Twelve-week scan, crl= 65.57 mm, = 12 weeks+6 days. (d) Thirteen-week scan, clear view of head and body. (e) Another view of (d), showing the vertebral column.

Chapter 6: Implantation and early stages of fetal development
91
the coelomic epithelium represents the formation of primordial gonads. Th e size of the fetus is now approxi-mately 7.0–9.0 mm, and it will continue to grow at a rate of around 1 mm per day during the fi rst trimester.
By the beginning of the second trimester, the basic brain structure is complete, and genitalia begin to show signs of gender characteristics.
Ultrasound confi rmation of clinical pregnancy
1. Gestational sac : can be seen at around 4 weeks’ gestation, but may not be visible until the end of the fi fth week. It is characteristic of early pregnancy, but does not correspond to anatomical features of the embryo. Gestational sacs are also found in ectopic pregnancies.
2. Yolk sac : visible during the fi fth week, and grows to be no larger than 6 mm. Larger yolk sacs usually indicate an abnormal pregnancy; yolk sacs that are misshapen, are “fl oating” within the gestational sac and contain echogenic (instead of sonolucent) material are ominous fi ndings for the pregnancy.
3. Fetal heartbeat (FH ): using transvaginal ultra-sound, fetal cardiac activity can sometimes be seen along the edge of the yolk sac before a fetal cell mass is identifi able. In normal pregnancies, the fetal heartbeat may not be seen until the fetal pole is around 4 mm in size. Failure to identify a FH in a fetus >4 mm in size is an ominous sign.
4. Fetal pole : the fetus in its somite stage, fi rst vis-ible separation from the yolk sac by transvaginal scan (TVS) just after 6 weeks gestation (Day 35 post ovulation).
5. Crown–rump length (CRL ): single most accur-ate measure of gestational age up to 12 weeks gestation.
Pregnancy failures
1. Miscarriage : spontaneous abortion prior to 20 weeks’ gestation.
2. Biochemical pregnancy : early pregnancy loss, prior to 6 weeks from last menstrual period.
3. Blighted ovum : anembryonic gestation. Sac appears normal on TVS, but an embryo never develops; probably due to early embryonic death with continued trophoblast development.
4. Missed abortion : nonviable intrauterine preg-nancy that has not yet aborted. TVS shows ges-tational sac with no FH; can be due to a blighted ovum, or early demise of an embryo after detection of FH. The cervical os is closed.
5. Threatened abortion : vaginal bleeding and/or abdominal/pelvic pain during early pregnancy; the
cervical os is closed, and no tissue has been passed. FH is still present on TVS .
6. Inevitable abortion : vaginal bleeding, usually with abdominal pain and cramps. FH is absent, cervical os is open, but no tissue has been passed. Usually progresses to complete abortion.
7. Incomplete abortion : Heavy vaginal bleeding, with tissue having been passed, but some remain-ing in utero.
8. Complete abortion : bleeding, abdominal pain, all products of conception have been passed; empty uterus must be confi rmed by TVS.
9. Recurrent abortion : history of more than three spontaneous abortions.
Further reading Implantation Bourgain C , Devroey P ( 2007 ) Histologic and functional
aspects of the endometrium in the implantatory phase . Gynecologic and Obstetric Investigation 64 (3): 131 –133.
Campbell S , Swan HR , Seif MW , Kimber SJ , Aplin JD ( 1995 ) Cell adhesion molecules on the oocyte and preimplantation human embryo . Molecular Human Reproduction 1 (4): 171 –178.
Cheon YP , Xu X , Bagchi MK , Bagchi IC ( 2003 ) IRG1 is a novel target of progesterone receptor and plays a critical role during implantation in the mouse . Endocrinology 144 (12): 5623 –5630.
Duc-Goiran P , Mignot TM , Bourgeois C , Ferré F ( 1999 ) Embryo-maternal interactions at the implantation site: a delicate equilibrium (Review) . European Journal of Obstetrics, Gynecology, and Reproductive Biology 83 (1): 85 –100.
Grewal S , Carver JG , Ridley AJ , Mardon HJ ( 2008 ) Implantation of the human embryo requires Rac1 dependent endometrial stromal migration . Proceedings of the National Academy of Sciences USA 105 : 16189 –16194.
Horcajadas JA , Pellicer A , Simón C ( 2007 ) Wide genomic analysis of human endometrial receptivity: new times, new opportunities . Human Reproduction Update 13 (1): 77 –86.
King A , Burrows T , Verma S , Hiby S , Loke YW ( 1998 ) Human uterine lymphocytes . Human Reproduction Update 4 (5): 480 –485.
Kliman HJ ( 2000 ) Th e story of decidualization, menstruation, and trophoblast invasion . American Journal of Pathology 157 : 1759 –1768.
Lee K , Jeong J , Kwak I , et al . ( 2006 ) Indian hedgehog is a major mediator of progesterone signaling in the mouse uterus . Nature Genetics 38 : 1204 –1209.
1. Gestational sac: can be seen at around 4 weeks’ gestation, but may not be visible until the end of the fi fth week. It is characteristic of early pregnancy, but does not correspond to anatomical features of the embryo. Gestational sacs are also found in ectopic pregnancies.
2. Yolk sac : visible during the fi fth week, and grows to be no larger than 6 mm. Larger yolk sacs usually indicate an abnormal pregnancy; yolk sacs that are misshapen, are “fl oating” within the gestational sac and contain echogenic (instead of sonolucent) material are ominous fi ndings for the pregnancy.
3. Fetal heartbeat (FH): using transvaginal ultra-sound, fetal cardiac activity can sometimes be seen along the edge of the yolk sac before a fetal cell mass is identifi able. In normal pregnancies, the fetal heartbeat may not be seen until the fetal pole is around 4 mm in size. Failure to identify a FH in a fetus >4 mm in size is an ominous sign.
4. Fetal pole : the fetus in its somite stage, fi rst vis-ible separation from the yolk sac by transvaginal scan (TVS) just after 6 weeks gestation (Day 35 post ovulation).
5. Crown–rump length (CRL ): single most accur-ate measure of gestational age up to 12 weeks gestation.
1. Miscarriage : spontaneous abortion prior to 20 weeks’ gestation.
2. Biochemical pregnancy : early pregnancy loss, prior to 6 weeks from last menstrual period.
3. Blighted ovum: anembryonic gestation. Sac appears normal on TVS, but an embryo never develops; probably due to early embryonic death with continued trophoblast development.
4. Missed abortion : nonviable intrauterine preg-nancy that has not yet aborted. TVS shows ges-tational sac with no FH; can be due to a blighted ovum, or early demise of an embryo after detection of FH. The cervical os is closed.
5. Threatened abortion : vaginal bleeding and/or abdominal/pelvic pain during early pregnancy; the
cervical os is closed, and no tissue has been passed.FH is still present on TVS .
6. Inevitable abortion : vaginal bleeding, usually withabdominal pain and cramps. FH is absent, cervicalos is open, but no tissue has been passed. Usuallyprogresses to complete abortion.
7. Incomplete abortion: Heavy vaginal bleeding,with tissue having been passed, but some remain-ing in utero.
8. Complete abortion: bleeding, abdominal pain, allproducts of conception have been passed; emptyuterus must be confi rmed by TVS.
9. Recurrent abortion: history of more than threespontaneous abortions.

Chapter 6: Implantation and early stages of fetal development
92
Mardon H , Grewal S ( 2007 ) Experimental models for investigating implantation of the human embryo . Seminars in Reproductive Medicine 25 : 410 –417.
Nikas G , Drakakis P , Loutradis D , et al . ( 1995 ) Uterine pinopodes as markers of the ‘nidation window’ in cycling women receiving exogenous oestradiol and progesterone . Human Reproduction 10 (5): 1208 –1213.
Parr MB , Parr EL ( 1964 ) Uterine luminal epithelium: protrusions mediate endocytosis, not apocrine secretion, in the rat . Biology of Reproduction 11 (2): 220 –233.
Psychoyos A ( 1986 ) Uterine receptivity for nidation . Annals of the New York Academy of Sciences 476 : 36 –42.
Psychoyos A , Nikas G , Gravanis A ( 1995 ) Th e role of prostaglandins in blastocyst implantation . Human Reproduction 10 (Suppl. 2): 30 –42.
Sherwin JR , Sharkey AM , Cameo P , et al . ( 2007 ) Identifi cation of novel genes regulated by hCG in baboon endometrium . Endocrinology 148 : 618 –626.
Simon C , Gimeno MJ , Mercader A , et al . ( 1997 ) Embryonic regulation of integrins in endometrial epithelial cells . Journal of Clinical Endocrinology and Metabolism 82 : 2607 –2616.
Simon L , Spiewak KA , Ekman GC , et al . ( 2009 ) Stromal progesterone receptors mediate induction of IHH in uterine epithelium . Endocrinology 150 : 3871 –3876.
Wang H , Dey SK ( 2006 ) Roadmap to embryo implantation . Nature Reviews, Genetics 7 : 185 –199.
Wilcox AJ , Baird DD , Dunson D , McChesney R , Weinberg CR ( 2001 ) Natural limits of pregnancy testing in relation to the expected menstrual period . JAMA 286 (14): 1759 –61. Erratum in: JAMA 2002;287(2): 192.
Wilcox AJ , Baird DD , Weinberg CR ( 1999 ) Time of implantation of the conceptus and loss of pregnancy . New England Journal of Medicine 340 (23): 1796 –1799.
Embryogenesis www.visembryo.com http://embryology.med.unsw.edu.au/ Dorus S , Anderson JR , Vallender EJ , et al . ( 2006 ) Sonic
Hedgehog, a key development gene, experienced intensifi ed molecular evolution in primates . Human Molecular Genetics 15 (13): 2031 –2037.
Gilbert SF ( 2000 ) Developmental Biology . Sinauer Associates , Sunderland, MA .
Herzog W , Zeng X , Lele Z , et al . ( 2003 ) Adenohypophysis formation in the zebrafi sh and its dependence on sonic hedgehog . Developmental Biology 254 : 1.
O’Rahilly RF , Müller F ( 1987 ) Developmental Stages in Human Embryos . Carnegie Institution of Washington , Washington, DC .

Chapter
93
Stem cell biology
Stem cells and stem cell lines Every cell in an individual has a unique chromosome complement, with 20 000–25 000 genes coded into a DNA sequence of 3 billion base pairs, packed into 23 pairs of chromosomes: a total of 46 chromosomes in each diploid human cell. All of these cells have the same genetic information, copied during mitotic divisions by replicating the DNA in each cell cycle . Th e pattern of gene activity in each cell (gene expression/transcrip-tion) dictates its function and fate, enabling diff erent cells to diff erentiate and carry out distinct functions.
Aft er an oocyte has been fertilized the one-cell zygote is totipotent , with the potential to give rise to a complete organism, including both embryonic and extraembryonic cells. As cell division proceeds, blast-omeres lose the potential to give rise to an entire organ-ism, and by the time that a fully expanded blastocyst has formed, three types of morphologically and molecu-larly distinct cells have emerged: trophectoderm cells surround an inner cell mass, which contains epi-blast progenitor cells and primitive endoderm cells. Th e embryo itself is derived exclusively from epiblast progenitor cells; trophectoderm cells will form fetal components of the placenta, and primitive endoderm will form the yolk sac, which is derived from extrae-mbryonic endoderm. Continued development of the embryo requires the support of both of these extraem-bryonic cell types.
Epiblast progenitor cells of the blastocyst inner cell mass are considered to be pluripotent , as they have the potential to give rise to the three primary germ layers that will form all of the tissues of the fetus: mesoderm, endoderm and ectoderm. Signifi cantly, these progeni-tor cells do not have the potential to give rise to a whole organism without the supporting extraembryonic cells. Following implantation, the pluripotent embry-onic cells become committed to more specialized
cells that increasingly lose their potential to contrib-ute to all three germ layers. Multipotent cells have been identifi ed in the developing embryo and in the adult, which have the potential to continually give rise to the same cell ( self-renew ) and also have the poten-tial to give rise to other cells with a more specialized function. Hematopoietic stem cells are multipotent cells that replenish all blood cells by dividing to form two types of cell: one daughter cell maintains a stem cell population, and the second daughter cell has the potential to continue to alter its pattern of gene expres-sion and diff erentiate. Th e daughter cells that become more specialized with each cell division go through distinct populations of transit amplifying cells , pro-liferative cells that retain their self-renewal property until they reach the end of their production line, and are terminally diff erentiated. Other types of stem cell, such as neural stem cells are oligopotent , giving rise to diverse but restricted populations of specifi c self-renewing subtypes. Unipotent cells, such as spermato-gonial stem cells, are self-renewing cells that have the potential to give rise to a single lineage, spermatogonia. Figure 7.1 illustrates a hierarchy of stem cell potential.
Two properties are unique to all types of stem cell: 1. Th ey have the capacity for long-term self-renewal. 2. Th ey have the potential to give rise to cells other
than themselves.
A stem cell line is a population of cells that has been grown and maintained in vitro. When maintained under appropriate conditions, these cells continue to grow in tissue culture for very long periods of time.
Mammalian stem cell lines Following the fi rst derivation and culture of human embryonic stem cell lines in the late 1990s (Th omson et al ., 1998 ), debate and controversy escalated
7
In-Vitro Fertilization: Th ired Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 7: Stem cell biology
94
surrounding the use of surplus human embryos donated for research. Despite the controversial ethico-legal perspectives, in many countries throughout the world, IVF clinics have embryos that are either unsuitable for treatment, or are surplus to the patient’s requirements. Given the opportunity for appropri-ate counseling and informed consent, many patients choose to make a contribution to science by donating surplus embryos for research rather than allowing them to perish (Franklin et al ., 2008 ). Th ere is no doubt that embryos donated for stem cell research represent a very valuable resource for scientifi c investigation, with the potential to make a signifi cant contribution to our understanding of early developmental proc-esses and the molecular pathology of disease. Stem cell biology has become an integral part of ART; the principles and the science underpinning this new area of developmental and regenerative biology should be
viewed within the perspective and frame of reference of the fi rst stages of postimplantation development, as presented in the brief synopsis in Chapter 6 .
Human embryonic stem cells (hESCs) Human embryonic stem cells are derived from the in-vitro expansion of epiblast progenitors within the inner cell mass of a preimplantation blastocyst. hESCs are capable of indefi nite self-renewal, and maintain the potential to diff erentiate into cell types from the three embryonic germ layers (pluripotency). Because they remain pluripotent when maintained in vitro, they provide an ideal resource for investigating and study-ing the pathways that lead to the establishment of cells that might be relevant to clinical treatment, such as dopamine-producing neurons and insulin-producing cells of the pancreas.
Th e goal of hESC research is to elucidate the path-ways that direct diff erentiation in vitro, with the aim of providing functional and therapeutically relevant cells. Th ese cells can be used to investigate mechanisms of disease progression, and for research into drugs that might inhibit or reverse pathological processes. hESCs also provide an insight into aspects of early embry-onic development that are otherwise inaccessible to research, due to ethical and practical considerations; they can be used as a tool to investigate how cells can be manipulated to regenerate damaged or diseased cells in the human body. Lastly, hESC-diff erentiated cells may eventually prove to be useful in cell transplantation approaches for the treatment of disease.
Several strategies have been applied to promote the diff erentiation or selection of therapeutically relevant cell types, including the addition of growth factors, cytokines and other ways of manipulating gene expres-sion. One major hurdle to this approach is that the process of directing the diff erentiation of hESCs into functionally relevant specialized cells is very ineffi -cient. Th is ineffi ciency may be the result of heterogen-eity within a starting stem cell population, in addition to the lack of information about the developmental events that promote the emergence of specialized cells in vivo. Th e constraints of in-vitro culture conditions also hinder the ability to mimic in-vivo events.
Tissue stem cells in fetal or adult tissue can supply cells to parts of the body that require a continuous sup-ply of regenerative cells. Tissue stem cells include blood and intestinal stem cells – these are partially committed cells that can function to regenerate their respective adult
Totipotentnon-self-renewing
Restriction Cell Source
Pluripotentself-renewing
Broad potentialself-renewing
Limited potentiallimited self-renewal
Limited divisionnon-functional
Non-mitoticfunctional
Zygote
Embryonicstem cell
Multipotentstem cells
Tissueprogenitor
Committedprogenitors
Differentiated
Neuron,cardiomyocyte,hepatocyte, etc.
Progenitor-1 Progenitor-2
Glia, cardiacmuscle, etc.
Zygote
Blastocyst
Embryo or adultbrain,
bone marrow,cord blood
Brain orspinal cord,
GI tract, heart
Brain subregion,skin, pancreas,
liver
Specifictissue/organ
sites
Figure 7.1 Potential pathways for stem cell development (Adapted from: FH Gage, Mammalian neural stem cells (2000) Science 1433. With permission from AAAS.)

Chapter 7: Stem cell biology
95
tissues as required. Th ey commonly reside in a micro-environment ( niche ) in a quiescent state where they are provided with signals and support that promote the maintenance of self-renewal. Stem cells exit the niche as they undergo cellular commitment /diff erentiation.
Multipotent stem cells All blood cell types are continuously replaced • from a store of hematopoietic stem cells (HSCs) in the bone marrow. Th e lining of the gut (gut epithelium) has intestinal • stem cells in the small intestine that produce four diff erent cell lineages (Paneth, goblet, absorptive columnar, enteroendocrine). Epidermal stem cells in the skin and hair follicle • can regenerate damaged epithelium. Skeletal muscle stem cells (satellite cells) are • quiescent cells that can also give rise to committed progeny such as myofi bers in response to injury or disease.
Oligopotent stem cells Neural stem cells are restricted self-renewing • subtypes that give rise to three lineages: neurons, oligodendrocytes, astrocytes.
Unipotent stem cells
Spermatogonial stem cells give rise to • spermatogonia.
HSCs in treatment
• Leukemias, lymphomas and other blood disorders have been successfully treated with bone marrow transplants since the 1960s. The donor tissue must be human leukocyte antigen (HLA) matched to that of the recipient, or the cells will be rejected by the recipient’s immune system. During the past decade, IVF in combination with • preimplantation genetic diagnosis (PGD) has been used to select embryos that are HLA matched to a sibling who has a blood disorder. Cord blood iso-lated from the baby (“savior sibling”) at the time of delivery is then prepared to provide a supply of HSCs for transplant to the sibling. It had been suggested that HSCs may have “plasti-• city”, i.e., the ability to engraft in other locations and then transdiff erentiate to cell types appropriate to their new location. However, so far this concept is unsubstantiated, and there is no evidence that blood-forming stem cells can serve as a signifi cant source of regenerative cells in the repair of non-blood tissues.
Diff erentiation Cells can be distinguished from one another by their patterns of gene expression, which includes expres-sion of both protein coding and noncoding RNAs, the secretion of proteins, their response to extracel-lular signals and the distribution of epigenetic chro-matin modifi cation. Changes to any or all of these processes can infl uence the diff erentiation of stem cells. For example, hESCs express the transcription factors OCT4, NANOG and SOX2 and require extra-cellular signals such as fi broblast growth factor (FGF) and Activin/Nodal to maintain self-renewal. Changes in the levels and balance between FGF and Activin/Nodal can infl uence the maintenance and diff erenti-ation of hESCs: in the presence of too much Activin/Nodal they resemble endoderm cells, and too little Activin/Nodal will cause diff erentiation into ectoderm cells. Th e mechanisms involved in the maintenance of hESCs is poorly elucidated, but is likely to involve cell signaling pathways that function at diff erent levels, with multiple feedback controls and intercellular gene regulation: 1. Gene expression: transcription factors are
proteins that function to promote or repress gene expression at the DNA level. For example, OCT4 is thought to maintain hESCs by binding to genomic regulatory regions to promote the expression of pluripotency-associated genes and repress the expression of genes associated with diff erentiation.
2. Extracellular signals: small proteins that are produced and secreted ( cytokines ) by a stem cell niche can contribute to the maintenance of self-renewal. These proteins are often required to maintain stem cells in culture, such as the addition of cytokines FGF and epidermal growth factor (EGF) to neural stem cells grown in vitro.
3. Chromatin modifi cations: DNA is packaged with histones to form nucleosomes. Post-translational modifi cation of histone tails forms a code that can determine states of gene expression that are heritable, modifying gene expression by infl uencing the access of transcription factors to genomic regulatory regions.
4. Physical context: the presence of extracellular matrix and physical contact with other cells can infl uence the maintenance and diff erentiation potential of stem cells.
• Leukemias, lymphomas and other blood disorders have been successfully treated with bone marrow transplants since the 1960s. The donor tissue must be human leukocyte antigen (HLA) matched to that of the recipient, or the cells will be rejected by the recipient’s immune system. During the past decade, IVF in combination with • preimplantation genetic diagnosis (PGD) has been used to select embryos that are HLA matched to a sibling who has a blood disorder. Cord blood iso-lated from the baby (“savior sibling”) at the time of delivery is then prepared to provide a supply of HSCs for transplant to the sibling. It had been suggested that HSCs may have “plasti-•city”, i.e., the ability to engraft in other locations and then transdiff erentiate to cell types appropriate to their new location. However, so far this concept is unsubstantiated, and there is no evidence that blood-forming stem cells can serve as a signifi cant source of regenerative cells in the repair of non-blood tissues.

Chapter 7: Stem cell biology
96
Potential therapeutic applications for ESCs
1. Platform for drug discovery: hESCs can be diff eren-tiated into clinically relevant cells from individuals that harbor disease-associated gene expression. For example, hESCs have been established from individuals with amyotrophic lateral sclerosis and these hESCs were diff erentiated to motor neurons, the cells that are damaged in these patients. These hES-diff erentiated cells can be used to screen for small molecules (drugs) that might inhibit the pro-gression of the disease and be eff ective in patient treatment.
2. Exogenous: transplantation of stem cells that have been diff erentiated in vitro towards a particular cell lineage, e.g., neuronal stem cells for neurodegener-ative diseases that involve death or dysfunction of just one, or a few cell types, such as dopaminergic neurons to treat Parkinson’s disease, insulin-pro-ducing B-cells to treat diabetes, etc. This approach has at least two signifi cant considerations :
in-vitro stem cell diff erentiation must be com-• pletely controlled, as there may be a possibility of malignant transformation transplant rejection unless the cells are immune • matched.
3. Autologous: the patient’s own stem cells are manip-ulated in vitro to induce/repress gene expression, and returned to the specifi c site that requires healing/treatment.
4. Endogenous stem cell renewal: the patient’s own stem cells are manipulated to renew themselves in situ; this requires:
identifi cation of stem cells in diff erent parts of the • body interpretation of how they interact with their • niche/microenvironment.
Evolution of stem cell research Th e derivation of human ESCs in 1998 ignited an explo-sion of interest in stem cell biology and its therapeutic potential, and research in the fi eld evolved very rapidly over the subsequent decade. In the words of the French philosopher Auguste Comte (1798–1857) “To under-stand science, it is necessary to know its history,” and this is particularly true of stem cell science, where each signifi cant achievement has been based upon the fi nd-ings of prior decades of research. Successful derivation of human ESCs was based on research using murine ESCs, and this required information that was gained from previous stem cell models using mouse and human embryonal carcinoma cell lines. Similarly, the recent elucidation of discrete factors that can induce somatic cells into forming pluripotent stem cells
(iPSCs) depended on studies in mouse and human embryonic stem cells. Th ere is no doubt that novel trends will continue to emerge, and in order to fully comprehend the potential and the possible directions that lie in the future of stem cell research, it is import-ant to be aware of the milestones that have marked its evolution so far.
Early culture systems During the early 1960s, Robert Edwards recognized the extraordinary potential of stem cell biology, and in collaboration with Robin Cole isolated stem cells from the inner cell mass (ICM) of rabbit blastocysts . Th ey cultured zona-free rabbit ICM on collagen sur-faces, sometimes with HeLa feeder layers, and estab-lished cell colonies that showed diff erentiation to muscle, blood islands, neurons and complex groups of diff erentiating cells ( Figure 7.2 ). Four immortal cell lines (two epithelioid and two fi broblastic) that sur-vived more than 200 generations of subculture were established and cryopreserved. All cell lines remained diploid for several generations (Cole et al ., 1965 , 1966 ; Edwards, 2008 ).
In further studies with Richard Gardner ( 1968 ), ICM cells isolated from mice with marker (coat color) genes were injected directly into the blastocoelic cav-ity of recipient mice, forming chimeras which showed that the graft ed cells had colonized several diff erent tissues; this indicated that the injected ICM cells were multipotent (Gardner, 1968 ). Aft er human blasto-cysts fi rst became available through IVF, Edwards and his team attempted to prepare human ESCs in vitro (Fishel et al ., 1984 ), but this early work had to be aban-doned due to ethico-legal problems surrounding the use of human embryos for research.
Embryonal carcinoma (EC) and embryonal germ (EG) cell lines In the early 1970s, stem cell lines that could be propa-gated in vitro were derived from murine teratocarcin-omas (Kahn and Ephrussi, 1970 ); these cell lines were capable of unlimited self-renewal and multilineage diff erentiation. Mouse EC cells express antigens and proteins that are similar to cells present in the ICM, which led to the concept that EC cells are an in-vitro counterpart of the pluripotent cells present in the ICM (Martin, 1981 ); this provided the intellectual frame-work for working towards derivation of both mouse and human embryonic stem (ES) cells. Human EC
1. Platform for drug discovery: hESCs can be diff eren-tiated into clinically relevant cells from individualsthat harbor disease-associated gene expression.For example, hESCs have been established fromindividuals with amyotrophic lateral sclerosis andthese hESCs were diff erentiated to motor neurons,the cells that are damaged in these patients. ThesehES-diff erentiated cells can be used to screen forsmall molecules (drugs) that might inhibit the pro-gression of the disease and be eff ective in patienttreatment.
2. Exogenous: transplantation of stem cells that havebeen diff erentiated in vitro towards a particular celllineage, e.g., neuronal stem cells for neurodegener-ative diseases that involve death or dysfunction of just one, or a few cell types, such as dopaminergicneurons to treat Parkinson’s disease, insulin-pro-ducing B-cells to treat diabetes, etc. This approachhas at least two signifi cant considerations :
in-vitro stem cell diff erentiation must be com-•pletely controlled, as there may be a possibility of malignant transformation transplant rejection unless the cells are immune•matched.
3. Autologous: the patient’s own stem cells are manip-ulated in vitro to induce/repress gene expression,and returned to the specifi c site that requireshealing/treatment.
4. Endogenous stem cell renewal: the patient’s ownstem cells are manipulated to renew themselves insitu; this requires:
identifi cation of stem cells in diff erent parts of the•body interpretation of how they interact with their•niche/microenvironment.

Chapter 7: Stem cell biology
97
Figure 7.2 Cell colonies derived from intact zona-free rabbit blastocysts after 20 days in culture (Cole et al ., 1966 ). (a) Cell masses derived from a zona-free rabbit blastocyst. (b) Muscle diff erentiating after continued culture. (c) A single blood island that developed among cell outgrowths from rabbit ICM. (d) A group of neurons in the same outgrowths. (e) A complex group of diff erentiating cells in which muscle cells are mixed with various types of diff erentiating cells – a pathologist discerned several cell types in this mass of cells. (Reprinted with permis-sion from: RG Edwards, Reproductive Biomedicine Online , 2008 )
(a) (b)
(c) (d)
(e)
lines were established in 1977 (Hogan et al ., 1977 ), and these proved to diff er from mouse EC lines, both in expression of surface markers, and in their in-vitro properties. Unlike mouse EC lines, the human cells are highly aneuploid, and have a limited ability to
diff erentiate into a wider range of somatic cell types. Nonetheless, these human cell lines provided a useful model in which to study cell diff erentiation (Andrews et al ., 1984b ; Th ompson et al ., 1984 ; Pera et al ., 1989 ). Both mouse and human EC culture systems enabled

Chapter 7: Stem cell biology
98
numerous improvements in technique and method-ology, as well as initiating studies on factors that are involved in the control of diff erentiation in vitro.
Stem cell lines derived from mouse testicular tera-tomas (EG cells) were found to contribute to a variety of tissues in chimeras, including germ cells (Stevens, 1967 ); this provided a practical way to introduce modifi cations to the mouse germline (Bradley et al ., 1984 ). Pluripotent EG cells were successfully derived directly from primordial germ cells in vitro in 1992 (Matsui et al ., 1992 ; Resnick et al ., 1992 ).
Mouse embryonic stem cells Using culture conditions that had been used for mouse EC cells (inactivated fi broblast feeder layers and serum), the fi rst mouse ES cell lines were derived from the ICM of mouse blastocysts (Evans and Kaufman, 1981 ; Martin, 1981 ). It was subsequently found that the effi ciency of mouse ES cell derivation is strongly infl uenced by genetic background, and that diff er-ent culture conditions were required for strains that were initially thought to be nonpermissive. Further experiments revealed that mouse ES cells could be sus-tained by conditioned medium, harvested from feeder layers, in the absence of the feeder cells themselves. Fractionation of conditioned medium, led to the iden-tifi cation of leukemia inhibitory factor (LIF) as one of the cytokines that sustains mouse ES cells (Smith et al ., 1988 ; Williams et al ., 1988 ). LIF activates the transcrip-tion factor Stat3, which inhibits diff erentiation and promotes viability. Further investigation of the signal-ing pathways showed that the proliferative eff ect of LIF requires a fi nely tuned balance between positive and negative eff ectors/factors. If serum is removed from the medium, mouse ES cells can be maintained in an undiff erentiated state by adding LIF in combination with bone morphogenetic protein (BMP), a member of the TGF-alpha superfamily (Ying et al ., 2003 ).
Th e subsequent two decades of research using murine ESCs led to numerous advances in culture system techniques and technology, and the identifi -cation of several types of in-vitro diff erentiated cells (including neural tissue) introduced the therapeutic potential and hope of eventual therapies to treat degenerative diseases – neurodegenerative disease in particular. Th e murine ES model contributed enor-mously to many diff erent aspects of developmental biology: a large collection of genes, factors, markers, and signaling pathways involved in diff erentiation
have now been identifi ed, providing clues towards achieving directed diff erentiation of these pluripotent cells in vitro (Yu et al ., 2007 ).
Human embryonic stem cells (hESCs) A considerable delay (17 years) ensued between the derivation of mouse ES cells in 1981, and the fi rst estab-lishment of human ES cell lines in 1998. Th is was due to at least two factors: 1. Suboptimal media and conditions for human
embryo culture meant that human blastocysts were rarely available (especially for research purposes). Media optimized for extended culture was introduced during the mid-1990s, and blastocyst culture then became a more practical reality.
2. Initial culture systems for hESC derivation were based on those that were successful in the mouse, and it eventually became apparent that there are signifi cant species-specifi c diff erences between mouse and human ES cells.
Isolation of ICMs from human blastocysts was reported in 1994 (Bongso et al ., 1994 ), but they were cultured in conditions that allowed derivation of mouse ES cells, and this resulted only in diff erenti-ation of the human cells instead of their derivation into stable pluripotent cell lines. In the mid-1990s, ES cell lines were derived from two nonhuman primates: the rhesus monkey and the common marmoset (Th omson et al ., 1995 , 1996 ). Using experience gained from these primate models, in 1998 Th ompson and his colleagues then reported the isolation of pluripotent stem cell lines derived from human blastocyst ICM cultured on inac-tivated mouse feeder layers. Th ese cell lines expressed markers for pluripotency, and could be maintained undiff erentiated in long-term culture. Th e cultured cells also maintained the potential to form derivatives from all three germ layers when injected into severe combined immunodefi ciency (SCID) mice. Media containing LIF and its related cytokines, required for mouse ESCs, failed to support human or nonhuman primate ES cells (Th omson et al ., 1998 ; Dahéron et al ., 2004 ; Humphrey et al ., 2004 ); the fact that fi broblast feeder layers supported both mouse and human ES cells was apparently a fortunate coincidence.
Reubinoff et al . ( 2000 ) then reported directed dif-ferentiation of hESCs, producing three neural cell lines (astrocytes, dendrocytes, mature neurons) from an early

Chapter 7: Stem cell biology
99
neural progenitor stem cell in spontaneously diff eren-tiating cultures. A huge expansion in research activity followed this initial report, and over the next few years panels of markers associated with pluripotency and with stages of diff erentiation were identifi ed. Research continues into elucidating pathways of diff erentiation, and identifying factors that sustain hESCs in culture, as well as active factors that decay with de- diff erentiation, or change during re-diff erentiation. Th e body of pub-lished literature surrounding hESCs is now vast; by manipulating culture conditions, spontaneous dif-ferentiation to numerous diff erent cell types has been observed, including beating heart cells (Mummery et al ., 2002 ), insulin-secreting cells, hepatocytes, car-tilage, etc. Protocols are now available for directing at least partial diff erentiation of hESCs towards numerous diff erent fates: early endoderm, hepatic cells, pancre-atic cells, cardiomyocytes, endothelial cells, osteogenic cells, hematopoietic cells, lymphocytes, myeloid cells, etc (see Sullivan et al ., 2007 ). hESC lines have also been genetically modifi ed, with fl uorescent reporter genes introduced into key gene loci that can be traced during in-vitro diff erentiation in order to identify subsets of cells along developmental pathways (Davis et al ., 2008a ; Hatzistavrou et al ., 2009 ).
Epiblast stem cells (EpiSCs) As described in Chapter 6 , one of the fi rst stages of post-implantation development is the separation of the ICM into two lineages, the hypoblast and the pluripotent epiblast. Experiments with mouse embryos established that the epiblast in the late blastocyst is functionally and molecularly distinct from blastomeres, and from the ICM (Nichols and Smith, 2009 ). A strategically important milestone was reached in 2007, with the isolation of pluripotent stem cell lines derived from postimplantation (E5.5 to E6) mouse and rat epiblast (Brons et al ., 2007 ; Tesar et al ., 2007 ). Intriguingly, these EpiSCs diff er signifi cantly from mouse ESCs, but have key features in common with human cells. Th e two fac-tors required for mouse ESC derivation (LIF and/or BMP4) have no eff ect on epiblast cell isolation, a simi-lar situation to human ESC derivation. Instead, the sig-naling factors that are important for human ESCs (FGF and Activin/Nodal) are apparently critical for EpiSC derivation. Th e pattern of gene expression by EpiSCs diff ers from that of mouse ESCs, but they do retain the ability to proliferate indefi nitely, as well as the poten-tial for multilineage diff erentiation. Mouse ES cells can
be induced to become EpiSCs, and the reverse transi-tion has recently been observed (Bao et al ., 2009 ). It is possible that the unique properties that hESCs have in common with EpiSCs could refl ect a diff erent origin that had not previously been recognized in hESC, i.e., they may represent a later stage of development (post-implantation epiblast) than mouse ES cells; Activin/Nodal signaling seems to have an evolutionarily con-served role in the maintenance of pluripotency. Th is also reinforces the signifi cant species-specifi c diff er-ences in embryology and signaling pathways between humans and rodents.
Induced pluripotent cell lines (iPSCs/piPSCs) Th e concept of reversing the programming of diff eren-tiated tissues to pluripotent states was introduced with the fi rst somatic cell nuclear transfer (SCNT) experi-ments by John Gurdon during the late 1950s, using Xenopus oocytes (Gurdon, 1962 ). Several decades later, the birth of “Dolly the Sheep” provided the fi rst con-fi rmation in mammals that a diff erentiated somatic cell could be converted to a totipotent state by inserting its nucleus into an enucleated oocyte.
Somatic cell nuclear transfer: cloning ( Figure 7.3 )
1. Therapeutic cloning : the nucleus of an adult som-atic (diff erentiated) cell is reprogrammed by inser-tion into an enucleated donor oocyte. The oocyte is then activated by electrofusion to stimulate cleav-age, grown in culture to the blastocyst stage, and the ICM of this blastocyst used for stem cell der-ivation. The resulting stem cell lines are immuno-logically identical (HLA-matched) to the somatic cell that was reprogrammed, and could theor-etically be used for potential therapies without transplant rejection. The technique has recently been successful in nonhuman primates (rhesus macaque), although with very low effi ciency: two primate ESC lines were derived from the use of 304 oocytes (Byrne et al ., 2007 ). A report that several patient-specifi c stem cell lines had been estab-lished in Korea subsequently proved to be based on data that was fabricated, and the papers were withdrawn (Hwang et al ., 2004 , 2005 ). In view of the extreme diffi culty in obtaining donor oocytes, and the ineffi ciency of the technique so far, it may be that pursuing research with iPS cells is a better strategy than therapeutic cloning.
2. Reproductive cloning : SCNT is carried out as for therapeutic cloning, but the resulting embryo is transferred to the uterus. Dolly , the
1. Therapeutic cloning : the nucleus of an adult som-atic (diff erentiated) cell is reprogrammed by inser-tion into an enucleated donor oocyte. The oocyte is then activated by electrofusion to stimulate cleav-age, grown in culture to the blastocyst stage, andthe ICM of this blastocyst used for stem cell der-ivation. The resulting stem cell lines are immuno-logically identical (HLA-matched) to the somaticcell that was reprogrammed, and could theor-etically be used for potential therapies withouttransplant rejection. The technique has recentlybeen successful in nonhuman primates (rhesusmacaque), although with very low effi ciency: twoprimate ESC lines were derived from the use of 304oocytes (Byrne et al ., 2007 ). A report that severallpatient-specifi c stem cell lines had been estab-lished in Korea subsequently proved to be basedon data that was fabricated, and the papers werewithdrawn (Hwang et al ., 2004 , 2005 ). In view of lthe extreme diffi culty in obtaining donor oocytes,and the ineffi ciency of the technique so far, it maybe that pursuing research with iPS cells is a betterstrategy than therapeutic cloning.
2. Reproductive cloning : SCNT is carried outas for therapeutic cloning, but the resultingembryo is transferred to the uterus. Dolly , the

Chapter 7: Stem cell biology
100
much-celebrated sheep, was the fi rst example of successful mammalian reproductive cloning, dem-onstrating that a diff erentiated adult cell could be reprogrammed to generate an entire organism (Wilmut et al ., 1997 ). This success confi rmed John Gurdon’s remarkable discoveries during the 1950s, when he was able to produce tadpoles after som-atic cell nuclear transfer into Xenopus laevis eggs (Gurdon, 1962 ). The technique has been used in a variety of large and small animals, including cows, goats, mice, pigs, cats, rabbits and a gaur. However, reproductive cloning is both expensive and highly ineffi cient – more than 90% of cloning attempts fail, and imprinting defects have been identifi ed in cloned animals, with abnormalities of immune function, growth and numerous other disor-ders. Experiments with cloned mice indicate that approximately 4% of their genes function abnor-mally, due to imprinting defects.
With accumulated information regarding pluripo-tency in ESC, pinpointing key genes that might be used to reprogram somatic cells became a major research goal. Panels of genes that are enriched in ESC popu-lations, and thought to be involved in maintenance of pluripotency were screened, with the target of
identifying factors that have the ability to re-program somatic mouse cells into proliferation. From a panel of 24 target genes, four factors were found that together induced a transformation of mouse fi broblasts into cells that closely resemble mouse ES cells: OCT4, SOX2, c-Myc and Klf4 (Takahashi and Yamanaka, 2006 ). Th e experiments were conducted by using retroviruses to insert key pluripotency genes into the fi broblasts; the cells that resulted had properties analogous to ESCs in culture, and also formed teratomas when injected into mice. Th e same technique was subsequently applied to successfully reprogram human fi broblasts into hES-like cells (Takahashi et al ., 2007a ; Lowry et al ., 2008 ). A further independent study using human cells screened a panel of 14 genes that are enriched in hESCs, and succeeded in reprogramming human fi broblasts with the introduction of genes for OCT4, SOX2, NANOG and LIN28 (Yu et al ., 2007 ). Human iPS cells satisfy all the original criteria proposed for characterization of hESCs: morphology is similar, they express typical hESC surface antigens and genes, diff erentiate into multiple lineages in vitro, and when injected into SCID mice they form teratomas containing cells derived from all three primary germ layers. Since this initial report, numerous combinations of somatic cell type
much-celebrated sheep, was the fi rst example of successful mammalian reproductive cloning, dem-onstrating that a diff erentiated adult cell could bereprogrammed to generate an entire organism(Wilmut et al., 1997 ). This success confi rmed Johnl Gurdon’s remarkable discoveries during the 1950s,when he was able to produce tadpoles after som-atic cell nuclear transfer into Xenopus laevis eggs(Gurdon, 1962 ). The technique has been used in avariety of large and small animals, including cows,goats, mice, pigs, cats, rabbits and a gaur. However,reproductive cloning is both expensive and highlyineffi cient – more than 90% of cloning attemptsfail, and imprinting defects have been identifi edin cloned animals, with abnormalities of immunefunction, growth and numerous other disor-ders. Experiments with cloned mice indicate thatapproximately 4% of their genes function abnor-mally, due to imprinting defects.
Oocyte retrieval Donor cell isolation and culture
EnucleationMaturation Nuclear transfer
REPRODUCTIVECLONING
THERAPEUTICCLONING
Activation
Embryo cultureisolation of ICM andderivation of stem cell linesTransfer to uterus
Electrofusion
++++++++++++
+
+
++
+
Figure 7.3 Transfer of a diploid somatic cell nucleus into an enucleated metaphase II oocyte followed by activation by electrofusion leads to the creation of an embryo that has the chromosome complement of the somatic cell. A resulting blastocyst stage embryo can be transferred to a recipient uterus and allowed to develop to term into an animal with characteristics of the transferred somatic nucleus (reproductive clon-ing) or inner cell mass cells may be used to generate stem cell lines that are genetically matched to the donor of the somatic cell (therapeutic cloning).

Chapter 7: Stem cell biology
101
and cocktails of factors have been studied, and con-tinue to be investigated: some cell types can be repro-grammed more effi ciently than others, and diff erent types of cell respond to diff erent expression levels and combinations of factors. Th e number of factors investi-gated continues to grow, and the original four now only head a list of related proteins that seem to enhance the effi ciency of transformation in some cells (Heng et al ., 2010 ). Eff orts to elucidate the mechanisms by which such a limited number of transcription factors can erase and reprogram a diff erentiated state continue: the DNA binding sites of OCT4 , SOX2 and NANOG have been studied, and it seems that these three factors can also activate or repress the expression of many other genes, including transcription factors that are important dur-ing early stages of development (Boyer et al ., 2005 ).
Although iPSCs provide an excellent and powerful model for studying the fi ne details of cell biology and diff erentiation, the effi ciency of reprogramming adult cells is very low (0.1%), and their capacity for diff er-entiation is lower, and more variable than that of hESCs (Hua et al ., 2010 ). Selecting the appropriate type of cell, timing, balance of factors, identifying small molecules that might augment effi ciency, and the absolute levels of gene expression needed are all aspects that require further research. In terms of therapeutic potential, iPSCs have the major advantage that a patient’s own cells can be used for reprogramming, which overcomes the problem of immune matching. However, using viral (retrovirus, lentivirus, adenovirus) or plasmid vectors to introduce genetic material carries the considerable risk of causing genetic mutations at the insertion sites, and alternative methods of delivering the genes are under investigation, including transient transfection and using a “piggyBac” transposon that uses a host factor to carry the genes, and then allows the exogenous genes to be excised (see Müller et al ., 2009 and Shao and Wu, 2010 for reviews).
Factors used to induce pluripotency
OCT4 POU domain transcription factor . • Expression restricted to pluripotent cells of the • embryo. Expressed in undiff erentiated ES, EC and EG cells. • Essential for formation of the ICM. • In the absence of OCT4 , all cells in the embryo • become trophectoderm .
Deletion in ES cells causes diff erentiation into • trophectoderm Overexpression causes diff erentiation to endo-• derm/mesoderm
SOX2 High mobility group (HMG) box transcription factor. • Expressed in ICM and trophectoderm. • Required for development of the embryonic • lineage. Also required for proliferation of extraembryonic • ectoderm. Interacts specifi cally with OCT4 to infl uence expres-• sion of target genes. SOX2 controls OCT4 expression, and they per-• petuate their own expression when they are co-expressed.
c-Myc Transcription factor that activates expression of a • large number of genes through binding on enhan-cer box sequences (E-boxes). Has a direct role in DNA replication, can drive cell • proliferation by upregulating cyclins/downregulat-ing p21. Also has roles in cell growth, apoptosis , diff erenti-• ation, stem cell renewal. Proto-oncogene: upregulated in many types of • cancers.
Klf4: A member of the Krüppel-like family of tran-scription factors
Can act as a transcriptional activator or repressor, • depending on promoter context and interaction with other transcription factors.
NANOG Homeodomain transcription factor. • Expression is tightly associated with pluripotency. •
Essential for early development, and for • reprogramming. Required for development of the epiblast . •
LIN28: marker of undiff erentiated hESCs Encodes a cytoplasmic mRNA binding protein that • binds to and enhances the translation of IGF2 mRNA.
Protein-induced pluripotent stem cell lines (piPSCs) In further attempts to overcome the problem of viral vectors, modifi ed versions of the protein products themselves have also been used. Stable iPSCs from human fi broblasts were generated by using a cell-penetrating peptide (CPP) to deliver the four proteins OCT4 , SOX2, Klf4, c-Myc (Zhou et al ., 2009 ; Cho et al ., 2010 ). Th e cells produced by
OCT4 POU domain transcription factor . • Expression restricted to pluripotent cells of the •embryo. Expressed in undiff erentiated ES, EC and EG cells.• Essential for formation of the ICM.• In the absence of OCT4 , all cells in the embryo •become trophectoderm .
Deletion in ES cells causes diff erentiation into •trophectoderm Overexpression causes diff erentiation to endo-•derm/mesoderm
SOX2 High mobility group (HMG) box transcription factor.• Expressed in ICM and trophectoderm.• Required for development of the embryonic•lineage. Also required for proliferation of extraembryonic• ectoderm. Interacts specifi cally with OCT4 to infl uence expres-•sion of target genes. SOX2 controls OCT4 expression, and they per-• petuate their own expression when they areco-expressed.
c-Myc Transcription factor that activates expression of a•large number of genes through binding on enhan-cer box sequences (E-boxes). Has a direct role in DNA replication, can drive cell• proliferation by upregulating cyclins/downregulat-ing p21. Also has roles in cell growth, apoptosis , diff erenti-• ation, stem cell renewal. Proto-oncogene: upregulated in many types of •cancers.
Klf4: A member of the Krüppel-like family of tran-scription factors
Can act as a transcriptional activator or repressor,• depending on promoter context and interactionwith other transcription factors.
NANOG Homeodomain transcription factor.• Expression is tightly associated with pluripotency. •
Essential for early development, and for•reprogramming.Required for development of the epiblast .•
LIN28: marker of undiff erentiated hESCs Encodes a cytoplasmic mRNA binding protein that•binds to and enhances the translation of IGF2 mRNA.

Chapter 7: Stem cell biology
102
this DNA-vector free, direct protein transduction method have been called “protein-induced pluri-potent stem cells”, piPSC . Experiments have been carried out using recombinant proteins, as well as proteins derived from cell fractions. However, so far the generation of piPSC is very slow and ineffi cient; numerous variables involved in applying this tech-nology remain to be optimized.
hESC culture systems Th e fi rst human ESCs were derived using inacti-vated mouse fi broblasts as feeder layers. A great deal of research has been devoted to both improving the effi ciency of derivation/propagation, and towards establishing conditions that are free from xenobiotic hazard in cells, reagents and media supplements (animal cells always carry the risk of pathogen trans-mission or viral infection, and cells grown in the pres-ence of animal-derived products cannot be used for human therapies). Mouse fi broblast feeder layers can be replaced with human fi broblasts or feeder condi-tioned medium, substrates such as Matrigel and lam-inin have been used, and numerous experiments have been carried out using combinations of additional growth factors and cytokines. Basic fi broblast growth factor and members of the TGF-beta superfamily are important in regulating self-renewal, and it has become apparent that maintaining the undiff erenti-ated state involves extensive cross-talk between the intracellular signaling pathways activated by factors such as FGF, TGF-beta and BMP (Rao and Zandstra, 2005 ). In 2005 , Vallier et al . reported successful prolonged culture of hESCs in a chemically defi ned medium (CDM) containing activin A (INHBA)/nodal (NODAL) and FGF2; cells cultured in this medium maintained their fundamental characteris-tics of pluripotency. Other members of the TGF-beta superfamily (BMP11/GDF11 and myostatin/GDF8) have also been identifi ed that promote self-renewal in feeder-free and serum-free conditions (Hannan et al ., 2009 ). However, to date initial derivation of a stem cell line is still more effi cient with the support of a feeder layer.
Derivation and propagation of hESCs requires a signifi cant commitment of time and resources. Establishing a culture of hESCs takes from 3 to 6 weeks, and the cultures need daily attention once established. With the appropriate level of skill and attention, they can be kept in continuous culture for
years, with aliquots cryopreserved during subculture. It has become clear that there is probably no stand-ard culture method or medium that is optimal for all lines and all purposes (see under “Books” in Further reading).
Human ES cells have been derived not only from blastocyst ICM, but also from later stage blastocysts, morulae (Stojkovic et al ., 2004 ), single blastomeres (Klimanskaya et al ., 2007 ), and from parthenogen-etic embryos (Mai et al ., 2007 ; Revazova et al ., 2007 ). It is not yet known whether the pluripotent cell lines derived from these sources have any consistent devel-opmental diff erences, or whether they have an equiva-lent potential.
Derivation of research stem cell lines from blastocyst ICM ( Figures 7.4a and 7.4b )
Protocol based on Sullivan et al ., 2007 ; all animal-based products must be avoided if lines are being derived for potential therapeutic use.
1. Prepare feeder layers: seed mitotically inactivated fi broblast onto gelatinized four-well culture plates at a density of approximately 50 000 cells/cm 3 . Mouse embryonic fi broblasts (MEFs) are commonly used, inactivated either with mitomycin C or by gamma-irradiation (human fi broblast cells can also be used, isolated from a variety of sources including newborn foreskin, but for research purposes, deriv-ation on MEF has practical advantages and thus far appears to be more effi cient).
2. Remove/dissolve the zona pellucida : diff erent methods include the use of pronase, acid Tyrode’s solution, or allowing the blastocyst to hatch com-pletely in culture.
3. Remove the trophectoderm layer, by complement-mediated lysis (immunosurgery), or by manual dissection.
4. Plate the isolated ICM clump onto a well-developed, confl uent feeder layer, and incubate in human ES derivation medium, undisturbed, for 48 hours.
5. After several days, outgrowths of cells from the ICM will appear. hESCs grow in fl at two-dimensional clumps, and have prominent nucleoli; these can be isolated and subcultured into fresh culture dishes. The explants should not be allowed to become over-confl uent and crowd the dish, or they will begin to diff erentiate.
6. If the subcultured cells continue to proliferate without signs of diff erentiation, they are a “putative ES line,” and require extensive characterization to confi rm.
7. Batches of cells can be cryopreserved at intervals during subculture.
Protocol based on Sullivan et al ., 2007 ; all animal-basedlproducts must be avoided if lines are being derived forpotential therapeutic use.
1. Prepare feeder layers: seed mitotically inactivatedfi broblast onto gelatinized four-well culture platesat a density of approximately 50 000 cells/cm3 .Mouse embryonic fi broblasts (MEFs) are commonlyused, inactivated either with mitomycin C or bygamma-irradiation (human fi broblast cells can alsobe used, isolated from a variety of sources includingnewborn foreskin, but for research purposes, deriv-ation on MEF has practical advantages and thus farappears to be more effi cient).
2. Remove/dissolve the zona pellucida : diff erentmethods include the use of pronase, acid Tyrode’ssolution, or allowing the blastocyst to hatch com-pletely in culture.
3. Remove the trophectoderm layer, by complement-mediated lysis (immunosurgery), or by manualdissection.
4. Plate the isolated ICM clump onto a well-developed,confl uent feeder layer, and incubate in human ESderivation medium, undisturbed, for 48 hours.
5. After several days, outgrowths of cells from the ICMwill appear. hESCs grow in fl at two-dimensionalclumps, and have prominent nucleoli; these can beisolated and subcultured into fresh culture dishes.The explants should not be allowed to becomeover-confl uent and crowd the dish, or they willbegin to diff erentiate.
6. If the subcultured cells continue to proliferate withoutsigns of diff erentiation, they are a “putative ES line,” and require extensive characterization to confi rm.
7. Batches of cells can be cryopreserved at intervalsduring subculture.

Chapter 7: Stem cell biology
103
ZP
(a)
ICMTE
Remove ZP
Isolate ICM
Plate ICM onfeeder cells
Feeder cellsMechanical (laser) surgery
Immunosurgery
Observe for ESC outgrowth
Blastocyst
YY
YYY
YY
Y
YY Y
Y
(b)
Figure 7.4 (a) Cartoon outlining derivation of a stem cell line from a blastocyst inner cell mass (ICM) (with thanks to Alice Chen). ZP = zona pel-lucida; TE = trophectoderm; ESC = embryonic stem cell. (b) Phase contrast image of a human stem cell colony, on a background of inactivated mouse fi broblasts (with thanks to Dr. Kathy Niakon).
Characterization of ESC lines
1. The cells should have the ability to be propagated in long-term culture, without visible signs of transformation.
2. Cryopreserved aliquots of cells should maintain the ability to continue propagation after freeze-thawing.
3. Identify cell-surface markers characteristic of ESCs: the glycolipids SSEA3 and SSEA4, and keratan sulfate antigens Tra-1–60 and Tra-1–81.
4. Identify protein markers of pluripotency: Oct4, Nanog, Sox2.
1. The cells should have the ability to be propagated in long-term culture, without visible signs of transformation.
2. Cryopreserved aliquots of cells should maintain the ability to continue propagation after freeze-thawing.
3. Identify cell-surface markers characteristic of ESCs: the glycolipids SSEA3 and SSEA4, and keratan sulfate antigens Tra-1–60 and Tra-1–81.
4. Identify protein markers of pluripotency: Oct4, Nanog, Sox2.
5. Analyze chromosomal karyotype. 6. If feeder layers are removed, they should round up
and clump into embryoid bodies containing undir-ected diff erentiated cell types from the three germ layers.
7. Injection of the ESCs into an immunosuppressed (SCID) mouse should result in teratoma formation. More sophisticated molecular biology tools are now
being used in order to identify specifi c transcriptional profi les, combining immunotranscriptional and poly-some translation state analyses to identify a large num-ber of genes and cell surface markers (Kolle et al ., 2009 )
5. Analyze chromosomal karyotype. 6. If feeder layers are removed, they should round up
and clump into embryoid bodies containing undir-ected diff erentiated cell types from the three germlayers.
7. Injection of the ESCs into an immunosuppressed(SCID) mouse should result in teratoma formation. More sophisticated molecular biology tools are now
being used in order to identify specifi c transcriptionalprofi les, combining immunotranscriptional and poly-some translation state analyses to identify a large num-ber of genes and cell surface markers (Kolle et al ., 2009 ) l

Chapter 7: Stem cell biology
104
Problems with established human ESCs
• Tendency to become aneuploid after extended passaging . Do not like to grow as single cells, making genetic • modifi cation (targeting) diffi cult. Diffi cult to drive along specifi c diff erentiation • pathways.
ESC markers of pluripotency A recent report (Hough et al ., 2009 ) suggests that “pluripotency” in hESCs may not be an all-or-noth-ing state: hESC cultures are in fact heterogeneous. Analyzing transcripts of single hESCs for lineage-specifi c transcription factors revealed that there is a gradient and a hierarchy of pluripotency gene expres-sion , with many cells co-expressing both pluripotency and lineage specifi c genes. Th ese authors suggest that only a small fraction of the hESC culture population lies at the top of the developmental hierarchy, and that pluripotent stem cell populations may simultaneously express both stem cell and lineage specifi c genes. Transcription factor networks that control pluripo-tency are dependent on upstream extrinsic signaling pathways, and cells along the continuum of diff eren-tiation show a progressively decreasing potential for self-renewal, with decreased expression of stem cell surface markers and pluripotency genes. Th e spatial organization of hESC cultures also infl uences the fate of individual cells, and engineering the microenvir-onment (niche) can be used to direct the rate and direction of diff erentiation by regulating the balance between inducing and inhibiting factors in the signal-ing pathways (Peerani et al ., 2007 ).
Stem cell banking and registries Several hundred human embryonic stem cell lines have now been established in countries through-out the world, including several lines carrying gene defects for inherited genetic disease, derived from embryos identifi ed as abnormal in PGD cycles. Research is accelerating via new and sophisticated molecular biology tools for gene sequencing, micro-arrays to map gene expression in single cells, cytokine and cDNA libraries, etc.
Th is fast-moving and multidisciplinary research is of critical importance to medical science, and there is a crucial need for collaboration and free exchange of
information. Initiatives to facilitate collaboration and establish bench marks and good practice models have been set up (see Andrews et al ., 2005 ; Franklin et al ., 2008 ), and stem cell registries have been developed in order to collect, organize and disseminate infor-mation about specifi c cell lines (see Borstlap et al ., 2010 for review of stem cell registries). In May 2004, the world’s fi rst Stem Cell Bank was opened in the UK ( www.ukstemcellbank.org.uk/ ), established in order to provide a repository for human stem cell lines of all types, and to supply well-characterized cell lines for use in basic research. Th e Bank has a catalogue of characterized stem cell lines that have been depos-ited by research groups in several diff erent countries, and details of lines that are being characterized, or are due for release can also be found on their website. Applications to access the Bank’s stem cell lines must be fi rst approved by a UK Medical Research Council (MRC) Stem Cell Steering Committee who will review the research proposal, and the credentials of the research team
In March 2009, in response to a new Executive Order from President Obama, the National Institutes of Health (NIH) in the USA published a registry of cell lines, and guidelines to establish policy and procedures for NIH-funded stem cell research: http://stemcells.nih.gov/research/registry/ ; http://stemcells.nih.gov/policy/2009guidelines.htm .
Stem cell biology is now arguably the most powerful tool available for the advancement of med-ical science. Th e possibility of studying cell-fate transitions, controlling proliferation and directing diff erentiation by manipulating core sets of tran-scription factors adds a new dimension to the fi elds of regenerative medicine, degenerative disease, and the uncontrolled proliferation of cancerous disease. Culture systems and selected populations of stem cells can be used to screen drugs and new approaches to treatment. Understanding the regulation of self-renewal at the molecular level will lead to improved systems for hESC derivation and propagation, and also has the potential to yield further insight into aspects of development that might increase the effi -ciency of clinical IVF. Human embryonic stem cells undergoing diff erentiation in culture also give us information about a period that has not previously been accessible for research, the fi rst stages of early postimplantation human development that are described in Chapter 6 .
• Tendency to become aneuploid after extendedpassaging . Do not like to grow as single cells, making genetic•modifi cation (targeting) diffi cult. Diffi cult to drive along specifi c diff erentiation•pathways.

Chapter 7: Stem cell biology
105
Further reading Website information www.hta.gov.uk/ www.regenmd.com/research_links.htm www.regenmd.com/index.htm http://stemcells.nih.gov/info/faqs.asp http://isscr.org/science/faq.htm www.news.wisc.edu/packages/stemcells/illustration.html www.news.wisc.edu/packages/stemcells/ www.mrc.ac.uk/index/public-interest/public-topical_
issues/public-stem_cells.htm#furtherinfo
Books Freshney RI , Stacey GN , Auerbach JA ( 2007 ) Culture of
Human Stem Cells. Wiley-Liss , Chichester, UK . Sell , S (Ed.) ( 2004 ) Stem Cells Handbook . Humana Press ,
New York . Simon C , Pellicer A ( 2009 ) Stem Cells in Human
Reproduction: Basic Science and Th erapeutic Potential . Informa Healthcare , London .
Sullivan S , Cowan CA , Eggan K ( 2007 ) Human Embryonic Stem Cells: Th e Practical Handbook . Wiley , Chichester .
Publications Andrews PW ( 2002 ) From teratocarcinomas to embryonic
stem cells . Philosophical Transactions of the Royal Society of London, Series B 357 : 405 –417.
Andrews PW , Banting G , Damjanov I , Arnaud D , Avner P ( 1984a ) Th ree monoclonal antibodies defi ning distinct diff erentiation antigens associated with diff erent high molecular weight polypeptides on the surface of human embryonal carcinoma cells . Hybridoma 3 : 347 –361
Andrews PW , Benvenisty N , McKay R , et al. ( 2005 ) Th e International Stem Cell Initiative: toward benchmarks for human embryonic stem cell research . Nature Biotechnology 23 (7): 795 –797.
Andrews PW , Damjanov I , Simon D , et al. ( 1984b ) Pluripotent embryonal carcinoma clones derived from the human teratocarcinoma cell line Tera-2 . Laboratory Investigation 50 : 147 –162.
Andrews PW , Goodfellow PN , Shevinsky LH , Bronson DL , Knowles BB ( 1982 ) Cell-surface antigens of a clonal human embryonal carcinoma cell line: Morphological and antigenic diff erentiation in culture . International Journal of Cancer 29 : 523 –531.
Avilion AA , Nicolis SK , Pevny LH , et al. ( 2003 ) Multipotent cell lineages in early mouse development depend on SOX2 function . Genes and Development 17 : 126 –140.
Bao S , Tang F , Li X , et al. ( 2009 ) Epigenetic reversion of post-implantation epiblast to pluripotent embryonic stem cells . Nature 461 : 1292 –1295.
Beattie GM , Lopez AD , Bucay N , et al. ( 2005 ) Activin A maintains pluripotency of human embryonic stem cells in the absence of feeder layers . Stem Cells 23 : 489 –495.
Bendall SC , Stewart MH , Menendez P , et al . ( 2007 ) IGF and FGF cooperatively establish the regulatory stem cell niche of pluripotent human cells in vitro . Nature 448 : 1015 –1021.
Bongso A , Fong CY , Ng SC , Ratnam S ( 1994 ) Isolation and culture of inner cell mass cells from human blastocysts . Human Reproduction 9 : 2110 –2117.
Borstlap J , Luong MX , Rooke HM , et al. ( 2010 ) International stem cell registries . In Vitro Cellular and Developmental Biology. Animal 46 (3–4): 242 –246.
Boyer LA , Lee TI , Cole MF , et al. ( 2005 ) Core transcriptional regulatory circuitry in human embryonic stem cells . Cell 122 (6): 947 –956.
Bradley A , Evans M , Kaufman MH , Robertson E ( 1984 ) Formation of germ-line chimaeras from embryo-derive teratocarcinoma cell lines . Nature 309 : 255 –256.
Brandenberger R , Wei H , Zhang S , et al . ( 2004 ) Transcriptome characterization elucidates signaling networks that control human ES cell growth and diff erentiation . Nature Biotechnology 22 : 707 –716.
Brons IG , Smithers LE , Trotter MW , et al. ( 2007 ) Derivation of pluripotent epiblast stem cells from mammalian embryos . Nature 12 ;448(7150): 191 –195
Byrne JA ( 2008 ) Generation of isogenic pluripotent stem cells . Human Molecular Genetics 17 (R1): R37 –41.
Byrne JA , Pedersen DA , Clepper LL , et al. ( 2007 ) Producing primate embryonic stem cells by somatic cell nuclear transfer . Nature 450 (7169): 497 –502.
Chambers I , Silva J , Colby D , et al. ( 2007 ) Nanog safeguards pluripotency and mediates germline development . Nature 450 : 1230 –1234.
Cho JH , Lee C-S , Kwon Y-W , et al. ( 2010 ) Induction of pluripotent stem cells from adult somatic cells by protein-based reprogramming without genetic manipulation. Blood First Edition Paper, e-pub ahead of print May 2010.
Cole RJ , Edwards RG , Paul J ( 1965 ) Cytodiff erentiation in cell colonies and cell strains derived from cleaving ova and blastocysts of the rabbit . Experimental Cell Research 37 : 501 –504.
Cole RJ , Edwards RG , Paul J ( 1966 ) Cytodiff erentiation and embryogenesis in cell colonies and tissue cultures derived from ova and blastocysts of the rabbit . Developmental Biology 13 : 285 –307.
Dahéron L , Opitz SL , Zaehres H , et al. ( 2004 ) LIF/STAT3 signalling fails to maintain self-renewal of human embryonic stem cells . Stem Cells 22 (5): 770 –778.

Chapter 7: Stem cell biology
106
Davis RP , Costa M , Grandela C , et al. ( 2008a ) A protocol for removal of antibiotic resistance cassettes from human embryonic stem cells genetically modifi ed by homologous recombination or transgenesis . Nature Protocols 3 : 1550 –1558.
Davis RP , Ng ES , Costa M , et al. ( 2008b ) Targeting a GFP reporter gene to the MIXL1 locus of human embryonic stem cells identifi es human primitive streak-like cells and enables isolation of primitive hematopoietic precursors . Blood 111 : 1876 –1884.
Dietrich JE , Hiragi T ( 2007 ) Stochastic patterning in the mouse pre-implantation embryo . Development 134 (23): 4219 –4231.
Edwards RG ( 2004 ) Stem cells today . Reproductive Biomedicine Online 8 (3): 275 –306.
Edwards RG ( 2008 ) From embryonic stem cells to blastema and MRL mice . Reproductive Biomedicine Online 16 (3): 425 –461.
Evans M , Kaufman MH ( 1981 ) Establishment in culture of stem cells from mouse embryos Nature 292 : 154 –156.
Fishel S , Edwards RG , Evans CJ ( 1984 ) Human chorionic gonadotrophin secreted by preimplantation embryos . Science 223 : 816 –818.
Franklin SB , Hunt C , Cornwell G , et al. ( 2008 ) hESCCO: development of good practice models for hES cell derivation . Regenerative Medicine 3 (1): 105 –116.
Gardner Rl ( 1968 ) Mouse chimaeras obtained by the injection of cells into the blastocyst . Nature 220 : 596 –597.
Guo G , Yang J , Nichols J , et al. ( 2009 ) Klf4 reverts developmentally programmed restriction of ground state pluripotency . Development 136 (7): 1063 –1069.
Gurdon JB ( 1962 ) Th e developmental capacity of nuclei taken from intestinal epithelial cells of feeding tadpoles . Journal of Embryology and Experimental Morphology 10 : 622 –640.
Gurdon JB ( 1968 ) Transplanted nuclei and cell diff erentiation . Scientifi c American 219 (6): 24 –35.
Gurdon JB , Byrne JA ( 2003 ) Th e fi rst half-century of nuclear transplantation . Proceedings of the National Academy of Sciences of the USA 100 (14): 8048 –8052
Gurdon JB , Colman A ( 1999 ) Th e future of cloning . Nature 402 : 743 –746.
Hannan NR , Jamshidi P , Pera MF , Wolvetang EJ ( 2009 ) BMP-11 and myostatin support undiff erentiated growth of human embryonic stem cells in feeder-free cultures . Cloning Stem Cells ( 3 ): 427 –435.
Hatzistavrou T , Micallef SJ , Ng ES , et al. ( 2009 ) ErythRED, a hESC line enabling identifi cation of erythroid cells . Nature Methods 6 (9): 659 –662.
Heng BC , Richards M , Ge Z , SHu Y ( 2010 ) Induced adult stem (iAS) cells and induced transit amplifying progenitor (iTAP) cells – a possible alternative to
induced pluripotent stem (iPS) cells? Journal of Tissue Engineering and Regenerative Medicine 4 (2): 159 –162.
Hogan B , Fellows M , Avner P , Jacob F ( 1977 ) Isolation of a human teratoma cell line which expresses F9 antigen . Nature 270 : 515 –518.
Hough SR , Laslett AL , Grimmond SB , Kolle G , Pera MF ( 2009 ) A continuum of cell states spans pluripotency and lineage commitment in human embryonic stem cells . PLoS One 4 (11): e7708 .
Hua B-Y , Weicka JP , Yub J , et al. ( 2010 ) Neural diff erentiation of human induced pluripotent stem cells follows developmental principles but with variable potency . Proceedings of the National Academy of Sciences of the USA 107 (9): 4335 –4340
Humphrey RK , Beattie GM , Lopez AD , et al. ( 2004 ) Stem Cells 22 (4): 522 –530.
Hwang W-S , Roh SI , Lee BC , et al . ( 2005 ) Patient-specifi c embryonic stem cells derived from human SCNT blastocysts . Science 308 : 1777 –1783.
Hwang W-S , Ryu YJ , Park JH , et al . ( 2004 ) Evidence of a pluripotent human embryonic stem cell line derived from a cloned blastocyst . Science 303 : 1669 –1674.
Illmensee K ( 2002 ) Biotechnology in reproductive medicine . Diff erentiation 69 (4–5): 167 –173.
Kahn BW , Ephrussi B ( 1970 ) Developmental potentialities of clonal in vitro cultures of mouse testicular teratoma . Journal of the National Cancer Institute 44 : 1015 –1029.
Kaji K , Norrby K , Paca A , et al. ( 2009 ) Virus-free induction of pluripotency and subsequent excision of reprogramming factors . Nature 458 (7239): 771 –775.
Klimanskaya I , Chung Y , Becker S , Lu SJ , Lanza R ( 2007 ) Derivation of human embryonic stem cells from single blastomeres . Nature Protocols 2 (8): 1964 –1972.
Kolle G , Ho SHM , Zhou Q , et al. ( 2009 ) Identifi cation of human embryonic stem cell surface markers by combined membrane-polysome translation state array analysis and immunotranscriptional profi ling . Stem Cells 27 (10): 2446 –2456.
Laslett AL , Fryga A , Pera MF ( 2007a ) Flow cytometric analysis of human embryonic stem cells. In: Loring JF (ed.) Human Stem Cell Manual: A Laboratory Guide . Elsevier , pp. 96–107.
Laslett AL , Grimmond S , Gardiner B , et al. ( 2007b ) Transcriptional analysis of early lineage commitment in human embryonic stem cells . BMC Developmental Biology 7 : 12 .
Laslett AL , Lin A , Pera MF ( 2007c ) Characterization and diff erentiation of human embryonic stem cells. In: Masters JR , et al . (eds.) Embryonic Stem Cells . Springer , pp. 27–40.
Lowry WE , Richter L , Yachecko R , et al. ( 2008 ) Generation of human induced pluripotent stem cells from dermal

Chapter 7: Stem cell biology
107
fi broblasts . Proceedings of the National Academy of Sciences of the USA 105 (8): 2883 –2888.
Mai Q , Yu Y , Li T , et al. ( 2007 ) Derivation of human embryonic stem cell lines from parthenogenetic blastocysts . Cell Research 17 (12): 1008 –1019.
Martin GR ( 1981 ) Isolation of a pluripotent cell line from early mouse embryos cultured in medium conditioned by teratocarcinoma stem cells . Proceedings of the National Academy of Sciences of the USA 78 : 7634 –7638.
Matsui Y , Zsebo K , Hogan BL ( 1992 ) Derivation of pluripotential embryonic stem cells from murine primordial germ cells in culture . Cell 70 : 841 –847.
Müller LU , Daley GQ , Williams DA .( 2009 ) Upping the ante: recent advances in direct reprogramming . Molecular Th erapy 17 (6): 947 –953.
Mullor JL , Sánchez P , Altaba AR ( 2003 ) Pathways and consequences: Hedgehog signaling in human disease . Trends in Cell Biology 12 (12): 562 –569.
Mummery C , Ward D , van den Brink CE , et al . ( 2002 ) Cardiomyocyte diff erentiation of mouse and human embryonic stem cells . Journal of Anatomy 200 : 233 –242.
Ng ES , Davis R , Stanley EG and Elefanty AG ( 2008 ) A protocol describing the use of a recombinant protein-based, animal product free medium (APEL) for human embryonic stem cell diff erentiation as spin embryoid bodies . Nature Protocols 3 : 768 –776.
Nichols J , Smith A ( 2009 ) Naive and primed pluripotent states . Cell Stem Cell 4 : 487 –492.
Nichols J , Zevnik B , Anastassiadis K , et al. ( 1998 ) Formation of pluripotent stem cells in the mammalian embryo depends on the POU transcription factor Oct-4 . Cell 95 : 379 –391.
Niwa H , Miyazaki J , Smith AG ( 2000 ) Quantitative expression of Oct-3/4 defi nes diff erentiation, dediff erentiation or self-renewal of ES cells . Nature Genetics 24 : 372 –376.
Pedersen R ( 2005 ) Developments in human embryonic stem cells . Reproductive BioMedicine Online 10 (Suppl. 1): 60 –62.
Peerani R , Rao BM , Bauwens C , et al. ( 2007 ) Niche-mediated control of human embryonic stem cell self-renewal and diff erentiation . EMBO Journal 26 (22): 4744 –4755.
Pera MF , Cooper S , Mills J , Parrington JM ( 1989 ) Isolation and characterization of a multipotent clone of human embryonal carcinoma-cells . Diff erentiation 42 : 10 –23.
Pierce GB ( 1974 ) Neoplasms, diff erentiations and mutations . American Journal of Pathology 77 (1): 103 –118.
Rao BM , Zandstra PW ( 2005 ) Culture development for human embryonic stem cell propagation: molecular aspects and challenges . Current Opinion in Biotechnology 16 (5): 568 –576.
Resnick JL , Bixler LS , Cheng L , Donovan PJ ( 1992 ) Long-term proliferation of mouse primordial germ cells in culture . Nature 359 : 550 –551.
Reubinoff BE , Pera MF , Fong C-Y , Trounson A , Bongso A ( 2000 ) Embryonic stem cell lines from human blastocysts: somatic diff erentiation in vitro . Nature Biotechnology 18 : 299 –404.
Revazova ES , Turovets NA , Kochetkova OD , et al. ( 2007 ) Patient-specifi c stem cell lines derived from human parthenogenetic blastocysts . Cloning Stem Cells 9 (3): 432 –449.
Seifi nejad A , Tabebordbar M , Baharvand H , Boyer LA , Hosseini Salekdeh G ( 2010 ) Progress and promise towards safe induced pluripotent stem cells for therapy. Stem Cell Review Feb 24 [e-pub ahead of print].
Sermon CKD , Simon C , Braude P , et al. ( 2009 ) Creation of a registry for human embryonic stem cells carrying an inherited defect: joint collaboration between ESHRE and hESCreg . Human Reproduction 24 (7): 1556 –1560.
Shao L , Wu WS ( 2010 ) Gene-delivery systems for iPS cell generation . Expert Opinion on Biological Th erapy 10 (2): 231 –242.
Silva J , Nichols J , Th eunissen TW , et al. ( 2009 ) Nanog is the gateway to the pluripotent ground state . Cell 138 : 722 –737.
Smith AG , Heath JK , Donaldson DD , et al. ( 1988 ) Inhibition of pluripotential embryonic stem cell diff erentiation by purifi ed polypeptides . Nature 336 (6200): 688 –690.
Stevens LC ( 1967 ) Origin of testicular teratomas from primordial germ cells in mice . Journal of the National Cancer Institute 38 (4): 549 –552.
Stevens LC ( 1970 ) Th e development of transplantable teratocarcinomas from intratesticular graft s of pre- and postimplantation mouse embryos . Developmental Biology 21 : 364 –382.
Stojkovic M , Lako M , Stojkovic P , et al . ( 2004 ) Derivation of human embryonic stem cells from day-8 blastocysts recovered aft er three-step in vitro culture . Stem Cells 22 : 790 –797.
Strelchenko N , Verlinsky O , Kukharenko V , Verlinsky Y ( 2004 ) Morula-derived human embryonic stem cells . Reproductive Biomedicine Online 9 : 623 –629.
Takahashi K , Okita K , Nakagawa M , Yamanaka S ( 2007a ) Induction of pluripotent stem cells from fi broblast cultures . Nature Protocols 2 (12): 3081 –3089.
Takahashi K , Tanabe K , Ohnuki M , et al. ( 2007b ) Induction of pluripotent stem cells from adult human fi broblasts by defi ned factors . Cell 131 (5): 861 –872.
Takahashi K , Yamanaka S ( 2006 ) Induction of pluripotent stem cells from mouse embryonic and adult fi broblast cultures by defi ned factors . Cell 126 (4): 663 –676.
Tesar PJ , Chenoweth JG , Brook FA , et al. ( 2007 ) New cell lines from mouse epiblast share defi ning features with

Chapter 7: Stem cell biology
108
human embryonic stem cells . Nature 448 : 196 –199.
Th omson JA , Itskovitz-Eldor J , Shapiro SS , et al. ( 1998 ) Embryonic stem cell lines derived from human blastocysts . Science 282 : 1145 –1147.
Th omson JA , Kalishman J , Golos TG , et al. ( 1995 ) Isolation of a primate embryonic stem cell line . Proceedings of the National Academy of Sciences of the USA 92 : 7844 –7848.
Th omson JA , Kalishman J , Golos TG , et al. ( 1996 ) Pluripotent cell lines derived from common marmoset ( Callithrix jacchus ) blastocysts . Biology of Reproduction 55 : 688 –690.
Th ompson S , Stern PL , Webb M , et al. ( 1984 ) Cloned human teratoma cells diff erentiate into neuron-like cells and other cell types in retinoic acid . Journal of Cell Science 72 : 37 –64.
Trounson A ( 2002 ) Human embryonic stem cells: mother of all cell and tissue types Proceedings of Serono Symposia International Conference: “Robert G Edwards at 75” . Reproductive Biomedicine Online 4 (Suppl. 1): 58 –63.
Vallier L , Alexander M , Pedersen RA ( 2005 ) Activin/Nodal and FGF pathways cooperate to maintain pluripotency of human embryonic stem cells . Journal of Cell Science 118 : 4495 –4509.
Williams RL , Hilton DJ , Pease S , et al. ( 1988 ) Myeloid leukaemia inhibitory factor maintains the developmental potential of embryonic stem cells . Nature 336 (6200): 684 –687.
Wilmut I , Schnieke AE , McWhir J , Kind AJ , Campbell KH ( 1997 ) Viable off spring derived from fetal and adult mammalian cells . Nature 385 : 810 –813.
Wolf DP , Mitalipov S , Norgren RB Jr. ( 2001 ) Nuclear transfer technology in mammalian cloning . Archives of Medical Research 32 (6): 609 –613.
Woltjen K , Michael IP , Mohseni P , et al. ( 2009 ) piggyBac transposition reprograms fi broblasts to induced pluripotent stem cells . Nature 458 (7239): 766 –770.
Ying QL , Nichols J , Chambers I , Smith A ( 2003 ) BMP induction of Id proteins suppresses diff erentiation and sustains embryonic stem cell self-renewal in collaboration with STAT3 . Cell 115 (3): 281 –292.
Yu J , Vodyanik MA , Smuga-Otto K , et al. ( 2007 ) Induced pluripotent stem cell lines derived from human somatic cells . Science 318 (5858): 1917 –1920.
Zhou H , Ding S ( 2010 ) Evolution of induced pluripotent stem cell technology. Current Opinion in Hematology May 3 [e-pub ahead of print].
Zhou H , Wu S , Duan L , Ding S ( 2009 ) Generation of induced pluripotent stem cells using recombinant proteins . Cell Stem Cell 4 (5): 381 –384.

Chapter
109
The clinical in-vitro fertilization laboratory
Introduction In the armory of medical technology available for alleviation of disease and quality of life enhancement, there is nothing to match the unique contribution of assisted reproductive technology (ART). Th ere is no other life experience that matches the birth of a baby in signifi cance and importance. Th e responsibility of nurturing and watching children grow and develop alters the appreciation of life and health, with a result-ing long-term impact upon individuals, families and, ultimately, society. Th us, the combination of oocyte and sperm to create an embryo with the potential to develop into a unique individual cannot be regarded lightly, as merely another form of invasive medical technology, but must be treated with the respect and responsibility merited by the most fundamental areas of human life.
Successful assisted reproduction involves the care-ful coordination of both a medical and a scientifi c approach for each couple undertaking a treatment cycle, with close collaboration between doctors, sci-entists, nurses and counselors. Only meticulous atten-tion to detail at every step of each patient’s treatment can optimize their chance of delivering a healthy baby . Appropriate patient selection, ovarian stimulation, monitoring and timing of oocyte retrieval should pro-vide the in-vitro fertilization (IVF) laboratory with viable gametes capable of producing healthy embryos. It is the responsibility of the IVF laboratory to ensure a stable, nontoxic, pathogen-free environment with opti-mum parameters for oocyte fertilization and embryo development. Th e fi rst part of this book reveals the complexity of variables involved in assuring successful fertilization and embryo development, together with the fascinating and elegant systems of control that have been elucidated at the molecular level. It is essential for
the clinical biologist to be aware that the control mecha-nisms involved in human IVF are complex, and exquis-itely sensitive to even apparently minor changes in the environment of gametes and embryos. Temperature and pH are of crucial importance, and many other fac-tors can potentially aff ect cells at the molecular level. Multiple variables are involved, and the basic science of each step must be carefully controlled, while allowing for individual variation between patients and between treatment cycles. In addition, as technology continues to evolve, the success of new innovations in technique and technology can only be gauged by comparison with a standard of effi cient and reproducible established procedures. Th e IVF laboratory therefore, has a duty and responsibility to ensure that all of the components and elements involved are strictly controlled and regu-lated via an eff ective system of quality management (as outlined in Chapter 9 ).
The assisted conception treatment cycle
• Consultation: history, examination, investigations, counseling, consent(s) Drug scheduling regimen: GnRH agonist pituitary • downregulation or oral contraceptive pill to sched-ule withdrawal bleed Baseline assessment at start of treatment cycle • Gonadotropin stimulation • Follicular phase monitoring, ultrasound/endo-• crinology Induction of ovulation • Oocyte retrieval (OCR) • In-vitro fertilization/ICSI • Embryo transfer • Supernumerary embryo cryopreservation • Luteal phase support • Day 15–18 pregnancy test • Ultrasound assessment to confi rm gestational sac/• fetal heartbeat
• Consultation: history, examination, investigations,counseling, consent(s) Drug scheduling regimen: GnRH agonist pituitary• downregulation or oral contraceptive pill to sched-ule withdrawal bleed Baseline assessment at start of treatment cycle • Gonadotropin stimulation • Follicular phase monitoring, ultrasound/endo-• crinology Induction of ovulation• Oocyte retrieval (OCR)• In-vitro fertilization/ICSI • Embryo transfer • Supernumerary embryo cryopreservation• Luteal phase support• Day 15–18 pregnancy test • Ultrasound assessment to confi rm gestational sac/• fetal heartbeat
8
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 8: The clinical in-vitro fertilization laboratory
110
Setting up a laboratory: design, equipment and facilities Th e design of an IVF laboratory should provide a dis-traction- and risk-free environment in which uninter-rupted concentrated attention can be comfortably and safely dedicated to each manipulation, with sensible and logical planning of workstations that are practical and easy to clean. Priority must be given to minimizing the potential for introducing infection or contamin-ation from any source, and therefore the tissue culture area must provide aseptic facilities for safe manipula-tion of gametes and embryos, allowing for the high-est standards of sterile technique; fl oors, surfaces and components must be easy to clean on a daily basis. Th e space should be designated as a restricted access area, with facilities for changing into clean operating theater dress and shoes before entry.
Laboratory space layout Th e range of treatment types to be off ered, the number of cycles per year, and the manner in which the cycles will be managed all dictate the appropriate layout design and the equipment and supplies required. Four separate areas of work should be equipped according to need, arranged and set up to accommodate the fl ow of work according to the sequence of procedures in an IVF cycle: 1. Andrology : semen assessment and sperm
preparation; surgical sperm retrieval 2. Embryology : oocyte retrieval, fertilization,
embryo culture and transfer 3. Cryopreservation : sperm, oocytes, embryos,
ovarian and testicular tissue 4. Micromanipulation : ICSI, assisted hatching ,
embryo and polar body biopsy.
Careful consideration should be given to the phys-ical maneuvers involved, ensuring ease and safety of movement between areas to minimize the possibility of accidents. Bench height, adjustable chairs, microscope eye height and effi cient use of space and surfaces all con-tribute to a working environment that minimizes dis-traction and fatigue. Th e location of storage areas and equipment such as incubators and centrifuges should be logically planned for effi ciency and safety within each working area; the use of mobile laboratory compo-nents allows fl exibility to meet changing requirements. Many IVF laboratories are now designed with curved
joins between walls, fl oors and ceilings to ensure that no dust settles. For optimal cleanliness on reaching the entrance of the laboratory, two-stage entrance/exits can be incorporated into the changing room areas, so that outdoor clothing is removed at the external section, and scrubs/protective clothing donned at the second stage. Hand washing facilities must be available in the chan-ging area; sinks should be avoided in culture area, as they can act as a source of microbial contamination.
Light exposure during ART procedures In the course of normal physiology, gametes and embryos exist in a dark environment, and therefore exposure to light is not a “natural” situation. Th e poten-tial of introducing metabolic stress through light expos-ure was taken into consideration during the fi rst trials of human IVF in Oldham and Cambridge: dissecting microscopes were fi tted with green fi lters, background lighting in the laboratory was kept low, and during the time of the embryo transfer procedure the lights were extinguished in the operating theater until the embryo transfer catheter had been safely handed over to the physician. Increasingly sophisticated technology in IVF has added the use of more powerful microscopy, with high-intensity light sources. Some spectra of light are known to be associated with generation of reactive oxygen species (ROS), and further data has accumu-lated about the harmful eff ects of ROS in IVF. Th ree groups have recently examined various aspects and eff ects of light exposure in IVF procedures (Takenaka et al ., 2007 ; Ottosen et al ., 2007 ; Korhonen et al ., 2009 ). Th ese three studies concluded that certain wavelengths of light are potentially harmful in ART, and the extent of the damage is related to the duration of expos-ure, wavelength and intensity. Wavelengths <300 nm UV are absorbed by plastic; near UV-wavelengths of 300–400 nm are associated with increased apoptosis in mouse blastocysts. Ottosen et al . ( 2007 ) confi rmed that 95% of the radiation exposure was from microscopes, and recommended the use of green fi lters. Th ey sug-gest that ambient light was not a signifi cant hazard, but Takenaka et al . ( 2007 ) found that cool fl uorescent light, as commonly used in laboratories, produces a higher level of ROS and apoptosis in mouse and hamster zygotes than does warm fl uorescent light or sunlight.
Laboratory equipment Equipment should be selected based on its suitability for the intended purpose, capacity for the intended

Chapter 8: The clinical in-vitro fertilization laboratory
111
workload, ease of use and maintenance, availability of service and repair contracts to quality standards, and validation of evidence regarding its correct function. All equipment used in clinical treatments must be of highest standard available, validated for the intended use, safety checked and properly calibrated, regularly cleaned and maintained. Temperature and gas levels must be strictly monitored and recorded.
Service contracts should be set up with reliable companies, who must provide calibration certifi cates for the machines used to service and calibrate equip-ment in the IVF laboratory. Provision must be made for emergency call-out, with alarms fi tted to all vital equipment and back-up machines held in reserve. Essential equipment that require contracts for service and calibration include :
Incubators • Air fi ltration equipment • Flow cabinets • Microscopes • Heated surfaces/microscope stages • ICSI/Micromanipulation workstation • Centrifuges • Refrigerators and freezers • Embryo/oocyte freezing machines • Osmometers • Liquid nitrogen storage dewars • Electronic witnessing system • Ultrapure water system. •
A camera and monitor system that can display and record images is also recommended as part of the basic laboratory set-up, for teaching, assessment and record keeping .
Incubators Carefully calibrated and accurately controlled CO 2 incubators are critical to successful IVF. Th e choice of a humidifi ed or nonhumidifi ed incubator depends upon the type of tissue culture system used: whereas humid-ity is required for standard four-well “open” culture, the use of an equilibrated humidifi ed overlay of clinical grade mineral oil allows the use of incubators without humidity. Dry incubators carry less risk of fungal con-tamination, and are easier to clean .
Traditional stand-alone incubators can accom-modate culture dishes for many diff erent patients in a secure, well-insulated environment. Recent mod-els deliver a range of gas concentrations, with CO 2
concentrations of 5-6% and variable N 2 levels to reduce oxygen concentrations from ambient 21% to as low as 5% (Meintjes et al ., 2009 ). Th e larger models may incorporate a water-jacket in the door for additional insulation and can be run dry or at 95% relative humid-ity when water is added to the tray at the bottom of the chamber. Th e water-jacket not only helps to maintain a consistent temperature under normal circumstances, but also in the event of a power failure. Inner gas-tight split doors are essential in order to minimize recovery time aft er door opening, and CO 2 levels must be regu-larly (preferably continuously) monitored using an infrared CO 2 sensor. A single large incubator should not be used to house more than 12 cases at a time .
Smaller models such as the benchtop humidifi ed MINC (COOK IVF) or K-Systems G185 are portable and therefore more fl exible, with pre-mixed gas and sealed gas-tight chambers so that the dishes for each patient can be isolated. Th ese mini-incubators are less prone to variation in temperature and pH, exclude the use of laboratory air in the gas mix and do not need constant CO 2 calibration with external monitoring devices. However, it is extremely important to fi nd a reliable source for the gas mixture, both in the accuracy of the percentages of each gas and in their purity.
Large incubators can also be used to equilibrate tubes and bottles of media; this is not possible when only mini-incubators are used, so that HEPES-buff ered media might be required for the majority of prepara-tory procedures. Large incubators also have the advan-tage of allowing independent probes to be installed, with failure alarms that can operate remotely. Some also have fi tted HEPA-VOC fi lters .
Incubators must be regularly monitored, and read-ings of the LED display checked and calibrated against independent recordings of temperature and pH moni-tored by probes placed in a standard “test” culture system. Temperature stability can be monitored with 24-hour thermocouple readings as part of the standard main-tenance schedule. Th ere should be a schedule to ensure regular dismantling and cleaning, and a yearly inspection and general servicing by the supplier is recommended. Repeated opening and closing of the incubator aff ects the stability of the tissue culture environment, and the use of an accessory small benchtop mini-incubator dur-ing oocyte retrievals and manipulations helps to minim-ize disturbance of the larger incubators .
Irrespective of the type used, in all stand-alone incubators the dishes must be removed from the con-trolled environment for each stage of manipulation,

Chapter 8: The clinical in-vitro fertilization laboratory
112
exposing gametes or embryos to suboptimal temper-atures and changes in pH due to reduced CO 2 concen-tration. Th is has led to the introduction of integrated workstations that incorporate imaging systems and controlled atmosphere, providing a fully integrated incubator and fl ow cabinet in one system. Th ese inte-grated systems reduce the risks inherent in carrying dishes of oocytes or embryos around the laboratory for diff erent procedures. Custom-built isolator units are used in some laboratories, which can provide direct access from the fl ow cabinet to the incubator so that the culture dish never leaves the controlled environment. In the Ruskinn Ac-tive IVF System , the entire fl ow cabinet is environmentally controlled and acts as incubator and fl ow cabinet. Th ese inte-grated workstations are costly, and evidence of their validation in improving success rates is currently awaited.
Recent advances in incubator technology also incorporate a microscope and imaging system for con-tinuous monitoring of embryo development using time-lapse photography of individual embryos, for example:
EmbryoScope from Unisense FertiliTech A/S ( www.fertilitech.com/ ) InCu-View Live ( www.sanyo-biomedical.com ).
Electronic witnessing systems Systems are available that provide electronic identity checking/witnessing, using either barcode readers or radio frequency identifi cation. IVF Witness ( www.ivfwitness.com ) and OCTAX Ferti Proof™ ( www.mtg-de.com/ ) utilize RFID (radio frequency iden-tifi cation) technology to read labels attached to all labware, enabling sperm and oocytes to be tracked throughout the IVF process. Th is technology reduces the chance of human error and helps to ensure that the resulting embryo is transferred to the correct patient.
Automated witnessing systems such as Embryo-Matcher ( www.fertqms.com ) can also be incorporated into the incubator imaging system, recording bar codes of dishes while monitoring embryo development. Th e data can be transmitted to a computer for continuous monitoring either on site or remotely.
Electronic witnessing systems have the advantage that they can be programmed to include traceability for all the media and batches of consumables used for a specifi c case. Th ey also provide information on who
performs specifi c procedures and the time that it takes for completion, which is very useful for audit purposes. However, it is essential that full risk assessments and validation checks are performed before introducing e-witnessing, rather than just accepting that a barcode system will work effi ciently.
Ambient air quality Air cleanliness is classifi ed according to the number and size of particles within a sample of air, measured in particles per cubic foot or cubic meter of air.
Laboratory air quality should be maintained by use of positive air pressure relative to adjacent areas; the airfl ow pressures in clean areas should be continuously monitored and frequently recorded. Adjacent rooms with diff erent clean area classifi cation should have a pressure diff erential of 10–15 pascals, with the highest pressure in the most critical areas. High effi ciency par-ticulate air (HEPA) fi lters that remove particles smaller than 0.3 µm and fi lters to remove volatile organic com-pounds, which can adversely aff ect the health of human gametes and embryos, can also be used (Cohen et al ., 1997 ; Cutting et al ., 2004 ). Filters must be regularly inspected and changed to ensure that their effi ciency is not reduced.
Th e environment in a clean room is produced by incorporating parallel streams of HEPA-fi ltered air (laminar fl ow) that blow across the room to expel any dust and particles in the airfl ow by the shortest route, moving at a uniform velocity of 0.3–0.45 meters per second. Th e air velocity over critical areas must be at a suffi ciently high level to sweep particles away from the area and ensure that particles do not thermally migrate from the laminar fl ow. At least 20 changes of air per hour are usually required for clean rooms classifi ed as Grade B, C and D (see Table 8.1 ).
Th e airfl ow can either be vertical downfl ow (enter-ing via fi lters in the roof, exiting through vents in the fl oor) or horizontal crossfl ow (entering through fi lters in one sidewall and exhausted above the fl oor in the sidewall opposite and/or recirculated via a bank of fi lters).
Th e US Federal Standard 209E defi nes air quality based upon the maximum allowable number of par-ticles 0.5 μm and larger per cubic foot of air: Class 1, 100, 1000, 10 000 and 100 000. Th e lower the number, the cleaner the air. Th e ISO classifi cations are defi ned as ISO Class 1, 2, 3,4, etc. through to Class 9. Th e clean-est, ultrapure air is Class 1. Guidelines suggested by

Chapter 8: The clinical in-vitro fertilization laboratory
113
regulatory and legislative authorities for IVF labora-tories are based on those for Good Manufacturing Procedures (GMP), which defi ne four grades of clean area (A–D) for aseptic handling and processing of products that are to be used in clinical treatment ( Tables 8.1a and 8.1b ). Each area has recommenda-tions regarding required facilities, environmental and physical monitoring of viable and nonviable particles, and personnel attire.
Grade A (equivalent to Class 100 [US Federal • Standard 209E], ISO 5 [ISO 14644–1]) is the most stringent, to be used for high risk operations that require complete asepsis, carried out within laminar fl ow biological safety cabinets (BSC). Grade B (equivalent to Class 100, ISO 5) provides • the background environment for a Grade A zone, e.g., clean room in which the BSC is housed. Grade C (equivalent to Class 10 000, ISO 7) is a • clean area for carrying out preparatory stages in manufacture of aseptically prepared products, e.g., preparation of solutions to be fi ltered. Grade D (equivalent to Class 100 000, ISO 8) is a • clean area for carrying out less critical stages in manufacture of aseptically prepared products, such as handling of components aft er washing.
Personnel entering all grades of clean area must main-tain high standards of hygiene and cleanliness at all times, and should not enter clean areas in circum-stances that might introduce microbiological haz-ards, i.e., when ill or with open wounds. Changing and washing procedures must be defi ned and adhered to, with no outdoor clothing introduced into clean areas. Wearing of watches, jewelry and cosmetics is discour-aged. Changing rooms for outdoor clothing should lead into a Grade D area (not B or C). Protective cloth-ing for the diff erent areas is defi ned:
Grade D: protective clothing and shoes, hair, • beard, moustache covered Grade C: single or 2-piece suit with high neck, • wrists covered, shoes/overshoes, hair beard moustache covered; non-shedding materials Grade A and B: headgear, beard and moustache • covered, masks, gloves, non-shedding materials, and clothing should retain particles shed by operators.
Th e Tissue and Cells Directive issued by the European Union (Directive 2003/94/EC) stipulates that where human cells and tissue are exposed to the environment during processing, the air quality should be Grade A with the background environment at least
Table 8.1 (a) Comparison of air classifi cation systems
WHO GMP US 209E US Customary ISO/TC (209) ISO 14644 EEC GMP
Grade A M 3.5 Class 100 ISO 5 Grade A
Grade B M 3.5 Class 100 ISO 5 Grade B
Grade C M 5.5 Class 10 000 ISO 7 Grade C
Grade D M 6.5 Class 100 000 ISO 8 Grade D
Table 8.1(b) Classifi cation of clean areas in terms of airborne particles
At rest In operation
Maximum permitted number of particles/m 3
Grade 0.5–5.0 µm >5 µm 0.5–5.0 µm >5 µm
A 3 500 0 3 500 0
B 3 500 0 350 000 2 000
C 350 000 2 000 3 500 000 20 000
D 3 500 000 20 000 Not defi ned Not defi ned
“At rest” = equipment installed and operating; “in operation” = installed equipment functioning and specifi ed number of personnel present.

Chapter 8: The clinical in-vitro fertilization laboratory
114
equivalent to Grade D, unless a less stringent air qual-ity may be justifi ed and documented as achieving the quality and safety required for the type of tissue and cells, process and human application concerned. Since there is no documented evidence of disease transmis-sion in ART treatment that can be attributed to air qual-ity in the laboratory, the European Society for Human Reproduction and Embryology (ESHRE) suggests that less stringent air quality is justifi ed for ART.
Th e regulatory authority in the UK (Human Fertilisation and Embryology Authority, HFEA) rec-ommends that all work in the IVF laboratory be carried out in Class II fl ow cabinets delivering Grade C qual-ity air to ensure safe handling of gametes and embryos, with the background environment as close as possible to Grade D ( www.hfea.gov.uk ).
Cell culture CO 2 incubators are available (Th ermo Forma, www.thermo.com ) that are equipped with a HEPA fi lter airfl ow system that continuously fi lters the entire chamber volume every 60 seconds, providing Class 100/Grade B air quality within 5 minutes of clos-ing the incubator door. Th ese incubators also incorp-orate a sterilization cycle (Steri-Cycle™) , and can be supplied with an additional ceramic fi lter that excludes volatile low molecular weight organic and inorganic molecules, collectively known as volatile organic com-pounds (VOCs). Some air purifi cation systems also incorporate UV fi lters.
Volatile organic compounds Th e importance of ambient air and the possible con-sequences of chemical air contamination have been reviewed by Cohen et al . ( 1997 ). Whereas most organ-isms and species are protected to some extent from hazards in their ambient environment through their immune, digestive and epithelial systems, oocytes and embryos in vitro have no such protection, and their active and passive absorption mechanisms are largely indiscriminate. IVF laboratories set up in buildings within polluted areas, or close to airports or industrial manufacturing sites, may be subject to serious chem-ical air contamination, which may be refl ected by inad-equate pregnancy and live birth rates. Large traditional incubators obtain their ambient air directly from the laboratory room; gas mixtures are supplied in gas bot-tles, which may be contaminated with organic com-pounds or metallic contaminants. Pressurized rooms using HEPA fi ltration are used by many IVF labora-tories, with standards applied to pharmaceutical clean
rooms; however, HEPA fi ltration cannot eff ectively retain gaseous low molecular weight organic and inor-ganic molecules.
Th e four most common air pollutants are: 1. Volatile organic compounds (VOCs): in urban
and dense suburban areas, VOCs are produced by industry, by vehicle and heating exhausts, as well as by a variety of cleaning procedures. Instruments such as microscopes, television monitors or furniture (as a result of manufacturing processes) may also produce VOCs; perfumes, aft er-shave and other highly scented aerosols are also potential sources, and all theater and laboratory staff should be discouraged from their use.
2. Small inorganic molecules such as N 2 O, SO 2 , CO. 3. Substances derived from building materials, such
as aldehydes from fl ooring adhesives, substituted benzenes, phenol and n -decane released from vinyl fl oor tiles – fl ooring adhesives have been found to be particularly aggressive in arresting embryo development. Newly painted surfaces frequently present a hazard, as many paints contain substances that are highly toxic in the IVF laboratory; laboratory renovations and painting should always be planned during a period when treatment cycles are not being performed .
4. Other polluting compounds which may be released by pesticides or by aerosols containing butane or iso-butane as a propellant. Liquids such as fl oor waxes may contain heavy metals, which have a drastic eff ect on embryo implantation potential.
Cohen and colleagues conducted a detailed study of chemical air contamination in all areas of their IVF laboratory, which revealed dynamic interactive proc-esses between air-handling systems, spaces, tools, disposable materials and other items unique to their laboratory. Anesthetic gases, refrigerants, cleaning agents, hydrocarbons and aromatic compounds were detected, and some accumulated specifi cally in incuba-tors. Th e authors suggest that there may be an interaction between water-soluble and lipid-soluble solid phases such as those in incubators: whereas some contaminants may be absorbed by culture media, this may be counter-acted by providing a larger sink such as a humidifi cation pan in the incubator. Mineral oil may act as a sink for other components. Unfi ltered outside air may be cleaner than HEPA-fi ltered laboratory air or air obtained from incubators, due to accumulation of VOCs derived from adjacent spaces or specifi c laboratory products,

Chapter 8: The clinical in-vitro fertilization laboratory
115
including sterile Petri dishes. Standards for supplies of compressed gases are based upon criteria that are not designed for cultured and unprotected cells, with no perspective of the specifi c clean air needs of IVF. New incubators can have VOC concentrations more than 100-fold higher than used incubators from the same manufacturer – allowing the emission of gases from new laboratory products is crucial. Systems are now available for installation into existing air conditioning systems that can clean the air and reduce VOCs ( http://zandair.com/air-purifi cation-fi lter-PCOC3.html ).
VOCs can be measured in the laboratory using hand-held monitors that use photo ionization moni-tors (e.g., VOC Meter, Research Instruments, www.researchinstruments.com , Eco sensor C21). Th ese meters are very sensitive, and can be used to screen equipment and consumables to pinpoint sources of VOCs. Active fi ltration units with activated carbon fi lters and oxidizing material have now been devel-oped specifi cally for IVF laboratories, and these can be placed inside cell-culture incubators or in the laboratory spaces themselves (CODA Filters, www.IVFonline.com; Cohen et al ., 1997 ; Boone et al ., 1999 ). As always, prevention is the best strategy, and eff orts should be made to eliminate potential sources such as alcohol disinfectants and anesthetic gases – as well as perfumes/aft er-shave lotions – from the laboratory .
Biological safety cabinets A biological safety cabinet or BSC is an enclosed work-space that provides protection either to workers, the products being handled, or both. BSCs provide pro-tection from infectious disease agents, by sterilizing the air that is exposed to these agents. Th e air may be sterilized by UV light, heat or passage through a HEPA fi lter that removes particles larger than 0.3 µm in diam-eter. BSCs are designated by class, based on the degree of hazard containment and the type of protection they provide. In order to ensure maximum eff ectiveness, certain specifi cations must be met: (a) Whenever possible, a 30 cm clearance should be
provided behind and on each side of the cabinet, to ensure eff ective air return to the laboratory. Th is also allows easy access for maintenance .
(b) Th e cabinet should have 30–35 cm clearance above it, for exhaust fi lter changes.
(c) Th e operational integrity of a new BSC should be validated by certifi cation before it is put into service, or aft er it has been repaired or relocated.
(d) All containers and equipment should be surface decontaminated and removed from the cabinet when the work is completed. Th e work surface, cabinet sides and back, and interior of the glass should be wiped down (70% ethanol and Fertisafe [ www.research-instruments.com ] are eff ective disinfectants) at the end of each day.
(e) Th e cabinet should be allowed to run for 5 minutes aft er materials are brought in or removed.
BSC Classes Class I ( Figure 8.1a ) – provides personnel and envir-onmental protection, but no product protection. Cabinets have an open front, negative pressure and are ventilated. Nonsterile room air enters and circulates through the cabinet. Th e environment is protected by fi ltering exhaust air through a 0.3 µm HEPA fi l-ter. Th e inward airfl ow protects personnel as long as a minimum velocity of 75 linear feet per minute (lfpm) is maintained through the front opening. Th is type of cabinet is useful to enclose equipment or procedures that have a potential to generate aerosols (centrifuges, homogenizing tissues, cage dumping), and can be used for work involving microbiological agents of moderate to high risk.
Class II – incorporates both charcoal and HEPA fi lters to ensure an environment that is close to sterile. It provides product, personnel and environment pro-tection, using a stream of unidirectional air moving at a steady velocity along parallel lines (“laminar fl ow”). Th e laminar fl ow, together with HEPA fi ltration, cap-tures and removes airborne contaminants and provides a particulate-free work environment. Airfl ow is drawn around the operator into the front grille of the cabinet, providing personnel protection. A downward fl ow of HEPA-fi ltered air minimizes the chance of cross-contamination along the work surface. Exhaust air is HEPA fi ltered to protect the environment, and may be recirculated back into the laboratory (Type A, Figure 8.1b ) or ducted out of the building (Type B).
Class II cabinets provide a microbe-free environ-ment for cell culture, and are recommended for manip-ulations in an IVF laboratory. Th ey can be modifi ed to accommodate microscopes, centrifuges or other equipment, but the modifi cation should be tested and certifi ed to ensure that the basic systems operate prop-erly aft er modifi cation. No material should be placed on front or rear grille openings, and laboratory doors should be kept closed during use to ensure adequate

Chapter 8: The clinical in-vitro fertilization laboratory
116
Figure 8.1 (a, b, c) Schematic diagrams of airfl ow in biological safety cabinets. (Reproduced with permission from Elder, K., Baker, D. J. and Ribes, J.A. 2004. Infections, Infertility and Assisted Reproduction . Cambridge: Cambridge University Press.)

Chapter 8: The clinical in-vitro fertilization laboratory
117
airfl ow within the cabinet. It should be noted that the laminar fl ow of air can have a signifi cant cooling eff ect on culture dishes; some laboratories choose to switch off the fl ow of air at appropriate times when it is safe to do so.
Class III – is used for routine anaerobe work, and is designed for work with high-risk organisms in max-imum containment facilities. Th is cabinet provides maximum protection to the environment and the worker. It is completely enclosed with negative pres-sure, plus access for passage of materials through a dunk tank or double-door pass through box that can be decontaminated between uses. Air coming into and going out of the cabinet is HEPA fi ltered, and exhaust air passes through two HEPA fi lters, or a HEPA fi lter and an air incinerator before discharge to the outdoors. Infectious material within the cabinet is handled with rubber gloves that are attached and sealed to ports in the cabinet ( Figure 8.1c ).
Horizontal laminar fl ow “clean bench” – provides only product protection, and is not a BSC. HEPA fi l-tered air is discharged across the work surface towards the user. Th ese can be used for clean activities, but should never be used when handling cell cultures or infectious materials.
Vertical laminar fl ow “clean bench” – is also not a BSC, but is useful in hospital pharmacies for prep-aration of intravenous drugs. Although they generally have a sash, the air is usually discharged into the room under the sash.
Water quality Although the majority of media required for an IVF laboratory are now commercially available, if any solu-tions are to be prepared “in house,” a reliable source of ultrapure water is a critical factor. A pure water source is also required for washing and rinsing nondispos-able equipment. Weimer et al ., ( 1998 a) carried out a complete analysis of impurities that can be found in water: this universal solvent provides a medium for most biological and chemical reactions, and is more susceptible to contamination by other substances than any other common solvent. Both surface and ground water are contaminated with a wide range of substances, including fertilizers, pesticides, herbicides, detergents, industrial waste effl uent and waste solvents, with sea-sonal fl uctuations in temperature and precipitation aff ecting the levels of contamination. Four categories of contaminants are present: inorganics (dissolved
cationic and anionic species), organics, particles and microorganisms such as bacteria, algae, mold and fungi. Chlorine, chloramines, polyionic substrates, ozone and fl uorine may be added to water during treat-ment processes, and must be removed from water for cell culture media preparation. In water purifi cation, analysis of the feed water source is crucial to determine the proper fi ltration steps required, and water-process-ing protocols should be adapted to meet regional requirements. Processing systems include particulate fi ltration, activated carbon cartridge fi ltration , reverse osmosis (RO) and electrodeionization (EDI), an ultra-violet oxidation system , followed by a Milli-Q PF Plus purifi cation before fi nal fi ltration through a 0.22 mm fi lter to scavenge any trace particles and prevent reverse bacterial contamination from the environment.
IVF laboratory personnel should be familiar with any subtle variations in their water source, as well as the capabilities of their water purifi cation system, and develop protocols to ensure consistently high-quality ultrapure water supplies, following manufacturers’ instructions for monitoring, cleaning, fi lter replace-ment and maintenance schedules.
Supplies A basic list of supplies is outlined at in the appen-dix at the end of this chapter; the exact combination required will depend upon the tissue culture system and techniques of manipulation used. Disposable supplies are used whenever possible and must be guaranteed nontoxic tissue culture grade, in particu-lar the culture vessels, needles, collecting system and catheters for oocyte aspiration and embryo transfer. Disposable glass pipettes are required for gamete and embryo manipulations, and these can be purchased pre-sterilized and packaged. If nonsterile dispos-able pipettes are purchased, they must be soaked and rinsed with tissue culture grade sterile water and dry heat sterilized before use. In preparing to han-dle gametes or embryos, examine each pipette and rinse with sterile medium to ensure that it is clean and residue-free.
Important considerations in the selection of sup-plies include:
Suitability for intended purpose • Suitable storage facilities (i.e., storerooms away • from excessive heat/direct sunlight) Compliance of suppliers to a contract with • specifi ed terms and conditions

Chapter 8: The clinical in-vitro fertilization laboratory
118
Disposable plastics CE marked or mouse embryo • tested where possible Media with quality certifi cation, mouse embryo • tested and proven track record, with validation evidence Delivery of perishable items such as media under • controlled conditions Batch numbers to be recorded for quality • assurance purposes Health and safety of operators handling potentially • infectious bodily fl uids.
Routine schedules of cleaning, maintenance, and servicing must be established for each item of equip-ment, and checklist records maintained for daily, weekly, monthly and annual schedules of cleaning and maintenance of all items used, together with checks for restocking and expiry dates of supplies.
Tissue culture media Original IVF culture systems were based on simple media developed for organ explant and somatic cell culture, designed to mimic physiological conditions. Analysis of tubal and uterine fl uids, together with research into embryo metabolism, then led to the devel-opment of complex media. Many controlled studies have shown fertilization and cleavage to be satisfactory in a variety of simple and complex media (comprehen-sive reviews are published by Bavister, 1995 ; Edwards and Brody, 1995 ; Biggers, 2008 ). Metabolic and nutri-tional requirements of mammalian embryos are complex, stage specifi c, and, in many cases, species specifi c; several decades of research in laboratory and livestock animal systems have shown that, although there are some basic similarities, culture requirements of diff erent species must be considered independ-ently. Understanding metabolic pathways of embryos and their substrate and nutrient preferences has led to major advances in the ability to support embryo devel-opment in vitro.
Culture media: physical parameters
• Osmolarity = osmoles of solute particles per liter of solution Temperature-dependent (volume changes with temperature) Osmolarity of tubal/uterine secretions = 275–305 mOsm/L Osmolality = the osmotic concentration of a solu-• tion, mOsm/kg of solvent
Temperature-independent One osmole = Avogadro’s number of osmoticallyactive particles = 6.02 × 10 23 Physiological pH range of body fl uids = 7.2–7.5. • pH is related to an equilibrium between gas phase CO
2 and CO
2 /HCO
3 dissolved in the medium, with
carbonic acid as an intermediate. Henderson–Hasselbach equation :
CO 2 (gas) ↔ CO
2 (dissolved) ↔ H
2 CO
3 + H + + HCO
3
pH = pK a + log
10 [H + ]
= log of the reciprocal of the molar concentra-tion of hydrogen ions
pK a = ionization constant for the acid
pH is aff ected by: Temperature (less CO •
2 dissolved at higher
temperature) Atmospheric pressure (more CO •
2 in solution at
higher pressure) Presence of other solutes such as amino acids and • complex salt mixtures, since pK
a is a function of
salt concentration. HEPES-buff ered medium has been equilibrated to a • pH of 7.4 in the presence of bicarbonate; exposure to a CO
2 atmosphere will lower the pH, and therefore
culture dishes containing HEPES-buff ered medium should be equilibrated at 37°C only, and not in a CO
2
incubator . Temperature fl uctuations during storage and hand-• ling can aff ect pH, and should therefore be avoided:
acid pH destroys glutamine and pyruvate • some salts or amino acids may precipitate out of • solution, and further aff ect pH.
Fertilization can be achieved in very simple media such as Earle’s, or a TALP-based formulation, but the situation becomes more complex thereaft er (see Chapter 5 for details of embryo metabolism). Prior to 1997, single media formulations were used for all stages of IVF. However, research in animal systems during the 1990s led to elucidation of the metabolic biochem-istry and molecular mechanisms involved in gamete maturation, activation, fertilization, genomic activa-tion, cleavage, compaction and blastocyst formation. Th is drew attention to the fact that nutrient and ionic requirements diff er during all these diff erent stages. Inappropriate culture conditions expose embryos to cellular stress which could result in retarded cleav-age, cleavage arrest, cytoplasmic blebbing, impaired energy production, inadequate genome activation and transcription. Blastocyst formation is followed by an exponential increase in protein synthesis, with
• Osmolarity = osmoles of solute particles per liter of solution Temperature-dependent (volume changes withtemperature) Osmolarity of tubal/uterine secretions= 275–305 mOsm/L Osmolality = the osmotic concentration of a solu-•tion, mOsm/kg of solvent
Temperature-independent One osmole = Avogadro’s number of osmoticallyactive particles = 6.02 × 1023
Physiological pH range of body fl uids = 7.2–7.5.•pH is related to an equilibrium between gas phaseCO
2 and CO
2 /HCO
3 dissolved in the medium, with
carbonic acid as an intermediate. Henderson–Hasselbach equation :
CO 2 (gas) ↔ CO
2(dissolved) ↔ H
2CO
3+ H+ + HCO
3
pH = pKa + log
10 [H + ]
= log of the reciprocal of the molar concentra-tion of hydrogen ions
pK a
= ionization constant for the acid
pH is aff ected by: Temperature (less CO •
2 dissolved at higher
temperature) Atmospheric pressure (more CO•
2 in solution at
higher pressure)Presence of other solutes such as amino acids and• complex salt mixtures, since pK
ais a function of
salt concentration. HEPES-buff ered medium has been equilibrated to a•pH of 7.4 in the presence of bicarbonate; exposureto a CO
2atmosphere will lower the pH, and therefore
culture dishes containing HEPES-buff ered mediumshould be equilibrated at 37°C only, and not in a CO
2
incubator . Temperature fl uctuations during storage and hand-• ling can aff ect pH, and should therefore be avoided:
acid pH destroys glutamine and pyruvate •some salts or amino acids may precipitate out of •solution, and further aff ect pH.

Chapter 8: The clinical in-vitro fertilization laboratory
119
neosynthesis of glycoproteins, histones and new sur-face antigens.
Although the specifi c needs of embryos during their preimplantation development have by no means been completely defi ned, sequential, stage-specifi c and chemically defi ned media are used in IVF systems. Media formulations endeavor to mimic the natural in-vivo situation and take into account the signifi cant changes in embryo physiology and metabolism that occur during the preimplantation period. Th ree diff er-ent types of protocols are used worldwide: 1. One-step culture using a single medium
formulation (nonrenewal monoculture) 2. Single medium formulation, renewed on D2/D3
(renewal monoculture) 3. Two-step culture using two diff erent media
formulations (sequential media culture).
Although two-step sequential media have been favored in recent years, doubts have been raised as to whether these more complex protocols have any advantage over one-step protocols (see Biggers and Summers, 2008 for review).
Commercial media is “ready to use,” with protein supplements added, and may also contain other com-ponents or factors. Diff erent formulations are avail-able for sperm preparation, oocyte washing during retrieval, insemination/fertilization, early cleavage, blastocyst development and freezing/thawing. Media containing HEPES, which maintains a relatively stable pH even in ambient air, can be used for sperm prepar-ation, oocyte harvesting and washing, and during ICSI procedures; however, HEPES-buff ered medium will become acidic when placed in a CO 2 atmosphere, and therefore the gametes should be washed in HEPES-free medium before being placed in the culture incubator .
Media used in embryo culture and manipulation (see Table 8.2 )
Simple media: balanced salt solutions (BSS)
Contain combinations of Na, K, Cl, Ca, Pi, Mg, HCO • 3 ,
glucose, ± phenol red Salt concentrations/balance diff er slightly in diff er-• ent formulations: Ringer’s: contains Na, K, Cl, Ca only Earle’s, Hank’s, Tyrode’s etc.: also contain Pi, Mg, HCO
3 , glucose.
Complex media Contain the inorganic salts of BSS, as well as amino acids, fatty acids, vitamins, other substrates (nucleotide
bases, cholesterol, glutathione , other macromol-ecules), antibiotics, and other labile substances to be added before use (pyruvate, lactate, glutamine, methionine, bicarbonate):
Minimal essential medium (MEM) • Dulbecco’s modifi ed MEM • Ham’s F-10, F-12 • BWW, TC199, KSOM, etc. •
Media optimized for preimplantation embryos
Menezo B2, “complex,” designed for bovine embryo • culture (1976) Human tubal fl uid (HTF), “simple,” contains pyruvate • and lactate (Quinn, 1995 ) P1, Basal IX HTF: no pyruvate or lactate, contains • EDTA and glutamine HTF-12: no phosphate, low level of glucose + EDTA, • taurine, glutathione G1/S1, “simple,” contains EDTA, lactate/pyruvate, • amino acids G2/S2, “complex,” high level of glucose • Cook IVF: Sydney IVF Cleavage/Sydney IVF Blastocyst • medium Cooper Surgical • Sage • MediCult EmbryoAssist, BlastAssist • FertiPro N.V. Ferticult/Ferticult G3 • Irvine Scientifi c ECM/Multiblast Medium•
Life Global, IVFonline.com •
Phosphate buff ered saline (PBS) and HEPES buff -ers: commonly used to stabilize pH solutions used for washing in room atmosphere, e.g., follicle fl ushing, cryopreservation protocols, sperm preparation.
Rigorous quality control is essential in media prep-aration, including knowledge of the source of all ingre-dients, especially the water, which must be tested to make sure that it is endotoxin-free, low in ion content, and guaranteed free of organic molecules and microor-ganisms. Pharmaceutical grade reagents are required in order to follow Good Manufacturing Practice (GMP). Each batch of culture media prepared must be checked for osmolality (285 ± 2 mOsm/kg) and pH (7.35–7.45), and subjected to quality control procedures with LAL (limulus amebocyte lysate) test for endotoxins and sperm survival or mouse embryo toxicity before use. Culture media can rapidly deteriorate during storage, with a decrease in its ability to support embryo devel-opment, and careful attention must be paid to storage conditions and manufacturers’ recommended expiry dates. Commercially prepared, pretested high-quality
Simple media: balanced salt solutions (BSS)
Contain combinations of Na, K, Cl, Ca, Pi, Mg, HCO •3,
glucose, ± phenol red Salt concentrations/balance diff er slightly in diff er-•ent formulations: Ringer’s: contains Na, K, Cl, Ca only Earle’s, Hank’s, Tyrode’s etc.: also contain Pi, Mg, HCO
3 , glucose.
Complex media Contain the inorganic salts of BSS, as well as amino acids, fatty acids, vitamins, other substrates(nucleotide
bases, cholesterol, glutathione , other macromol-ecules), antibiotics, and other labile substances tobe added before use (pyruvate, lactate, glutamine,methionine, bicarbonate):
Minimal essential medium (MEM) • Dulbecco’s modifi ed MEM• Ham’s F-10, F-12• BWW, TC199, KSOM, etc. •
Media optimized for preimplantation embryos
Menezo B2, “complex,” designed for bovine embryo•culture (1976) Human tubal fl uid (HTF), “simple,” contains pyruvate• and lactate (Quinn, 1995 ) P1, Basal IX HTF: no pyruvate or lactate, contains•EDTA and glutamine HTF-12: no phosphate, low level of glucose + EDTA,• taurine, glutathione G1/S1, “simple,” contains EDTA, lactate/pyruvate,• amino acids G2/S2, “complex,” high level of glucose • Cook IVF: Sydney IVF Cleavage/Sydney IVF Blastocyst• medium Cooper Surgical • Sage• MediCult EmbryoAssist, BlastAssist• FertiPro N.V. Ferticult/Ferticult G3 • Irvine Scientifi c ECM/Multiblast Medium• Life Global, IVFonline.com•
Phosphate buff ered saline (PBS) and HEPES buff -ers: commonly used to stabilize pH solutions used forwashing in room atmosphere, e.g., follicle fl ushing,cryopreservation protocols, sperm preparation.

Chapter 8: The clinical in-vitro fertilization laboratory
120
culture media is available for purchase from a number of suppliers worldwide, so that media preparation for rou-tine use in the laboratory is not necessary, and may not be a cost-eff ective exercise when time and quality con-trol are taken into account. Th ere is so far no fi rm sci-entifi c evidence that any medium is superior to another in routine IVF, and choice should depend upon consid-erations such as quality control and testing procedures applied in its manufacture, cost, and, in particular, guar-anteed effi cient supply delivery in relation to shelf life. Aft er delivery, the medium may be aliquoted in suitable small volumes, such that one aliquot can be used for a single patient’s gamete preparation and culture (includ-ing sperm preparation). Shelf life is dependent on spe-cifi c composition and conditions of storage; generally, the more “complex” the media, the shorter its useful life-span, with an average of approximately 4–6 weeks. All media must be equilibrated for temperature and pH for 4–6 hours before use, ideally by overnight incubation.
Important factors when choosing commercial media
• Information available about composition (not always easy to obtain) Information about quality control during production • Information about endotoxin testing • Assurance of regular, reliable delivery under con-• trolled conditions Acceptable shelf life • Delivery of batches well before expiry date • Validation evidence of use in human IVF – i.e., proven • track record Tested using appropriate bioassay • Certifi cates of analysis available • Serum or serum derivatives should be from virally • screened sources
Protein supplement Protein, or an equivalent macromolecule (e.g., poly-vinyl alcohol, hyaluronate), is required in human IVF for:
Sperm capacitation – involves the removal of • sterols from the plasma membrane, and this requires a sterol acceptor molecule (such as albumin) in the medium. Handling – a molecule with surfactant properties • is needed to facilitate sperm and embryo handling in order to prevent sticking to pipettes and dishes. Proteins also act as lipid and peptide carriers, • chelators, cell surface protectors, regulators of redox potential, and are a source of fi xed nitrogen/amino acids aft er hydrolysis.
Bovine serum albumin was previously used for human embryo culture, but this is now recognized to carry the risk of disease transmission, including prion disease (Creutzfeldt–Jakob disease, CJD). In domestic animals, media supplemented with whole serum was found to aff ect embryo development at several dif-ferent levels (Leese, 1998 ), and its presence is associ-ated with the development of abnormally large fetuses when used to grow embryos to the blastocyst stage (Th ompson et al ., 1995 ). Although the mechanisms involved are unresolved, the fi ndings led to further concerns about the use of whole serum in human IVF, particularly in extended culture systems, and serum substitutes are used instead.
Albumin is the major protein constituent of the embryo’s environment; it can be incorporated by the embryo, it binds lipids and may help to bind and
• Information available about composition (notalways easy to obtain) Information about quality control during production • Information about endotoxin testing • Assurance of regular, reliable delivery under con-•trolled conditions Acceptable shelf life• Delivery of batches well before expiry date • Validation evidence of use in human IVF – i.e., proven•track record Tested using appropriate bioassay • Certifi cates of analysis available • Serum or serum derivatives should be from virally•screened sources
Table 8.2 International regulations regarding the use of IVF culture media
Australia Regulated by the Australian Therapeutic Goods Administration (TGA) as a Class III medical device
USA Regulated by the FDA as a Class II medical device with special conditions under the 510k Pre-market notifi cation scheme
Japan Classed as a laboratory reagent in Japan, and as such, has no formal regulatory review or approval
China No offi cial designation of the IVF media as a medical device, but regulatory approval by the Chinese Regulator (SFDA) is required to apply for hospital tenders
France IVF media products are seen as a “hybrid” product in France (i.e., somewhere between drug and device) and are regulated as a PTA (Produit Therapeutique Annexe) by the French Regulatory Authority (AFSSaPS)
European Union (excl. France)
IVF cell culture media has not been offi cially declared a medical device in the EU

Chapter 8: The clinical in-vitro fertilization laboratory
121
stabilize growth factors. Th eoretically it may not be indispensable, but it does eff ectively replace serum, and has a major role both in maintaining embryo quality and in preventing gametes and embryos from sticking to glass or plastic surfaces, facilitating their manipulation. Commercially prepared media are sup-plied complete; most contain a serum substitute such as human serum albumin (HSA). Human serum contains approximately 4.5% albumin, i.e., 45 mg/mL. A supple-ment of 10% human serum albumin (HSA) provides an albumin concentration of 4.5%. Serum Substitute Supplement (SSS) is a 6% protein solution made up of 84% HSA, 16% alpha- and beta-globulins, plus a trace of gamma globulins. Although disease transmission from commercial preparations of HSA were a concern in the past, recombinant preparations are now available and are used routinely in commercial culture media.
Growth factors Growth factors play a key role in growth and diff eren-tiation from the time of morula/blastocyst transition . However, defi ning their precise role and potential for improving in-vitro preimplantation development is complicated by factors such as gene expression of both the factors and their receptors. Th ere is also the potential of ascribing positive eff ects to specifi c fac-tors when the result may in fact be due to a combin-ation of a myriad of other causes. Th e mammalian blastocyst expresses ligands and receptors for several growth factors, many of which can cross-react, mak-ing it diffi cult to interpret the eff ects of single factors added to a medium. Insulin, LIF, EGF/TGF-α, TGF-β, PDGG, HB-EGF have all been studied in IVF culture, and, although it is clear that these and other growth factors may infl uence in-vitro blastocyst development and hatching, further assessment remains an area of research – a comprehensive review was published by Richter in 2008. It has been suggested that the mechan-ism whereby serum induces abnormalities in domestic animal systems may involve the overexpression of cer-tain growth factors – there is no doubt that complex and delicate regulatory systems are involved.
Culture of embryos in “groups” rather than sin-gly has been found to improve viability and implant-ation in some systems: it is possible that autocrine/paracrine eff ects or “trophic” factors exist between embryos. However, observed eff ects of “group” culture will inevitably be related to the composition of the cul-ture medium and the precise physical conditions used
for embryo culture, and in particular the number of embryos in relation to the volume of media used per culture drop .
Follicular fl ushing media Ideally, if a patient has responded well to follicular phase stimulation with appropriate monitoring and timing of ovulation induction , the oocyte retrieval will proceed smoothly with effi cient recovery of oocytes without the need to fl ush follicles. If the number of follicles is low or the procedure is diffi cult for technical reasons, follicles may be fl ushed with a physiological solution to assist recovery of all the oocytes. Follicles can be fl ushed with balanced salt solutions such as Earle’s (EBSS) or lac-tated Ringer’s solution , and heparin may be added at a concentration of 2 units/mL. HEPES-buff ered media can also be used for fl ushing. Temperature and pH of fl ushing media must be carefully controlled, and the oocytes recovered from fl ushing media subsequently washed in culture media before transfer to their fi nal culture droplet or well.
Tissue culture systems Vessels successfully used for IVF include test-tubes, four-well culture dishes, organ culture dishes and Petri dishes containing microdroplets of culture medium under a layer of clinical grade mineral or silicone oil. Whatever the system employed, it must be capable of rigidly maintaining fi xed stable parameters of tempera-ture, pH and osmolarity. Human oocytes are extremely sensitive to transient cooling in vitro, and modest reduc-tions in temperature can cause irreversible disruption of the meiotic spindle, with possible chromosome dis-persal. Temperature-induced chromosome disruption may contribute to aneuploidy, and the high rates of preclinical and spontaneous abortion that follow IVF and ICSI. Th erefore, it is essential to control tempera-ture fl uctuation from the moment of follicle aspiration, and during all oocyte and embryo manipulations, by using heated microscope stages and heating blocks or platforms. Most importantly, the temperature within the media itself must be maintained at the optimal tem-perature, rather than the temperature of the dish.
An overlay of equilibrated oil as part of the tissue culture system confers specifi c advantages : 1. Th e oil acts as a physical barrier, separating
droplets of medium from the atmosphere and airborne particles or pathogens .

Chapter 8: The clinical in-vitro fertilization laboratory
122
2. Oil prevents evaporation and delays gas diff usion, thereby keeping pH, temperature and osmolality of the medium stable during gamete manipulations, protecting the embryos from signifi cant fl uctuations in their microenvironment (aliquots of medium without an oil overlay begin to show an immediate rise in pH as soon as they are removed from the incubator).
3. Oil prevents evaporation: humidifi ed and pre-equilibrated oil allows the use of nonhumidifi ed incubators, which are easier to clean and maintain. It has been suggested that oil could enhance
embryo development by removing lipid-soluble tox-ins from the medium; on the other hand, an oil over-lay prevents free diff usion of metabolic by-products such as ammonia, and accumulation of ammonia in culture media is toxic to the embryo. Th e use of an oil overlay also infl uences oxygen concentration in the medium, with resulting eff ects on the delicate bal-ance of embryo metabolism; as mentioned previously, it can absorb and concentrate harmful VOCs in the incubator atmosphere. Oil is diffi cult to sterilize and inappropriate handling can lead it to be a source of fungal contamination.
Two types of oil have been used in culture over-lays, from a mineral or a silicone source (see box below). Silicone oil, commonly used as a stationary phase in gas chromatography or as an anti-foaming agent, should not be confused with mineral oil, which is obtained from fractionated distillation in the pet-rol industry .
Types of oil used in culture overlays
1. Paraffi n oil – also known as white mineral oil or liquid paraffi n Merck Index: “Liquid Petrolatum” (Petrolatum = • Vaseline) Is derived from petroleum, and exists in many • diff erent forms with diff ering melting points and viscosities Available in “light” or “heavy” forms • Light – density = 0.83–0.89 • Batch to batch variations are common, since they • are a mixture of hydrocarbons with fl uctuating composition
2. Silicone oil (dimethyl-polysiloxane) (Erbach et al ., 1995 ) Polymer, available in many viscosities, from 10 to • 600 000 centistokes Composition should be more stable than that of • paraffi n
• Problems have been encountered with Zn 2+ con-tamination, and toxicity after degradation as a result of exposure to sunlight (Provo and Herr, 1998 )
Oil preparation Commercial companies now supply washed, steri-lized oil that is ready for use in overlays. If obtained from other sources, mineral or silicone oil should be sterile as supplied, and does not require steriliza-tion or fi ltration. High temperature for sterilization may be detrimental to the oil itself, and the proced-ure may also “leach” potential toxins from the con-tainer. Provo and Herr ( 1998 ) reported that exposure of mineral oil to direct sunlight for a period of 4 hours resulted in a highly embryotoxic overlay, and they recommend that washed oil should be shielded from light and treated as a photoreactive compound. Contaminants have been reported in certain types of oil. Washing procedures remove water-soluble tox-ins, but non-water-soluble toxins may also be present which will not be removed by washing. Th erefore it is prudent not only to wash, but to test every batch of oil before use with, at the very least, a sperm survival test as a quality control procedure. Erbach et al . ( 1995 ) suggested that zinc might be a contaminant in sili-cone oil, and found that washing the oil with EDTA removed a toxicity factor that may have been due to the presence of zinc. Some mineral oil products may also contain preservatives such as alpha-tocopherol . Oil can be carefully washed in sterile disposable tis-sue culture fl asks (without vigorous shaking) with either Milli-Q water , sterile saline solution or a sim-ple culture medium without protein or lipid-soluble components, in a ratio of 5:1 (oil:aq). Th e oil can be further “equilibrated” by bubbling 5% CO 2 through the mixture before allowing the phases to separate and settle. Washed oil can be stored either at room temperature or at 4°C in equilibrium with the aque-ous layer, or separated before storage, but should be prepared at least 2 days prior to its use.
Oil overlays must be further equilibrated in the CO 2 incubator for several hours (or overnight) before introducing media/gametes/embryos. Conaghan ( 2008 ) established experimentally that even relatively small volumes of medium (50 µL) with an oil overlay require a minimum of 8 hours equilibration in order to establish a stable pH under normal culture condi-tions. However, once equilibrated, the oil acts as an eff ective buff er, maintaining pH for up to 10 minutes
1. Paraffi n oil – also known as white mineral oil orliquid paraffi n Merck Index: “Liquid Petrolatum” (Petrolatum =•Vaseline) Is derived from petroleum, and exists in many• diff erent forms with diff ering melting points andviscosities Available in “light” or “heavy” forms •Light – density = 0.83–0.89•Batch to batch variations are common, since they• are a mixture of hydrocarbons with fl uctuatingcomposition
2. Silicone oil (dimethyl-polysiloxane) (Erbach et al .,l 1995 ) Polymer, available in many viscosities, from 10 to• 600 000 centistokes Composition should be more stable than that of •paraffi n
• Problems have been encountered with Zn 2+ con-tamination, and toxicity after degradation as a resultof exposure to sunlight (Provo and Herr, 1998 )

Chapter 8: The clinical in-vitro fertilization laboratory
123
aft er removing dishes from the incubator, whereas media without an oil overlay show a dramatic rise in pH as soon as the dishes are removed from the CO 2 atmosphere.
Co-culture systems Co-culture systems played an important role in the evolution of modern culture systems, using a substrate layer of feeder cells in order to support the growth of human embryos and regulate their metabolic turnover processes. A variety of diff erent types of homologous and autologous cells were used as feeder layers in the past, including tubal epithelial cells, explants of endo-metrial tissue, granulosa cells, as well as the animal cells used in commercial vaccine production, African green monkey kidney (Vero). For the same develop-mental stage, embryos co-cultured to the blastocyst stage were found to have higher numbers of cells and a fully cohesive inner cell mass when compared with embryos cultured in simple media. It was postulated that improved development occurs as a result of four diff erent possible mechanisms: 1. “Metabolic locks” : co-culture cell layers can
provide a supply of small molecular weight metabolites which simpler culture media lack. Th is supply may assist continued cell metabolism required for genome activation, and divert the potential for abnormal metabolic processes which may lead to cleavage arrest.
2. Th e feeder cell layer may supply growth factors essential for development.
3. Toxic compounds resulting from cell metabolism can be removed: heavy metal ions may be chelated by glycine produced by feeder cells, and ammonium and urea may be recycled through feeder cell metabolic cycles.
4. Feeder cells can synthesize reducing agents which prevent the formation of free radicals.
Th e use of feeder cells during the late 1980s played an important role in research into embryo metabolism and preimplantation development, and the observa-tions and data obtained were instrumental in helping to develop more appropriate stage-specifi c culture media and systems. However, maintaining a safe and eff ective co-culture system is diffi cult and labor intensive, and their use carries the risk of potential disease transmis-sion, or even retrovirus-induced cell transformation in the feeder layer. Although accumulated experimental
data suggest that the ability of human embryos to develop in vitro during the early cleavage stages is more a measure of their adaptability and survival capabilities than of the suitability of the medium, the use of stage-specifi c media, with composition that is based upon research into early embryo metabolism (see Chapter 5 ), has now largely made the use of co- cultures redun-dant, as well as introducing an unacceptable risk in clinical practice.
Emerging technologies Research continues into technologies that will improve the outcome of in-vitro embryo culture, with the goal of minimizing environmental stress imposed upon the embryo during laboratory manipulations. Th e active integrated workstation is one approach, aiming to eliminate fl uctuations in the physical parameters of the environment. However, carrying out the manipu-lations in these systems is more diffi cult for the oper-ator, and involves additional training, experience and a learning curve. An alternative approach is to mimic dynamic in-vivo conditions by exposing them to con-tinuous movement: “embryo rocking” using a dynamic microfunnel culture system (Heo et al ., 2010 ), tilting platforms (Matsuura et al ., 2010 ) or with microfl uidic technolog y, the use of chambers or devices that enable continuous fl uid movement in a micro- or nano-envi-ronment. Th e gametes/embryos can be perfused with media that gradually changes in composition, provid-ing diff erent chemical substrates for diff erent stages during development. Th is could have the eff ect of removing metabolic by-products such as ammonia, or simply disrupting any micro-gradients that may form in small culture droplets. Although microfl uidic plat-forms for ART procedures have theoretical advantages, and a number of diff erent devices are under trial, there are practical considerations yet to be addressed before they can be successfully implemented (for review, see Swain et al ., 2008 , 2009 ).
Appendix Equipment and supplies for embryology
CO 2 incubator Dissecting microscope Inverted microscope Heated surfaces for microscope and manipulation areas Heating block for test-tubes

Chapter 8: The clinical in-vitro fertilization laboratory
124
Laminar fl ow cabinet Oven for heat-sterilizing Small autoclave Water bath Pipette 10–1000 mL Eppendorf Refrigerator Supply of medical grade CO 2 Supply of 5% CO 2 in air (or special gas mixtures) Wash bottle + Millex fi lter for gas Rubber tubing Pipette canisters Clinical grade mineral or paraffi n oil Culture media Glassware for media preparation Osmometer (for media preparation) Weighing balance Tissue culture plastics: (Nunc, Corning, Sterilin) Flasks for media and oil: 50 mL, 175 mL Culture dishes: 60, 35 mm OCR (oocyte retrieval) needles Test-tubes for OCR: 17 mL disposable Transfer catheters and stylets: embryo, GIFT, IUI Syringes Needles Disposable pipettes: 1, 5, 10, 25 mL “Pipetus” pipetting device Eppendorf tips, small and large Millipore fi lters: 0.22, 0.8 mm Glass Pasteur pipettes (Volac) Pipette bulbs Test-tube racks Rubbish bags Tissues Tape for labeling 7X detergent (Flow) 70% ethanol Sterile gloves, latex and non-latex Oil: Boots, Squibb, Sigma, Medicult Supply of purifi ed water: Milli-Q system or Analar Glassware for making culture media: beakers, fl asks, measuring cylinder
Further reading ASRM Guidelines Th e Practice Committee of the American Society for
Reproductive Medicine and the Practice Committee of the Society for Assisted Reproductive Technology
( 2008 ) Revised guidelines for human embryology and andrology laboratories . Fertility and Sterility 90 : S45 –59.
ESHRE Guidelines Magli MC , Van den Abbeel E , Lundin K , et al. ( 2008 )
Revised guidelines for good practice in IVF laboratories . Human Reproduction 23 (6): 1253 –1262.
Website information Association of Clinical Embryologists –
www.embryologists.org.uk COSHH – www.hse.gov.uk/coshh Department of Health – www.dh.gov.uk Th e Human Fertilisation and Embryology Authority –
www.hfea.gov.uk
Publications Almeida PA , Bolton VN ( 1996 ) Th e eff ect of temperature
fl uctuations on the cytoskeletal organisation and chromosomal constitution of the human oocyte . Zygote 3 : 357 –365.
Angell RR , Templeton AA , Aitken RJ ( 1986 ) Chromosome studies in human in vitro fertilisation Human Genetics 72 : 333 –339.
Ashwood-Smith MJ , Hollands P , Edwards RG ( 1989 ) Th e use of Albuminar (TM) as a medium supplement in clinical IVF . Human Reproduction 4 : 702 –705.
Bavister BD ( 1995 ) Culture of preimplantation embryos: facts and artifacts . Human Reproduction Update 1 (2): 91 –148.
Bavister BD , Andrews JC ( 1988 ) A rapid sperm motility bioassay procedure for quality control testing of water and culture media . Journal of In Vitro Fertilization and Embryo Transfer 5 : 67 –68.
Biggers JD , Summers MC ( 2008 ) Choosing a culture medium: making informed choices . Fertility and Sterility 90 (3): 473 –483.
Blechová R , Pivodová D ( 2001 ) LAL test – an alternative method of detection of bacterial endotoxins . Acta Veterinaria 70 : 291 –296.
Bongso A , Ng SC , Ratnam S ( 1990 ) Cocultures: their relevance to assisted reproduction . Human Reproduction 5 : 893 –900.
Boone WR , Johnson JE , Locke AJ , Crane MM , Price TM ( 1999 ) Control of air quality in an assisted reproductive technology laboratory . Fertility and Sterility 71 : 150 –154.
Campbell S , Swann HR , Aplin JD , et al. ( 1995 ) CD44 is expressed throughout pre-implantation human embryo development . Human Reproduction 10 : 425 –430.

Chapter 8: The clinical in-vitro fertilization laboratory
125
Cohen J , Gilligan A , Esposito W , Schimmel T , Dale B ( 1997 ) Ambient air and its potential eff ects on conception in vitro . Human Reproduction 12 (8): 1742 –1749.
Colls P , Goodall N , Zheng X , Munné S ( 2009 ) Increased effi ciency of preimplantation genetic diagnosis for aneuploidy by testing 12 chromosomes . Reproductive Biomedicine Online 19 (4): 532 –538.
Conaghan J ( 2008 ) Real-time pH profi ling of IVF culture medium using an incubator device with continuous monitoring . Journal of Clinical Embryology 11 (2): 25 –26.
Cutting R , Pritchard J , Clarke H , Martin K ( 2004 ) Establishing quality control in the new IVF laboratory . Human Fertility 7 (2): 119 –125.
Danforth RA , Piana SD , Smith M ( 1987 ) High purity water: an important component for success in in vitro fertilization . American Biotechnology Laboratory 5 : 58 –60.
Davidson A , Vermesh M , Lobo RA , Paulsen RJ ( 1988 ) Mouse embryo culture as quality control for human in vitro fertilisation: the one-cell versus two-cell model . Fertility and Sterility 49 : 516 –521.
Dumoulin JC , Land JA , Van Montfoort AP , et al. ( 2010 ) Eff ect of in vitro culture of human embryos on birthweight of newborns . Human Reproduction 25 (3): 605 –612.
Dumoulin JS , Menheere PP , Evers JL , et al. ( 1991 ) Th e eff ects of endotoxins on gametes and preimplantation embryos cultured in vitro . Human Reproduction 6 : 730 –734.
Edwards RG , Brody SA ( 1995 ) Human fertilization in the laboratory. In: Principles and Practice of Assisted Human Reproduction . Saunders , Philadelphia, PA , pp. 351–413.
Elder K , Elliott T ( 1998 ) Troubleshooting and problem solving in IVF. Worldwide Conferences on Reproductive Biology . Ladybrook Publishing , Australia .
Elliott T , Elder K (eds.) ( 1997 ) Blastocyst culture, transfer, and freezing. Worldwide Conferences on Reproductive Biology . Ladybrook Publishing , Australia .
Erbach GT , Bhatnagar P , Baltz JM , Biggers JD ( 1995 ) Zinc is a possible toxic contaminant of silicone oil in microdrop cultures of preimplantation mouse embryos . Human Reproduction 10 : 3248 –3254.
Fleetham J , Mahadevan MM ( 1988 ) Purifi cation of water for in vitro fertilization and embryo transfer . Journal of In Vitro Fertilization and Embryo Transfer 5 : 171 –174.
Fleming TP , Pratt HPM , Braude PR ( 1987 ) Th e use of mouse preimplantation embryos for quality control of culture reagents in human in vitro fertilisation programs: a cautionary note . Fertility and Sterility 47 : 858 –860.
Gardner D ( 1999 ) Development of new serum-free media for the culture and transfer of human blastocysts . Human Reproduction 13 (Suppl. 4): 218 –225.
George MA , Braude PR , Johnson MH , Sweetnam DG ( 1989 ) Quality control in the IVF laboratory: in vitro and in vivo development of mouse embryos is unaff ected by the quality of water used in culture media . Human Reproduction 4 : 826 –831.
Heo YS , Cabrera LM , Bormann CL , et al. ( 2010 ) Dynamic microfunnel culture enhances mouse embryo development and pregnancy rates . Human Reproduction 25 (3): 613 –622.
Johnson C , Hofmann G , Scott R ( 1994 ) Th e use of oil overlay for in vitro fertilisation and culture . Assisted Reproduction Review 4 : 198 –201.
Kane MT , Morgan PM , Coonan C ( 1997 ) Peptide growth factors and preimplantation development . Human Reproduction Update 3 (2): 137 –157.
Kattal N , Cohen J , Barmat L , et al . ( 2007 ) Role of co-culture in human IVF: a meta-analysis . Fertility and Sterility 86 (3): S225 –S226.
Kimber SJ , Sneddon SF , Bloor DJ , et al. ( 2008 ) Expression of genes involved in early cell fate decisions in human embryos and their regulation by growth factors . Reproduction 135 : 635 –647.
Korhonen K , Sjövall S , Viitanen J , et al. ( 2009 ) Viability of bovine embryos following exposure to the green fi ltered or wider bandwidth light during in vitro embryo production . Human Reproduction 24 : 308 –314.
Leese HJ , Donnay I , Th ompson JG ( 1998 ) Human assisted conception: a cautionary tale. Lessons from domestic animals . Human Reproduction 13 : 184 –202.
Ma S , Kalousek DK , Zouves C , Yuen BH , Gomel V , Moon YS ( 1990 ) Th e chromosomal complements of cleaved human embryos resulting from in vitro fertilisation . Journal of In Vitro Fertilization and Embryo Transfer 7 : 16 –21.
Marrs RP , Saito H , Yee B , Sato F , Brown J ( 1984 ) Eff ect of variation of in vitro culture techniques upon oocyte fertilization and embryo development in human in vitro fertilization procedures . Fertility and Sterility 41 : 519 –523.
Matson PL ( 1998 ) Internal and external quality assurance in the IVF laboratory . Human Reproduction Supplement 13 (Suppl. 4): 156 –165.
Matsuura K , Hayasahi N , Kuroda Y , et al. ( 2010 ) Improved development of mouse and human embryos using a tilting embryo culture system . Reproductive Biomedicine Online 20 (3): 358 –364.
Meintjes M , Chantilis SJ , Douglas JD , et al. ( 2009 ) A controlled, randomized trial evaluating the eff ect of lowered incubator oxygen tension on live births in a predominantly blastocyst transfer program . Human Reproduction 24 (2): 300 –307.
Ménézo Y ( 1976 ) Milieu synthétique pour la survie et la maturation des gametes et pour la culture de l’oeuf fécondé . Comptes Rendus de l’Academie des Sciences Paris, Serie D 282 : 1967 –1970.

Chapter 8: The clinical in-vitro fertilization laboratory
126
Munné S , Howles CM , Wells D ( 2009 ) Th e role of preimplantation genetic diagnosis in diagnosing embryo aneuploidy . Current Opinion in Obstetrics and Gynecology 21 (5): 442 –449.
Naaktgeboren N ( 1987 ) Quality control of culture media for in vitro fertilisation. In Vitro Fertilisation Program, Academic Hospital, Vrije Universiteit, Brussels, Belgium . Annales de Biologie Clinique (Paris) 45 : 368 –372.
Ottosen LD , Hindkjaer J , Ingerslev J ( 2007 ) Light exposure of the ovum and preimplantation embryo during ART procedures . Journal of Assisted Reproduction and Genetics 24 (2–3): 99 –103.
Pearson FC ( 1985 ) Pyrogens: Endotoxins, LAL Testing, and Depyrogenation . Marcel Dekker , New York , pp. 98–100, 206–211.
Pellestor F , Girardet A , Andreo B , Anal F , Humeau C ( 1994 ) Relationship between morphology and chromosomal constitution in human preimplantation embryos . Molecular Reproduction and Development 39 : 141 –146.
Pickering SJ , Braude PR , Johnson MH , Cant A , Currie J ( 1990 ) Transient cooling to room temperature can cause irreversible disruption of the meiotic spindle in the human oocyte . Fertility and Sterility 54 : 102 –108.
Plachot M , De Grouchy J , Montagut J , et al. ( 1987 ) Multicentric study of chromosome analysis in human oocytes and embryos in an IVF programme . Human Reproduction 2 : 29 .
Provo MC , Herr C ( 1998 ) Washed paraffi n oil becomes toxic to mouse embryos upon exposure to sunlight . Th eriogenology 49 (1): 214 .
Purdy J ( 1982 ) Methods for fertilization and embryo culture in vitro. In: Edwards RG , Purdy , JM (eds.) Human Conception In Vitro. Academic Press , London , p. 135.
Quinn P ( 1995 ) Enhanced results in mouse and human embryo culture using a modifi ed human tubal fl uid medium lacking glucose and phosphate . Journal of Assisted Reproduction and Genetics 12 : 97 –105.
Quinn P ( 2000 ) Review of media used in ART laboratories . Journal of Andrology 21 (5): 610 –615.
Quinn P , Warner GM , Klein JF , Kirby C ( 1985 ) Culture factors aff ecting the success rate of in vitro fertilization and embryo transfer . Annals of the New York Academy of Sciences 412 : 195 .
Richter KS ( 2008 ) Th e importance of growth factors for preimplantation embryo development and in-vitro culture . Current Opinion in Obstetrics and Gynecology 20 (3): 292 –304.
Rinehart JS , Bavister BD , Gerrity M ( 1988 ) Quality control in the in vitro fertilization laboratory: comparison of
bioassay systems for water quality . Journal of In Vitro Fertilization and Embryo Transfer 5 : 335 –342.
Rinehart J , Chapman C , McKiernan S , Bavister B ( 1998 ) A protein-free chemically defi ned embryo culture medium produces pregnancy rates similar to human tubal fl uid (HTF) supplemented with 10% synthetic serum substitute (SSS). Abstracts of the 14th Annual meeting of the ESHRE, Göteborg 1998 . Human Reproduction 13 : 59 .
Staessen C , Van den Abbeel E , Carle M , et al. ( 1990 ) Comparison between human serum and Albuminar-20(TM) supplement for in vitro fertilization . Human Reproduction 5 : 336 –341.
Summers MC , Biggers JD ( 2003 ) Chemically defi ned media and the culture of mammalian preimplantation embryos: historical perspective and current issues . Human Reproduction Update 9 (6): 557 –582.
Swain J , Pool TB , Takayama S , Smith GD ( 2008 ) Microfl uidic technology in ART: is it time to go with the fl ow? Journal of Clinical Embryology 11 (2): 5 –18.
Swain J , Pool TB , Takayama S , Smith GD ( 2009 ) Microfl uidics in ART. In: Gardner DK , et al . (eds.) Textbook of Assisted Reproductive Technologies , 3rd edn. Informa Healthcare , London .
Takenaka M , Horiuchi T , Yanagimachi R ( 2007 ) Eff ects of light on development of mammalian zygotes . Proceedings of the National Academy of Sciences of the USA 104 (36): 14289 –14293.
Th ompson JG , Gardner DK , Pugh A , MacMillan W , Teruit JJR ( 1995 ) Lamb birth weight is aff ected by culture system utilized during in vitro pre-elongation development of ovine embryos . Biology of Reproduction 53 : 1385 –1391.
Wales RG ( 1970 ) Eff ect of ions on the development of preimplantation mouse embryos in vitro . Australian Journal of Biological Sciences 23 : 421 –429.
Weimer KE , Anderson A , Stewart B ( 1998a ) Th e importance of water quality for media preparation . Human Reproduction Supplement 13 (Suppl. 4): 166 –172.
Weimer KE , Cohen J , Tucker MJ , Godke A ( 1998b ) Th e application of co-culture in assisted reproduction: 10 years of experience with human embryos . Human Reproduction Supplement 13 (Suppl. 4): 226 –238.
Yovich JL , Edirisinghe W , Yovich JM , Stanger J , Matson P ( 1988 ) Methods of water purifi cation for the preparation of culture media in an IVF-ET programme . Human Reproduction 3 : 245 –248.
Zorn TMT , Pinhal MAS , Nader HB , et al. ( 1995 ) Biosynthesis of glucosaminoglycans in the endometrium during the initial stages of pregnancy of the mouse . Cellular and Molecular Biology 41 : 97 –106.

Chapter
127
Quality management in the IVF laboratory
Th ere is no doubt that success in ART is crucially dependent on carefully controlled conditions in every aspect of the IVF laboratory routine ( Figure 9.1 ).
From the beginning of the twenty-fi rst century onwards, laboratories that off er human ART treatment or are involved in the handling of human gametes and/or tissue became subject to increasing demands and precepts set down by regulatory and legislative author-ities. Th e regulations diff er from country to country, and some directives (e.g., the European Tissue Directive 2004/23/EC-2006/86/EC) are subject to interpretation according to legislation or guidelines set down by national authorities in individual countries. In many countries, it has become necessary to obtain accredit-ation and/or certifi cation by a national or international body that will carry out in-depth assessments and inspections to ensure that all aspects of facilities and treatment meet a required standard.
ISO9001:2000 Th e International Organisation for Standardisation (ISO) ( www.iso.org ) is a network of the national standards institutes of 159 countries, consisting of one member per country; a Central Secretariat in Geneva, Switzerland, coordinates the system. Th e ISO is an independent body, not associated with the government of any particular country. Some of the 159 member institutes may be a part of their country’s government structure, but others have been set up by national part-nerships of industry associations, and therefore are in the private business domain. ISO therefore tries to reach a consensus on issues that concern both busi-ness requirements, and the broader needs of society. Th eir standard for quality management is published as ISO9001:2000.
In order to obtain ISO certifi cation, a unit with an established quality management system (QMS) is
assessed by an external auditor to evaluate the eff ect-iveness of the QMS. If all the requirements of the ISO standard are met, a certifi cate is issued stating that the QMS conforms to the standards laid down in ISO9001:2000. Many countries now require that IVF clinics and laboratories show evidence such as this, that an eff ective QMS is in place . ART laboratories in the USA should conform to the American Society for Reproductive Medicine guidelines (ASRM, 2008) and must undergo certifi cation and accreditation by an appropriate agency, such as the College of American Pathologists (CAP) or Joint Commission International (JCI). In the UK, all IVF clinics must apply for a license from the Human Fertilisation and Embryology Authority (HFEA) and ensure that all of their proce-dures are compliant with the HFEA Code of Practice . Th e HFEA monitors all UK data, and carries out annual audits and inspections.
Th e fi nal impact of legislative, regulatory, accredit-ation and certifi cation requirements is that every ART laboratory should have an eff ective total quality man-agement (TQM) system . TQM is a system that can monitor all procedures and components of the labora-tory; this must include not only pregnancy and implant-ation rates, but also a systematic check and survey of all laboratory material, supplies, equipment and instru-ments, procedures, protocols and staff performance.
Irrespective of the numerous fi ne details involved in TQM, the fi rst, and ultimate, test of quality control must rest with pregnancy and live birth rates per treat-ment cycle. An ongoing record of the results of fertil-ization, cleavage and embryo development provide the best short-term evidence of good quality control (QC). Daily records in the form of a laboratory logbook or electronic database are essential, summarizing details of patients and outcome of laboratory procedures: age, cause of infertility, stimulation protocol, number
9
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 9: Quality management in the IVF laboratory
128
of oocytes retrieved, semen analysis, sperm prepar-ation details, insemination time, fertilization, cleav-age, embryo transfer and cryopreservation. Details of media and oil batches and all consumables that come into contact with gametes and embryos must also be recorded for reference, and the introduction of any new methods or materials must be documented.
Defi nitions used in quality management
• Quality : fi tness for purpose . Quality management system : a system that encom-• passes quality control, quality assurance and quality improvement by providing defi ned sets of proce-dures for the management of each component. Quality policy : a statement defi ning the purpose of • the organization and its commitment to a defi ned quality objective. Quality control : inspection of a system to ensure • that a product or service is delivered under optimal conditions. Quality assurance : monitoring the eff ectiveness of • QC and indicating preventive and corrective action taken when errors are detected.
• Quality Audit : review and checking of the qual-ity management system to ensure its correct operation. External Quality Assurance: testing a product or ser-• vice against an external standard.
A QMS in the IVF laboratory aims to achieve spe-cifi c goals: 1. Identify all of the processes to be included in the
QMS: provision and management of resources • ART processes • evaluation and continual improvement • monitoring of key performance indicators • (KPIs)
2. Make available the resources and information necessary to operate and support these processes
3. Implement any actions necessary to ensure that the processes are eff ective and subject to continual improvement.
A QMS ensures continuous assessment and improvement of all component parts of the patient
• Quality : fi tness for purpose . Quality management system : a system that encom-•passes quality control, quality assurance and qualityimprovement by providing defi ned sets of proce-dures for the management of each component. Quality policy : a statement defi ning the purpose of •the organization and its commitment to a defi nedquality objective. Quality control : inspection of a system to ensure•that a product or service is delivered under optimalconditions. Quality assurance : monitoring the eff ectiveness of •QC and indicating preventive and corrective actiontaken when errors are detected.
• Quality Audit : review and checking of the qual-ity management system to ensure its correctoperation. External Quality Assurance: testing a product or ser-• vice against an external standard.
Stimulation
Laboratory Embryo transfer& luteal support
Air quality# of incubators # of embryologists& training level
Gas phase
Culture system
Culture media
Tissue culture ware/contact supplies
Oil overlay
# of embryos / drop
Impact on endometrialreceptivity
Oocytequality
QC & QA
OutcomePatient
Diet
Figure 9.1 Critical elements of an ART treatment cycle (with thanks to David Gardner, Melbourne, Australia).

Chapter 9: Quality management in the IVF laboratory
129
treatment cycle. KPIs to be monitored include rates of fertilization, cleavage, survival of injected oocytes, pregnancy, implantation and live births; patient sat-isfaction with the quality of the service should also be monitored. Graphic analysis of these parameters can reveal problems early so that corrective action can be taken promptly to minimize the extent of any problem that might arise (Kastrop, 2003 ).
Basic elements of a quality management system A formal QMS should include :
Scope: a list of all treatments provided and links to • the forms and documents used Normative reference values: defi nition of a • successful outcome Terms and defi nitions: those used in IVF • Management responsibility: organization chart • showing lines of responsibility and accountability of all staff Resource management: provision of suffi cient • resources, including staff , to deliver the service Product realization: treatment plans, procedures, • purchasing, traceability, witnessing Measurement, analysis, improvement: monitoring • of KPIs, reporting of adverse incidents, corrective and preventive action to improve service.
Implementing QMS in the IVF laboratory Th e fi rst key requirement for implementing a formal QMS is appropriately educated and trained personnel, with training records that are regularly updated. Other key requirements include: 1. Complete list/index of standard operating
procedures (SOPs) 2. Housekeeping procedures: cleaning and
decontamination 3. Correct operation, calibration and maintenance of
all instruments with manual and logbook records 4. Proper procedure, policy and safety manuals 5. Consistent and correct execution of appropriate
techniques and methods 6. Comprehensive documentation, record-keeping
and reporting of results 7. System for specimen collection and handling,
including verifi cation of patient identity and chain of custody
8. Safety procedures including appropriate handling and storage of materials
9. Infection control measures 10. Documentation of suppliers and dates of receipt
and expiry of consumables 11. System of performance appraisal, correction of
defi ciencies and implementation of advances and improvements
12. Quality materials, tested with bioassays when appropriate
13. Quality assurance program .
Laboratory equipment Equipment failure or suboptimal operation in an IVF laboratory can seriously jeopardize the prognosis for patients undergoing treatment, and therefore service contracts should be set up with reliable companies. As part of the service, the companies should be able to provide calibration certifi cates for the tools that they use in servicing and calibrating the equipment. Alarms should be fi tted to all vital equipment, and provision made for emergency call-out. Back-up equipment should be held in reserve.
Electrical appliances must be tested for safety before fi rst use (e.g., by portable appliance testing) and then regularly tested by a trained operator. Th ey should be designated as a potential source of fi re, and must not be used if faulty; any faults must be reported and repaired immediately. Contracts for service and calibration should be held for:
Incubators • Incubator alarms • Flow cabinets • Microscopes • Micromanipulator stations • Heated surfaces/microscope stages • Centrifuges • Refrigerators and freezers • Embryo/oocyte freezing machines • Osmometers • Liquid nitrogen storage dewars • Low-level nitrogen alarms in the dewars • Air fi ltration equipment • Electronic witnessing system . •
Key items of equipment in daily use also require systems of continuous monitoring to ensure optimal performance. Computer-controlled data acquisition

Chapter 9: Quality management in the IVF laboratory
130
and monitoring systems are now available, with con-tinuous monitoring and logging soft ware systems that support multiple instrument inputs ( Figure 9.2 , Facilities Monitoring Systems, www.fmonsys.com/ ). Th is system can continuously check and record air-borne particle counts, as well as data from key equip-ment such as incubators, freezers, refrigerators and liquid nitrogen storage vessels. Th e data is monitored in real-time, and the computerized system can dis-play historical data acquisition and analysis, trend-lines, correlation studies and various levels of alarm notifi cation. Variation outside set parameters is cov-ered by an alarm system that is monitored 24 hours a day .
Temperature and pH are known to be critical parameters that must be carefully controlled, and their
measurement in an IVF culture system requires special attention:
Temperature Th e temperature of incubators, water baths, heating blocks, heated surfaces and microscope stages should not rely on a digital display from the equipment, but must be independently recorded and controlled, with individ-ual fi ne tuning for each. Always note that the tempera-ture of the incubator, bath or surface will diff er from that in the culture media within a drop, tube or dish; 37°C should be the temperature to aim for within the media, not for the incubator or heating device. Setpoints should be defi ned for each dish on each separate device, using a calibrated thermometer with type K thermocouple.
Figure 9.2 Data from FMS in the IVF laboratory at Bourn Hall Clinic. The background shows the diff erent monitoring modules that can be viewed: CO
2 sensors, HEPA sensors, incubator temperature, refrigerators, freezers. Insets: 24-hour records from a single incubator showing
(a) CO 2 concentration and (b) temperature. Note dips during peak laboratory activity times, 8–10.30 am. See color plate section.

Chapter 9: Quality management in the IVF laboratory
131
pH An “optimal” pH for in-vitro culture has not been pre-cisely defi ned or characterized, and according to the manufacturers’ information, the range of acceptable pH diff ers with media type, since the hydrogen ion concentration is determined by the overall compos-ition, including concentrations of amino acids and protein supplement. Diff erent media companies advise that incubators are run at diff erent CO 2 concentrations in order to optimize the pH for their media .
pH is a number that refl ects dynamic culture con-ditions – it changes rapidly if acid/base concentrations change. Although it is a critical parameter, in practice it is not easy to monitor eff ectively, especially in micro-drop culture under oil. A standard glass probe pH meter is fragile, requires a volume of at least 1 mL that needs to be equilibrated (cannot be used for microdrops), is not standardized, and therefore readings taken do not represent actual culture conditions. A number of alter-native devices are available for use in IVF culture sys-tems, but none provide an ideal solution to the problem of pH monitoring, and the diff erent devices can yield diff erent results when used to test a variety of diff erent media and solutions. Th erefore, whatever device is used, careful validation and calibration is essential; it is unwise
Figure 9.2 (cont.)
Media pH range
P1 7.1–7.3
Quinn’s Advantage 7.1–7.3
Basal XI 7.2–7.35
Global 7.25–7.3
G1.3 7.30 ± 0.10
IVF 500 7.35 ± 0.10
HTF 7.40 ± 0.10
Medicult None specifi ed; “pH tested”

Chapter 9: Quality management in the IVF laboratory
132
to rely on only one method. Although pH measurement is important, and is useful in monitoring manipulation and handling procedures, a change in pH refl ecting CO 2 concentration takes time, and depends upon the volume and the culture system being used. Please refer to Pool ( 2004 ) for a comprehensive review of the science behind culture media pH, and its importance in human IVF .
Devices used to monitor pH in culture media
1. ISFET (ion sensitive fi eld eff ect transistor) probes: Can be used in small volumes outside the incuba-• tor, is simple and fast. Requires frequent calibration and cleaning (sen-• sitive to protein deposits), expensive.
2. RI pH meter : Can be used for measurements inside the incuba-• tor, but not for microdrop culture. Slow, drifts over time, and calibration is diffi cult/• time consuming.
3. MTG pH meter : pH Online TM , “fl uorescent decay time” pH meter:
Allows continuous pH measurement inside the • incubator; can be used to monitor pH in up to 10 incubators simultaneously . Requires disposable four-well Nunc dish, with one • well fi tted with a pH reactive fl uorochrome spot. Simple to use, but expensive and slow. •
4. Blood gas analyzer: Accurate, but not suitable for microdrops. • Method of choice for initial media pH testing. • Sampling errors can be a problem . •
5. Beckmann pH meter: Can be used to measure pH in 5 mL aliquots of • media after overnight incubation in test-tubes with loose-fi tting caps (see Pool, 2004 ). Electrode selection, cleaning and regular replace-• ment is important. Must be correctly calibrated before each use. •
Incubator CO 2
In contrast to pH measurements, a properly calibrated device can measure CO 2 and provide fast and repro-ducible results, as well as detect rapid changes in gas concentration: very important in case of incubator malfunction. Th e “standard” Fyrite kit for measur-ing CO 2 is inaccurate, and Fyrite is toxic – these kits should not be used in the IVF laboratory. Infrared gas analyzers (Hereaus/Th ermo/Bacharach, K-Systems, Vaisala) are available that can provide accurate meas-urements of gas concentrations. Th e devices must be calibrated with a reference gas, and should be used at least once per week to measure actual incubator CO 2
with reference to the digital display. Incubator gases can also be monitored with independent probes as part of a facilities monitoring system.
Equipment monitoring for QMS 1. Incubators
Independent readings of temperature and • gases; calibrated thermometer inside the incubator as standard. Monitor CO • 2 supply cylinders regularly; ensure that autochangers are functional. For humidifi ed incubators, check water levels • daily. Each incubator should have a 24-hour • surveillance system, with alarms accessible to staff when at home or at work. A back-up secondary power source should • be installed, and a contingency plan made available to all laboratory staff with back-up arrangements clearly outlined in writing.
2. Heated surfaces and water baths Record the temperature of water baths daily, • using a calibrated thermometer in a tube of water. Use a thermocouple to record the temperature • of heated surfaces of fl ow cabinets and the temperature of media drops in culture dishes (the temperature of the surface usually diff ers from the temperature of media in the culture dish). Defi ne acceptable limits of maxima and • minima, and record action taken when these are exceeded .
3. Refrigerators and freezers Record temperatures daily, using calibrated • thermometers. Defi ne acceptable limits of maximum and • minimum temperatures, and record any action taken when these are exceeded.
4. Liquid nitrogen dewars Should always have an alarm to indicate low • nitrogen levels (or increasing temperature, or both). Top up nitrogen levels at least once per week • (be careful not to overfi ll, as liquid nitrogen pouring over the top can damage the seal at the neck). Monitor weekly nitrogen usage by recording •
1. ISFET (ion sensitive fi eld eff ect transistor) probes: Can be used in small volumes outside the incuba-•tor, is simple and fast. Requires frequent calibration and cleaning (sen-•sitive to protein deposits), expensive.
2. RI pH meter : Can be used for measurements inside the incuba-• tor, but not for microdrop culture. Slow, drifts over time, and calibration is diffi cult/• time consuming.
3. MTG pH meter : pH OnlineTM, “fl uorescent decaytime” pH meter:
Allows continuous pH measurement inside the• incubator; can be used to monitor pH in up to 10incubators simultaneously . Requires disposable four-well Nunc dish, with one• well fi tted with a pH reactive fl uorochrome spot. Simple to use, but expensive and slow.•
4. Blood gas analyzer: Accurate, but not suitable for microdrops. • Method of choice for initial media pH testing. • Sampling errors can be a problem . •
5. Beckmann pH meter: Can be used to measure pH in 5 mL aliquots of •media after overnight incubation in test-tubeswith loose-fi tting caps (see Pool, 2004 ). Electrode selection, cleaning and regular replace-•ment is important. Must be correctly calibrated before each use. •

Chapter 9: Quality management in the IVF laboratory
133
the liquid N 2 level before top-up, and plot the readings on a graph in order to detect any gradual increase in usage, indicating a slow vacuum leak.
Records of all readings should be kept and can be plotted on a graph, with acceptable limits and any cor-rective action noted on the records. A graph provides a useful means of quickly monitoring and analyzing results visually : 1. Dispersion: increased frequency of both high and
low numbers 2. Trend: progressive drift (in one direction) from a
mean 3. Shift : abrupt change from the mean.
Bioassays Guidelines issued by ESHRE (2008), the HFEA (2008), ASRM (2008) and the Association of Clinical Embryologists (ACE) in the UK, state that all tissue cul-ture media prepared in the laboratory should undergo quality control testing with an appropriate bioassay system. A range of bioassays to detect toxicity and sub-optimal culture conditions have been tried, including: 1. Human or hamster sperm survival (Critchlow
et al ., 1989 ; Nijs et al ., 2009 ) 2. Continued culture of multipronucleate embryos 3. Somatic cell lines: LAL test for endotoxins
(Blechová and Pivodová, 2001 ), HeLa – test for cytotoxins (Painter, 1978 )
4. Culture of mouse embryos from either the one-cell or two-cell stage.
Th e validity of a mouse embryo bioassay has been questioned as a reliable assay for extrapolation to clin-ical IVF: it assumes that the requirements of human and mouse embryos are the same, and we know that this is a false assumption. Th e mouse embryo cannot regulate its endogenous metabolic pool before the late two-cell stage; this is not the case for human or bovine embryos. Mouse embryos will develop from the two-cell stage onwards in a wide variety of cell culture media .
Although none of the systems currently available can guarantee the detection of subtle levels of tox-icity, they can be helpful in providing baseline data for comparative purposes, and for identifying spe-cifi c problems. Any bioassay done routinely and fre-quently with baseline data for comparing deviations from the norm will be helpful in minimizing the ran-dom introduction of contaminants into the system,
and is a useful investment of time and resources in an IVF laboratory.
New batches of media, oil, material or supplies used in the culture system, if not pretested, should be tested before use. Th e physico-chemical limits of culture media testing are crucial: osmolarity must be within the limits of 275-305 mOsm, with a total variation of no more than 30 mOsm. pH must be within the limits of 7.2–7.5, with a maximal variation of 0.4 units of pH. Larger variations in either parameter indicate poor technique/technology and inadequate controls during manufacture, leading to poor reproducibility.
Tissue culture plastics have on occasion been found to be subject to variation in quality: well–well variations have been observed even within a single four-well plate, and rinsing plates with media before use may be a useful precaution. Studies have shown that oil can interact with diff erent plastic supports, and this can aff ect embryo development. Manufacturers of plasticware used for tissue culture may change the chemical formulation of their products without noti-fi cation, and such changes in manufacture of syringes, fi lters and culture dishes may sometimes be embryo-toxic. It is also important to store plasticware at an ambient room temperature, away from direct sun-light, as this can aff ect the properties of the plastic.
Embryos are very sensitive quality control indi-cators: in routine IVF culture a normal fertilization rate in the order of >70% and cleavage rate of >95% is expected. Th e cleavage rate is important, as a block at the two-pronucleate stage indicates a serious prob-lem. At least 65% of inseminated oocytes should result in cleaved embryos on Day 2. Th e appearance of the blastomeres and the presence of fragmentation are also good indicators: blastomeres in the early human embryo should be bright and clear, without granules in the cytoplasm. During cell division, the nucleo- cytoplasmic ratio is important, and this can be aff ected by culture medium osmolarity; in the presence of low osmolarity, the size of the embryo increases relative to the volume of the cytoplasm, and cytoplasmic blebs are formed to compensate; in order to achieve an adequate nuclear/cytoplasmic ratio for entry into mitosis. However, in forming blebs, the embryo loses not only cytoplasm but also mRNA and proteins, which are necessary for further development .
Any trend or shift in data should be investi-gated, with consideration of patient age and activity level: batches of materials (plasticware and media), air quality, temperature/CO 2 levels in incubators and

Chapter 9: Quality management in the IVF laboratory
134
fl ow cabinets, water quality, oil and gloves should all be investigated.
Useful routine QC procedures Sperm survival test Th e test should be performed in protein-free media, since protein may act as a buff er for potential toxicity. Select a normal sample of washed prepared spermatozoa and assess for count, motility and progression. Divide the selected sample into four aliquots: add test mater-ial to two aliquots, and equivalent control material (in current use) to the remaining two aliquots. Incubate one control and one test sample at 37°C, and one of each at room temperature. Assess each sample for count, motil-ity and progression aft er 24 and 48 hours (a computer-aided system can be used if available). Test and control samples should show equivalent survival. If there is any doubt, repeat the test.
Culture of surplus oocytes Surplus oocytes from patients who have large numbers of oocytes retrieved, may be used to test new culture material. Culture at least six embryos in the control media, and a maximum of four in test media .
Multipronucleate embryo culture Oocytes that show abnormal fertilization on Day 1 aft er insemination can be used for testing new batches of material. Observe, score and assess each embryo daily until Day 6 aft er insemination.
Culture of surplus embryos Surplus embryos aft er embryo transfer that are not suit-able for freezing have also been used for testing new cul-ture material, but this practice is not allowed under an HFEA treatment license in the UK: “An embryo may not be kept under a treatment license if it is no longer to be used in the treatment of a woman, or if any information that may be obtained from keeping it will not be of spe-cifi c use in the treatment or diagnosis of the individuals whose gametes were used to produce it. If there is some specifi c value for a couple in continuing to culture spare embryos from a particular treatment cycle, this should be done with the knowledge and agreement of the couple concerned” (HFEA Code of Practice, Ch(94)09) . Th e HFEA Act as amended in 2009 does now allow surplus embryos to be used for training purposes, provided that written patient consent is obtained.
Key points in the use of bioassays
• Choice of bioassay Selection of materials to test • Frequency of testing • Establish a set of standards, routine and schedule • Establish acceptable performance range • Document all results • Review results regularly • Do not use anything that fails the bioassay • Write a standard operating procedure for any cor-• rective action required.
Risk assessments and standard operating procedures Th e standard IVF unit has many areas of risk which should be assessed:
Transport and storage of liquid nitrogen and • compressed gases (e.g., transport of liquid nitrogen in elevators requires the dewar to be transported on its own, with “hazard” signs on all fl oors in between, to prevent the elevator from being used by anyone else) Fire • Infection (bacterial, viral) in theater, scan rooms, • laboratories, treatment rooms, consultation rooms, waiting area Staff health and safety in all clinical areas and • during all clinical activities Patient health and safety during all procedures • including diagnostic Patient confi dentiality • Equipment: use, maintenance, assessment, • emergency cover Regulatory restrictions for: •
confi dentiality of patients • security and confi dentiality of current and • archived patient records storage and confi dentiality of data • audit •
IT support • Security of laboratory stores • Witnessing (a risk assessment is needed when • introducing electronic witnessing systems to ensure they are as eff ective).
Standard operating procedures (SOPs) must be listed on a regularly updated document, and be avail-able to all laboratory personnel. Each SOP should exist
• Choice of bioassay Selection of materials to test• Frequency of testing• Establish a set of standards, routine and schedule • Establish acceptable performance range • Document all results• Review results regularly • Do not use anything that fails the bioassay • Write a standard operating procedure for any cor-•rective action required.

Chapter 9: Quality management in the IVF laboratory
135
in only one version, with version number, date and author, and must be updated at least annually, or when any changes are made. Th ey should refer to all associ-ated documentation including patient consent, be part of a document control system, and be archived and no longer available when new version created.
Th e SOPs should describe in detail: Th e procedures used • Th e expected end product • All equipment and reagents required for each • procedure.
Th ey should also include: Information on health and safety and infection • control SOPs for: •
housekeeping, cleaning and decontamination • patient identifi cation, chain of custody and • witnessing of all procedures storage and audit of cryopreserved material •
Validation evidence of the procedure described. •
Key points of a QMS
• Review and update all processes regularly . Ensure traceability by recording batch numbers and • expiry dates of all consumables, including plastics and culture media. Monitor and service equipment frequently, keeping • detailed records. Monitor KPIs to check laboratory performance. •
Basic housekeeping procedures in the IVF laboratory Daily cleaning routine During the course of procedures any spillage should be immediately cleaned with damp tissue and the use of an appropriate disinfectant (e.g., Trigene wipes). No detergent or alcohol should be used whilst oocytes/embryos are being handled. Should it be necessary to use either of the above, allow residual traces to evapor-ate for a at least 20 minutes before removing oocytes/embryos from incubators.
At the end of each day : 1. Heat seal, double bag, and dispose of all waste
from procedures 2. Remove all pipette holders for washing and
sterilizing before reuse
3. Reseal and resterilize pipette canisters 4. Clean fl ow hoods, work benches, and all
equipment by washing with a solution of distilled water and 7X laboratory detergent (Flow Laboratories), followed by wiping with 70% denatured alcohol or specifi c detergent sprays developed for IVF laboratories such as Oosafe ( www.parallabls.com ), or Fertisafe
5. Prepare each workstation for the following day’s work, with clean rubbish bags, pipette holder and Pasteur pipettes.
Washing procedures If the laboratory has a system for preparation of ultrapure water, particular attention must be paid to instructions for maintenance and chemical cleaning. Water purity is essential for washing procedures, and the system should be periodically checked for organic contamination and endotoxins.
Pipettes Pre-washed and sterilized pipettes are available, but the following procedure can be used if necessary: 1. Soak new pipettes overnight in fresh Analar or
Milli-Q water, ensuring that they are completely covered
2. Drain the pipettes and rinse with fresh water 3. Drain again and dry at 100°C for 1–2 hours 4. Place in a clean pipette canister (tips forward), and
dry heat sterilize for 3 hours at 180°C 5. Aft er cooling, record date and use within 1 month
of sterilization.
Nondisposable items (glassware, etc.): handle with nonpowdered gloves, rinsed in purifi ed water 1. Soak in distilled water containing 3–5% 7X (Flow
Laboratories) 2. Sonicate small items for 5–10 minutes in an
ultrasonic cleaning bath 3. Rinse eight times with distilled water, then twice
with Analar or Milli-Q water 4. Dry, seal in aluminum foil or double wrap in
autoclave bags as appropriate 5. Autoclave, or dry heat sterilize at 180°C for 3
hours
• Review and update all processes regularly . Ensure traceability by recording batch numbers and •expiry dates of all consumables, including plastics and culture media. Monitor and service equipment frequently, keeping •detailed records. Monitor KPIs to check laboratory performance.•

Chapter 9: Quality management in the IVF laboratory
136
6. Record date of sterilization, and store in a clean, dust-free area.
Incubator maintenance Schedule for cleaning should be based on : •
External environment (climate: humid or dry?) How oft en the incubator is used Type of incubator Where it is housed (clean room, hospital room?)
Follow manufacturer’s instructions for the • particular incubator regarding cleaning agents (hydrogen peroxide can normally be used, followed by rinsing with distilled water) Fungal contamination in a humidifi ed incubator • can be avoided by placing a piece of autoclaved copper in the water pan.
Microbiological testing and contamination in the laboratory Th e risk of introducing infection into the laboratory can be minimized by screening patients for infectious agents where indicated by medical history and physical examination. Th e risk of infectious agent transmission in ART procedures varies in diff erent populations and geographical regions; a risk assessment should be car-ried out according to the prevalence of disease in the specifi c patient population, bearing in mind the possi-bility of “silent” infection prior to detectable serocon-version. National and international guidelines in many countries now recommend that patients attending for ART procedures should undergo routine testing for HIV 1 and 2, hepatitis B and C at least annually; in some cases, viral screening for both partners prior to each cycle is mandatory. Human T-cell lympho-tropic virus (HTLV I and II) has a low prevalence in Western countries, but HTLV I is principally endemic in Japan, Central Africa, the Caribbean and Malaysia, and HTLV II is prevalent in Central America and the southern USA. Screening for these viruses prior to blood or organ donation is now mandatory in some countries; guidelines for HTLV I and II patient screen-ing prior to ART procedures should be adapted to local regulations and epidemiology. Routine screening for genital infections, i.e., syphilis, gonorrhea, chlamydia, cytomegalovirus, herpes simplex, human papilloma virus and vaginal infections, should be assessed within the context of patient population, prevalence of disease and full medical history/physical examination of both
partners (e.g., malaria, sickle cell disease, Trypanosoma cruzi ). For syphilis testing, a validated testing algo-rithm must be applied to exclude the presence of active infection with Treponema pallidum .
Eff ective handling, cleaning and maintenance schedules, together with strict adherence to aseptic technique should make routine microbiological test-ing unnecessary, but it may be required in order to identify a source of contamination in a culture system. It is required as part of some of the ISO 9000 series quality management protocols and is recommended by the UK Department of Health for laboratories that off er tissue banking facilities, including ovarian and testicular tissue .
Culture systems should be under constant vigilance to detect early signs of possible microbial contamin-ation, in order to avert serious subsequent problems. Any turbidity or drastic color change in media is a clear refl ection of contamination, and an inseminated cul-ture dish that shows all sperm dead or immotile should prompt further investigation for possible microbial contamination. A practical and simple method that can be used for checking bacterial and fungal contam-ination in the incubator or culture medium is to leave an aliquot of culture medium without an oil overlay in the incubator for 5 days. Organisms contaminating the medium or the incubator that are a hazard under IVF culture conditions will multiply in this optimal growth environment of nutrients, temperature, pH and humidity. Th e aliquot can then be checked for con-tamination by looking for turbidity and change in color (if medium with a pH indicator is used), and stained for microscopic observation of bacteria or fungi. Th is test can be used as an ongoing procedure for sterility testing of the incubator as well as the culture medium .
Methods used for microbiological testing of the environment include air sampling, settle plates, con-tact plates and glove print tests. Although air sampling by either settle plates or Anderson air fi ltration systems are rarely indicated in an ART laboratory, except in evaluating an episode of contamination or outbreak, specifi c air quality testing is now a requirement under the European Tissue Directive. Table 9.1 shows average values used for guidance in defi ning acceptable limits for viable particle detection (microbiological contam-ination) in monitoring areas of diff erent air quality.
Routine culture of bacteria or fungal spores is expected in most environments, and does not refl ect the environment in the sterile hood where procedures are performed. Settle plates are noninhibitory culture

Chapter 9: Quality management in the IVF laboratory
137
media plates that are left out on a work surface so that bacteria and mold spores can settle out of the air onto the plate. Th is method represents an unconcentrated air volume assessment, and the procedure used should spe-cify the length of time of exposure for the plate (1 hour vs. 12 or 24 hours). Air fi lters such as the Anderson air fi lter apparatus actively collect (suck in) air through a fi l-ter. Th e fi lter is then placed on a culture medium to allow bacterial and fungal growth. Using this technique, the number of cubic feet of air to be processed must be spe-cifi ed; it is used mainly in clinical transplant areas (e.g., bone marrow transplant). Isolation of spores is expected and usually does not correlate with patient disease .
Fungal contamination in the laboratory Th e ability of fungi to form spores that can survive in a wide range of physical extremes makes them a continuous source of potential contamination, and a laboratory that is not kept strictly and rigorously clean at all times provides an ideal environment for them to thrive. Fungal spores may be introduced from the environment, or from central heating/air condition-ing systems, and can grow in incubators, water baths, sinks, refrigerators and on walls and surfaces that escape regular thorough cleaning. Th ey thrive in a moist environment where there is a substrate, such as air fi lters, heat exchangers, humidifi ers, water pumps, cooling units, wet carpet, ceiling tiles, condensation on windows – even indoor plants. In most cases, a thor-ough routine of regular cleaning together with com-prehensive visual inspection should eliminate fungal contamination in the laboratory.
Contamination in an incubator is usually detected when the same fungus grows in multiple culture dishes. In this case, the incubator must be decontami-nated according to the manufacturer’s instructions: each manufacturer has specifi cations about safe and
appropriate decontamination procedures. Th e use of qua-ternary ammonium compounds, chlorine and alcohol solutions must be dictated by the reactivity of these com-pounds with the components of the incubator. Following decontamination, the incubators must be wiped down with sterile water to remove any residual cleaning solu-tion that might volatize and contaminate the cultures. Full decontamination procedures should be carried out during laboratory “down” periods, when no embryos are being cultured. Decontamination should include all surfaces, the water pan and the fan blades (which are very effi cient at dispersing spores). Occasionally decontam-ination may fail – some institutions have been forced to replace the incubators. Many incubators now incorporate an in-built sterilizing cycle to assist in regular decontam-ination (Th ermo, Forma, Steri-Cycle™).
Further reading Books Elder KT , Baker D , Ribes J ( 2005 ) Infections, Infertility and
Assisted Reproduction . Cambridge University Press , Cambridge .
Keel BA , May JV , De Jonge , CJ (eds.) ( 2000 ) Handbook of the Assisted Reproduction Laboratory . CRC Press , Boca Raton, FL .
Mortimer D , Mortimer S ( 2007 ) Quality and Risk Management in the IVF Laboratory . Cambridge University Press , Cambridge .
Useful websites Association of Clinical Embryologists –
www.embryologists.org.uk College of American Pathologists, Accreditation and
Laboratory Improvement – www.cap.org/apps/cap.portal?_nfpb=true&_pageLabel=accreditation
COSHH – www.hse.gov.uk/coshh Health and Safety – www.hse.gov.uk
Table 9.1 Average values for limits of microbial detection in areas of defi ned air quality
GradeAir sample (CFU/m 3 )
Settle plates (90 mm diameter) (CFU/4 hours)
Contact plates (55 mm diameter) (CFU/plate)
Glove print (5 fi ngers) (CFU/glove)
A <3 <3 <3 <3
B 10 5 5 5
C 100 50 25 –
D 200 100 50 –
CFU, colony forming units.

Chapter 9: Quality management in the IVF laboratory
138
Human Fertilisation and Embryology Authority – www.hfea.gov.uk
International Organisation for Standardisation (ISO) – www.iso.org
Joint Commission International (JCI) – www.jointcommissioninternational.org/
Department of Health – www.dh.gov.uk
ASRM Guidelines Th e Practice Committee of the American Society for
Reproductive Medicine and the Practice Committee of the Society for Assisted Reproductive Technology ( 2008 ) Revised guidelines for human embryology and andrology laboratories . Fertility and Sterility 90 : S45 –59.
ESHRE Guidelines Magli MC , Van den Abbeel E , Lundin K , et al. ( 2008 )
Revised guidelines for good practice in IVF laboratories . Human Reproduction 23 (6): 1253 –1262.
Publications Blechová R , Pivodová , D ( 2001 ) LAL test – an alternative
method of detection of bacterial endotoxins . Acta Veterinaria 70 : 291 –296.
Carson B , Alper M , Keck C ( 2005 ) Quality Management Systems for Assisted Reproductive Technology ISO 9001: 2000. Taylor & Francis, London.
Cohen J , Gilligan A , Esposito W , Schimmel T , Dale B ( 1997 ) Ambient air and its potential eff ects on conception in vitro . Human Reproduction 12 : 1742 –1749.
Critchlow JD , Matson PL , Newman MC , et al. ( 1989 ) Quality control in an in vitro fertilisation laboratory: use of human sperm survival studies . Human Reproduction 4 : 545 –549.
Cutting R , Pritchard J , Clarke H , Martin K ( 2004 ) Establishing quality control in the new IVF laboratory . Human Fertility 7 (2): 119 –125.
Gilling-Smith C , Emiliani S , Almeida P , Liesnard C , Englert Y ( 2005 ) Laboratory safety during assisted reproduction in patients with blood-borne viruses . Human Reproduction 20 : 1433 –1438.
Kastrop PM ( 2003 ) Quality management in the ART laboratory . Reproductive Biomedicine Online 7 (6): 691 –694.
Meintjes M , Chantilis SJ , Douglas JD , et al. ( 2009 ) A controlled, randomized trial evaluating the eff ect of lowered incubator oxygen tension on live births in a predominantly blastocyst transfer program . Human Reproduction 24 (2): 300 –307.
Nijs M , Franssen K , Cox A , et al. ( 2009 ) Reprotoxicity of intrauterine insemination and in vitro fertilization-embryo transfer disposables and products: a 4-year survey . Fertility and Sterility 92 (2): 527 –535.
Painter RB ( 1978 ) DNA synthesis inhibition in HeLa cells as a simple test for agents that damage human DNA . Journal of Environmental Pathology and Toxicology 2 (1): 65 –78.
Phillips KP , Leveille MC , Klaman P , Baltz JM ( 2000 ) Intracellular pH regulation in preimplantation embryos . Human Reproduction 15 : 896 –904.
Pool T ( 2004 ) Optimising pH in clinical embryology . Clinical Embryologist 7 (3): 1 –17.
Rinehart JS , Bavister BD , Gerrity M ( 1988 ) Quality control in the in vitro fertilization laboratory: comparison of bioassay systems for water quality . Journal of In Vitro Fertilization and Embryo Transfer 5 : 335 –425.
Tedder RS , Zuckerman MA , Goldstone AH , et al. ( 1995 ) Hepatitis B transmission from contaminated cryopreservation tank . Lancet 346 : 137 –140.
Tomlinson M ( 2005 ) Managing risks associated with cryopreservation . Human Reproduction 20 : 1433 –1438.

Chapter
139
Sperm and ART
Introduction At least 50% of couples referred for infertility investi-gation and treatment are found to have a contributing male factor. Male factor infertility can represent a var-iety of defects, which result in abnormal sperm number, morphology or function. Detailed analysis of sperm assessment and function are important for accurate diagnosis, and are described in detail in numerous textbooks of practical andrology and semen analysis. A comprehensive review of semen analysis is beyond the scope of this book, and only details relevant to assisted conception treatment will be described here.
Th e World Health Organization (WHO) labora-tory manual (2010) describes standard conditions for the collection of semen samples, their delivery and the standardization of laboratory assessment proce-dures. Th is manual represents a major revision over the previous (WHO, 1999) edition and includes new “Reference Values” to allow decisions to be made about patient management, and proposes that the 5th centile of a population of men, whose partners con-ceived within 12 months of stopping contraceptive use, potentially defi nes “normal” from “abnormal.” Th erefore the lower reference limits (5th centile and 95% confi dence intervals) are 15 × 10 6 /mL (12–16) for concentration, 32% (31–34) for good forward pro-gressive movement within 60 minutes of ejaculation and 4% (3–4) for normal morphology (see WHO man-ual 2010 ; Appendix A1.1). Th e introduction of exter-nal quality control and quality assurance schemes in semen assessment have highlighted the fact that accur-ate analysis of seminal fl uid is notoriously diffi cult to standardize, with many technical variables, and the quality of semen analysis in diff erent laboratories can be highly variable (Matson, 1995 ). Th is implies that diagnosis and treatment modality chosen for a patient could diff er according to the laboratory carrying out
the assessment. Without good semen analysis data, patients may be off ered inappropriate treatments or no treatment at all; it is essential that an assisted repro-ductive service should ensure that laboratory person-nel are adequately and correctly trained in basic semen assessment techniques according to WHO guidelines. Even the most confi dent of laboratories should have a discipline of monitored standards. Th e routine appli-cation of intracytoplasmic sperm injection (ICSI) provides eff ective treatment for even the most severe cases of male infertility which were previously felt to be beyond hope, and the fact that fertilization can be achieved from semen with “hopeless” sperm param-eters has forced a review of standard semen analysis and sperm function testing. Th is chapter will address only the basic principles required in the practical fea-tures of sperm preparation procedures for assisted conception techniques.
Semen assessment Sample collection and handling (a) Record information – prior to sample production
the patient should be asked to confi rm their personal details and if necessary provide suitable identifi cation. Th ey should be asked when they last ejaculated, and for a history of recent illness, medication taken, smoking and alcohol consumption; this information should be noted on the fi nal report form. Once the sample has been produced the patient should sign a consent form agreeing to the use of that sample for analysis or treatment.
(b) Provide adequate instructions – the patient should be given written instructions about the process involved, including precise details about the location and time that their sample will be
10
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. (©) K. Elder and B. Dale 2011.

Chapter 10: Sperm and ART
140
required. Th ey should be informed of the need to abstain from sexual intercourse or masturbation for between 3 and 5 days before their sample is to be produced. Care should be taken over language diffi culties and for patients with special needs.
(c) Methods of sample production – the sample should ideally be produced by masturbation aft er the required period of abstinence. However, it is acknowledged that this is not possible for all patients. A small number of men can only produce a sample at intercourse and in these cases they should be provided with a silastic (nonspermicidal) condom. No other condoms are permissible. Samples produced by coitus interruptus without a condom should not be accepted for analysis.
(d) Location of production – whenever possible all samples for analysis or treatment should be produced on site. It is unacceptable to ask a patient to produce a sample in a lavatory, and there should be a special room set aside for this purpose. Where it is not possible to produce a sample on site, a sample produced at home should be brought to the laboratory within one hour.
(e) Specimen container – samples should be collected into a pre-weighed wide-necked plastic or glass container. All specimen containers should be cytotoxically tested as some plastics are detrimental to sperm motility (see Box 2.1 of WHO, 2010, for details). Samples previously assessed as having high viscosity benefi t from collection into pots containing 1 mL of medium. Prior to production the patient should be asked to pass urine and then rinse his hands and penis.
(f) Treatment of samples post-production – once produced, the patient and a member of staff should check that the sample container is identifi ed with the patient’s name or identifi cation number, and the time of sample production. Th e samples should be placed in an incubator at 37°C for up to one hour to allow liquefaction.
Macroscopic evaluation Once the process of liquefaction has occurred (usually within 30–60 minutes of ejaculation), the sample should be examined macroscopically, with evaluation of :
• Appearance and consistency – semen should be a grayish opalescent liquid with a neutral odor. Any unpleasant smell or discoloration (e.g., contains
blood), or the presence of mucus or jelly should be reported. • Liquefaction and viscosity – although semen is ejaculated as a coagulum, it should liquefy within 30 minutes. If a sample fails to liquefy or is highly viscous aft er liquefaction this should be noted. • Volume – measured by weighing the container in which the specimen was ejaculated and subtracting the full weight from the empty weight. Th e volume can be inferred from the weight assuming the density of semen to be 1 g/mL. Th e use of volumetric methods to measure semen volume is no longer recommended. • pH – the most convenient way to measure the pH of a sample is to use pH paper.
Macroscopic anomalies can provide import-ant information about the patient and should not be ignored. For example, a low pH can indicate infection of the genital tract, and a low volume could suggest a retrograde ejaculation, a leakage from the sample con-tainer, or that the patient failed to collect the entire sample he produced .
Sperm motility Since sperm motility decreases with increasing expos-ure to seminal plasma, this should be the fi rst assess-ment carried out. Th ere are three important aspects to correctly estimating sperm motility:
• Observation chamber – a variety of types are available, but this should have a minimum depth of 20 µm to allow the sperm to move freely. A number of companies produce disposable chambers designed for motility observation (e.g., Microcell), but an alternative strategy is to place a 10 µL drop of semen on a glass microscope slide and cover it with a 22 mm diameter coverslip. NB: the depth of a Makler chamber (10 µm) makes it unsuitable for accurate motility measurements. However, when the purpose of assessment is the selection of an appropriate method of preparing the sample for assisted conception procedures, the Makler chamber does allow simultaneous judgment of approximate motile and immotile concentrations, and a quick assessment of type of sperm motility. • Temperature – the microscope slide should be maintained at 37°C on a heated stage during motility assessment for correct identifi cation of motility grade.

Chapter 10: Sperm and ART
141
• Microscope – observe the sample at ×200 or ×400 magnifi cation using a phase contrast objective. • Grading system – approximately 200 sperm should be examined and each sperm classifi ed as belonging to one of four motility grades. Figure 10.1 outlines the diff erence between the motility grades, with a fl ow chart explaining how to classify them. A percentage for the number of sperm belonging to each category should be calculated .
Aggregated or agglutinated spermatozoa
A high number of aggregated or agglutinated • spermatozoa can make accurate motility assessment impossible. A motility count should then be performed only on the free-swimming portion, with this noted in the report.
Less than 50% of the spermatozoa are motile
If less than 50% of the spermatozoa are motile, • a vitality test, such as a hypo-osmotic swelling (HOS) test, is recommended in order to determine if the nonmotile sperm are dead or alive.
Sperm concentration Methods used to determine sperm concentration have long been a subject of debate. Andrologists tend to
agree that using a hemocytometer is the most appro-priate, as it provides the most reproducible result with the lowest coeffi cient of variation when used properly. Since it normally relies upon the use of fi xatives to kill spermatozoa before they are placed on the count-ing chamber, its use is oft en thought to be in confl ict with the principles of trying to reduce chemical con-taminants in the IVF laboratory. Many embryolo-gists, however, use water instead of fi xative in which to dilute the spermatozoa and the osmotic shock is suf-fi cient to immobilize sperm suffi ciently for a count to be undertaken. Others prefer to use a Makler cham-ber or disposable chambers such as the Microcell. If an alternative chamber is chosen, then it is important that its accuracy is regularly checked using a thorough internal quality control system. Th is should preferably be checked against a hemocytometer as the gold stand-ard. Whatever chamber is chosen, it is important to pay special consideration to samples in which no spermato-zoa are observed. Th ese samples should be centrifuged at >3000 g for 15 minutes; a sample can be classifi ed as truly azoospermic only if no sperm are observed in the pellet aft er centrifugation.
Before performing the count, note the presence of agglutination and type if present (H-H, T-T, H-T), and any debris and cells other than spermatozoa, such as red or white blood cells.
Examine the counting grid and count the number of motile sperm in 20 squares. If the count appears on initial observation to be less than 10 million/mL, all 100 squares should be counted. Count the total num-ber of sperm in the same group of squares, and calcu-late motility:
Sperm density in millions/mL = the number of sperm in 10 squares of the grid.
Th e sperm concentration should be reported in millions per mL .
Sperm antibody detection Antibodies directed against sperm can be detected by two methods, the mixed antiglobulin reaction (MAR) test and the immunobead test . Th ey diff er slightly in their approach and methodology, but their inter-pretation is similar, in that they rely upon the iden-tifi cation of motile spermatozoa with adherent latex spheres or beads. Kits (SpermMar, FertiPro N.V., Belgium; Microm, UK) are available for antisperm antibody screening in semen samples; the MAR test will nonspecifi cally detect IgG, IgA or IgM antibodies,
Is the sperm swimming forward at ≥ 5 times the length of its own head in one second?
Is the sperm moving forward at all(i.e. moving between 1 and 5
head lengths per second)?
Is the flagellum beating or is thesperm shaking on the spot but
not progressing?
The sperm is not moving and the flagellum is not beating
Yes
Yes
Yes
Yes Grade d
Grade c
Grade b
No
No
No
Grade a
Figure 10.1 Flow chart for grading sperm motility.

Chapter 10: Sperm and ART
142
and specifi c latex particle immunobeads (BioRad) can be used to distinguish between the diff erent categories of antibody. Although the results of the two tests do not always agree, it is generally considered that a test is clinically signifi cant only if >50% of sperm have anti-bodies directed against them. In cases where the test cannot be performed due to an insuffi cient number of motile sperm, the sample can be tested indirectly by using the sperm of a donor (known to have no sperm antibodies in his semen) as part of the test: the donor sperm acts as a reagent in the assay. Th e percentage of spermatozoa with adherent particles should be recorded on the report form aft er evaluating 200 sperm.
Sperm morphology estimation Sperm morphology assessment is one of the most controversial measures in semen analysis. Th is is due partly to several changes in reporting the dimen-sions of normal spermatozoa in successive editions of the WHO manual, but is also due to the technical diffi culty of making accurate morphology measure-ments without the aid of a computerized system. All morphology measurements should be made using fi xed smears stained by the Papanicolaou method or the Diff -Quick or Shorr stains (prestained slides are also available: Testsimplets, Waldeck GmbH, www.waldeck-online.com ). Stained slides should be examined by bright-fi eld optics using an oil-immer-sion objective at ×1000 magnifi cation. At least 200 spermatozoa should be examined and an eyepiece graticule can be used to measure individual sperm-atozoa if necessary. Th e normal head has an oval shape with a length:width ratio of 1.50:1.75. A well-defi ned acrosomal region should cover 40–70% of the head area. No neck, midpiece or tail defects should be evident, and cytoplasmic droplets should constitute no more than one-third the size of a normal sperm head. Figure 10.2 illustrates some examples of typical sperm abnormalities. Count the number of sperm that display: 1. Abnormal heads 2. Tail abnormality 3. Midpiece abnormalities 4. Immature forms.
All borderline forms are classifi ed as abnormal. Calculate the percentage of each abnormal form, and add together the percentages to yield the total percent-age of abnormal forms in the sample .
A normal, fertile semen sample contains a very high proportion of morphologically abnormal forms, and the signifi cance of abnormal sperm morphology is not entirely understood. Although sperm of abnormal morphology evidently have reduced fertilizing potential, the true anomalies present in abnormal sperm cells have been only partially characterized; a correlation has been found with specifi c defi ciencies such as poor zona pellu-cida binding and penetration, poor response to agonists that modulate intracellular calcium concentrations, and with biochemical markers such as reactive oxygen species production and enhanced creatine phosphoki-nase activity. Th e signifi cance of sperm morphology is
Figure 10.2 Common abnormalities found in human sperm morphology.

Chapter 10: Sperm and ART
143
discussed further in Chapter 13 , under intracytoplasmic morphologically-selected sperm injection (IMSI).
Other cells in semen Other (non-sperm) cells can sometimes be observed during the semen analysis, either in the wet (motility) preparation, or in the stained morphology slide. Th ese include epithelial cells from the urethra, erythrocytes, germ cells and leukocytes. Whilst epithelial cells and erythrocytes are easily identifi able from their morph-ology, germ cells and leukocytes can easily be confused. Th erefore specifi c stains are needed to discriminate between the two cell types and to correctly enumer-ate their concentration on the semen analysis report. Leukocytes can be identifi ed using a peroxidase-based stain, or with the use of specifi c monoclonal anti-bodies. Th e concentration of any non-sperm cell can be calculated relative to the sperm concentration using the equation c = n × s /100, where n is the number of a given cell type in the same fi eld as 100 sperm, and s is the sperm concentration in millions per mL.
Internal and external quality control procedures A fi nal but important part of the semen analysis is the application of internal and external quality con-trol procedures to the semenology laboratory. Several studies have shown that samples analyzed in diff erent laboratories can give rise to radically diff erent results, in some cases leading to an inappropriate diagnosis for the patient. Many techniques have been outlined that can be used to monitor the performance of a labora-tory, and these are described in more detail in the 5th edition of the WHO manual. Any laboratory involved in making diagnoses should have such protocols in place and should be members of an external quality assessment scheme for andrology.
Sperm kinematics In the early 1980s several studies used time lapse pho-tography to analyze detailed movement characteristics of sperm in time and space (sperm kinematics). Th e motion of spermatozoa can be described in a number of diff erent ways (see Mortimer, 1994 ):
VSL = straight line velocity VCL = curvilinear velocity VAP = average path velocity ALH = amplitude of lateral head displacement.
Th ese early data led to the suggestion that specifi c pat-terns of sperm motility behavior were advantageous. For example, only spermatozoa with a high degree of lateral head displacement are able to penetrate cervical mucus. Th e development of computerized systems allowed such measurements to be made more rapidly as well as allowing the analysis of more sophisticated behavior patterns, such as sperm hyperactivation. Although the measurement of sperm hyperactivation has been controversial, it has been linked with IVF suc-cess. However, this technology is not used routinely as the prognostic value is poor and the high cost of the machines precludes their use in all but the most spe-cialized laboratories (see Tomlinson et al ., 2010 for review).
DNA fragmentation As detailed in Chapter 3, spermatogenesis is a com-plex and dynamic process of proliferation and dif-ferentiation, involving mitosis, meiosis, changes in cytoplasmic architecture, replacement of histones with transition proteins and the fi nal addition of protamines, leading to a highly packaged chroma-tin. It is not surprising therefore that ejaculated spermatozoa have a variety of abnormalities at the nuclear, cytoskeletal and organelle levels. Th ere is now evidence to suggest that sperm DNA integrity may be useful in predicting male fertility potential. Th e fi rst manuscript describing in-situ detection of sperm DNA fragmentation was published 25 years ago, and a surge in published reports about sperm DNA fragmentation then appeared between 2005 and 2010. Th ese studies provide strong evidence that semen samples in which more than a third of the DNA is fragmented have a reduced chance of result-ing in clinical pregnancy (Sakkas and Alvarez, 2010 ). Sperm DNA fragmentation may result from aber-rant chromatin packaging during spermatogenesis, apoptosis before ejaculation, excessive production of reactive oxygen species in the ejaculate, exposure to environmental or industrial toxins, genetics, oxi-dative stress, smoking, etc. Current standard sperm preparation techniques depend on a sedimentation or migration approach to separate spermatozoa based on their motility or density with molecu-lar events being overlooked. Th us, the use of sperm with DNA damage during IVF may be one of the reasons for suboptimal pregnancy and low live birth rates.

Chapter 10: Sperm and ART
144
Sperm chromatin assays Sperm condensation quality and sperm morphology studies suggest that the quality of chromatin packaging in human sperm, as assessed by its binding capacity for specifi c dyes and fl uorochromes, can be used as an adjunct to the assessment of morphology. Sperm of poor morphology may possess loosely packaged chro-matin, and this may contribute to a failure in sperm decondensation during fertilization.
Damaged chromatin will take up the following dyes:
1. Chromomycin (CMA3) staining
Fix prepared semen samples or semen smears in • 3:1 v/v of methanol/glacial acetic acid, at 4°C for 5 minutes. Treat each slide for 20 minutes with 100 mL CMA3 • solution: 0.25 mg/mL in McIlvane’s buff er, pH 7.0, containing 10 mM MgCl 2 . Evaluate the slides using fl uorescent microscopy. •
2. Aniline blue staining (AAB)
Fix the samples in 3% buff ered glutaraldehyde for • 30 minutes. Stain the slides with 5% aqueous aniline blue and • mix with 4% acetic acid (pH 3.5) for 7 minutes. Th ree classes of head staining can be noted: •
unstained (gray/white) partially stained entire sperm head dark blue intensity.
Detection of DNA fragmentation by the TUNEL assay Kits for DNA fragmentation analyses are now avail-able, for example the in situ cell death detection kit by Roche Diagnostics, Mannheim, Germany .
Wash a semen aliquot containing 1–2 × 10 • 6 spermatozoa with phosphate-buff ered saline (PBS) by centrifugation at 500 g at room temperature for 5 minutes. Remove the seminal plasma and wash the pellet • twice in PBS with 1% bovine serum albumin (BSA). Suspend the pellet in 100 μL of PBS/BSA 1% and • fi x it in 100 μL of 4% paraformaldehyde in PBS (pH 7.4) for 1 hour at room temperature, with agitation. Wash the cells again in PBS/1% BSA, spot a 10 • μL aliquot onto a demarcated area on a clean microscope slide and allow this to air dry.
Rinse the slides twice in PBS, and then • permeabilize using 0.1% Triton X100 in 0.1 % sodium citrate for 2 min on ice . Wash again twice with PBS, add terminal • deoxyribonucleotidyl transferase (TdT)-mediated dUTP nick-end label in order to allow DNA elongation, and incubate the slides in a humidifi ed chamber at 37°C for 60 min. Rinse slides twice in PBS and counterstain with 1 • mg/mL 4,6 diamidoino-2-phenylindole (DAPI) to visualize the nucleus. Include negative (omitting TdT from the reaction • mixture) and positive (using only DNAse I, 1 mg/mL for 30 min at room temperature) controls in each sample tested. Evaluate a total of 500 sperm per sample • using fl uorescence microscopy for fl uorescein isothiocyanate (FITC). Count the number of sperm per fi eld stained with DAPI (blue); the number of cells with green FITC fl uorescence (TUNEL positive) is expressed as a percentage of the total sample.
Preparation of sperm for in-vitro fertilization At the time of oocyte retrieval or intrauterine insemin-ation (IUI), the laboratory should already be familiar with the male partner’s semen profi le, and can refer to features that might infl uence the choice of sperm prep-aration method used. Semen is a nonsterile body fl uid that can transmit infection, and viral screening tests should be confi rmed as negative before the sample is handled for preparation in the laboratory. Aseptic technique should be maintained throughout.
Th e choice of sperm preparation method or com-bination of methods depends upon the assessment of:
motile count • ratio between motile:immotile counts • volume • presence of antibodies, agglutination, pus cells or • debris.
Ejaculated semen is a viscous liquid composed of a mixture of testicular and epididymal secretions con-taining spermatozoa, mixed with prostatic secretions produced at the time of ejaculation. Th is seminal plasma contains substances that inhibit capacitation and prevent fertilization. Th e purpose of sperm prep-aration is to concentrate the motile spermatozoa in

Chapter 10: Sperm and ART
145
a fraction that is free of seminal plasma and debris. Early IVF practice involved preparing sperm by sim-ple washing and centrifugation, but this method also concentrates cells, debris and immotile sperm, which can jeopardize fertilization. Aitken and Clarkson ( 1987 ) demonstrated that leukocytes and dead sperm in semen can generate reactive oxygen species (ROS), and these can initiate lipid peroxidation in human sperm membranes. Peroxidation of sperm membrane unsaturated fatty acids leads to a loss of membrane fl uidity, which inhibits sperm fusion events during the process of fertilization. When preparing sperm for assisted conception it is advantageous to separ-ate motile sperm from leukocytes and dead sperm as eff ectively and effi ciently as possible. However, if intracytoplasmic sperm injection (ICSI) is the treat-ment of choice, sperm fusion events are of course bypassed, and direct high-speed centrifugation of these suboptimal sperm samples does not appear to jeopardize fertilization by ICSI.
Sperm samples that show moderate to high counts (>35 × 10 6 motile sperm/mL) with good forward pro-gression and motility can be prepared using a basic overlay and swim-up technique. Discontinuous buoy-ant density gradient centrifugation is the method of choice for samples that show: 1. Low motility 2. Poor forward progression 3. Large amounts of debris and/or high numbers of
cells 4. Antisperm antibodies.
At the end of each preparation procedure, adjust the pH of the resulting samples by gassing gently with 5% CO 2 , and store the samples at room temperature until fi nal preparation for insemination .
Standard swim-up or layering 1. Pipette 2 mL of HEPES-buff ered culture medium
into a round-bottomed disposable test-tube. 2. Gently pipette approximately 1.5 mL neat semen
underneath the medium (being very careful not to disturb the interface formed between the semen and the medium).
3. Tightly cap the tube and allow it to stand at room temperature for up to 2 hours (the ejaculate can also be divided into several tubes for layering if necessary).
4. Harvest the resulting top and middle clouded layers into a conical test-tube and spin at 200 g for 5 minutes.
5. Remove the supernatant and resuspend the pellet in 2 mL medium. Centrifuge again, discard the supernatant, and resuspend the pellet in 1 mL medium.
6. Assess this sample for count and motility, gas the surface gently with 5% CO 2 in air, and store at room temperature prior to dilution for the insemination procedure .
Alternatively, 2 mL of medium can be gently lay-ered over the semen sample in its pot, which provides a larger interface surface area. Aft er 10–45 minutes, sus-pend an aliquot of this layer in 1 mL of medium, and process as above. Th e time allowed for swim-up should be adjusted according to the quality of the initial sam-ple: the percentage of abnormal sperm that will appear in the medium increases with time, and continues to do so aft er normal motile density has reached its opti-mum level.
Pellet and swim-up Th is method is used when the semen has been collected into medium or medium + albumin . It is also useful for viscous samples (once the viscosity has been decreased, by vigorous pipetting or syringing) and when the total volume of semen is very low. Th is method is not recom-mended when motility is very poor or when there is a large degree of cellular contamination and debris (the sperm will be concentrated with this prior to the swim-up). 1. Mix semen and medium and centrifuge once.
Note : In some cases (i.e., oligo/asthenospermia) much more semen will need to be prepared, and the volume of medium used should be increased accordingly. As a general rule be careful not to take far more of the semen than is required.
2. Carefully remove all the supernatant and then very gently pipette about 0.75 mL of medium over the pellet, taking care not to disturb it.
3. Allow the sperm to swim up into the medium. If the sample has poor motility it sometimes helps to lay the centrifuge tube on its side.
10 minutes is suffi cient for very motile sperm • (activity 3–4) 1 hour plus may be required for poorly motile • sperm.

Chapter 10: Sperm and ART
146
In general do not leave for too long, as some • cells and debris will become resuspended .
4. Carefully remove supernatant from pellet and place in a clean centrifuge tube.
5. Centrifuge again, resuspend in medium, assess count and motility, and gas with CO 2 before storing at room temperature.
Th is method has the disadvantage of exposing motile sperm to peroxidative damage during centri-fugation with defective sperm and white cells. Aitken ( 1990 ) has shown that unselected sperm exhibit higher levels of ROS production in response to centrifuga-tion than the functionally competent sperm selected prior to centrifugation by the layering method. Sperm that are selected prior to centrifugation produce much lower levels of ROS and their functional capacity is not impaired.
Discontinuous buoyant density gradient centrifugation Buoyant density gradient “kits” for sperm preparation are commercially available. Th ese are based upon either coated silica particles, a mixture of Ficoll and iodixa-nol, or highly purifi ed arabinogalactan. Individual experiences comparing the use of these products have reported no signifi cant diff erences between them. Buoyant density gradients apparently protect the sperm from the trauma of centrifugation, and a high proportion of functional sperm can be recovered from the gradients. Discontinuous two- or three-step gradi-ents are simple to prepare and highly eff ective in pre-paring motile sperm fractions from suboptimal semen samples. A single layer of 90–100% density can also be used for simple fi ltration by layering the sample on top of the column and allowing the sperm to migrate through the density medium, where they can be har-vested from the bottom of the test-tube.
Methods Manufacturers’ instructions should be followed for the diff erent commercial preparations, but “recipes” can be adapted according to each individual semen sam-ple, in particular with respect to volumes, speed of cen-trifugation, and length of centrifugation. In general, a longer centrifugation time increases the recovery of both motile and immotile sperm; normal immo-tile sperm are only decelerated by the particles, and aft er long spinning they will reach the bottom of the
gradient. Higher centrifugation speeds increase the recovery of motile sperm, and also of lower density particles; therefore, if the gradients are spun at a higher speed, a shorter time should be used. Debris, round cells, and abnormal forms with amorphous heads and cytoplasmic droplets never reach the bottom of the tube because of their low density. Gradients with larger volumes result in improved fi ltration, but decreased yield. Th e three layers of a mini-gradient improve fi l-tration, and the smaller volumes improve recovery of sperm from severely oligospermic samples. Large amounts of debris can disrupt gradients and prevent adequate fi ltration. Th ere is a limit to the number of cells that can be loaded onto any gradient, and samples with high density or a large amount of debris should be distributed in smaller volumes over several gradients. Severely asthenozoospermic samples, with a normal sperm density but poor motility can also be distributed over a series of mini-gradients.
Th e temperature of the prepared gradients also aff ects the “merging of gradients,” which is improved at 37°C compared to room temperature.
Isotonic gradient solution 10 × concentrated EBS (or other media concentrate): 10 mL 5% human serum albumin: 19 mL Sodium pyruvate: 113 mg Sodium lactate 60%: 0·37 mL 1 M HEPES: 12 mL Gentamicin sulfate, 5 mg/mL: 12 mL
Mix, and fi lter this solution through a 0.22 mm Millipore fi lter
Add 90 mL density gradient preparation media Store at + 4°C for up to 1 week.
Two-step gradient, 80/40
Can be used for all samples which contain> 4×10 • 6 motile sperm/mL . Should be used for all specimens with known or • suspected antisperm antibodies:
80%: 8 mL isotonic + 2 mL culture medium 40%: 4 mL isotonic + 6 mL culture medium.
1. Gradients: pipette 2.0–2.5 mL of 80% into the bottom of a conical centrifuge tube, and gently overlay with an equal volume of 40%.
2. Layer up to 2 mL of sample on top of the 40% layer. 3. Centrifuge at 600 g for 20 minutes.

Chapter 10: Sperm and ART
147
Cells, debris and immotile/abnormal sperm accu-mulate at the interfaces, and the pellet should con-tain functionally normal sperm. Recovery of a good pellet is infl uenced by the amount of debris and immotile sperm, which impede the travel of the normal motile sperm .
4. Carefully recover the pellet at the bottom of the 80% layer, resuspend in 1 mL of medium, and assess (even if there is no visible pellet, a suffi cient number of sperm can usually be recovered by aspirating the bottom portion of the 80% layer).
5. If the sample looks suffi ciently clean, centrifuge for 5 minutes at 200 g , resuspend the pellet in fresh medium, and assess the fi nal preparation.
6. If there is a high percentage of immotile sperm, centrifuge at 200 g for 5 minutes, remove the supernatant, carefully layer 1 mL fresh medium over the pellet, and allow the motile sperm to swim up for 15–30 minutes. Collect the supernatant and assess the fi nal preparation.
If at least 10 6 motile sperm/mL have been recov-ered, spin at 200 g for 5 minutes and resuspend in fresh medium. Th is will be the fi nal preparation to be diluted before insemination, therefore the volume of medium added will depend upon the calculated assessment .
Mini-gradient (95/70/50)
1. Gradients: make layers with 0.3 mL of each solution: 95, then 70, then 50.
2. Dilute the semen 1:1 with culture medium, and centrifuge at 200 g for 10 minutes .
3. Resuspend the pellet in 0.3 mL culture medium, and layer over mini-gradient (resuspend in a larger volume if it is to be distributed over several gradients).
4. Centrifuge at 600 g for 20–30 minutes. 5. Recover the pellet(s), resuspend in 0.5 mL culture
medium, and assess count and motility. Proceed exactly as for two-step gradient preparation: either centrifuge at 200 g for 5 minutes and resuspend the pellet, or layer over the pellet for a further preparation by swim-up. Th e concentration of the fi nal preparation should be adjusted to a sperm
density of approximately 10 6 motile sperm per mL if possible.
If a sample is being prepared for ICSI, note that residual polyvinylpyrrolidone (PVP)-coated parti-cles in the preparation will interact with PVP used for sperm immobilization, resulting in a gelatinous mass from which the sperm cannot be aspirated. Careful washing of the preparation to remove all traces of gra-dient preparation is essential when handling samples for ICSI (one wash is usually suffi cient).
Sedimentation method or layering under paraffi n oil Th is method is useful for samples with very low counts and poor motility. It is very eff ective in remov-ing debris, but requires several hours of preparation time. 1. Mix the semen with a large volume of medium,
pipetting thoroughly to break down viscosity etc., and wash the sample by dilution and centrifugation twice .
2. Alternatively: process the entire sample (undiluted) on an appropriate discontinuous buoyant density gradient.
3. Resuspend the pellet in a reduced volume of medium so that the fi nal motile sperm concentration is not too dilute.
4. Layer this fi nal suspension under paraffi n oil (making one large droplet) in a small Petri dish. Place in a desiccator and gas with 5% CO 2 .
5. Leave at room temperature for 3–24 hours. Th e duration of sedimentation depends upon the amount of cells, debris and motile spermatozoa; a longer period is usually more eff ective in reducing cells and debris, but may also reduce the number of freely motile sperm in the upper part of the droplet.
6. Carefully aspirate motile sperm by pipetting the upper part of the droplet. Aspiration can be made more effi cient by using a fi ne drawn pipette and also by positioning the droplet under the stereomicroscope, to ensure that as little debris as possible is collected .
High-speed centrifugation and washing Cryptozoospermic (or nearly cryptozoospermic) samples which must be prepared for ICSI can be either centrifuged directly (without dilution) at 1800 g
95% 9.5 mL gradient solution + 0.5 mL culture medium
70% 7.0 mL + 3.0 mL
50% 5.0 mL + 5.0 mL

Chapter 10: Sperm and ART
148
for 5 minutes, or diluted with medium and then cen-trifuged at 1800 g for 5 minutes . 1. Wash the pellet with a small volume of medium
(0.5 mL approximately) and centrifuge at 200 g for 5 minutes.
2. Recover this pellet in a minimal volume of medium (20–50 mL), and overlay with mineral oil. Single sperm for microinjection can then be retrieved from this droplet using the micromanipulator.
It is important to bear in mind that every semen specimen has diff erent characteristics and param-eters, and it is illogical to apply an identical prepar-ation technique to each specimen. All preparation methods are adaptable in some way: layering can be carried out in test-tubes, but a wider vessel increases the area exposed to culture medium and decreases the depth of the specimen, increasing the potential return of motile sperm from oligoasthenospermic samples. Centrifugation times for buoyant density gradients may be adjusted according to the quality of the spe-cimen to give optimum results. It is important to tai-lor preparation techniques to fi t the parameters of the semen specimen, rather than to have fi xed recipes. A trial preparation prior to oocyte retrieval may be advisable in choosing the suitable technique for par-ticular patients .
Chemical enhancement of sperm motility prior to insemination Pentoxifylline is a methylxanthine-derived phospho-diesterase inhibitor which is known to elevate sperm-atozoal intracellular levels of cAMP in vitro. It has been postulated that the resulting increase in intra cellular adenosine triphosphate (ATP) enhances sperm motil-ity in samples that are assessed as having poor pro-gressive motility, with an increase in fertilization and pregnancy rates for suboptimal semen samples. 2-De-oxyadenosine has also been used to achieve a similar eff ect. Th e protocol involves a 30-minute preincuba-tion of prepared sperm with the stimulant; the result-ing sperm suspension is then washed to remove the stimulant, and the preparation is used immediately for insemination.
Stock solutions
1 mM PF: dissolve 22 mg pentoxifylline in 10 mL medium.
3 mM 2-DA: dissolve 8 mg 2-deoxyadenosine in 10 mL medium. Gas with 5% CO 2 to adjust pH. Store at 4°C for a maximum period of one month.
Procedure
1. Gas and warm PF or 2-DA solutions, and also an additional 10 mL medium.
2. 35–40 minutes prior to insemination time, add an equal volume of PF or 2-DA solutions to the sperm preparation suspension.
3. Incubate at 37°C for 30 minutes. 4. Centrifuge, 5 minutes at 200 g , and resuspend
pellet in warm medium. 5. Analyze the sperm suspension for count and
motility, dilute to appropriate concentration for insemination, and inseminate oocytes immediately .
Sperm preparation for ICSI/IMSI A combination of sperm preparation methods can be used; extremely oligospermic/asthenozoospermic samples cannot be prepared by buoyant density centri-fugation or swim-up techniques. 1. Centrifuge the whole sample, 1800 g , 5 minutes,
wash with medium, and resuspend the pellet in a small volume of medium.
2. Apply this sample directly to the injection dish (without PVP/SpermSlow), or add an aliquot of the suspension to a drop of HEPES-buff ered medium.
3. If possible, use the injection pipette to select a moving sperm with apparently normal morphology from this drop and transfer it into the drop to be used for sperm immobilization.
4. If there is debris attached to the sperm, clean it by pipetting the sperm back and forth with the injection pipette.
5. If the sperm still has some movement in the immobilization drop, immobilize it by crushing the tail and proceed with the injection as described in Chapter 11 .
6. It may sometimes be helpful to connect the sperm droplet to another small medium droplet by means of a bridge of medium, and allow motile sperm to swim out into the clean droplet. Overloading a PVP/SpermSlow droplet with very poor sperm can seriously hamper the selection procedure, due

Chapter 10: Sperm and ART
149
to the presence of excessive amounts of debris. Using a bridge of medium allows motile sperm to swim into the second, clean droplet .
Even if the results of semen analysis show no motile sperm, it may be possible to see occasional slight tail movement in a medium drop without PVP. If abso-lutely no motile sperm are found, immotile sperm may be used. Th e fertilization rate with immotile sperm is generally lower than that with motile sperm, and oocytes with a single pronucleus are seen more oft en in these cases, possibly indicating incomplete oocyte acti-vation . Previous assessment with a vital stain may be helpful before deciding upon ICSI treatment. However, embryologists may be left with the dilemma of making a decision regarding injection in situations where there are only immotile sperm, the vitality stain/HOS test indicates the sperm tested are not alive and there is no donor back-up.
Hypo-osmotic swelling test (HOS) Th e HOS test assesses the osmoregulatory ability of the sperm, and therefore the functional integrity of its membranes. It can be used to discriminate viable from nonviable sperm cells in a sample which has zero or little apparent motility. Th e test is based upon the ability of live spermatozoa to withstand the moderate stress of a hypo-osmotic environment – they react to this stress by swelling of the tail. Dead spermatozoa whose plasma membranes are no longer intact do not show tail swelling. HOS test diluent is a solution of 150 mOsm/kg osmolarity, and can be made by dissolving 7.35 g sodium citrate and 13.51 g fructose in 1000 mL of reagent-grade water (alternatively, sperm prepar-ation medium can be diluted 1:1 with reagent-grade water). Mix an aliquot of the sample with approxi-mately 10 times the volume of diluent, incubate at 37°C for 30 minutes, remix and transfer one drop of the mixture to a clean microscope slide. Cover with a coverslip, and examine using phase-contrast micros-copy at a magnifi cation of ×400–500 for the presence of swollen (coiled) tails. Osmotically incompetent and dead spermatozoa swell so much that the plasma membrane bursts, allowing the tail to straighten out again.
100% abnormal heads If the semen analysis shows 100% head anomalies, it may still be possible to fi nd the occasional normal form in the sample. In cases where no normal forms
are found, the fertilization and implantation rates may be lower; however, debate continues about this subject, and individual judgment should be applied to each case, with careful assessment of several diff erent semen samples.
Fertilization and pregnancy have now been dem-onstrated using samples from men with globozoosper-mia, a 100% head anomaly where all sperm lack an acrosomal cap; in these cases the oocytes need to be artifi cially activated post-ICSI for fertilization to occur. However, there is evidence to suggest that such defects which are genetically determined have a high probabil-ity of being transmitted to the off spring, and debate continues as to whether it is ethically advisable to off er treatment to these men.
Sticky sperm Sperm that have a tendency to stick to the injection pipette make the injection procedure more diffi cult. If the sperm is caught in the pipette, try to release it by repeatedly aspirating and blowing with the injection system.
Excessive amounts of debris Large amounts of debris in the sperm preparation may block the injection pipette, or become attached to the outside of the pipette. A blocked pipette may be cleared by blowing a small amount of the air already in the pip-ette through it. Another useful technique is to insert the injection pipette into the lumen of the holding pipette, and then apply negative suction to the holding pipette and simultaneous positive pressure to the injection pipette. Debris attached to the outside of the injection pipette can be cleaned by rubbing the pipette against the holding pipette, against the oocyte, or against the oil at the edge of the medium drop. It may be necessary (and preferable) to change the pipette if it cannot be quickly cleared.
Sperm preparation after retrograde ejaculation and electroejaculation When treating patients with ejaculatory dysfunction, with or without the aid of electroejaculation, both ante-grade and retrograde ejaculation (into the bladder) are commonly found. When retrograde ejaculation is anticipated, the patient should fi rst empty his blad-der, and then drink an alkaline drink (e.g., bicarbon-ate of soda), and empty his bladder again 30 minutes

Chapter 10: Sperm and ART
150
later before producing a sample that can then be col-lected from a urine sample by centrifugation. In cases of spinal cord injury, the bladder is emptied via a cath-eter and approximately 20 mL of culture medium then instilled. Aft er electroejaculation, the bladder is again emptied, and the entire sample centrifuged. Th e result-ing pellet(s) are resuspended in medium and processed on appropriate density gradients. As with all abnormal semen samples, a fl exible approach is required in order to obtain a suitable sample for insemination; ICSI is recommended as the treatment of choice .
Surgical sperm retrieval Until the mid-1990s, virtually all patients with obstructive or nonobstructive azoospermia (see Appendix for list of pathologies) had untreatable male sterility; this situation was completely reversed by the ability to combine ICSI with surgical techniques to recover samples from the epididymis and directly from the testis. 1. Epididymal sperm can be obtained by open
microscopic surgery (MESA) or by percutaneous puncture (PESA), using a 21-gauge “butterfl y” or equivalent needle to aspirate fl uid. If large numbers of sperm are found, they can be processed by buoyant density gradient centrifugation. Samples with fewer sperm can be washed and centrifuged with IVF medium a number of times, and the concentrated sample is then added to microdroplets in the injection dish. Motile spermatozoa “swim out” to the periphery of the droplets, where they can be collected and transferred to clean drops of medium for injection later.
2. Testicular sperm is obtained by open biopsy (testicular sperm extraction, TESE) or by percutaneous needle biopsy (testicular fi ne needle aspiration, TEFNA) , and samples can be processed in a variety of ways: • Crush the biopsy sample between two
microscope slides, and expose sperm by shredding the tissue either with glass slides, by needle dissection, by dissection using microscissors, or by maceration using a microgrinder (available from Hunter Scientifi c). Concentrate the debris by centrifugation and examine under high-power microscopy to look for spermatozoa . Large quantities of debris are invariably present, and
it may be diffi cult to fi nd sperm (especially with cases of focal spermatogenesis ). Further processing steps will depend upon the quality of the sample: it may be loaded onto a small single-step buoyant density gradient, or sperm simply harvested “by hand” under the microscope. Use a large needle, assisted hatching pipette or biopsy pipette to collect and pool live sperm in a clean drop of medium.
• Tubules in the biopsy sample can be carefully unraveled under the dissecting microscope, using fi ne watchmakers’ forceps. Cut the tubules into small lengths of 1–2 cm, and “milk” the contents by squeezing from the middle to an open end (analogous to squeezing a tube of toothpaste). Th e cells can be picked out of the dish and examined under the ICSI microscope , or placed into a centrifuge tube of clean medium for further preparation. An alternative approach is to slit the segments of tubule rather than “milking” to release the cells. Fresh testicular sperm are oft en immotile and combined with Sertoli cells, but free-swimming sperm are usually seen aft er further incubation. In cases of obstructive azoospermia , pregnancies have been achieved from testicular sperm incubated up to 3 days aft er the biopsy procedure, but the proportion of motile sperm in a testicular biopsy sample is usually highest aft er 24 hours’ incubation. Incubation at 32°C instead of 37°C may also be of benefi t (Van den Berg, 1998 ). If fresh sperm is to be used, the biopsy procedure should be carried out the day before the planned oocyte retrieval. In cryopreserved samples, a higher proportion of frozen testicular sperm have been found to retain their motility on thawing if they have been incubated for 24–48 hours before freezing; however, in cases of nonobstructive azoospermia , incubation for longer than 24 hours is not recommended. When biopsied sperm are processed in advance, any motile sperm found using an injection needle can be stored in empty zonae before freezing (see Chapter 12 ); this has the advantage that the sperm are then readily available at the time of ICSI, which can save considerable time.

Chapter 10: Sperm and ART
151
Spermatid identifi cation In some cases of severe testicular dysfunction, no spermatozoa can be found either in the ejaculate or in testicular tissue, but precursor cells (round, elong-ating or elongated spermatids) may be identifi ed. Although there was initial enthusiasm in the late 1990s with the technique of round spermatid nucleus injec-tion (ROSNI), this was short-lived with the prospect of unresolved genetic concerns and poor activating capacity of the immature sperm cells. Spermatid injec-tion is forbidden by the HFEA in the UK, and also by regulatory authorities in some other countries. Males with meiotic arrest of spermatogenesis are counseled towards the use of donor sperm.
Using Hoff man Modulation Contrast systems, four categories of spermatids can be observed and identifi ed according to their shape, amount of cytoplasm, and size of tail: round, elongating, elongated and mature sperma-tids just prior to their release from Sertoli cells. However, in practice it can be diffi cult to confi dently identify immature sperm cells in a wet preparation. Round sper-matids must be distinguished from other round cells such as spermatogonia, spermatocytes, polymorpho-nuclear leukocytes, lymphocytes and erythrocytes. Th eir diameter (6.5–8 μm) is similar to that of eryth-rocytes (7.2 μm) and small lymphocytes. Round sper-matids may be observed at three diff erent phases: Golgi, cap and acrosome phase (where the nucleus moves towards a peripheral position). When the cell is rotated, a centrally located smooth (uncondensed) nucleus can be seen, and a developing acrosomal structure may be observed as a bright spot or small protrusion on one side of the cell, adjacent to the spermatid nucleus. Sertoli cell nuclei are very fl at and transparent, with a prominent central or adjacent nucleus, whereas the ROS is a three-dimensional round cell ( Figure 10.3a ). Phase 3 is a tran-sition between round and elongated forms – elongated spermatids have an elongated nucleus at one side of the cell, and a larger cytoplasmic region on the other side, surrounding the developing tail ( Figure 10.3b ).
Pathology of azoospermia Th e Johnsen score is an assessment of the degree of spermatogenesis found in a biopsy: a number of tubules are assessed, and each one is given a score for the most advanced stage of spermatogenesis seen:
1 = no cells present in the tubule 2 = Sertoli cells 3 = spermatogonia
4–5 = spermatocytes 6–7 = spermatids 8–10 = spermatozoa .
Mean Johnsen score (MJS) = average of all the tubules assessed, i.e.:
MJS = 2 is the Sertoli cell only syndrome MJS = 8–10 is normal spermatogenesis MJS between 2 and 8 represents varying degrees of subnormal spermatogenesis , but a qualitative description is required.
Th ere is a correlation between testicular size and MJS.
Pathologies A. Pretesticular: defi cient gonadotropin drive – low
FSH B. Androgen resistance: familial
pseudohermaphroditism C. Testicular failure: no spermatogenesis – raised
FSH
Figure 10.3 (a and b) Scanning electron micrographs of early spermatid detected in azoospermic ejaculate. (Courtesy of Professor B. Bartoov, Israel.)

Chapter 10: Sperm and ART
152
D. Post-testicular duct obstruction: functional sperm usually present, size of testes is normal, FSH is not raised.
Pretesticular Th ese are pathologies that result in secondary testicu-lar failure (hypogonadotropic hypogonadism) due to decreased gonadotropin release (low serum FSH). Testicular biopsy may show a prepubertal appearance, with precursors of Sertoli cells, prespermatogenic cells and absence of Leydig cells. 1. Congenital
partial or complete Kallman’s syndrome , • GnRH defi ciency associated with agenesis of the fi rst cranial nerve and thus anosmia low FSH and LH, small but potentially normal • testes.
2. Acquired: space-occupying lesions pituitary tumors • craniopharyngioma • trauma , meningitis , sarcoidosis • Cushing’s syndrome (adrenal hypoplasia ) • congenital adrenal hyperplasia • hemochromatosis. •
Androgen resistance Familial incomplete male pseudohermaphroditism, type 1: partial or complete defects in amount or func-tion of the androgen receptor. Patients fall into a wide spectrum of disorders, probably due to variable mani-festations of a single gene defect. Cryptorchidism is common, and the testes remain small in size. Th e testes demonstrate normal Leydig cells and tubules containing both germ cells and Sertoli cells, but there is usually no maturation beyond the primary spermatocyte. Plasma testosterone and LH are high, suggesting that there is a defect in the feedback control of testosterone on the hypothalamus . Th ere are four (phenotypically) separate clinical disorders: 1. Rosewater’s syndrome (mildest form) 2. Reinfenstein’s syndrome 3. Gilbert–Dreyfus syndrome 4. Lub’s syndrome (most severe) – phenotypic
females with partial Wolffi an duct development and masculine skeletal development.
Testicular failure Th is can be congenital or acquired, and testicular biopsy can show a wide variation in appearance, e.g.:
Sclerosing tubular degeneration is seen in Klinefelter’s syndrome . Disorganization with extensive hyalinization and tubular atrophy is seen aft er orchitis.
1. Congenital Klinefelter’s syndrome (XXY) • autosomal abnormalities • torsion (maturation arrest) • cryptorchidism, anorchia • sickle cell disease • myotonic muscular dystrophy • Noonan’s syndrome (male Turner’s). •
2. Acquired mumps orchitis • epididymo-orchitis • testicular trauma • inguinal/scrotal surgery • radiotherapy. •
Post-testicular: obstructive causes of azoospermia Testicular biopsy shows well-preserved normal sperm-atogenesis, and there may be sloughing of superfi -cial layers of the seminiferous epithelium. Th e upper epididymis is the most common site of genital tract obstruction (two-thirds of lesions), and multifocal sites of obstruction may be present. Obstructive lesions can be caused by specifi c or nonspecifi c infection, and edema and/or hematoma as a result of trauma can lead to epididymal or vasal obstruction. 1. Congenital:
Congenital absence of the vas deferens • (CAVD – female partner should be screened for cystic fi brosis mutations) Cystic fi brosis • Young’s syndrome • Zinner’s syndrome : congenital absence of the • vas deferens, corpus and cauda epididymis, seminal vesicle, ampulla and ejaculatory duct – may be bilateral or unilateral and can be associated with ipsilateral renal agenesis – due to failure of the Wolffi an (mesonephric) duct .
2. Acquired TB • Gonococcal or chlamydial infection • surgical trauma • smallpox • bilharziasis •

Chapter 10: Sperm and ART
153
fi lariasis • vasectomy. •
Other causes of spermatogenic failure or disorder Th ese may be associated with defective testoster-one synthesis, decreased metabolic clearance rates, increased binding of testosterone to plasma proteins, increased plasma estradiol and low, normal or mod-erately elevated serum FSH levels. 1. Systemic illness
fevers, burns, head trauma chronic renal failure thyrotoxicosis, diabetes male anorexia nervosa surgery, general anesthesia.
2. Drugs/industrial toxins (a) Th erapeutic: sulfasalazine, nitrofurantoin,
cimetidine, niridazole, colchicine, spironolactone, testosterone injections, cytotoxic agents
(b) Occupational: carbon disulfi de (rayon), lead, dibromochloropropane, radiation
(c) Recreational abuse: alcohol, opiates, anabolic steroids.
3. Absent spermatogenesis : germinal aplasia or hypoplasia, Sertoli cell only (del Castillo) syndrome. Only Sertoli cells are present in the tubular epithelium, none of the spermatogenic elements remain. In germinal cell hypoplasia, there is a generalized reduction in the numbers of germ cells of all stages. Th e numbers of more mature cells are greatly reduced, and the germinal epithelium has a loose, poorly populated appearance. Th ere are two forms: (a) serum FSH is grossly elevated, Sertoli cells
show severe abnormalities on electron microscopy – no inhibin production
(b) serum FSH is normal – normal inhibin production.
Testis size is oft en not markedly reduced, and this may lead to diagnostic diffi culties. Th ese patients are frequently misdiagnosed as having an obstructive lesion, and biopsy is the only means of making a correct diagnosis .
4. Leydig cell failure leads to low testosterone levels, and raised serum FSH and LH. In this situation the testis is atrophied, with gross reduction in size.
5. Immotile sperm – Kartagener’s immotile cilia syndrome . Normal numbers of sperm are present in the semen, but they are all immotile. Transmission electron microscopy shows that the central fi laments of the tails are absent, and this anomaly may be present in cilia throughout the body, resulting in chronic sinusitis and bronchiectasis.
6. Retrograde ejaculation : diabetes, multiple sclerosis, sympathectomy, prostatectomy, funnel bladder neck.
7. Ejaculatory failure: spinal cord injury, multiple sclerosis, diabetes, abdominal aortic surgery, abdominoperineal resection, psychomimetic/antihypertensive drugs, hypogonadism.
Chromosomal anomalies Klinefelter’s syndrome
Bilateral testicular atrophy, signs of hypogonadism • with a greater span than height, oft en with gynecomastia . FSH and LH are extremely high, oft en with low • testosterone. Diagnosis can be made on clinical and • biochemical grounds, and confi rmed by buccal smear or karyotype (XXY). Aff ects 1 in 400 live-born males, and is found in • around 7% of infertile men. Testicular histology: obvious and gross • spermatogenic failure with disappearance of all the spermatogenic elements in all the tubules. Marked hyperplasia of the Leydig cells .
46XX Klinefelter’s Patients are phenotypically male, with same clinical and endocrinological features as the XXY patient. H-Y antigen has been demonstrated: despite apparent absence of Y chromosome, there is expression of some Y genes.
46XX (Noonan’s syndrome) Male equivalent of Turner’s (XO): normal male pheno-type, but are usually cryptorchid and show varying degrees of hypoandrogenization.
Th ere is testicular atrophy , raised FSH and LH, and reduced testosterone.

Chapter 10: Sperm and ART
154
Robertsonian translocation A form of chromosomal aberration which involves the fusion of long arms of acrocentric chromosomes at the centromere. Breaks occur at the extreme ends of the short arms of two nonhomologous acrocentric chromosomes; these small segments are lost, and the larger segments fuse at their centromeric region, pro-ducing a new, large submetacentric or metacentric chromosome.
“Balanced translocations” may produce only minor defi ciencies, but translocation heterozygotes have reduced frequencies of crossing over and are usu-ally subfertile through the production of abnormal gametes.
Appendix
Sperm preparation: equipment and materials
Semen sterile collection pot 60 mL Microscope (phase is useful) Counting chamber (Makler, Sefi Medical Instruments, POB 7295, Haifa 31070 Israel, or Horwell Haemocytometer) Centrifuge with swing-out rotor (Mistral 1000, MSE) Centrifuge tubes (15 mL, Corning) Microscope slides Coverslips Disposable test-tubes: 4 mL, 10 mL Culture media Buoyant density media:
Pure Sperm (Scandinavian IVF AB) IxtaPrep (MediCult) Sil-Select (MICROM) Isolate (Irvine Scientifi c)
Glass Pasteur pipettes Disposable pipettes: 1, 5, 10 mL Spirit burner + methanol or gas Bunsen burner Plastic ampules or straws for sperm freezing Sperm cryopreservation media ( Chapter 12 ) Supply of liquid nitrogen and storage dewars
Further reading Aitken RJ ( 1988 ) Assessment of sperm function for IVF .
Human Reproduction 3 : 89 –95. Aitken RJ ( 1989 ) Th e role of free oxygen radicals and sperm
function . International Journal of Andrology 12 : 95 –97.
Aitken RJ ( 1990 ) Evaluation of human sperm function . British Medical Bulletin 46 : 654 –674.
Aitken RJ , Clarkson JS ( 1987 ) Cellular basis of defective sperm function and its association with the genesis of reactive oxygen species by human spermatozoa . Journal of Reproductive Fertility 81 : 459 –469.
Aitken RJ , Comhaire FH , Eliasson R , et al . ( 1999 ) WHO Manual for the Examination of Human Semen and Semen-Cervical Mucus Interaction , 2nd edn. Cambridge University Press , Cambridge .
Aitken RJ , Gordon E , Harkiss D , et al . ( 1998 ) Relative impact of oxidative stress on the functional competence and genomic integrity of human spermatozoa . Biology of Reproduction 59 : 1037 –1046.
Barratt CLR , Bolton AE , Cooke ID ( 1990 ) Functional signifi cance of white blood cells in the male and female reproductive tract . Human Reproduction 5 (6): 639 –648.
Braude PR , Bolton VN ( 1984 ) Th e preparation of spermatozoa for in vitro fertilization by buoyant density centrifugation. In: Feichtinger W , Kemeter P (eds.) Recent Progress in Human In Vitro Fertilisation . Cofese , Palermo , pp. 125–134.
Cohen J , Edwards RG , Fehilly C , et al . ( 1985 ) In vitro fertilization: a treatment for male infertility . Fertility and Sterility 43 : 422 –432.
Comhaire F , Depoorter B , Vermeulen L , Schoonjans F ( 1995 ) Assessment of sperm concentration. In: Hedon B , Bringer J , Mares P (eds.) Fertility and Sterility: A Current Overview (IFFS 1995) . Parthenon Publishing Group , New York , pp. 297–302.
Donnelly ET , McClure N , Lewis SEM ( 1999 ) Th e eff ect of ascorbate and alpha-tocopherol supplementation in vitro on DNA integrity and hydrogen peroxide-induced DNA damage in human spermatozoa . Mutagenesis 14 (5): 505 –512.
Dravland JE , Mortimer D ( 1985 ) A simple discontinuous Percoll gradient for washing human spermatozoa . IRCS Medical Science 13 : 16 –18.
Edwards RG , Fishel SG , Cohen J , Fehilly CB , Purdy JM , Steptoe PC , Webster JM ( 1984 ) Factors infl uencing the success of in vitro fertilization for alleviating human infertility . Journal of In Vitro Fertilization and Embryo Transfer 1 : 3 –23.
Elder KI , Elliott T ( 1998 ) Th e use of testicular and epididymal sperm in IVF. Worldwide Conferences on Reproductive Biology . Ladybrook Publishing , Australia .
Elder KT , Wick KL , Edwards RG ( 1990 ) Seminal plasma anti-sperm antibodies and IVF: the eff ect of semen sample collection into 50% serum . Human Reproduction 5 : 179 –184.
Evenson DP , Jost LJ , Marshal D , et al . ( 1999 ) Utility of the sperm chromatin structure assay as a diagnostic and prognostic tool in the human fertility clinic . Human Reproduction 14 : 1039 –1049.

Chapter 10: Sperm and ART
155
Fleming SD , Meniru GI , Hall JA , Fishel SB ( 1997 ) Semen analysis and sperm preparation. In: A Handbook of Intrauterine Insemination . Cambridge University Press , Cambridge .
Franken D ( 1998 ) Sperm morphology: a closer look – is sperm morphology related to chromatin packaging? Alpha Newsletter 14 : 1 –3.
Glover TD , Barratt CLR , Tyler JPA , Hennessey JF ( 1990 ) Human Male Fertility and Semen Analysis. Academic Press , London .
Grobler GM , De Villiers TJ , Kruger TF , Van Der Merwe JP , Menkveld R ( 1990 ) Part Two – Th e Tygerberg Experience. In: Acosta AA , Swanson RJ , Ackerman SB , et al . (eds.) Human Spermatozoa in Assisted Reproduction . Williams & Wilkins , Baltimore , pp. 280–285.
Hall J , Fishel S , Green S , et al . ( 1995 ) Intracytoplasmic sperm injection versus high insemination concentration in-vitro fertilization in cases of very severe teratozoospermia . Human Reproduction 10 : 493 –496.
Hamamah S , Gatti J-L ( 1998 ) Role of the ionic environment and internal pH on sperm activity . Human Reproduction 13 (Suppl. 4): 20 –30.
Hinsch E , Ponce AA , Hägele W , et al . ( 1997 ) A new combined in-vitro test model for the identifi cation of substances aff ecting essential sperm functions . Human Reproduction 12 (8): 1673 –1681.
Hughes CM , McKelvey-Martin VJ , Lewis SE ( 1999 ) Human sperm DNA integrity assessed by the Comet and ELISA assays . Mutagenesis 14 (1): 71 –75.
Jager S , Kremer J , Van-Schlochteren-Draaisma T ( 1978 ) A simple method of screening for antisperm antibodies in the human male: detection of spermatozoa surface IgG with the direct mixed antiglobulin reaction carried out on untreated fresh human semen . International Journal of Fertility 23 : 12 .
Lessey BA , Garner DL ( 1983 ) Isolation of motile spermatozoa by density gradient centrifugation in Percoll . Gamete Research 7 : 49 –52.
Makler A ( 1978 ) A new chamber for rapid sperm count and motility evaluation . Fertility and Sterility 30 : 414 .
Matson PL ( 1995 ) External quality assessment for semen analysis and sperm antibody detection: results of a pilot scheme . Human Reproduction 10 : 620 –625.
Ménézo Y , Dale B ( 1995 ) Paternal contribution to successful embryogenesis . Human Reproduction 10 : 1326 –1327.
Menkveld R , Oettler EE , Kruger TF , et al . ( 1991 ) Atlas of Human Sperm Morphology. Williams & Wilkins , Baltimore .
Mortimer D ( 1991 ) Sperm preparation techniques and iatrogenic failures of in-vitro fertilization . Human Reproduction 6 (2): 173 –176.
Mortimer D ( 1994 ) Practical Laboratory Andrology. Oxford University Press , New York .
Pacey AA ( 2006 ) IS quality assurance in semen analysis still really necessary? A view from the andrology laboratory . Human Reproduction 21 (5): 1105 –1109.
Pacey AA ( 2010 ) Quality assurance and quality control in laboratory andrology . Asian Journal of Andrology 12 (1): 21 –25.
Rainsbury PA ( 1992 ) Th e treatment of male factor infertility due to sexual dysfunction. In: Brinsden PR , Rainsbury PA (eds.) In Vitro Fertilization and Assisted Reproduction. Parthenon Publishing Group , Carnforth, UK .
Sakkas D , Alvarez JG ( 2010 ) Sperm DNA fragmentation: mechanisms of origin, impact on reproductive outcome, and analysis . Fertility and Sterility 93 (4): 1027 –1036.
Sakkas D , Mariethosz E , St John J ( 1999 ) Abnormal sperm parameters in humans are indicative of an abortive apoptotic Mechanism linked to the FAS-Mediated pathway . Experimental Cell Research 251 : 350 –355.
Sakkas D , Urmer F , Bizzaro D , et al . ( 1998 ) Sperm nuclear DNA damage and altered chromatin structure: eff ect on fertilization and embryo development . Human Reproduction 13 (Suppl. 4): 11 –19.
Sato K , Tanaka F , Hasegawa H ( 2004 ) Appearance of the oocyte activation of mouse round spermatids cultured in vitro . Human Cell 17 (4): 177 –180.
Sousa M , Barros A , Tesarik J ( 1998 ) Current problems with spermatid conception . Human Reproduction 13 : 255 –258.
Stewart B ( 1998 ) New horizons in male infertility: the use of testicular and epididymal sperm in IVF . Alpha Newsletter 13 : 1 –3.
Tomlinson MJ , Pooley K , Simpson T , et al . ( 2010 ) Validation of a novel computer-assisted sperm analysis (CASA) system using multitarget-tracking algorithms . Fertility and Sterility 93 (6): 1911 –1920.
Twigg JP , Fulton N , Gomez E , et al . ( 1998a ) Analysis of the impact of intracellular reactive oxygen species generation on the structural and functional integrity of human spermatozoa and functional integrity of human spermatozoa: lipid peroxidation, DNA fragmentation and eff ectiveness of antioxidants . Human Reproduction 13 (6): 1429 –1436.
Twigg JP , Irvine DS , Aitken RJ ( 1998b ) Oxidative damage to DNA in human spermatozoa does not preclude pronucleus formation at intracytoplasmic sperm injection . Human Reproduction 13 (7): 1864 –1871.
Van den Berg M ( 1998 ) In: Elder K , Elliott T (eds.) Th e Use of Epidemiological and Testicular Sperm in IUF . World Wide Conferences on Reproductive Biology, Ladybrook Publishing , Australia .
Van der Ven H , Bhattacharya AK , Binor Z , Leto S , Zaneveld LJD ( 1982 ) Inhibition of human sperm capacitation by a high molecular weight factor from human seminal plasma . Fertility and Sterility 38 : 753 –755.

Chapter 10: Sperm and ART
156
Vanderzwalmen P , Zech H , Birkenfeld A , et al . ( 1997 ) Intracytoplasmic injection of spermatids retrieved from testicular tissue: infl uence of testicular pathology, type of selected spermatids and oocyte activation . Human Reproduction 12 : 1203 –1213.
Yovich JL ( 1992 ) Assisted reproduction for male factor infertility. In: Brinsden PR , Rainsbury PA (eds.) In
Vitro Fertilization and Assisted Reproduction . Parthenon Publishing Group , Carnforth, UK .
Yovich JM , Edirisinghe WR , Cummins JM , Yovich JL ( 1990 ) Infl uence of pentoxifylline in severe male factor infertility . Fertility and Sterility 53 : 715 –722.
World Health Organization ( 2010 ) WHO Manual for the Examination and Processing of Human Semen , 5th edn. WHO , Geneva .

Chapter
157
Oocyte retrieval and embryo culture
Preparation for each case Every individual treatment cycle involves a number of diff erent stages and manipulations in the laboratory, and each case must be assessed and prepared for in advance; the aft ernoon prior to the procedure (the day aft er hCG administration) is a convenient time to make the preparations. Th e laboratory staff should ensure that all appropriate consent forms have been signed by both partners, including consent for special procedures and storage of cryopreserved embryos . Details of any pre-vious assisted conception treatment should be studied, including response to stimulation, number and quality of oocytes, timing of insemination, fertilization rate, embryo quality and embryo transfer procedure, and judgements regarding whether any parameters at any stage could be altered or improved in the present cycle should be made. Th e risk of introducing any infection into the laboratory via gametes and samples must be absolutely minimized: screening tests such as human immunodefi ciency virus (HIV 1 and 2: Anti-HIV 1, 2) and hepatitis B (HbsAg/Anti-HBc) and C (Anti-HCV-Ab) should be confi rmed, as well as any other tests indicated by the patients’ history (e.g., HTLV-I antibody, RhD, malaria, Trypanosoma cruzi ). If donor gametes are to be used, additional tests for the donor are required: chlamydia, cytomegalovirus and a validated testing algorithm to exclude the presence of active infec-tion with Treponema pallidum for syphilis testing.
Laboratory preparation: checklist for each case
• Results of viral screening tests for both partners Consent forms signed by both partners • Specifi c details or instructions regarding insem-• ination, cryopreservation, number of embryos for transfer, etc.
• Results of viral screening tests for both partners Consent forms signed by both partners• Specifi c details or instructions regarding insem-•ination, cryopreservation, number of embryos for transfer, etc.
Results of semen assessments; note any special • features or precautions for semen collection or preparation • Previous history, current response to stimulation; note any special features of ultrasound scans, endo-crine assays, or IVF laboratory results Current cycle history: number of follicles, endocrine • parameters, potential ovarian hyperstimulation syn-drome (OHSS)
Laboratory case notes, media, culture vessels and tubes for sperm preparation, with clear and adequate labeling throughout should be prepared. All labeling should have a minimum of the patient’s full name and a unique identifi er, for example patient number. When donor sperm is used, the donor code should uniquely identify that specifi c donor. Tissue culture dishes or plates must be equilibrated in the CO 2 incubator over-night. Th e choice of culture system used is a matter of individual preference and previous experience; micro-droplets under oil, four-well dishes and organ culture dishes are amongst those most commonly used.
Microdroplets under oil Pour previously equilibrated mineral oil into • 60 mm Petri dishes that are clearly marked with each patient’s full name . Using either a Pasteur pipette or adjustable • pipettor and sterile tips, carefully place eight or nine droplets of medium around the edge of the dish. One or two droplets may be placed centrally, to be used as wash drops. Examine the follicular growth records to assess • approximately how many drops/dishes should be prepared; each drop may contain one or two oocytes. Droplet size can range from 50 to 250 µL per droplet.
Results of semen assessments; note any special• features or precautions for semen collection orpreparation
• Previous history, current response to stimulation;note any special features of ultrasound scans, endo-crine assays, or IVF laboratory results Current cycle history: number of follicles, endocrine•parameters, potential ovarian hyperstimulation syn-drome (OHSS)
11
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. (©) K. Elder and B. Dale 2011.

Chapter 11: Oocyte retrieval and embryo culture
158
Four-well plates Th is system may also be used in combination with an overlay of equilibrated mineral oil.
Prepare labeled and numbered plates containing • 0.5–1 mL of tissue culture medium; each well is normally used to incubate up to three oocytes. Equilibrate overnight – if used without an oil • overlay, the incubator must be humidifi ed . Small Petri dishes with approximately 2 mL of • HEPES-containing medium may also be prepared, to be used for washing oocytes immediately aft er identifi cation in the follicular aspirates (media containing HEPES should not be equilibrated in a CO 2 atmosphere).
Organ culture (center-well) dishes can also be used for group culture: place three 250 µL drops in the cen-ter well, and three to four oocytes in each drop.
Laboratory supplies for labeling and preparation
• Pots for semen collection Test-tubes for sperm preparation: conical tubes, • small and large round-bottomed tubes Aliquots of media for each patient • Culture vessels for overnight equilibration • Paperwork for recording case details and results •
Oocyte retrieval (OCR) and identifi cation A Class II biological safety cabinet is recommended for handling of follicular aspirates to avoid risk of infec-tion, but be aware that the laminar fl ow of air can have a dramatic cooling eff ect on the samples.
Prior to the follicle aspiration procedure : 1. Ensure: heating blocks, stages and trays are
warmed to a temperature that will maintain the medium in the dishes at 37°C; media to be used for fl ushing/rinsing must also be warmed and equilibrated to correct pH.
2. Prewarm collection test-tubes and 60 mm Petri dishes for scanning aspirates.
3. Prepare a sterile Pasteur pipette plus holder, a fi ne-drawn blunt Pasteur pipette as a probe for manipulations, and 1 mL syringes with attached needles for dissection.
4. Check patient ID, confi rm names and unique identifi ers on dishes and laboratory case notes with medical notes.
If follicular aspirates cannot be examined immedi-ately, they should be collected into test-tubes that are completely fi lled with fl uid, tightly sealed, and rigor-ously maintained at 37°C until they reach the labora-tory. Aliquot the contents of each test-tube into two or three Petri dishes, forming a thin layer of fl uid that can be quickly, carefully and easily scanned for the presence of an oocyte, using a stereo dissecting microscope with transmitted illumination base and heated stage. Low-power magnifi cation (×6–12) can be used for scan-ning the fl uid, and oocyte identifi cation verifi ed using higher magnifi cation (×25–50). Always work quickly and carefully, with rigid attention to sterile technique, maintaining correct temperature and pH at all times .
Oocyte identifi cation Th e oocyte usually appears within varying quantities of cumulus cells and, if very mature, may be pale and diffi -cult to see (immature oocytes are dark and also diffi cult to see). Granulosa cells are clearer and more “fl uff y,” present in amorphous, oft en iridescent clumps. Blood clots, especially from the collection needle, should be carefully dissected with 23-gauge needles to check for the presence of cumulus cells.
Th e presence of blood clots within the cumulus–oocyte complex (COC) may be a refl ection of poor fol-licular development, with an eff ect on the competence of the corresponding oocyte (Ebner, 2008 ). When a COC is identifi ed, assess its stage of maturity by noting the vol-ume, density and condition of the surrounding cumu-lus cells and the expansion of coronal cells. It is unlikely that the oocyte itself can be seen, since it will most com-monly be surrounded by cumulus cells. However, when an oocyte can be observed with minimal cumulus cells, the presence of a single polar body indicates that it has reached the stage of metaphase II. Th e appearance of the COC can be used to classify the oocyte according to the following scheme ( Figure 11.1 ):
1. Germinal vesicle : the oocyte is very immature. Th ere is no expansion of the surrounding cells, which are tightly packed around the oocyte. A large nucleus (the germinal vesicle) is still present and may occasionally be seen with the help of an inverted microscope. Maturation occasionally takes place in vitro from this stage, and germinal vesicles are preincubated for 24 hours before insemination ( Figure 11.1e ).
2. Metaphase I : the oocyte is surrounded by a tightly apposed layer of corona cells; tightly
• Pots for semen collection Test-tubes for sperm preparation: conical tubes,•small and large round-bottomed tubes Aliquots of media for each patient • Culture vessels for overnight equilibration• Paperwork for recording case details and results •

Chapter 11: Oocyte retrieval and embryo culture
159
(c)
(d) (e)
(a) (b)
Figure 11.1 Images after oocyte retrieval, before and after hyaluronidase denudation. Cumulus–oocyte complexes, without denudation: (a) Cumulus–oocyte complex visualized under dissecting microscope, ×25 magnifi cation. See color plate section; (b) phase-contrast image of mature metaphase II cumulus–oocyte complex, fi rst polar body visible. See color plate section; (c) cumulus–oocyte complex with clumped refractile areas indicating signs of luteinization. See color plate section; (d) empty zona pellucida. Phase contrast images after denudation: (e) Germinal vesicle; (f) metaphase I oocyte, polar body not extruded; (g) preovulatory metaphase II oocyte, polar body extruded; (h) postmature oocyte, showing granularity in the perivitelline space; (i) dysmorphic metaphase II oocyte showing a large necrotic fi rst polar body. (Images (h) and (i) courtesy of Thomas Ebner, Austria.)

Chapter 11: Oocyte retrieval and embryo culture
160
packed cumulus with little extracellular matrix may surround this with a maximum size of approximately fi ve oocyte diameters. If the oocyte can be seen, it no longer shows a germinal vesicle. Th e absence of a polar body indicates that the oocyte is in metaphase I, and these immature oocytes can be preincubated for 6–24 hours before insemination ( Figure 11.1f ).
3. Metaphase II (a) Preovulatory (harvested from Graafi an
follicles): this is the optimal level of maturity, appropriate for successful fertilization. Coronal cells are still apposed to the oocyte, but are fully radiating; one polar body has been extruded. Th e cumulus has expanded into a fl uff y viscous mass that can be easily stretched, with abundant extracellular matrix ( Figure 11.1a and b ).
(b) Mature : the oocyte can oft en be seen clearly as a pale orb; little coronal material is present and is dissociated from the oocyte. Th e cumulus is very profuse but is still cellular. Th e latest events of this stage involve a condensation of cumulus into small black (refractile) drops, as if a tight corona is reforming around the oocyte. Th e perivitelline space oft en shows granularity ( Figure 11.1h ).
(c) Luteinized : the oocyte is very pale and oft en is diffi cult to fi nd. Th e cumulus has broken down and becomes a gelatinous mass around the oocyte. Th ese oocytes have a low probability of fertilization, and are usually inseminated with little delay (Figure 11.1).
(d) Atretic : the oocyte is very dark, and can be diffi cult to identify. Granulosa cells are fragmented, and have a lace-like appearance.
(f) (g)
(h)
Figure 11.1 (cont.)
(i)

Chapter 11: Oocyte retrieval and embryo culture
161
Gross morphological assessment of oocyte matur-ity is highly subjective, and open to inaccuracies. In preparation for intracytoplasmic sperm injection (ICSI), the oocytes are completely denuded of sur-rounding cells using hyaluronidase, allowing accurate assessment of nuclear maturity and cytoplasm; this process has made it apparent that gross COC morph-ology does not necessarily correlate with nuclear maturity, and there is considerable confl ict in the data available regarding the association between oocyte morphology and treatment outcome (see Ebner, 2006 , for review). A number of dysmorphic features can be identifi ed in denuded oocytes, including areas of necrosis, organelle clustering, vacuolation or accumu-lating aggregates of smooth endoplasmic reticulum (sER). Anomalies of the zona pellucida and nonspher-ical oocytes can also be seen. In practice, a wide var-iety of unusual and surprising dysmorphisms are oft en observed – please refer to the image database at www.ivf.net for an interesting collection of photographs and histories.
Some features of dysmorphism may be associ-ated with the endocrine environment during ovar-ian stimulation, in particular the structure of the zona pellucida and/or oolemma (Ebner, 2002 , 2006 ). Although aberrations in the morphology of oocytes are not necessarily of any consequence to fertiliza-tion or early cleavage aft er ICSI, it is possible that embryos generated from dysmorphic oocytes have a reduced potential for implantation and further devel-opment. Repeated appearance of some dysmorphic features such as sER aggregation, central granulation or vacuoles in an individual patient’s oocyte cohort may indicate an underlying intrinsic problem in the process of oocyte development within the ovary .
Dysmorphic oocyte features ( Figure 11.2 )
• Irregular shape Areas of necrosis in the cytoplasm • Cytoplasmic granularity • Organelle clustering • Aggregates of sER • Vacuoles/Vesicles • Anomalies of the zona pellucida •
Van Blerkom and Henry ( 1992 ) reported aneuploidy in 50% of oocytes with cytoplasmic dysmorphism; it is not clear whether oocyte aneuploidy is a fundamental devel-opmental phenomenon, or a patient-specifi c response to induced ovarian stimulation. In 1996, the same group related the oxygen content of human follicular fl uid to
oocyte quality and subsequent implantation potential. Th ey propose that low oxygen tension associated with poor blood fl ow to follicles lowers the pH and produces anomalies in chromosomal organization and micro-tubule assembly, which might cause segregation disor-ders. Measurement of blood fl ow to individual follicles by power color Doppler ultrasound (Gregory and Leese, 1996 ) confi rmed the observations of Van Blerkom et al . ( 1997 ) in correlating follicular blood fl ow with implant-ation; the incidence of triploid zygotes was also found to be signifi cantly higher when oocytes were derived from follicles with poor vascularity. Follicular vascularity may also infl uence free cortisol levels in follicular fl uid by pro-moting its diff usion across the follicle boundary.
Insemination Oocytes are routinely inseminated with a concentration of 100 000 progressively motile sperm per milliliter. If the prepared sperm show suboptimal parameters of motility or morphology, the insemination concentra-tion may be accordingly increased. Some reports have suggested that the use of a high insemination concen-tration of up to 300 000 progressively motile sperm per milliliter may be a useful prelude before deciding upon ICSI treatment for male factor patients. Traditionally, inseminated oocytes were incubated overnight in the presence of the prepared sperm sample; however, sperm binding to the zona pellucid a normally takes place within 1–3 hours of insemination, and fertil-ization occurs very rapidly thereaft er. A few hours of sperm–oocyte contact, yields the same time course of events that is observed aft er overnight incubation, and oocytes can be washed free of excess sperm aft er 3 hours incubation (Gianaroli et al ., 1996; Ménézo and Barak, 2000 ).
For a culture system of microdroplets under oil, each oocyte is transferred into a drop containing motile sperm at a concentration of approximately 100 000 sperm/mL. In a four-well system, a measured volume of prepared sperm is added to each well, to a fi nal concentration of approximately 100 000 progres-sively motile sperm per well.
Insemination
For microdroplets under oil, the oil overlays for insem-ination dishes must be prepared earlier, so that there is at least 4–6 hours of equilibration time .
1. Prepare a dilution of prepared sperm, containing 100 000 motile sperm/mL
• Irregular shape Areas of necrosis in the cytoplasm• Cytoplasmic granularity • Organelle clustering • Aggregates of sER • Vacuoles/Vesicles• Anomalies of the zona pellucida •
For microdroplets under oil, the oil overlays for insem-ination dishes must be prepared earlier, so that thereis at least 4–6 hours of equilibration time .
1. Prepare a dilution of prepared sperm, containing100 000 motile sperm/mL

Chapter 11: Oocyte retrieval and embryo culture
162
• Assess a drop of the dilution on a glass slide, under ×10 magnifi cation – at least 20 motile sperm should be visible in the fi eld. Equilibrate the suspension at 37• °C for 30 minutes, 5% CO
2 .
Place droplets of the sperm suspension under the • previously prepared and equilibrated oil overlays. Examine each oocyte before transfer to the insem-• ination drop, and dissect the cumulus to remove bubbles, large clumps of granulosa cells or blood clots if necessary.
2. If oocytes are in pre-measured culture droplets, e.g., 240 µL, add 10 µL of a prepared sperm suspen-sion that has been adjusted to 2.5 ×10 6 /mL. Final concentration = approximately 100 000 • sperm/mL, or 25 000 sperm per oocyte.
3. Prepare labeled 35 mm Petri dishes containing equilibrated oil, to be used for culture of the zygotes after scoring for fertilization the following day .
Four-well dishes and organ culture dishes
Add 0.5–1.0 mL of prepared sperm suspension to • each well or drop. Total: approximately 100 000 motile sperm per well/• drop.
Scoring of fertilization on Day 1 Dissecting fertilized oocytes Inseminated oocytes are dissected 17–20 hours fol-lowing insemination in order to assess fertilization. Oocytes at this time are normally covered with a layer of dispersed coronal and cumulus cells, which must be carefully removed so that the cell cytoplasm can be examined for the presence of two pronuclei and two polar bodies, indicating normal fertiliza-tion. Th e choice of dissection procedure is a matter of
• Assess a drop of the dilution on a glass slide,under ×10 magnifi cation – at least 20 motilesperm should be visible in the fi eld. Equilibrate the suspension at 37• °C for 30 minutes,5% CO
2.
Place droplets of the sperm suspension under the•previously prepared and equilibrated oil overlays. Examine each oocyte before transfer to the insem-•ination drop, and dissect the cumulus to removebubbles, large clumps of granulosa cells or bloodclots if necessary.
2. If oocytes are in pre-measured culture droplets,e.g., 240 µL, add 10 µL of a prepared sperm suspen-sion that has been adjusted to 2.5 ×10 6 /mL. Final concentration = approximately 100 000• sperm/mL, or 25 000 sperm per oocyte.
3. Prepare labeled 35 mm Petri dishes containingequilibrated oil, to be used for culture of the zygotesafter scoring for fertilization the following day .
Four-well dishes and organ culture dishes
Add 0.5–1.0 mL of prepared sperm suspension to• each well or drop. Total: approximately 100 000 motile sperm per well/•drop.
Figure 11.2 Normal and dysmorphic oocytes (A, B). Normal appearing oocytes with no visually outstand-ing features (C–F). Varying degrees of organelle clusters (*) (central granular-ity) observed from mild to very severe. (G, N) Aggregation (arrows) of smooth endoplasmic reticulum as a fl at, clear disc in the middle of the cytoplasm of the oocyte. (H) A dark “horse shoe shaped” (large arrow) cytoplasmic inclusion. (I, J, K) Varying degrees (mild to severe) of fl uid-fi lled vacuoles within the cytoplasm. (L) Organelle cluster with fragmented polar body (arrow) and increased perivitelline debris (*) and space. (K–M) Combination of cytoplasmic dysmorphisms and extra-cytoplasmic phenotypes. PB1 = fi rst polar body. (From: Meriano et al ., 2001 Human Reproduction 16(10): 2118–23, with per-mission from Oxford University Press).

Chapter 11: Oocyte retrieval and embryo culture
163
individual preference, and sometimes a combination of methods may be necessary for particular cases. Whatever the method used, it must be carried out carefully, delicately and speedily, taking care not to expose the fertilized oocytes to changes in tempera-ture and pH. Scoring for pronuclei should be carried out within the appropriate time span, before pro-nuclei merge during syngamy: cleaved embryos with abnormal fertilization are indistinguishable from those with two pronuclei.
Dissection techniques 1. Narrow-gauge pipetting : narrow-gauge pipettes
can be made (see below), but commercial hand-held pipetting devices are simpler and more convenient. “Flexipet” and “Stripper” are hand-held pipetting devices for cumulus/corona removal, with sterile disposable polycarbonate capillaries of specifi ed inner diameters ranging from 135 up to 175 or 600 µm. Variations that incorporate a capillary that attaches to a tiny pressure “bulb” inserted into a hollow metal tube are also available, e.g., Swemed.
Use the microscope at ×25 magnifi cation, and • choose a tip with a diameter slightly larger than the oocyte (a tip that is too small will damage the oocyte, therefore take care in selecting the appropriate diameter). Aspirate approximately 2 cm of clean culture • medium into the tip, providing a protective buff er. Th is allows easy fl ushing of the oocyte, and prevents it from sticking to the inside surface of the tip. Place the tip over the oocyte and gently • aspirate it into the shaft . If the oocyte does not easily enter, change • to a larger diameter pipette (however, if the diameter is too large, it will be ineff ective for cumulus removal ). Gently aspirate and expel the oocyte through • the pipette, retaining the initial buff er volume, until suffi cient cumulus and corona is removed to allow clear visualization of the cell cytoplasm and pronuclei.
2. Needle dissection : use two 26-gauge needles attached to 1 mL syringes, microscope at ×25 magnifi cation. Use one needle as a guide, anchoring a piece of cellular debris if possible; slide the other needle down the fi rst one, “shaving”
cells from around the zona pellucida , with a scissors-like action.
3. Rolling : use one 23-gauge needle attached to a syringe, and a fi ne glass probe. With the microscope at ×12 magnifi cation, use the needle to score lines in each droplet on the base of the plastic dish. Adjust the magnifi cation to ×25, and push the oocyte gently over the scratches with a fi re polished glass probe until the adhering cells are teased away. Th is technique may be helpful to remove adherent sticky blood clots. However, it should not be used with dishes that are coated with a specifi c non-embryotoxic layer.
Great care must be taken with any technique to avoid damaging the zona pellucida or the oocyte either by puncture or overdistortion. Breaks or cracks in the zona can sometimes be seen, and a small portion of the oocyte may extrude through the crack (this may have occurred during dissection or during the aspiration process). Occasionally the zona is very fragile, fractur-ing or distorting at the slightest touch; it is probably best not to continue the dissection in these cases.
Making narrow-gauge pipettes
The preparation of fi nely drawn pipettes with an inner diameter slightly larger than the circumference of an oocyte is an acquired skill which requires practice and patience.
Hold both ends of the pipette, and roll an area • approximately 2.5 cm below the tapered section of the pipette over a gentle fl ame (Bunsen or spirit burner). As the glass begins to melt, quickly pull the pipette • in both directions to separate. Before the glass has a chance to cool, carefully • and quickly break the pipette at an appropriate position. The tip must have a clean break, without rough or • uneven edges; these will damage the oocyte during dissection. Examine the tip of each pipette to ensure that it is of • accurate diameter, with smooth clean edges .
Pronuclear scoring An inverted microscope is recommended for accurate scoring of fertilization; although the pronuclei can be seen with dissecting microscopes, it can oft en be dif-fi cult to distinguish normal pronuclei from vacuoles or other irregularities in the cytoplasm. Normally fer-tilized oocytes should have two pronuclei, two polar
The preparation of fi nely drawn pipettes with an innerdiameter slightly larger than the circumference of anoocyte is an acquired skill which requires practice andpatience.
Hold both ends of the pipette, and roll an area•approximately 2.5 cm below the tapered sectionof the pipette over a gentle fl ame (Bunsen or spiritburner). As the glass begins to melt, quickly pull the pipette• in both directions to separate. Before the glass has a chance to cool, carefully•and quickly break the pipette at an appropriateposition. The tip must have a clean break, without rough or•uneven edges; these will damage the oocyte duringdissection. Examine the tip of each pipette to ensure that it is of • accurate diameter, with smooth clean edges .

Chapter 11: Oocyte retrieval and embryo culture
164
bodies, regular shape with intact zona pellucida , and a clear healthy cytoplasm. A variety of diff erent features may be observed: the cytoplasm of normally fertilized oocytes is usually slightly granular, whereas the cyto-plasm of unfertilized oocytes tends to be completely clear and featureless. Th e cytoplasm can vary from slightly granular and healthy-looking, to brown or dark and degenerate. Th e shape of the oocyte may also vary, from perfectly spherical to irregular (see Figure 11.2 ). A clear halo of peripheral cytoplasm 5–10 mm thick is an indication of good activation and re-initia-tion of meiosis. Th e pattern and alignment of nucleoli may also be signifi cant (Scott and Smith 1998 ; Tesarik and Greco, 1999 ).
Approximately 5% of fertilized oocytes in human IVF routinely show abnormal fertilization, with three or more pronuclei visible; this is attributed to polyspermy, or non-extrusion of the second polar body. Fluorescent in-situ hybridization (FISH) ana-lysis indicates that 80–90% of these zygotes are mosaic aft er cleavage. Single pronucleate zygotes obtained aft er conventional IVF analyzed by FISH to determine their ploidy, reveal that a proportion of these zygotes are diploid (Levron et al ., 1995 ). It seems that during the course of their interaction, it is possible for human gamete nuclei to associate together and form diploid, single pronucleate zygotes. Th ese fi ndings may indicate a variation of human pronuclear interaction during syngamy, and the authors suggest that single pronucle-ate zygotes which develop with normal cleavage may be selected for transfer in cases where no other suitable embryos are available.
Details of morphology and fertilization should be recorded for each zygote, for reference when choosing embryos for transfer. Remove zygotes with normal fer-tilization at the time of scoring from the insemination drops or wells, transfer into new dishes or plates con-taining pre-equilibrated culture medium, and return them to the incubator for a further 24 hours of culture. Th ose with abnormal fertilization such as multipronu-cleate zygotes should be discarded, so that there is no possibility of their being selected for embryo transfer; aft er cleavage these are indistinguishable from nor-mally fertilized oocytes.
Although the presence of two pronuclei confi rms fertilization, their absence does not necessarily indicate fertilization failure, and may instead represent either parthenogenetic activation, or a delay in timing of one or more of the events involved in fertilization ( Figure 11.3 ). Numerous studies have accumulated evidence to
demonstrate that up to 40% of oocytes with no sign of fertilization 17–27 hours aft er insemination may have the appearance of morphologically normal embryos on the following day, with morphology and cleavage rate similar to that of zygotes with obvious pronuclei on Day 1. However, around a third of these zygotes may subsequently arrest on Day 2 (Plachot et al ., 1993 ). Cytogenetic analysis of these embryos reveals a higher incidence of chromosomal anomalies and a high rate of haploidy, confi rming parthenogenetic activation (Plachot et al ., 1988 , 1993 ).
Delayed fertilization with the appearance of pro-nuclei on Day 2 may also be observed, and these embryos also tend to have an impaired developmen-tal potential. Delayed fertilization can be attributed to morphological or endocrine oocyte defects in some cases, and to sperm defects in others. No obvious asso-ciation with either oocyte or sperm defects can be found in a number of cases (Oehninger et al ., 1989 ).
Reinsemination Reinsemination of oocytes that fail to demonstrate clear pronuclei at the time of scoring for fertilization is a practice that has been widely questioned scientif-ically. Fertilization or cleavage may subsequently be observed on day 2, but this may be as a consequence of the initial insemination, and the delay in fertil-ization may be attributed either to functional disor-ders of the sperm, or maturation delay of the oocyte. Th ese embryos generally have a poor prognosis for implantation.
“Rescue ICSI” is another option, whereby unfer-tilized oocytes are microinjected with a single sperm from the original sample. Th is practice is banned in some countries such as the UK, since it cannot be cer-tain if a sperm has already entered the oocyte and fer-tilization is delayed. Others reserve rescue ICSI only for cases where there is complete failure to fertilize following conventional IVF. A recent report indicates that a better pregnancy rate can be achieved follow-ing rescue ICSI if the fertilized oocytes are frozen and transferred in a subsequent frozen-thawed cycle, to ensure better synchronization of the embryo and uterus for implantation (Sermondade et al ., 2010 ).
Selection of pronucleate embryos for cryopreservation Legislation in some countries forbids embryo freezing, but allows cryopreservation at the zygote stage, before

Chapter 11: Oocyte retrieval and embryo culture
165
(a) (b)
(c) (d)
Figure 11.3 Phase contrast micrographs of fertilized human oocytes. (a) Normal fertilization: two pronuclei, one polar body. See color plate section. (b) Abnormal fertilization: three pronuclei. See color plate section. (c) Abnormal fertilization, no pronuclei, two polar bodies. (d) Zygote showing two pronuclei, numerous vacuoles, and irregular perivitelline space, illustrating that severely dysmorphic oocytes are capable of fertilization (with thanks to Marc van den Bergh).
syngamy. In countries that allow both zygote and embryo freezing, a patient who has a large cohort of oocytes with two clearly visible pronuclei on Day 1 may have a selected number kept in culture for transfer on Day 2 or 3, and the remainder considered for pronucle-ate stage cryopreservation. Th e decision as to number of embryos to be frozen at the pronucleate stage should take into consideration the patient’s previous history regarding cleavage and quality of embryos. Zygotes to be frozen should have a regular outline, distinct zona and clearly visible pronuclei. Th e cryopreservation procedure must be initiated while the pronuclei are still visible, before the onset of syngamy.
Selection of embryos for transfer Historically, embryo transfer was carried out 2 days (approximately 48–54 hours) aft er oocyte retrieval, but transfer has been carried out from as early as one hour post-ICSI (AOT, activated oocyte transfer, Dale et al ., 1999 ) to 5 days later, at the blastocyst stage . Trials of zygote transfer on Day1 also achieved acceptable preg-nancy rates (Scott and Smith, 1998 ; Tesarik and Greco, 1999; Tesarik et al ., 2000 ); it seems that the specifi c timing of transfer may not be crucial for the human implantation process. On Day 2, cleaved embryos may contain from two to six blastomeres. Embryo transfer

Chapter 11: Oocyte retrieval and embryo culture
166
one day later, on Day 3, or on Day 5 at the blastocyst stage is advocated as a means of selecting better quality embryos, by the elimination of those that arrest at earl-ier cleavage stages in vitro.
Sequence of events observed by time-lapse cinematography (Mio and Maeda, 2008 )
Day 0 = day of OCR, insemination approximately 4–5 hours post OCR.
Activation of the zygote genome begins at this stage, with massive increase in transcription and trans-lation; this cell cycle requires a full 24 hours.
By 96 hours post insemination, on Day 4: compact-ing morula stage (around 32 cells).
Day 5: diff erentiation to blastocyst stage. Cell num-ber may vary considerably, from 50 to 100–120 cells for early expanding blastocysts.
Hatching may start as early as the morning of Day 5, but is usually observed on Day 6/7.
Two major problems continue to hinder the eff ect-iveness of ART treatment: low implantation rates and a high incidence of multiple pregnancies. Poor endomet-rial receptivity and adverse uterine contractions can both contribute to early embryo loss, but the low effi ciency of assisted conception is widely attributed to genetic defects in the embryo. More than 40% of ART-derived embryos are known to harbor chromosomal abnormalities. Errors in meiotic and mitotic segregation of chromosomes
in the oocyte and during the cleavage of early embryos can lead to diff erent patterns of aneuploidy, includ-ing polyploidy and chaotic mosaics, which account for around one-third of aneuploidies involving more than one chromosome per cell. However, despite the fact that grossly abnormal chromosome complements are lethal, in most cases the morphology of embryos that are genet-ically normal does not diff er markedly from those with aneuploid, polyploid or mosaic chromosomal comple-ments. Consequently, genetically abnormal embryos aft er IVF or ICSI may be graded as suitable for transfer using subjective selection criteria. Developing a reliable diagnostic test that can be used to identify embryos with the greatest developmental competence continues to be a major priority in human ART, in the hope of eventu-ally selecting a single embryo that is likely to result in a healthy live birth following transfer.
In selecting embryos for transfer, the limitations of evaluating embryos based on morphological criteria alone are well recognized: correlations between gross morphology and implantation are weak and inaccur-ate, unless the embryos are clearly degenerating/frag-mented. Objective criteria for evaluating embryos are available in laboratories with research facilities, but may be out of reach for a routine clinical IVF laboratory without access to specialized equipment and facilities. Objective measurements of human embryo viability that have been applied include:
High-resolution videocinematography • Computer-assisted morphometric analysis • Blastomere or polar body biopsy for cytogenetic • analysis Culture of cumulus cells • Oxygen levels in follicular fl uid /perifollicular • vascularization Distribution of mitochondria and ATP levels in • blastomeres Metabolic assessment of culture media (amino • acid profi ling, metabolomics) Gene expression/expression of mRNA in cumulus • cells and/or embryos.
High-resolution videocinematography As early as 1989, Cohen et al . carried out a classic experi-ment that aimed to clearly defi ne morphological cri-teria that might be used for embryo assessment, using a detailed analysis of videotaped images. Immediately before embryo transfer, embryos were recorded on VHS for 30–90 seconds, at several focal points, using Nomarski
Hours post insemination:
Observation:
1.5 ± 0.2 Sperm penetrated2.0 ± 0.2 Sperm incorporated2.5 ± 1.2 Second polar body extruded2.5 ± 0.5 Cone appearance (interaction
between sperm midpiece and oocyte plasma membrane)
3.7 ± 0.7 Appearance of cytoplasmic fl are (may represent sperm aster)
4.5 ± 0.8 Cone disappears5.5 ± 0.5 Cytoplasmic fl are disappears6.6 ± 0.3 Male pronucleus formed6.8 ± 0.3 Female pronucleus formed8.8 ± 0.7 Both pronuclei abutted9.0 ± 0.5 Halo appears19.2 ± 1.1 Halo disappears24.8 ± 1.0 Syngamy27.3 ± 1.0 First cleavage commenced37.2 ± 1.2 Second cleavage commenced
Day 0 = day of OCR, insemination approximately 4–5hours post OCR.
Activation of the zygote genome begins at thisstage, with massive increase in transcription and trans-lation; this cell cycle requires a full 24 hours.
By 96 hours post insemination, on Day 4: compact-ing morula stage (around 32 cells).
Day 5: diff erentiation to blastocyst stage. Cell num-ber may vary considerably, from 50 to 100–120 cells forearly expanding blastocysts.
Hatching may start as early as the morning of Day5, but is usually observed on Day 6/7.
Hours post insemination:
Observation:
1.5 ± 0.2 Sperm penetrated2.0 ± 0.2 Sperm incorporated2.5 ± 1.2 Second polar body extruded2.5 ± 0.5 Cone appearance (interaction
between sperm midpieceand oocyte plasma membrane)
3.7 ± 0.7 Appearance of cytoplasmicfl are (may represent sperm aster)
4.5 ± 0.8 Cone disappears5.5 ± 0.5 Cytoplasmic fl are disappears6.6 ± 0.3 Male pronucleus formed6.8 ± 0.3 Female pronucleus formed8.8 ± 0.7 Both pronuclei abutted9.0 ± 0.5 Halo appears19.2 ± 1.1 Halo disappears24.8 ± 1.0 Syngamy27.3 ± 1.0 First cleavage commenced37.2 ± 1.2 Second cleavage commenced

Chapter 11: Oocyte retrieval and embryo culture
167
optics and an overall magnifi cation of ×1400. Th e record-ings were subsequently analyzed by observers who were unaware of the outcome of the IVF procedure, and they objectively assessed a total of 11 diff erent parameters:
Nine parameters were judged (+) or (–), and vari-ation in zona thickness and percentage of extracellu-lar fragments were given a numerical value. Analysis of these criteria showed no clear correlation with any intracellular features of morphology, but that the most important predictor of fresh embryo implantation was the percentage of variation in thickness of the zona pellucida . Embryos with a thick, even zona had a poor prognosis for implantation; those whose zona had thin patches also had “swollen,” more refractile blast-omeres, and had few or no fragments. Th is observation was one of the parameters that led the group to intro-duce the use of assisted hatching (see Chapter 13 ). In analyzing frozen-thawed embryos, the best predictor of implantation was cell–cell adherence. Th e propor-tion of thawed embryos with more than one abnormal-ity (77%) was higher than that of fresh embryos (38%) despite similar implantation rates (18% versus 15%).
More than twenty years have elapsed since these observations were published, and the quest to identify specifi c morphological markers of embryo implant-ation potential still continues – now with the help of more sophisticated technology to measure both prop-erties of the zona and detailed embryo morphology .
Zona pellucida birefringence Polarized microscopy allows three layers to be distin-guished in the zona, with the innermost layer show-ing the greatest birefringence (i.e., a higher level of light retardance). Several studies have investigated a possible correlation between this zona property and implantation potential (Montag et al ., 2008 ; Madaschi et al ., 2009 ); there is no doubt that properties of the zona may be important in assessing oocyte/embryo
potential, particularly in response to exogenous FSH stimulation, but further studies are required in order to establish a clear correlation.
Computer-assisted morphometric analysis High-resolution digital images of embryos can be assessed in detail with the help of computer-assisted multilevel analysis, which provides a three- dimensional picture of embryo morphology. Th e FertiMorph multi-level system from IH-Medical , Denmark is equipped with a computer-controlled motorized stepper mounted on the microscope, and this system will automatically focus through diff erent focal planes in the embryo to produce a sequence of digital images. Automatic calcu-lations of morphometric information from the image sequences describe features and measurements of each embryo, including size of nucleus and blastomeres and their spatial positions within the embryo, as well as features of the zona pellucida ; all of the information is stored in a database. To date, clinical results following the use of this system are limited. Preliminary results indicated that implantation was aff ected by the num-ber and size of blastomeres on Day 3, and prediction of embryo implantation was superior to that of trad-itional manual scoring systems (Paternot et al ., 2009 ). Additional information about morphology and embryo development is also accumulating from the use of mod-ern systems that allow time-lapse photography in com-bination with culture systems.
Aneuploidy screening Cytogenetic analysis of a biopsied polar body or blasto-mere can be used to screen embryos in order to detect those with an abnormal chromosome composition, a strategy known as aneuploidy screening or preim-plantation genetic screening (PGS) . Th e techniques employed for biopsy and diagnosis are described in Chapters 13 and 14 , as well as the associated pros and cons. PGS has been a subject of considerable debate (Kuliev and Verlinsky, 2008 ; Mastenbroek et al ., 2008 ; Sermondade and Mandelbaum, 2009 ), and it is now discouraged in guidelines issued by the European Society for Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM).
Follicular indicators of embryo health Each assisted conception cycle generates a number of waste products: luteinized granulosa cells, follicular
Cell organelles visible Cellular extrusions
Blastomeres all intact Cytoplasmic vacuoles
Identical blastomere size Blastomeres contracted
Smooth membranes % variation in zona thickness
Dark blastomeres % extracellular fragments
Cell–cell adherence

Chapter 11: Oocyte retrieval and embryo culture
168
fl uids harvested from follicles at the time of oocyte retrieval and cumulus cells that can be removed and separated from the oocytes. Th ese products have all been assayed to provide indices of embryo develop-mental competence. Biomarkers quantifi ed in serum and follicular fl uid include cytokines, C-reactive pro-tein and leptin (Wunder et al ., 2005 ), inhibin B (Chang et al ., 2002 ) and reactive oxygen species (Das et al ., 2006 ). Cumulus cell gene expression profi les have also been linked to the implantation potential of oocytes and embryos (McKenzie et al ., 2004 ). While many of these parameters are indicative of follicular diff eren-tiated status at the time of oocyte harvest, follicular fl uid is a highly concentrated cellular exudate, which is accumulated over an extended period. Consequently, to date neither follicular fl uid nor granulosa cell assays at the time of oocyte collection have provided a consist-ent measure for assessing the implantation potential of individual embryos. Th e degree of follicular vascular-ization and its relationship to mitochondrial segrega-tion in embryonic blastomeres has also been promoted as a determinant of embryo developmental compe-tence (Van Blerkom et al ., 2000 ).
Secreted factors Assessment of products secreted by the embryo, the embryonic “secretome,” may be a better indicator of embryo development in vitro and in vivo than meas-urements of the follicular environment. For example, secretion of factors that regulate gamete transport and/or prepare the female tract for implantation has been used to predict embryo health. In this context, measurement of the amount of soluble human leuko-cyte antigen-G (HLA-G) into embryo culture media has been directly related to embryo quality and via-bility (Sher et al ., 2004 ). mRNAs for HLA-G can be detected in human blastocysts , but the cellular origins and biology of soluble HLA-G are not clear (Sargent, 2005 ). Th e suitability of HLA-G as a predictor of embryo developmental potential has also been ques-tioned, as the amount of HLA-G measured in embryo culture media appears to exceed the total protein con-tent of the embryo itself (Ménézo et al ., 2006 ).
Embryo metabolism Advances in technology have facilitated noninvasive measurement of amino acid uptake/output into the spent culture medium of individual embryos; it is now possible to quantify the products of embryo
metabolism, and use these measurements as a basis for identifying healthy embryos. During early develop-ment in vivo and in vitro, each preimplantation embryo will utilize numerous substrates from its immediate environment: oxygen for respiration, sugars, energy sources such as glucose and proteins/amino acids. Th e embryo also secretes many waste products of metabol-ism into its immediate environment. Th e turnover of these substrates and products can be measured either in the embryos themselves or in their culture environ-ment (Gardner, 2007 ).Th e rapid development of tech-nologies to measure embryo metabolism has created a new analytical science for embryo selection, the science of “embryo metabolomics.” Metabolomics is defi ned as “the systematic analysis of the inventory of meta-bolites – as small molecule biomarkers – that represent the functional phenotype at the cellular level” (Posillico et al ., 2007 ). Th e fi eld of embryo metabolomics is rap-idly expanding and includes the noninvasive meas-urement of amino acid turnover in spent embryo culture media using established technologies such as high performance liquid chromatography (HPLC, as detailed above), as well as methods such as gas chro-matography and mass spectrometry, nuclear magnetic resonance spectroscopy and Raman near infrared spectroscopy. Quantifying embryo metabolism has also been extended to include measurement of embryo oxygen consumption by respirometry. Details of the advantages and disadvantages associated with each of these diff erent methods are reviewed by Posillico et al . ( 2007 ).
Th e use of amino acid turnover to predict the devel-opmental competence of individual embryos is based on the premise that metabolism is intrinsic to early embryo health and that the embryonic metabolome is immediately perturbed when embryos are stressed (Houghton and Leese, 2004 ; Lane and Gardner, 2005 ). Diff erent methods can be used to quantify the metabo-lome (for review see Hollywood et al ., 2006 ); to date the methodologies that best suit the measurement of amino acid turnover by individual embryos are HPLC and mass spectrometry.
Amino acid profi ling has been extensively tested as a valid clinical diagnostic test for embryo selection in animal species, including mice, cows and pigs, as well as humans (Houghton et al ., 2002 ). Collectively the data on amino acid metabolism across these species indicates that :
(i) the net rates of depletion or appearance of amino acids by individual embryos vary between

Chapter 11: Oocyte retrieval and embryo culture
169
amino acids and the stage of preimplantation development
(ii) there is no diff erence between the turnover of essential and non-essential amino acids as defi ned by Eagle in 1959
(iii) the turnover of amino acids is moderated by the concentrations of the amino acids in the embryo culture media.
Net depletion of glutamine and arginine and the net appearance of alanine have been found to be common features between pig, cow and human embryos. Th e association of metabolic profi les of certain amino acids (particularly asparagine, glycine and leucine) with embryo viability is based on a var-iety of complex interactions and may involve energy production, mitochondrial function, regulation of pH and osmolarity. Nevertheless, on the basis of the turnover of three to fi ve key amino acids, it is possible to discriminate with some confi dence between mor-phologically similar cleavage stage human embryos which are metabolically “quiet” (Leese, 2002 ), but have the capacity to undergo zygotic genome acti-vation and blastocyst development, and embryos which are metabolically active but are destined to undergo cleavage arrest (Houghton et al ., 2002 ). Interestingly, amino acid turnover by early cleav-age embryos appears to be linked to embryo genetic health (Picton et al ., 2010 ). In this context inadequate energy production has been postulated as a cause of aneuploidy induction, due to errors during the ener-gy-dependent processes of chromosome alignment, segregation and polar body formation (Bielanska et al ., 2002a ; Ziebe et al ., 2003 ).
Preliminary trials of in-vitro amino acid profi l-ing suggested that this strategy can be used to iden-tify cleavage stage embryos with high implantation potential (Brison et al ., 2004 ). Metabolic profi les of developmentally competent, frozen-thawed human embryos were also consistent with those of fresh embryos (Brison et al ., 2004 ), and metabolic profi les could be used to identify frozen-thawed embryos with the potential to develop to the blastocyst stage in vitro.
Although initial results have been encouraging, the relevance of embryo metabolomics to the selection of the best embryo for transfer has been the subject of considerable debate, reviewed in a collection of papers published as the proceedings of a meeting on this spe-cifi c topic (Sturmey et al ., 2008 ).
Gene expression studies Th e activity of individual genes in an embryo change continuously in response to fl uctuating intrinsic requirements or environmental conditions. Embryonic gene expression has been assessed at diff erent stages of preimplantation development, using real-time PCR analysis of cDNA fragments as a measure of mRNA transcripts (Adjaye et al ., 1998 ). More recently, in-vitro transcription techniques have been developed that allow oocyte and embryo mRNA to be amplifi ed to a level that can be analyzed by microarrays (Wells, 2007 ). Although the technology is far from routine clinical application, as a research tool it is hoped that data accumulated over time from gene expression studies may eventually lead to the identifi cation of markers for embryo viability and implantation potential.
Embryo grading Divergent national strategies defi ne the maximum number of embryos that can be transferred in any one cycle, and there is now a trend towards elective single embryo transfer (eSET) for selected patient popula-tions, in order to decrease the incidence of multiple births associated with ART . In the UK, the HFEA introduced a “Multiple Births, Single Embryo Transfer Policy” in 2009, setting a maximum multiple birth rate for each UK clinic of 20%. In routine clinical practice, embryo selection for transfer continues to be based primarily on morphological assessment, oft en with multiple observations over the course of the embryo’s development; for cleavage stage embryos, assessment criteria include:
rate of division judged by the number of • blastomeres size, shape, symmetry and cytoplasmic appearance • of the blastomeres presence of anucleate cytoplasmic fragments • appearance of the zona pellucid a. •
Criteria are frequently combined to produce compos-ite scoring systems which may incorporate pronuclear scoring of zygotes. Online Quality Control schemes are available, where participants can compare their scoring criteria for embryo assessments with those of others ( www.fertaid.com , www.embryologists.org.uk/ ).
Although morphological assessment is recognized to be highly subjective, arbitrary and unsatisfactory, it is quick, noninvasive, easy to carry out in routine prac-tice, and does help to eliminate those embryos with the

Chapter 11: Oocyte retrieval and embryo culture
170
poorest prognosis. Evaluation of blastomere shape, size and number will refl ect synchronous cleavage of the blastomeres, and embryos with asynchrony in either the timing of cleavage, or the process of blasto-mere division will be given lower scores. Unfortunately embryo cleavage in vitro rarely follows the postulated theoretical timing of early development, and compu-ter-assisted morphometric analyses confi rm that large variations in blastomere size and fragmentation are frequently observed; large variations in blastomere size have been linked to increased chromosomal errors (Hnida and Ziebe, 2007 ).
Zygote scoring Schemes for identifying healthy viable embryos at the zygote stage were proposed by Scott et al . ( 2000 ) and Tesarik and Greco ( 1999 ). Criteria suggested as pre-dictive of optimal implantation potential include :
close alignment of nucleoli in a row • adequate separation of pronuclei • heterogeneous cytoplasm with a clear “halo” • cleavage within 24–26 hours. •
Th e scoring systems were reviewed by James ( 2007 ), and are compared in Table 11.1 . Th e timing of assessment is critical, as pronuclear development is a dynamic pro-cess and zygote scoring should therefore be used with caution and only in conjunction with other methods of evaluation .
Early cleavage Timing of the fi rst cell division of the embryo has been investigated as a predictor of developmental compe-tence, with the suggestion that “early cleavage” is asso-ciated with higher pregnancy rates. However, there is only a certain window where true early cleavage can be seen, and this extra assessment may be diffi cult to fi t into the normal routine of an IVF laboratory. Once the embryos have undergone the second division to the four-cell stage, those that might have cleaved a few hours earlier will have similar morphology to those that did not, and it is not possible to diff erentiate between them.
Multinucleation Multinucleated blastomeres can sometimes be observed at early cleavage stages, most easily on Day 2 ( Figure 11.4 ). Karyotyping and FISH analysis
confi rms that their presence may be more common in arrested embryos, and may occur more readily in some patients.
Multinucleated blastomeres have larger volumes than mononucleated blastomeres within the same embryo, and these mononucleated blastomeres are also smaller than mononucleated blastomeres in embryos with no multinucleation. Transfer of embryos with multinucleated blastomeres may be associated with decreased implantation, pregnancy and birth rates and should be excluded from transfer when possible (Meriano et al ., 2004 ; Hnida and Ziebe, 2007 ).
Cumulative scoring systems Multi-day scoring systems can enhance embryo selection by combining both developmental rate and morphological assessment (Skiadas and Racowsky, 2007 ).
Th ese should provide a more accurate picture of developmental progression than can be obtained from a single observation. However, the ultimate combin-ation of morphological features required for optimal evaluation of developmental competence has yet to be resolved. Th e optimal timing of embryo transfer will be more accurately determined when agreement on this is reached.
Fragments Fragmentation in the human embryo is very com-mon, affecting up to 75% of all embryos developed in vitro (Alikani, 2007 ); it is not clear whether this is an effect of culture conditions and follicular stimu-lation, or a characteristic of human development ( Figure 11.5 ). Extensive fragmentation is known to be associated with implantation failure, but the relationship between the degree of fragmentation and the developmental potential of the embryo is far from clear. Alikani et al . ( 1999 ) found that when embryos with more than 15% fragmentation were cultured to blastocyst stage, they formed fewer morulas, fewer cavities and fewer blastocysts com-pared to those embryos with less than 15% fragmen-tation. When fragmentation was greater than 35%, all processes were compromised. Retrospective ana-lysis of embryo transfer data revealed that nearly 90% of embryos selected for transfer were developed from embryos with less than 15% fragmentation observed on Day 3.

Chapter 11: Oocyte retrieval and embryo culture
171
Alikani and Cohen ( 1995 ) used an analysis of pat-terns of cell fragmentation in the human embryo as a means of determining the relationship between cell fragmentation and implantation potential, with the conclusion that not only the degree, but also the pattern of embryo fragmentation determine its implantation
potential. Five distinct patterns of fragmentation which can be seen by Day 3 were identifi ed:
Type I: <5% of the volume of the perivitelline space (PVS) occupied by fragments. Type II: small, localized fragments associated with one or two cells.
Table 11.1 Comparison of pronuclear morphology scoring systems, with a representative illustration of pronuclei in each scoring group
Scott et al ., 2000 Series 1
Scott et al ., 2000 Series 2 Scott, 2003
Tesarik and Greco,
, 1999
Tesarik et al . ,,
2000 Pronuclear morphology
Grade 1 Z1 Z1 Pattern 0 Pattern 0
Grade 3 Z2 Z2 Pattern 0 Pattern 0
Grade 2 Z3 Z3–2 Pattern 2 Non-pattern 0
Grade 4 Z3 Z3–1 Pattern 5 Non-pattern 0
Grade 4 Z3 Z3–4 Pattern 1 Non-pattern 0
Grade 4 Z3 Z3–4 Pattern 3 Non-pattern 0
Grade 5 Z3 Z3–1 Pattern 4 Non-pattern 0
Grade 5 Z4 Z4–2 Pattern 4 Non-pattern 0
Grade 5 Z4 Z4–1 NA Non-pattern 0

Chapter 11: Oocyte retrieval and embryo culture
172 Figure 11.5 (a) Day 3 human embryo with type 3 fragments. (b) Day 3 embryo with type 4 fragmentation.
(a)
(b)
Figure 11.4 A two-cell embryo showing two nuclei in each. (Reprinted with permission, J Meriano 2004, Reproductive Biomedicine Online .)
Type III: small, scattered fragments associated with multiple cells. Type IV: large, scattered fragments associated with several unevenly sized cells and scattered throughout the PVS. Type V: fragments throughout the PVS, appearing degenerate such that cell boundaries are invisible, associated with contracted and granular cytoplasm .
Some embryos have no distinct pattern (NDP) of fragmentation.
No defi nite cause of fragmentation has been identi-fi ed, although speculations include high spermatozoal numbers and consequently high levels of free radicals, temperature or pH shock, and stimulation protocols. Apoptosis has been suggested as a possible cause, and a progressive shortening of telomere length, which induces apoptosis, has been linked with fragmenta-tion (Keefe et al ., 2005 ); however, this study was not defi nitive. Mitotically inactive cells do not exhibit frag-mentation (Liu et al ., 2002 ), and it has been suggested that aberrant cytokinesis in the presence of spindle and cytoskeletal abnormalities may be associated with fragmentation.
Observed via the scanning electron microscope, the surface of fragments is made up of irregularly shaped blebs and protrusions, very diff erent to the regular surface of blastomeres, which is organized into short, regular microvilli ( Figure 11.6 ).
Interestingly, programmed cell death in somatic cell s also starts with surface blebbing, and is caused, in part, by a calcium-induced disorganization of the cyto-skeleton. We can speculate that similar mechanisms operate within human embryos, but there is so far no scientifi c evidence that this is the case.
There does appear to be an element of program-ming in this partial embryonic autodestruction, as embryos from certain patients, irrespective of the types of procedure applied in successive IVF attempts, are always prone to fragmentation. Surprisingly, fragmented embryos, repaired or not, do implant and often come to term. Time-lapse photography technology has clearly demonstrated that an individ-ual embryo can radically change its morphological appearance in a short period of time: fragments that are apparent at a particular moment in time can be subsequently absorbed with no evidence of their prior existence (Hamberger et al ., 1998 ; Hashimoto et al ., 2009 ; Mio and Maeda, 2008 ). This demonstrates the highly regulative nature of the human embryo, as

Chapter 11: Oocyte retrieval and embryo culture
173
it can apparently lose over half of its cellular mass and still recover, and also confirms the general con-sensus that the mature oocyte contains much more material than it needs for development. The reasons why part, and only part, of an early embryo should become disorganized and degenerate are a mystery. Different degrees of fragmentation argue against the idea that the embryo is purposely casting off excess cytoplasm, somewhat analogous to the situation in annelids and marsupials that shed cytoplasmic lobes rich in yolk, and favors the idea of partial degener-ation. Perhaps it involves cell polarization, where organelles gather to one side of the cell. It is certain that pH, calcium and transcellular currents trigger cell polarization, which may in certain cases lead to an abnormal polarization, and therefore to frag-mentation. Describing fragmentation as a degenera-tive process may not be justified, but more research
is needed to elucidate whether the implantation of embryos with extensive fragmentation at the cleav-age stages has any long-term effects.
Embryo grading: cleavage stages After more than 30 years, and the birth of close to 10 million babies, the basic selection criteria in a routine IVF laboratory without research facilities continue to be based on assessment of morphology ( Figure 11.7 ). Preimplantation genetic screening by FISH analysis of biopsied blastomeres has shown a surprising discrepancy between gross morphology and genetic normality of embryos. Even the most “beautiful” Grade 1 embryos may have numerical chromosomal anomalies, whilst those judged to be of “poorer” quality, with uneven blastomeres and fragments, may have a normal chromosome com-plement. The image database on www.ivf.net has
Figure 11.6 Scanning electron micrographs. (a, b) Two views of a human four-cell embryo showing 20% fragmentation. (c–e) Magnifi cation of corresponding areas showing regular short microvilli of vital blastomeres and intercellular areas. (f) Magnifi cation of the surface of a cytoplasmic fragment showing irregular blebs and protrusions. (With permission from Dale et al ., 1995 .)

Chapter 11: Oocyte retrieval and embryo culture
174
Figure 11.7 Morphological variations in cleavage stage human embryos. (a) Two-cell embryo on Day 2, no fragments. (b) Day 2 embryo, Grade 3. (c) Day 2 embryo, uneven blastomeres with one large dominant blastomere. (d) Day 2 embryo, one blastomere shows large vacuole, Grade 2/3. (e) Four-cell embryo on Day 2, Grade 1. See color plate section. (f) Grade 3 embryo on Day 2. See color plate section. (g) Grade 4 embryo on Day 2. (h) Day 3 six-cell embryo, Grade 1. (i) Day 3 eight-cell embryo, Grade 1. Images (c) and (g) kindly supplied by Thomas Ebner, Austria; (g) by Marc van den Bergh, Switzerland; (e) and (f) by Oleksii Barash, Ukraine; (h) by Gemma Fabozzi, Naples. Despite the extreme diff erence in their morphology, the single transfer of embryos (e) and (f) both led to healthy live births (photos and history courtesy of Oleksii Barash, Ukraine).
(a) (b)
(c)
(d)
(e)
(f)

Chapter 11: Oocyte retrieval and embryo culture
175
(g) (h)
(i)
Figure 11.7 (cont.)
a valuable collection of photographs showing sin-gle embryos that led to a live birth after transfer, which clearly confirm that our subjective assess-ment of embryo morphology often fails to predict its implantation potential in reality .
Grade 1/A Even, regular spherical blastomeres • Moderate refractility (i.e., not very dark) • Intact zona • No, or very few, fragments (less than 10%) •
Allowance should be made for the appearance of blastomeres that are in division or that have divided
asynchronously with their sisters, e.g., three- fi ve- six- or seven-cell embryos, which may be uneven. As always, individual judgment is important, and this is a highly subjective assessment.
Grade 2/B Uneven or irregular shaped blastomeres • Mild variation in refractility • No more than 10% fragmentation of blastomeres •
Grade 3/C Fragmentation of no more than 50% of • blastomeres

Chapter 11: Oocyte retrieval and embryo culture
176
Remaining blastomeres must be at least in • reasonable (Grade 2) condition Refractility associated with cell viability • Intact zona pellucida •
Grade 4/D More than 50% of the blastomeres are fragmented • Gross variation in refractility. • Remaining blastomeres appear viable •
Grade 5 Zygotes with two pronuclei on Day 2 (delayed • fertilization or reinsemination on Day 1)
Grade 6 Nonviable: fragmented, lysed, contracted or dark • blastomeres No viable cells •
It is important to bear in mind that the time dur-ing which the assessment and judgment is made rep-resents only a tiny instant of a rapidly evolving process of development. Embryos can be judged quite diff er-ently at two diff erent periods in time, as may be seen if a comparison is made between assessments made in the morning, and later in the day immediately before transfer. Individual judgment should be exercised in determining which embryos are selected. In general, those embryos at later stages and of higher grades are preferred, but the choice is oft en not clear cut. Th e Grade 2 category covers a wide range of morpho-logical states but, provided the blastomeres are not grossly abnormal, a later stage Grade 2 embryo may be selected in preference to an earlier stage Grade 1 embryo. Attention should also be paid to the appear-ance of the zona pellucida and to the pattern of frag-mentation. Embryos of Grade 3 or 4 are transferred only where no better embryos are available. If only pronucleate embryos are available on Day 2, they should be cultured further and transferred only if cleavage occurs.
Blastocyst transfer Th e transfer of blastocysts on Day 5 or 6 may have the advantage of allowing better synchrony between the embryo and endometrium, as well as eliminating embryos that cannot develop aft er activation of the zygote genome due to genetic or metabolic defects.
Following the development of new generation sequen-tial embryo culture media, single blastocyst transfer has been promoted as a means of improving the suc-cess of IVF, while at the same time reducing multiple birth rates (Gardner et al ., 1998 ). However, blastocyst generation in vitro is costly both in terms of time and laboratory resources, and there is continuing debate as to whether sequential, two-step culture confers sig-nifi cant benefi t over one-step culture systems (Biggers et al ., 2005 ). An important prerequisite for blastocyst culture is an optimal IVF laboratory culture envir-onment; there is no advantage in extended culture unless satisfactory implantation rates are already obtained aft er culture to Day 2 or 3. Published litera-ture indicates that a policy of careful embryo evalu-ation at cleavage stages can lead to success rates aft er Day 3 transfer that broadly match the success rates achieved with blastocyst transfer. One of the hesita-tions of culturing embryos to the blastocyst stage was the poor survival rate for supernumerary blastocysts aft er slow freezing. However, the increasing use of vit-rifi cation for blastocyst freezing with associated high survival rate post-thaw (see Chapter 12 ) has made single blastocyst transfer a more viable option, and this also facilitates a policy for elective single embryo transfer (eSET).
Concern has also been expressed about the safety of prolonged culture to the blastocyst stage and the risk of potential aberrant epigenetic programming during extended in-vitro development (Huntriss and Picton, 2008 ; see Chapter 15 ).
Potential benefi ts of blastocyst transfer (Gardner et al ., 2007 )
• True embryo viability can be assessed, post embry-onic genome activation . Embryos with limited developmental potential are • eliminated. Embryonic stage is synchronized with the uterus, • reducing cellular stress on the embryo. Exposure of the embryo to a hyperstimulated uter-• ine environment is minimized. Possibility of uterine contractions is reduced, minim-• izing the chance of embryo expulsion. Cleavage stage embryo biopsy can be carried out, • and embryos transferred at blastocyst stage when results are available. High implantation rate; reduces the need to transfer • multiple embryos.
• True embryo viability can be assessed, post embry-onic genome activation . Embryos with limited developmental potential are• eliminated. Embryonic stage is synchronized with the uterus,•reducing cellular stress on the embryo. Exposure of the embryo to a hyperstimulated uter-• ine environment is minimized. Possibility of uterine contractions is reduced, minim-•izing the chance of embryo expulsion. Cleavage stage embryo biopsy can be carried out,• and embryos transferred at blastocyst stage whenresults are available. High implantation rate; reduces the need to transfer•multiple embryos.

Chapter 11: Oocyte retrieval and embryo culture
177
• Reduction in multiple gestation rate as only one or two embryos need be transferred.
Th e ability to identify healthy viable blastocysts is an important factor in the success of blastocyst transfer, and a grading system has been devised that takes into consideration the degree of expansion, hatching sta-tus, the development of the inner cell mass (ICM) and the development of the trophectoderm (Gardner and Schoolcraft , 1999 ). Careful assessment of all morpho-logical parameters available will optimize the chance of achieving satisfactory implantation rates aft er blasto-cyst transfer.
Blastocysts are initially graded numerically, from 1 to 6 (this can be performed under a dissecting microscope ): 1. Early blastocyst: the blastocoele occupies less than
half the volume of the embryo. 2. Blastocyst: the blastocoele occupies half the
volume of the embryo or more. 3. Full blastocyst : the blastocoele completely fi lls the
embryo, but the zona has not thinned. 4. Expanded blastocyst : the volume of the blastocoele
is larger than that of the embryo, and the zona is thinning.
5. Hatching blastocyst : the trophectoderm has started to herniate through the zona.
6. Hatched blastocyst : the blastocyst has completely escaped from the zona.
Th e morphology of the ICM and trophectoderm are then assessed under an inverted microscope:
Examples of stages of human blastocyst develop ment are illustrated in Figure 11.8 ; Figure 11.9 illustrates the limitations of morphological assessment.
Blastocyst transfer has also been used as a strategy for the treatment of patients who carry chromosomal translocations; chromosome translocations cause a
delay in the cell cycl e, and abnormal or slowly devel-oping embryos are eliminated during in-vitro culture. Several normal pregnancies have been successfully established aft er transfer of healthy blastocysts in a group of patients carrying translocations (Ménézo et al ., 2001 ).
Remaining embryos Aft er embryo transfer, remaining embryos of Grades 1 or 2 which show less than 20% fragmentation at the time of assessment may be cryopreserved on Day 2 or Day 3. Embryos of suboptimal morphology at this time can be further cultured until Day 6, with daily assess-ment. Th ose that develop to blastocysts on Days 5 or 6 can also be cryopreserved.
Embryo transfer procedure Materials 1. Pre-equilibrated, warmed culture medium 2. 1 mL disposable syringe 3. Embryo transfer catheter 4. Sterile disposable gloves (nonpowdered) 5. Clean Petri dish 6. Sterile Pasteur pipette and glass probe 7. Dissecting microscope with warm stage
Although it may seem obvious that correct iden-tifi cation of patient and embryos is vital, errors in communication do happen and can lead to a disas-trous mistake, especially should there be patients with similar names undergoing treatment at the same time. Electronic identity/witnessing systems are now avail-able to confi rm identities of doctor, nurse, embryolo-gist and patient, but if such a system is not available, a routine discipline of identifi cation should be fol-lowed to ensure that there is no possibility of mistaken identity :
1. Ensure that medical notes always accompany a patient who is being prepared for embryo transfer.
2. Name and medical numbers on medical notes and patient identity bracelet should be checked by two people, i.e., the clinician in charge of the procedure and the assisting nurse.
3. Th e doctor should also check name and number verbally with the patient, and doctor, nurse and
• Reduction in multiple gestation rate as only one or two embryos need be transferred.
ICM Trophectoder m
A. Tightly packed, many cells,
A. Many cells forming a cohesive epithelium
B. Loosely grouped, several cells
B. Few cells forming a loose epithelium
C. Very few cells C. Very few large cells

Chapter 11: Oocyte retrieval and embryo culture
178
Figure 11.8 Stages in blastocyst development. (a) Compacting morula (see color plate section, between pp. 00 and 00, for color version of this fi gure). (b) Early stages of cavitation, See color plate section. (c) Fully expanded top-grade blastocyst with well-developed ICM and troph-ectoderm, thinned zona, hatching process initiated. See color plate section. (d) Top-grade blastocyst in the process of hatching. (e) Hatching blastocyst about to leave the zona. See color plate section. (f) Fully hatched blastocyst and empty zona.
(a) (b)
(c)
(d)
patient may sign an appropriate form confi rming that the details are correct.
4. Th e duty embryologist should check the same details with the embryology records, and also sign the same form in the presence of the doctor.
Preparation of embryos for transfer Th e rate of multiple gestation resulting from IVF/ET is unacceptably high, and legislation in the UK and a few other European countries now prohibits the trans-fer of more than two embryos in a treatment cycle for

Chapter 11: Oocyte retrieval and embryo culture
179
Figure 11.9 Limitations of morphological blastocyst assessment . Although each of the embryos pictured here would be graded as lesser quality compared with the “classic” optimal grade blastocysts seen in Figure 11.8 , each of these embryos resulted in a healthy live birth after single embryo transfer on Day 5. Image (a) is a thawed embryo (two blastocysts were thawed on Day 5 [slow-freeze protocol], the one pic-tured here survived and was transferred on the same day). (With thanks to Oleksii Barash, Clinic of Reproductive Medicine “Nadiya,” Ukraine.) See color plate section.
(e) (f)
Figure 11.8 (cont.)
(a) (b)
certain patient groups. Elective single embryo trans-fer (eSET) is recommended for selected patients with a good prognosis, i.e., young age, tubal infertility only, fi rst attempt or previous history of pregnancy and/or delivery . 1. Prepare a droplet (or well) of fresh medium for the
selected embryos.
2. When the embryos for transfer have been identifi ed and scored, and their details recorded (number, developmental stage and grade), place them together in the pre-equilibrated droplet or well. No more than two embryos should be selected. If medium with a higher density is used (i.e., with 50–75% serum), this transfer should be carried out

Chapter 11: Oocyte retrieval and embryo culture
180
carefully, as the embryos will “fl oat” in the higher density medium and must be allowed to settle before aspiration into the embryo transfer catheter.
3. Aft er gently pushing the embryos together, leave them under low power on the heated stage of the microscope, in focus.
4. Turn off the microscope light. 5. Wash your hands with a surgical scrub
preparation, and don sterile gloves. 6. Fill a 1 mL sterile syringe with warm medium, and
eject any air bubbles. 7. Check that the catheter to be used moves freely
through its outer sheath, attach it to the syringe and eject the medium from the syringe through the catheter, discarding the medium. Syringes designed specifi cally for embryo transfer are available, and
these allow better control than a standard 1 mL syringe.
8. Draw up warm medium through the catheter into the syringe, and then push the piston down to the 0.1 mL mark, ejecting excess medium and again discarding it .
9. Pour some clean warm medium into the warm Petri dish on the microscope stage (for rinsing the catheter tip).
10. Place the end of the catheter into the drop or well, away from the embryos, and inject a small amount of medium to break the boundary of surface tension that may appear at the end of the catheter. Aspirate the embryos into the catheter, so that the volume to be transferred is 15–20 µL.
(c) (d)
(e) (f)
Figure 11.9 (cont.)

Chapter 11: Oocyte retrieval and embryo culture
181
11. If the embryos have been loaded from a droplet under oil, rinse the tip of the catheter in the Petri dish containing clean warm medium.
Hand the catheter and syringe to the clinician for transfer to the patient. When the catheter is returned after the procedure, carefully inspect it, rotating under the microscope. It is especially important to ensure that no embryo is buried in any mucus pre-sent; note and record the presence of mucus and/or blood. Loosen the Lueur fitting, and allow the fluid in the catheter to drain into the clean Petri dish while continuing to observe through the microscope. Inform the doctor and patient as soon as you have confirmed that no embryos have been returned. If any embryos have been returned, they should be reloaded into a clean catheter, and the transfer pro-cedure repeated. If difficulties arise during the trans-fer procedure causing delay, return the embryos to the culture drop in the interim, until the physician is confident that they can be safely transferred to the uterus of the patient .
Th ere is no doubt that the technique of embryo transfer, although apparently a simple and straight-forward procedure, is absolutely critical in safe delivery of the embryos to the site of their potential implantation. Studies repeatedly show that pregnancy rates can vary in the hands of diff erent operators, and with the use of diff erent embryo transfer catheters. In a study of embryo transfer procedures under ultra-sound-guided control, Woolcott and Stanger ( 1998 ) observed guiding cannula and transfer catheter placement in relation to the endometrial surface and uterine fundus during embryo transfer. Th eir results indicated that tactile assessment of embryo transfer catheter was unreliable, in that the cannula and the catheter could be seen to abut the fundal endomet-rium, and indent or embed in the endometrium in a signifi cant number of cases. Endometrial movement due to sub-endometrial myometrial contraction was obvious in 36% of cases, and this movement was asso-ciated with a reduced pregnancy rate. Th eir studies highlight the fact that “blind” embryo transfer pro-cedures may oft en lead to an unsatisfactory outcome, and they recommend the use of ultrasound guidance as a routine during embryo transfer.
In-vitro maturation In-vitro maturation (IVM) of human oocytes from antral follicles is an emerging new technology which
has several advantages over traditional controlled ovarian hyperstimulation (COH) for IVF, particularly in reducing the risk of OHSS for patients with polycys-tic ovaries (PCO) , as well as maintaining lower costs of treatment. Although IVM is still in a developmental stage for human clinical IVF, several hundred children have been born following the use of this technique, and consequently it may be considered as an alternative treatment strategy for selected patient groups. IVM technology has been successfully used in farm ani-mals for decades, and collection of immature oocytes continues to be routine. Pincus and Enzmann ( 1935 ) were the fi rst to show that immature rabbit oocytes removed from their natural ovarian environment were capable of undergoing spontaneous maturation and fertilization in vitro. Robert Edwards made simi-lar observations in human oocytes in 1965. Lucinda Veeck and colleagues matured human oocytes in the laboratory that had been retrieved from COH cycles in 1983, and these subsequently fertilized and resulted in live births. However, such “rescued” oocytes are oft en suboptimal, showing a high incidence of aneu-ploidy as well as other defects. Current technology aims to retrieve immature oocytes from unstimulated or slightly stimulated small antral follicles, and cul-ture these cumulus- enclosed oocytes in a specifi cally designed medium. Cha et al . ( 1991 ) reported the fi rst human live births aft er retrieval of immature oocytes from antral follicles.
Th e phrase “cytoplasmic maturity” was coined by Delage in 1901, to point out that it was not necessarily synchronous with nuclear maturity. Th is is certainly true for human oocytes, where a metaphase II nucleus does not guarantee developmental competence. Whereas nuclear maturation is relatively visible, cytoplasmic maturity is much more diffi cult to assess microscopically. Th e aim of IVM is to retrieve and rescue immature oocytes before they are adversely aff ected by the endocrine and paracrine infl uences of the growing dominant follicle. Studies in the bovine have shown that oocytes retrieved in later phases of follicular development have more mitochondrial RNA (mRNA) transcripts compared with oocytes from less developed follicles, correlated with good embryonic developmental potential. Data from ani-mals suggest that mRNA instability and the absence or abundance of certain transcripts such as LH and FSH receptors, connexin 43, and cyclooxygenase-2 in the cumulus of oocytes from small antral follicles aft er resumption of meiosis in vitro are predictors of

Chapter 11: Oocyte retrieval and embryo culture
182
oocyte quality. Th e presence of other key components that have been described in rodents, such as growth diff erentiation factor-9 (GDF-9) and bone morpho-genetic protein-15 (BMP-15) , mediate important biochemical changes in oocytes required for normal postmeiotic events.
Although protocols are by no means standard, it seems that an initial priming of the ovaries with low doses of FSH from Days 2–6 improves success, fol-lowed by administration of hCG and co-culture of the oocytes with granulosa/cumulus cells in a medium that is supplemented with FSH and LH or hCG. Th ere are several considerations to be taken into account while handling immature oocytes: since the volume of follicular fl uid retrieved in IVM procedures is small and oft en contains blood, it is advisable to use heparin (2–5 IU/mL) in HEPES-buff ered medium to minim-ize blood clotting. As in traditional IVF technology, attention should be given to pH and temperature set-tings. Oocytes from small antral follicles diff er mor-phologically from mature oocytes and are oft en found enclosed within a compacted mass of surrounding granulosa cells. Th e degree of expansion of the cumu-lus cells may be infl uenced by the size of the follicle, as well as by the exposure to gonadotropins and/or hCG in vivo.
Immediately aft er retrieval, cumulus-enclosed immature oocytes are placed in IVM medium for 24–48 hours. Numerous IVM media formulations are commercially available, composed of standard IVF medium with the addition of recombinant FSH and hCG. Patient-inactivated serum or follicular fl uid is oft en added to the maturation media as an exogenous protein source. Growth factors, lipids, glycoproteins, steroid hormones, cytokines and other factors in the serum or follicular fl uid may be instrumental in the regulation of oocyte maturation and account for its preference over synthetic serum substitute or human albumin .
ICSI is the preferred method of insemination in IVM, since oocytes are frequently denuded of gran-ulosa cells for evaluation of maturational status and there are fears of zona pellucida hardening during the IVM process. Studies comparing ICSI versus IVF for the insemination of IVM oocytes have shown that ICSI results in higher rates of fertilization than IVF; however, the developmental potential of the fertilized oocytes was similar irrespective of the insemination method. Child et al . ( 2002 ) compared the outcome
of IVM cycles with IVF in women of comparable age with PCO and polycystic ovary syndrome. Th e absolute number of oocytes collected, metaphase II oocytes, fertilized oocytes and cleaved embryos was signifi cantly higher in the IVF group. Th e implant-ation rate was higher in the IVF group (17.1%) than in the IVM group (9.5%), but there were 12 (11.2%) cases of OHSS in the IVF group, compared with none in the IVM group .
Although results are promising, IVM in the human requires further basic research before being applied routinely to the IVF laboratory. Th e complexities of oocyte maturation, in particular the unknowns in cytoplasmic maturity (see Chapter 4 ) and the inher-ent problems in methylation that may be induced by suboptimal culture conditions (Ménézo et al ., 2010 ) warrant caution.
Transport IVF and transport ICSI Th e facilities of a central expert IVF laboratory can be used to off er treatment in hospitals that do not have the necessary laboratory space and personnel. Carefully selected patients undergo ovarian stimula-tion, monitoring and oocyte retrieval under the care and management of a gynecologist who has a close liaison with an IVF laboratory team in a location that can be reached ideally within 2 hours of the hospital or clinic where the oocyte retrieval procedure takes place. It is an advantage to select patients with simple , uncomplicated infertility and good ovarian response, and close communication and coordination between the patient, physician and IVF laboratory team is essential.
Selection criteria for transport IVF/ICSI
1. Women 35 years of age or less 2. Tubal damage as the sole cause of subfertility
Exclusion criteria 1. Women over 35 years of age 2. Patients with LH:FSH ratio higher than 3:1 3. Patients with laparoscopically proven moderate or
severe endometriosis 4. Patients requesting oocyte donation or donor
insemination 5. Three previously unsuccessful IVF treatment cycles
A GnRH-agonist/FSH long protocol is used for superovulation so that a simplifi ed monitoring
1. Women 35 years of age or less2. Tubal damage as the sole cause of subfertility
Exclusion criteria1. Women over 35 years of age 2. Patients with LH:FSH ratio higher than 3:13. Patients with laparoscopically proven moderate or
severe endometriosis4. Patients requesting oocyte donation or donor
insemination 5. Three previously unsuccessful IVF treatment cycles

Chapter 11: Oocyte retrieval and embryo culture
183
regimen can be used (ultrasound assessment and optional serum estradiol levels) and to allow sched-uled admission of patients into the stimulation phase. Th is protocol also allows latitude in the administra-tion of hCG, so that the timing of oocyte retrieval can be scheduled in a routine operating list. Ovulation is induced by hCG administration 36 hours prior to the planned follicular aspiration.
Th e couple under treatment must visit the central unit before hCG is given, both to receive detailed infor-mation and consent forms, and to familiarize them-selves with the journey and the facilities. Th e husband will return to the central unit on the morning of oocyte retrieval to produce a semen sample and to collect a prewarmed portable incubator. Th e portable incubator, plugged into a car cigarette lighter, is then used to trans-port the follicular aspirates which have been collected in the peripheral hospital or clinic. Follicular aspirates are collected under ultrasound -guided control into sterile test-tubes (without fl ushing). It is essential that each test-tube is fi lled completely and tightly capped in order to prevent pH fl uctuations. A heated test-tube rack during aspiration must be used to prevent tem-perature fl uctuations in the aspirates. At the end of the oocyte retrieval procedure, the partner transports the follicular aspirates, together with the treatment records, to the central laboratory for oocyte identifi ca-tion and subsequent insemination and culture .
Th e embryo transfer procedure is carried out 48 hours later at the central unit. Patient follow-up is car-ried out by the physician at the peripheral unit. Provided that the instructions and inclusion criteria are strictly adhered to, a highly motivated, well-coordinated team working in close liaison can achieve success rates com-parable to those obtained in the specialist center, and IVF treatment can thus be off ered to couples to whom it might otherwise be unavailable. Transport ICSI can also be successfully off ered on a similar basis (see Chapter 13 ).
Conclusion In view of the complexity of the elegant biochemis-try and physiology involved in the development of a competent oocyte that will fertilize and develop suc-cessfully in vitro, as well as the delicate balance that must be required within each contributing compo-nent and compartment, it seems miraculous indeed that the application of essentially ill-defi ned strategies has led to the successful birth of so many children.
Although success rates have improved signifi cantly over the past two decades, there continues to be a wastage of embryos that fail to implant. A great deal more research is required to identify and defi ne factors involved in the development of competent oocytes and viable embryos, and new data from the application of current research using metabolomic and proteomic strategies are awaited.
Further reading Books Edwards , RG , Purdy , JM ( 1982 ) Human Conception In Vitro ,
Academic Press , London . Elder K , Cohen J (eds.) ( 2007 ) Preimplantation Embryo
Evaluation and Selection . Informa Press , London . Pasquale P , Tucker MJ , Guelmann. V (eds.) ( 2003 ) A Color
Atlas for Human Assisted Reproduction . Lippincott Williams & Wilkins , Philadelphia .
Veeck L ( 1998 ) An Atlas of Human Gametes and Conceptuses . Parthenon Publishing , New York .
Publications Adjaye J , Daniels R , Monk M ( 1998 ) Th e construction of
cDNA libraries from human single preimplantation embryos and their use in the study of gene expression during development . Journal of Assisted Reproduction and Genetics 15 (5): 344 –348.
Alikani M ( 2007 ) Th e origins and consequences of fragmentation in mammalian eggs and embryos. In: Elder K , Cohen J (eds.) Preimplantation Embryo Evaluation and Selection . Informa Press , London , pp. 89–100.
Alikani M , Cohen J ( 1995 ) Patterns of cell fragmentation in the human embryo in vitro . Journal of Assisted Reproduction and Genetics 12 (Suppl.): 28s .
Alikani M , Cohen J , Tomkin G , et al . ( 1999 ) Human embryo fragmentation in vitro and its implications for pregnancy and implantation . Fertility and Sterility 71 (5): 836 –842.
Alikani M , Palermo G , Adler A , Bertoli M , Blake M , Cohen J ( 1995 ) Intracytoplasmic sperm injection in dysmorphic human oocytes . Zygote 3 : 283 –288.
Alikani M , Weimer K ( 1997 ) Embryo number for transfer should not be strictly regulated . Fertility and Sterility 68 : 782 –784.
Almeida PA , Bolton VN ( 1993 ) Immaturity and chromosomal abnormalities in oocytes that fail to develop pronuclei following insemination in vitro . Human Reproduction 8 : 229 –232.
Almeida PA , Bolton VN ( 1995 ) Th e eff ect of temperature fl uctuations on the cytoskeletal organisation and

Chapter 11: Oocyte retrieval and embryo culture
184
chromosomal constitution of the human oocyte . Zygote 3 : 357 –365.
Angell RR , Templeton AA , Aitken RJ ( 1986 ) Chromosome studies in human in vitro fertilization . Human Genetics 72 : 333 .
Ben-Rafael Z , Kopf G , Blasco Lo , Tureck RW , Mastoianni L ( 1986 ) Fertilization and cleavage aft er reinsemination of human oocytes in vitro . Fertility and Sterility 45 (1): 58 –62.
Bielanska M , Tan SL , Ao A ( 2002a ) High rate of myxoploidy among human blastocysts cultured in vitro . Fertility and Sterility 78 (6): 1248 –1253.
Bielanska M , Tan SL Ao A ( 2002b ) A diff erent probe combinations for assessment of postzygotic chromosomal imbalances in human embryos . Journal of Assisted Reproduction and Genetics 19 (4): 177 –182.
Biggers JD , McGinnis LK , Lawitts JA ( 2005 ) One-step versus two-step culture of mouse preimplantation embryos: is there a diff erence? Human Reproduction 20 (12): 3376 –3384.
Bolton VN , Hawes SM , Taylor CT , Parsons JH ( 1989 ) Development of spare human preimplantation embryos in vitro: an analysis of the correlations among gross morphology, cleavage rates, and development to the blastocyst . Journal of In Vitro Fertilization and Embryo Transfer 7 : 186 .
Brison DR ( 2000 ) Apoptosis in mammalian preimplantation embryos: regulation by survival factors . Human Fertility 3 : 36 –47.
Brison DR , Houghton FD , Falconer D , et al . ( 2004 ) Identifi cation of viable embryos in IVF by non-invasive measurement of amino acid turnover . Human Reproduction 19 (10): 2319 –2324.
Canipari R , Epifano O , Siracusa G , Salustri A ( 1995 ) Mouse oocytes inhibit plasminogen activator production by ovarian cumulus and granulosa cells . Developmental Biology 167 : 371 –378.
Caro C , Trounson A ( 1986 ) Successful fertilization and embryo development, and pregnancy in human in vitro fertilization (IVF) using a chemically defi ned culture medium containing no protein . Journal of In Vitro Fertilization Embryo Transfer 3 : 215 –217.
Chang CL , Wang TH , Horng SG , et al . ( 2002 ) Th e concentration of inhibin B in follicular fl uid: relation to oocyte maturation and embryo Human Reproduction 17 (7): 1724 –1728.
Clyde JM , Hogg JE , Rutherford AJ , Picton HM ( 2003 ) Karyotyping of human metaphase II oocytes by multifl uor fl uorescence in situ hybridization . Fertility and Sterility 80 (4): 1003 –1011.
Cohen J , Inge KL , Suzman M , Wiker SR , Wright G ( 1989 ) Videocinematography of fresh and cryopreserved embryos: a retrospective analysis of embryonic morphology and implantation . Fertility and Sterility 51 : 820 .
Combelles CMH , Fissore RA , Albertini DF , Racowsky C ( 2006 ) In vitro maturation of human oocytes and cumulus cells using a co-culture three-dimensional collagen gel system . Human Reproduction 20 (5): 1349 –1358.
Dale B , Fiorentino A , De Stefano RD , et al . ( 1999 ) Pregnancies aft er activated oocyte transfer: a new alternative for infertility treatment . Human Reproduction 14 : 1771 –1772.
Dale B , Tosti E , Iaccarino M ( 1995 ) Is the plasma membrane of the human oocyte reorganised following fertilisation and early cleavage? Zygote 3 (1): 31 –36.
D’Amour K , Gage FH ( 2000 ) New tools for human developmental biology . Nature Biotechnology 18 (4): 381 –382.
Das S , Chattopadhyay R , Ghosh S , et al . ( 2006 ) Reactive oxygen species level in follicular fl uid – embryo quality marker in IVF? Human Reproduction 21 (9): 2403 –2407.
Diamond MP , Rogers BJ , Webster BW , Vaughn WK , Wentz AC ( 1985 ) Polyspermy: eff ect of varying stimulation protocols and inseminating sperm concentrations . Fertility and Sterility 43 (5): 777 –780.
Eagle H ( 1959 ) Amino acid metabolism in mammalian cell cultures . Science 130 : 432 –437.
Ebner T ( 2006 ) Is oocyte morphology prognostic of embryo developmental potential aft er ICSI? Reproductive Biomedicine Online 12 (4): 507 –512.
Ebner T ( 2008 ) Blood clots in the cumulus-oocyte complex predict poor oocyte quality and post-fertilization development . Reproductive Biomedicine Online 16 (6): 801 –807.
Ebner T , Moser M , Sommergruber M , et al . ( 2002 ) First polar body morphology and blastocyst formation rate in ICSI patients . Human Reproduction 17 (9): 2415 –2418.
Elder K , Elliott T ( 1999 ) Blastocyst Update . Worldwide Conferences in Reproductive Biology, Ladybrook Publications , Australia .
Englert Y , Puissant F , Camus M , Degueldre M , Leroy F ( 1986 ) Factors leading to tripronucleate eggs during human in vitro fertilization . Human Reproduction 1 (2): 117 –119.
Falcone P , Gambera L , Pisoni M , et al . ( 2008 ) Correlation between oocyte preincubation time and pregnancy rate aft er intracytoplasmic sperm injection . Gynecological Endocrinology 24 (6): 25 –29.

Chapter 11: Oocyte retrieval and embryo culture
185
Gardner DK ( 1999 ) Development of serum-free media for the culture and transfer of human blastocysts . Human Reproduction 13 (Suppl. 4): 218 –225.
Gardner DK ( 2007 ) Noninvasive metabolic assessment of single cells . Methods in Molecular Medicine 132 : 1 –9.
Gardner DK , Schoolcraft WB ( 1999 ) In vitro culture of human blastocysts. In: Jansen R , Mortimer D (eds.) Towards Reproductive Certainty: Infertility and Genetics beyond 1999 . Parthenon Publishing Group , Carnforth, UK .
Gardner DK , Schoolcraft WB , Wagley L , et al . ( 1998 ) A prospective randomized trial of blastocyst culture and transfer in in-vitro fertilization . Human Reproduction 13 (12): 3434 –3440.
Gardner DK , Stevens J , Sheehan CB , Schoolcraft WB ( 2007 ) Analysis of blastocyst morphology. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Taylor-Francis , London , pp. 79–88.
Gianaroli L , Magli C , Ferraretti A , et al . ( 1996 ) Reducing the time of sperm-oocyte interaction in human IVF improves the implantation rate . Human Reproduction 11 : 166 –171.
Gott AL , Hardy K , Winston RML , Leese HJ ( 1990 ) Noninvasive measurement of pyruvate and glucose uptake and lactate production by single human preimplantation embryos . Human Reproduction 5 : 104 –110.
Gregory L ( 1998 ) Ovarian markers of implantation potential in assisted reproduction . Human Reproduction Supplement 134 : 117 –132.
Gregory L , Leese HJ ( 1996 ) Determinants of oocyte and pre-implantation embryo quality metabolic requirements and the potential role of cumulus cells . Human Reproduction 11 : 96 –102.
Grifo JA , Boyle A , Fischer E ( 1990 ) Preembryo biopsy and analysis of blastomeres by in situ hybridisation . American Journal of Obstetrics and Gynecology 163 : 2013 –2019.
Hamberger L , Nilsson L , Sjögren A ( 1998 ) Microscopic imaging techniques: practical aspects . Human Reproduction 13 : Abstract book 1: 15 .
Harrison K , Wilson L , Breen T , et al . ( 1988 ) Fertilization of human oocytes in relation to varying delay before insemination . Fertility and Sterility 50 (2): 294 –297.
Hashimoto S , Iwamoto D , Taniguchi S , et al . ( 2009 ) Successful culture and time-lapse photography of individual human embryos using non-porous poly-(dimethylsiloxane) micro-well plates . Fertility and Sterility 92 (3): S36 –S36.
Hnida C , Ziebe S ( 2007 ) Morphometric analysis of human embryos. In: Elder K , Cohen J (eds.) Preimplantation
Embryo Evaluation and Selection . Informa Press , London , pp. 89–100.
Hollywood K Brison DR, Goodacre R ( 2006 ) Metabolomics: current technologies and future trends . Proteomics 6 (17): 4716 –4723.
Hook EB ( 1983 ) Down syndrome rates and relaxed selection at older maternal ages . American Journal of Human Genetics 35 (6): 1307 –1313.
Hook EB , Cross PK ( 1987 ) Rates of mutant and inherited structural cytogenetic abnormalities detected at amniocentesis: results on about 63,000 fetuses . Annals of Human Genetics 51 (Pt 1): 27 –55.
Houghton FD , Hawkhead JA , Humpherson PG , et al . ( 2002 ) Non-invasive amino acid turnover predicts human embryo developmental capacity . Human Reproduction 17 (4): 999 –1005.
Houghton FD , Leese HJ ( 2004 ) Metabolism and developmental competence of the preimplantation embryo . European Journal of Obstetrics, Gynecology and Reproductive Biology 115 (Suppl. 1): S92 –96.
Huntriss J , Picton H ( 2008 ) Epigenetic consequences of assisted reproduction and infertility on the human preimplantation embryo . Human Fertility 11 (2): 85 –94.
Hurley J , Huntriss J , Adjaye J ( 2000 ) Molecular approaches to the study of gene expression during human preimplantation development . Human Fertility 3 : 48 –51.
James A ( 2007 ) Human pronuclei as a mode of predicting viability. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Taylor-Francis , London , pp. 31–40.
Kahraman S , Yakin K , Dönmez E , et al . ( 2000 ) Relationship between granular cytoplasm of oocytes and pregnancy outcome following intracytoplasmic sperm injection . Human Reproduction 15 (11): 2390 –2393.
Keefe DL , Franco S , Liu L , et al . ( 2005 ) Telomere length predicts embryo fragmentation aft er in vitro fertilization in women – toward a telomere theory of reproductive aging in women . American Journal of Obstetrics and Gynecology 192 (4): 1256–1260; discussion 1260 –1261.
Khan I , Staessen C , Van den Abbeel E , et al . ( 1989 ) Time of insemination and its effect on in vitro fertilization, cleavage and pregnancy rates in GnRH agonist/HMG-stimulated cycles . Human Reproduction 4 (5): 531 –535.
Kimber SJ , Sneddon SF , Bloor DJ , et al . ( 2008 ) Expression of genes involved in early cell fate decisions in human embryos and their regulation by growth factors . Reproduction 135 : 635 –647.

Chapter 11: Oocyte retrieval and embryo culture
186
Kruger TF , Stander FSH , Smith K , Van Der Merue JP , Lombard CJ ( 1987 ) Th e eff ect of serum supplementation on the cleavage of human embryos . Journal of In Vitro Fertilization and Embryo Transfer 4 : 10 .
Kuliev A , Verlinsky Y ( 2008 ) Impact of preimplantation genetic diagnosis for chromosomal disorders on reproductive outcome . Reproductive Biomedicine Online 16 (1): 9 –10.
Lane M , Gardner DK ( 2005 ) Understanding cellular disruptions during early embryo development that perturb viability and fetal development . Reproduction and Fertility Development 17 (3): 371 –378.
Leese HJ ( 1987 ) Analysis of embryos by noninvasive methods . Human Reproduction 2 : 37 –40.
Leese HJ ( 2002 ) Quiet please, do not disturb: a hypothesis of embryo metabolism and viability . Bioessays 24 (9): 845 –849.
Leese HJ , Baumann CG , Brison DR , McEvoy TG , Sturmey RG ( 2008 ) Metabolism of the viable mammalian embryo: quietness revisited . Molecular Human Reproduction 14 (12): 667 –672.
Leese HJ , Donnay I , Th ompson JG ( 1998 ) Human assisted conception: a cautionary tale. Lessons from domestic animals . Human Reproduction 13 (Suppl. 4): 184 –202.
Lesny P , Killick SR ( 2004 ) Th e junctional zone of the uterus and its contractions . British Journal of Obstetrics and Gynaecology 111 (11): 1182 –1189.
Levron J , Munné S , Willadsen S , Rosenwaks Z , Cohen J ( 1995 ) Male and female genomes associated in a single pronucleus in human zygotes . Journal of Assisted Reproduction and Genetics 12 (Suppl.): 27s .
Lin YC , Chang SY , Lan KC , et al . ( 2003 ) Human oocyte maturity in vivo determines the outcome of blastocyst development in vitro . Journal of Assisted Reproduction and Genetics 20 (12): 506 –512.
Liu L , Blasco MA , Keefe DL ( 2002 ) Requirement of functional telomeres for metaphase chromosome alignments and integrity of meiotic spindles . EMBO Reports 3 (3): 230 –234.
Lundqvist M , Johansson Ö Milton K , Westin C , Simberg N ( 2001 ) Does pronuclear morphology and/or early cleavage rate predict embryo implantation potential? Reproductive Biomedicine Online 2 : 12 –16.
Ma S , Kalousek DK , Zouves C , et al . ( 1990 ) Th e chromosomal complements of cleaved human embryos resulting from in vitro fertilization . Journal of In Vitro Fertilization and Embryo Transfer 7 : 16 –21.
Madaschi C , Aoki T , de Almeida Ferreira Braga DP , et al . ( 2009 ) Zona pellucida birefringence score and meiotic spindle visualization in relation to embryo development and ICSI outcomes . Reproductive Biomedicine Online 18 (5): 681 –686.
Marrs RP , Saito H , Yee B , Sato F , Brown J ( 1984 ) Eff ect of variation of in vitro culture techniques upon oocyte fertilization and embryo development in human in vitro fertilization procedures . Fertility and Sterility 41 : 519 –523.
Mastenbroek S , Twisk M , van der Veen F , Repping S ( 2008 ) Preimplantation genetic screening . Reproductive BioMedicine Online 17 (2): 293 .
McKenzie LJ , Pangas SA , Carson SA , et al . ( 2004 ) Human cumulus granulosa cell gene expression: a predictor of fertilization and embryo selection in women undergoing IVF . Human Reproduction 19 (12): 2869 –2874.
Ménézo Y , Barak Y ( 2000 ) Comparison between day-2 embryos obtained either from ICSI or resulting from short insemination IVF: infl uence of maternal age . Human Reproduction 15 (8): 1776 –1780.
Ménézo Y , Chouteau J , Veiga A ( 2001 ) In vitro fertilization and blastocyst transfer for carriers of chromosomal translocation . European Journal of Obstetrics, Gynecology and Reproductive Biology 96 (2): 193 –195.
Ménézo Y , Dumont M , Hazout A , et al . ( 1995 ) Culture and co-culture techniques. In: Hedon B , Bringer J , Mares P. (eds.) Fertility and Sterility , IFFS-95, Parthenon Publishing Group , New York , pp. 413–418.
Ménézo Y , Elder K , Viville S ( 2006 ) Soluble HLA-G release by the human embryo: an interesting artefact? Reproductive Biomedicine Online 13 (6): 763 –764.
Ménézo Y , Guerin JF , Czyba JC ( 1990 ) Improvement of human early embryo development in vitro by co-culture on monolayers of Vero cells . Biological Reproduction 42 : 301 –305.
Ménézo Y , Hazout A , Dumont M , Herbaut N , Nicollet B ( 1992 ) Coculture of embryos on Vero cells and transfer of blastocyst in human . Human Reproduction 7 : 101 –106.
Ménézo Y , Janny L ( 1997 ) Infl uence of paternal factors in early embryogenesis. In: Barratt C , De Jonge C , Mortimer D , Parinaud J (eds.) Genetics of Human Male Infertility . EDK , Paris , pp. 246–257.
Ménézo Y , Testart J , Perrone D ( 1984 ) Serum is not necessary in human in vitro fertilization, early embryo culture, and transfer . Fertility and Sterility 42 : 750 .
Ménézo Y , Veiga A , Benkhalifa M ( 1998 ) Improved methods for blastocyst formation and culture . Human Reproduction Supplement 13 (Suppl. 4): 256 –265.
Meriano JS , Alexis J , Visram-Zaver S , Cruz M , Casper RF ( 2001 ) Tracking of oocyte dysmorphisms for ICSI patients may prove relevant to the outcome in subsequent patient cycles . Human Reproduction 16 (10): 2118 –2123.

Chapter 11: Oocyte retrieval and embryo culture
187
Meriano JS , Clark C , Kadesky K , Laskin CA ( 2004 ) Binucleated and multinucleated blastomeres in embryos derived from human assisted reproduction cycles . Reproductive Biomedicine Online 9 (5): 511 –520.
Michael AE , Gregory L , Piercy EC , et al . ( 1995 ) Ovarian 11β-hydroxysteroid dehydrogenase activity is inversely related to the outcome of in vitro fertilization-embryo transfer treatment cycles . Fertility and Sterility 64 (3): 590 –598.
Mio Y , Maeda K ( 2008 ) Time-lapse cinematography of dynamic changes occurring during in vitro development of human embryos . American Journal of Obstetrics and Gynecology 199 : 660 .e1–660.e5.
Montag M , Schimming T , Koster M , et al . ( 2008 ) Oocyte zona birefringence intensity is associated with embryonic implantation potential in ICSI cycles . Reproductive Biomedicine Online 16 (2): 239 –244.
Muggleton-Harris AL , Findlay I , Whittingham DG ( 1990 ) Improvement of the culture conditions for the development of human preimplantation embryos . Human Reproduction 5 : 217 –520.
Munné S , Alikani M , Levron J , et al . ( 1995a ) Fluorescent in situ hybridisation in human blastomeres. In: Hedon B , Bringer J , Mares P (eds.) Fertility and Sterility . IFFS-95, Parthenon Publishing Group , New York , pp. 425–438.
Munné S , Alikani M Tomkin G , Grifo J , Cohen J ( 1995b ) Embryo morphology, developmental rates, and maternal age are correlated with chromosomal abnormalities . Fertility and Sterility 64 : 382 –391.
Munné S , Cohen J ( 1998 ) Chromosome abnormalities in human embryos . Human Reproduction Update 4 (6): 842 –855.
Munné S , Lee A , Rosenwaks Z , Grifo J , Cohen J ( 1993 ) Diagnosis of major chromosome aneuploidies in human preimplantation embryos . Human Reproduction 8 : 2185 –2191.
Munné S , Wells D ( 2003 ) Questions concerning the suitability of comparative genomic hybridization for preimplantation genetic diagnosis . Fertility and Sterility 80 (4): 871 –872; discussion 875.
Oehninger S , Acosta AA , Veeck LL , Simonetti S , Muasher SJ ( 1989 ) Delayed fertilisation during in vitro fertilization and embryo transfer cycles: analysis of cause and impact of overall results . Fertility and Sterility 52 : 991 –997.
Pampiglione JS , Mills C , Campbell S , et al . ( 1990 ) Th e clinical outcome of reinsemination of human oocytes fertilized in vitro . Fertility and Sterility 53 : 306 –310.
Paternot G , Devroe J , Debrock S , D’Hooghe TM , Spiessens C ( 2009 ) Intra- and inter-observer analysis in the morphological assessment of
early-stage embryos . Reproductive Biology and Endocrinology 7 : 105 .
Pickering SJ , Braude PR , Johnson MH , Cant A , Currie J ( 1990 ) Transient cooling to room temperature can cause irreversible disruption of the meiotic spindle in the human oocyte . Fertility and Sterility 54 : 102 –108.
Picton HM , Elder K , Houghton FD , et al . ( 2010 ) Association between amino acid turnover and chromosome aneuploidy during human preimplantation embryo development in vitro. Molecular Human Reproduction 2010; advance access, doi: 10.1093/molehr/gaq040
Plachot M , de Grouchy J , Montagut J , et al . ( 1987 ) Multi-centric study of chromosome analysis in human oocytes and embryos in an IVF programme . Human Reproduction 2 : 29 .
Plachot M , Mandelbaum J , Junca AM , Cohen J , Salat-Baroux J ( 1993 ) Coculture of human embryo with granulosa cells . Contraception, Fertility and Sex 19 : 632 –634.
Plachot M , Veiga A , Montagut J , et al . ( 1988 ) Are clinical and biological IVF parameters correlated with chromosomal disorders in early life: a multicentric study . Human Reproduction 3 : 627 –635.
Platteau P , Staessen C , Michiels A , et al . ( 2006 ) Which patients with recurrent implantation failure aft er IVF benefi t from PGD for aneuploidy screening? Reproductive Biomedicine Online (3): 334 –339.
Posillico JT , and Th e Metabolomics Study Group for Assisted Reproductive Technologies ( 2007 ) Selection of viable embryos and gametes by rapid, noninvasive metabolomic profi ling of oxidative stress biomarkers. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Taylor-Francis , London , pp. 245–262.
Purdy JM ( 1982 ) Methods for fertilization and embryo culture in vitro, In: Edwards RG , Purdy JM (eds.) Human Conception In Vitro. Academic Press , London , p. 135.
Quinn P , Warner GM , Klein JE , Kirby C ( 1985 ) Culture factors aff ecting the success rate of in vitro fertilization and embryo transfer . Annals of the New York Academy of Sciences 412 : 195 .
Roert J , Verhoeff A , van Lent M , Hisman GJ , Zeilmaker GH ( 1995 ) Results of decentralised in vitro fertilization treatment with transport and satellite clinics . Human Reproduction 10 : 563 –567.
Salha O , Nugent D , Dada T , et al . ( 1998 ) Th e relationship between follicular fl uid aspirate volume and oocyte maturity in in vitro fertilization cycles . Human Reproduction 13 (7): 1901 –1906.

Chapter 11: Oocyte retrieval and embryo culture
188
Sargent IL ( 2005 ) Does ‘soluble’ HLA-G really exist? Another twist to the tale . Molecular Human Reproduction 11 (10): 695 –698.
Scott L ( 2003 ) Pronuclear score as a predictor of embryo development . Reproductive BioMedicine Online 6 : 201 –214.
Scott L , Alvero R , Leondires M , et al . ( 2000 ) Th e morphology of human pronuclear embryos is positively related to blastocyst development and implantation . Human Reproduction 15 : 2394 –2403.
Scott L , Smith S ( 1998 ) Th e successful use of pronuclear embryo transfers the day following oocyte retrieval . Human Reproduction 13 : 1003 –1013.
Sermondade N , Hugues JN , Cedrin-Durnerin I , et al . ( 2010 ) Should all embryos from day 1 rescue intracytoplasmic sperm injection be transferred during frozen-thawed cycle? Fertility and Sterility Jan 14. [Epub ahead of print]
Sermondade N , Mandelbaum J ( 2009 ) Mastenbroek controversy or how much ink is spilled on preimplantation genetic screening subject? Gynécologie Obstétrique & Fertilité 37 (3): 252 –256.
Sher G , Keskintepe L , Nouriani M , Roussev R , Batzofi n J ( 2004 ) Expression of sHLA-G in supernatants of individually cultured 46-h embryos: a potentially valuable indicator of ‘embryo competency’ and IVF outcome . Reproductive Biomedicine Online 9 (1): 74 –78.
Skiadas CC , Racowsky C ( 2007 ) Development rate, cumulative scoring and embryonic viability. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Taylor-Francis , London , pp. 101–122.
Son WY , Chung JT , Demirtas E , et al . ( 2008 ) Comparison of in-vitro maturation cycles with and without in-vivo matured oocytes retrieved . Reproductive Biomedicine Online 17 (1): 59 –67.
Sturmey RG , Brison DR , Leese HJ ( 2008 ) Symposium: innovative techniques in human embryo viability assessment. Assessing embryo viability by measurement of amino acid turnover . Reproductive Biomedicine Online 17 (4): 486 –496.
Tesarik J , Greco E ( 1999 ) Th e probability of abnormal preimplantation development can be predicted by a single static observation on pronuclear stage morphology . Human Reproduction 14 : 1318 –1323.
Tesarik J , Junca AM , Hazout A , et al . ( 2000 ) Embryos with high implantation potential
aft er intracytoplasmic sperm injection can be recognized by a simple, non-invasive examination of pronuclear morphology . Human Reproduction 15 : 1396 –1399.
Van Blerkom J ( 1996 ) Th e infl uence of intrinsic and extrinsic factors on the developmental potential of chromosomal normality of the human oocyte . Journal of the Society of Gynecological Investigation 3 : 3 –11.
Van Blerkom J , Atczak M , Schrader R ( 1997 ) Th e developmental potential of the human oocyte is related to the dissolved oxygen content of follicular fl uid: association with vascular endothelial growth factor concentrations and perifollicular blood fl ow characteristics . Human Reproduction 12 : 1047 –1055.
Van Blerkom J , Davis P , Alexander S ( 2000 ) Diff erential mitochondrial distribution in human pronuclear embryos leads to disproportionate inheritance between blastomeres: relationship to microtubular organization, ATP content and competence . Human Reproduction 15 (12): 2621 –2633.
Van Blerkom J , Henry G ( 1992 ) Oocyte dysmorphism and aneuploidy in meiotically mature human oocytes aft er ovarian stimulation . Human Reproduction 7 : 379 –390.
Veeck LL ( 1986 ) Insemination and fertilization. In: Jones HW Jr., Jones GS , Hodgen GD , Rosenwaks Z (eds.) In Vitro Fertilization – Norfolk . Williams & Wilkins , Baltimore , p. 183.
Veeck LL ( 1988 ) Oocyte assessment and biological performance . Annals of the New York Academy of Sciences 541 : 259 –262.
Verlinsky Y , Cieslak J , Freidine M , et al . ( 1995 ) Pregnancies following pre-conception diagnosis of common aneuploidies by fl uorescent in situ hybridisation . Molecular Human Reproduction 10 : 1927 –1934.
Verlinsky Y , Strom C , Cieslak J , et al . ( 1996 ) Birth of healthy children aft er preimplantation diagnosis of common aneuploidies by polar body fl uorescent in situ hybridisation analysis . Fertility and Sterility 66 : 126 –129.
Weimer KE , Cohen J , Tucker MJ , Godke A ( 1998 ) Th e application of co-culture in assisted reproduction: 10 years of experience with human embryos . Human Reproduction Supplement 13 (Suppl. 4): 226 –238.
Wells D ( 2007 ) Future genetic and other technologies for assessing embryos. In: Elder K , Cohen J (eds.) Preimplantation Embryo Evaluation and Selection . Informa Press , London , pp. 287–300.

Chapter 11: Oocyte retrieval and embryo culture
189
Woolcott R , Stanger J ( 1997 ) Potentially important variables identifi ed by trans-vaginal ultrasound guided embryo transfer . Human Reproduction 12 : 963 –966.
Woolcott R , Stanger J ( 1998 ) Ultrasound tracking of the movement of embryo-associated air bubbles on standing aft er transfer . Human Reproduction 13 (8): 2107 –2109.
Wunder DM , Mueller MD , Birkhäuser MH , Bersinger NA ( 2005 ) Steroids and protein markers in the follicular fl uid as indicators of oocyte quality in patients with and without endometriosis . Journal of Assisted Reproduction and Genetics 22 (6): 257 –264.
Ziebe S , Loft A , Petersen JH , et al . ( 2001 ) Embryo quality and developmental potential is compromised by age . Acta Obstetricia et Gynecologica Scandinavica 80 (2): 169 –174.
Ziebe S , Lundin K , Janssens R , Helmgaard L , Arce JC ( 2007 ) MERIT (Menotrophin vs Recombinant FSH in vitro Fertilisation Trial) Group. Infl uence of ovarian stimulation with HP-hMG or recombinant FSH on embryo quality parameters in patients undergoing IVF . Human Reproduction 22 (9): 2404 –2413.
Ziebe S , Lundin K , Loft A , et al . ( 2003 ) CEMAS II and Study Group; FISH analysis for chromosomes 13, 16, 18, 21, 22, X and Y in all blastomeres of IVF pre-embryos from 144 randomly selected donated human oocytes and impact on pre-embryo morphology . Human Reproduction 18 (12): 2575 –2581.
In-vitro maturation Albertini DF , Sanfi ns A , Combelles CM ( 2003 )
Origins and manifestations of oocyte maturation competencies . Reproductive Biomedicine Online 6 : 410 –415.
Barnes FL , Sirard MA ( 2000 ) Oocyte maturation . Seminars in Reproductive Medicine 18 : 123 –131.
Cha KY , Han SY , Chung HM , et al . ( 2000 ) Pregnancies and deliveries aft er in vitro maturation culture followed by in vitro fertilization and embryo transfer without stimulation in women with polycystic ovary syndrome . Fertility and Sterility 73 : 978 .
Cha KY , Koo JJ , Ko JJ , et al . ( 1991 ) Pregnancy aft er in vitro fertilization of human follicular oocytes collected from nonstimulated cycles, their culture in vitro and their transfer in a donor oocyte program . Fertility and Sterility 55 : 109 –113.
Chian RC , Buckett WM , Tan SL ( 2004a ) In-vitro maturation of human oocytes . Reproductive Biomedicine Online 8 : 148 –166.
Chian RC , Buckett WM , Tulandi T , Tan SL ( 2000 ) Prospective randomized study of human chorionic gonadotrophin priming before immature
oocyte retrieval from unstimulated women with polycystic ovarian syndrome . Human Reproduction 15 : 165 –170.
Chian RC , Gulekli B , Buckett WM , Tan SL ( 2001 ) Pregnancy and delivery aft er cryopreservation of zygotes produced by in-vitro matured oocytes retrieved from a woman with polycystic ovarian syndrome . Human Reproduction 16 : 1700 –1702.
Chian RC , Lim JH , Tan SL ( 2004b ) State of the art in in-vitro oocyte maturation . Current Opinion in Obstetrics and Gynecology 16 : 211 –219.
Child TJ , Abdul-Jalil AK , Gulekli B , Tan SL ( 2001 ) In vitro maturation and fertilization of oocytes from unstimulated normal ovaries, polycystic ovaries, and women with polycystic ovary syndrome . Fertility and Sterility 76 : 936 –942.
Child TJ , Phillips SJ , Abdul-Jalil AK , Gulekli B , Tan SL ( 2002 ) A comparison of in vitro maturation and in vitro fertilization for women with polycystic ovaries . Obstetrics and Gynecology 100 : 665 –670.
Combelles CMH , Fissore RA , Albertini DF , Racowsky C ( 2006 ) In vitro maturation of human oocytes and cumulus cells using a co-culture three-dimensional collagen gel system . Human Reproduction 20 (5): 1349 –1358.
Edwards RG ( 1965 ) Maturation in vitro of human ovarian oocytes . Lancet 2 : 926 –969.
Hreinsson J , Rosenlund B , Frid B , et al . ( 2003 ) Recombinant LH is equally eff ective as recombinant hCG in promoting oocyte maturation in a clinical in-vitro maturation programme: a randomized study . Human Reproduction 18 (10): 2131 –2136.
Ménézo Y , Elder K , Benkhalifa M , Dale B ( 2010 ) DNA methylation and gene expression in IVF . Reproductive Biomedicine Online 20 (6): 709 –710.
Moor RM , Dai Y , Lee C , Fulka J Jr. ( 1998 ) Oocyte maturation and embryonic failure . Human Reproduction Update 4 : 223 –236.
Picton H , Briggs D , Gosden R ( 1998 ) Th e molecular basis of oocyte growth and development . Molecular and Cellular Endocrinology 145 : 27 –37.
Pincus G , Enzmann EV ( 1935 ) Comparative behavior of mammalian eggs in vivo and in vitro . Journal of Experimental Medicine 62 : 665 –678.
Roberts R , Franks S , Hardy K ( 2002 ) Culture environment modulates maturation and metabolism of human oocytes . Human Reproduction 17 : 2950 –2956.
Sutton ML , Gilchrist RB , Th ompson JG ( 2003 ) Eff ects of in-vivo and in-vitro environments on the metabolism of the cumulus–oocyte complex and its infl uence on oocyte developmental capacity . Human Reproduction Update 9 : 35 –48.

Chapter 11: Oocyte retrieval and embryo culture
190
Tan SL , Child T ( 2001 ) In-vitro maturation of oocytes from unstimulated polycystic ovaries . Reproductive Biomedicine Online 4 (Suppl. 1): 18 –23.
Trounson A , Wood C , Kausche A ( 1994 ) In vitro maturation and the fertilization and developmental competence of oocytes recovered from untreated
polycystic ovarian patients . Fertility and Sterility 62 : 353 –362.
Veeck LL , Wortham JW Jr., Witmyer J , et al . ( 1983 ) Maturation and fertilization of morphologically immature human oocytes in a program of in vitro fertilization . Fertility and Sterility 39 : 594 –602.

Chapter
191
Cryopreservation of gametes and embryos
Principles of cryobiology Th e fi rst live births following frozen-thawed embryo transfer were reported in 1984 and 1985 by groups in Australia, the Netherlands and the UK. Since that time, the original protocols have been modifi ed and simpli-fi ed such that cryopreservation as an adjunct to a rou-tine IVF program may lead to successful survival of up to 80% of the embryos frozen, with subsequent preg-nancy and live birth rates that contribute signifi cantly to cumulative conception rates aft er fresh embryo transfer. Although the routine protocols required are simple and easily undertaken, an understanding of the basic principles of cryobiology involved is essential to ensure that the methodology is correctly and success-fully applied, in order to minimize cell damage during the processes of freezing and thawing. Th ere are two major classes of physical stresses that cells are exposed to during freezing: 1. Direct eff ects of reduced temperature 2. Physical changes associated with ice formation .
Direct eff ects of reduced temperatures Cold shock injury (damage to cell structure and function arising from a sudden reduction in tem-perature) is species-specifi c and well documented for spermatozoa (cattle, pig), oocytes and embryos (pig). Th is phenomenon is associated with modifi cations in membrane permeability and changes in the cyto-skeletal structure (reviewed by Watson and Morris, 1987 ), but is not evident following conventional cool-ing of human sperm and embryos. However, when freezing oocytes, ovarian tissue and testicular tissue, the possibility of sublethal injuries does exist, par-ticularly those associated with breakdown of mitotic spindles.
Physical changes associated with ice formation
Th e temperature changes observed during the freezing of an aqueous solution are illustrated in Figure 12.1 . Water and aqueous solutions have a strong tendency to cool below their melting point before nucleation of ice occurs: this phenomenon is referred to as supercooling, or more correctly under-cooling. For example, whilst 0°C is the melting point of ice, the temperature of water may be reduced sig-nifi cantly below 0°C before ice formation occurs, and in carefully controlled conditions water may be cooled to approximately –40°C before ice nucleation becomes inevitable (homogeneous nucleation temperature). Following ice nucleation and initial crystal growth the temperature rises to its melting point and remains relatively constant at that temperature during the sub-sequent phase change to ice (“latent heat plateau”), when the temperature then changes more rapidly to the environment temperature.
12 0
–2
–4
–6Te
mp
era
ture
(d
eg
C)
–8Time
Figure 12.1 Temperature changes during the freezing of an aqueous solution of glycerol (5% w/v).
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 12: Cryopreservation of gametes and embryos
192
Th e tendency of a system to supercool is related to a number of factors including temperature, rate of cooling, volume, exclusion of atmospheric ice nuclei and purity of particulates. In cryopreservation of cells and tissues in IVF systems, there is thus a strong tendency for supercooling to occur. To avoid the damaging eff ects of supercooling on cells and in par-ticular embryos (see below) ice formation is initiated in a controlled manner. Th is is commonly referred to as “seeding” – although, strictly speaking, this term refers to the introduction of a crystal to an under-cooled solution. “Nucleation” is the initiation of ice other than by seeding, and this is the process gener-ally practiced in IVF.
Supercooling and cell survival Controlled ice formation during freezing is recog-nized to be a key factor in determining the viabil-ity of embryos following freezing and thawing (see Whittingham, 1977 ). In a carefully controlled series of experiments, samples which were nucleated below –9°C had a low viability, whilst nucleation at higher subzero temperatures of –5°C to –7.5°C resulted in much higher viability ( Figure 12.2 ).
An analysis of the spontaneous nucleation behav-ior of straws ( Figure 12.3 ) clearly demonstrates that if nucleation is not controlled, a poor recovery of embryos would be expected .
Th e physical basis of this injury is clear from exam-ination of the thermal histories of supercooled straws
( Figure 12.4 ). Th e diff erences between laboratories that achieve good results and those that are less suc-cessful can oft en be attributed to the practical step of ice nucleation, or “seeding.” Straws can be frozen hori-zontally or vertically – this has no eff ect on viability or ease of ice nucleation. Embryos sink in the cryopro-tective additive and will always be found at the wall of the straw when frozen horizontally, or at the bottom of the column of liquid when frozen vertically. Following thermal equilibration (“holding”) at the nucleation temperature (–7°C), ice formation is initiated by touching the outside of the straw or ampule with a liquid nitrogen cooled spatula, forceps, cotton bud etc., at the level of the meniscus (seeding at both ends of a horizontal straw has also been advocated). Th is causes a local cold spot on the vessel wall, which leads to ice nucleation. Immediately following ice nucleation the temperature will rise rapidly (cf. Figure 12.1 ) and the ice front will propagate through the sample. Following ice formation the temperature returns at a rate of 2.5°C/min to –7°C. Cellular dehydration then occurs during subsequent slow cooling .
By contrast, in a straw supercooled to –15°C, spon-taneous ice formation again results in a temperature rise followed by a rapid rate of cooling at 10°C/min to –5°C. Th e combination of a rapid rate of cooling and a large reduction in temperature does not allow the cell to dehydrate, and lethal intracellular ice formation is then inevitable ( Table 12.1 ). Th is has been observed by direct cryomicroscopy.
Ice crystallization in an aqueous solution eff ect-ively removes some water from solution. Th e remain-ing aqueous phase becomes more concentrated, and a two-phase system of ice and concentrated solution coexists. As the temperature is reduced, more ice forms and the residual non-frozen phase becomes increas-ingly concentrated. For example, in glycerol and water a two-phase system occurs at all temperatures to –45°C. At –45°C the non-frozen phase solidifi es, with a glycerol concentration of 64% w/v; this is the eutectic temperature. In dilute aqueous solutions such as culture media, there is a dramatic increase in ionic composition following ice formation and by –10°C the salt concentration reaches c . 3 molal – not surprisingly, this is lethal to cells. Cryoprotective additives reduce cellular damage during freezing and thawing by simply increasing the volume of the residual unfrozen phase. Th is reduces the ionic composition of the solution at any subzero temperature. It must also be noted that all
100
80
60
40
20
Sur
viva
l (%
)
0–4 –5 –6 –7 –8 –9 –10 –11 –12
Nucleation Temperature (deg C)
Figure 12.2 The survival of mouse cell embryos after seeding at various subzero temperatures. Redrawn from Whittingham ( 1977 ).

Chapter 12: Cryopreservation of gametes and embryos
193
other physical parameters of the solution change fol-lowing the formation of ice, including gas content, vis-cosity and pH.
Cryoprotectants Cryoprotectant additives (CPAs) are thought to pro-tect cells by stabilizing intracellular proteins, reducing or eliminating lethal intracellular ice formation, and by moderating the impact of concentrated intra- and extracellular electrolytes. Th e fi rst successful use of a cryoprotectant was in 1949, when Polge et al . used
glycerol to freeze semen; glycerol is still commonly used as a cryoprotectant today. All cryoprotectants are completely miscible with water, easily permeate cell membranes, and some (but not all) are nontoxic even at high concentrations. All are hyperosmotic, and they can be divided into two groups : 1. Permeating: glycerol, ethylene glycol (EG), 1,2-
propanediol (PROH) and dimethylsulfoxide (DMSO) penetrate the cell membrane, although more slowly than water. Inside the cell, they stabilize intracellular proteins, reduce the
Figure 12.3 The measured nucleation temperatures within 0.25 mL straws cool-ing at 0.3°C/min.
Figure 12.4 Measured temperatures within straws. During conventional cryopreservation the straws are held at a temperature of –7°C and nucleated, the resultant rise in temperature following ice nucleation is small. In the absence of induced nucleation the straws may reach very low temperatures before spontan-eous nucleation occurs. A large rise in temperature to the melting point of the suspending medium then occurs followed by a rapid reduction in temperature; this will inevitably result in intracellular ice for-mation within embryos or oocytes.

Chapter 12: Cryopreservation of gametes and embryos
194
temperature at which intracellular ice forms, and minimize osmotic damage due to electrolyte concentration eff ects. Glycerol penetrates tissue less readily than DMSO, PROH and EG. Th ese newer cryoprotectants have higher water solubility, rapid tissue penetration and induce less osmotic damage at high concentrations.
2. Non-permeating: a variety of sugars, polymers and amphipathic compounds have been used as non-permeating cryoprotectants. Raffi nose and lactose decrease the percentage of unfrozen water and/or decrease salt concentrations. Glycine, proline and trehalose are amphipathic compounds that interact with membrane lipids and proteins to alter phase transitions and hydration status .
Cryoprotectants should always be used in combin-ation with non-permeating osmolytes such as sucrose or mannitol. Th ese act as osmotic buff ers to protect against cell swelling during the addition/removal of cryoprotectants. Egg yolk has been added to cryo-preservation medium used to preserve animal sperm, since the low-density lipoprotein fraction of egg yolk is thought to protect against cold shock. However, this is no longer recommended for freezing human cells, as it introduces batch-to-batch variation and the possibility of bacterial contamination .
Th e pioneering studies on mammalian embryo cryopreservation used either glycerol or DMSO as cryoprotectants, but these have been superseded by the protocol of Lasalle et al . ( 1985 ), which uses PROH. PROH is considered to have a higher permeability to human embryos than either glycerol or DMSO, and is less toxic than DMSO. Th e real toxicity of cryopro-tectants in cells is largely unknown; Stanic et al . ( 2000 ) reported that most of the decrease in sperm motility during cryopreservation was due to exposure to cryo-protectants rather than to the freezing process.
Factors that aff ect cellular response to freezing Surface area In general, the larger the cell, the slower it must be cooled to survive freezing. For example, a human oocyte has a diameter of 120 µm, a volume of 9.05 × 10 5 µm 3 and a surface area of 4.5 × 10 4 µm 2 ; a human sperm cell has a volume of 28 µm and a surface area of 120 µm 2 . Th us, the fl attened paddle-shaped sperm cell has a surface area to volume ratio of 4.3, whereas the ratio in the spherical oocyte is only 0.05. Consequently, when exposed to CPAs, spermatozoa reach osmotic equilibrium much faster than oocytes, and optimum
Table 12.1 Factors associated with cooling and cryopreservation that contribute to cellular injury and death in biological systems (reproduced with permission from Shaw et al . 2000 )
System Type/cause of damage
All Intracellular ice formation, extracellular ice formation, apoptosis, toxicity, calcium imbalance, free radicals, ATP levels, general metabolism, fertilization failure, cleavage failure, intracellular pH, parthenogenetic activation, cleavage
Membrane Rupture, leakage, fusion, microvilli, phase transition
Chromosomes Loss/gain, polyspermy, polygny (failure to extrude polar body), tetraploidy.
DNA Apoptosis, fusion, rearrangements
Cytoskeleton Microtubules dissolve, actin
Proteins/enzymes Dehydration, loss of function
Ultrastructure Microvilli, mitochondria, vesicles, cortical granules, zona pellucida
Zona pellucida Hardening, fracture
Lipids Free radicals?

Chapter 12: Cryopreservation of gametes and embryos
195
cooling rates for spermatozoa are much higher than those for oocytes and embryos .
Cell volume changes At temperatures near 0°C, abrupt changes in volume can immediately damage cells and also make them more susceptible to stress during subsequent cooling or thawing procedures; therefore extreme fl uctuations in cell volume must be avoided during CPA equilibra-tion. Th e duration of exposure to these potentially toxic chemicals should also be minimized: CPA toxicity can be reduced by lowering the temperature of exposure, but this would require a longer exposure time.
Cooling to subzero temperature When large cells such as oocytes are frozen in molar concentrations of CPAs, their survival is strongly dependent on cooling rate, and the specifi c optimum cooling rate depends on both the type and the concen-tration of CPA. Cell survival is equally dependent on warming rate, and the optimum warming rate depends on both the CPA and its concentration, as well as on the cooling rate that preceded it. Cryobiology studies have shown that diff erent types of cell have diff erent optimal cooling rates, even when frozen in the same solution. Th is is especially relevant to the cryopreservation of tissues such as ovarian cortex that are made up of many diff erent types of cell, each with its own characteristic size, shape and permeability properties. Cooling and warming conditions that are optimal for one cell type may be harmful to others.
Osmotic events As mentioned above, when aqueous solutions are frozen, water is removed in the form of ice, causing the cells to become increasingly concentrated as the temperature falls. Th e reverse occurs during thawing. Cells in suspension are not punctured by ice crystals (see Figure 12.5 ), nor are they mechanically dam-aged by ice. Cells partition into the unfrozen fraction and are exposed to increasing hypertonic solutions. Varying amounts of water may be removed osmotic-ally from the cell, dependent on the rate of cooling. At “slow” rates of cooling, cells may remain essen-tially in equilibrium with the external solution. As the rate of cooling is increased, there is less time for water to move from the cell, which becomes increas-ingly supercooled until eventually intracellular ice is formed. An optimum rate of cooling results from the
balance of these two phenomena. At rates of cooling slower than the optimum, cell death is due to long periods of exposure to hypertonic conditions. At rates of cooling faster than the optimum, cell death is associated with intracellular ice formation, which is inevitably lethal. Th e actual value of the optimum rate is determined by a number of biophysical fac-tors, including cell volume and surface area, per-meability to water, Arrhenius activation energy, and type and concentration of cryoprotective additives. As the cells are frozen, they must respond osmotic-ally to large changes in extracellular fl uid concentra-tions: the effl ux of water during slow freezing (<2°C/min) causes oocytes to undergo osmotic dehydration, with resulting contraction.
Removal of cryoprotectant Although cells in suspension can tolerate exposure to very high concentrations of CPAs, whether or not they survive the freeze-thaw process depends on how the CPA solution is removed. When frozen cells are warmed rapidly, the melting process is equivalent to rapid dilution of the CPA that was concentrated dur-ing the freezing process. As the extracellular milieu
Figure 12.5 Light microscopy of a human oocyte following ice nucleation in the extracellular medium. The oocyte is not punc-tured by ice crystals.

Chapter 12: Cryopreservation of gametes and embryos
196
begins to melt, the rapid infl ux of water into the cells can cause osmotic shock at subzero temperatures. Sensitivity to osmotic shock is therefore a function of the cell’s permeability to water and solutes. Th is shock can be reduced by using a non-permeating substance such as sucrose as an osmotic buff er. Tissues are even more sensitive to osmotic eff ects than are cell suspen-sions, because cells located in the interior of a piece of tissue can respond osmotically only when the neigh-boring cells have also responded .
Cryopreservation protocols Two basic types of cryopreservation are used for cells and tissues: slow freezing and vitrifi cation.
Equilibrium freezing (slow freezing) Th e procedures used for slow freezing of oocytes, embryos and ovarian cortex are generally quite simi-lar. Th e cells or tissues are equilibrated in an aqueous solution containing an optimal concentration (1.0–1.5 M) of cryoprotectant and sucrose (0.1 M) and fro-zen in straws or ampules. Following CPA exposure the temperature is slowly lowered, and ice crystal growth is initiated in the solution (“seeding”). Th e ampules or straws are seeded at –6.5 to –7°C, cooled slowly at 0.3–0.5°C /min to approximately –40°C, then quickly cooled to –150°C before fi nal transfer into liquid nitrogen for storage. Embryos and spermatozoa do not deteriorate when stored even for decades in liquid nitrogen.
Non-equilibrium protocols: vitrifi cation/ultra-rapid freezing Vitrifi cation combines the use of concentrated cryo-protectant solutions with ultra-rapid cooling in order to avoid the formation of ice. Samples reach low tem-peratures in a state that has the molecular structure of a viscous liquid without crystals, forming an amorphous glassy solid. Rapid cooling is oft en carried out by direct contact with liquid nitrogen, and therefore program-mable freezing machines are not needed. Th ere is an inverse correlation between the cryoprotectant con-centrations and cooling rates required, and successful vitrifi cation is based on the use of very high concen-trations of cryoprotectant or cryoprotectant mixtures, with an extremely high cooling rate. However, CPAs are toxic, and high CPA concentrations increase the risk of osmotic shock to the cells, due to a rapid change
in ionic conditions. In order to use vitrifi cation in ART programs, experiments have been directed towards fi nding a practical means of achieving very high cooling and warming rates, with minimal potential toxicity:
A balance must be achieved between the lowest • level of least hazardous CPA and maximal cooling rate. Adequate dehydration and permeation of cells • is essential, and therefore exposure time is important. In order to avoid the formation of both • intracellular and extracellular ice, the initial cooling rate must exceed the critical cooling rate (CCR) of the solution; in human ART, experimental evidence suggests that the cooling rate should be >20 000°C/min, and preferably >50 000°C/min.
Th e cooling rate is aff ected by several parameters, and diff erent methods have been employed in order to fi nd an eff ective and practical solution, by vary-ing CP solutions, combinations, exposure times, and temperature. Th e addition of sugars (sucrose, trehal-ose, fructose, sorbitol saccharose, raffi nose) reduces the concentration of CP required; the permeability of mixtures is higher than that of individual components, and diff erent combinations of CP have also been tried. Vitrifi cation solutions are developed with the lowest possible concentration of CP compatible with achiev-ing glass formation. Reducing volume to a minimum reduces potential toxicity and osmotic damage, and methods have been devised to reduce the volume of CP down to between 0.1 µL and 2 µL. Reducing the drop size, or increasing the number of embryos per drop risks diluting the CP with medium carried over from the culture drop, and this could allow the sample to freeze, with lethal results Two diff erent types of carrier have been used: 1. “Open” systems: the sample comes into direct
contact with liquid nitrogen, and a cooling rate of 23 000°C/min can be achieved.
Electron microscope grid Open pulled straw Cryoloop Cryoleaf™ (McGill)
2. “Closed” systems: the carrier, but not the sample itself, is in direct contact with liquid nitrogen; the cooling rate is slower, around 12 000°C/min.
Cryotip

Chapter 12: Cryopreservation of gametes and embryos
197
CryoLock Cryo BioSystem HSV straw
Th e thawing rate must also be rapid, in order to pre-vent devitrifi cation and ice crystal formation during the transition state. Th e samples are kept in air (room temperature) for 1–3 seconds; for open systems, the sample is then immersed in dilution medium at 37°C, and for closed systems, the carrier is immersed in a 37°C water bath before transferring the sample to the dilution medium. Th e CP is diluted in several steps, in order to counterbalance osmotic eff ects as the CP leaves the cell.
Comparison of slow freezing vs. vitrifi cation
Slow freezing
Low concentrations of permeating + non-permeat-• ing cryoprotectants (1.5/0.1–0.3), PROH or DMSO/sucrose. Requires controlled-rate freezing machine, 2°C/min, • then 0.3°C/min. Nucleation (seeding) and transfer to liquid nitrogen • is critical. Well-established protocols and techniques. •
Vitrifi cation
Avoids formation of ice that can damage • membranes. Rapid method, simple equipment. • No specialized controlled rate freezer required. • Application into clinical practice has been slow, due • to concerns about toxicity of high CP concentrations (up to 6 M). Use of very low volumes reduces toxicity risk. • Requires critical process control: zero tolerance to • any changes/fl uctuations. Samples must be handled and moved very rapidly. • Avoid accidental warming: stored samples are very • fragile, and could be susceptible to mini-devitrifi ca-tion cycles during routine dewar use in a busy IVF laboratory. “Open” systems: direct contact with liquid nitrogen. •
Numerous reports have now been published that confi rm successful use of vitrifi cation in human ART cryostorage, and several authors recommend vitrifi -cation instead of slow freezing for oocytes and blasto-cyst stage embryos in particular. However, questions remain about the long-term stability of the “glassy state” of the vitrifi ed cells, which are prone to fracture; this may be a hazard under normal working conditions in the IVF laboratory with routine access to storage tanks.
Questions have also been raised about the safety of “open” vitrifi cation, in the perspective of the discussion below .
Storage of cryopreserved samples During the early 1990s the transmission of hepatitis B virus between frozen bone marrow samples in a liquid nitrogen storage tank was demonstrated. Th is incident raised the possibility of pathogen transmis-sion between samples in ART laboratories, and led to further consideration of potential sources of con-tamination and means of avoiding the transmission of infection.
Potential sources of contamination include: 1. Within the freezing apparatus . Vapor phase
controlled rate freezers spray nonsterile liquid nitrogen directly onto the samples. Th is may be further compounded by liquid condensation that may accumulate within ducting between freezing runs. Ideally, a freezing apparatus should have the capability of being sterilized between freezing runs, but this is not a practical option .
2. During storage . Straws may be contaminated on the outside, or seals and plugs may leak. Particulates may then transfer via the liquid nitrogen within the storage vessel .
3. From liquid nitrogen . Generally, liquid nitrogen has a very low microbial count when it is manufactured. However, contamination may occur during storage and distribution. Any part of the distribution chain that periodically warms up, in particular transfer dewars or dry shippers, may become heavily contaminated. Th e microbial quality of the liquid nitrogen when delivered from the manufacturer varies widely with geographical region and more extreme reports of microbial contamination may refl ect local industrial practices.
Th e HFEA in the UK prepared a consultation document with guidelines for safe storage of human gametes in liquid nitrogen (HFEA, 1998); basic recom-mendations include patient screening for hepatitis B, hepatitis C and HIV, careful hygiene throughout, dou-ble containment of storage straws and the use of sealed ampules. Th e risks of cross-contamination during the quarantine period need to be assessed and procedures put in place to minimize these risks. However, the litera-ture now available on animal models and human IVF has been reviewed by Pomeroy et al . ( 2009 ), and this
Slow freezing
Low concentrations of permeating + non-permeat-•ing cryoprotectants (1.5/0.1–0.3), PROH or DMSO/sucrose. Requires controlled-rate freezing machine, 2°C/min, •then 0.3°C/min. Nucleation (seeding) and transfer to liquid nitrogen •is critical. Well-established protocols and techniques. •
Vitrifi cation
Avoids formation of ice that can damage •membranes. Rapid method, simple equipment. • No specialized controlled rate freezer required.• Application into clinical practice has been slow, due •to concerns about toxicity of high CP concentrations (up to 6 M). Use of very low volumes reduces toxicity risk.• Requires critical process control: zero tolerance to •any changes/fl uctuations. Samples must be handled and moved very rapidly.• Avoid accidental warming: stored samples are very •fragile, and could be susceptible to mini-devitrifi ca-tion cycles during routine dewar use in a busy IVF laboratory. “Open” systems: direct contact with liquid nitrogen. •

Chapter 12: Cryopreservation of gametes and embryos
198
review suggests that in practice, the risk of cross-con-tamination in IVF working conditions is negligible.
Embryo cryopreservation Following fresh embryo transfer in a stimulated IVF cycle, supernumerary embryos are available for cryo-preservation in a large number of cycles. In a routine IVF practice, more than half of stimulated IVF cycles may yield surplus embryos suitable for cryopreserva-tion (although this is now subject to legislative control in particular countries of the world). In addition to enhan-cing the clinical benefi ts and cumulative conception rate possible for a couple following a single cycle of ovarian stimulation and IVF, a successful cryopreservation pro-gram off ers other benefi ts including the possibility of avoiding fresh embryo transfer in stimulated cycles with a potential for ovarian hyperstimulation syndrome, or in which factors that may jeopardize implantation are apparent (e.g., bleeding, unfavorable endometrium, polyps or an extremely diffi cult embryo transfer) .
Consent to storage after cryopreservation
A unit that off ers embryo cryopreservation must also be aware of logistic, legal, moral and ethical problems that can arise, and ensure that all patients are fully informed and counseled. Both partners must sign comprehensive consent forms indicating how long the embryos are to be stored, and defi ne legal own-ership in case of divorce or separation, death of one of the partners, or loss of contact between the Unit and the couple. Cryopreserved samples cannot in practice be maintained in storage indefi nitely, and there must be a clear clinic policy to ensure that records are cor-rectly maintained, with regular audits of the storage banks. Clinic administration may mandate that all cou-ples with cryopreserved embryos in storage must be contacted annually, and asked to return a signed form indicating whether they wish to continue storage. In the UK, options for couples include:
1. Continue storage. 2. Return for frozen embryo transfer. 3. Donate their embryos for research projects
approved by appropriate ethics committees/Internal Review Boards and the HFEA.
4. Donate their frozen embryos for transfer to another infertile couple.
5. Have the embryos thawed and disposed of .
Selection of embryos for freezing Using PROH as cryoprotectant, embryos can be fro-zen at either the pronucleate or early cleavage stages.
Careful selection of viable embryos will optimize their potential for surviving freeze-thawing.
Pronucleate Th e cell should have an intact zona pellucida , and healthy cytoplasm with two distinct pronuclei clearly visible. Accurate timing of zygote freezing is essential to avoid periods of the cell cycle that are highly sensitive to cooling. For example, during the period when pronuclei start to migrate before syngamy, with DNA synthesis and formation of the mitotic spindle, the microtubular system is highly vulnerable to temperature fl uctuation, leading to possible scattering of the chromosomes. Zygotes processed for freezing at this stage will no longer survive cryopreservation. Th e timing of pronu-cleate freezing is crucial, and the process must be initi-ated while the pronuclei are still distinctly apparent, no later than 20–22 hours aft er insemination.
Cleavage Two- to eight-cell embryos should be of good quality, grade 1 or 2, with less than 20% cytoplasmic fragments. Uneven blastomeres and a high degree of fragmen-tation jeopardize survival potential; embryos with damage aft er thawing may still be viable and result in pregnancies, but their prognosis for implantation is reduced.
Embryo cryopreservation: method Details of each patient and the associated embryos must be carefully recorded on appropriate data sheets. Meticulous and complete record keeping is crucial, and must include the patient’s date of birth, medical number, date of oocyte retrieval (OCR), date of cryopreservation, number and type of embryos frozen, number of straws or ampules used, together with clear and accurate identifi cation of storage ves-sel and location within the storage vessel. Th e data sheets should also confi rm that both partners have signed consent forms. Both ampules and straws have been successfully used for embryo storage, and each has advantages and disadvantages. Th e choice between them is a matter of individual preference, as well as availability of storage space and laboratory time to prepare and sterilize ampules. When straws are used, they must be handled with care to avoid external contamination, and to avoid inadvertent temperature fl uctuations during seeding or trans-fer to the storage dewar. Th e measured temperature excursions within straws can be very dramatic (see
A unit that off ers embryo cryopreservation must alsobe aware of logistic, legal, moral and ethical problemsthat can arise, and ensure that all patients are fully informed and counseled. Both partners must signcomprehensive consent forms indicating how longthe embryos are to be stored, and defi ne legal own-ership in case of divorce or separation, death of one of the partners, or loss of contact between the Unit andthe couple. Cryopreserved samples cannot in practicebe maintained in storage indefi nitely, and there mustbe a clear clinic policy to ensure that records are cor-rectly maintained, with regular audits of the storagebanks. Clinic administration may mandate that all cou-ples with cryopreserved embryos in storage must becontacted annually, and asked to return a signed formindicating whether they wish to continue storage. Inthe UK, options for couples include:
1. Continue storage. 2. Return for frozen embryo transfer. 3. Donate their embryos for research projects
approved by appropriate ethics committees/Internal Review Boards and the HFEA.
4. Donate their frozen embryos for transfer to anotherinfertile couple.
5. Have the embryos thawed and disposed of .

Chapter 12: Cryopreservation of gametes and embryos
199
Figure 12.6 ). It is likely that in straws frozen horizon-tally the embryos will be adjacent to the wall, where they will be exposed to the highest thermal gradient; great care must be taken in handling cryopreserved material. Plastic cryovials are not recommended for embryo freezing .
Ready-to-use media for freezing and thawing embryos are available from the majority of compan-ies who supply culture media. Individual methods and protocols vary slightly with the diff erent preparations, and manufacturers’ instructions should be followed for each.
Care must be taken to ensure that no air bubbles • are trapped within the freezing medium aft er the sample has been loaded, into either ampules or straws. Air bubbles can sometimes be seen in both vessels on thawing, and these present a hazard to the fragile dehydrated embryo. Warming solutions
to 37°C before starting the procedure may eff ectively act as a “degassing” mechanism. It is common practice to cool human embryos • within the controlled rate freezing apparatus down to below –100°C aft er the slow cooling to –30°C, before transfer to liquid nitrogen. In veterinary IVF cryopreservation, straws are oft en transferred to liquid nitrogen directly from –30°C. Th is procedure would give equally good results for human embryos and is indeed used by some laboratories with no reduction in viability. However, it is essential that the transfer is carried out rapidly (within 5 seconds) because the temperature of the straws may rise very rapidly when they are removed from the controlled rate device (see Figure 12.6 ). Cooling to temperatures below –100°C within the freezing machine carries less risk, but does consume considerably more liquid nitrogen .
Figure 12.6 Measured temperatures within straws following removal from a controlled rate freezer or from a liquid nitrogen vessel at various points during the freezing cycle. Prior to nucleation the temperature rise within 5 seconds is suffi cient to prevent ice nucleation. At –30°C the sample temperature may rise very quickly and if transfer to liquid nitrogen is carried out at this point of the freezing program, care must be taken to ensure that the increase in temperature is minimized. Following liquid nitrogen immersion the temperature of straws may rise by 130°C within 20 seconds.

Chapter 12: Cryopreservation of gametes and embryos
200
Sample protocols
Sample protocol for embryo slow freezing
1. Equilibrate selected and washed embryos in 1,2-propanediol (1.5 M) at room temperature, to allow uptake of the CP into the cells. This is usually done in two steps, the second step incorporating 0.1 M sucrose.
2. Load equilibrated embryos into straws or ampules. 3. Cool the samples at a rate of 2°C/min to –7°C, and
“hold” at this temperature to allow thermal equili-bration before ice nucleation (seeding).
4. Following seeding, with initiation and growth of ice crystals, cool the samples at a slow rate, –0.3°C/min, down to –30°C.
5. Cool the samples rapidly to liquid nitrogen temper-atures, then plunge and store in liquid nitrogen.
Sample protocol for embryo thawing after slow freezing
1. Samples are thawed in two stages: hold straws in air for 40 seconds, and then transfer to a 30°C water bath for a further minute.
2. Remove cryoprotectant by dilution through solu-tions containing 0.2 M sucrose, and then wash three times in culture medium.
The thawing protocol is carried out at room tem-perature, and the embryos placed in equilibrated cul-ture medium at room temperature before being allowed to warm gradually to 37°C in the incubator. Pronucleate embryos may be cultured overnight to confi rm con-tinued development, and cleavage stage embryos are incubated for a minimum of 1 hour before transfer .
Use of glass ampules
Tissue-culture washed borosilicate glass ampules with a fi ne-drawn neck can be used for embryo cryostorage.
Fill the ampule with approximately 0.4 mL of the • sucrose/PROH solution using a needle and syringe. Carefully transfer the embryos using a fi ne-drawn • Pasteur pipette. Using a high-intensity fl ame, carefully heat-seal the • neck of the ampule. It is important to ensure (under the microscope) that the seal is complete, without leaks: leakage of liquid nitrogen into the ampule during freezing will cause it to explode immedi-ately upon thawing. It is often impossible to detect whether the glass neck is completely sealed, and the possibility of explosion can be avoided by opening the ampule under liquid nitrogen before thawing.
Ice nucleation: practical points 1. Because straws have a large surface area,
small diameter and a thin wall, very rapid warming occurs when they are removed from a cold environment. Measured temperature excursions that occur at diff erent points of the cryopreservation procedure are illustrated in Figure 12.6 . If straws are removed from the controlled rate freezing apparatus for excessive lengths of time during the nucleation procedure, they can warm to a temperature that is too high for ice nucleation to occur . Ice nucleation may occur because of the local cooling induced by the nucleating tool, but it is possible that the bulk temperature of the fl uid may not allow ice crystal growth to propagate through the sample. In some laboratories, it is common practice to check that ice propagation has occurred throughout the sample, usually 1 minute aft er the seeding procedure. If straws are removed from the controlled rate cooling equipment, this in itself may cause melting of the nucleated ice.
2. Th e thermal control of the freezing apparatus may not be suffi ciently accurate or stable at the nucleation temperature. Th e temperature achieved may allow nucleation to occur because of the thermal mass of the nucleating tool, but may not be suffi ciently low to allow subsequent ice propagation. Any thermal fl uctuations within the freezing apparatus may also lead to the melting of ice.
3. Within straws, nucleation of ice at temperatures very close to the melting point results in a very slow propagation of ice through the sample. In some cases, the ice propagation can actually become blocked, and embryos are then eff ectively supercooled. In this case the embryos would not be expected to survive further cooling .
Blastocyst freezing Th e fi rst reports of successful human blastocyst cryo-preservation were published in 1985 (Cohen et al ., 1985 ; Fehilly et al ., 1985 ), but blastocyst freezing became routine in IVF only aft er media for eff ective extended culture became available during the 1990s. Using Vero cell co- culture to enhance extended cul-ture, Ménézo et al . ( 1992 ) explored the use of a com-bination of glycerol and sucrose as cryoprotectants to
Sample protocol for embryo slow freezing
1. Equilibrate selected and washed embryos in 1,2-propanediol (1.5 M) at room temperature, to allowuptake of the CP into the cells. This is usually donein two steps, the second step incorporating 0.1 Msucrose.
2. Load equilibrated embryos into straws or ampules. 3. Cool the samples at a rate of 2°C/min to –7°C, and
“hold” at this temperature to allow thermal equili-bration before ice nucleation (seeding).
4. Following seeding, with initiation and growth of icecrystals, cool the samples at a slow rate, –0.3°C/min,down to –30°C.
5. Cool the samples rapidly to liquid nitrogen temper-atures, then plunge and store in liquid nitrogen.
Sample protocol for embryo thawing after slowfreezing
1. Samples are thawed in two stages: hold straws inair for 40 seconds, and then transfer to a 30°C waterbath for a further minute.
2. Remove cryoprotectant by dilution through solu-tions containing 0.2 M sucrose, and then wash threetimes in culture medium.
The thawing protocol is carried out at room tem-perature, and the embryos placed in equilibrated cul-ture medium at room temperature before being allowedto warm gradually to 37°C in the incubator. Pronucleateembryos may be cultured overnight to confi rm con-tinued development, and cleavage stage embryos areincubated for a minimum of 1 hour before transfer .
Tissue-culture washed borosilicate glass ampuleswith a fi ne-drawn neck can be used for embryocryostorage.
Fill the ampule with approximately 0.4 mL of the•sucrose/PROH solution using a needle and syringe. Carefully transfer the embryos using a fi ne-drawn•Pasteur pipette. Using a high-intensity fl ame, carefully heat-seal the•neck of the ampule. It is important to ensure (underthe microscope) that the seal is complete, withoutleaks: leakage of liquid nitrogen into the ampuleduring freezing will cause it to explode immedi-ately upon thawing. It is often impossible to detectwhether the glass neck is completely sealed, andthe possibility of explosion can be avoided byopening the ampule under liquid nitrogen beforethawing.

Chapter 12: Cryopreservation of gametes and embryos
201
freeze surplus expanded blastocysts, and the protocols were later modifi ed to obtain satisfactory freeze-thaw rates. Inconsistent success rates were reported initially, but this may have been partly due to lack of experience with selection criteria for freezing, and also a need to understand the subtleties of cryopreservation and the impact that even the slightest variation might have on consistency. Extended culture to blastocyst stage is now routine in many IVF laboratories, and the com-panies that supply blastocyst media also off er blasto-cyst cryopreservation media and protocols. Glycerol is the cryoprotectant of choice for slow freezing of blas-tocysts, and extra sucrose dilutions in the thaw have led to a substantial overall improvement.
Using strict criteria to select potentially viable blas-tocysts is crucial to success:
Growth rate: expanded blastocyst stage on Day 5/• Day 6. Overall cell number >60 cells (depending on day • of development). Relative cell allocation to trophectoderm /inner • cell mass. Original quality of early stage embryo : pronucleus • formation and orientation, blastomere regularity, mono-nucleation, fragmentation, appropriate cleavage stage for time of development.
Blastocyst vitrifi cation Although it is currently too early to reach conclu-sions about pregnancy rates, blastocyst vitrifi cation has recently become an increasing trend, with reports of very favorable survival, implantation and clinical pregnancy rates (Hong et al ., 2009 ). Initial trials with human blastocysts were reported by Lane et al . in 1999 , and commercial kits for blastocyst vitrifi cation are available – as always, the ultimate success of the proto-col will be related to the operator’s experience and care-ful attention to detail. In common with all aspects of human ART, careful research into the consequences of such new therapies continues to be essential. In large expanded blastocysts, collapsing the blastocoelic cav-ity with an ICSI needle immediately before processing increases survival rates aft er both slow freezing and vit-rifi cation (Kader et al ., 2009 ).
Assisted hatching and cryopreservation Freeze-thawing is known to cause hardening of the zona pellucida, and the application of assisted hatching ,
particularly at the blastocyst stage, has been suggested as benefi cial to implantation aft er freeze-thawing (Tucker, 1991 ). In some cases, zona fracture can be a routine result of some cryopreservation protocols (Van den Abbeel et al ., 2000 ). Embryos with existing holes in the zona following PGD procedures can successfully survive and implant (Magli et al ., 2006 ).
Clinical aspects of frozen embryo transfer Freeze-thawed embryos must be transferred to a uterus that is optimally receptive for implantation, in a postovulatory secretory phase. Patients with regu-lar ovulatory cycles and an adequate luteal phase may have their embryos transferred in a natural cycle, monitored by ultrasound and blood or urine lutein-izing hormone (LH) levels in order to pinpoint ovu-lation. Older patients or those with irregular cycles may have their embryos transferred in an artifi cial cycle: hormone replacement therapy with exogen-ous steroids is administered aft er creating an arti-fi cial menopause by downregulation with a GnRH agonist .
Transfer in a natural menstrual cycle 1. Patient selection: regular cycles, 28 ± 3 days,
previously assay luteal phase progesterone to confi rm ovulation. An ovulation “kit” such as Clearplan can also be used in a previous cycle to confi rm that the patient has regular ovulatory cycles.
2. Cycle monitoring from Day 10 until ovulation is confi rmed, by ultrasound scan and plasma LH. Ultrasound scan should also confi rm appropriate endometrial development; the cycle should be canceled if the endometrial thickness is <8 mm at the time of the LH surge.
3. Timing of the embryo transfer: Pronucleate embryos: thaw on Day 1 aft er • ovulation (3 days aft er the LH surge: LH + 3), culture overnight Cleavage stage embryos: thaw and transfer on • Day 2 or 3 aft er ovulation (LH + 4/5) Blastocysts : thaw and transfer on Day 4 or 5 • aft er ovulation (LH + 6/7).
Patients with irregular cycles may be induced to ovu-late using clomifene citrate or gonadotropins, and

Chapter 12: Cryopreservation of gametes and embryos
202
embryo transfer timed in relation to the endogen-ous LH surge or following administration of human chorionic gonadotropin (hCG). Although it is pos-sible to estimate embryo transfer time using an ovu-lation “kit” to detect the LH surge, this is far less accurate, and does present a risk of inappropriate timing.
Schedule for frozen embryo transfer in a hormone replacement cycle
1. Patient selection: oligomenorrhea/irregular cycles, or age >38 years.
2. Downregulate with GnRH analogue (buserelin or nafarelin) for at least 14 days; continue downregu-lation until the time of embryo transfer.
3. Administer estradiol valerate :
4. Progesterone from Day 15–16, choice between: Gestone 50 mg intramuscular or • Cyclogest pessaries 200 mg twice daily or • Utrogestan pessaries 100 mg three times daily or • 8% Crinone gel per vaginam, once daily. • Double the dose from Day 17 onwards (100 mg Gestone , 400 mg twice daily Cyclogest, 200 mg three times daily Utrogestan, 8% Crinone gel PV, twice daily).
5. Embryo transfer (a) Pronucleate: thaw on Day 16 of the artifi cial
cycle, culture overnight before transfer on Day 17 or 18.
(b) Cleavage stage embryos: thaw and replace on Day 17 or 18.
(c) Blastocysts: thaw and replace Day 19 or 20. 6. If pregnancy is established, continue hormone
replacement (HRT) therapy with 8 mg estradiol valerate and the higher dose of progesterone sup-plement daily until Day 77 after embryo transfer. Gradually withdraw the drugs with monitoring of blood P4 (progesterone) levels.
This protocol is also successfully used for the treat-ment of agonadal women who require ovum or embryo donation. In combination with prior gonadotropin releasing hormone (GnRH) pituitary suppression, the artifi cial cycle can be timed to a prescheduled program according to the patient’s (or clinic’s) convenience.
Semen cryopreservation Cryopreserved semen has long been used successfully for artifi cial insemination (AI), intrauterine insem-ination (IUI) and IVF. Although freeze-thawing does produce damage to the cells with loss of up to 50% of pre-freeze motility, since large numbers of cells are available, successful fertilization can be achieved even with low cryosurvival rates. Th ere is, however, a notice-able diff erence in sperm cryosurvival rates between normal semen and semen with abnormal parameters such as low count and motility; samples from men who require sperm cryopreservation prior to chemotherapy treatment for malignant disease frequently show very poor cryosurvival rates. Th e routine introduction of ICSI into IVF practice has surmounted this problem, so that successful fertilization using ICSI is possible even with extremely poor cryosurvival of suboptimal samples .
Eff ects of cryropreservation on sperm Sperm membranes have an unusual lipid compos-ition, with relative proportions of phospholipids, glycolipids and sterols that diff er from those of other cell membranes. Reduction in temperature alters the membrane lipid organization and modifi es the kin-etics or intra-membrane proteins, leading to lowered permeability and loss of fl uidity. Th is loss of fl uidity is associated with lower sperm survival on thawing. Figure 12.7 illustrates the ultrastructure of human sperm following freezing with 10% glycerol as cryo-protectant. Frozen/thawed sperm behave in a similar way to capacitated sperm, which may lead to a short-ened lifespan within the female tract; therefore the timing of insemination is important when using fro-zen sperm samples.
Semen can be successfully cryopreserved using either glycerol alone at a concentration of 10–15%, or a complex cryoprotective medium such as Human Sperm Preservation Medium (HPSM, Sperm Freeze™, FertiPro, Belgium) or Test Yolk Buff er (TYB medium, Irvine Scientifi c, Santa Ana, CA), Quinn’s Sperm Freeze Medium (SAGE), Sperm Freezing Medium (Medicult). Adding the cryoprotectant gradually, dropwise, helps to minimize potential damage due to volume changes within the cell. Cooling and freezing can be carried out by using a programmed cell freezer, or by simply suspending the prepared specimens in liquid nitrogen vapor for a period of 30 minutes .
1. Patient selection: oligomenorrhea/irregular cycles,or age >38 years.
2. Downregulate with GnRH analogue (buserelin ornafarelin) for at least 14 days; continue downregu-lation until the time of embryo transfer.
3. Administer estradiol valerate :
4. Progesterone from Day 15–16, choice between: Gestone 50 mg intramuscular or• Cyclogest pessaries 200 mg twice daily or• Utrogestan pessaries 100 mg three times daily or •8% Crinone gel per vaginam, once daily.•Double the dose from Day 17 onwards (100 mgGestone , 400 mg twice daily Cyclogest, 200 mgthree times daily Utrogestan, 8% Crinone gel PV,twice daily).
5. Embryo transfer (a) Pronucleate: thaw on Day 16 of the artifi cial
cycle, culture overnight before transfer on Day17 or 18.
(b) Cleavage stage embryos: thaw and replace onDay 17 or 18.
(c) Blastocysts: thaw and replace Day 19 or 20. 6. If pregnancy is established, continue hormone
replacement (HRT) therapy with 8 mg estradiolvalerate and the higher dose of progesterone sup-plement daily until Day 77 after embryo transfer.Gradually withdraw the drugs with monitoring of blood P4 (progesterone) levels.
This protocol is also successfully used for the treat-ment of agonadal women who require ovumor embryo donation. In combination with priorgonadotropin releasing hormone (GnRH) pituitarysuppression, the artifi cial cycle can be timed to aprescheduled program according to the patient’s(or clinic’s) convenience.
Days 1–5 2 mgDays 6–9 4 mgDays 10–13 6 mgDays 14 onwards 4 mg

Chapter 12: Cryopreservation of gametes and embryos
203
(a)
(b)
Figure 12.7 Ultrastructure of human sperm following freezing in a 0.25 mL straw; cells were suspended in glycerol (10%). (a) Freeze fracture followed by etching reveals the structure of ice crystals, cells are entrapped within the freeze concentrated material and few cell structures are evident. (b) Freeze substitution followed by sectioning shows cells entrapped within the freeze concentrated matrix.
Method Samples should be prepared and frozen within 1–2 hours of ejaculation . 1. Allow the sample to liquefy, and perform semen
analysis according to standard laboratory technique; label two plastic conical tubes and an appropriate number of 0.5 mL freezing straws or ampules for each specimen. Record all details on appropriate record sheets.
2. Add small aliquots of cryoprotectant medium (CPM) to the semen at room temperature over
a period of 2 minutes, to a ratio of 1:1. If the ejaculated volume is greater than 5 mL, divide the sample into two aliquots before mixing with CPM.
3. Aliquot the diluted sample into straws or ampules, labeling aliquots for assessment of post-thaw count and motility.
4. Dilute specimens with CPM according to count.
60 million/mL dilute 1:1 semen:CPM
20–60 million/mL dilute 2:1 semen:CPM
20 million/mL dilute 4:1 semen:CPM

Chapter 12: Cryopreservation of gametes and embryos
204
5. Reassess the number of motile sperm/mL, which should ideally be 10 million or above.
6. Aliquot into prelabeled straws.
Manual freezing 1. Place the ampules or straws (in goblets) on a metal
cane. 2. Refrigerate at 4°C for 15 minutes. 3. Place into liquid nitrogen vapor for 25 minutes . 4. Plunge into liquid nitrogen for storage, and record
storage details.
Th e sample must be carefully washed or prepared by density gradient centrifugation to remove all traces of cryoprotectant medium before it is used for insemin-ation by intrauterine insemination (IUI) or IVF.
Methods to improve sperm survival Sperm survival and pregnancy rates are lower when the frozen samples used are from infertile men compared with samples from fertile donors, and there is evidence to suggest that sperm preparation in order to remove immotile and damaged sperm prior to freezing may help to select a population of sperm with a better chance of survival. Th e use of stimulants such as pentoxifylline may also improve survival aft er thawing (see Chapter 10 ).
Cryopreservation of testicular and epididymal sperm Whereas the relatively poor survival rates (50%) obtained aft er freeze-thawing semen samples have not in the past presented a major problem due to the abundance of cells in the original specimens, it is not always possible to obtain an ejaculated semen sam-ple; the current use of suboptimal ejaculate, epididy-mal and testicular samples in combination with ICSI demands a diff erent approach in order to recover as many sperm cells as possible from each sample. Sample cryopreservation in cases of epididymal and testicular aspiration or biopsy has considerable advantages both to the patient and to the clinical and laboratory staff , in that sperm and oocyte retrieval procedures may be carried out on separate occasions; this strategy is now a successful routine in the majority of ART programs off ering this form of treatment. Generally epididymal and testicular samples are cryopreserved using proto-cols developed for ejaculated sperm: this may not be
optimal. Many changes to the membranes of sperm occur during maturation, and it is likely that the water permeability of testicular sperm, a major factor in determining the cellular response to freezing, is very diff erent from that of ejaculated sperm.
In cases where prolonged washing and searching yield only very few sperm, sperm can be frozen indi-vidually or in small groups by injecting them into empty zona pellucida “shells,” using a crude freez-ing solution with 8% glycerol in phosphate-buff ered saline supplemented with 3% human serum albumin. Samples are recovered aft er washing the zonae through droplets, and more than 70% of sperm survive using this procedure with resulting successful pregnancy rates (Walmsley et al ., 1999 ).
Th e criteria for sperm freezing have now changed, in that even the most inadequate samples can be fro-zen/thawed for successful ICSI. It is no longer neces-sary to do testicular sperm aspiration/percutaneous epididymal sperm aspiration on the same day as the oocyte retrieval – numerous groups report success with frozen/thawed testicular and epididymal samples. All biopsy samples can be successfully frozen. Th e use of cryopreservation buff ers without egg yolk is recom-mended for testicular and epididymal samples.
Testicular biopsy samples Freezing whole biopsy samples without prior pro-cessing is not recommended, as cryoprotectant solu-tion will not equilibrate evenly throughout the tissue. Pieces of macerated or minced tissue can, however, be frozen with some success. It has also been reported that a higher proportion of testicular sperm retain their motility on thawing if they have been incubated 24–48 hours before freezing, and Van den Berg ( 1998 ) sug-gests that incubation at 32°C may be benefi cial. If there is doubt about sperm viability aft er thawing, a simple hypo-osmotic swelling test will identify viable sperm before injection.
Cryopreservation of semen for cancer patients Patients who are to be treated with combined chemo-therapy for various types of cancer, such as Hodgkin’s disease and testicular tumors, are frequently young or even adolescent. Recent progress in oncology has given these patients a greatly improved prognosis for

Chapter 12: Cryopreservation of gametes and embryos
205
successful recovery, and cryopreservation of sperm-atozoa before initiating treatment can preserve fertility for the majority of patients.
All cancer treatment regimens are toxic to sperm-atogenesis , and the majority of patients will be azoo-spermic aft er 7–8 weeks of treatment. In some cases spermatogenesis is restored aft er some years, but in others there is minimal recovery even aft er a decade. Animal studies have indicated that spermatogenesis may be protected from the adverse eff ects of chemo-therapy by inhibiting pituitary control of sperm-atogenesis with GnRH agonists , androgens or male contraceptive regimens. Similar protective regimens in humans are currently ineff ective, and the strategy remains experimental.
Currently, there are no pretreatment parameters that can predict a patient’s prognosis for recovery of fer-tility; the possibility of erectile dysfunction aft er treat-ment should also be borne in mind. Patients should be given general advice about the need for contraception when recovery is unpredictable, and advised to seek medical help early if fertility is required. Informed consent forms should be signed aft er discussion and counseling. Ideally, three sperm samples are collected before chemotherapy is initiated; animal studies sug-gest that chemotherapy may have a mutagenic eff ect on late-stage germinal cells, but in the absence of a known clinical signifi cance in humans, sample col-lection aft er the start of treatment is preferable to no storage at all. Patients should be informed of the poten-tial risks and receive appropriate counseling in such cases. Spermatogenesis is oft en already impaired due to the eff ects of the disease: many demonstrate hypo-thalamic dysfunction, and in severe cases pituitary gonadotropin secretion is altered. Th e tremendous stress caused by cancer reduces fertility potential by the action of stress hormones in the brain, leading to altered catecholamine secretion, rise in prolactin and corticotropin-releasing factor, which in turn suppress the release of GnRH. However, in the light of ICSI treat-ment success rates, semen samples should be frozen regardless of their quality. Prior to sample collection for storage, patients should be screened for hepatitis B and C and HIV.
Patients are naturally concerned that their cancer treatment might cause an increased risk of congenital malformation in a subsequent pregnancy: the results of studies to date are reassuring, although insuffi cient data have been accumulated for each cancer or treat-ment regimen. Th ere are now several published reports
of successful treatment for couples using sperm stored prior to treatment; type of treatment depends upon the quality of the sample, but pregnancies and live births are reported aft er AI, IUI, IVF and ICSI.
In the future, autotransplantation of cryopreserved testicular tissue may become an alternative option for young men who are not yet producing sperm, or who are unable to produce an ejaculate. Research has shown that gonocytes from immature mice injected into the tubules of sterilized hosts restore spermatogenesis and produce fertile spermatozoa – hopefully, this strat-egy may one day provide another option for cancer patients, especially for children.
Oocyte cryopreservation Prior to 1997, the options for preserving a young woman’s fertility aft er treatment for malignant disease were very limited: a full IVF treatment cycle with cryopreserva-tion of embryos prior to the initiation of chemo therapy, or oocyte or embryo donation following recovery from the malignant disease. Th e fi rst option is available only to women with partners to provide a semen sample for fertilization of the harvested oocytes. However, the suc-cess of frozen embryo cryopreservation in a competent IVF program is such that these patients maintain a very good chance of achieving a pregnancy aft er transfer of frozen-thawed embryos following recovery from their disease. On the other hand, this strategy also raises the risk of creating embryos with a higher than aver-age chance of being orphaned. Many of the legal and ethical problems created by the cryopreservation and storage of embryos might be overcome by preserving oocytes, especially for young women about to undergo treatment for malignant disease that will result in loss of ovarian function. Oocyte cryopreservation may also be indicated in patients with a known family history of premature ovarian failure, and may be advantageous in various clinical scenarios, such as in ovarian hyper-stimulation syndrome, unexpected lack of sperm fol-lowing oocyte retrieval, egg donation programs and in order to extend the duration of natural fertility .
Human oocytes are particularly susceptible to freeze-thaw damage due to their size and complexity. Th ey must not only survive thawing, but also preserve their potential for fertilization and development. Th e fi rst pregnancies with human oocyte freezing were reported in the 1980s (Chen, 1986 ; Al Hasani et al ., 1987 ), but the procedure was abandoned for approximately 10 years due to low survival and fertilization rates, thought to be

Chapter 12: Cryopreservation of gametes and embryos
206
due primarily to hardening of the zona pellucida and to spindle damage causing aneuploidy. Since 1997, focus has intensifi ed on modifying protocols to increase sur-vival rates, in particular to avoid activation/premature release of cortical granules, zona hardening and the detection/avoidance of spindle damage and aneuploidy. In 2009, Noyes et al . reported the birth of more than 900 babies aft er oocyte cryopreservation, with no apparent increased incidence of congenital anomalies. Attempts to monitor alterations in the permeability of the plasma membrane, assess warming and rehydration protocols and use ICSI to improve fertilization rates have resulted in signifi cant clinical progress.
Several intrinsic diffi culties are associated with human oocyte freezing, due mainly to their high volume:surface area ratio and low membrane per-meability. Intracellular ice formation causes critical damage to the cytoskeleton, which is also sensitive to osmotic stress. Disruption of the meiotic spindle can cause chromosome defects and aneuploidy. Lowering the temperature, or the cryoprotectant agents them-selves may cause an increase in intracellular Ca 2+ leading to changes in the intracellular signaling mech-anisms and oocyte activation . Finally, since the zona hardens aft er freezing it is necessary to employ ICSI for fertilization of the thawed oocyte.
Freezing can result in parthenogenetic activation, leading to premature release of cortical granules (CGs). It is also important to consider the cytoplasmic matur-ity of the oocyte at freezing and the potentially toxic eff ects of cryoprotectants .
Several modifi cations have been made in order to improve the eff ectiveness of oocyte freezing: 1. Complete removal of the cumulus and coronal
mass increases survival rates. 2. Altering sucrose concentrations from 0.1 to 0.2,
0.3 or 0.5 mol/L increases oocyte dehydration and survival .
3. Choline has been used as a substitute for sodium (Stachecki et al ., 2006 ; Boldt et al ., 2006 ) on the basis that cryodamage to the Na + /K + pump might lead to high intracellular concentrations of Na + with a resulting effl ux of protons. Choline does not cross the plasma membrane, is less toxic than high sucrose and does not aff ect osmotic pressure of the cell.
Not surprisingly, damage caused by oocyte freezing appears to be protocol-dependent (Rienzi et al ., 2004 ). Using a Polscope to observe the meiotic spindle following
freeze-thaw procedures, these authors observed that the spindle disintegrates during freeze-thawing, and oocytes must reconstruct their spindles aft er thawing. Other authors using confocal or electron microscopy have shown that elevated sucrose concentrations may prevent spindle damage (Cottichio et al ., 2006; Nottola et al ., 2008 ). Th e timing of freezing aft er oocyte retrieval also seems to be important, with lower pregnancy rates reported from oocytes that were frozen more than 2 hours aft er OCR (Parmegiani et al ., 2009 ). Germinal vesicle stage oocytes show better survival (Sereni et al ., 2000 ), probably because these immature oocytes lack a spindle apparatus; however, the oocytes need to be matured in vitro post thaw, and this currently has lim-ited success.
Th e thawing process is equally fraught with diffi -culties. Osmotic stress caused by rehydration must be minimized in order to prevent degeneration, and reassembly of the spindle post-thaw takes at least 3–4 hours.
Vitrifi cation of human oocytes has many poten-tial advantages over slow freezing. Th e fi rst live birth was reported by Kuleshova et al . in 1999 , and numer-ous studies with favorable results were published between 2005 and 2009. Th e main concerns with vitrifi cation are the toxicity of high concentrations of cryoprotectant, and extreme osmotic changes. Huang et al . ( 2007 ) showed less damage to the spin-dle and chromosomes after vitrification compared to slow freezing. Cobo et al . ( 2008 ) compared sib-ling fresh oocytes with vitrifi ed donor oocytes using the Cryotop method , reporting very high survival rates aft er warming (97%), and fertilization, blasto-cyst development and pregnancy rates for recipients that were equivalent to those obtained with the use of fresh donor oocytes.
Unfortunately, the published data on the subject of oocyte preservation are not homogeneous and are thus diffi cult to analyze. Diff erent studies used sources of oocytes from diff erent populations (pre-chemotherapy, egg donation, IVF), and there is also immense variability in protocols and procedures. In addition, results are reported in diff erent ways, refer-ring to success ranging from live birth per oocyte to simple freeze-thaw survival per oocyte. However, oocyte preservation is an emerging technology with encouraging results: to date, more than a thousand births have been reported aft er transfer of embryos generated from both slow-freeze and vitrifi ed oocytes. Follow-up will continue to be important, and patients

Chapter 12: Cryopreservation of gametes and embryos
207
should be off ered realistic information and appropri-ate counseling until further research improves the outcome and confi rms the safety of both slow freezing and vitrifi cation techniques.
Ovarian tissue cryopreservation Cryopreservation and banking of ovarian tissue is another attractive strategy for fertility conservation, indicated primarily for young women who will suff er anticipated loss of ovarian function due to premature ovarian failure , cancer or other diseases. Since follicle number diminishes with age, this option is open only to patients who are less than 30 years old and have had no previous chemo- or radiotherapy. Th e uterus must be functional and the patient should have a high prob-ability of long-term survival aft er treatment. Th e type of malignancy is also important, as any risk of ovarian metastasis must be avoided. As discussed in the pre-vious section, cryopreservation of mature metaphase II oocytes is also an option for women wishing to pre-serve their fertility. However, there are several poten-tial advantages of freezing ovarian tissue rather than oocytes: 1. Small pieces of tissue contain very large numbers
of primordial follicles and can be stored for children as well as for young adults.
2. Laparoscopic ovarian biopsy/oophorectomy can be carried out rapidly before chemotherapy, any time during the menstrual cycle, thereby avoiding delays in initiating therapy.
3. Germline cells are removed from cytotoxic harm and the entire tissue can be returned to the patient by graft ing.
4. Storing cortical tissue theoretically preserves natural cell–cell interactions and intra-ovarian signals, and graft ing can potentially restore both steroidogenic and gametogenic function – both important factors for the quality of life of the patient.
Th ere are several options for freezing ovarian tissues ( Figure 12.8 ), which depend on permeability proper-ties, optimal cooling rates, susceptibility to cryo-injury and potential options aft er thawing .
Fragments or thin slices of ovarian cortex Although storage of slices of ovarian cortex is an attractive alternative to mature oocyte freezing, there are a number of technical problems associated with the cryopreservation of ovarian tissues compared to isolated oocytes. Tissues respond very diff erently to ice formation than do cell suspensions. Cells in tissues are usually closely packed, and they also have inter-acting connections with each other and with base-ment membranes. Tissues have a three-dimensional structure and are traversed by fi ne capillaries or other blood vessels. Changes in extracellular ice surround-ing the tissue during the freezing process, and re-crystallization during warming of the tissue are both hazardous. In the hands of experienced cryobiologists morphological assessments of cryopreserved human ovarian cortex at the light microscope (Gook et al ., 1999 ) and electron microscope (Picton et al ., 2000 ; Kim et al ., 2001 ) have confi rmed that cellular damage in the tissue can be minimal. However, the choice of an inappropriate CPA together with poor laboratory practice can lead to extensive cellular damage which
Figure 12.8 Options for ovarian tissue preservation.

Chapter 12: Cryopreservation of gametes and embryos
208
will compromise tissue viability on thawing (Picton et al ., 2000 ). Th e problems of achieving adequate per-meation of tissue fragments with CPA can be over-come either by preparation of thin strips of tissue <1 mm thick which provides maximal surface area for solute penetration (Newton et al ., 1998 ), or by dis-sociation of the tissue into follicles or isolated cells before freezing (Cox et al ., 1996 ). Most procedures stipulate that ovarian cortex slices are thawed rapidly by being swirled in a water bath at ~20°C or 37°C, and the CPA is progressively diluted from the tissue by repeated rinses with fresh medium .
Hemi-ovaries or whole ovaries Th ere are obvious advantages in conserving the whole ovary, in that the entire primordial popula-tion is retained and the cells and oocytes remain in their natural environment. Th ere is also the potential for restoration of endocrine function and the men-strual cycle, preventing menopausal symptoms and improving quality of life. Th e main challenge with whole ovary preservation is that permeation is diffi -cult and requires perfusion via the ovarian artery or vascular pedicle. Th e tissue is denser, with a complex structure of diff erent cell types, a high cell density, a low surface area/volume ratio and decreased effi -ciency of heat transfer. Vitrifi cation is particularly diffi cult since large amounts of cryoprotectant are required and diff erent parts of the ovary will vitrify at diff erent times. Th e cortex and primordial follicles are sustained by very small capillaries which are eas-ily damaged, and this can lead to ischemic follicle loss and death of cortical tissue. Th e vessels can also frac-ture during warming, and pedicle lacerations can lead to possible thrombosis. Finally, revascularization is a time-consuming surgical procedure .
Dissected intact isolated primordial follicles and denuded primordial oocytes from isolated primordial follicles While it may be possible to store ovarian tissue for young cancer patients, where there is any risk of reintroducing malignant cells in the tissue graft (Shaw and Trounson, 1997 ), a far safer strategy is to culture the follicles to maturity in vitro (Picton et al ., 2000 ). Following fertilization by IVF or ICSI, embryos that are free from contamination could be transferred back to the patient. Freezing isolated primordial follicles has several advantages over freezing metaphase II oocytes, including their availability, size, lack of accessory cells,
nuclear status (prophase I with intact nuclear mem-brane), absence of zona pellucida , CGs and low meta-bolic rate. Th e disadvantage of the technique is that prolonged in-vitro maturation is required, and follicle culture is diffi cult and unreliable – the growth from primordial to antral follicle takes approximately 70–90 days. Human follicle culture is still an emerging tech-nology, but recent data are encouraging, and it may eventually be possible to grow primordial follicles to antral stages aft er cryopreservation (Picton et al ., 2000 ). Nonetheless, a considerable amount of research is still needed to confi rm that this strategy is safe, and that it does not induce epigenetic alterations in the female gametes, a possibility that has already been confi rmed in a murine model system (Eppig et al ., 2009 ).
Techniques for cryopreservation of ovarian tissue Slow freezing of tissue has many intrinsic problems, but experimental slow freezing of human ovarian tissue slices have resulted in high rates of follicle survival aft er thawing (Nugent et al ., 1998 ; Hovatta et al ., 2004 ).
Tissue vitrifi cation involves diffi cult challenges:
Delivery of high intracellular concentrations of • cryoprotectant in order to achieve high levels of dehydration. Contact time with solutions must be controlled so • that rapid cooling and high heat transfer rates can be achieved whilst avoiding toxicity.
Th e outcome of the procedure depends on the sample size, the logistics of cooling and storage, direct contact with the liquid nitrogen and specialized containers. Protocols are either “open” (direct contact with liquid nitrogen) or “closed” (container in contact with liquid nitrogen . “Open” protocols are advantageous for rapid cooling:
Direct cover vitrifi cation (DCV, Chen • et al ., 2006 ) Solid surface vitrifi cation (SSV, Huang • et al ., 2008 ) “Carrier-less” (Li • et al ., 2007 ) – drop tissue into shallow container of liquid nitrogen Copper grids, 42 mm holes (Isachenko • et al ., 2007 ) Cryotissue – metal strip full of holes (Kagawa • et al ., 2008 ).
Since tissue is involved, the danger of contamination using the open methods is much greater than in the case of oocytes.

Chapter 12: Cryopreservation of gametes and embryos
209
Several closed devices off er an alternative: Cryotube, Cryobag, Straw, Crovial, Cryotip, Cryopette and the Ohio-Cryo (Kader et al ., 2008 ).
Success of ovarian tissue preservation Th ere are varying degrees of success with all the above techniques. Intact or denuded follicles survive the thaw, but do not grow well aft er isolation, whereas tissue frag-ments or slices may show signs of injury/necrosis aft er culture. Tissues may be xenotransplanted in a SCID mouse or in chorioallantoic membrane (CAM) in the chick embryo. Alternatively tissue may be orthotopically or heterotopically autotransplanted; orthotopic sites include the pelvic peritoneum, the ovary or the ovarian fossa, and heterotopic sites include the rectus abdominis muscle, the abdominal wall, the breast or the forearm.
In whole ovaries , ultrastructural and apoptotic analyses have been used to assess viability aft er thaw/recovery. To date there has been success with cryo/transplant in rodents, rabbits, sheep and marmo-set monkeys, and successful restoration of fertility in sheep aft er orthotopic transplantation of cortical strips to the ovarian pedicle. Th ese graft s continue to function for up to 2 years. Cryopreservation experi-ments that used whole ovaries led to tissue survival in rats, rabbits, dogs, sheep and humans (Martinez-Madrid et al ., 2004 ). Whole ovary vitrifi cation and tra nsplantation has been successfully performed in infantile rats, mice, rabbits, pigs and sheep.
Current status of ovarian transplantation (2010)
• Short-term restoration of natural fertility is possible. Graft follicle content is infl uenced by patient age and • previous treatment and possibly by graft location . Lipid peroxidation occurs in murine and human • ovarian grafts; vitamin E can signifi cantly reduce lipid peroxidation and increase follicle survival. Gonadotropin environment probably has no eff ect • on graft survival although low gonadotropins may be detrimental. Follicle survival has been demonstrated in ortho-• topic and heterotopic human autografts. Live births after autotransplantation are now being • reported in clinical practice.
Autotransplantation in the human Donnez et al . ( 2004 ) reported the fi rst live birth aft er orthotopic transplantation of human cryopreserved ovarian tissue; they detected live follicles from 16 to 26 weeks aft er graft ing, and some of the graft s still
functioned aft er 3 years. Overall results to date are very encouraging, with 17 pregnancies, and 10 live births reported up to February 2010. A patient who had ovarian cortical tissue cryopreserved prior to treatment for Ewing’s sarcoma in 2004 had six cortical strips transplanted aft er recovery from the disease, and has since delivered two healthy daughters: the fi rst in 2007, and the second in 2008 (Andersen et al ., 2008 ).
Considering the experimental status of this new technique in ART , it is paramount to test and opti-mize freeze-thawing results before off ering a service to patients. Post-thaw tissue integrity, follicle counts and viability stains should be carried out. Th e EU Tissue Banking Directive regulations ask for central-ized specialized cryobanks with rigid quality control to prevent transmission of disease. Clinical, psycho-logical and ethical considerations must be consid-ered since transplantation can only be performed as an experimental procedure and there is a potential risk of re-seeding tumor cells. On a more sober note, consent forms must be adequate and discussed with the patient in the event of death. In conclusion, cryo-preservation of ovarian tissue is in its infancy, but is already successful as a tool for fertility preservation.
Further reading Principles of cryobiology Fogarty NM , Maxwell WM , Eppleston J , Evans G ( 2000 )
Th e viability of transferred sheep embryos aft er long-term cryopreservation . Reproduction, Fertility, and Development 12 : 31 –37.
Fuller BJ ( 2003 ) Gene expression in response to low temperatures in mammalian cells: a review of current ideas . Cryo Letters 24 (2): 95 –102.
Lasalle B , Testart J , Renard JP ( 1985 ) Human embryo features that infl uence the success of cryopreservation with the use of 1,2 propanediol . Fertility and Sterility 44 : 645 –641.
Leibo SP ( 1976 ) Freezing damage of bovine erythrocytes: simulation using glycerol concentration changes at sub-zero temperatures . Cryobiology 13 : 587 –598.
Leibo SP , Oda K ( 1993 ) High survival of mouse zygotes and embryos cooled rapidly or slowly in ethylene glycol plus polyvinylpyrrolidone . Cryo Letters 14 : 133 –144.
Leibo SP , Semple ME , Kroetsch TG ( 1994 ) In vitro fertilization of oocytes by 37-year-old bovine spermatozoa . Th eriogenology 42 : 1257 –1262.
• Short-term restoration of natural fertility is possible. Graft follicle content is infl uenced by patient age and •previous treatment and possibly by graft location . Lipid peroxidation occurs in murine and human •ovarian grafts; vitamin E can signifi cantly reduce lipid peroxidation and increase follicle survival. Gonadotropin environment probably has no eff ect •on graft survival although low gonadotropins may be detrimental. Follicle survival has been demonstrated in ortho-•topic and heterotopic human autografts. Live births after autotransplantation are now being •reported in clinical practice.

Chapter 12: Cryopreservation of gametes and embryos
210
Liebermann J , Nawroth F , Isachenko V , et al . ( 2002 ) Potential importance of vitrifi cation in reproductive medicine . Biology of Reproduction 67 (6): 1671 –1680.
Mazur P ( 1963 ) Kinetics of water loss from cells at subzero temperatures and the likelihood of intracellular freezing . Journal of General Physiology 47 : 347 –369.
Mazur P ( 1970 ) Cryobiology: the freezing of living systems . Science 168 : 93 –94.
Mazur P ( 1984 ) Freezing of living cells: mechanisms and implications . American Journal of Physiology 247 : 125 –142.
McWilliams RB , Gibbons WE , Leibo SP ( 1995 ) Osmotic and physiological responses of mouse and human ova to mono- and disaccharides . Human Reproduction 10 : 1163 –1171.
Morató R , Izquierdo D , Paramio MT , Mogas T ( 2008 ) Cryotops versus open-pulled straws (OPS) as carriers for the cryopreservation of bovine oocytes: eff ects on spindle and chromosome confi guration and embryo development . Cryobiology 57 (2): 137 –141.
Parks JE ( 1997 ) Hypothermia and mammalian gametes. In: Karow A , Critser JK (eds) Reproductive Tissue Banking – Scientifi c Principles . Academic Press , San Diego .
Pegg DE ( 1996 ) Cryopreservation: a perspective. In: Hervé P , Rifl e G , Vuitton D , Dureau G , Bechtel P , Justrabo E (eds.) Organ Transplantation and Tissue Graft ing . John Libbey , London , pp. 375–378.
Pegg DE ( 2002 ) Th e history and principles of cryopreservation . Seminars in Reproductive Medicine 20 (1): 5 –13.
Pegg DE , Karow AM ( 1987 ) Th e Biophysics of Organ Cryopreservation . Plenum , New York .
Smith AU ( 1952 ) Behaviour of fertilized rabbit eggs exposed to glycerol and to low temperatures . Nature 170 : 373 .
Tucker MJ , Liebermann J ( 2007 ) Vitrifi cation in Assisted Reproduction: A User’s Manual and Troubleshooting Guide . Informa Healthcare , New York .
Watson PF , Morris GJ ( 1987 ) Cold shock injury in animal cells. In: Bowler P , Fuller J (eds.) Temperature and Animal Cells . Symposia of the Society for Experimental Biology no. 41, Company of Biologists , Cambridge, UK .
Whittingham DG ( 1977 ) Some factors aff ecting embryo storage in laboratory animals. In: Th e Freezing of Mammalian Embryos, Ciba Foundation Symposium 52 : 97 –108.
Whittingham DG , Leibo SP , Mazur P ( 1972 ) Survival of mouse embryos frozen to –196°C and –269°C . Science 178 : 411 –414.
Storage of cryopreserved samples Bahadur G , Tedder RS ( 1997 ) Safety during sperm banking .
Human Reproduction 12 : 198 –198.
British Andrology Society ( 1993 ) British Andrology Society guidelines for the screening of semen donors for donor insemination . Human Reproduction 8 : 1521 –1523.
Department of Health ( 1997 ) Guidance on the processing, storage and issue of bone marrow and blood stem cells.
Fountain D , Ralston M , Higgins N , et al . ( 1997 ) Liquid nitrogen freezers: potential source of hematopoietic stem cell components . Transfusion 37 : 585 –591.
Hawkins AE , Zuckerman MA , Briggs M , et al . ( 1996 ) Hepatitis B nucleotide sequence analysis – linking an outbreak of acute Hepatitis B to contamination of a cryopreservation tank . Journal of Virological Methods 60 : 81 –88.
Human Fertilisation and Embryology Authority ( 1998 ) Consultation on the safe cryopreservation of gametes and embryos . HFEA , London .
Hunt CJ , Pegg DE ( 1996 ) Improved temperature stability in gas phase nitrogen refrigerators: use of a copper heat shunt . Cryobiology 33 : 544 –551.
McKee TA , Avery S , Majid A , et al . ( 1996 ) Risks for transmission of hepatitis C virus during artifi cial insemination . Fertility and Sterility 66 : 161 –163.
Pomeroy KO , Harris S , Conaghan J , et al . ( 2009 ) Storage of cryopreserved reproductive tissues: evidence that cross-contamination of infectious agents is a negligible risk. Fertility and Sterility doi:10.1016/j.fertnstert.2009.04.031 [Epub ahead of print].
Russell PH , Lyaruu VH , Millar JD , Curry MR , Watson PF ( 1997 ) Th e potential transmission of infectious agents by semen packaging during storage for artifi cial insemination . Animal Reproduction Science 47 : 337 –342.
Tedder RS , Zuckerman AH , Goldstone AH , et al . Hepatitis B transmission from contaminated cryopreservation tank . Lancet 1995 ; 346 : 137 –140.
Tomlinson M , Sakkas D ( 2000 ) Safe and eff ective cryopreservation – should sperm banks and fertility centres move toward storage in nitrogen vapour? Human Reproduction 15 (12): 2460 –2463.
Embryo freezing Ashwood-Smith MJ ( 1986 ) Th e cryopreservation of human
embryos . Human Reproduction 1 : 319 –332. Cohen J , Simons RF , Edwards RG , Fehilly CB , Fishel
SB ( 1985 ) Pregnancies following the frozen storage of expanding human blastocysts . Journal of In Vitro Fertilization and Embryo Transfer 2 : 59 –64.
Cohen J , Devane GW , Elsner CW , et al . ( 1988 ) Cryopreservation of zygotes and early cleaved human embryos . Fertility and Sterility 49 : 2.
Fehilly CB , Cohen J , Simons RF , Fishel SB , Edwards RG ( 1985 ) Cryopreservation of cleaving embryos and expanded blastocysts in the human: a comparative study . Fertility and Sterility 44 : 638 –644.

Chapter 12: Cryopreservation of gametes and embryos
211
Givens C , Markun L , Chenette P , et al . ( 2009 ) Outcomes of natural cycles versus programmed cycles for 1677 frozen-thawed embryo transfers . Reproductive Biomedicine Online 19 (3): 380 –384.
Guerif F , Cadoret V , Poindron J , Lansac J , Royere D ( 2003 ) Overnight incubation improves selection of frozen-thawed blastocysts for transfer: preliminary study using supernumerary embryos . Th eriogenology 60 (8): 1457 –1466.
Hartshorne GM , Wick K , Elder K , Dyson H ( 1990 ) Eff ect of cell number at freezing upon survival and viability of cleaving embryos generated from stimulated IVF cycles . Human Reproduction 5 : 857 –861.
Hartshorne GM , Elder K , Crow J , Dyson H , Edwards RG ( 1991 ) Th e infl uence of in vitro development upon post-thaw survival and implantation of cryopreserved human blastocysts . Human Reproduction 6 : 136 –141.
Jones HW Jr., Veeck LL , Muasher SJ ( 1995 ) Cryopreservation: the problem of evaluation . Human Reproduction 10 : 2136 –2138.
Kader AA , Choi A , Orief Y , Agarwal A ( 2009 ) Factors aff ecting the outcome of human blastocyst vitrifi cation . Reproductive Biology and Endocrinology 7 : 99 .
Lassalle B , Testart J , Renard JP ( 1985 ) Human embryo features that infl uence the success of cryopreservation with the use of 1, 2, propanediol . Fertility and Sterility 44 : 645 –651.
Loutradi KE , Kolibianakis EM , Venetis CA , et al . ( 2008 ) Cryopreservation of human embryos by vitrifi cation or slow freezing: a systematic review and meta-analysis . Fertility and Sterility 90 (1): 186 –193.
Magli MC , Gianaroli L , Grieco N , et al . ( 2006 ) Cryopreservation of biopsied embryos at the blastocyst stage . Human Reproduction 21 (10): 2656 –2660.
Martino A , Songsasen N , Leibo SP ( 1996 ) Development into blastocysts of bovine oocytes cryopreserved by ultra-rapid cooling . Biology of Reproduction 54 : 1059 –1069.
Ménézo Y , Nicollet B , Herbaut N , André D ( 1992 ) Freezing cocultured human blastocysts . Fertility and Sterility 58 (5): 977 –980.
Noyes N , Reh A , McCaff rey C , Tan O , Krey L ( 2009 ) Impact of developmental stage at cryopreservation and transfer on clinical outcome of frozen embryo cycles . Reproductive Biomedicine Online 19 (Suppl. 3): 9 –15.
Pribenszky C , Losonczi E , Molnár M , et al . ( 2010 ) Prediction of in-vitro developmental competence of early cleavage-stage mouse embryos with compact time-lapse equipment . Reproductive BioMedicine Online 20 (3): 371 –379.
Rall WF ( 1987 ) Factors aff ecting the survival of mouse embryos cryopreserved by vitrifi cation . Cryobiology 24 : 387 –402.
Rall WF , Fahy GM ( 1985 ) Ice-free cryopreservation of mouse embryos at –196°C by vitrifi cation . Nature 313 : 573 –575.
Rama Raju GA , Jaya Prakash G , Murali Krishna K , Madan K ( 2009 ) Neonatal outcome aft er vitrifi ed day 3 embryo transfers: a preliminary study . Fertility and Sterility 92 (1): 143 –148.
Riggs R , Mayer J , Dowling-Lacey D , et al . ( 2010 ) Does storage time infl uence post-thaw survival and pregnancy outcome? An analysis of 11,768 cryopreserved human embryos . Fertility and Sterility 93 (1): 109 –115.
Schmidt CL , Taney FH , de Ziegler D , et al . ( 1989 ) Transfer of cryopreserved-thawed embryos: the natural cycle versus controlled preparation of the endometrium with gonadotropin-releasing hormone agonist and exogenous estradiol and progesterone (GEEP) . Fertility and Sterility 52 : 1609 –1616.
Schuster TG , Hickner-Cruz K , Ohl DA , Goldman E , Smith GD ( 2003 ) Legal considerations for cryopreservation of sperm and embryos . Fertility and Sterility 80 (1): 61 –66.
Sher G , Keskintepe L , Mukaida T , et al . ( 2008 ) Selective vitrifi cation of euploid oocytes markedly improves survival, fertilization and pregnancy-generating potential . Reproductive Biomedicine Online 17 (4): 524 –529.
Shu Y , Watt J , Gebhardt J , et al . ( 2009 ) Th e value of fast blastocoele re-expansion in the selection of a viable thawed blastocyst for transfer . Fertility and Sterility 91 (2): 401 –406.
Testart J , Belaisch Allart J , Lassalle B , et al . ( 1987 ) Factors infl uencing the success rate of human embryo freezing in an in vitro fertilization and embryo transfer program . Fertility and Sterility 48 : 107 –112.
Trounson A , Mohr L ( 1983 ) Human pregnancy following cryopreservation, thawing, and transfer of an eight-cell embryo . Nature 305 : 707 –709.
Tucker MJ , Cohen J , Massey JB , et al . ( 1991 ) Partial dissection of the zona pellucida of frozen-thawed human embryos may enhance blastocyst hatching, implantation, and pregnancy rates . American Journal of Obstetrics and Gynecology 165 (2): 341 –344.
Vajta G , Holm P , Kuwayama M , et al . ( 1998 ) Open pulled straw (OPS) vitrifi cation: a new way to reduce cryoinjuries of bovine ova and embryos . Molecular Reproduction and Development 51 : 53 –58.
Van den Abbeel E , Camus M , Verheyen G , et al . ( 2005 ) Slow controlled-rate freezing of sequentially cultured human blastocysts: an evaluation of two freezing strategies . Human Reproduction 20 (10): 2939 –2945.
Van Den Abbeel E , Van Steirteghem A ( 2000 ) Zona pellucida damage to human embryos aft er cryopreservation and the consequences for their blastomere survival and in-vitro viability . Human Reproduction 15 (2): 373 –378.

Chapter 12: Cryopreservation of gametes and embryos
212
Wennerholm UB , Söderström-Anttila V, Bergh C, et al . ( 2009 ) Children born aft er cryopreservation of embryos or oocytes: a systematic review of outcome data . Human Reproduction 24 (9): 2158 –2172.
Youssry M , Ozmen B , Zohni K , Diedrich K , Al-Hasani S ( 2008 ) Current aspects of blastocyst cryopreservation . Reproductive Biomedicine Online 16 (2): 311 –320.
Sperm freezing Gilmore JA , Liu J , Gao DY , Critser JK ( 1997 ) Determination
of optimal cryoprotectants and procedures for their addition and removal from human spermatozoa . Human Reproduction 12 : 12 –18.
Giraud MN , Motta C , Boucher D , Grizard G ( 2000 ) Membrane fl uidity predicts the outcome of cryopreservation of human spermatozoa . Human Reproduction 15 : 2160 –2164.
Hammerstedt RH , Graham JK , Nolan JP ( 1990 ) Cryopreservation of human sperm . Journal of Andrology 11 (1): 73 –88.
Leibo SP , Bradley L ( 1999 ) Comparative cryobiology of mammalian spermatozoa. In: Gagnon C (ed.) The Male Gamete: From Basic Knowledge to Clinical Applications . Cache River Press , Vienna, IL , pp. 501–516.
Mahadevan M , Trounson A ( 1983 ) Eff ects of CPM and dilution methods on the preservation of human spermatozoa . Andrologia 15 : 355 –366.
McLaughlin EA , Ford WCL , Hill MGR ( 1990 ) A comparison of the freezing of human semen in the uncirculated vapour above liquid nitrogen and in a commercial semi-programmable freezer . Human Reproduction 5 : 734 –738.
Meirow D , Schenker JG ( 1995 ) Cancer and male infertility . Human Reproduction 10 : 2017 –2022.
Morris GJ , Acton E , Avery S ( 1999 ) A new approach to sperm cryopreservation . Human Reproduction 14 : 1013 –1021.
Polge C , Smith AU , Parkes AS ( 1949 ) Revival of spermatozoa aft er vitrifi cation and dehydration at low temperatures . Nature 164 : 666 –667.
Stanic P , Tandara M , Sonicki Z , et al . ( 2000 ) Comparison of protective media and freezing techniques for cryopreservation of human semen . European Journal of Obstetrics, Gynecology and Reproductive Biology 91 : 65 –70.
Walmsley R , Cohen J , Ferrara-Congedo T , Reing A , Garrisi J ( 1999 ) Th e fi rst births and ongoing pregnancies associated with sperm cryopreservation within evacuated egg zonae . Human Reproduction 13 : 61 –70.
Watson PF ( 2000 ) Th e causes of reduced fertility with cryopreserved semen . Animal Reproduction Science 60 : 481 –492.
Wyns C , Curaba M , Vanabelle B , Van Langendonckt A , Donnez J ( 2010 ) Options for fertility preservation in prepubertal boys . Human Reproduction Update 16 (3): 312 –328.
Van den Berg M ( 1998 ) In: Elder K , Elliott T. (eds.) Th e Use of Epididymal and Testicular Sperm in IVF . World Wide Conferences on Reproduction Biology, Ladybrook Publishing , Australia .
Oocyte cryopreservation Al-Hasani S , Diedrich K , van der Ven H , et al . ( 1987 )
Cryopreservation of human oocytes . Human Reproduction 2 : 695 –700.
Al-Hasani S , Ludwig M , Diedrich K , et al . ( 1996 ) Preliminary results on the incidence of polyploidy in cryopreserved human oocytes aft er ICSI . Human Reproduction 11 : Abstract book 1, 50 –51.
Amorim CA , Gonçalves PB , Figueiredo JR ( 2003 ) Cryopreservation of oocytes from pre-antral follicles . Human Reproduction Update 9 (2): 119 –129.
Amorim CA , Van Langendonckt A , David A , Dolmans MM , Donnez J ( 2009 ) Survival of human pre-antral follicles aft er cryopreservation of ovarian tissue, follicular isolation and in vitro culture in a calcium alginate matrix . Human Reproduction 24 (1): 92 –99.
Boldt J , Tidswell J , Sayer A , Kilani R , Cline D ( 2006 ) Human oocyte cryopreservation: 5-year experience with a sodium-depleted slow freezing method . Reproductive Biomedicine Online 13 : 96 –100.
Cao YX , Xing Q , Li L , et al . ( 2009 ) Comparison of survival and embryonic development in human oocytes cryopreserved by slow-freezing and vitrifi cation . Fertility and Sterility 92 (4): 1306 –1311.
Chen C ( 1986 ) Pregnancy aft er human oocyte cryopreservation . Lancet 1 : 884 –886.
Chen SU , Lien YR , Chao KH , et al . ( 2003 ) Eff ects of cryopreservation on meiotic spindles of oocytes and its dynamics aft er thawing: clinical implications in oocyte freezing – a review article . Molecular and Cellular Endocrinology 202 (1–2): 101 –107.
Chen SU , Lien YR , Chen HF , et al . ( 2005 ) Observational clinical follow-up of oocyte cryopreservation using a slow-freezing method with 1,2-propanediol plus sucrose followed by ICSI . Human Reproduction 20 (7): 1975 –1980.
Cobo A , Kuwayama M , Perez S , et al . ( 2008 ) Comparison of concomitant outcome achieved with fresh and cryopreserved donor oocyte vitrifi ed by the cryotop method . Fertility and Sterility 89 (6): 1657 –1664.
Coticchio G , De Santis L , Rossi G , et al . ( 2006 ) Sucrose concentration infl uences the rate of human oocytes with normal spindle and chromosome confi gurations aft er slow-cooling cryopreservation . Human Reproduction 21 (7): 1771 –1776.

Chapter 12: Cryopreservation of gametes and embryos
213
Edgar DH , Gook DA ( 2007 ) How should the clinical effi ciency of oocyte cryopreservation be measured? Reproductive Biomedicine Online 14 (4): 430 –435.
Eppig JJ , O’Brien MJ , Wigglesworth K , et al . ( 2009 ) Eff ect of in vitro maturation of mouse oocytes on the health and lifespan of adult off spring . Human Reproduction 24 (4): 922 –928.
Gook DA , Osborn SM , Johnston WIH ( 1993 ) Cryopreservation of mouse and human oocytes using 1,2-propanediol and the confi guration of the meiotic spindle . Human Reproduction 8 : 1101 –1109.
Gook DA , Osborn SM , Bourne H , Johnston WIH ( 1994 ) Fertilization of human oocytes following cryopreservation: normal karyotypes and absence of stray chromosomes . Human Reproduction 9 : 684 –691.
Gook DA , Osborn SM , Johnston WIH ( 1995a ) Parthenogenetic activation of human oocytes following cryopreservation using 1,2-propanediol . Human Reproduction 10 : 654 –658.
Gook DA , Schiewe MC , Osborn SM , et al . ( 1995b ) Intracytoplasmic sperm injection and embryo development of human oocytes cryopreserved using 1,2-propanediol . Human Reproduction 10 : 2637 –2641.
Hong S , Sepilian V , Chung H , Kim T ( 2009 ) Cryopreserved human blastocysts aft er vitrifi cation result in excellent implantation and clinical pregnancy rates Fertility and Sterility 92 (6): 2062 –2064.
Huang J , Chen H , Tan S , Chian R ( 2007 ) Eff ect of choline-supplemented sodium-depleted slow freezing versus vitrifi cation on mouse oocytes meiotic spindles and chromosome abnormalities . Fertility and Sterility 88 (2): 1093 –1110.
Kuleshova L , Gianaroli L , Magli C , Ferraretti A , Trounson A ( 1999 ) Birth following vitrifi cation of a small number of human oocytes: case report . Human Reproduction 14 : 3077 –3079.
Kuwayama M , Vajta G , Kato O , Leibo SP ( 2005 ) Highly effi cient vitrifi cation method for cryopreservation of human oocytes . Reproductive Biomedicine Online 11 (3): 300 –308.
Lane M , Bavister BD , Lyons EA , Forest KT ( 1999 ) Containerless vitrifi cation of mammalian oocytes and embryos- adapting a proven method for fl ash-cooling protein crystals to the cryopreservation of live cells . Nature Biotechnology 17 : 1234 –1236.
Nottola S , Coticchio G , De Santis L , et al . ( 2008 ) Ultrastructure of human mature oocytes aft er slow cooling cryopreservation with ethylene glycol . Reproductive Biomedicine Online 17 (3): 368 –377.
Noyes N , Porcu E , Borini A ( 2009 ) Over 900 oocyte cryopreservation babies born with no apparent increase in congenital anomalies . Reproductive Biomedicine Online 18 (6): 769 –776.
Parmegiani L , Cognigni GE , Bernardi S , et al . ( 2008 ) Freezing within 2 h from oocyte retrieval increases the effi ciency of human oocyte cryopreservation when using a slow freezing/rapid thawing protocol with high sucrose concentration . Human Reproduction 23 (8): 1771 –1777.
Parmegiani L , Bertocci F , Garello C , Salvarani MC , Tambuscio G , Fabbri R ( 2009 ) Effi ciency of human oocyte slow freezing: results from fi ve assisted reproduction centres . Reproductive Biomedicine Online 18 (3): 352 –359.
Paynter SJ , Borini A , Bianchi V , et al . ( 2005 ) Volume changes of mature human oocytes on exposure to cryoprotectant solutions used in slow cooling procedures . Human Reproduction 20 (5): 1194 –1199.
Pickering SJ , Braude PR , Johnson MH , Cant A , Currie J ( 1990 ) Transient cooling to room temperature can cause irreversible disruption of the meiotic spindle in the human oocyte . Fertility and Sterility 54 : 102 –108.
Porcu E , Fabbri R , Seracchioli R , et al . ( 1997 ) Birth of a healthy female aft er intracytoplasmic sperm injection of cryopreserved human oocytes . Fertility and Sterility 68 : 724 –726.
Rienzi L , Martinez F , Ubaldi F , et al . ( 2004 ) Polscope analysis of meiotic spindle changes in living metaphase II human oocytes during the freezing and thawing procedures. Human Reproduction 19 (3): 655 –659.
Sereni E , Bonu M , Borini A ( 2000 ) High survival rates aft er cryopreservation of human prophase oocytes . Fertility and Sterility 74 (Suppl. 1): S161 .
Stachecki JJ , Cohen J , Willadsen SM ( 1999 ) Cryopreservation of mouse oocytes: Th e eff ect of replacing sodium with choline in the freezing medium . Cryobiology 37 : 346 –354.
Stachecki J , Cohen J , Garrisi J , Munne S , Willadsen SM ( 2006 ) Cryopreservation of unfertilized human oocytes . Reproductive Biomedicine Online 13 (2): 222 –227.
Van den Abbeel E , Schneider U , Liu J , et al . ( 2007 ) Osmotic responses and tolerance limits to changes in external osmolalities, and oolemma permeability characteristics, of human in vitro matured MII oocytes . Human Reproduction 22 (7): 1959 –1972.
Yoon TK , Kim TJ , Park SE , Hong SW , Ko JJ , Chung HM , Cha KY ( 2003 ) Live births aft er vitrifi cation of oocytes in a stimulated in vitro fertilization-embryo transfer program . Fertility and Sterility 79 (6): 1323 –1326.
Gonadal tissue preservation Andersen CY , Rosendahl M , Byskov AG , et al . ( 2008 ) Two
successful pregnancies following autotransplantation of frozen/thawed ovarian tissue . Human Reproduction 23 (10): 2266 –2272.
Chen SU , Chien CL , Wu MY , et al . ( 2006 ) Novel direct cover vitrifi cation for cryopreservation of ovarian tissues

Chapter 12: Cryopreservation of gametes and embryos
214
increases follicle viability and pregnancy capability in mice . Human Reproduction 21 (11): 2794 –800.
Cox SL , Shaw J , Jenkin G ( 1996 ) Transplantation of cryopreserved fetal ovarian tissue to adult recipients in mice . Journal of Reproduction and Fertility 107 (2): 315 –322.
Demirci B , Lornage J , Salle B , et al . ( 2003 ) Th e cryopreservation of ovarian tissue: uses and indications in veterinary medicine . Th eriogenology 60 (6): 999 –1010.
Demeestere I , Simon P , Buxant F , et al . ( 2006 ) Ovarian function and spontaneous pregnancy aft er combined heterotopic and orthotopic cryopreserved ovarian tissue transplantation in a patient previously treated with bone marrow transplantation: case report . Human Reproduction 21 (8): 2010 –2014.
Demeestere I , Simon P , Emiliani S , Delbaere A , Englert Y ( 2007 ) Fertility preservation: successful transplantation of cryopreserved ovarian tissue in a young patient previously treated for Hodgkin’s disease . Oncologist 12 (12): 1437 –1442.
Dolmans MM , Donnez J , Camboni A , et al . ( 2009 ) IVF outcome in patients with orthotopically transplanted ovarian tissue . Human Reproduction 24 (11): 2778 –2787.
Donnez J , Dolmans MM , Demylle D , et al . ( 2004 ) Livebirth aft er orthotopic transplantation of cryopreserved ovarian tissue . Lancet 364 (9443): 1405 –1410.
Donnez J , Martinez-Madrid B , Jadou Pl , et al . ( 2006 ) Ovarian tissue cryopreservation and transplantation: a review . Human Reproduction Update 12 : 519 –535.
Donnez J , Jadoul P , Squiffl et J , et al . ( 2009 ) Cryopreservation and autotransplantation of human ovarian tissue prior to cytotoxic therapy – a technique in its infancy but already successful in fertility preservation . European Journal of Cancer 45 (9): 1547 –1553.
Gook DA , Edgar DH , Stern C ( 1999 ) Eff ect of cooling rate and dehydration regimen on the histological appearance of human ovarian cortex following cryopreservation in 1,2-propanediol . Human Reproduction 14 : 2061 –2068.
Gosden RG ( 2002 ) Gonadal tissue cryopreservation and transplantation . Reproductive Biomedicine Online 4 (Suppl. 1): 64 –67.
Gosden RG , Oktay K , Radford JA , et al . ( 1997 ) Ovarian tissue banking . Human Reproduction Update 3 , CD-ROM, item 1, video.
Hovatta O ( 2004 ) Cryopreservation and culture of human ovarian cortical tissue containing early follicles . European Journal of Obstetrics, Gynecology, and Reproductive Biology 113 (Suppl. 1): S50 –54.
Huang L , Mo Y , Wang W , Li Y , Zhang Q , Yang D ( 2008 ) Cryopreservation of human ovarian tissue by solid-surface vitrifi cation . European Journal of Obstetrics, Gynecology and Reproductive Biology 139 (2): 193 –198.
Isachenko V , Isachenko E , Reinsberg J , et al . ( 2007 ) Cryopreservation of human ovarian tissue: comparison
of rapid and conventional freezing . Cryobiology 55 (3): 261 –268.
Isachenko V , Lapidus I , Isachenko E , et al . ( 2009 ) Human ovarian tissue vitrifi cation versus conventional freezing: morphological, endocrinological, and molecular biological evaluation . Reproduction 138 (2): 319 –327.
Isachenko V , Isachenko E , Kreienberg R , Woriedh M , Weiss J ( 2010 ) Human ovarian tissue cryopreservation: quality of follicles as a criteria of eff ectiveness . Reproductive Biomedicine Online 20 (4): 441 –442.
Kader A , Biscotti C , Agarwal A , Sharma R , Falcone T ( 2008 ) Comparison of post-warming degeneration and apoptosis of porcine ovarian tissue following vitrifi cation using the Ohio-Cryo device and slow cryopreservation . Fertility and Sterility 90 : S288 –S288.
Kagawa N , Kuwayama M , Silber S , et al . ( 2008 ) Successful vitrifi cation method for bovine and human ovarian tissue: the cryotissue method . Human Reproduction 23 (Suppl. 1): 145 .
Kagawa N , Silber S , Kuwayama M ( 2009 ) Successful vitrifi cation of bovine and human ovarian tissue . Reproductive Biomedicine Online 18 (4): 568 –577.
Kim SS , Battaglia DE , Soules MR ( 2001 ) Th e future of human ovarian cryopreservation and transplantation . Fertility and Sterility 75 : 1049 –1056.
Kim SS , Lee WS , Chung MK , et al . ( 2009 ) Long-term ovarian function and fertility aft er heterotopic autotransplantation of cryobanked human ovarian tissue: 8-year experience in cancer patients . Fertility and Sterility 91 (6): 2349 –2354.
Li YB , Zhou CQ , Yang GF , Wang Q , Dong Y ( 2007 ) Modifi ed vitrifi cation method for cryopreservation of human ovarian tissues . Chinese Medical Journal (Engl.) 120 (2): 110 –114.
Martinez-Madrid B , Dolmans MM , Van Langendonckt A , Defrère S , Donnez J ( 2004 ) Freeze-thawing intact human ovary with its vascular pedicle with a passive cooling device . Fertility and Sterility 82 (5): 1390 –1394.
Newton H , Aubard Y , Rutherford A , Sharma V , Gosden RG ( 1996 ) Low temperature storage and graft ing of human ovarian tissue . Human Reproduction 11 : 487 –491.
Newton H , Fisher J , Arnold JR , et al . ( 1998 ) Permeation of human ovarian tissue with cryoprotective agents in preparation for cryopreservation . Human Reproduction 13 : 376 –380.
Nugent D , Meirow D , Brook PF , Aubard Y , Gosden RG ( 1997 ) Transplantation in reproductive medicine: previous experience, present knowledge, and future prospects . Human Reproduction Update 3 : 267 –280.
Nugent D , Newton H , Gosden RG , Rutherford AJ ( 1998 ) Investigation of follicle survival aft er human heterotopic graft ing . Human Reproduction 13 (1): 22 –23.

Chapter 12: Cryopreservation of gametes and embryos
215
Oktay K , Nugent D , Newton H ( 1997 ) Isolation and characterisation of primordial follicles from fresh and cryopreserved human ovarian tissue . Fertility and Sterility 67 : 481 –486.
Oktay K , Newton H , Aubard Y , Salha O , Gosden RG ( 1998 ) Cryopreservation of immature human oocytes and ovarian tissue: an emerging technology? Fertility and Sterility 69 : 1 –7.
Onions VJ , Webb R , McNeilly AS , Campbell BK ( 2009 ) Ovarian endocrine profi le and long-term vascular patency following heterotopic autotransplantation of cryopreserved whole ovine ovaries . Human Reproduction 24 (11): 2845 –2855.
Picton HM , Kim SS , Gosden RG ( 2000 ) Cryopreservation of gonadal tissue and cells . British Medical Bulletin 56 : 603 –615.
Shaw J , Trounson AO ( 1997 ) Ovarian banking for cancer patients – oncological implications in the replacement of ovarian tissue . Human Reproduction 12 : 403 –405.
Shaw JM , Oranratnachai A , Trounson AO ( 2000 ) Fundamental cryobiology of mammalian oocytes and ovarian tissue . Th eriogenology 53 : 59 –72.
Tryde Schmidt KL , Yding Andersen C , Starup J , et al . ( 2004 ) Orthotopic autotransplantation of cryopreserved ovarian tissue to a woman cured of cancer – follicular growth, steroid production and oocyte retrieval . Reproductive Biomedicine Online 8 (4): 448 –453.

Chapter
1
216
Micromanipulation techniques
Introduction Biologists and physiologists began to micromanipulate cells during the last century, using a variety of manipu-lator systems to dissect or record from cells. Th e earli-est attempt to inject sperm was recorded in 1914, when G.I. Kite injected starfi sh oocytes with sperm, but with inconclusive results (Lillie, 1914 ). Experiments in which sperm were injected into eggs around the mid-1960s were primarily designed to investigate the early events of fertilization, i.e., the role of membrane fusion, acti-vation of the oocyte and the formation of the pronuclei. Two series of early experiments by independent groups demonstrated major species diff erences. Hiramoto showed in the 1960s that microinjection of spermato-zoa into unfertilized sea urchin oocytes did not induce activation of the oocyte or condensation of the sperm nucleus, whereas others demonstrated the opposite in frog oocytes. Ryuzo Yanagimachi and his group later demonstrated that isolated hamster nuclei could develop into pronuclei aft er microinjection into homologous eggs, and a similar result was obtained when freeze-dried human spermatozoa were injected into a hamster egg. Th ese experiments indicated that membrane fusion events can be bypassed during the activation of mam-malian oocytes, without compromising the initiation of development. Th e experiments not only provided infor-mation on the mechanism of fertilization, but also led to a new technique in clinical embryology .
Th e fi rst clinical application of microsurgical techniques was partial zona dissection (PZD) devel-oped by Jacques Cohen and colleagues to aid fertil-ization in human oocytes Th is mechanical technique involves breaching a slit in the zona pellucida with a sharp glass micropipette and subsequently placing the dissected oocyte into a suspension of spermato-zoa, on the assumption that sperm entry is facilitated by the slit. In the same year, S.C. Ng and colleagues
in Singapore reported the fi rst pregnancy from sub-zonal sperm injection (SUZI) , where several sperm-atozoa are inserted into the perivitelline space. In 1990, the same group reported activation of human oocytes following intracytoplasmic injection (ICSI) of human spermatozoa , and in 1992 Palermo and col-leagues in Brussels reported the fi rst live birth from this technique of ICSI. Since the time of these pioneer-ing reports, many healthy ICSI babies have been born worldwide. Th e technique of assisted hatching was also developed during the 1990s, using microman-ipulation to cut a slit in the zona pellucida or dissolve a hole in the zona with an acid solution (zona drill-ing , ZD). Assisted hatching was proposed as a means of facilitating embryo implantation in selected cases. Figure 13.1 shows a diagrammatic representation of these micromanipulation procedures.
ICSI – intracytoplasmic sperm injection Genetic implications Prior to 1992, the majority of cases of severe male infertility were virtually untreatable, and failure of fertilization was observed in up to 30% of IVF treatments for male infertility. Th e introduction of micromanipulation techniques such as ZD, PZD and SUZI raised the hopes of a better prognosis for these cases, but did not overall provide a substantial improvement in success rates. Th e introduction and successful application of ICSI by GianPiero Palermo and colleagues at Th e Free University in Brussels, Belgium, produced a dramatic improvement in the treatment of severe male infertility by assisted repro-ductive technology.
Th e establishment of ICSI as a routine technique was quickly followed by the introduction of techniques
13
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 13: Micromanipulation techniques
217
for collecting sperm samples from the epididymis and directly from the testis, so that the whole spectrum of male infertility can now be treated, from suboptimal ejaculate samples or ejaculatory failure, to obstructive and nonobstructive causes of azoospermia. However, an increasing number of genetic defects have been found to be associated with male infertility: a higher incidence of numerical and structural chromosomal aberrations is found in infertile and subfertile men than in the general population, in particular karyo-types 47XXY, 47XYY, 46XX, 46X, derY, Robertsonian translocations , reciprocal translocations, inversions and additional marker chromosomes. Between 12% and 18% of men with azoospermia or severe oligo-spermia (less than 300 000 sperm in the ejaculate) have deletions in intervals 5 and 6 on the long arm of the Y chromosome. Microdeletions of the q11 region of the Y chromosome are related to the dysfunction of Deleted in AZoospermia (DAZ) and RNA-binding motif (RBM) genes, and androgen receptor (AR) gene mutations have also been reported in infertile men. In a population of approximately 3000 infertile men, the pathological (nonpolymorphic, phenotype associ-ated) microdeletions rate in at least one of four crit-ical regions on the Y chromosome was found to be as high as 22%, with an additional (as yet unknown) percentage being attributed to cryptic mosaicism. Furthermore, it appears that microdeletions will be transmitted in at least 10% of unselected father/son pairs. Th ree to ten per cent of infertile men present with congenital bilateral absence of the vas deferens (CBAVD), and approximately 65% of these individuals
carry the gene for cystic fi brosis (CF), with defects in the cystic fi brosis conductance regulator (CFTR) gene. Many are compound heterozygous for the CFTR muta-tion, with an increased risk of having children with CF or CBVAD.
Although the genetic risk for couples who require ICSI treatment has yet to be fully defi ned, karyotyping, and preferably also Y-microdeletion analysis is recom-mended as part of the pretreatment screening pro-cess for all men referred for ICSI (Qureshi et al ., 1996 ; Simoni et al ., 1998 ). Th e couple should also have access to professional genetic counseling to discuss poten-tial risks, and appropriate informed consent must be obtained before treatment.
Surgical sperm retrieval In cases of obstructive azoospermia , samples can be aspirated from the epididymis. Th e original “open” microsurgical technique of microepididymal sperm aspiration (MESA) was superseded by the simpler pro-cedure of percutaneous epididymal sperm aspiration (PESA), which can be carried out by fertility special-ists without microsurgical skills, and can be performed under local anesthetic or mild sedation as an outpatient procedure. Aspiration is carried out using a 25-gauge butterfl y needle connected to a syringe. If sperm can-not be aspirated from the epididymis, a modifi cation of the technique using wide-bore needle aspiration of the testis, testicular sperm aspiration (TESA) or testicular fi ne needle aspiration (TEFNA) oft en harvests suffi cient testicular spermatozoa to carry out an ICSI procedure. In nonobstructive azoospermia, spermatogenesis is
Figure 13.1 Micromanipulation techniques include subzonal injection (SZI), intracytoplasmic sperm injection (ICSI), zona drilling (ZD) and partial zona dissection (PZD).

Chapter 13: Micromanipulation techniques
218
impaired. Th e epididymis is devoid of sperm, but the testis usually contains focal areas of spermatogenesis. Multiple biopsies may be required in order to iden-tify these areas. Th e focal nature of spermatogenesis in such patients makes diagnosis based upon a single biopsy unrealistic, but prepared testicular samples can also be cryopreserved for a future ICSI procedure at the time of diagnostic testicular biopsy. Th e biopsy is car-ried out either by multiple needle aspirations (TEFNA or TESA) or by open biopsy (testicular sperm extrac-tion: TESE), and both procedures may be safely carried out with local anesthetic or mild sedation.
Indications for ICSI Th e ICSI procedure involves the injection of a single immobilized spermatozoon directly into an oocyte, and therefore not only can it be used for cases in which there are extremely low numbers of sperm, but in bypassing gamete interaction at the level of the zona pellucida and the vitelline membrane it can also be used in the treat-ment of qualitative or functional sperm disorders. 1. Couples who have suff ered recurrent failure of
fertilization aft er IVF-ET may have one or more disorders of gamete dysfunction in which there is a barrier to fertilization at the level of the acrosome reaction , zona pellucida binding or interaction, zona penetration, or fusion with the oolemma. ICSI should be off ered to patients who have unexplained failure of fertilization in a previous IVF-ET cycle.
2. Severe oligospermia can be treated with ICSI; in patients where as many normal vital sperm can be recovered as there are oocytes to be inseminated, fertilization can be achieved in approximately 90% of cases. In extreme cases of cryptozoospermia, where no sperm cells can be seen by standard microscopy, centrifugation of the neat sample at a higher than usual centrifugal force (1800 g , 5 minutes) may result in the recovery of an adequate number of sperm cells.
3. Severe asthenozoospermia, including patients with sperm ultrastructural abnormalities such as Kartagener’s syndrome, or “9 + 0” axoneme disorders can be treated by ICSI.
4. Teratozoospermia, including absolute teratozoospermia or globozoospermia.
5. In cases of CBAVD, vasectomy or postinfl ammatory obstruction of the vas, sperm samples can be retrieved by PESA, TESA or TESE.
6. Samples can be recovered by needle or open biopsy of the testis in cases of nonobstructive azoospermia .
7. In cases of ejaculatory dysfunction, such as retrograde ejaculation, a suffi cient number of sperm cells can usually be recovered from the urine.
8. Paraplegic males have been given the chance of biological fatherhood using electro ejaculation and IVF (see www.multicept.dk ); they may also be successfully treated using a combination of PESA/TESA/TESE and ICSI.
9. Immunological factors – couples in whom there may be antisperm antibodies in female sera/follicular fl uid , or antisperm antibodies in seminal plasma following vasectomy reversal or genital tract infection can be successfully treated by ICSI.
10. Oncology – male patients starting chemotherapy or radiotherapy should have semen samples frozen for use in the future; ICSI off ers the patient an excellent chance of achieving fertilization following recovery from their disease and treatment. Testicular biopsy specimens may also be cryopreserved for these patients as a further back-up when the quality of the ejaculate is inadequate for freezing.
11. For preimplantation genetic diagnosis where PCR is used, ICSI should be used as the means of fertilization to prevent sperm contamination of the sample .
Although the main indication for ICSI was origin-ally for the treatment of male factor infertility, its use has become far more widespread, with an increasing trend to use it routinely for indications that include moderate male subfertility, advanced maternal age, low responder patients, donor oocytes or sperm; indeed, some clinics now use ICSI as a routine for all indications. European data for 2005 showed that the proportion of ICSI cycles in diff erent countries ranged from 58% to 67%; in the USA, 62.2% of fresh non-donor cycles used ICSI during 2006. However, several randomized controlled studies have compared the effi cacy of IVF versus ICSI in couples with non-male factor infertility, with results that showed no diff erence in fertilization or pregnancy rates. A Cochrane review (van Rumste et al ., 2004 ) concluded that the use of ICSI for non-male factor infertility remains an open question, and further research should focus on live birth rates and adverse events. In their 2008 report on good clinical treatment

Chapter 13: Micromanipulation techniques
219
in assisted reproduction , the European Society for Human Reproduction and Embryology (ESHRE) pub-lished an Executive Summary that concludes: “ICSI should be considered in the presence of severe sperm abnormalities or a history of fertilization failure in conventional IVF attempts. It must be emphasized that ICSI does not represent the most suitable treatment for female pathologies such as poor ovarian response or previous implantation failure.”
Practical aspects When scheduling patients for ICSI, it is important that the whole IVF team should appreciate the extra dimension of time and eff ort required for every case, and make an eff ort to schedule the laboratory work-load accordingly. ICSI demands the same meticulous attention to detail that is needed in all IVF manipula-tions, but the number of details requiring attention is dramatically increased. Successful results with ICSI can only be achieved with the dedication of concen-trated time, eff ort and patience.
Location of ICSI set-up Th e laboratory should preferably be on a ground fl oor, near a structural frame or wall to minimize vibration interference, and must be kept dust-free. Th e equip-ment must be installed on a substantial bench top, away from distractions of traffi c such as people or trol-leys, etc. Any vibration will seriously interfere with the injection procedure, and it is essential to make sure that the equipment is completely stable, using anti-vibration equipment if necessary. Subdued light-ing is helpful for microscopy. Well in advance of any ICSI procedure, ensure that the microscope is set up optically and checked. Ensure that the tool holders and all other parts of the micromanipulation system are correctly fi tted and adjusted for optimal range of movement, and that the microtools can be accurately aligned .
Micro-injection equipment All the major microscopy companies now supply micro-injection set-ups ready for use. Th e essential element is an inverted microscope with ×10, ×20 and ×40 objectives, Hoff man modulation contrast optics in order to visualize the cells on plastic Petri dishes (Nomarski optics uses polarized light and cannot be used through plastic). Th e micromanipulators consist of two coarse motorized manipulators and two fi ne
mechanical, electrical or hydraulic joysticks, together with micro-syringes capable of delivering minute quan-tities of liquid. Tables 13.1 and 13.2 compare the diff er-ent types of equipment currently available. For training purposes it is advisable to have a camera attached to one of the microscope optical outlets.
Microtools Two types of microtools are used: 1. Holding pipettes to hold and immobilize the
oocyte Outer diameter: 0.080–0.150 mm Inner diameter: 0.018–0.025 mm Fire-polished aperture
2. Injection pipettes to immobilize, aspirate and inject the sperm cell
Outer diameter: 0.0068–0.0078 mm Inner diameter: 0.0048–0.0056 mm Beveled tip, sometimes tipped with a spike.
Both microtools are bent to an angle of approximately 30° at the distal end in order to facilitate horizontal positioning and manipulation adjustment within cul-ture dishes. Aspiration pipettes (of diff erent diameters) may also be used to aspirate anucleate fragments, or to biopsy blastomeres for preimplantation diagnosis. A third type of microtool may be used for piercing or cutting the zona pellucida in assisted zona hatch-ing techniques . Uniform microtool quality is crucial for consistent results, and specifi cally tooled, sterile, ready-to-use holding and injection pipettes are com-mercially available. A blunt injection pipette can dam-age the oocyte by compression, whereas a pipette with too large a diameter will damage the oocyte by inject-ing too much fl uid .
Supplies Most manufacturers of tissue culture media supply all the components necessary for micromanipulation techniques.
Polyvinyl pyrrolidine (PVP) A viscous solution of 10% polyvinyl pyrrolidine is used to reduce sperm motility prior to immobilization and aspiration into the injection pipette. Experienced operators can carry out the procedure without the use of PVP, but it is helpful in the initial stages of learning and practice. Experimental evidence has shown that PVP can interact with acrosomal and mitochondrial

Chapter 13: Micromanipulation techniques
220
Table 13.1 Micromanipulator
Manipulator type Pros Cons Examples
Manual
Fluid-fi lled: oil, fl uorinert, distilled water
Easy control Air bubbles render control diffi cult. Leakage of fl uid can be messy, requires careful priming. Time-consuming to set up and fl ush system. Glass syringes expensive
Narashige, Eppendorf
Air-fi lled OK for holding pipette Good control only if set up carefully, with a bubble of oil between air and media
Research Instruments, Narashige
Pneumatic Injection controlled by foot pedal
Pressure leakage Tritech
Piezo Drill Less disruption to the cytoplasm
Diffi cult learning curve; possible use of mercury
PrimeTech
Comments contributed by M. Blayney, A. Burnley, L. Devlin, D. Kastelic, M. van den Berg and B. Woodward.
Table 13.2 Joysticks
Joystick type Pros Cons Examples
Hanging joystick Comfortable to use for short cases
Elevated hand position can be uncomfortable during long ICSI cases
Narashige
Standing joystick All-in-one 3-D control May fall aside, with possible oocyte damage
Narishige, Eppendorf
Mechanical Separate coarse and fi ne manipulators. Very little to go wrong
Usually fi xed to the microscope, with possible vibration transmission; 2-D control separate to “up-down” control
Research Instruments
Hydraulic Smooth System fails if there are any leaks, the oil degrades in sunlight
Narashige
Motorized Very convenient if positions can be stored in memory. Movements are quick, decreasing ICSI procedure time
Some have a delay, pipette continues to move over a small distance. Potential for breakdown, diffi cult to repair in-house
Eppendorf, Narashige
Comments contributed by M. Blayney, A. Burnley, L. Devlin, D. Kastelic, M. van den Berg and B. Woodward.
membranes, as well as cause chromatin deterioration aft er prolonged exposure, and questions have been raised about the wisdom/safety of injecting this artifi -cial agent directly into ooplasm. Although no adverse
eff ects have as yet been reported, it should be used cautiously, with attention to the time that the sperm is exposed to the polymer, and with eff orts to minimize the amount that is injected into the oocyte cytoplasm.

Chapter 13: Micromanipulation techniques
221
Hyaluronic acid (HA) Hyaluronic acid (HA), a natural component of the cumulus–oocyte complex, can be used as an alternative to PVP. HA has a relatively high negative charge and a high hydration capacity, so that viscous solutions can be prepared which can be used to slow sperm motility for the ICSI procedure; a commercial preparation using recombinant HA is available (Sperm Slow, Medicult).Th e motility of spermatozoa in a hyaluronate solution resembles that in the extracellular matrix of mature cumulus cells, and spermatozoa resume normal motil-ity once returned to culture medium. Binding to HA has also been used as a marker of sperm maturity, and this off ers added benefi t to its use as an alternative to PVP for sperm impedance (van den Bergh et al ., 2009 ); a further advantage is that it degrades to natural sugar molecules that can be readily metabolized by cellular pathways .
Hyaluronidase Th is enzyme is used to loosen and disperse cells of the cumulus and corona, prior to their removal from the oocyte by dissection. Preparations of sheep or bovine origin were commonly used in the past, but human recombinant hyaluronidase is now available (e.g., Cumulase, Origio; Hyase, Vitrolife), and its use is pref-erable in order to minimize risks of disease transmis-sion from the animal sources.
ICSI – step by step Selecting sperm for injection As discussed in Chapter 10 , there is evidence that sperm with DNA damage can have an adverse eff ect on the outcome of ART. Eff orts have been made to develop techniques that will enhance sperm prepar-ation methods that can be used to identify and select sperm with lesser levels of chromatin or DNA dam-age. Technologies that have been applied include magnetic-activated cell sorting (MACS, Said et al ., 2008 ), electrophoretic separation of sperm on the basis of their charge and size (Fleming et al ., 2008 ), binding to hyaluronic acid as an indication of sperm maturity (Huszar et al ., 2007 ), using PICSI (Petri-dish ICSI) dishes containing hyaluronic acid bonded to the Petri dish ( www.midatlanticdiagnostics.com ), assess-ment of sperm head birefringence (Gianaroli et al ., 2008 ), and the use of high-magnifi cation microscopy (Bartoov et al ., 2003 ). To date, intracytoplasmic mor-phologically selected sperm injection (IMSI) appears
to be the technique that shows the most promise in sperm selection for ICSI, and will be discussed in more detail below.
Oocyte preparation and handling Patients for ICSI have oocyte retrieval scheduled aft er programmed controlled ovarian hyperstimulation (COH), according to protocols described in Chapter 2 . Oocyte identifi cation is carried out immediately aft er follicle aspiration, using a dissecting microscope with heated stage. Take care to maintain stable temperature and pH of the aspirates at all times. At the end of the oocyte retrieval, note quality and assess the maturity of the oocytes, and preincubate them at 37°C in an atmosphere of CO 2 in air until preparations are ready for cumulus–corona removal.
Cumulus–corona removal 1. Prepare a culture dish containing one drop of
hyaluronidase solution and 5 wash drops of a HEPES-buff ered medium, covered with an overlay of equilibrated mineral oil (denudation may also be carried out in Nunc four-well dishes). Incubate at 37°C for 30–60 minutes. Note : HEPES-buff ered medium has been adjusted to pH 7.4 and usually 5 mM bicarbonate, and exposure to a CO 2 atmosphere will cause the pH to drop; therefore culture dishes that contain HEPES-buff ered media should be warmed to 37°C in a warming oven, and not in a CO 2 incubator.
2. Prepare a thin glass probe and select denudation pipettes.
3. Remove the oocyte and hyaluronidase dishes from the incubator. Place one to four oocytes together into the enzyme drop, agitating gently until the cells start to dissociate. Do not leave them in the enzyme for more than 1 minute. Carefully aspirate the oocytes, leaving as much cumulus as possible behind. Wash by transferring them through at least fi ve drops of culture medium, and change to a fi ne-bore tip for aspiration in order to remove all of the coronal cells. Remaining corona cells may hinder the injection process by blocking the needle or obscuring clear observation of the cytoplasm and sperm.
4. Assess the quality and maturity of each oocyte under an inverted microscope. Use the glass probe to roll the oocytes around gently in order to identify the polar body, and examine the ooplasm

Chapter 13: Micromanipulation techniques
222
for vacuoles or other abnormalities. Separate metaphase I or germinal vesicle (GV) oocytes from metaphase II oocytes, label them, and return to the incubator until ready for the injection procedure.
5. Examine the oocytes again before starting the injection procedure to see if any more have extruded the fi rst polar body. ICSI is carried out on all morphologically intact oocytes with fi rst polar body extruded.
Figure 13.2 illustrates diff erent stages of egg maturity that are revealed aft er hyalase treatment and corona dissection.
Preparation for injection 1. Prepare injection dishes with 4–8 droplets of
2–5 μL of HEPES-buff ered culture medium for each individual oocyte, and a 5 μL droplet of PVP for the sperm. Th e droplets can be arranged in a circle with sperm/PVP in the center, or in parallel groups, but must be positioned so that they are not too close to the edge of the dish, where manipulation will be diffi cult. Th e oocyte droplets should not be too close to the sperm/PVP, in order to avoid mixing – use an arrangement that allows quick and easy distinction between sperm and oocyte droplets, with numbers etched on the bottom of the dish. Small volumes of media evaporate very quickly, and they should be covered immediately with a layer of oil. Equilibrate the dishes in the incubator for at least 20–30 minutes, and keep them in the incubator until you are ready
to begin the procedure. If Falcon 1006 dishes are being used with HEPES-buff ered medium, the lids must be tightly fi xed if they are to be equilibrated in a CO 2 incubator. Dishes with HEPES medium and no lids should be warmed to 37°C without CO 2 atmosphere .
2. A prepared and pre-equilibrated traditional culture dish should be available, to transfer and further culture the oocytes aft er injection.
Micromanipulator 1. Make sure that the microscope heating stage
is at a temperature that will maintain droplet temperature in the dishes at 37°C, ensure that all controls are set to neutral and can be comfortably operated, and that you are confi dent that all parts function smoothly before you begin. It is essential to check that you can smoothly carry out very small movements. Th is involves not only the equipment itself, but its position on the bench in relation to your (comfortable) seating position.
2. Insert holding and injection pipettes into the pipette holders, tighten well, and if an oil-fi lled system is being used, make sure that there are no air bubbles in the tubing system. Bubbles interfere with sensitivity when attempting to control movement with fi ne precision.
3. Align the pipettes so that the working tips are parallel to the microscope stage. First align the holding pipette under low magnifi cation, then align the injection pipette, again under low
Figure 13.2 Variations in egg matur-ity found after hyalase treatment and corona dissection. (a) Germinal vesicle; (b) metaphase I; (c) metaphase II.

Chapter 13: Micromanipulation techniques
223
magnifi cation. Check the position of both under high magnifi cation. It is important to begin with pipettes in accurate alignment, with both working tips sharply in focus. If a part of the length is out of focus, the pipette is probably not parallel to the stage, but pointing upwards or downwards.
4. Adjust the injection controls: if using an oil system, the oil should just reach the distal end of the pipette; do not try to fi ll the needle with oil, this will work only if you leave a tiny 5 mm gap of air between the oil and the medium. Briefl y touch the tips of both pipettes in oil, and then in medium, so that the ends fi ll by capillary action (a drop of oil behind the drop of medium will act as a buff er). Th e injection dish is still in the incubator, so you should be using a “blank” dish for this!
Transfer of gametes to the injection dish 1. Carefully add a small aliquot of sperm
suspension (0.3–0.5 mL, depending on the concentration of prepared sperm) to the edge of the central PVP droplet. Th e viscous solution should facilitate sperm handling by slowing down their motility, and also prevents the sperm cells from sticking to the injection pipette during the procedure. Be careful of sperm density: too many sperm will make selection and immobilization more diffi cult.
2. Aft er the sperm droplet has been carefully examined for the presence of debris or any other factors that might cause technical diffi culties, examine all the denuded oocytes again for the presence of a fi rst polar body; wash them gently with HEPES-buff ered medium and transfer one oocyte into each oocyte droplet on the injection dish, taking care to avoid too much handling or cooling of the oocytes. Keep the oocytes in the incubator until you are confi dent that the injection procedure can proceed smoothly. Until suffi cient experience of the procedure has been gained, it may be advisable to keep sperm and oocyte dishes separate, avoiding overexposure of the oocytes while selecting and immobilizing sperm .
3. Place the injection dish with central sperm droplet on the microscope stage. Using the coarse controls
of the manipulator, lower the injection pipette into the drop.
Sperm selection and immobilization 1. Select sperm that appear morphologically
normal. Sperm can be selected and stored in the PVP drop for a limited period of time (be aware that prolonged exposure to PVP can cause damage to sperm membranes) before starting the injection procedure; this is an advantage in cases of extreme cryptozoospermia, and reduces oocyte exposure time. If SpermSlow is being used for immobilization, the sperm become rigid and stick to the dish aft er approximately 30 minutes.
2. Immobilize motile spermatozoa by crushing their tails: select the sperm to be aspirated, and lower the tip of the injection needle onto the midpiece of the sperm, striking down and across, and crushing the tail against the bottom of the dish. Th is “tail crushing” impairs motility and destabilizes the cell membrane; the latter may be required for sperm head decondensation. If the resulting sperm has a “bent” tail, it will be diffi cult to aspirate into the needle, and will stick inside it. When this happens, abandon that sperm and repeat the procedure with another sperm. Do not strike too hard, or the sperm will stick to the bottom of the dish, also making aspiration into the needle diffi cult. Aft er some practice, sperm immobilization in routine ICSI cases can be carried out quite quickly. If the preparation contains only a few sperm with barely recognizable movement and a large amount of debris, this part of the procedure can be very tedious and require great patience!
3. Aspirate the selected immobilized sperm into the injection pipette. Sperm were traditionally aspirated into the pipette tail-fi rst, but they can be aspirated head-fi rst (Woodward et al ., 2008a ). Position the sperm approximately 20 µm from the tip.
4. Lift the injection needle slightly, and move the microscope stage so that the injection pipette is positioned in the fi rst oocyte drop. If the sperm moves up the pipette (due to the diff erence in density between culture medium and PVP) bring it back near the tip before beginning the injection procedure .

Chapter 13: Micromanipulation techniques
224
Injection procedure 1. Lower the holding pipette into the fi rst oocyte
droplet, and position it adjacent to the cell. Using both microtools, slowly rotate the oocyte to locate the polar body. Aspirate gently so that the cell attaches to the pipette. Th e pressure should be great enough to hold the oocyte in place, but not so strong that it causes the oolemma to bulge outwards .
Polar body positioning at 6 or 12 o’clock in order to minimize the possibility of damaging the meiotic spindle was thought to be important, but later evidence using polarized microscopy to visualize the spindle itself suggests that polar body positioning is
of less benefi t than minimizing the duration of the ICSI procedure (Woodward et al ., 2008b ).
2. Move the injection pipette close to the oocyte, and check that it is in the same plane as the right outer border of the oolemma on the equatorial plane at the 3 o’clock position. Check that the sperm can be moved smoothly within the injection needle, and position it near the beveled tip.
3. Advance the pipette through the zona pellucida until the tip almost touches the oocyte membrane at the 9 o’clock position ( Figure 13.3 ). If the pipette is in the wrong plane, entry into the cell will be diffi cult. Th e membrane may rupture spontaneously, or may require negative pressure,
Figure 13.3 ICSI. (a) Metaphase II oocyte with injection needle in position prior to injection. (b) Injection needle within the cytoplasm, prior to release of sperm. (c) Post-injection illustrating the typical track left following withdrawal of the needle. (d) Post-injection, oocyte with a very elastic membrane. (With thanks to Agnese Fiorentino.) (See color plate section).
(a) (b)
(c) (d)

Chapter 13: Micromanipulation techniques
225
sucking the membrane into the pipette before expelling the sperm. When it breaks, there will be a sudden fl ux of cytoplasm into the pipette. Inject the sperm slowly into the oocyte with a minimal amount of fl uid (1–2 picoliters). Th e sperm should be ejected past the tip of the pipette, to ensure a tight insertion among the organelles, which will hold it in place while the pipette is withdrawn. Some surplus medium may be re-aspirated to reduce the size of the breach created during perforation. If the plasma membrane is elastic and diffi cult to break, it may be necessary to withdraw the pipette from the fi rst membrane invagination and slowly repeat the procedure.
4. Gently remove the injection pipette, and examine the breach area. Th e membrane should be funnel-shaped, pointing in towards the center. If the border of the oolemma is everted, cytoplasm may leak out, and the oocyte may subsequently cytolyse. Release the oocyte from the holding pipette.
5. Repeat the sperm aspiration and injection until all the selected metaphase II oocytes have been injected.
6. Wash all the oocytes in culture medium, transfer to the prepared, warmed culture dish, and incubate overnight in the CO 2 incubator.
Injection procedure: important points
1. All conditions must be stable: temperature, pH, equipment properly set up, adjusted, aligned, and checked for leaks and air bubbles. Check every-thing, including secure and comfortable operating position, before you begin.
2. Correct immobilization of sperm . 3. Advance far enough into the ooplasm with the
injection pipette. 4. Ensure that the plasma membrane is broken
(immediate membrane rupture after introducing the injection needle results in a lower probability of fertilization).
5. Inject a minimal volume. 6. If the sperm comes out of the ooplasm into the
perivitelline space, reinject.
Assessment of fertilization and cleavage 16 to 18 hours aft er injection, assess the number and morphology of pronuclei through an inverted micro-scope, rolling the oocyte gently with a glass probe.
Polar bodies should also be counted, with reference to digynic zygotes or activated eggs; polar bodies may fragment, even in normal monospermic fertilization. Rapid cleavage (20–26 hours post-injection) can occur in ICSI zygotes (see also the discussion of “silent fertil-ization” in the “Causes of early embryo arrest” section in Chapter 5 ).
Evaluate normally fertilized, cleaved embryos aft er a further 24 hours of culture. Embryo transfer is usually performed approximately 48–72 hours aft er microinjection. Suitable supernumerary embryos may be cryopreserved either on Day 1 (pronucleate stage) or aft er the transfer procedure on Day 2 or Day 3 (early cleavage stage).
No fertilization after ICSI Complete failure of fertilization is rare aft er ICSI; most of these cases involve semen containing no motile sperm, or round-headed sperm. Some cases of failed fertilization may be attributed to low oocyte num-ber, abnormal oocyte morphology, or fragile oocytes which are easily damaged by the trauma of the injec-tion. Fertilization rates using epididymal and testicular sperm are equivalent to those for ejaculated sperm, but the use of immature sperm cells results in a dramatic decrease in fertilization and pregnancy rates. Th e most common cause of failed fertilization in ICSI is due to highly elastic plasma membranes and diffi culty in rupturing the oocyte membrane: essentially you have not placed the spermatozoon in the cytoplasm of the oocyte. Figure 13.4 shows the variations that can be seen on Day 1 aft er ICSI.
Transport ICSI In the same manner that nearby peripheral hospitals or clinics can use a central IVF laboratory to off er assisted conception treatment, a central ICSI labora-tory can off er this specialized technique to peripheral hospitals that do not have the equipment or expert-ise. Preovulatory oocytes and prepared sperm from patients are transported from the peripheral unit by the male partner immediately aft er the oocyte recovery procedure. Culture tubes containing the gametes are transported in a portable incubator, as described for transport IVF in Chapter 11 . On arrival at the central unit, the oocytes can be transferred to culture dishes and prepared for the ICSI procedure, and sperm prep-aration assessed and adjusted if necessary. Fertilized
1. All conditions must be stable: temperature, pH, equipment properly set up, adjusted, aligned, and checked for leaks and air bubbles. Check every-thing, including secure and comfortable operating position, before you begin.
2. Correct immobilization of sperm . 3. Advance far enough into the ooplasm with the
injection pipette. 4. Ensure that the plasma membrane is broken
(immediate membrane rupture after introducing the injection needle results in a lower probability of fertilization).
5. Inject a minimal volume. 6. If the sperm comes out of the ooplasm into the
perivitelline space, reinject.

Chapter 13: Micromanipulation techniques
226
oocytes are cultured to the early cleavage stage, and the embryos may then be transported by the male partner back to the peripheral unit for the embryo transfer procedure. Supernumerary embryos may also be cryopreserved at the central unit if appropriate. As with transport IVF, cooperation between participating units is particularly important in order to provide an eff ective service. Well-planned protocols are essential for selection, consultation and counseling of patients, the handling, preparation and transport of gametes, and communication of treatment cycle details/trans-port arrangements between units.
IMSI – intracytoplasmic morphologically selected sperm Sperm morphology has long been accepted as one of the best indicators for a positive outcome in human fer-tilization, whether via natural fertilization, IUI, IVF or ICSI. More recently, IMSI, a more strict technique for selecting “normal sperm,” has been shown to improve pregnancy rates and decrease abortion rates, at least in some patient categories. Th is procedure, originally promoted by Bartoov and colleagues ( 2003 ), consists of real time, high magnifi cation, motile sperm organellar morphology examination (MSOME) that uses 24 char-acteristics to defi ne the normal morphology of seven sperm organelles: acrosome, post-acrosomal lamina, neck, mitochondria, tail, outer dense fi bers and the
nucleus. MSOME is performed with an inverted light microscope equipped with high-power Nomarski optics enhanced by digital imaging that allows the embryolo-gist to magnify sperm up to 6000 times, compared to the traditional 400 times with ICSI. Figure 13.5 shows IMSI photographs of a single normal human spermato-zoon and a selection of dysmorphic spermatozoa.
Patient selection for IMSI Potentially all males with severe oligospermia and samples dissected from the testicles (TESE) can benefi t from application of IMSI .
Equipment and materials for IMSI IMSI requires a standard ICSI micromanipulator with two modifi cations: 1. In order to use a higher magnifi cation objective,
ranging from ×60 in air to ×100 with oil immersion, sperm observation and selection must be carried out using glass-bottomed dishes or slides of 0.17 mm thickness .
2. Since the specimens must be observed on a glass surface, the Hoff man modulation contrast optics used in ICSI is replaced by Nomarski optics.
Th e optical signal is then enhanced by a video zoom and digital imaging system, giving a fi nal magnifi ca-tion of up to ×10 000. Th e image is observed, stored
Figure 13.4 Diagrams showing varia-tions of fertilization after ICSI. PN: pro-nuclei; PB: polar body; (a) two pronuclei, two polar bodies; (b) three pronuclei, one polar body; (c) one pronucleus, two polar bodies; (d) no pronuclei, one polar body; (e) early cleavage (with thanks to Gian franco Coppola).

Chapter 13: Micromanipulation techniques
227
Figure 13.5 IMSI: A single normal human spermatozoon showing true dimensions in μm, and a selection of dysmorphic spermatozoa. Nomarski optics at ×6000 magnifi cation.
and analyzed using specifi c soft ware supplied by the microscopy company.
Procedure Th e type of injection dish is the most important criter-ion for IMSI. Since sperm identifi cation and selection is made on glass with Nomarski optics, and the injection procedure is usually carried out in plastic dishes with Hoff man optics, special glass-bottomed dishes have been designed so that the two procedures may be car-ried out in the same dish. In this case, the operator uses Nomarski Diff erential Interference Contrast (DIC) for the injection procedure. Tissue culture medium, PVP, paraffi n oil and microtools remain unchanged .
Assisted hatching (AH) Cohen and colleagues postulated in the 1990s that the inability of blastocysts to hatch from the zona pellucida may be one of the factors involved in the high implant-ation failure rate of human IVF procedures. Th e human zona becomes more brittle and loses its elasticity aft er fertilization, and spontaneous hardening also occurs aft er in-vitro and in-vivo aging. Th e zona also changes in its sensitivity to low pH, so that it is easier to create a hole with acid Tyrode’s solution in a zygote than in an unfertilized oocyte. Early observations from video cinematography studies suggested that embryos with a thick, even zona pellucida on Day 2 had a poor prog-nosis for implantation (see Chapter 11 ). In addition, embryos produced as a result of microsurgical fertil-ization had a higher implantation rate, and hatched one
day earlier than expected (Day 5 instead of Day 6) aft er in-vitro culture. Original trials on AH were performed on Day 2 embryos, but studies by Dale and colleagues in Naples (Dale et al ., 1991 ; Gualtieri et al ., 1992 ) on the formation of intercellular junctions and, in particular tight junctions and desmosomes, indicated that Day 3 was a more suitable time for AH. Following these obser-vations, a series of experiments in a mouse embryo sys-tem led to the development of a clinical protocol, with the following notable features : 1. Large holes are more effi cient in supporting
hatching than small holes: if the hole is too small, the embryo can become “trapped” and fail to hatch. Zona drilling using an acid Tyrode’s solution prevented “trapping” which occurred as a result of mechanical partial zona drilling: optimal hole size is approximately half the size of a single blastomere, 15–20 μm.
2. Embryos with these large gaps in their zonae should be transferred aft er the onset of compaction, on Day 3: if embryo transfer is traumatic, blastomeres may escape through the gap in the zona. Embryo transfer must therefore be gentle and atraumatic.
3. Embryos must be preselected for assisted hatching, based upon previous IVF history (repeated failed implantation), maternal age, basal FSH levels, cleavage rates and morphology of the embryos with attention to zona thickness or variation.
Laser assisted hatching Successful assisted hatching can be carried out with the use of a 1.48 mm diode laser (FertilaseTM, MTG, Germany); a few milliseconds of laser irradiation instantly makes an opening in the zona pellucida , and apertures ranging from 3 to 25 μm can be obtained. Th e procedure has been shown to be safe, simple and rapid. However, the equipment is expensive, and zona drilling with acid Tyrode’s solution can also be used ( Figure 13.6 ).
Acid Tyrode’s protocol Th e protocol below for assisted hatching by acid drilling of the zona pellucida is adapted from J. Cohen (2007).
Tyrode’s solution is acidifi ed by titrating to pH 2.3–2.5 with HCl. 1. Perform zona drilling with acid Tyrode’s (AT)
solution approximately 72 hours aft er oocyte retrieval, with embryo transfer 5–7 hours later

Chapter 13: Micromanipulation techniques
228
(i.e., drill before the formation of intercellular connections, but transfer aft er they have been established).
2. Perform the procedure in HEPES-buff ered human tubal fl uid (HTF) medium with 15% human serum
albumin or other protein supplement (e.g., SPS, Sage).
3. Use a straight microtool with an aperture of 10–12 µm.
4. Embryos are held in small microdroplets (25 µL) under mineral oil in a depression slide or shallow Falcon 1006 dish containing one droplet of AT solution and four wash droplets .
5. Micromanipulate each embryo individually, and immediately wash each embryo three to four times to remove the acidic medium.
AH with acid Tyrode’s, step-by-step Th e key to successful assisted hatching is to prod-uce a gap in the zona without exposing the embryo to acidifi ed solution. Aspirating AT solution through a needle of very small diameter leaves consider-able negative pressure within the needle aft er it is removed from the AT droplet, and this will result in culture medium being aspirated as soon as the needle enters the embryo culture droplet. Th is will dilute the AT solution, making it ineff ective for dissolving the zona pellucida. In order to avoid this technical prob-lem, the system should be prepared well in advance, so that the hatching needle will be precisely in the correct position relative to the embryo as soon as it is lowered into the droplet of medium. Applying slight positive pressure as soon as the needle breaks the surface of the drop will also help to counteract the residual suction. 1. Front load the microneedle with AT solution
before each hatching event; the meniscus of the acidic fl uid is diffi cult to control, and therefore precisely controlled suction is important .
2. Pre-align the embryo onto the holding pipette (syringe suction system) so that the AT-fi lled microneedle at the 3 o’clock area is exposed to empty perivitelline space or to extracellular fragments.
3. When the embryo is in position on the holding pipette, lower the AT-fi lled needle into the medium and bring it next to the target area as quickly as possible. In order to avoid diluting the AT solution with medium of normal pH, there should be no more than a 2-second delay before the hatching begins: releasing fl uid that is not suffi ciently acidic will damage the embryo, without aff ecting the zona pellucida.
(a)
Figure 13.6 Assisted hatching. (a) Laser-hatched four-cell embryo. (See color plate section) (b) Assisted hatching with acid Tyrode’s.
(b)

Chapter 13: Micromanipulation techniques
229
4. Expel acidic medium gently over a small (30 µm) area by holding the needle tip very close to the zona; using small circular motions can avoid excess acid in a single area. Th e circular motions should create a hole that is nearly rectangular.
5. If thinning is not immediately obvious, stop the procedure immediately: the total time required to breach the zona should not exceed a couple of seconds; most zona will yield within less than 5 seconds.
6. Th e inside of the zona is more diffi cult to pierce, and the expulsion pressure may need to be increased. Th e optical system should be optimized for this part of the procedure, as the stream of acid may be relatively invisible, and the piercing of the inside of the zona may be almost imperceptible. Zona breakthrough should cover an area of at least 20 μm, and not a single small point.
7. As soon as the zona is breached, reverse the fl ow through the AH needle immediately. All of the expelled acid solution must be aspirated, paying particular attention to any solution that might have entered the PVS. Move the embryo to another area of the droplet, away from excess AT.
8. A small “inside” hole may be widened mechanically by moving the microneedle through the opening in a tearing motion while continuing gentle suction.
9. Carefully transfer the embryo through the wash droplets, and return to culture for incubation prior to embryo transfer.
Polar body or blastomere biopsy Th e next chapter will discuss the genetic and chromo-somal analysis of cells biopsied from oocytes (the polar body), cleavage stage embryos and blastocysts. Th e standard equipment used for embryo biopsy is a slightly modifi ed ICSI apparatus, with specifi c microtools. Biopsy is carried out in two stages: the zona pellucida must be breached, and then the cells are aspirated.
Th e optimal time for embryo biopsy is before strong intercellular junctions are formed, which is usually Day 3. Biopsy is extremely diffi cult with com-pacted embryos, and cleavage stage embryos should be incubated in Ca/Mg-free media to facilitate the biopsy procedure. To avoid contamination with extracellular sperm that could be attached to the zona, it is import-ant that the oocytes are fertilized using ICSI. A variety
of techniques can be used to carry out the biopsy, as described below. A hole in the zona can be created mechanically (as in PZD ), using a laser, or by drilling with AT solution. If using AT drilling, the AT should fi rst be prewarmed to 37°C; a pipette of 8–10 µL con-taining AT is placed adjacent to the zona pellucida and the solution expelled from the pipette until the zona thins and eventually breaches. Th e cell is then moved away from any excess AT. For biopsy, a second micro-pipette, fi re-polished with an inner diameter of 30–40 µm) is used to aspirate the blastomere. Th e pipette is pushed through the breach in the zona and, by gentle aspiration, the cell drawn up into the pipette. When the cell is clearly free from the embryo, the pipette is moved sideways and the cell expelled. If the cell lyses, another cell should be aspirated.
Cleavage stage biopsy techniques Th e totipotency of cleavage stage blastomeres ensures
that removal of a small number for diagnosis does not aff ect the ability of the remainder to compensate and thus adequately diff erentiate to all required cell lineages on development (see more on this subject in Chapter 7 ).
Aspiration ( Figure 13.7a ) Th e biopsy micropipette is used like a needle to punc-ture the zona pellucida of an embryo held in place with a holding micropipette. A blastomere is then removed by suction into an aspiration micropipette. Th e zona may also be punctured by administering AT solution to a limited spot on the surface or by using a sharpened dissection pipette or a laser to drill a hole in the zona.
Extrusion (a) Stitch and pull ( Figure 13.7b )
Th is method involves initial zona drilling with either a laser or acid Tyrode’s to create a hole. A stitching move-ment with the microneedle is then used to displace and remove a blastomere which is then pushed out of the incision by pushing the zona with a microneedle at a distance from the hole.
(b) Displacement ( Figure 13.7c )
A beveled pipette is used to make the fi rst incision in the zona. A second incision is then made through which one blastomere is displaced by applying a gen-tle fl ow of medium, causing the blastomere to emerge from the fi rst incision site .

Chapter 13: Micromanipulation techniques
230
Typical clinical protocol for cleavage stage embryo biopsy for PGD
Day 1 (1 day after oocyte collection) 1. Set up culture dishes (one for each normally
fertilized embryo): Label a four-well dish (Nunclon) with the patient’s name and embryo number on the base of the dish and on the front panel. Put 0.5 mL of cleavage stage or blastocyst culture medium in each well and cover with a monolayer of washed oil. Place the dishes in the incubator to equilibrate overnight.
Day 2 (2 days after oocyte collection)
2. After scoring the embryos, transfer each embryo into blastocyst culture medium in well 1 of the appropriately labeled four-well dish, wash and transfer to well 2 and transfer to the incubator for overnight culture. The timing of the switch between cleavage stage and blastocyst culture media may diff er depending on the medium used.
3. In the warming oven, place 10 mL of HEPES-buff ered biopsy medium (Ca 2+ /Mg 2+ -free) and Falcon dishes (1006) for the biopsy. In the incubator, place enough washed oil for the biopsy procedure (allow 4 mL per embryo).
Day 3 (day of embryo biopsy)
4. Half an hour before the biopsy : (a) Set up a biopsy dish (1006 Falcon) for each
embryo and label it with the patient’s name and embryo number. Take a Gilson pipette set at 10 µl and a sterile yellow tip and fl ush the tip (×10) with the HEPES-buff ered biopsy medium. Pipette three drops of HEPES-buff ered biopsy medium and one drop of AT as shown in Figure 13.8 – it is important that the dish is oriented as shown in relation to the “bumps” on the outside of the dish. Immediately cover the dish with 4 mL of washed and pre-equilibrated oil to avoid evaporation and put the prepared dishes in the warming oven until required.
Day 1 (1 day after oocyte collection) 1. Set up culture dishes (one for each normally
fertilized embryo): Label a four-well dish (Nunclon)with the patient’s name and embryo number onthe base of the dish and on the front panel. Put0.5 mL of cleavage stage or blastocyst culturemedium in each well and cover with a monolayerof washed oil. Place the dishes in the incubator toequilibrate overnight.
Day 2 (2 days after oocyte collection)
2. After scoring the embryos, transfer each embryointo blastocyst culture medium in well 1 of theappropriately labeled four-well dish, wash andtransfer to well 2 and transfer to the incubatorfor overnight culture. The timing of the switchbetween cleavage stage and blastocyst culturemedia may diff er depending on the mediumused.
Figure 13.7 Cleavage stage biopsy techniques: (a) aspiration; (b) stitch and pull; (c) displacement.
(a) (b)
(c)
3. In the warming oven, place 10 mL of HEPES-buff eredbiopsy medium (Ca 2+ /Mg2+ -free) and Falcon dishes(1006) for the biopsy. In the incubator, place enoughwashed oil for the biopsy procedure (allow 4 mL perembryo).
Day 3 (day of embryo biopsy)
4. Half an hour before the biopsy : (a) Set up a biopsy dish (1006 Falcon) for each
embryo and label it with the patient’s nameand embryo number. Take a Gilson pipette setat 10 µl and a sterile yellow tip and fl ush the tip(×10) with the HEPES-buff ered biopsy medium.Pipette three drops of HEPES-buff ered biopsymedium and one drop of AT as shown in Figure13.8 – it is important that the dish is oriented asshown in relation to the “bumps” on the outsideof the dish. Immediately cover the dish with 4mL of washed and pre-equilibrated oil to avoidevaporation and put the prepared dishes in thewarming oven until required.

Chapter 13: Micromanipulation techniques
231
Biopsy medium
Acid Tyrode’s
Figure 13.8 Biopsy dish for PGD.
(b) Set up a four-well dish for transferring the embryos into biopsy medium with 0.5 ml of HEPES-buff ered biopsy medium in each of the wells, cover with oil and place in the warming oven.
5. About 15 minutes before each biopsy, take the appropriately labeled biopsy dish and the four-well transfer dish from the warming oven and care-fully wash successive embryos through each well of HEPES-buff ered medium , transferring minimal medium between wells. Leave the embryo in each well for at least 1 minute: it is essential to completely remove the divalent cations from the culture medium to promote the reversal of any compaction. Place the embryo into the middle of the three droplets in the biopsy dish (the two other droplets are spare in case of diffi culties dur-ing biopsy).
6. Biopsy cells. 7. At the end of the biopsy procedure, transfer the
embryo into well 3 of the four-well culture dish – this is a washing stage to remove the HEPES-buff ered biopsy medium . Finally, transfer the embryo with minimal medium to well 4 and return to culture .
8. Return the biopsy dish with the isolated blast-omeres to the fl ow hood for sample preparation.
9. Repeat until all of the embryos have been biopsied.
10. When the PGD analysis result is available, assess the morphology of each embryo and count the number of cells as accurately as possible to get an indication of division post biopsy.
11. In consultation with the other members of the PGD team and fi nally with the couple them-selves, select a maximum of two genetically unaff ected embryos with the best morphology for transfer.
Blastocyst stage biopsy Th e advantage of blastocyst biopsy is that a lar-ger number of cells can be removed from the outer trophectoderm layer without aff ecting the inner cell mass from which the fetus later develops. However, trophectoderm cells (TE) may have diverged gen-etically from the inner cell mass (ICM), as confi ned placental mosaicism, observed in at least 1% of con-ceptions: the chromosome status of the embryo dif-fers from that of the placenta. Recent studies have indicated that blastocysts may have high levels of chromosomal mosaicism. Preferential allocation of abnormal cells to the TE may be a mechanism of early development; in this case the TE would not be rep-resentative of the rest of the embryo, which would complicate and compromise PGD. Blastocyst biopsy may be performed using stitch and pull, aspiration, and herniation techniques.
Aspiration ( Figure 13.9a ) A number of cells are sucked from the mural troph-ectoderm cell layer opposite to the inner cell mass, through the aspiration micropipette. Th e microneedle is also used to break cell–cell contacts as the TE cells herniate through the hole .
Extrusion technique ( Figure 13.9b ) Partially dissolve a section of the zona with AT solution or with a laser, and use two siliconized glass micronee-dles to extrude mural TE cells with a stitch and pull motion through the zona.
Herniation Make a tear in the zona opposite the inner cell mass, and leave the embryos for several hours until a hernia-tion of the mural TE can be seen. Remove the emerging cells by cutting with a glass needle or scalpel blade. Th e incubation time required means that this method is less useful for transfer in the same cycle .
Polar body biopsy Since the oocyte of a carrier contains either the abnor-mal or normal gene for a particular genetic disorder, analysis of the status of the gene from the polar body (PB) will indirectly determine which gene is present in the oocyte. However, for analysis of single gene and chromosomal defects, recombination events during

Chapter 13: Micromanipulation techniques
232
meiosis I require biopsy and analysis of PB2 to con-fi rm which allele is present in the zygote. Both polar bodies can be removed together aft er fertilization ( Figure 13.10 ), or PB1 can be removed before, and PB2 aft er fertilization.
Method 1. Immobilize the oocyte using a holding pipette. 2. Insert a beveled micropipette (12–15 μm
diameter) through the zona to the perivitelline space and aspirate the polar body into the pipette as it detaches from the ooplasm; a breach in the zona can also be created with the use of a laser. Th e two polar bodies are distinguished by morphology, the fi rst having a crinkly appearance and the second being smooth, possibly with a visible interphase nucleus under interference contrast.
Appendix Equipment for ICSI For microinjection Dissecting microscope with heated stage Inverted microscope with heated stage, attached to micromanipulators
×4 objective for locating oocytes and drops ×20 or ×40 objective for microsurgery ×15 eyepiece Hoff man modulation contrast optics Video monitoring facility
Bilateral micromanipulators for manipulation in three dimensions Microtool holders Two suction devices with steel syringes (80–100 mL) fi lled with light mineral oil (BDH), or appropriate alternative device for controlling holding and injection micropipettes Incubator Supply of 5% CO 2 in air.
Supplies Shallow Falcon Petri dishes (Type 1006) Culture medium Culture medium + HEPES Human serum albumin (HSA) Hyaluronidase solution Mineral oil PVP solution Pasteur pipettes Hand-pulled polished glass pipettes
(a) (b)
(c)
Figure 13.10 Polar body biopsy. (a) Position the polar bodies at 5–6 o’clock position, and penetrate the zona with the biopsy pipette. (b) Gently aspirate the polar bodies from under the zona pellucida. (c) Expel the polar bodies into the medium and remove the biopsied zygote from the biopsy medium.
Figure 13.9 Blastocyst biopsy techniques: (a) aspiration; (b) stitch and pull.
Microneedle
TE
(a)
ICM
Aspirationmicropipette
Cells sucked intomicropipette whilecell contacts are cut
Microneedle
(b)
ICM
Acid Tyrode’sweakened zona
Trophectoderm cells removedusing stitching movement

Chapter 13: Micromanipulation techniques
233
Pipette bulbs Holding pipettes
ICSI needles.
Adjustment of manipulators for ICSI (with thanks to Terry Leonard) Th is guide refers to the Nikon/Narishige system; the same principles apply to an Olympus system, but the details are slightly diff erent. Before attempting to fi t or adjust the micromanipulators, fi rst adjust the micro-scope optically, ideally using an oocyte in the same type of Petri dish to be used for ICSI. Th e microscope set-tings will infl uence the working distance of the micro-tools. Th e fi nal position of the micromanipulators on the microscope will depend upon: (a) the angle at which the tool holder is fi xed (b) the combined length of the tool holder and needle
from the point where it is held in the tool holder attachment to the center of the light source.
Before fi nding the ideal position for the microman-ipulators, they should be fi tted correctly to the micro-scope, and fi nal adjustments made later.
Micromanipulator parts
1. Mounting bar: this joins the coarse manipulator to the microscope.
2. Coarse manipulator: consists of three parts, each controlling one of the three dimensions of movement. Th ere are two types: manually operated and motor driven.
3. Fine manipulator: consists of two parts: (a) the driving section: attached to the coarse
manipulator, controls fi ne movements directed by joystick.
(b) ball joint/tool holder attachment: attached to the driving section, used both to hold the microtool holder and to vary the angle at which it is held.
4. Joystick: links to the driving section via oil-fi lled tubes. Th e movement of the joystick is scaled down and transferred to the fi ne manipulator.
Th e mounting arrangement which attaches the coarse manipulator to the microscope is L-shaped. In the Nikon/Narishige system, the mounting is fi tted to the illumination pillar .
Th e mounting bar position is marked with a white • L-shape.
Th e mounting bars have tracks into which the • coarse manipulator fi ts, and the position of the coarse manipulator can be adjusted along these tracks. Th e entire mounting bar can be adjusted up and down.
Adjusting the coarse manipulators 1. Set the mounting bars at 90 degrees from the
microscope stage or bench top. 2. Set the second part of the mounting at 90 degrees
to the fi rst, and ensure that the track is set fl at. 3. Attach the coarse micromanipulator and adjust
the lower section (left /right movement) so that it is parallel with the mounting bar. Set the other two sections of the coarse manipulator at right angles to each other.
Attaching the fi ne manipulator Th e fi ne manipulator is attached to the coarse manipu-lator by a small metal rod (coupling bar). Th is can be screwed into one of the two holes on the driving sec-tion of the fi ne manipulator, depending on the side on which it is to be used. In order to fi t the fi ne manipu-lator on the right hand side, fi nd the “R” mark on the driving section and screw the coupling bar into the hole directly behind this mark. Attach the coupling bar/driving section to the coarse manipulator and tighten. Position the driving section so that it is parallel with the microscope or 90 degrees to the bench. Attach the left hand side in the same manner, screwing the coupling bar into the hole directly behind the “L” mark. Arrange the joysticks so that the “R” and “L” marks are facing the operator on the appropriate sides .
Attaching the ball joint/tool holder attachment Th e ball joint/tool holder attachment has a black metal bar projecting from it. Th is is fi tted into the V-groove of the driving unit. Th e ball joint is then rotated to an appropriate angle so that when a needle is held in it, the tip of the microtool will be parallel with the microscope stage. Th e extent to which it is rotated will depend upon the angle at which the microtool is bent. For example, for a microtool which is angled at 35 degrees from the plane of the needle, the ball joint must be rotated 35 degrees anticlockwise from the vertical position.
Th e manipulators should now be attached in the correct manner, but they may not be in the optimal working position. Th e ideal position will vary depend-ing upon the angle of the needle and the combined length of the microtool and tool holder. It is therefore

Chapter 13: Micromanipulation techniques
234
best to have a fi xed tool angle, a fi xed length of pro-jection of the tool from the tool holder, and a fi xed (marked) point where the tool holder is clamped to the tool holding attachment. If any of these three factors change, the fi ne adjustments will require resetting .
Finding the best position for the micromanipulators Adjust the three coarse manipulators so that they • are in the middle of their range of movements. Adjust the range of movements of the three fi ne • manipulators on the joystick so that they are in the middle of the scales.
Forward/backward movement First ensure that the hole in the stage is positioned dir-ectly in the middle of the light path. View the micro-manipulator from the side of the microscope, then align the tool holder attachment with the middle of the hole in the microscope stage. Th is can be adjusted by changing the position of the coupling bar on the fi ne manipulator, the projection from the ball joint, or the two screws on the very top of the coarse manipulator which controls the forward/backward movement.
Left/right movement Place a microtool holder together with a microtool in the tool holder attachment. Attach it at the very tip of the tool holder, and gently slide it along towards the light source. If it will not reach the light source, the entire manipulator should be moved to the left . Likewise, if it reaches it too soon (before the marked point) the entire manipulator should be shift ed to the right. Th is adjust-ment is performed by loosening the bolts that attach the coarse micromanipulator to the mounting bar. Aft er this adjustment, ensure that the micromanipulator is still parallel to the bar .
Up/down movement Adjust the manipulator so that the microtool is approxi-mately 0.5 cm from the surface of the stage. For large adjustments loosen the bolts that attach the mounting bar to the microscope and move up or down. Remember to ensure that it is still 90 degrees from the bench aft er adjustment. Fine up/down adjustments can be made by moving the small sliding section above the ball joint.
Alignment of the ICSI needle in the manipulator When using a Narishige tool holder, push the needle in so that 4–5 cm of the needle is outside the holder.
Place the tool holder in the right hand micromanipula-tor with the needle tip over the light source. Th e angle at which the tool holder is held should be such that the angled tip of the needle is parallel with the stage of the microscope. Under a very low power (×4 objective), place the tip of the ICSI needle in the fi eld of vision of the microscope. Loosen the tool holder attachment and rotate the tool holder so that the bent portion of the needle appears to be straight. Ensure that you can focus on a good portion of the needle (from the tip). Th e portion of the needle aft er the bend will be out of focus. If the microscope has a graticule, make sure that the movement of the needle from right to left does not vary. Place the ICSI needle along the middle of the microscope fi eld with the tip almost in the center. Align the holding pipette in the same manner so that the tips of the needle and pipette are facing each other, and then raise them up away from the stage .
Perform the fi nal adjustment of the angle at which the tool holder is held within a sperm droplet. Find a nonmotile sperm and then bring the ICSI needle into the same optical plane. Raise the ICSI needle off the surface of the Petri dish very slightly, move it over the top of the sperm, and try to touch the sperm by lower-ing the needle. If it is impossible to touch the sperm, the needle is not parallel with the surface. Th e end of the needle will be lower than the tip. To rectify this, raise the needle and rotate the ball point anticlockwise slightly, lower the needle, and try to touch the sperm again. If the tip of the needle can touch the sperm, but the rest of the needle is not in focus, the tip of the needle is lower than the bend. To rectify this, raise the needle and rotate the ball joint slightly in a clockwise direction.
Ratio of movement and joysticks 1. Focus on the tip of the microtool. 2. Loosen the two screws on the movement
adjustment rings. 3. Ignore the ratios written on the side of the joystick,
and rotate the adjustment rings anticlockwise until you are satisfi ed with the movement as observed down the microscope .
When all of the adjustments and alignments are made, the need to repeat any of these should be minimal, unless the style of the needle or tool holder is changed. When removing the tool holder from its attachment, keep the ball joint at the same angle so that when a new needle is inserted, it will be at approximately the right

Chapter 13: Micromanipulation techniques
235
angle for use. Fine adjustments will be necessary for each manipulation.
Further reading Useful websites ICSI, follow-up and risks: www.ivfctrstl.org/icsi-safe.htm,
www.advancedfertility.com/icsirisks.htm Micromanipulation images: www.ivf.net/ivf/
micromanipulation-b338_0-en.html
Micromanipulation tools: www.zdlinc.com/icsi_tools.htm
Publications Antinori S , Versaci C , Dani G , et al . ( 1997 ) Successful
fertilization and pregnancy aft er injection of frozen-thawed round spermatids into human oocytes . Human Reproduction 12 : 554 –556.
Barak Y , Ménézo Y , Veiga A , Elder K ( 2001 ) A physiological replacement for polyvinylpyrrolidone (PVP) in assisted reproductive technology . Human Fertility 4 : 99 –103.
Bartoov B , Berkovitz A , Eltes F , et al. ( 2003 ) Pregnancy rates are higher with intracytoplasmic morphologically selected sperm injection than with conventional intracytoplasmic injection . Fertility and Sterility 80 (6): 1413 –1419.
Bonduelle M , Aytoz A , Wilikens A , et al . ( 1998 ) Prospective follow-up study of 1,987 children born aft er intracytoplasmic sperm injection (ICSI). In: Filicori M , Flamigni C (eds.) Treatment of Infertility: Th e New Frontiers . Communication Media for Education , Princeton Junction, NJ , pp. 445–461.
Bonduelle M , Schrijver F De , Haentjens P , Devroey P , Tournaye H ( 2008 ) Neonatal data on 530 children born aft er ICSI using testicular spermatozoa. In: Abstracts of the 24th Annual Meeting of the ESHRE , Barcelona , Spain .
Bowen JR , Gibson FL , Leslie GI , Saunders DM ( 1998 ) Medical and developmental outcome at 1 year for children conceived by intracytoplasmic sperm injection . Lancet 351 : 1553 –1562.
Burmeister L , Palermo GD , Rosenwaks Z ( 2001 ) IVF: the new era . International Journal of Fertility and Women’s Medicine 46 (3): 137 –144.
Chatzimeletiou K , Morrison EE , Panagiotidis Y , et al. ( 2005 ) Comparison of eff ects of zona drilling by non-contact infrared laser or acid Tyrode’s on the development of human biopsied embryos as revealed by blastomere viability, cytoskeletal analysis and molecular cytogenetics . Reproductive Biomedicine Online 11 (6): 697 –710.
Cohen J ( 1991 ) Assisted hatching of human embryos . Journal of In Vitro Fertilization and Embryo Transfer 8 (4): 179 –189.
Cohen J ( 2007 ) Manipulating embryo development. In: Elder K , Cohen J (eds.) Preimplantation Embryo Evaluation and Selection . Informa Press , London , pp. 135–144.
Cohen J , Alikani M , Trowbridge J , Rosenwaks Z ( 1992 ) Implantation enhancement by selective assisted hatching using zona drilling of embryos with poor prognosis . Human Reproduction 7 : 685 –91.
Combelles CM ( 2008 ) What are the trade-off s between one-cell and two-cell biopsies of preimplantation embryos . Human Reproduction 23 (3): 493 –498.
Cummins JM , Jequier AM ( 1995 ) Concerns and recommendations for Intracytoplasmic sperm injection (ICSI) treatment . Human Reproduction 10 (Suppl. 1): 138 –143.
Dale B , Gualtieri R , Talevi R , et al. ( 1991 ) Intercellular communication in the early human embryo . Molecular Reproduction and Development 29 : 22 –28.
DeFelici M , Siracusa G ( 1982 ) “Spontaneous” hardening of the zona pellucida of mouse oocytes during in vitro culture . Gamete Research 6 : 107 –112.
de Vos A , Van Steirteghem A ( 2001 ) Aspects of biopsy procedures prior to preimplantation genetic diagnosis . Prenatal Diagnosis 21 (9): 767 –780.
ESHRE ( 2008 ) Good Clinical Treatment in Assisted Reproduction: ESHRE position paper, June 2008. Available online at: www.eshre.eu/ESHRE/English/Guidelines-Legal/ESHRE-Position-Papers/page.aspx/942 .
Fleming SD , Ilad RS , Griffi n A-M G , et al. ( 2008 ) Prospective controlled trial of an electrophoretic method of sperm preparation for assisted reproduction: comparison with density gradient centrifugation . Human Reproduction 23 (12): 2646 –2651.
Germond M , Nocera D , Senn A , et al. ( 1995 ) Microdissection of mouse and human zona pellucida using a 1.48 m diode laser beam: effi ciency and safety of the procedure . Fertility and Sterility 25 : 604 –611.
Gianaroli L , Magli MC , Selman HA , et al . ( 1999 ) Diagnostic testicular biopsy and cryopreservation of testicular tissue as an alternative to repeated surgical openings in the treatment of azoospermic men . Human Reproduction 14 : 1034 –1038.
Gianaroli L , Magli MC , Collodel G , et al. ( 2008 ) Sperm head’s birefringence: a new criterion for sperm selection . Fertility and Sterility 90 (1): 104 –112.
Goossens V , De Rycke M , De Vos A , et al. ( 2008 ) Diagnostic effi ciency, embryonic development and clinical outcome aft er the biopsy of one or two blastomeres for preimplantation genetic diagnosis . Human Reproduction 23 (3): 481 –492.
Gualtieri R , Santella L , Dale B ( 1992 ) Tight junctions and cavitation in the human pre-embryo . Molecular Reproduction and Development 32 : 81 –87.

Chapter 13: Micromanipulation techniques
236
Hamberger L , Sjögren A , Lundin K ( 1995 ) Microfertilization techniques: choice of correct indications. In: Hedon B , Bringer J , Mares P (eds.) Fertility and Sterility: A Current Overview . IFFS-95, Parthenon Publishing Group , New York , pp. 405–408.
Hardy K , Wright C , Rice S , et al. ( 2000 ) Future developments in assisted reproduction in humans . Reproduction 123 (2): 171 –183.
Harper J (ed.) ( 2009 ) Preimplantation Genetic Diagnosis , 2nd edn. Cambridge University Press .
Hiramoto Y ( 1962 ) Microinjection of the live spermatozoa into sea urchin eggs . Experimental Cell Research 27 : 416 –426.
Hirsch A ( 2007 ) Th e investigation and treatment of the infertile male: pathophysiology and principles of treatment. In: Brinsden P (ed.) A Textbook of In Vitro Fertilization and Assisted Reproduction , 3rd edn. Parthenon Publishing Group , London .
Huszar G , Jakab A , Sakkas D , et al. ( 2007 ) Fertility testing and ICSI sperm selection by hyaluronic acid binding: clinical and genetic aspects . Reproductive Biomedicine Online 14 (5): 650 –663.
Jequier AM ( 1986 ) Infertility in the Male: Current Reviews in Obstetrics and Gynaecology . Churchill Livingstone , Edinburgh .
Kent-First M , Kol S , Muallem A ( 1996 ) Infertility in intracytoplasmic sperm injection derived sons . Lancet 348 : 332 .
Kim ED , Bischoff FZ , Lipshultz LI , Lamb DJ ( 1998 ) Genetic concerns for the sub-fertile male in the era of ICSI . Prenatal Diagnosis 18 : 1349 –1365.
Kobayashi K , Mizuno K , Hida A ( 1994 ) PCR analysis of the Y chromosome long arm in azoospermic patients: evidence for a second locus required for spermatogenesis . Human Molecular Genetics 3 : 1965 –1967.
Kurinczuk J ( 1997 ) Birth defects in infants conceived by intracytoplasmic sperm injection: an alternative interpretation . British Medical Journal 315 : 1260 –1265.
Leunens L , Celestin-Westreich S , Bonduelle M , Liebaers I Ponjaert-Kristoff ersen I ( 2008 ) Follow-up of cognitive and motor development of 10-year-old singleton children born aft er ICSI compared with spontaneously conceived children . Human Reproduction 23 : 105 –111.
Lillie FR ( 1914 ) Studies of fertilisation IV. Th e mechanism of fertilization in Arbacia . Journal of Experimental Zoology 16 : 523 .
Longo FJ ( 1981 ) Changes in the zonae pellucidae and plasmalemmae of ageing mouse eggs . Biological Reproduction 25 : 299 –411.
Nagy ZP , Liu J , Joris H , Devroey P , Van Steirteghem A ( 1993a ) Intracytoplasmic single sperm injection of 1-day old unfertilized human oocytes . Human Reproduction 8 : 2180 –2184.
Nagy ZP , Liu J , Joris H , Devroey P , Van Steirteghem A ( 1993b ) Time-course of oocyte activation, pronucleus formation and cleavage in human oocytes fertilized by intracytoplasmic sperm injection . Human Reproduction 9 : 1743 –1748.
Nagy ZP , Janssenswillen C , Silber S , Devroey P , Van Steirteghem AC ( 1995 ) Using ejaculated, fresh, and frozen-thawed epididymal and testicular spermatozoa gives rise to comparable results aft er intracytoplasmic injection . Human Reproduction 9 : 1743 –1748.
Oates RD , Cobl SM , Harns DH , et al. ( 1996 ) Effi ciency of ICSI using intentionally cryopreserved epididymal sperm . Human Reproduction 600 : 133 –138.
Palermo G , Joris H , Devroey P , Van Steirteghem AC ( 1992 ) Pregnancies aft er intracytoplasmic injection of single spermatozoon into an oocyte . Lancet 340 : 17 –18.
Palermo G , Joris H , Derde M-P , et al. ( 1993 ) Sperm characteristics and outcome of human assisted fertilization by subzonal insemination and intracytoplasmic sperm injection . Fertility and Sterility 59 : 826 –835.
Qureshi SJ , Ross AR , Ma K , et al. ( 1996 ) Polymerase chain reaction screening for Y chromosome microdeletions: a fi rst step towards the diagnosis of genetically-determined spermatogenic failure in men . Molecular Human Reproduction 2 (10): 775 –779.
Safran A , Reubinoff E , Porat-Katz A , Lewin A ( 1998 ) Assisted reproduction for the treatment of azoospermia . Human Reproduction 13 (Suppl. 4): 41 –60.
Said TM , Agarwal A , Zborowski M , et al. ( 2008 ) utility of magnetic cell separation as a molecular sperm preparation technique . Journal of Andrology 29 (2): 134 –142.
Shimizu T , Ooki T , Suzuki M , Kamiyama H ( 2009 ) An investigation of the separation of mature spermatozoa using Sperm Slow™ for intracytoplasmic sperm injection and its clinical results . Fertility and Sterility 92 (3): S139 –S139.
Silber SJ , Johnson L ( 1998 ) Are spermatid injections of any clinical value? ROSNI and ROSI revisited: round spermatid nucleus injection and round spermatid injection . Human Reproduction 13 : 509 –515.
Silber SJ , Van Steirteghem AC , Liu J , et al. ( 1995 ) High fertilization and pregnancy rate aft er intracytoplasmic sperm injection with spermatozoa obtained from testicle biopsy . Human Reproduction 10 : 148 –152.
Simoni M , Kamischke A , Nieschlag E ( 1998 ) Th e current status of the molecular diagnosis of Y-chromosomal microdeletions in the work-up of male infertility . Human Reproduction 13 (7): 1764 –1768.
Sousa M , Mendoza C , Barros A , Tesarik J ( 1996 ) Calcium responses of human oocytes aft er intracytoplasmic injection of leucocytes, spermatocytes and round spermatids . Molecular Human Reproduction 11 : 853 –857.

Chapter 13: Micromanipulation techniques
237
Sutcliff e AG , Taylor B , Li J , et al. ( 1999 ) Children born aft er intracytoplasmic sperm injection: population control study . BMJ 318 (7185): 704 –705.
Svalander P , Forsberg A-S , Jakobsson A-H , Wikland M ( 1995 ) Factors of importance for the establishment of a successful program of intracytoplasmic sperm injection treatment for male infertility . Fertility and Sterility 65 : 828 –837.
te Velde E, Van Baar A , Van Kooij R ( 1998 ) Lancet 351 (9115): 1524 –1525.
Twigg JP , Irvine DS , Aitken RJ ( 1998 ) Oxidative damage to DNA in human spermatozoa does not preclude pronucleus formation at intracytoplasmic sperm injection . Human Reproduction 13 (7): 1864 –1871.
Wang WH , Kaskar K , Ren Y , et al. ( 2008a ) Comparison of development and implantation of human embryos biopsied with two diff erent methods: aspiration and displacement . Fertility and Sterility 90 (S1): S343 .
Wang WH , Kaskar K , Gill J , DeSplinter T ( 2008b ) A simplifi ed technique for embryo biopsy for preimplantation genetic diagnosis . Fertility and Sterility 90 (2): 438 –442.
Van Assche E , Bonduelle M , Tournaye H ( 1996 ) Cytogenetics of male infertility . Human Reproduction 11 (Suppl. 4): 1 –26.
van den Bergh M , Fahy-Deshe M , Hohl MK ( 2009 ) Pronuclear zygote score following intracytoplasmic injection of hyaluronan-bound spermatozoa: a prospective randomized study . Reproductive Biomedicine Online 19 (6): 796 –801.
Vanderzwalmen P , Nijs M , Stecher A , et al. ( 1998 ) Is there a future for spermatid injection? Human Reproduction 13 (Suppl. 4): 71 –84.
van Rumste M , Evers JLH , Farquhar C ( 2004 ) Intra-cytoplasmic sperm injection versus conventional techniques for oocyte insemination during in vitro fertilisation in patients with non-male subfertility: A Cochrane Review . Human Reproduction 19 (2): 223 –227.
Van Steirteghem A , Liu J , Nagy P , et al. ( 1995 ) Microinsemination. In: Hebon B , Bringer J , Mares P (eds.) Fertility and Sterility: A Current Overview . IFFS-95, Parthenon Publishing Group , New York , pp. 295–404.
Woldringh GH , Janssen IM , Hehir-Kwa JY , et al. ( 2009 ) Constitutional DNA copy numbers in ICSI children . Human Reproduction 24 (1): 233 –240.
Woodward BJ , Sookram ( 2010 ) Polar body positioning during ICSI: does it matter? Human Fertility (in press).
Woodward BJ , Campbell KH , Ramsewak SS ( 2008a ) A comparison of headfi rst and tailfi rst microinjection of sperm at intracytoplasmic sperm injection . Fertility and Sterility 89 (3): 711 –714.
Woodward BJ, Montgomery S, Hartshorne G, Campbell K, Kennedy R ( 2008b ) Spindle position assessment prior to ICSI does not benefi t fertilization or early embryo quality. RBM Online. 16(2): 232–238.
Worrilow K , Eid S , Matthews J , et al. ( 2007 ) A multi-site clinical trial evaluating PICSI® versus intracytoplasmic sperm injection (ICSI): positive clinical outcomes observed in a prospective, randomized and double-blinded study . Fertility and Sterility 92 (3): S36–S37 .
Yanagimachi R ( 2001 ) Gamete manipulation for development: new methods for conception . Reproduction and Fertility Development 13 (1): 3 –14.

Chapter
1
238
Preimplantation genetic diagnosis Joyce Harper
Preimplantation genetic diagnosis (PGD) is an early form of prenatal diagnosis, developed in the late 1980s to help couples who are at risk of transmitting an inher-ited disease to their off spring. If such couples wish to have a healthy family, the main option open to them is prenatal diagnosis by amniocentesis or chorionic villus sampling (CVS). Th e disadvantage of prenatal diagno-sis is that if the diagnosis shows the fetus to be aff ected, the couple have to decide whether they wish to termin-ate the pregnancy or carry on with the knowledge that their child is going to be aff ected by the genetic disease. PGD off ers some of these couples an alternative, as the diagnosis is performed on the preimplantation embryo and only unaff ected embryos are transferred to the patient. Th e pregnancy is therefore initiated with the knowledge that the fetus is free from the disease.
Th e majority of patients referred for PGD are those who have already experienced several terminations of aff ected pregnancies, those with moral or religious objections to termination, patients who have expe-rienced repeated miscarriages due to unbalanced chromosome arrangements in the fetus and infertility patients who are also carrying a genetic or chromo-somal abnormality.
PGD covers several fi elds: IVF, genetics, embryo biopsy and single cell diagnosis. Before discussing embryo biopsy and single cell diagnosis, it is import-ant to outline the inheritance of genetic disease and the principles of prenatal diagnosis.
The genetics of inherited disease Th ree groups of inherited disease can be diagnosed by PGD: 1. Single gene defects 2. Triplet repeat disorders
3. Chromosomal abnormalities.
Single gene defects may aff ect the autosomes (chro-mosomes 1–22) or the sex chromosomes (X and Y). Single gene defects are inherited by autosomal reces-sive, autosomal dominant and X-linked (sex-linked) modes. Th e triplet repeat disorders are a group of diseases caused by an expansion of a triplet repeat of base pairs on a chromosome. Chromosomal abnor-malities , such as translocations and inversions, can lead to a fetus with an unbalanced chromosome complement.
Since chromosomes exist in pairs (one of each pair inherited from each parent), genes are present in two copies, with the exception of those carried on the sex chromosomes in males: they have only one X and one Y chromosome. Th e majority of genetically inherited diseases are caused by a mutation within a specifi c gene, which causes the gene to be inactive or faulty. Whether the disease is expressed when both or only a single copy of the gene carries a mutation depends upon the mode of inheritance. Th e muta-tions that lead to a disease can be caused by a single change, or by more complicated changes in the bases within the gene. Th is change may be a deletion, sub-stitution or insertion in the base sequence. Within a single gene, there are “hot spots” prone to mutation. For example, over 800 cystic fi brosis (CF) mutations have been identifi ed, but, in the UK, 70% of individ-uals who carry CF have the same mutation, deltaF508, caused by a deletion of three base pairs in exon 10 of the CF gene.
Age-related aneuploidy is also an important factor that may lead to chromosomally abnormal off spring. Th is is not an inherited disease, and it can occur in any pregnancy.
14
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 14: Preimplantation genetic diagnosis
239
Autosomal recessive disease Th e inheritance of autosomal recessive disease is shown in Figure 14.1 .
Autosomal recessive inheritance accounts for the majority of genetic disease. If an individual has one normal gene and one abnormal gene, he or she is a car-rier of the disease and will usually be unaff ected. Th e individual will be aff ected by the disease if the genes inherited from both the mother and the father carry the mutation. For example, if both the mother and the father are carriers of CF, the off spring have a 1 in 4 chance of being aff ected, a 1 in 4 chance of being unaff ected, and a 2 in 4 chance of being a carrier.
Th e most common autosomal recessive single gene defect is beta-thalassemia , which is caused by a muta-tion in the beta-globin gene . However, there are many diff erent mutations for beta-thalassemia, especially
between diff erent ethnic groups: the majority of cou-ples carry diff erent mutations (compound heterozy-gotes) and this complicates PGD (see section on PCR diagnosis).
Cystic fi brosis is the most common autosomal recessive single gene defect for which PGD has been applied. Since deltaF508 is such a common mutation, there are many couples in whom both partners carry this mutation, making PGD relatively simple .
Table 14.1 shows the major autosomal single gene defects that have been diagnosed by PGD.
Autosomal dominant disorders A single copy of the mutated gene will lead to the dis-ease in disorders that are dominant in their inheritance ( Figure 14.2 ). Th ese diseases are not as life-threatening as some recessive diseases, and therefore aff ected indi-viduals can still reproduce and transmit the disease to their off spring. Many dominant disorders are late in onset, such as Huntington’s disease and some inherited cancers.
PGD has been developed for dominant diseases, such as myotonic dystrophy, Marfan’s syndrome , polyposis coli , Charcot–Marie–Tooth disease and Huntington’s disease ( Table 14.2 ).
X-linked diseases X-linked diseases aff ect genes that are carried on the X chromosome, and more than 400 such diseases have been identifi ed. Th ey can be inherited in a recessive or dominant manner, but almost all severe types have recessive inheritance. Males inherit the X chromosome from their mother, and if this inherited X chromo-some is abnormal they will be aff ected with the disease ( Figure 14.3 ). Th erefore, carrier mothers transmit the disease to half of their male off spring, and half of her daughters will be carriers. With PGD, sexing can be
A
Parents
B C D
A
Gametes
B C D
A
Offspring
C
Affected Normal
Mutant allele
Carriers(unaffected)
B CA D B D
Figure 14.1 Autosomal recessive inheritance.
Table 14.1 PGD for autosomal recessive diseases
Cystic fi brosis (various mutations)
Sickle cell anemia
Tay–Sachs disease
Spinal muscular atrophy
β-Thalassemia
Adrenogenital syndrome
Hypophosphatemia

Chapter 14: Preimplantation genetic diagnosis
240
performed at the cleavage embryo stage and female embryos selected for transfer or specifi c diagnosis can be carried out using PCR, which allows the transfer of non-aff ected males and non-carrier females.
X-linked diseases reported as diagnosed by embryo sexing are listed in Table 14.3a . Th e X-linked diseases where a specifi c diagnosis has been performed are listed in Table 14.3b .
Triplet repeat disorders A new class of genetic disorders was classifi ed during the 1990s: the triplet repeat disorders are caused by the expansion of a triplet repeat of bases within a gene, and are usually associated with neurological disorders. Each disease has a range of repeats associated with a spectrum from normal individual to aff ected individ-uals. For example, for the triplet repeat responsible for fragile X syndrome , a normal individual will have from 6 to 54 triplet repeats; those having the “premuta-tion” will carry between 54 and 200 repeats, and those aff ected with fragile X will have over 200 repeats.
Fragile X was originally thought to be an X-linked disease, as males are generally aff ected, but it has been reclassifi ed as a triplet repeat disorder. It is caused by
Table 14.2 PGD for autosomal dominant diseases
Marfan’s syndrome
Familial adenomatous polyposis coli
Huntington’s disease
Myotonic dystrophy
Osteogenesis imperfecta
A
Parents
B C D
A
Gametes
B C D
A
Offspring
C
Affected Unaffected
Mutant allele
A DB C B D
Figure 14.2 Autosomal dominant inheritance.
Xp
Parents
Y 1
1
122 1
2
Xm
MotherFather
Xm
Xp
Gametes
Y Xm Xm
Xm
Offspring
Y
Affectedboy
Normalboy
Carriergirl
Normalgirl
Mutant allele
Xm XpXm Y Xm Xp
2
Figure 14.3 X-linked inheritance.

Chapter 14: Preimplantation genetic diagnosis
241
the unstable expansion of a CGG repeat in the 5′-untranslated region of the FMR1 gene, which is on the X chromosome. Th is triplet expansion results in mental retardation. Females carrying the premutation are at risk of transmitting the full mutation to their off spring, and, since males inherit the X chromosome from their mothers and have a single X chromosome, their male off spring are at a 50% risk of inheriting fragile X. Females who inherit the expanded gene from their mothers will also inherit a normal X chromosome from their father, and show vari-able disease manifestations. Males carrying the premuta-tion are at risk only of transmitting the premutation to their female off spring, who will be carrier females.
Huntington’s disease (HD) is a progressive neuro-psychiatric disorder of late onset that is inherited in a dominant fashion. Th e gene is on chromosome 4, and involves a CAG triplet repeat where expansion beyond 36 results in HD. Th e age of onset is about 40 years and patients oft en die by their mid 50s. PGD has been performed for HD, but it draws some ethical discus-sion: many potential carriers of HD know that they have a 50% risk of being aff ected because one of their parents is aff ected, but they do not wish to know their own HD status. For prenatal testing and PGD, an exclu-sion test can be off ered, where patients are given a risk factor without being told their actual status .
Myotonic dystrophy (DM) or Steinert’s disease is a progressive muscular dystrophy. Th e gene is on chromosome 19 and DM is caused by expansion in a CTG repeat at the 3′-untranslated part of the DM kin-ase gene. Normal individuals have between 5 and 37 repeats, and aff ected individuals may have anything from 50 to several thousand repeats. Intermediate numbers of repeats can give rise to a premutation. PGD can be performed for DM.
Chromosomal abnormalities Abnormalities that involve whole chromosomes are usually lethal. Th ose compatible with life involve the sex chromosomes, such as Turner’s syndrome (XO), Klinefelter’s syndrome (XXY) or Down’s syndrome (three copies of chromosome 21).
Th e most common chromosome abnormality is a chromosome translocation, where two chromosomes have broken and rejoined to the opposite chromosome. If the chromosomes are still balanced, i.e., all the gen-etic material is still present, the patient is described as having a balanced translocation. Th e majority of patients carrying a balanced translocation do not real-ize they have abnormal chromosomes until they try to reproduce. During meiosis , the segregation of the chromosomes becomes confused, and unbalanced chromosome complements are formed in the gametes, leading to the formation of an embryo with abnormal chromosomes (unbalanced translocation). Th erefore patients carrying balanced translocations may experi-ence infertility, repeated miscarriage or the birth of a child with abnormal chromosomes.
Robertsonian translocations involve breakages around the centromere of the “acrocentric” chromo-somes (13, 14, 15, 21, 22). Th ese chromosomes contain a satellite region on their short arm, and loss of this area
Table 14.3 PGD for X-linked diseases
(a) Sexing
Duchenne muscular dystrophy
Becker muscular dystrophy
Chronic granulomatosis
Hunter’s syndrome
Hemophilia
Adrenoleukodystrophy
Barth syndrome
X-linked hydrocephalus
X-linked ataxia
X-linked incontinentia pigmentosa
X-linked mental retardation
X-linked Wiscott–Aldrich
X-linked spastic paraplegia
Laber’s optic atrophy
Sensory motor neuron disease
Retinitis pigmentosa
Bruton’s disease
Menkes disease
(b) Specifi c diagnoses
Duchenne muscular dystrophy
Hemophilia
Lesch–Nyhan syndrome
Charcot–Marie–Tooth

Chapter 14: Preimplantation genetic diagnosis
242
has no eff ect on phenotype. Since two of the acrocen-tric chromosomes join together, the patient has only 45 chromosomes. Robertsonian translocations can be diagnosed using PGD, as only the number of chromo-somes present needs to be identifi ed.
Reciprocal translocations involve breaks at any location on two chromosomes and thus can involve any chromosomes. Th e fact that every couple has diff erent chromosome breakpoints makes PGD diffi cult .
Chromosome abnormalities can also be caused by chromosome inversions, insertions, deletions or rear-rangements (such as ring chromosomes).
Age-related aneuploidy Women over the age of 35 are known to be at increased risk of having a fetus with a chromosome abnormal-ity. However, only 20% of Down’s syndrome babies are born to women over the age of 35. Screening methods have been developed to help identify those pregnan-cies at risk, as the use of age alone as an indication for prenatal diagnosis of age-related aneuploidy will miss the majority of aff ected pregnancies. Biochemical (plasma alpha-fetoprotein, hCG, unconjugated estriol) and ultrasound screening methods are there-fore used to determine which pregnancies are at risk. Patients found to be at risk undergo prenatal diagno-sis, with a karyotype performed to ascertain the sta-tus of the fetus. Th e chromosomes most commonly involved in age-related aneuploidy are 13, 16, 18, 21, X and Y .
Serum screening During the second trimester of pregnancy (16–17 weeks) a number of markers have been found to help identify pregnancies with chromosome abnormalities. Down’s syndrome pregnancies show lower maternal serum alpha-fetoprotein (AFP) and unconjugated estriol, whereas human chorionic gonadotropin (hCG) levels are two times higher than normal. Taking into account the patient’s age, the use of the triple test to measure AFP, free beta-hCG and unconjugated estriol can increase the detection rate to 70%, thereby redu-cing the number of women who require invasive pre-natal diagnosis.
Ongoing research is directed towards trying to iden-tify fi rst trimester markers for aneuploidy. Pregnancy-associated plasma protein A (PAPP A) is reduced in Down’s syndrome pregnancies.
Ultrasound During the fi rst trimester of pregnancy, ultrasound detection of nuchal translucency measuring greater than 3 mm is associated with a chromosome abnor-mality. Th is is caused by fl uid accumulation at the back of the fetal neck. In conjunction with maternal age, studies have shown this to give a detection rate of 86% with a false positive rate of 4.5%. When used in com-bination with fi rst and second trimester serum screen-ing, a detection rate of over 90% was reported.
In the second trimester, ultrasound markers such as cardiac malformations, duodenal atresia, hydrops, choroid plexus cysts, nuchal edema, renal pyelecta-sis, omphalocele, hypoplastic midphalanx of the fi ft h fi nger, and short femur and humerus can be used to screen for aneuploidy. Th e addition of digital imaging and computer analysis of two-dimensional ultrasound pictures allows three- and four-dimensional images to be built up, which allow more in-depth assessment of cardiac and neural abnormalities, and show a clearer picture of what specifi c abnormalities look like.
Prenatal diagnosis of inherited disorders Couples who have already had an aff ected pregnancy or child, or have a family member aff ected with the dis-ease are aware that they are at risk of transmitting an inherited disease. Prenatal diagnosis is the main option open to such couples and to those who have a positive serum or ultrasound screen. Chorionic villus sampling (CVS) and amniocentesis are the methods of choice for prenatal diagnosis; techniques such as fetal blood sam-pling are rarely used.
Chorionic villus sampling (CVS) CVS can be performed transcervically between 10 and 12 weeks of gestation, or from 12 weeks onwards by the transabdominal route. A sample of cells is removed from the placenta and used for diagnosis of chromo-somal, metabolic and DNA analysis. Th e disadvantages of the procedure are that it cannot be used for neural tube and other congenital abnormalities, and some studies have suggested a risk of limb reduction deform-ities if it is performed too early, or by inexperienced operators. Th ere is also a 1–2% risk of miscarriage, which is a little higher than the risk aft er amniocen-tesis. In 1.5% of cases, the karyotype of the placenta is

Chapter 14: Preimplantation genetic diagnosis
243
found to be diff erent from that of the embryo (confi ned placental mosaicism).
Amniocentesis Th is is the most common method used for prenatal diagnosis usually performed in the second trimester, from 15 weeks onwards. Under ultrasound guidance, 15–20 mL of amniotic fl uid is aspirated; this can be used for the diagnosis of chromosome abnormalities, meas-urement of specifi c substances, detection of inborn errors of metabolism such as Tay–Sachs disease , meas-urement of enzyme activity and diagnosis of neural tube defects. Its disadvantages include the potential of causing fetal loss (1%) and rarely there may be contin-ued leakage of the amniotic fl uid. Th e main limitation of this technique is that results are available only very late in the pregnancy (17–20 weeks), so that a second trimester termination has to be induced.
Fetal blood sampling, cordocentesis or PUBS (percutaneous umbilical blood sampling) Th is is used less frequently than CVS or amniocen-tesis; samples can be taken from 18 weeks’ gestation to term. Fetal blood is taken from the cord or int-rahepatic umbilical vein and used for fetal karyo-typing (quick result), evaluation of fetal status (if an infection is thought to be present) and hemato-logical abnormalities (Rh or immune hemolytic dis-ease). Th e most common indication is karyotyping for single or multiple congenital abnormalities and mosaicism.
Fetal tissue sampling Using ultrasound guidance it is possible to biopsy skin, liver, muscle and fl uid collections from the urinary tract, abdomen, thorax and cystic hygroma.
Diagnostic testing Following CVS or amniocentesis, the sample must be diagnosed in order to identify the status of the fetus. Two tests are used: the polymerase chain reaction (PCR) or karyotyping. PCR is used for the detection of single gene defects, the triple repeat disorders, and identifi cation of sex. A karyotype is performed for any diagnosis which involves chromosome identifi cation, i.e., in those patients carrying chromosome abnor-malities or who are at risk of age-related aneuploidy. In some situations, fl uorescent in-situ hybridization
(FISH) is used to complement the karyotype result. More recently DNA microarray-based technology has been developed.
PCR PCR is a technique whereby a portion of DNA is amp-lifi ed thousands of times, and it is probably the most important technique used for genetic testing. For pre-natal diagnosis, PCR can be used to detect the normal or mutated gene by amplifying the region around the mutation. Th is is achieved using primers which have a complementary sequence to a region of the gene. Primers are selected which bind to either side of the mutation, they bind to their complementary sequence, and copies are generated for the region in between by a number of cycles of heating (to denature the DNA) and cooling (to allow synthesis). Th is is achieved with the use of an enzyme that can connect bases together and can also withstand the high temperatures needed for denaturation. Th e fi rst such enzyme to be used for PCR was Taq polymerase .
Once the DNA sequence of interest has been cop-ied, the PCR products are analyzed using a number of diff erent techniques. Th e simplest method, which can be used to detect an insertion or deletion, is to separate the PCR products by polyacrylamide gel electrophor-esis; more recently techniques such as single-stranded conformational polymorphism (SSCP) , amplifi cation refractory mutation system (ARMS) and heteroduplex analysis have been developed.
Using these techniques even just a single base change within a gene can be detected. PCR will be dis-cussed in more detail in the section concerning PGD diagnosis.
Karyotyping Karyotype analysis is the ideal method to examine the chromosomes of a cell. For prenatal diagnosis, the sam-ple obtained by CVS or amniocentesis is cultured to increase the number of cells, and mitotic inhibitors are used to arrest some of the cells in metaphase. Agents which elongate the metaphase chromosomes are also used. Slide preparations of the nuclei are treated with Giemsa stain, which results in a specifi c banding pat-tern for each chromosome. Using this method, missing or extra chromosomes, translocations, inversions, etc. can be identifi ed. Occasionally the results of a karyo-type may be inconclusive, and FISH can be used to help elucidate the diagnosis .

Chapter 14: Preimplantation genetic diagnosis
244
Karyotyping is also used to check the number of chromosomes in diagnosis of age-related aneuploidy.
FISH FISH uses DNA probes that bind to complementary sequences on specifi c chromosomes. Th ere are three types of FISH probes : 1. Repeat sequences or alpha satellite probes,
which can be used in interphase and metaphase chromosomes. Th ey bind to repeat sequences, usually to the centromeres (with the exception of chromosomes 9 and Y) and can be used directly labeled with fl uorochromes. Th ey require only 1 hour for hybridization and have been cloned in plasmids and cosmids. Probes for 13/21 and 14/22 cross-hybridize.
2. Locus-specifi c probes can be used in interphase or metaphase chromosomes and bind to a unique sequence. Th ey require 6–12 hours for hybridization and have been cloned in cosmids or YACs (yeast artifi cial chromosomes).
3. Chromosome paints can only be used in metaphase chromosomes, and they paint the entire chromosome.
Th ere are several stages to the FISH technique : 1. Cell spreading. 2. Pepsin digestion. Th is is required to remove any
protein from around the nuclei and is especially important for blastomeres.
3. Fixing. A paraformaldehyde fi xative is used to ensure that the nuclei are stuck onto the slide.
4. Denaturation. Th is makes the nuclear and probe DNA single-stranded.
5. Hybridization. Allows the probes to fi nd and bind to the complementary sequence.
6. Posthybridization washes. Removes any unbound probe.
7. Detection – for use with indirect probes. 8. Visualization.
Arrays Two types of arrays are used in molecular diagnos-tic testing: array comparative genomic hybridization (A-CGH) and single nucleotide polymorphism (SNP) arrays. SNP arrays can examine the chromosome con-tent as well as look at individual genes. Th e problem has
been in interpreting these arrays as so much informa-tion is obtained, especially in relation to copy number variants. A-CGH only examines the chromosomes and is easier to interpret. It is possible that array technology will replace FISH, PCR and karyotyping in the future.
Preimplantation genetic diagnosis PGD is comparable to prenatal diagnosis. Th e embryo biopsy is equivalent to the CVS or amniocentesis and the single cell diagnosis equates to the prenatal diag-nosis. Since two techniques are involved, biopsy and diagnosis, a PGD team is made up of an IVF and a gen-etics team. Th e embryo biopsy technique should be performed by a trained embryologist, but the diagnosis must be performed by a genetics department.
Embryo biopsy Cell biopsies can be taken from oocytes/embryos at three diff erent stages: 1. Oocyte/zygote (polar body biopsy) 2. Six- to eight-cell cleavage stage embryo (cleavage
stage biopsy) 3. Blastocyst stage embryos (blastocyst biopsy).
Th e majority of PGD centers have been using cleavage stage biopsy for PGD. However, in recent years polar body biopsy has been commonly used in countries where manipulation of the embryo is not allowed (e.g., Germany). Blastocyst biopsy has only recently been reported for clinical PGD but its use may increase with the introduction of array technology into the PGD arena.
As outlined in Chapter 13 , embryo biopsy is per-formed using micromanipulation equipment used for ICSI, and all of the biopsy techniques involve two stages: zona drilling, and aspiration (or herniation in the case of blastocyst biopsy). Table 14.4 outlines an overview of embryo biopsy methods; the techniques are discussed in detail in Chapter 13 .
Polar body biopsy Biopsy of the fi rst polar body was developed in order to overcome ethical objections to embryo biopsy. Some individuals opt for PGD in order to avoid ter-mination of pregnancy, and performing the test on the preimplantation embryo may be as objectionable as termination of pregnancy. Polar body biopsy was fi rst used for the detection of CF, but due to crossing-over

Chapter 14: Preimplantation genetic diagnosis
245
events the second polar body was required in some situations. Biopsy of the fi rst and second polar body is recommended if polar body biopsy is going to be used for PGD .
Cleavage stage biopsy Biopsies performed at earlier stages (four cells) may alter the ratio of inner cel l mass to trophectoderm cells , which may be detrimental to embryo development. Th erefore, the main strategy used for embryo biopsy has been to biopsy embryos at the six- to eight-cell stage, on Day 3 post insemination.
Several difficulties arise from cleavage stage embryo biopsy: the first is that human embryonic cells are very fragile and easily lyse. If this occurs during the biopsy procedure, the nucleus may be lost and another cell will have to be removed. Compaction occurs between the eight-cell and morula stage, and during compaction the cells of the embryo can no longer be distinguished as they flatten out over each other to maximize intercellular contacts. If the biopsy is performed at this stage, it is very difficult to remove a blastomere, as it has established strong contact with adjacent blastomeres. Trying to remove a cell from a compacted embryo may also result in lysis of the cell. The thickness and dynamics of the zona pellucid a also vary between patients and can
lead to some problems during the biopsy proced-ure. In many cases, numerous sperm are associated with the zona pellucida and therefore intracytoplas-mic sperm injection (ICSI) should always be used with PCR techniques to reduce the risk of sperm contamination.
In the human, the cryopreservation of embryos in IVF treatment cycles is routine, and from frozen embryo replacement cycles up to 50% of blastomeres can be destroyed and the embryo is still capable of producing a viable fetus. No increase in fetal abnor-malities has been reported following transfer of cryopreserved embryos in which some cells have been destroyed by freezing/thawing. Studies exam-ining the eff ect of embryo biopsy have shown that at the eight-cell stage, removal of two cells was not detrimental to embryo metabolism or development and is an effi cient process with more than 90% of the embryos surviving. Data from the ESHRE PGD consortium show that 97% of embryo biopsies were successful.
Pregnancies obtained from biopsied embryos aft er PGD have been studied. Biochemical and ultrasound measurements showed that there were no signifi cant developmental diff erences between these pregnancies and controls. Deliveries, including infant birth weight and Apgar scores, were consid-ered to be normal.
Table 14.4 The three methods of embryo biopsy used in preimplantation genetic diagnosis. Reproduced with permission from Harper 2009.
Day performed Types of cells removed
Indications Zona drilling
Cell removal Limitations
Polar body First PB Day 0 Second PB Day 1 Or simultaneously
on Day 1
First and second polar bodies
PGS Monogenics
carried by mother
Laser Mechanical Beveled
pipette
Aspiration Only maternal chromosomes/genes
Cleavage-stage
Day 3 Blastomeres PGS Monogenics Sexing Chromosome
abnormalities
Laser Mechanical Acid Tyrodes
Aspiration Displacement
Postzygotic mosaicism
Blastocyst Day 5 Trophectoderm PGS Monogenics Sexing Chromosome
abnormalities
Laser Mechanical Acid Tyrodes
Herniation Postzygotic mosaicism
Some embryos will arrest prior to biopsy
Short time for diagnosis

Chapter 14: Preimplantation genetic diagnosis
246
Blastocyst biopsy Blastocyst biopsy can be performed on Day 5 or Day 6 post insemination, and has the advantage that a larger number of cells can be removed from the outer troph-ectoderm layer without aff ecting the inner cell mass from which the fetus later develops. Analysis of a larger number of cells is of benefi t in diagnosis of monogenic diseases. However, trophectoderm cells (TE) may have diverged genetically from the inner cell mass (ICM) as confi ned placental mosaicism is observed in at least 1% of conceptions, where the chromosome status of the embryo is diff erent from the placenta. Studies indicate that blastocysts may have high levels of chromosomal mosaicism. Vitrifi cation as a method of cryopreserving blastocysts has recently shown excellent results; vitri-fying aft er blastocyst biopsy allows more time for the diagnosis.
Th e main limitation of blastocyst biopsy is that a limited number of embryos will reach the blastocyst stage. Although improvements in culture conditions have increased the numbers of blastocysts available, for PGD to be successful a large number of embryos are required to ensure that normal embryos are available for transfer; this may not be the case when embryos are cultured to the blastocyst stage.
Single cell diagnosis Cells removed from the embryo aft er biopsy are used for diagnosis, as outlined in Table 14.5 . PCR is used for the single cell diagnosis of single gene defects, trip-let repeat disorders and embryo sexing. Karyotyping requires a metaphase spread of chromosomes, and therefore this cannot be used on single embryonic cells; these cells do not divide well in culture, and it is diffi cult to obtain metaphase spreads. In cases where a metaphase spread is obtained, the chromosomes are short and diffi cult to band. Th erefore FISH is used to examine chromosomes in embryos for embryo sex-ing, chromosome abnormalities and aneuploidy. Array technology has been applied in PGD.
Molecular diagnosis PCR diagnosis from a single cell is used for the diagno-sis of single gene defects, triplet repeat disorders and embryo sex, but it is not a simple procedure. Th e two major problems encountered are contamination and allele dropout (see below), which both complicate the procedure. If a diagnosis is available on whole DNA, it
should be possible to make such a diagnosis sensitive at the single cell level. However, some modifi cations of the procedure may be required. A common method of making the PCR procedure more sensitive is the use of nested PCR, where an inner set of primers amplifi es the original PCR product. Since amplifi cation failure can occur, it is essential that PGD does not rely on a negative result. To ensure that a single cell PCR method is accurate and sensitive, a preliminary workup is usu-ally performed on single cells, such as buccal cells, from normal, carrier and aff ected individuals. Th e analyses of PGD PCR products have been performed by heteroduplex analysis, SSCP, ARMS and restriction endonuclease digestion. Fluorescent PCR is a quanti-tative PCR method that can also be used. For the diag-nosis of some diseases, such as fragile X, polymorphic markers may be used that identify which chromosome the embryo has inherited; i.e., the normal or at-risk chromosome.
Contamination Single cell PCR is so sensitive that it will amplify any DNA that may contaminate the PCR reaction, such as a stray cumulus or sperm cell that may have been released from the zona during the biopsy, cells from the atmosphere or DNA found in the air or medium. To reduce these problems to a minimum, steps have to be taken to eliminate contamination. Th ese include work-ing in a positive pressure PCR room, performing ICSI for all PCR diagnosis and examining PCR products in a separate laboratory. Misdiagnoses reported aft er PGD probably arise from contamination. Th ese prob-lems can be reduced with the use of a multiplex PCR with markers that can identify all four parental alleles to ensure that the amplifi ed product is of embryonic origin .
Allele dropout Allele dropout (ADO), or preferential amplifi cation, refers to the situation where one of the two alleles preferentially amplifi es over the other. For example, for a heterozygous cell, the normal allele may pref-erentially amplify so that the diagnosis would only identify the normal allele – the embryo would be diagnosed as normal instead of heterozygous. Th is would not cause a problem for recessive conditions where both partners carry the same mutation, but would create problems for dominant disorders, or in cases where the couple carry diff erent mutations for a recessive disorder, as aff ected embryos could be

Chapter 14: Preimplantation genetic diagnosis
247
diagnosed as normal. To reduce this problem, meth-ods can be built into the diagnosis to ensure that both alleles can be identifi ed.
FISH diagnosis Fluorescent in-situ hybridization (FISH) allows every nucleus within an embryo to be examined, but the number of chromosomes that can be analyzed at one time is limited. Using two rounds of FISH on a single nucleus allows a panel of seven to nine chromosomes to be screened (commonly including X, Y, 13, 16, 18, 21, 22), but repeated denaturation leads to DNA degen-eration and decreases the effi ciency of the procedure. Repeat and locus-specifi c probes can be used for cleav-age or blastocyst biopsies as the embryonic nuclei are in interphase, but chromosome paints can be used on polar bodies.
FISH has been used since 1991 to sex embryos for PGD in cases of X-linked disease. It has advantages over PCR sexing as the copy number is identifi ed: the diff er-ence between XO and XX can be determined, and there
is no risk of contamination. Usually, probes for chromo-somes X, Y and 18 are used and only embryos showing normal female chromosomes are transferred. However, the best method to perform PGD for X-linked disease is a specifi c diagnosis of the disorder using a molecu-lar method. Th is will diff erentiate between the aff ected male, unaff ected male, carrier female and non-carrier female.
With the development of a wider range of locus-specifi c probes, FISH can be used for the detection of chromosome imbalances in patients carrying chromosome abnormalities. In these situations, a normal and balanced chromosome pattern cannot be distinguished. If the female carries the translocation, polar body biopsy can be performed and chromo-some paints used. For Robertsonian translocations, probes for any area of the chromosome involved can be used, but for reciprocal translocations probes are used either side of the break points. A-CGH is being developed to diagnose chromosome imbalances in embryos .
Table 14.5 Methods used for preimplantation genetic diagnosis. Reproduced with permission from Harper 2009.
Indications Cell preparation Protocol Limitations
FISH Sexing Chromosome
abnormalities PGS
Spreading cells using methanol:acetic acid or Tween HCl
Fix Denature Hybridization Wash off unbound probe Visualize
Cumulus contamination
Mosaicism Overlapping signals Failure of probes to
bind
PCR Sexing Monogenic disorders
Tubing cells into lysis buff er
Lyse cell Cycles of denaturing,
annealing, elongation Detect products
Cumulus contamination
Sperm contamination (use ICSI)
Other contamination Amplifi cation failure Allele dropout
Metaphase CGH Sexing Chromosome
abnormalities PGS
Tubing cells into lysis buff er
Lyse cell, whole genome amplifi cation
Co-hybridization with control sample on to metaphase spread
Analysis of each chromosome using CGH software
Contamination Mosaicism Procedure takes
several days and so currently embryos are frozen
Requires many skills, PCR, and cytogenetics
FISH, fl uorescent in situ hybridization; PGS, preimplantation genetic selection; PCR, polymerase chain reaction; ICSI, intracytoplasmic sperm injection; CGH, comparative genomic hybridization.

Chapter 14: Preimplantation genetic diagnosis
248
PGD of age-related aneuploidy (preimplantation genetic screening, PGS) Preimplantation genetic screening (PGS) has been used extensively in an attempt to select the best embryo to transfer for patients going through IVF. Indications have included t hose patients with advanced maternal age, repeated implantation failure, repeated miscar-riage with a normal karyotype and severe male factor. Initial studies reported an improvement in pregnancy rate when using PGS with FISH to detect the common aneuploidies (13, 16, 18, 21, 22, etc.). To date ten ran-domized controlled trials using cleavage stage biopsy and one using blastocyst biopsy have shown no increase in delivery rates when using PGS for a variety of indi-cations. Some studies showed a signifi cant decrease in delivery rates in the treatment group. For PGS to be used successfully, the negative eff ect of the biopsy must be compensated for by the advantage of the gen-etic testing. Using FISH at cleavage stages does not do this due to limitations in the FISH procedure (a limited number of probes can be used and the technique is not 100% effi cient) and the high levels of mosaicism seen at cleavage stages which will result in false positives and negatives .
Current work is looking at polar body or blastocyst biopsy and the use of array technology to determine if PGS has a future in the fi eld of ART .
Chromosomal mosaicism FISH, metaphase and array CGH have been used for the analysis of chromosome patterns in human pre-implantation embryos which have been donated for research purposes. Studies on abnormally fertilized embryos (such as polyspermic embryos) have shown, as expected, that these embryos were highly abnormal, in agreement with the karyotype data obtained from such embryos. In the majority of cases, mosaicism was observed and, in some cases, normal diploid embryos were found from supposedly polyspermic embryos; this may have been due to misidentifi cation of a vacu-ole as a pronucleus. As expected, embryos from older women show high levels of chromosome abnormalities but interestingly normally fertilized, normally devel-oping embryos also show high levels of chromosomal abnormalities. In order to categorize these abnormal-ities, the patterns have been divided into four groups. Embryos are either :
(a) uniformly diploid, (b) uniformly abnormal, such as Down’s syndrome or
Turner’s, (c) mosaic, where usually both diploid cells and
aneuploid, haploid or polyploid nuclei are present or
(d) chaotic embryos, where every nucleus shows a diff erent chromosome complement.
Th e data from FISH and CGH analysis show a higher rate of abnormalities than has previously been reported from karyotyping data. However, since mosaic and chaotic embryos are common, if only one or two cells are analyzable from an embryo, then karyotyp-ing would underestimate the level of chromosome abnormalities.
Normal, abnormal and mosaic embryos have all been observed in fetal development. It has been esti-mated that in 1% of conceptions the placenta has a diff erent karyotype from the fetus (confi ned placental mosaicism – CPM). CPM was fi rst detected when fi rst trimester fetal karyotyping aft er chorionic villus sam-pling showed discrepancies between chorionic cells and the embryo proper. Th e presence of two cell lines could arise due to an abnormal chromosome arrange-ment caused by a postzygotic event, or the chromosome loss from a trisomic embryo, which restores the dip-loid state (trisomic rescue). Several mechanisms would indicate that these abnormal cells are more likely to be found in the trophectoderm, and hence the placenta. First, only a few cells from a blastocyst give rise to the embryo and it would be unlikely that the abnormal cells would be found in the embryo; second, in most cases a fetus with abnormal chromosomes will not be compatible with life. Th e chaotic group of embryos was an unexpected fi nding, as such embryos have not been observed in later stages of embryonic development, probably because these embryos would arrest and fail to implant .
Multinucleated blastomeres have been reported from both karyotyping and FISH analysis. Th e pres-ence of such blastomeres may be more common in arrested embryos, and may occur more readily in some patients. Binucleate blastomeres have been observed in mouse embryos at the morula stage, and it has been suggested that these blastomeres might be the precur-sors for mural trophectoderm giant cells. However, in human embryos the binucleate cells appear at cleavage stages before trophectoderm diff erentiation. Binucleate cells may arise from asymmetrical cytokinesis so that

Chapter 14: Preimplantation genetic diagnosis
249
one daughter cell contains two nuclei and the other is anucleate.
Embryos containing tetraploid cells may be a nor-mal part of development of the trophectoderm. Such cells have also been found in cattle, pig and sheep.
Overall, extrapolation of this data would suggest that few embryos are completely chromosomally nor-mal at early cleavage stage. However, various models for which there are experimental data may help to explain the observation that pregnancies following IVF do not result in an increased incidence of chromo somally abnormal infants. Few cells (possibly a single cell from an eight-cell embryo) diff erentiate to the embryo proper – the majority contribute to the cytotrophob-last and fetal membranes. Data accumulated on the chromosomal constitution of surplus nontransferred embryos from PGD cycles have revealed that, despite the fact that these embryos are from women of proven fertility, the incidence of postzygotic chromosomal anomalies is similar to that in embryos from routine IVF patients. Th is fi nding may provide one explanation for the apparently poor success rate of IVF procedures. A second signifi cant fi nding is that the incidence of the most bizarre type of anomaly, chaotically dividing embryos, is strongly patient-related. In repeated cycles, certain women regularly produced “chaotic” embryos while others did not, although the frequency of diploid mosaics was similar in both groups.
All the studies performed in recent years to analyze chromosomes in embryos have been carried out using embryos generated by IVF, which may not be repre-sentative of in-vivo development. However, the clas-sic studies of Hertig et al . ( 1956 ) showed that embryos from natural cycles also showed high levels of nuclear abnormalities, and from the studies of normally con-ceived pregnancies, we know that 60% of abortions are chromosomally abnormal .
Mosaicism and PGD Chromosomal mosaicism may cause a problem in PGD for some diseases, namely dominant disorders and chromosome abnormalities. A misdiagnosis of embryo sex would be unlikely to occur as an XX cell would have to be found in an XY embryo. XO cells have been identifi ed in male embryos, but XO embryos should never be considered for transfer; if the off spring have Turner’s syndrome, they would have the same risk of suff ering the X-linked disease as would a male. For recessive disorders, the presence of extra chromosomes
or a haploid cell would not lead to a misdiagnosis. A carrier embryo with a haploid cell would be diagnosed as normal or aff ected depending on which gene was present in the cell: this would be the same situation if allele dropout had occurred. For dominant disorders, a haploid cell could lead to a misdiagnosis; if a cell from an aff ected embryo carried only the unaff ected gene, the cell would be diagnosed as normal. Th erefore the same precautions as for allele dropout would have to be applied. For chromosome abnormalities, mosaic embryos containing some normal and some abnor-mal cells have been identifi ed, such as in cases where a few normal cells arise in an embryo which otherwise carried trisomy 21. If the normal cells are biopsied, the embryo would be diagnosed as normal, resulting in misdiagnosis. As with confi ned placental mosaicism, this problem cannot be solved. Patients undergoing PGD for chromosomal abnormalities have to be aware that chromosomal mosaicism can lead to a misdiag-nosis, but that this is a rare event. Th e probability can be reduced if two cells are used for the diagnosis, but this is not always technically feasible .
Ethics and laws Th e law governing PGD varies worldwide. Some countries have legislation regulating PGD, or PGD and embryo research, and others have no legislation. However, a few countries have banned cleavage stage biopsy – which is astonishing in view of the fact that the aim of PGD is to eliminate termination of pregnancy. Th e main arguments against PGD are that it may be abused, as in the case of embryo sex selection for fam-ily balancing, or for choosing certain characteristics, the so-called “Designer Baby.” Prenatal diagnosis has been abused for fetal sex selection in several countries for many years, but, as with all medical practices, the good should outweigh the bad: such practices should not be banned just because they could be abused. Legislation governing the use of PGD should elimin-ate such problems. In the UK, the Human Fertilisation and Embryology Authority (HFEA), which licenses all IVF practices, has banned embryo sexing for family balancing and they license all PGD centers. It must be remembered that it is no easy task to undergo PGD, mainly because the IVF procedure is so invasive and the pregnancy rate is low. If couples wished to select their baby, the cheaper and simpler route would be pre-natal diagnosis, where many diseases could be diag-nosed at one time.

Chapter 14: Preimplantation genetic diagnosis
250
The future of PGD PGD is more complicated than originally thought: the concept that a single cell would be representative of the rest of the embryo has been confused and compounded by the discovery of high levels of chromosomal mosai-cism in human embryos. Unfortunately, misdiagnoses do occur, mainly due to chromosomal mosaicism, allele dropout or contamination (possible from cumu-lus or sperm cells).
Cost is also an important consideration, as some single cell diagnoses are expensive techniques and array technology is currently very expensive. For example, the cost of FISH probes can equal the cost of an IVF treatment cycle, which makes PGD a very expensive technique. In the UK, some health author-ities have paid for PGD cycles, and in other countries government or health insurance funds are available; if patients have to meet the cost they may opt for prenatal diagnosis .
Data from the ESHRE PGD consortium shows that the delivery rate per cycle for PGD is similar to that seen in IVF, even though PGD patients are normally fertile. Th erefore, any center or patient embarking on PGD has to be aware that the diagnosis may not be 100% accurate due to mosaicism and allele dropout, and that the chance of an unaff ected baby aft er one cycle is low. Th e patients also have to decide whether undertaking an IVF cycle is more or less traumatic than natural con-ception and prenatal diagnosis. We have found that the natural pregnancy rate for patients registered for PGD is very high, as most of them have the alternative of pre-natal diagnosis.
Th e most logical, and highly motivated group of patients to treat by PGD are those who are infertile or who have experienced repeated miscarriages. Patients who carry chromosome abnormalities are one of the most diffi cult groups of patients to treat, due to limita-tions of available probes and the high levels of abnor-mal embryos they produce.
Additional techniques for single cell diagnosis include whole genome amplifi cation, where the whole genome is randomly amplifi ed to allow several diagno-ses to be performed on a single cell. Th is allows exam-ination of several mutations for a disease from one cell, and haplotyping can also be performed to ensure that the diagnosed DNA is embryonic. Products of whole genome amplifi cation may also be used to examine chromosomes using array CGH. For CGH, nick translation is used to label embryonic DNA with
a fl uorochrome (e.g., red), and some control DNA is labeled with a green fl uorochrome (control samples may be provided by the manufacturer in order to elim-inate a source of error). Both samples are cohybridized onto a control metaphase plate (metaphase CGH) or an array platform (array-CGH) and the ratio of red to green labeling indicates which chromosomes or parts of chromosomes are in excess or missing from the embryo. Th e advantage of array technology is that multiple defects can be assessed in a single test, com-pared to FISH, which requires a specifi c probe for each chromosome or region, and PCR, where a specifi c pri-mer is required for each sequence of interest.
Many couples around the world opt for PGD as an alternative to prenatal diagnosis, and several thou-sand babies have been born. Although it is a demand-ing technique that requires a fully equipped molecular biology laboratory, highly skilled molecular biologists and close collaboration with clinical geneticists, tech-nical breakthroughs over the past decade continue to make PGD a very real alternative for couples at risk. Hopefully, with improvements in IVF and single cell diagnosis, the range of diseases that can be diagnosed at the single cell level and the number of patients who can be treated will increase .
Further reading Books Elder K , Cohen J (eds.) ( 2007 ) Human Preimplantation
Embryo Evaluation and Selection . Informa Press , London . Harper J (ed.) ( 2009 ) Preimplantation Genetic Diagnosis , 2nd
edn. Cambridge University Press . Harper JC, Coonen E, De Rycke, et al. (2010) ESHRE PGD
Consortium data collection X: Cycles from January to December 2007 with pregnancy follow-up to October 2008, Human Reproduction Sep 2. [Epub ahead of print]
Harper JC, Harton G (2010) Th e use of arrays in PGD/PGS. Fertility and Sterility 94(4): 1173–1177.
Prenatal Diagnosis – special issue, December 1998 , 18(13). Issue dedicated to preimplantation genetics and diagnosis.
Publications Coonen E , Harper JC , Ramaekers FCS , et al. ( 1994 )
Presence of chromosomal mosaicism in abnormal preimplantation embryos detected by fl uorescent in situ hybridisation . Human Genetics 54 : 609 –615.
Delhanty JDA , Harper JC , Ao A , Handyside AH , Winston RML ( 1997 ) Multicolour FISH detects frequent chromosomal mosaicism and chaotic division in normal

Chapter 14: Preimplantation genetic diagnosis
251
preimplantation embryos from fertile patients . Human Genetics 99 : 755 –760.
Gianaroli L , Magli MC , Ferraretti AP , Munné S ( 1999 ) Preimplantation diagnosis for aneuploidies in patients undergoing in-vitro fertilization with a poor prognosis: identifi cation of the categories for which it should be proposed . Fertility and Sterility 72 (5): 837 –844.
Harper JC , Coonan E , Handyside AH, et al. ( 1995 ) Mosaicism of autosomes and sex chromosomes in morphologically normal, monospermic preimplantation human embryos . Prenatal Diagnosis 15 : 41 –49.
Hertig AT , Rock J , Adams EC ( 1956 ) A description of 34 human ova within the fi rst 17 days of development . American Journal of Anatomy 98 : 435 .
James RM , West JD ( 1994 ) A chimaeric animal model for confi ned placental mosaicism . Human Genetics 93 : 603 –604.
Munné S , Wells D ( 2003 ) Questions concerning the suitability of comparative genomic hybridization for preimplantation genetic diagnosis . Fertility and Sterility 80 (4): 871 –872; discussion 875.
Platteau P , Staessen C , Michiels A , et al. ( 2006 ) Which patients with recurrent implantation failure aft er IVF benefi t from PGD for aneuploidy screening? Reproductive Biomedicine Online 12 (3): 334 –339.
Sermondade N , Mandelbaum J ( 2009 ) Mastenbroek controversy or how much ink is spilled on preimplantation genetic screening subject? Gynécologie Obstétrique & Fertilité 37 (3): 252 –256.
Verlinsky Y , Cieslak J , Freidine M , et al. ( 1995 ) Pregnancies following pre-conception diagnosis of common aneuploidies by fl uorescent in situ hybridisation . Molecular Human Reproduction 10 : 1927 –1934.
Verlinsky Y , Strom C , Cieslak J , et al. ( 1996 ) Birth of healthy children aft er preimplantation diagnosis of common aneuploidies by polar body fl uorescent in situ hybridisation analysis . Fertility and Sterility 66 : 126 –129.
Wells D ( 2007 ) Future genetic and other technologies for assessing embryos. In: Elder K , Cohen J (eds.) Human Preimplantation Embryo Evaluation and Selection . Informa Press , London .

Chapter
1
252
Epigenetics and assisted reproduction John Huntriss
Introduction During mammalian development the growth of the fetus is regulated by genetic information that is inher-ited from both the sperm and the oocyte. Apart from the clear diff erences that are associated with the X and Y chromosomes, the parental genetic contributions to the embryo also diff er via a system of “epigenetic” marks. Th is functional non-equivalence between the parental genomes, how gametes and preimplantation embryos are reprogrammed, and how these delicate processes may be aff ected by assisted reproductive technology and infertility will be described in this chapter. A full understanding of the cellular and molecular biology of human reproduction must include a study of epigenet-ics and genomic imprinting.
Epigenetics Epigenetics is an additional “layer” of information that complements the information in the genomic DNA sequence; it is essentially a marking system that regu-lates gene expression and hence the phenotype of the cell. An epigenetic mark is a chemical modifi cation of the DNA bases themselves, or a modifi cation that leads to a change in chromatin structure. Th ese modifi ca-tions aff ect the way that sequence information is read by the cell by infl uencing interaction with transcrip-tion complexes and other regulatory factors. Th is level of gene expression may be termed the “epigenotype”; an incorrect representation of the information, such as occurs in an epigenetic disease, is an “epimutation.”
Th e biological mechanisms that are epigeneti-cally regulated include X-chromosome inactivation, parent-of-origin eff ects of genomic imprinting, as well as tissue-specifi c and age-dependent DNA modifi -cation. Epigenetic information is also responsible for the phenotypic variability of somatic cells within an organism, controlling how tissues and cells in the body
defi ne themselves. For example, within a human indi-vidual, the genotype (the gene complement) is the same for diff erent types of cell (e.g., a muscle cell or a liver cell) yet the cellular functions and phenotypes are very diff erent. Although the DNA sequence within these diff erent cells is identical, the repertoire of expressed genes diff ers greatly between cell types, a diff erence that is essential in determining the specifi c functions of diff erent cells.
Epigenetic marks Th e mechanisms that contribute to imprinting include DNA methylation , histone modifi cation and RNA-mediated (transcriptional) mechanisms. DNA methy-lation is stable but reprogrammable, heritable, and aff ects the regulation of gene expression. Th is type of epigenetic mark is believed to involve methylation of CpG dinucleotides around certain genes. For example, a gene whose active expression is required in a liver cell may be unmethylated across the majority of CpG sites within the vicinity of its genomic sequence, whereas a gene that needs to be silenced in the liver may be heavily methylated, repressing transcription by “lock-ing” the genes within an inaccessible heterochromatin structure.
Histone proteins are important in DNA pack-aging; they can be covalently modifi ed by a number of post-translational modifi cations that signifi cantly aff ect whether chromatin conformation is open or closed. “Open” chromatin is accessible to DNA replica-tion and transcription (gene expression), and “closed” chromatin is not accessible. Chromatin conformation is aff ected by modifi cation of histone tails via methyla-tion, acetylation, phosphorylation etc., especially those of H3 and H4 histones. Each diff erent modifi cation or combination of modifi cations aff ects chromatin struc-ture, and thus gene expression, diff erently. In many
15
In-Vitro Fertilization: Th ird Edition , ed. Kay Elder and Brian Dale. Published by Cambridge University Press. © K. Elder and B. Dale 2011.

Chapter 15: Epigenetics and assisted reproduction
253
situations, both DNA methylation and the histone modifi cation “code” probably contribute to the overall process of epigenetic regulation.
Histone nomenclature
Histone modifi cations are named by using:
the name of the histone (e.g., H3) • the abbreviation for the amino acid and its position • within the modifi ed histone protein (e.g., K9 for lysine at position 9) the type of epigenetic modifi cation (e.g., “me” for • methylation) the extent of the particular modifi cation (e.g., mono, • di or tri-methylation: me1, me2, me3).
Genomic imprinting Genomic imprinting is the exclusive expression of only one of the parental alleles of a gene, a unique mode of gene expression that aff ects the growth and devel-opment of the fetus according to whether an allele of a particular imprinted gene is inherited paternally or maternally. In normal circumstances, imprinting exerts fi ne control over the growth of the developing conceptus via the placenta. A number of human dis-eases involve abnormal regulation of imprinted genes or “parent of origin” eff ects, and disruption of imprint-ing can lead to cancer (Walter and Paulsen, 2003 ; Holm et al ., 2005 ). Genomic imprinting is particularly sus-ceptible to disruption during early preimplantation development, and is therefore vulnerable to potential aberrations that may be introduced through certain assisted reproductive technology (ART) procedures.
Approximately 80 mammalian genes that show imprinted (monoallelic) expression have been described to date, although more have been predicted by bioinformatic analysis. Genomic imprinting is regulated by imprinting control regions or imprint-ing centers (ICRs or ICs) that acquire epigenetic marks such as DNA methylation upon passage through the germline. Imprinted genes have diff erent methylation patterns (diff erentially methylated regions, DMRs) on the maternal and paternal alleles that play an import-ant regulatory role. DMRs typically consist of stretches of diff erentially methylated CpG sites that are close to an imprinted gene, and this epigenetic information regulates allele-specifi c gene expression. A germline DMR will therefore have a diff erent methylation pat-tern in the sperm than in the oocyte, and this diff er-ential marking will be recognized in the zygote and preimplantation embryo. Th e majority of imprinted
genes are located in clusters within the genome, and are regulated by ICRs that regulate all or most of the imprinted genes in a cluster.
Figure 15.1 shows a simplifi ed representation of diff erential allele marking of an imprinted gene in the germline, which leads to mono-allelic expression in somatic tissue of the off spring. Th e paternal allele is not methylated in sperm (left ), whilst the maternal allele is methylated in the oocyte (right). Th is diff er-ential methylation imprint persists aft er fertilization and early development. Th e epigenetic mark (methyla-tion) placed on the allele during oogenesis silences the maternal allele in the off spring and only the paternal allele is transcribed to mRNA (bent arrow ) .
Imprinted genes are also believed to play a role in the parent–off spring confl ict model (Moore and Haig, 1991 ), a theory proposing that the parental alle-les of these loci have diff erent interests with respect to regulation of fetal, placental and neonatal growth; i.e., the paternal genome will fi ght for the biggest size and health of the current litter (his litter), whereas the maternal genome will try to counter or moderate this eff ect in order to reduce current nutritional strain on herself and ensure that she will be able to raise future litters. Th is hypothesis is reinforced by the fact that many imprinted genes regulate growth of the fetus and placenta. Interestingly, disruption of certain imprinted mouse genes by knock-out experiments also aff ects maternal nurturing behavior. Imprinting may also pre-vent parthenogenesis, since it ensures that both paren-tal genomes are necessary for an embryo to develop to term (Kono, 2009 ).
Epigenetic reprogramming in the germline Th e mature oocyte and sperm are highly specialized cells, and this means that their cellular specialization needs a signifi cant amount of epigenetic information. Information inherited from the previous generation must be erased in primordial germ cells, so that new epigenetic information may be subsequently added according to whether the primordial germ cell is des-tined to become an oocyte or a sperm cell ( Figure 15.2 ). Extensive epigenetic reprogramming is therefore required in the primordial germ cells (erasure) and during gametogenesis (establishment) (see Morgan et al ., 2005 for review). Th e most complete information available is for reprogramming via DNA methylation , but other epigenetic marks (e.g., the histone code) are
Histone modifi cations are named by using:
the name of the histone (e.g., H3) • the abbreviation for the amino acid and its position •within the modifi ed histone protein (e.g., K9 for lysine at position 9) the type of epigenetic modifi cation (e.g., “me” for •methylation) the extent of the particular modifi cation (e.g., mono, •di or tri-methylation: me1, me2, me3).

Chapter 15: Epigenetics and assisted reproduction
254
also reprogrammed in primordial germ cells and dur-ing gametogenesis.
Erasure Reprogramming events have been studied extensively in the mouse (reviewed in Constância et al ., 1998 ). Mouse primordial germ cells (PGCs) are identifi able by embryonic day E7.5, and they then migrate to the genital ridge by day E10.5–11.5, where they form the gonadal primordia. At this stage, primordial germ cells still retain methylation patterns derived from the oocyte and sperm, and any of their respective modifi cations from early development. At day E13.5, male germ cells enter into mitotic arrest and female germ cells enter meiotic prophase. Between days E10.5 and E13.5 DNA is globally demethylated in the PGCs of both sexes, at imprinted genes and also at many DNA elements including IAPs (retroviral elements containing long terminal repeats), Line 1 sequences (long interspersed nucleotide elements), direct repeats and non-CpG island genes. Each elem-ent displays a unique erasure profi le, and diff erent degrees of demethylation occur between the various
elements (see Lees-Murdock and Walsh, 2008 for review).
Establishment Aft er methylation has been erased, the germ cells that are still diploid undergo de novo methylation. In mouse gametogenesis , the majority of DNA remethylation occurs around day E15.5 in both sexes, although timing does vary between the vari-ous elements; timing also diff ers between the male germline and female germline (Lees-Murdock and Walsh, 2008 ). IAPs, Line 1 sequences and other elem-ents are fully methylated in mature sperm. Certain genes escape this remethylation, for example those containing CpG islands (genomic regions with high densities of CpG nucleotides, which are distinct from the smaller diff erentially methylated CpG sites of imprinted genes ).
Imprinting marks are established according to the sex of the individual (i.e., whether the germ cell is an oogonium or spermatogonium), and most of the imprinted genes acquire methylation in the female germline. Th e H19 imprinted gene is one that is
Paternal allele unmethylated in sperm Maternal allele methylated in oocytes
Maternal allele
Maternal allele
Only paternal allele transcribed
Somatic tissues
CH3
CH3
Oocyte
Fertilization
Sperm
Paternal allele
Paternal allele
Figure 15.1 Epigenetic information from the germline regulates genomic imprinting.

Chapter 15: Epigenetics and assisted reproduction
255
methylated in the male germline. Despite the fact that epigenetic information has been erased in the primor-dial germ cells, suffi cient underlying epigenetic infor-mation remains so that the parental origin of all of the alleles can still be distinguished: for H19 in the male germline, the DMR on the paternal allele is completely remethylated by E15.5, whilst the maternal DMR is remethylated around birth.
In the female germline, maternal DMRs remain hypomethylated until the pachytene stage of meiosis I in the postnatal growing oocyte. Maternal methyla-tion imprints are acquired during oocyte growth, and the DMRs for diff erent imprinted genes appear to be remethylated at diff erent times. Th us imprinted genes Snrpn , Znf127 , Ndn are methylated by the primary fol-licle stage, Peg3 and Igf2r genes are methylated by the
Figure 15.2 The life cycle of genomic imprinting (adapted from Morgan et al ., 2005 ). Imprint erasure, establishment and maintenance are all features of the epigenetic reprogramming cycle that is required for genomic imprinting. In this fi gure, the imprint is via DNA methylation. Extensive reprogramming occurs in the primordial germ cells, erasing the imprints from the previous generation. Imprints are re-established during gametogenesis according to the sex of the embryo, maintained in the embryo, and translated into stable functional diff erences between the parental alleles in the developing conceptus. Extensive epigenetic reprogramming of the paternal pronucleus occurs in zygotes.

Chapter 15: Epigenetics and assisted reproduction
256
secondary follicle stage, and the Impact gene is methyl-ated by the antral follicle stage. As in the male germline, some underlying epigenetic signal is retained since the maternally inherited alleles of Snrpn , Zac1 and Peg1 genes are methylated before the paternally inherited alleles (Obata and Kono, 2002 ; Lucifero et al ., 2004 ; Hiura et al ., 2006 ).
Th e DNA methyltransferases (Dnmts) play a major role in the establishment of methylation imprints dur-ing gametogenesis ; the de novo methyltransferases Dnmt3a, Dnmt3b and the related protein Dnmt3L are expressed coordinately and work together to establish methylation imprints during oogenesis. Methylation at imprinted genes in oocytes appears to be depend-ent on the size of the oocyte, and it has been sug-gested that methylation is linked to the accumulation of DNA methyltransferases during the growth phase. In oocytes, histone H3K4 must be demethylated (via KDM1B histone demethylase) before the DNA methy-lation imprints are established; transcription through imprinted gene DMRs keeps chromatin domains open and accessible for methylation ( Figure 15.3 ).
Parental genomes are packaged diff erently in the gametes and during the fi rst stages of fertilization. Th e maternal genome from the oocyte is nucleosomal, whilst the paternal genome from the sperm is con-densed and packaged by protamines, which are quickly lost and replaced by histones aft er sperm entry into the oocyte. During pronuclear maturation, the paternal pronucleus undergoes signifi cant chromatin reorgan-ization, with active demethylation during the tran-sition from PN0 to PN5 and metaphase, followed by
histone acquisition towards the end of PN maturation. Th e male pronucleus gathers epigenetic marks such as H3K9me1 and me2, and H3K27me2/3, whilst the maternal pronucleus, largely rich in histone epigenetic marks, remains relatively unchanged from PN0 to PN5. Th is diff erence between male and female pronuclei is referred to as “epigenetic asymmetry.” By the end of pronuclear maturation (PN4/PN5), DNA methylation (5MeC) is removed from the male pronucleus. Further diff erential histone modifi cations between the parental genomes are observed in the early embryo (reviewed in Corry et al ., 2009 ).
DNA methylation is again reprogrammed during preimplantation development (reviewed in Reik et al ., 2001 ), with initial erasure and then de novo DNA methylation towards the end of the preimplantation period as diff erentiation occurs. Epigenetic diff er-ences are seen between the inner cell mass (ICM) and trophectoderm of the blastocyst: H3K27me1, me2 and me3 are present predominantly in the ICM (reviewed in Morgan et al ., 2005 ). Th e ICM and trophectoderm cell lineages of the mouse blastocyst are diff erentially marked by histone H3 lysine 27 methylation at key developmental genes .
Species-specifi c diff erences in mammalian reprogramming
Assessment of 5-methylcytosine immunostaining in diff erent mammalian zygotes shows:
The paternal pronucleus undergoes demethylation • in mouse, human and bovine zygotes, but not in sheep and rabbit zygotes.
Assessment of 5-methylcytosine immunostaining indiff erent mammalian zygotes shows:
The paternal pronucleus undergoes demethylation• in mouse, human and bovine zygotes, but not insheep and rabbit zygotes.
Figure 15.3 Regulation of imprinting in the mouse female germline. The approximate sequence of gene-specifi c imprint establishment in the mouse female germline is illustrated, showing factors that are relevant to the reprogramming events. Imprinted genes receive methyla-tion imprints at diff erent times during the oocyte growth phase. The lower panel shows key reprogramming phases that occur at imprinted genes and in the genome as a whole. GV = germinal vesicle; MII = metaphase II; PN = pronuclear; ICM = inner cell mass; TE = trophectoderm.

Chapter 15: Epigenetics and assisted reproduction
257
• Demethylation of the male pronucleus occurs more slowly in rat than in mouse. The male pronucleus is completely demethylated • within 4 hours of fertilization in the mouse, and pas-sive loss of methylation in the embryo continues up to the morula stage.
Imprint maintenance during preimplantation development Dynamic changes take place in the level of genomic DNA methylation during preimplantatio n develop-ment. Th e imprints that were established in the male and female germline must be recognized and main-tained during global DNA demethylation in the early embryo, so that the imprinting mark may be propagated during later development in order to allow expression of the appropriate allele.
Factors involved in imprint maintenance
Proteins essential for early development that are expressed by the mammalian oocyte (maternal eff ect genes) perform essential functions in maintaining methylation at imprinted loci :
DNA methyltransferase protein has two forms, • Dnmt1s (somatic form) and Dnmt1o (an oocyte-specifi c form). Dnmt1 maintains genomic imprints at a time when • there is genome-wide erasure of DNA methylation. Maternally-derived Dnmt1 proteins (Dnmt1o and/• or Dnmt1s) probably maintain methylation imprints at imprinted genes during the fi rst cell cycle . Zygotic Dnmt1s maintains the imprints from the • two-cell stage onward. Stella/PGC7 is required to maintain methylation at • several maternally expressed imprinted genes, and also to maintain the paternally derived methylation imprints at H19 and Rasgrf1 . The zinc fi nger protein Zfp57 maintains both pater-• nal and maternal methylation imprints at multiple imprinted regions after fertilization.
Depletion of Zfp57 from oocytes and embryos –results in loss of methylation imprints at a number of paternally methylated and methylated DMRs. Zfp57 is also required to establish the germline –methylation imprint at the Snrpn gene during oogenesis , but at no other tested loci.
Exactly how some unmethylated CpG sites (such as unmethylated DMRs) are protected from remethyla-tion events towards the end of preimplantation devel-opment is unclear. However, mice lacking the CpG
binding protein CGBP (a transcriptional activator protein that binds unmethylated CpG sites) die dur-ing the peri-implantation stages, and embryonic stem cells that lack this protein are hypomethylated. CGBP or related factors may therefore be involved .
Finally, the imprints must be “read” or recognized so that the alleles can be appropriately expressed; for example, the zinc fi nger protein CTCF regulates gen-omic imprinting by binding diff erentially methylated regions in a manner that is dictated by the methylation pattern.
Epidemiological data in ART Handling human gametes and embryos outside the human body could potentially introduce stresses that might later be manifested during development. In add-ition, ART procedures are performed during a period when dynamic and essential epigenetic reprogram-ming events are occurring on the genome of the gamete or embryo during normal development. Not surpris-ingly, data surrounding the subject is fragmented and incomplete, fraught with diff erences in sample size and selection criteria. At the time of writing, more than 10 million healthy children have been born aft er ART, bearing testimony to this remarkable technology of the twentieth century. However, developmental abnormal-ities must be rigidly monitored, and research on the epigenetic regulation of human gametes and embryos is fundamental. A summary of some of the syndromes that have been noted in ART children is presented below, together with examples of potential ART pathways that might possibly induce epigenetic mistakes.
Beckwith–Wiedemann syndrome (BWS) and ART BWS is caused by faulty expression of the imprinted genes on chromosome 11q15.5, and occurs sporadic-ally aft er natural conception at an approximate rate of 1 in 15 000 births. Th e syndrome is associated with large pre/postnatal growth (approximately 160% increase), childhood tumors (commonly Wilms’ tumor), mac-roglossia, exomphalos, organomegaly, hypoglycemia and hemihypertrophy. Approximately 20% of cases show paternal uniparental disomy of the 11q15.5 chromosome, and overexpression of the imprinted gene IGF2 is found in 80% of cases.
BWS registries rev eal that the syndrome has been observed in children conceived aft er assisted
• Demethylation of the male pronucleus occurs more slowly in rat than in mouse. The male pronucleus is completely demethylated •within 4 hours of fertilization in the mouse, and pas-sive loss of methylation in the embryo continues up to the morula stage.
Proteins essential for early development that are expressed by the mammalian oocyte (maternal eff ect genes) perform essential functions in maintaining methylation at imprinted loci :
DNA methyltransferase protein has two forms, •Dnmt1s (somatic form) and Dnmt1o (an oocyte-specifi c form). Dnmt1 maintains genomic imprints at a time when •there is genome-wide erasure of DNA methylation. Maternally-derived Dnmt1 proteins (Dnmt1o and/•or Dnmt1s) probably maintain methylation imprints at imprinted genes during the fi rst cell cycle . Zygotic Dnmt1s maintains the imprints from the •two-cell stage onward. Stella/PGC7 is required to maintain methylation at •several maternally expressed imprinted genes, and also to maintain the paternally derived methylation imprints at H19 and Rasgrf1. The zinc fi nger protein Zfp57 maintains both pater-•nal and maternal methylation imprints at multiple imprinted regions after fertilization.
Depletion of Zfp57 from oocytes and embryos –results in loss of methylation imprints at a number of paternally methylated and methylated DMRs. Zfp57 is also required to establish the germline –methylation imprint at the Snrpn gene during oogenesis , but at no other tested loci.

Chapter 15: Epigenetics and assisted reproduction
258
reproduction . Th e major epimutation identifi ed in these children is hypomethylation of the KvDMR1, a methylated imprinting control element on maternal (oocyte) chromosome 11p15.5, at the promoter region of the KCNQ1OT1 gene; 24 out of 25 ART children with BWS presented with hypomethylation at KvDMR1 (Lim et al ., 2009 ). Th e mechanism behind this methy-lation defect is currently being investigated.
To date, over sixty ART-conceived BWS cases have been reported (Maher et al ., 2003 ; DeBaun et al ., 2003 ; Gicquel et al ., 2003 ; Halliday et al ., 2004 ; Sutcliff e et al ., 2006 ). Th e cause of the BWS epimutation could not be linked to any particular aspect of ART or infertility, but a study that identifi ed nineteen ART-conceived chil-dren from a BWS registry found that the only common parameter that could be identifi ed was the use of ovar-ian stimulation (Chang et al ., 2005 ). Th is aspect will be covered in more detail later in this chapter.
A more generalized epigenetic defect may be associated with ART (such as ineffi cient maintenance of imprints in the preimplantation embryo), since epigenetic defects outside of KvDMR1 at the DMRs for the imprinted genes IGF2R , SNRPN and PEG1/MEST have been identifi ed in a small number of ART-conceived BWS patients (Rossignol et al ., 2006 ). However, widespread epigenetic errors are also seen in naturally conceived BWS patients. Hypomethylation at KvDMR1 has also been observed in three out of eighteen normal children that were conceived by ART (Gomes et al ., 2009 ), supporting the idea that there may be more “global” epigenetic defects associ-ated with ART. Maternal hypomethylation syndrome has been recently recognized as an imprinting syn-drome that features hypomethylation at multiple loci (Mackay et al ., 2006 , Boonen et al ., 2008 ). Th e study by Rossignol et al . ( 2006 ) therefore suggests that this hypomethylation syndrome, or related causes, might be associated with assisted reproduction .
Angelman syndrome and ART Angelman syndrome (AS) is a rare disease that aff ects approximately 1 in 15 000 newborns, caused by a spectrum of genetic defects, one of which is a defect at the chromosome 15 imprinting center. An increased incidence of AS has been reported following the use of ICSI (Cox et al ., 2002 ; Ørstavik et al ., 2003 ; Ludwig et al . 2005 ; Sutcliff e et al ., 2006 ); it has been suggested that some aspects of the ICSI technique might be responsible for the epigenetic abnormality, for example
introduction of the sperm acrosome and its digestive enzymes into the ooplasm, ICSI-induced mechanical stress on the oocyte, or disruption of cellular factors or structures required for correct imprinting of chromo-some 15. Paternal RNA-mediated mechanisms must also be considered. Loss of methylation at the SNRPN imprinting control region was observed in three cases (normally accounting for less than 5% of all AS cases, occurring in only 1 in 300 000 newborns). Conversely, no SNRPN methylation defects were observed in a study of 92 children born aft er ICSI (Manning et al ., 2000 ).
Retinoblastoma and ART Retinoblastoma is a childhood tumor of the retina. Th e RB1 gene acts as a tumor suppressor, and inacti-vation of the RB1 gene by epigenetic mechanisms (such as hypermethylation of the promoter region of the RB1 gene) can lead to tumor development. Retinoblastoma has also been observed aft er ART in several diff erent studies, one of which found a sig-nifi cantly increased risk of retinoblastoma in chil-dren that were conceived by IVF between 1995 to 2007; however, all of the cases arose between 1995 and 2002 and not thereaft er (Marees et al ., 2009 ). Until very recently, the RB1 gene was not thought to be imprinted, and so the incidence of retinoblastoma aft er ART may have been overlooked in some of the surveys of ART and imprinting disorders. However, a recent report has demonstrated that the RB1 gene is preferentially expressed from the maternal allele (Kanber et al ., 2009a ). It is possible that the ART-associated retinoblastoma cases may be caused by aberrant imprinting of the RB1 gene, although there is no data available at present.
Russell–Silver syndrome and ART Russell–Silver syndrome (RSS) features growth retard-ation and learning disabilities, and has been observed in several cases aft er ART. A girl conceived via IVF was reported to have hypermethylation at the PEG1/MEST DMR, although it is not clear whether this methylation defect is responsible for the syndrome (Kagami et al ., 2007 ). In this case, there was normal methylation at the H19 DMR, a region that is typically implicated in Russell–Silver syndrome. Partial hypermethylation at the PEG1/MEST DMR was present in the father, and the authors suggested that IVF treatment may have exac-erbated this pre-existing paternal methylation error. Several other cases of RSS in children conceived by

Chapter 15: Epigenetics and assisted reproduction
259
ART have been reported, but more studies are required to establish whether there is a true association .
ART induced epigenetic mistakes Culture media Certain cell culture medium compositions have been shown to aff ect epigenetic mechanisms and thus the regulation of imprinted genes in mammalian preim-plantation embryos. Non-imprinted genes may also be susceptible, indicating that “global” epigenetic changes may be manifested during cell culture. Specifi c chemi-cals that are present in culture media may also aff ect the epigenetic state of the in-vitro embryo; e.g., ammo-nia may accumulate in culture media as a by-product of embryonic metabolism and from breakdown of the culture medium. Mouse blastocysts cultured in the presence of 300 µM ammonium showed signifi cant upregulation of the H19 imprinted gene (Lane and Gardner, 2003 ). Optimizing culture media is there-fore critical, in order to minimize the risks of introdu-cing epigenetic disease to the in-vitro cultured cell (see Ménézo et al ., 2010 ).
Human embryonic stem cells (hESCs) have been used as a model for understanding epigenetic events in early human development. Like the preimplanta-tion embryo, hESCs are exposed to culture media and micromanipulation procedures that have the potential to alter the epigenetic state of the cell line. Research to date has focused on the epigenetic stability of hESCs, which is an important factor to consider if these cells are to be used to generate diff erentiated cell types for therapeutic application. Detailed studies of imprinted gene expression in hESC lines have identifi ed vari-able imprinting between diff erent cell lines. Global DNA methylation analysis in six hESC lines identifi ed numerous unstable loci (Allegrucci et al ., 2007 ) with methylation changes occurring during cell culture, aft er the stem cell lines were derived and during adap-tation to a serum-free media.
It is not clear whether the variability between hESCs is due to inter-individual diff erences in imprinting that were inherited from the founder embryo, or whether these are truly epigenetic disruptions introduced when the stem cells were derived or during subsequent cul-ture. Other mammalian cell types also undergo epi-genetic changes when cultured in vitro, suggesting that the in-vitro culture environment might induce cellular stress. For example, in-vitro culture of mouse embryonic fi broblasts downregulates the expression of
six imprinted genes via methylation of the respective gene promoters, and the silencing was specifi c to the imprinted genes (Pantoja et al ., 2005 ). It is not known whether this exact event occurs during culture of gam-etes and embryos, but similar gene expression changes have been described. Culture-induced eff ects in mouse preimplantation embryos caused an aberrant expres-sion bias towards the maternal allele of the imprinted Igf2 gene (Ohno et al ., 2001 ). Th ere is also evidence for altered IGF2 expression (Blondin et al ., 2000 ) and for reduced methylation at the imprinted SNRPN locus (Suzuki et al ., 2009 ) in bovine fetuses following in-vitro culture. Immunofl uorescence staining for 5-methylcy-tosine has revealed higher DNA methylation in both mouse and rat embryos developed in vitro compared to in-vivo controls (Zaitseva et al ., 2007 ). Animal stud-ies have shown that the addition of serum to media can result in culture-induced eff ects that persist beyond the preimplantation period, in particular the large off spring syndrome (LOS) , an overgrowth syndrome observed in ruminants conceived following IVF. Th is syndrome is caused by aberrant methylation and upregulation of the IGF2R gene aft er embryo culture in serum-containing media (Young et al ., 2001 ). Serum-induced imprinting defects have also been detected aft er culture of mouse embryos in medium containing fetal calf serum (FCS).
Animal models: imprinting and specifi c culture media compositions
Mouse embryo culture Whitten’s medium
Mouse embryos cultured from the two-cell stage • to the blastocyst showed aberrant expression of the H19 gene, with activation of the normally silent paternal allele; the imprint for this gene may be especially labile (Doherty et al ., 2000 ). Aberrant biallelic expression of fi ve imprinted genes • has been observed in the placenta after in-vitro cul-ture (Mann et al ., 2004 ). The authors suggested that culture-induced disruption of epigenetic mecha-nisms may be more severe in the placenta, as this tis-sue may not be able to restore imprints that are lost during preimplantation development in vitro.
M16 medium/G1/G2
Mouse gametes manipulated and fertilized in M16 medium followed by embryo culture in G1/G2 medium showed downregulation of around two-thirds of placental gene transcripts (Fauque et al ., 2010b ). Imprinted gene expression was also signifi -cantly aff ected. The authors suggested that a memory
Mouse embryo culture Whitten’s medium
Mouse embryos cultured from the two-cell stage•to the blastocyst showed aberrant expression of the H19 gene, with activation of the normally silentpaternal allele; the imprint for this gene may beespecially labile (Doherty et al ., 2000 ). l Aberrant biallelic expression of fi ve imprinted genes•has been observed in the placenta after in-vitro cul-ture (Mann et al., 2004 ). The authors suggested thatlculture-induced disruption of epigenetic mecha-nisms may be more severe in the placenta, as this tis-sue may not be able to restore imprints that are lostduring preimplantation development in vitro.
M16 medium/G1/G2
Mouse gametes manipulated and fertilized in M16medium followed by embryo culture in G1/G2medium showed downregulation of around two-thirds of placental gene transcripts (Fauque et al .,l 2010b ). Imprinted gene expression was also signifi -cantly aff ected. The authors suggested that a memory

Chapter 15: Epigenetics and assisted reproduction
260
of the epigenetic insult that was experienced during embryo culture was maintained, with an impact upon the placenta later in development.
HTF (Quinn’s Advantage) Mouse embryos showed aberrant • H19 expression when compared to in-vivo derived embryos (Li et al ., 2005 ). Embryonic stem cells derived from these embryos also had defective imprinting of Igf2 / H19 genes and histone modifi cations at a regulatory ICR.
Bovine embryo culture Culture of bovine embryos in Charles Rosenkrans 1 • (CR1aa) upregulated expression of the imprinting regulator Dnmt3a methyltransferase . Culture in KSOM containing amino acids caused • the upregulation of the Igf2r gene (Sagirkaya et al ., 2006 ).
ICSI Th ere is an association between male infertility and epigenetic problems, and the ICSI procedure bypasses natural barriers to fertilization. Injecting epigenetically abnormal sperm could potentially transmit abnormal-ities to the off spring, and, as described above with respect to the Angelman syndrome, the injection procedure also carries the risk of disturbing epigenetic processes in the oocyte (Manning et al ., 2000 ; Qiao et al ., 2009 ).
Immature gametes In view of the evidence that gametes progressively acquire epigenetic information, it is possible that imma-ture gametes do not have the full and correct comple-ment of epigenetic information necessary for normal development. Round spermatids (ROS) are transcrip-tionally active, and introducing their RNAs into the oocyte via ICSI may lead to altered gene expression, either directly or through RNA interference mecha-nisms (Borghol et al ., 2008 ). Ejaculated spermatozoa, elongated spermatids and round spermatids all have the correct paternal imprint on chromosome 15q11–13, suggesting that this specifi c paternal imprint is estab-lished in immature testicular spermatids. However, other imprinted regions must be assessed before round spermatid injection may be considered safe .
In-vitro maturation (IVM) and in-vitro growth (IVG) of oocytes Nuclear transfer experiments from staged mouse oocytes indicate that maternal imprints are laid down
progressively throughout oocyte growth, and that genes acquire their imprint at diff erent times; these observations have been supported by further molecu-lar studies. Th is raises the question as to whether in-vitro culture conditions used during IVG and IVM protocols are suitable for the correct establishment of maternal imprints in the oocyte. For example, the use of synthetic serum substitute (SSS) instead of FCS during bovine oocyte maturation led to reduced expression of the DNA methyltransferase Dnmt3a , an important regulator of imprinting in the germline and during early development (Sagirkaya et al ., 2007 ).
Clearly the technologies of oocyte in-vitro growth and manipulation must be fully researched with respect to maternal imprint establishment and stability, espe-cially where these methods are applied for human fer-tility treatment. Some genes may be more susceptible to defects in imprint establishment during in-vitro growth/maturation of human oocytes, and there may be variable stability of imprints once established.
Controlled ovarian hyperstimulation (COH) Evidence from both animal and human studies sug-gests that superovulation can cause epigenetic errors in assisted reproduction . Ovarian stimulation may induce oocyte maturation during an inappropriate time frame, or in a cellular and developmental con-text that is incompatible with achieving complete epigenetic programming of the oocyte, thus pushing lower quality oocytes to maturity. As indicated earl-ier, maternal imprints are established at diff erent times during the oocyte growth phase, and there is further evidence that imprinted gene methylation in oocytes is size-dependent. Superovulation could override this stepwise, progressive growth-dependent process and instead recruit young follicles that have not correctly established their imprinting during maturation.
Infertility and epigenetics Infertility in certain cases is due to defects in gameto-genesis ; since gametogenesis requires coordination of numerous cellular and molecular events, including epigenetic programming, it follows that that some cases of infertility may be associated with epigenetic defects. Imprinting defects in infertility may be a result of defects in gene expression, or due to mutation in the DNA methylation machinery of the gametes. Global DNA methylation analysis techniques have indicated that poor quality human sperm may have defective
of the epigenetic insult that was experienced duringembryo culture was maintained, with an impact uponthe placenta later in development.
HTF (Quinn’s Advantage) Mouse embryos showed aberrant • H19 expressionwhen compared to in-vivo derived embryos (Li et al ., 2005 ). Embryonic stem cells derived from theselembryos also had defective imprinting of Igf2 / H19genes and histone modifi cations at a regulatory ICR.
Bovine embryo culture Culture of bovine embryos in Charles Rosenkrans 1•(CR1aa) upregulated expression of the imprintingregulator Dnmt3a methyltransferase . Culture in KSOM containing amino acids caused•the upregulation of the Igf2r gene (Sagirkaya r et al .,l 2006 ).

Chapter 15: Epigenetics and assisted reproduction
261
erasure of methylation (Houshdaran et al ., 2007 ). Th e epigenetic status of the sperm may aff ect the outcome of results aft er assisted reproduction, as high “global” sperm DNA methylation has been correlated with improved pregnancy rates (Benchaib et al ., 2005 ). Methylation defects at several imprinted genes have been reported both in oligozoospermic patients and in patients with abnormal protamines (Hammoud et al ., 2009 ). Whether epigenetic disorders are actually inherited from infertile patients who harbor epimuta-tions is not clear. However, it has been reported that DNA methylation defects observed at imprinted loci in ART concepti are associated with mutations in the gene encoding DNMT3L , a gene that is important in imprint establishment, and these were also present in the parental sperm (Kobayashi et al ., 2009 ).
Summary An association between ART and an increased risk of at least some epigenetic disorders must clearly be consid-ered ( Figure 15.4 ), and sophisticated molecular studies that compare the “global” epigenetic status of children born in vivo and those born in vitro are now emerging (Katari et al ., 2009 ; Palermo et al ., 2008 ; Tierling et al .,
2009 ). Studies such as these will help us to understand the molecular processes that are aff ected by ART, and the potential risks associated with each technique. Research techniques must be developed that allow technologies to be rigorously tested, to precisely gauge their eff ect upon the epigenetic development of human gametes and pre-implantation embryos, so that ART protocols can be adapted in order to avoid potential problems. Animal studies are useful in highlighting problems associated with particular ART methods, but there are signifi cant diff erences between humans and other mammals with respect to epigenetic regulation, and in the regulation of imprinting during gametogenesis and early devel-opment. Further research on the epigenetic regulation of human gametes and preimplantation embryos is urgently needed, as well as further research on the safety aspects of existing and emerging ART treatments.
Further reading Reviews Amor DJ , Halliday J ( 2008 ) A review of known imprinting
syndromes and their association with assisted reproduction technologies . Human Reproduction 23 (12): 2826 –2834.
M
F
EMEX
PREIMPLANTATION DEVELOPMENT
PREIMPLANTATION DEVELOPMENTMALE GERM LINE
ROSI ICSI
Cryopreservation Effects
Implantation
Fertilisation
Ovulation growth phase
Erasure
% D
NA
M
ET
HY
LAT
ION
primordial germ cell
ART PROCEDURESASSOCIATED WITHEPIGENETIC ERRORS:
FEMALE GERM LINE
primordial germ cell
Maintenance at differential methylation at imprinted genes Demethylation Demethylation Demethylation
Stress
In Vitro Growth Superovulation ART PROCEDURES ASSOCIATED WITH EPIGENETIC ERRORS:
In Vitro Maturation
Ooplasmic Transfer Culture media?
Establishment
Culture media ART PROCEDURES ASSOCIATED WITH EPIGENETIC ERRORS: Blastocyst Culture
M F
Figure 15.4 Major DNA methylation reprogramming events during mammalian gametogenesis and preimplantation development shown together with a summary of the assisted reproductive technology (ART) procedures that are associated with epigenetic errors. The methyla-tion reprogramming panel (center panel, adapted from Reik et al. , 2001) indicates the level of methylation in male (M) and female (F) gametes (left side), and also in the paternally inherited (M) and the maternally inherited genomes (F) after fertilization, during preimplantation devel-opment (right side). The timing and nature of these reprogramming events varies between species. The dashed lines indicate the mainten-ance of diff erential methylation at imprinted genes during preimplantation development. The genome is remethylated diff erentially within the blastocyst in the embryonic (EM) and extraembryonic lineages (EX). Figure reprinted with permission from Huntriss and Piction, 2008.

Chapter 15: Epigenetics and assisted reproduction
262
Gosden R , Trasler J , Lucifero D , Faddy M ( 2003 ) Rare congenital disorders, imprinted genes, and assisted reproductive technology . Lancet 361 (9373): 1975 –1977.
Huntriss J , Picton HM ( 2008 ) Epigenetic consequences of assisted reproduction and infertility on the human preimplantation embryo . Human Fertility 11 (2): 85 –94.
Maher ER , Afnan M , Barratt CL ( 2003 ) Epigenetic risks related to assisted reproductive technologies: epigenetics, imprinting, ART and icebergs? Human Reproduction 18 (12): 2508 –2511.
Manipalviratn S , DeCherney A , Segars J ( 2009 ) Imprinting disorders and assisted reproductive technology . Fertility and Sterility 91 (2): 305 –315.
Research papers Abeyta MJ , Clark AT , Rodriguez RT , et al . ( 2004 ) Unique
gene expression signatures of independently-derived human embryonic stem cell lines . Human Molecular Genetics 13 : 601 –608.
Adewumi O , Afl atoonian B , Ahrlund-Richter L et al . ( 2007 ) Characterization of human embryonic stem cell lines by the International Stem Cell Initiative . Nature Biotechnology 25 : 803 –816.
Albert M , Peters AH ( 2009 ) Genetic and epigenetic control of early mouse development . Current Opinion in Genetics and Development 19 (2): 113 –121.
Allegrucci C , Wu YZ , Th urston A , et al . ( 2007 ) Restriction landmark genome scanning identifi es culture-induced DNA methylation instability in the human embryonic stem cell epigenome . Human Molecular Genetics 16 : 1253 –1268.
Anckaert E , Adriaenssens T , Romero S , Dremier S , Smitz J ( 2009a ) Unaltered imprinting establishment of key imprinted genes in mouse oocytes aft er in vitro follicle culture under variable follicle-stimulating hormone exposure . International Journal of Developmental Biology 53 (4): 541 –548.
Anckaert E , Adriaenssens T , Romero S , Smitz J ( 2009b ) Ammonium accumulation and use of mineral oil overlay do not alter imprinting establishment at three key imprinted genes in mouse oocytes grown and matured in a long-term follicle culture . Biology of Reproduction 81 (4): 666 –673.
Anteby I , Cohen E , Anteby E , BenEzra D ( 2001 ) Ocular manifestations in children born aft er in vitro fertilization . Archives of Ophthalmology 119 (10): 1525 –1529.
Apostolidou S , Abu-Amero S , O’Donoghue K, et al . ( 2007 ) Elevated placental expression of the imprinted PHLDA2 gene is associated with low birth weight . Journal of Molecular Medicine 85 : 379 –387.
Benchaib M , Braun V , Ressnikof D , et al . ( 2005 ) Infl uence of global sperm DNA methylation on IVF results . Human Reproduction 20 : 768 –773.
Beaujean N , Hartshorne G , Cavilla J , et al . ( 2004 ) Non-conservation of mammalian preimplantation methylation dynamics . Current Biology 14 (7): R266 –267.
Bell AC , Felsenfeld G ( 2000 ) Methylation of a CTCF-dependent boundary controls imprinted expression of the Igf2 gene . Nature 405 (6785): 482 –485.
Bliek J , Terhal P , van den Bogaard MJ , et al . ( 2006 ) Hypomethylation of the H19 gene causes not only Silver–Russell syndrome (SRS) but also isolated asymmetry or an SRS-like phenotype . American Journal of Human Genetics 78 : 604 –614.
Blondin P , Farin PW , Crosier AE , Alexander JE , Farin CE ( 2000 ) In vitro production of embryos alters levels of insulin-like growth factor-II messenger ribonucleic acid in bovine fetuses 63 days aft er transfer . Biology and Reproduction 62 (2): 384 –389.
Boissonnas CC , Abdalaoui HE , Haelewyn V , et al . ( 2010 ) Specifi c epigenetic alterations of IGF2-H19 locus in spermatozoa from infertile men . European Journal of Human Genetics 18 (1): 73 –80.
Boonen SE , Porksen S , Mackay DJ , et al . ( 2008 ) Clinical characterisation of the multiple maternal hypomethylation syndrome in siblings . European Journal of Human Genetics 16 : 453 –461.
Borghol N , Lornage J , Blachere T , Sophie Garret A , Lefevre A ( 2006 ) Epigenetic status of the H19 locus in human oocytes following in vitro maturation . Genomics 87 : 417 –426.
Borghol N , Blachère T , Lefèvre A ( 2008 ) Transcriptional and epigenetic status of protamine 1 and 2 genes following round spermatids injection into mouse oocytes . Genomics 91 (5): 415 –422.
Bourc’his D , Xu GL , Lin CS , Bollman B , Bestor TH ( 2001 ) Dnmt3L and the establishment of maternal genomic imprints . Science 294 (5551): 2536 –2539.
Bourque DK , Avila L , Peñaherrera M , von Dadelszen P , Robinson WP ( 2010 ) Decreased placental methylation at the H19/IGF2 imprinting control region is associated with normotensive intrauterine growth restriction but not preeclampsia . Placenta 31 (3): 197 –202.
Carlone DL , Skalnik DG ( 2001 ) CpG binding protein is crucial for early embryonic development . Molecular and Cellular Biology 21 (22): 7601 –7606.
Carlone DL , Lee JH , Young SR , et al . ( 2005 ) Reduced genomic cytosine methylation and defective cellular diff erentiation in embryonic stem cells lacking CpG binding protein . Molecular and Cellular Biology 25 (12): 4881 –4891.
Cetin I , Cozzi V , Antonazzo P ( 2003 ) Fetal development aft er assisted reproduction – a review . Placenta 24 (Suppl. B): S104 –113.

Chapter 15: Epigenetics and assisted reproduction
263
Chang AS , Moley KH , Wangler M , Feinberg AP , Debaun MR ( 2005 ) Association between Beckwith-Wiedemann syndrome and assisted reproductive technology: a case series of 19 patients . Fertility and Sterility 83 : 349 –354.
Chotalia M , Smallwood SA , Ruf N , et al . ( 2009 ) Transcription is required for establishment of germline methylation marks at imprinted genes . Genes and Development 23 (1): 105 –117.
Ciccone DN , Su H, Hevi S , et al . ( 2009 ) KDM1B is a histone H3K4 demethylase required to establish maternal genomic imprints . Nature 461 (7262): 415 –418.
Coan PM , Burton GJ , Ferguson-Smith AC ( 2005 ) Imprinted genes in the placenta – a review . Placenta 26 : S10 –20.
Constância M , Pickard B , Kelsey G , Reik W ( 1998 ) Imprinting mechanisms . Genome Research 8 (9): 881 –900.
Corry GN , Tanasijevic B , Barry ER , Krueger W , Rasmussen TP ( 2009 ) Epigenetic regulatory mechanisms during preimplantation development . Birth Defects Research C Embryo Today 87 (4): 297 –313.
Cox GF , Burger J , Lip V , et al . ( 2002 ) Intracytoplasmic sperm injection may increase the risk of imprinting defects . American Journal of Human Genetics 1 (1): 162 –164.
Dahl JA , Reiner AH , Klungland A , Wakayama T , Collas P ( 2010 ) Histone H3 lysine 27 methylation asymmetry on developmentally-regulated promoters distinguish the fi rst two lineages in mouse preimplantation embryos . PLoS One 5 (2): e9150 .
DeBaun MR , Niemitz EL , Feinberg AP ( 2003 ) Association of in vitro fertilization with Beckwith-Wiedemann syndrome and epigenetic alterations of LIT1 and H19 . American Journal of Human Genetics 72 : 156 –160.
Doherty AS , Mann MR , Tremblay KD , Bartolomei MS , Schultz RM ( 2000 ) Diff erential eff ects of culture on imprinted H19 expression in the preimplantation mouse embryo . Biology of Reproduction 62 (6): 1526 –1535.
Doornbos ME , Maas SM , McDonnell J , Vermeiden JP , Hennekam RC ( 2007 ) Infertility, assisted reproduction technologies and imprinting disturbances: a Dutch study . Human Reproduction 22 : 2476 –2480.
Fauque P , Jouannet P , Lesaff re C , et al . ( 2007 ) Assisted reproductive technology aff ects developmental kinetics, H19 imprinting control region methylation and H19 gene expression in individual mouse embryos . BMC Developmental Biology 7 : 116 .
Fauque P , Ripoche MA , Tost J , et al . ( 2010a ) Modulation of imprinted gene network in placenta results in normal development of in vitro manipulated mouse embryos. Human Molecular Genetics Feb 26. [Epub ahead of print]
Fauque P , Mondon F , Letourneur F , et al . ( 2010b ) In vitro fertilization and embryo culture strongly impact the
placental transcriptome in the mouse model . PLoS One 5 (2): e9218 .
Fernandez-Gonzalez R , Moreira P , Bilbao A , et al . ( 2004 ) Long-term eff ect of in vitro culture of mouse embryos with serum on mRNA expression of imprinting genes, development, and behavior . Proceedings of the National Academy of Sciences of the USA 101 : 5880 –5885.
Fortier AL , Lopes FL , Darricarrère N , Martel J , Trasler JM ( 2008 ) Superovulation alters the expression of imprinted genes in the midgestation mouse placenta . Human Molecular Genetics 17 (11): 1653 –1665.
Galli-Tsinopoulou A , Emmanouilidou E , Karagianni P , et al . ( 2008 ) A female infant with Silver Russell Syndrome, mesocardia and enlargement of the clitoris . Hormones (Athens) 7 : 77 –81.
Gicquel C , Gaston V , Mandelbaum J , et al . ( 2003 ) In vitro fertilization may increase the risk of Beckwith-Wiedemann syndrome related to the abnormal imprinting of the KCN1OT gene . American Journal of Human Genetics 72 : 1338 .
Ginsburg M , Snow MH , McLaren A ( 1990 ) Primordial germ cells in the mouse embryo during gastrulation . Development 110 : 521 –528.
Gomes MV , Huber J , Ferriani RA , Amaral Neto AM , Ramos ES ( 2009 ) Abnormal methylation at the KvDMR1 imprinting control region in clinically normal children conceived by assisted reproductive technologies . Molecular and Human Reproduction 15 (8): 471 –477.
Halliday J , Oke K , Breheny S , Algar EJ Amor D ( 2004 ) Beckwith-Wiedemann syndrome and IVF: a case-control study . American Journal of Human Genetics 75 : 526 –528.
Hammoud SS , Purwar J , Pfl ueger C , Cairns BR , Carrell DT ( 2009 ) Alterations in sperm DNA methylation patterns at imprinted loci in two classes of infertility. Fertility and Sterility Oct 30. [Epub ahead of print]
Hata K , Okano M , Lei H , Li E ( 2002 ) Dnmt3L cooperates with the Dnmt3 family of de novo DNA methyltransferases to establish maternal imprints in mice . Development 129 (8): 1983 –1993.
Hayashi S , Yang J , Christenson L , Yanagimachi R , Hecht NB ( 2003 ) Mouse preimplantation embryos developed from oocytes injected with round spermatids or spermatozoa have similar but distinct patterns of early messenger RNA expression , Biology of Reproduction 69 : 1170 –1176.
Hiendleder S , Mund C , Reichenbach HD , et al . ( 2004 ) Tissue-specifi c elevated genomic cytosine methylation levels are associated with an overgrowth phenotype of bovine fetuses derived by in vitro techniques . Biology of Reproduction 71 (1): 217 –223.
Hirasawa R , Chiba H , Kaneda M , et al . ( 2008 ) Maternal and zygotic Dnmt1 are necessary and suffi cient for the maintenance of DNA methylation imprints during

Chapter 15: Epigenetics and assisted reproduction
264
preimplantation development . Genes and Development 22 (12): 1607 –1616.
Hiura H , Obata Y , Komiyama J , Shirai M , Kono T ( 2006 ) Oocyte growth-dependent progression of maternal imprinting in mice . Genes to Cells 11 (4): 353 –361.
Holm TM , Jackson-Grusby L , Brambrink T , et al . ( 2005 ) Global loss of imprinting leads to widespread tumorigenesis in adult mice . Cancer Cell 8 : 275 –285.
Houshdaran S , Cortessis VK , Siegmund K , et al . ( 2007 ) Widespread epigenetic abnormalities suggest a broad DNA methylation erasure defect in abnormal human sperm . PLoS One 2 (12): e1289 .
Imamura T , Kerjean A , Heams T , et al . ( 2005 ) Dynamic CpG and non-CpG methylation of the Peg1/Mest gene in the mouse oocyte and preimplantation embryo . Journal of Biological Chemistry 280 : 20171 –20175.
Isles AR , Holland AJ ( 2005 ) Imprinted genes and mother-off spring interactions . Early Human Development 81 : 73 –77.
Kagami M , Nagai T , Fukami M , Yamazawa K , Ogata T ( 2007 ) Silver-Russell syndrome in a girl born aft er in vitro fertilization: partial hypermethylation at the diff erentially methylated region of PEG1/MEST . Journal of Assisted Reproduction and Genetics 24 : 131 –136.
Källén B , Finnström O , Nygren KG , Olausson PO ( 2005 ) In vitro fertilization (IVF) in Sweden: infant outcome aft er diff erent IVF fertilization methods . Fertility and Sterility 84 : 611 –617.
Källén B , Finnström O , Lindam A , et al . ( 2010 ) Congenital malformations in infants born aft er in vitro fertilization in Sweden . Birth Defects Research A: Clinical and Molecular Teratology 88 (3): 137 –143.
Kanber D , Berulava T , Ammerpohl O , et al . ( 2009 a) Th e human retinoblastoma gene is imprinted . PLoS Genetics 5 (12): e1000790 .
Kanber D , Buiting K , Zeschnigk M , Ludwig M , Horsthemke B ( 2009 b) Low frequency of imprinting defects in ICSI children born small for gestational age . European Journal of Human Genetics 17 (1): 22 –29.
Katari S , Turan N , Bibikova M , et al . ( 2009 ) DNA methylation and gene expression diff erences in children conceived in vitro or in vivo . Human Molecular Genetics 18 (20): 3769 –3778.
Kerjean A , Couvert P , Heams T , et al . ( 2003 ) In vitro follicular growth aff ects oocyte imprinting establishment in mice . European Journal of Human Genetics 11 : 493 –496.
Khosla S , Dean W , Brown D , Reik W , Feil R ( 2001 ) Culture of preimplantation mouse embryos aff ects fetal development and the expression of imprinted genes . Biology of Reproduction 64 : 918 –926.
Khoueiry R , Ibala-Rhomdane S , Méry L , et al . ( 2008 ) Dynamic CpG methylation of the KCNQ1OT1 gene
during maturation of human oocytes . Journal of Medical Genetics 45 (9): 583 –588.
Kim KP , Th urston A , Mummery C , et al . ( 2007 ) Gene-specifi c vulnerability to imprinting variability in human embryonic stem cell lines . Genome Research 17 : 1731 –1742.
Kishigami S , Van Th uan N , Hikichi T , et al . ( 2006 ) Epigenetic abnormalities of the mouse paternal zygotic genome associated with microinsemination of round spermatids . Developmental Biology 289 : 195 –205.
Kobayashi H , Sato A , Otsu E , et al . ( 2007 ) Aberrant DNA methylation of imprinted loci in sperm from oligospermic patients . Human Molecular Genetics 16 : 2542 –2551.
Kobayashi H , Hiura H , John RM , et al . ( 2009 ) DNA methylation errors at imprinted loci aft er assisted conception originate in the parental sperm . European Journal of Human Genetics 17 (12): 1582 –1591.
Kono T ( 2009 ) Genetic modifi cation for bimaternal embryo development . Reproduction and Fertility Development 21 (1): 31 –36.
Kurihara Y , Kawamura Y , Uchijima Y , et al . ( 2008 ) Maintenance of genomic methylation patterns during preimplantation development requires the somatic form of DNA methyltransferase 1 . Developmental Biology 313 (1): 335 –346.
Lane M , Gardner DK ( 2003 ) Ammonium induces aberrant blastocyst diff erentiation, metabolism, pH regulation, gene expression and subsequently alters fetal development in the mouse . Biology of Reproduction 69 : 1109 –1117.
Lee I , Finger PT , Grifo JA , et al . ( 2004 ) Retinoblastoma in a child conceived by in vitro fertilisation . British Journal of Ophthalmology 88 (8): 1098 –1099.
Lee YS , Latham KE , Vandevoort CA ( 2008 ) Eff ects of in vitro maturation on gene expression in rhesus monkey oocytes . Physiological Genomics 35 (2): 145 –158.
Lees-Murdock DJ , Walsh CP ( 2008 ) DNA methylation reprogramming in the germ line . Advances in Experimental Medicine and Biology 626 : 1 –15.
Lees-Murdock DJ , Lau HT , Castrillon DH , De Felici M , Walsh CP ( 2008 ) DNA methyltransferase loading, but not de novo methylation, is an oocyte-autonomous process stimulated by SCF signalling . Developmental Biology 321 (1): 238 –250.
Li T , Vu TH , Ulaner GA , et al . ( 2005 ) IVF results in de novo DNA methylation and histone methylation at an Igf2-H19 imprinting epigenetic switch . Molecular Human Reproduction 11 : 631 –640.
Li X , Ito M , Zhou F , et al . ( 2008 ) A maternal-zygotic eff ect gene, Zfp57, maintains both maternal and paternal imprints . Developmental Cell 15 (4): 547 –557.

Chapter 15: Epigenetics and assisted reproduction
265
Liang XW , Zhu JQ , Miao YL , et al . ( 2008 ) Loss of methylation imprint of Snrpn in postovulatory aging mouse oocyte . Biochemical and Biophysical Research Communications 371 (1): 16 –21.
Lim D , Bowdin SC , Tee L , et al . ( 2009 ) Clinical and molecular genetic features of Beckwith-Wiedemann syndrome associated with assisted reproductive technologies . Human Reproduction 24 (3): 741 –747.
Lucifero D , Mann MR , Bartolomei MS , Trasler JM ( 2004 ) Gene-specifi c timing and epigenetic memory in oocyte imprinting . Human Molecular Genetics 13 (8): 839 –849.
Lucifero D , La Salle S , Bourc’his D , et al . ( 2007 ) Coordinate regulation of DNA methyltransferase expression during oogenesis BMC Developmental Biology 7 : 36 .
Ludwig M , Katalinic A , Gross S , et al . ( 2005 ) Increased prevalence of imprinting defects in patients with Angelman syndrome born to subfertile couples . Journal of Medical Genetics 42 : 289 –291.
Luedi PP , Dietrich FS , Weidman JR , et al . ( 2007 ) Computational and experimental identifi cation of novel human imprinted genes . Genome Research 17 (12): 1723 –1730.
Mackay DJ , Boonen SE , Clayton-Smith J , et al . ( 2006 ) A maternal hypomethylation syndrome presenting as transient neonatal diabetes mellitus . Human Genetics 120 : 262 –269.
Maher ER , Reik W ( 2000 ) Beckwith-Wiedemann syndrome: imprinting in clusters revisited . Journal of Clinical Investigation 105 (3): 247 –252.
Maher ER , Brueton LA , Bowdin SC , et al . ( 2003 ) Beckwith-Wiedemann syndrome and assisted reproduction technology (ART) . Journal of Medical Genetics 40 : 62 –64.
Malter HE , Cohen J ( 2002 ) Ooplasmic transfer: animal models assist human studies . Reproductive Biomedicine Online 5 (1): 26 –35.
Mann MR , Lee SS , Doherty AS , et al . ( 2004 ) Selective loss of imprinting in the placenta following preimplantation development in culture . Development 131 : 3727 –3735.
Manning M , Lissens W , Bonduelle M , et al . ( 2000 ) Study of DNA-methylation patterns at chromosome 15q11-q13 in children born aft er ICSI reveals no imprinting defects . Molecular Human Reproduction 6 : 1049 –1053.
Manning M , Lissens W , Liebaers I , Van Steirteghem A , Weidner W ( 2001a ) Imprinting analysis in spermatozoa prepared for intracytoplasmic sperm injection (ICSI) . International Journal of Andrology 24 (2): 87 –94.
Manning M , Lissens W , Weidner W , Liebaers I ( 2001b ) DNA methylation analysis in immature testicular sperm cells at diff erent developmental stages . Urology International 67 (2): 151 –155.
Marees T , Dommering CJ , Imhof SM , et al . ( 2009 ) Incidence of retinoblastoma in Dutch children conceived
by IVF: an expanded study . Human Reproduction 24 (12): 3220 –3224.
Marques CJ , Carvalho F , Sousa M , Barros A ( 2004 ) Genomic imprinting in disruptive spermatogenesis . Lancet 363 : 1700 –1702.
Marques CJ , Costa P , Vaz B , et al . ( 2008 ) Abnormal methylation of imprinted genes in human sperm is associated with oligozoospermia . Molecular Human Reproduction 14 (2): 67 –74.
Marques CJ , Francisco T , Sousa S , et al . ( 2010 ) Methylation defects of imprinted genes in human testicular spermatozoa . Fertility and Sterility 94 (2): 585 –594.
Market-Velker BA , Zhang L , Magri LS , Bonvissuto AC , Mann MR ( 2010 ) Dual eff ects of superovulation: loss of maternal and paternal imprinted methylation in a dose-dependent manner . Human Molecular Genetics 19 (1): 36 –51.
McMinn J , Wei M , Schupf N , et al . ( 2006 ) Unbalanced placental expression of imprinted genes in human intrauterine growth restriction . Placenta 27 : 540 –549.
Ménézo Y , Elder K , Benkhalifa M , Dale B ( 2010 ) DNA methylation and gene expression in IVF . Reproductive Biomedicine Online 20 (6): 709 –710.
Meschede D , De Geyter C , Nieschlag E , Horst J ( 1995 ) Genetic risk in micromanipulative assisted reproduction . Human Reproduction 10 : 2880 –2886.
Moll AC , Imhof SM , Cruysberg JR , et al . ( 2003 ) Incidence of retinoblastoma in children born aft er in-vitro fertilisation . Lancet 361 (9354): 309 –310.
Monk M , Boubelik M , Lehnert S ( 1987 ) Temporal and regional changes in DNA methylation in the embryonic, extraembryonic and germ cell lineages during mouse embryo development . Development 99 (3): 371 –382.
Moore T , Haig D ( 1991 ) Genomic imprinting in mammalian development: a parental tug of war . Trends in Genetics 7 : 45 –49.
Morgan HD , Santos F , Green K , Dean W , Reik W ( 2005 ) Epigenetic reprogramming in mammals . Human Molecular Genetics 14 (Spec No 1): R47 –58.
Morison IM , Reeve AE ( 1998 ) A catalogue of imprinted genes and parent-of-origin eff ects in humans and animals . Human Molecular Genetics 7 : 1599 –1609.
Morison IM , Ramsay JP , Spencer HG ( 2005 ) A census of mammalian imprinting . Trends in Genetics 21 : 457 –465.
Nakamura T , Arai Y , Umehara H , et al . ( 2007 ) PGC7/Stella protects against DNA demethylation in early embryogenesis . Nature Cell Biology 9 (1): 64 –71.
Obata Y , Kono T ( 2002 ) Maternal primary imprinting is established at a specifi c time for each gene throughout oocyte growth . Journal of Biological Chemistry 277 : 5285 –5289.
Obata Y , Kaneko-Ishino T , Koide T , et al . ( 1998 ) Disruption of primary imprinting during oocyte growth leads to

Chapter 15: Epigenetics and assisted reproduction
266
the modifi ed expression of imprinted genes during embryogenesis . Development 125 : 1553 –1560.
Ohno M , Aoki N , Sasaki H ( 2001 ) Allele-specifi c detection of nascent transcripts by fl uorescence in situ hybridization reveals temporal and culture-induced changes in Igf2 imprinting during pre-implantation mouse development . Genes to Cells 6 : 249 –259.
Omisanjo OA , Biermann K , Hartmann S , et al . ( 2007 ) DNMT1 and HDAC1 gene expression in impaired spermatogenesis and testicular cancer . Histochemistry and Cell Biology 127 : 175 –181.
Ørstavik KH , Eiklid K , van der Hagen CB , et al . ( 2003 ) Another case of imprinting defect in a girl with Angelman syndrome who was conceived by intracytoplasmic semen injection . American Journal of Human Genetics 72 : 218 –219.
Palermo GD , Neri QV , Takeuchi T , et al . ( 2008 ) Genetic and epigenetic characteristics of ICSI children . Reproductive Biomedicine Online 17 (6): 820 –833.
Pantoja C , de Los Rios L , Matheu A , Antequera F , Serrano M ( 2005 ) Inactivation of imprinted genes induced by cellular stress and tumorigenesis . Cancer Research 65 : 26 –33.
Poplinski A , Tüttelmann F , Kanber D , Horsthemke B , Gromoll J ( 2009 ) Idiopathic male infertility is strongly associated with aberrant methylation of MEST and IGF2/H19 ICR1 . International Journal of Andrology Oct 30. [Epub ahead of print]
Probst AV , Santos F , Reik W , Almouzni G , Dean W ( 2007 ) Structural diff erences in centromeric heterochromatin are spatially reconciled on fertilisation in the mouse zygote . Chromosoma 116 (4): 403 –415.
Qiao J , Chen Y , Yan LY , et al . ( 2009 ) Changes in histone methylation during human oocyte maturation and IVF- or ICSI-derived embryo development . Fertility and Sterility 93 (5): 1628 –1636.
Reik W , Maher ER ( 1997 ) Imprinting in clusters: lessons from Beckwith-Wiedemann syndrome . Trends in Genetics 13 (8): 330 –334.
Reik W , Walter J ( 2001 ) Genomic imprinting: parental infl uence on the genome . Nature Reviews (Genetics) 2 : 21 –32.
Reik W , Dean W , Walter J ( 2001 ) Epigenetic reprogramming in mammalian development . Science 293 (5532): 1089 –1093.
Renard JP , Baldacci P , Richouxduranthon V , Pournin S , Babinet C ( 1994 ) A maternal factor aff ecting mouse blastocyst formation . Development 120 : 797 –802.
Rossignol S , Steunou V , Chalas C , et al . ( 2006 ) Th e epigenetic imprinting defect of patients with Beckwith-Wiedemann syndrome born aft er assisted reproductive technology is not restricted to the 11p15 region . Journal of Medical Genetics 43 : 902 –907.
Rugg-Gunn PJ , Ferguson-Smith AC , Pedersen RA ( 2005 ) Epigenetic status of human embryonic stem cells . Nature Genetics 37 : 585 –587.
Sagirkaya H , Misirlioglu M , Kaya A , et al . ( 2006 ) Developmental and molecular correlates of bovine preimplantation embryos . Reproduction 131 : 895 –904.
Sagirkaya H , Misirlioglu M , Kaya A , et al . ( 2007 ) Developmental potential of bovine oocytes cultured in diff erent maturation and culture conditions . Animal Reproduction Science 101 : 225 –240.
Santos F , Hendrich B , Reik W , Dean W ( 2002 ) Dynamic reprogramming of DNA methylation in the early mouse embryo . Developmental Biology 241 (1): 172 –182.
Sato A , Otsu E , Negishi H , Utsunomiya T , Arima T ( 2007 ) Aberrant DNA methylation of imprinted loci in superovulated oocytes . Human Reproduction 22 : 26 –35.
Shamanski FL , Kimura Y , Lavoir MC , Pedersen RA , Yanagimachi R ( 1999 ) Status of genomic imprinting in mouse spermatids . Human Reproduction 14 : 1050 –1056.
Shi W , Haaf T ( 2002 ) Aberrant methylation patterns at the two-cell stage as an indicator of early developmental failure . Molecular Reproduction and Development 63 : 329 –334.
Stouder C , Deutsch S , Paoloni-Giacobino A ( 2009 ) Superovulation in mice alters the methylation pattern of imprinted genes in the sperm of the off spring . Reproductive Toxicology 28 (4): 536 –541.
Sun BW , Yang AC , Feng Y , et al . ( 2006 ) Temporal and parental-specifi c expression of imprinted genes in a newly derived Chinese human embryonic stem cell line and embryoid bodies . Human Molecular Genetics 15 : 65 –75.
Sutcliff e AG , Peters CJ , Bowdin S , et al . ( 2006 ) Assisted reproductive therapies and imprinting disorders – a preliminary British survey . Human Reproduction 21 : 1009 –1011.
Suzuki J Jr., Th errien J , Filion F , et al . ( 2009 ) In vitro culture and somatic cell nuclear transfer aff ect imprinting of SNRPN gene in pre- and post-implantation stages of development in cattle . BMC Developmental Biology 9 : 9 .
Svensson J , Bjornstahl A , Ivarsson SA ( 2005 ) Increased risk of Silver–Russell syndrome aft er in vitro fertilization? Acta Paediatrica 94 : 1163 –1165.
Tierling S , Souren NY , Gries J , et al . ( 2009 ) Assisted reproductive technologies do not enhance the variability of DNA methylation imprints in human . Journal of Medical Genetics Nov 30. [Epub ahead of print]
Walter J , Paulsen M ( 2003 ) Imprinting and disease . Seminars in Cell and Developmental Biology 14 : 101 –110.
Yamazaki T , Yamagata K , Baba T ( 2007 ) Time-lapse and retrospective analysis of DNA methylation in

Chapter 15: Epigenetics and assisted reproduction
267
mouse preimplantation embryos by live cell imaging . Developmental Biology 304 : 409 –419.
Young LE , Fernandes K , McEvoy TG , et al . ( 2001 ) Epigenetic change in IGF2R is associated with fetal overgrowth aft er sheep embryo culture . Nature Genetics 27 : 153 –154.
Zaitseva I , Zaitsev S , Alenina N , Bader M , Krivokharchenko A ( 2007 ) Dynamics of DNA-demethylation in early
mouse and rat embryos developed in vivo and in vitro . Molecular Reproduction and Development 74 (10): 1255 –1261.
Ziyyat A , Lefevre A ( 2001 ) Diff erential gene expression in pre-implantation embryos from mouse oocytes injected with round spermatids or spermatozoa , Human Reproduction 16 : 1449 –1456.

268
absent spermatogenesis, eff ects, 153 acid Tyrode’s (AT) drilling of the zona
pellucida, 227 , 229 acrosome reaction (AR), 51 , 52 , 53 , 54 ,
73 , 218 acrosome reaction to ionophore
challenge (ARIC) test, 52 Active Integrated workstation, 123 adhesion molecules, 83 adrenal hypoplasia, 152 adrenocoticotropic hormone (ACTH),
19 adult stem cells. See stem cell biology age-related aneuploidy, 238 , 242 albumin, 8 , 120 , 121 17-alpha hydroxylase cytochrome
P450, 22 alpha-tocopherol, 122 amino acid metabolism, 168 amino acid profi ling, 168 amniocentesis, 242 , 243 amplifi cation refractory mutation
system (ARMS), 243 amygdala, 19 anaphase, 14 Anderson Air fi lter apparatus, 137 androgen binding proteins (ABP),
21 androgen secreting tumors, 23 androgens, 21 andrology, 110 androstenedione, 22 aneuploid, defi ned, 14 aneuploidy screening, 167 Angelman syndrome (AS), 258 ,
260 anterior pituitary gland, 19 anti-Müllerian hormone (AMH), 31 anti-testis factors, 30 apoptosis, 38 , 42 , 60 , 69 , 101 , 110 , 143 ,
172 arches, 89 aromatase cytochrome P450, 22 ART, 85 , 127 , 128 , 169 , 196 , 197 , 201 ,
204 , 209 , 221 , 248 , 253 and Angelman syndrome (AS),
258
and Beckwith–Wiedemann syndrome (BWS), 257 , 258
and retinoblastoma, 258 and risk of infectious agent
transmission, 136 and Russell–Silver syndrome, 258 ,
259 and stem cell biology, 94 COH for, 23 , 24 , 25 derived embryos, 166 epidemiological data in, 257 induced epigenetic mistakes, 259 ,
260 laboratories in USA, 127 light exposure during, 110 microfl uidic platforms, 123 ovarian stimulation during
cycles, 41 problems with eff ectiveness of, 166
ART protocols, 24 ascorbic acid (vitamin C), 8 assisted conception treatment cycle,
109 assisted hatching (AH), 110 , 150 , 167 ,
216 , 227 and cryopreservation, 201 features, 227 laser, 227 Tyrode’s solution protocol, 227 , 229
assisted reproduction, 16 , 23 , 46 , 109 , 219 , 258 , 260 , 261 , See also in-vitro fertilization (IVF) laboratory
assisted zona hatching techniques, 219 ATP cleavage, 8 atresia, 41 Auerbach, Leopold, 60 autosomal dominant disorders, 239 autosomal recessive diseases, 239 av family, 83 azoospermia, 22 , 35 , 150 , 151 , 152 , 217
bacterial cells, 1 balanced translocations, eff ects of, 154 Beckmann pH meter, 132 Beckwith–Wiedemann syndrome
(BWS), 10 , 257 , 258
beta-globin gene, 239 beta-thalassemia, 239 bilaminar embryonic disc, 86 bilateral tubal pregnancy, 85 biochemical pregnancy, 91 biogenic law, 1 biological safety cabinet (BSC), IVF,
115 class I, 115 class II, 115 class III, 117 horizontal laminar fl ow clean bench,
117 vertical laminar fl ow clean bench,
113 , 114 blastocoele formation and expansion,
69 blastocyst biopsy, 231 blastocyst expansion and hatching, 70 ,
73 , 82 , 84 , 85 cell fate and cell lineages, 70 , 71
blastocyst freezing method, 201 blastocyst ICM, 102 blastocyst stage, 4 , 60 , 64 , 66 , 68 , 69 , 72 ,
120 , 123 , 165 , 166 , 169 , 170 , 197 blastocyst transfer, 176
benefi ts, 176 , 177 blastocyst transition, 71 , 75 , 121 blastocyst trophectoderm, 82 blastocyst vitrifi cation, 201 blastocysts, 73 , 82 , 83 , 84 , 85 , 86 ,
96 , 98 , 99 , 102 , 118 , 121 , 168 , 169 , 177 , 201 , 206 , 227 , 230 , 259
blastomeres, 64 , 67 , 102 blighted ovum, 91 blood gas analyzer, 132 blood vessels, development, 88 bone morphogenetic protein-15
(BMP-15), 182 bovine embryo culture, 119 , 260 buserelin, 24
Ca ionophore A23187, 53 calcium release at fertilization, 57 calcium-induced calcium release
(CICR), 57
Index

Index
269
cAMP, 12 , 22 , 35 , 45 , 46 , 51 , 53 , 67 , 73 , 148
cancer patients, semen cryopreservation for, 205
capacitation, 51 , 52 capacitation in vitro , 52 capacitation in vivo , 51 carbohydrates, 5 carbon cartridge fi ltration, 117 cavitation, 68 , 69 cell aging, 5 cell cycle, 2 , 12 , 13 , 45 , 60 , 64 , 67 , 68 ,
93 , 166 , 177 , 198 , 257 checkpoints, 16 DNA-responsive, 16 G0 phase of, 16 G1 phase of, 13 meiotic, 16 phases, 13 protein activity, 45
cell cytoplasm, 8 cell migration, 87 cell theory, 1
principles, 1 cell–cell recognition, 5 cell-penetrating peptide (CPP), 101 cellular adhesion molecules, 87 cellular replication, 13 , 14 central nervous system (CNS), 19
role of reproduction, 19 centrioles, 58 centromere, defi ned, 14 centrosomes, 13 , 36 , 58 , 60 , 72
microtubular organization, 72 Charcot–Marie–Tooth disease, 239 chemically defi ned medium (CDM),
102 cholesterol side-chain cleavage
cytochrome P450, 22 chorionic villus sampling (CVS), 238 ,
242 chromatids, 2 , 13 , 14 , 37
defi ned, 14 chromatin, defi ned, 14 chromosomal abnormalities, 238 chromosomal anomalies, testing of,
153 chromosome failures, 16 chromosome reproduction, 14 chromosomes, defi ned, 14 Clearplan, 201 cleavage stage blastomeres, 229 clomifene citrate (Clomid), 24 c-Myc, 101 co-culture systems, 123 codons, 10 , 11 , 12 , 13 Cohen, Jacques, 216
coitus, 50 compaction, 67 , 68 complete abortion, 91 congenital absence of the vas deferens
(CAVD), 152 congenital adrenal hyperplasia, 152 congenital bilateral absence of the vas
deferens (CBAVD), 217 controlled ovarian hyperstimulation
(COH), 260 baseline assessment, 25 GnRH analogues, 24 , 25 suppression mechanism, 23
corpus luteum, 42 cortical granules (CG), 55 , 56 craniophraryngioma, 152 Creutzfeldt–Jakob disease (CJD), 120 Crinone gel, 26 , 202 crown–rump length (CRL), 91 cryobiology, principles of, 191 cryopreservation, 110 cryopreservation of gametes and
embryos, 191 cryopreservation of samples, storage,
197 , 198 consent, 198
cryopreservation protocols comparison of slow freezing and
vitrifi cation, 197 equilibrium freezing, 196 non-equilibrium freezing, 196 , 197
cryopreserved aliquots of cells, 103 cryopreserved embryos, 157 Cryotop method, 206 cryptorchidism, 152 cultured zona-free rabbit ICM, 96 cumulus granulosa cells, 41 cumulus–oocyte complex (COC), 42 Cushing’s syndrome, 23 , 152 cycle monitoring, 25 , 26 cyclic ADP ribose, 57 Cyclogest pessaries, 26 cysteine, 74 cystic fi brosis (CF), 152 , 217 , 238 ,
239 cystic fi brosis conductance regulator
(CFTR) gene, 217 cytochrome C, 8 cytochrome oxidase, 8 cytochrome P450 enzyme triad, 22 cytokinesis, 14 cytoplasmic maturity, 181 cytosine, 9
daughter cells, 14 , 15 DAX1 gene, 29 , 30 Decapeptyl, 24
decidua, 83 , 86 decidualization reaction, 83 2-deoxyadenosine, 148 deoxyribose, 8 dermatomes, 89 Desert hedgehog gene, 87 diakinesis, 16 diff erentially methylated regions
(DMRs), 253 , 255 , 256 , 257 digestive epithelial layer, 90 dihydrotestosterone, 31 diploid somatic cells, 100 diploid, defi ned, 14 disaccharides, 5 disposable supplies, used in IVF, 117 ,
118 DM kinase gene, 241 Dmrt1, 30 DNA duplexes, 15 DNA methylation, 6 , 12 , 64 , 252 , 253 ,
256 , 259 , 260 during preimplantation
development, 257 DNA methyltransferases (Dnmts),
256 DNA replication, 9 , 10 , 14 , 16 , 64 DNA-responsive cell cycle, 16 Dolly sheep, 99 Down’s syndrome, 241 , 242 drosophila gene, 87
Earle’s (EBSS) solution, 121 early blastocyst, 177 early embryo arrest, 71 , 72 early embryo cleavage, 64 early prophase, 13 E-cadherin, 68 , 71 E-cadherin phosphorylation, 68 ectoderm layer, 87 ectopic pregnancy, 85 Edwards, Robert , 96 , 181 elective single embryo transfer (eSET),
169 , 176 electrodeionization (EDI), 117 electronic identity checking/
witnessing, in IVF, 112 elongation, 13 embryo biopsy technique, 176 , 229 ,
238 , 244 , 245 blastocyst stage technique, 231 cleavage stage techniques, 229 , 231 polar body, 231
embryo cryopreservation, 198 method, 198 , 199 selection of embryos, 198 slow freezing protocol, 200 use of glass ampules, 200

Index
270
embryo culture, preparation for, 157 embryo development, 1
amino acids, role of, 73 , 74 blastocyst expansion and hatching,
70 , 71 cavitation, 68 , 69 , 70 cholesterol synthesis, 73 compaction, 67 , 68 deamination reactions, 74 electrolyte balance, 73 embryonic arrest, 71 , 72 genome activation, 64 , 65 , 66 , 67 glucose, eff ect of, 73 growth factors, 75 imprinting, 67 metabolic requirements, 72 , 73 ,
74 , 75 nucleotides, role of, 74 , 75 paternal factors, 72 preimplantation development,
64 upregulation of pentose phosphate
pathway, 72 , 73 vitamin requirements, 75
embryo grading, 176 cleavage stage, 173 , 175 grade 1/A, 175 grade 2/B, 175 grade 3/C, 176 grade 4/D, 176 grade 5, 176 grade 6, 176
embryo metabolomics, 168 embryo transfer procedure, 177
blastocyst transfer, 176 , 177 preparation for transfer, 178 , 179 ,
180 , 181 embryologist, 178 embryology, 99 , 110 , 178
clinical, 216 equipment and supplies for, 123 ,
124 EmbryoMatcher, 112 embryonal carcinoma (EC) cell lines,
96 , 98 embryonal germ (EG) cell lines,
96 , 98 embryonic arrest, 71 , 72 embryonic gene expression studies,
169 grading of embryos, 169 , 170
embryonic trophectoderm, 83 embryos, impact of reduced
temperatures, 191 and cooling rate, 195 cell volume changes, 195 osmotic events, 195
physical changes, 191 , 192 role of cryoprotectant additives
(CPAs), 194 supercooling and cell survival,
192 surface area, 195 without cryoprotectants, 196
endocrine glands, 19 endoderm layer, 87 endoplasmic reticulum (ER), 4 , 5 epiblast, 86 , 101 epiblast stem cells (EpiSC), 99
characteristics, 103 , 104 markers of pluripotency, 104
epididymal maturation, 34 epididymal sperm, 150 epididymal sperm cryopreservation,
204 epigenetic alterations of LitI and H19,
10 epigenetic change, 67 epigenetics, 252
and infertility, 260 , 261 epigenic marks, 252 , 253 epigenic reprogramming of
germlines, 253 diff erences between inner
cell mass (ICM) and trophectoderm, 256
erasure profi le, 254 establishment, 254 , 256 species-specifi c diff erences,
256 information, 252
estradiol (E2), 22 estradiol valerate, 202 estrogens, 21 , 22 , 25 , 44 , 45 , 85 European Society for Human
Reproduction and Embryology (ESHRE), 219
exons, 10 expanded blastocyst, 177 external quality assurance, 128 extraembryonic spaces, 86
Falcon tubes, 26 fatty acid oxidation, 8 feeder cell layer, 123 feeder cells, 123 female reproductive endocrinology
controlled ovarian hyperstimulation (COH), 23 , 24
estrogen mechanism, 22 feedback mechanism, 22 gonadotropin output, 22 ovulatory cycle, 22 serum, 22
two-cell two gonadotropin theory, 22
FertiMorph multilevel system, 167 fetal heartbeat (FH), 91 fetal pole, 91 fi broblast growth factor 9 (FGF-9), 31 fl are-up protocol, 24 fl uorescent in-situ hybridization
(FISH) technique, 170 , 173 , 243 , 244 , 247 , 248 , 250
analysis of cleaved human embryos, 72
analysis of fertilized oocytes, 164 folic acid, 75 follicle development
aft er puberty, 40 and oocytes, 39 during growth phase, 38 fi rst primordial follicles, 38 follicular cells, 39 follicular destiny, 41 , 42 growth factors, 39 role of cumulus cells, 39
follicle stimulating hormone (FSH), 19 , 21
in females, 21 in testis, 21 pituitary, 21 role in formation of follicular fl uid,
41 specifi c functions of, 19 suppression of, 23
follicular fl uid, 22 , 24 , 40 , 41 , 42 , 52 , 161 , 166 , 168 , 182 , 218
follicular vascularity, 161 forebrain, 89 fragile X syndrome, 240 , 241 freezing of embryos
blastocyst freezing method, 201 blastocyst vitrifi cation method,
201 cellular responses, 195 , 196 clinical aspects, 201 , 202 cryopreservation of semen for
cancer patients, 205 cryopreservation protocols, 196 ,
197 direct eff ects, 191 eff ects of cryoprotectants, 194 embryo transfer in hormone
replacement therapy, 202 ice nucleation method, 200 oocyte cryopreservation, 205 ,
206 ovarian tissue cryopreservation,
207 , 208 , 209 physical changes, 191

Index
271
physical stresses on, 191 selection procedure, 198 , 199 , 200 semen cryopreservation, 202 ,
204 storage of samples, 197 supercooling and cell survival,
192 testicular and epididymal sperm
cryopreservation, 204 full blastocyst, 177 Fyrite kit for measuring CO 2 , 132
G0 phase of the cell cycle, 16 G1 phase of cell cycle, 13 G2 phase of cell cycle, 13 1,4-galactosyltransferase (GalTase),
35 gamete activation, 51 , 52 , 53 gamete interaction, 50 , 51 gamete precursor cells, 28 gametogenesis, 1 , 14 , 17 , 19 , 67 , 253 ,
254 , 256 , 260 , 261 gap junctions, 68 Gardner, Richard, 96 gastrulation, 87 gene expression, in early development,
87 gene silencing, 9 genes, 10 genetic code, 11 genome activation, 64 , 65 , 66 , 67 , 68 ,
69 genomic imprinting, 67 , 253
during preimplantation development, 257
factors involved in, 257 germinal aplasia, 153 germinal vesicle breakdown (GBVD),
54 gestational sacs, 91 Gestone, 26 , 202 Gilbert–Dreyfus syndrome, 152 glutamine, 74 , 118 , 119 , 169 glutathione, 8 , 59 , 71 , 73 , 74 , 119 glycine, 74 glycocalyx barrier, 83 glycolipids, 5 glycolysis, 8 glycoproteins, 5 GnRH agonist treatment, 25 GnRH agonists, 21 , 23 , 24 , 25 , 26 , 109 ,
201 , 205 GnRH antagonist protocol, 25 GnRH antagonists, 24 GnRH pulse generator, 20 , 21 Golgi apparatus
lysosomes, 5
proteins, sequences passing through, 5
Golgi, Camillo, 5 gonadogenesis
early stages, 29 follicle development, 38 , 39 , 40 ,
41 , 42 morphological changes, 29 ovary development, 36 , 37 , 38 sex determination, 30 spermatogenesis, 32 , 33 , 34 , 35 , 36 testis development, 30 , 31 , 32
gonadotropin hormone releasing hormone (GnRH), 19
gonadotropic hormones, 19 , 21 gonadotropin stimulation, 25 gonadotropin-dependent follicles, 22 G-protein cell signaling pathway, 22 G-protein hypothesis, 56 Graafi an, 39 granulosa cell diff erentiation, 22 growth diff erentiation factor-9
(GDF-9), 40 , 182 growth hormone (GH), 19 guide RNA (gRNA), 11 Gurdon, John, 100
haploid, defi ned, 14 hatched blastocyst, 177 hatching blastocyst, 177 ,
See also blastocyst expansion and hatching
hedgehog genes, 87 HeLa cell contamination, 17 HeLa cells, 17 hematopoietic stem cells (HSC), 95 hemochromatosis, 152 Henderson–Hasselbach equation, 118 HEPA fi lter airfl ow system, 114 HEPA-VOC fi lters, 111 HEPES buff ered biopsy medium, 119 ,
148 , 231 herniation technique, 231 Hertwig, Oscar, 60 hESC culture systems, 102 heteroduplex analysis, 243 heteroduplexes, 15 heterotopic pregnancy, 85 hexose – 6 C’s, 5 HFEA Code of Practice, 127 , 134 histone nomenclature, 253 Hoff man modulation contrast optics,
151 , 219 , 226 , 232 Holland, Robert, 11 Holliday structure/junction, 15 Holliday, Robin, 15 homeobox, 11
homeobox genes, 11 , 87 homeodomain, 11 honorary hormone, 56 HOS test, 149 HTF (Quinn’s Advantage), 260 human embryo metabolism, 168 human embryo viability,
measurements of, 166 amino acid turnover, 168 , 169 aneuploidy screening, 167 computer-assisted morphometric
analysis, 167 cumulative scoring system, 170 early cleavage, 170 follicular indicators of embryo
health, 167 , 168 fragmentation in human embryo,
170 , 172 , 173 FSH stimulation, 167 gene expression studies, 169 , 170 high resolution
videocinematography, 166 , 167 multinucleated blastomeres, 170 secretion of factors, 168 zygote scoring, 170
human embryonic stem cells (hESCs), 98 , 99 , 104 , 259
human T-cell lymphotropic virus (HTLV I and II), 136
Huntington’s disease (HD), 239 , 241
hydrogen peroxide, disposal of, 5 hydroxyl groups, 11 hyperactive motility, 51 hypoblast, 87 hypogonadotropic hypogonadism, 23 hypoplasia, 153 hypotaurine, 8 hypothalamic nuclei, 19 hypothalamic or pituitary
insuffi ciency, 22 hypothalamic-hypophyseal portal
veins, 19 hypothalamus, 19 , 21 , 22 , 24 , 152
functions of, 19 role in reproduction, 19 , 21
ICSI microscope, 150 immature gametes, 260 immunobead test, 141 implantation, 1
adhesion stage, 83 and cellular morphology, 85 , 86 , 87 ,
88 , 90 , 91 apposition stage, 82 , 83 initiation of, 82 invasion stage, 83 , 84

Index
272
post developments, 85 requirement of successful, 84 steroid and, 85 window, 83 , 84
imprinting, 67 imprinting processes, 9 in-vitro culturing, 1 in-vitro fertilization (IVF) laboratory.
See also quality management in IVF laboratory
controlled mechanisms in, 109 embryo culturing in groups, 121 embryo handling, 120 embryo transfer procedures, 182 ,
183 emerging technologies, 123 equipment and supplies for
embryology, 123 , 124 facilities, 182 international regulations, 120 setting up of laboratory
24-hour thermocouple readings, 111
air cleanliness, 112 biological safety cabinets, 115 ,
117 camera and monitor system, 111 custom-built isolator units, 112 electronic witnessing systems,
112 equipment, 110 , 111 follicular fl ushing media, 121 , 122 growth factors, 121 hand washing facilities, 110 incubators, 111 , 112 light exposure controls, 110 protein supplements, 120 service contracts, 111 space layout, 110 storage areas, 110 supplies, 117 tissue culture media, 118 , 119 ,
120 tissue culture systems, 121 , 122 volatile organic compounds, 114 ,
115 water jackets, 111 water quality, 117
sperm capacitation, 120 tissue culture systems
co-culture systems, 123 oil preparation, 122 oil used in culture overlays,
122 incomplete abortion, 91 incubators, in IVF, 111
Indian hedgehog gene, 85 , 87 induced pluripotent cell lines (iPSC/
piPSC), 99 , 100 , 101 inevitable abortion, 91 inhibin, 22 inner cell mass (ICM) cells, 68 inositol 1,4,5-trisphosphate (IP3)-
induced calcium release (IICR), 57
inositol triphosphate second messenger system, 19
integrin family, 83 , 84 , 87 intracellular adenosine triphosphate
(ATP), 148 intracytoplasmic injection of
spermatozoa (ICSI), 50 intracytoplasmic morphologically
selected sperm (IMSI), 226 equipment and materials, 226 patient selection, 226 procedure, 227
intracytoplasmic sperm injection (ICSI), 72 , 139 , 161 , 245
adjustments of manipulators, 233 , 234
assessment of fertilization and cleavage, 225
failure of fertilization, 225 cumulus-corona removal, 221 , 222 equipment for, 232 genetic implications, 216 , 217 indications, 218 , 219 injection preparation, 222 injection procedure, 225 location for set-up, 219 micromanipulation stage, 222 , 223 oocyte preparation and handling,
221 practical aspects, 219 selection of sperm for injection, 221 sperm selection and
immobilization, 223 surgical sperm retrieval, 217 tools and solutions, 219 , 220 , 221 transfer of gametes to injection dish,
223 transportation of, 225 , 226
introns, 10 invasive trophoblasts, 83
Johnsen score, 151
Kallman’s syndrome, 152 Kartagener’s immotile cilia syndrome,
153 Karyotype analysis, 170 , 243 , 246 Khorana, Ghobind, 11
kinetochore, defi ned, 14 Klf4, 101 Klinefelter’s syndrome, 152 , 153 , 241 Krebs cycle, 8 K-Systems G185, 111
laboratory air quality, in IVF, 112 , 114 lactated Ringer’s solution, 121 laminin, 37 , 83 , 84 , 87 , 102 large granular lymphocytes (LGSs), 83 large off spring syndrome (LOS), 259 leukemia inhibitory factor (LIF), 84 Leydig (equivalent to ovarian theca)
cells, 21 failure of, 153
Leydig cells, 31 light exposure eff ects, in IVF, 110 Lin28, 101 Lub’s syndrome, 152 luteal phase, hormonal support of, 26 luteinization, 22 luteinizing hormone (LH), 19
in testis, 21 role in female reproduction
endocrinology, 22 role in testosterone production, 21 suppression of, 23
Luveris, 24 lysosomes, 5
M phase of cell cycle, 13 M16 medium/G1/G2, 259 male factor infertility, 139 male hypothalamo–pituitary unit, 21 male pronucleus, 257 male reproductive endocrinology, 21
and masculine features, 21 feedback mechanisms, 21 gonadotropins, 21 in males with hyperprolactinemia,
21 role of testosterone, 21 serum, 22 sexual maturity and reproductive
function, 22 sperm production, 21 spermatogenesis process, 21 vs female reproductive
endocrinology, 21 mammalian cell biology, 1
cell cytoplasm, 2 centrioles, 2 endoplasmic reticulum (ER), 4 , 5 Golgi apparatus, 5 membranes, 1 , 2 metabolism in cells
basic factors, 5
implantation (cont.)

Index
273
carbohydrates, 5 cytokines, 6 , 7 enzymes, 6 fats and lipids, 5 , 6 fundamental biology, 8 , 9 , 10 , 11 ,
12 , 13 , 14 , 15 , 16 , 17 metabolic pathways, 7 , 8 proteins, 6 reactive oxygen species (ROS), 8 redox reactions, 8 superoxide dismutase (SOD), 8
microfi laments, 2 microtubules, 2 microvilli, 2 mitochondria, 2 , 3 , 4 nucleus, 2 peroxisomes, 5
mammalian gametes, 52 Marfan’s syndrome, 239 master regulators of gene expression.
See microRNA (miRNA) maternal age and embryo quality, 71 maternal mRNA encoding, 64
translation, 65 Matrigel, 102 maturation promoting factor (MPF),
46 mean Johnsen score (MJS), 151 meiosis, 14 , 33 , 37 , 241
diff erences with mitosis, 14 , 16 errors in, 16 principles, 15
meiotic arrest, 16 , 56 meiotic divisions, 16 membrane-enclosed organelle, 4 meningitis, 152 menopause, 23 Merck Index, 122 mesenchymal cells, 87 mesoderm layer, 87 mesodermal somites, 87 metabolic locks, 123 metaphase, 14 methylation processes, 75 5-methyluracil, 75 microepididymal sperm aspiration
(MESA), 217 microfl uidic technology, 123 microfunnel culture system, 123 micromanipulate cells, 216 micromanipulation, 110 micromanipulation techniques, 216
early experiments, 216 hyaluronic acid (HA) solution, 221 hyaluronidase solution, 221 ICSI. See intracytoplasmic sperm
injection (ICSI)
joysticks, 220 , 234 micro-injection equipment, 219 micromanipulators, 220 , 234 microtools used, 219 polyvinyl pyrrolidine solution, 219 ,
220 supplies used, 219
microRNA (miRNA), 11 microscopic surgery (MESA), 150 microsurgical techniques, 216 microtubule organizing centers
(MTOC), 60 Milli-Q water, 122 miscarriage, 91 missed abortion, 91 mitochondrial RNA (mRNA)
transcripts, 181 mitogen activated protein kinase
(MAPK), 54 mitogenic colony stimulating factor
(MCSF), 75 mitomycin C, 102 mitosis, 14 , 36 , 66 mitotic cell cycle, 13 mitotic metaphase, 60 mixed antiglobulin reaction (MAR)
test, 141 monosaccharides, 5 morphological blastocyst assessment,
179 Mos protein, 46 motile sperm organellar morphology
examination (MSOME), 226 motile spermatozoa, 150 motility, 51 mouse embryonic fi broblasts (MEF),
102 M-phase promoting factor (MPF), 54 MTG pH meter, 132 Müllerian duct, 29 , 31 Müllerian inhibitory substance (MIS),
31 Multiple Births, Single Embryo
Transfer Policy, 169 mumps orchitis, 152 mural granulosa cells, 22 , 41 mutation in a single base, impact, 11 myotonic dystrophy (DM), 239 , 241 myxoploidy of trophectoderm cells, 69
NAADP + -induced calcium release, 58 NAD(H), 8 NADP(H), 8 nafarelin, 24 NANOG, 101 neural tube, viii , 87 , 88 , 89 , 242 , 243 neuroendocrine mechanisms, 21
Nirenberg, Marshall, 11 Nomarski optics, 219 Noonan’s syndrome, 152 , 153 norethisterone, 24 nuclear maturation
control of, 45 , 46 during the development of Graafi an
follicle, 45 resumption of meiosis, 45 timing of events, 45
nuclear organizing region (NOR), 65 , 66
nucleation, 192 nucleic acids, methylation of, 73 nucleolar precursor bodies (NPBs), 59 nucleoside diphosphate linked moiety
X, 74 nucleotide pool sanitization enzymes,
74 nucleotides, 8 , 9 , 11 , 39
Oct-4, 40 , 101 Oct-l, 11 OCTAX Ferti Proof™, 112 oligosaccharides, 5 oligospermia, 22 Omnis cellulae e celula, 1 oocyte retrieval (OCR) procedures, 26 oocyte–cumulus complex, 41 oocyte–granulosa cell communication
events, 41 oocytes, 8 , 14 , 16
abnormalities in, 20 activation, vii , 16 , 53 , 54 , 55 , 56 , 57 ,
149 , 206 activation of, 216 amphibian, 59 at fertilization, 56 cryopreservation, 205 , 206
improvement of, 206 issues with, 206 thawing diffi culties, 206
cryopreservation of, 164 cytoplasm, 57 , 59 dissection of fertilized, 162 , 163
making of narrow-gauge pipettes, 163
scoring of fertilization, 163 , 164 techniques, 163
embryo selection for transfer, 165 , 166
germinal vesicle stage, 206 growth, 42 , 43 human, 54 , 83 , 121 , 206
in-vitro maturation, 181 , 182 identifi cation, 158
aneuploidy, 161

Index
274
features of dysmorphism, 161 germinal vesicle, 158 maturity, 160 metaphase I, 160 metaphase II, 160
in ovary, 37 in-vitro maturation (IVM) and
in-vitro growth (IVG) of, 260 insemination of, 161
preparation, 161 , 162 mammalian, 57 , 59 , 70 , 257 maturation, 16 , 39 , 40 , 42 , 46 , 60 , 72 ,
182 , 260 stages in, 44 , 45
morphological changes, 161 nuclear maturation, 45 , 46 polarity, 43 preparation, 157
laboratory supplies for labeling and preparation, 158
laboratory, checklist, 157 microdroplets under oil used, 157 plates used, 158
reinsemination of, 164 retrieval, 24 , 158
observation using time-lapse cinematography, 166
role in follicle development, 39 , 40 role of membrane fusion in
activation of, 216 storing information, 43 surface of membrane, 54 viable, 46
oogenesis, vii , 36 , 37 , 43 , 44 , 45 , 55 , 58 , 64 , 67 , 253 , 256 , 257
oogonia, 36 , 37 , 38 orgasm, 50 ovarian steroidogenesis, 24 ovarian stimulation, 25 , 198 , 258 , 260
protocols, 24 with FSH during ART cycles, 41
ovaries, 20 , 25 , 29 , 182 hemi-, 208 whole, 209
ovary development oocytes, 37 oogonia, 37 ovarian reserve, 38 sex cords, 36
ovulation induction, 24 , 26 , 121 post 13–15 days, 86 post 15 days, 86 , 87 post 16–19 days, 87 post 19–21 days, 87 , 88 post 21–27 days, 89
post 28–35 days, 89 , 90 post 35–42 days, 90 post 7–12 days, 85
oxidative phosphorylation process, 8
p450 aromatase, 22 Palermo, GianPiero, 216 paraffi n oil, 122 parthenogenesis, 58 partial zona dissection (PZD), 216 ,
229 paternal Y-linked genes, 72 paternally inherited genes, 66 PCR technique, 243 pentose – 5 C’s, 5 percutaneous epididymal sperm
aspiration (PESA), 217 percutaneous puncture (PESA), 150 perivitelline space (PVS), 56 peroxisomes, 5 phenylketonuria, 11 phospholipase C zeta 1, 57 phosphorylation of sperm proteins,
51 Pit-l, 11 pituitary tumors, 152 plasminogen activator system, 84 pluripotency gene expression, 100 , 104
factors used, 101 pluripotent EG cells, 98 polar bodies, 16 polycystic ovarian disease (PCO), 23 ,
24 , 181 polyposis coli, 239 polysaccharides, 5 polysomes, 5 polyspermy, 51 POU factors, 11 pregnancy associated plasma protein
A (PAPP A), 242 pregnancy failures, 91 preimplantation genetic diagnosis
(PGD), 238 biopsy techniques
allele dropout (ADO), 246 blastocyst, 246 cleavage stage, 245 embryo, 244 FISH diagnosis, 247 molecular diagnosis, 246 PCR analysis, 246 polar body, 244 , 245 single cell diagnosis, 246
fi elds covered, 238 future, 250 inherited diseases diagnosed by,
238 , 239 , 240 , 241 , 242
of chromosomal mosaicism, 248 , 249
regulations, 249 screening of abnormalities
perinatal diagnosis of inherited disorders, 242 , 243 , 244
serum screening, 242 ultrasound, 242
team, 244 preimplantation genetic screening
(PGS) technique, 167 , 173 premature ovarian failure, 23 , 207 preovulatory antral follicles, 41 , 42 primitive sex cords, 29 primordial germ cells (PGCs), 28
biological processes, 28 development of testis, 30 identifi cation, 28 in mouse, 28 migration and proliferation of, 28 ,
41 morphological changes in
primordial gonads, 28 , 29 , 30 sex determination, 30
progesterone, 20 , 22 , 23 , 24 , 42 , 50 , 51 , 85 , 201 , 202
during decidualization, 83 , 84 production of, 44 , 45 receptors, 85 supplementation, 26 , 202 synthesis of p39 mos, 46
prolactin, 21 proliferating cell nuclear antigen
(PCNA), 40 pronucleate freezing, 198 prospermatogonial cells, 31 prostaglandins, 39 protamine crosslinking, 58 protein-induced pluripotent stem cell
(piPSC), 102 putative ES line, 102 (Pyr)-Glu-His-Trp-Ser-Tyr-Gly-Leu-
Arg-Pro-Gly-NH 2 ), 19 pyrollidone carboxylic acid (PCA), 74 pyruvate, 8 pyruvic acid, 8
quality assurance, 128 quality audit, 128 quality control, 128 quality management in IVF laboratory
basic housekeeping procedures, 135 end of the day procedures, 135 handling of non-disposable
items, 135 incubator maintenance, 136 pipettes, 135
oocytes (cont.)

Index
275
washing procedures, 135 bioassay system, 133
factors related to usage, 134 CO 2 monitoring, 132 culturing of embryos, 134 culturing of oocytes, 134 decontamination procedures, 137 defi nitions, 128 eff ective handling, cleaning, and
maintenance schedules, 136 equipment, 129 , 130
monitoring, 132 , 133 facilities monitoring systems (FMS),
129 formal QMS, 129 fungal contamination management,
137 genital infections testing, 136 implementation of QMS, 129 in diff erent countries, 127 incubator management, 132 , 136 ,
137 ISO9001–2000 127 , 128 key points in QMS, 135 microbiological testing and
contamination management, 136 , 137
pH control, 131 , 132 risk assessments and standard
operating procedures, 134 , 135 specifi c goals, 128 sperm survival test, 134 syphilis testing, 136 temperature control, 130 use of quaternary ammonium
compounds, 137 quality management system (QMS),
127 , 128 , 129 quality policy, 128 quality, defi ned, 128
reactive oxygen species (ROS), 8 reciprocal translocations, 242 recurrent abortion, 91 Reinfenstein’s syndrome, 152 reproductive cloning, 100 rescue ICSI, 164 retinoblastoma, 258 retoviral syncitin envelope gene, 70 retrograde ejaculation, 153 , 218 reverse osmosis (RO), 117 reverse transcriptase-polymerase
chain reaction (RT-PCR), 66 RI pH meter, 132 ribonuclease MRP, 11 ribonuclease P, 11 ribosomal RNA, 11
ribosomes, 5 RNA
basic structure, 11 DNA replication and, 11 polyadenylation patterns, 64 transcription mechanism, 12 translation mechanism, 12 , 13 , 14 translation of mRNA into
polypeptide chains, 12 , 13 types, 11
Robertsonian translocations, 154 , 217 , 241 , 242 , 247
Rosewater’s syndrome, 152 rough ER (sER), 5 round spermatid injection (ROSNI),
151 rRNA genes, 60 Ruskinn Ac-tive IVF System, 112
S phase of cell cycle, 13 S-adenosyl methionine, 73 sarcoidosis, 152 sclerotomes, 89 semen analysis, 139
cells in semen, 143 chromosomal anomalies, 153 detection of DNA fragmentation by
TUNEL assay, 144 DNA fragmentation, 143 internal and external quality control
procedures, 143 macroscopic evaluation, 140 pathologies, 153
androgen resistance, 152 azoospermia, 151 post-testicular failure, 152 pretesticular, 152 testicular failure, 152
Robertsonian translocation, 154 sample collection and handling,
139 , 140 sperm antibody detection, 141 , 142 sperm chromatin assays, 144 sperm concentration, 141 sperm kinematics, 143 sperm morphology estimation, 142 ,
143 sperm motility, 140 , 141 sperm preparation for ICSI/IMSI,
148 , 149 and 100% head anomalies, 149 excessive amounts of debris, 149 hypo-osmotic swelling test
(HOS), 149 sperm preparation aft er
retrograde ejaculation and electroejaculation, 149 , 150
sperm preparation equipments and materials, 154
sticky sperm, 149 surgical sperm retrieval, 150
sperm preparation for in vitro fertilization, 144 , 145
buoyant density gradient centrifugation monitoring, 146
chemical enhancement of sperm motility prior to insemination, 148
high-speed centrifugation and washing, 148
isotonic gradient solution, 146 methods, 146 mini-gradient analysis, 147 pellet and swim-up, 145 , 146 sedimentation method or
layering under paraffi n oil, 147 standard swim-up or layering,
145 two-step gradient analysis, 146 ,
147 spermatid identifi cation, 151
round, 151 semen cryopreservation, 202
eff ects on sperm, 202 manual freezing method, 204 method, 203 , 204 sperm survival methods, 204
Sertoli cells, 21 , 31 , 153 Sertoli–Leydig cells, 20 serum endocrinology in female, 22 , 23 sex determination, 30 sexual arousal, 19 sexual development, 16 short GnRH agonist protocol, 25 sickle cell anaemia, 11 silent fertilization, 71 silicone oil, 122 single gene defects, 238 , 239 single stranded conformational
polymorphism (SSCP), 243 small nuclear RNA (snRNA), 11 small nucleolar RNA (snoRNA), 11 smooth ER (sER), 5 SNP array analysis, 244 somatic cell nuclear transfer, 99 , 100 somatic cells, 1 , 16 , 28 , 31 , 35 , 56 , 57 ,
58 , 60 , 96 , 97 , 99 , 100 , 118 , 133 , 172 , 252
somites, 87 Sonic hedgehog gene, 87 SOX2, 101 sperm capacitation, 120 sperm factor hypothesis, 56 , 57 , 58 sperm preparation, 157

Index
276
sperm survival test, in IVF laboratory, 134
spermatid nuclei, 33 spermatocytes, 16 spermatocytogenesis, 33 spermatogenesis, 20 , 21 , 31 , 32 , 33 , 34 ,
58 , 59 , 67 , 72 , 143 , 150 , 151 , 152 , 153 , 205 , 217 , 218
failure of, 21 gene expression, 36 molecular features of, 34 phases, 32
spermatogenic failure, causes, 153 spermatogonia, 151 spermatozoa, 36 , 50 , 51 , 53 , 54 , 57 , 72 ,
134 , 139 , 141 , 142 , 149 , 150 , 151 , 191 , 194 , 205 , 216
motility in HA solution, 221 spermatozoal nucleoli, 59 spermatozoon, 51 spermiogenesis, 33 , 34
DNA structure, 35 gene expression, 35 , 36 morphological changes, 35 pathology aff ecting, 35
sperm–oocyte interaction breakdown of sperm nuclear
membrane, 59 events involved in, 51 gamete activation, 51 , 52 , 53 gamete interactions, 50 , 51 G-protein hypothesis, 56 intracellular calcium release, 57 oocyte activation, 53 , 54 pronucleus formation, 58 , 59 , 60 ratios, 51 soluble sperm factor hypothesis, 56 ,
57 , 58 sperm–oocyte fusion, 54 , 56 syngamy, 60
S-phase, 64 SRY, 29 Sry (Sex-determing region) gene,
29 , 31 SRY transcripts, 66 standard “test” culture system, 111 Steinert’s disease, 241 stem cell biology
cell lines, 93 cloning, 99 , 100 deriving from blastocyst (ICM), 102 hematopoietic, 95 hESC culture systems, 102 mammalian, 93 registries, 104 research, 96 , 102
early culture systems, 96
embryonal carcinoma (EC) and embryonal germ (EG) cell lines, 96 , 98
epiblast stem cells (EpiSC), 99 human embryonic stem cells
(hESC), 98 , 99 induced pluripotent cell lines
(iPSC/piPSC), 99 , 100 , 101 mouse embryonic stem cells, 98 protein-induced pluripotent cell
lines (piPSC), 101 therapeutic applications, 96
sterilization cycle (Steri-Cycle™), 114 stimulation protocols for IVF, 25 stop codons, 11 , 12 , 13 stromal decidualization, 83 subzonal sperm injection (SUZI), 216 sulfur-amino acids, 73 superoxide dismutase (SOD) enzyme,
8 Synarel, 24 synchrony, 19 syncytia, 37 syncytiotrophoblast phenotype, 84 syngamy, 60 , 64
Taq polymerase, 243 Tay–Sachs disease, 243 telophase, 14 testicular atrophy, 153 testicular fi ne needle aspiration
(TEFNA), 150 , 217 testicular sperm aspiration (TESA),
217 testicular sperm cryopreservation, 204
biopsy samples, 204 testicular sperm extraction (TESE),
150 testis development, 31
genetic control, 31 testes, 31 , 32
testis-determining factor (TDF), 30 testosterone, 21
normal range, 22 TGF-beta superfamily, 102 therapeutic cloning, 99 threatened abortion, 91 thymine, 75 thyroid stimulating hormone (TSH),
19 time-lapse photography technology,
112 , 167 , 172 tissue culture media, in IVF, 118
balanced salt solutions (BSS), 119 blastocyst formation, 118 , 119 commercial media, 119
advantages, 121 , 122
important factors, 120 GMP procedures, 119 , 120 HEPES media, 119 optimized for preimplantation
embryos, 119 physical parameters, 118 protocols, 119
tocopherol (vitamin E), 8 total quality management (TQM)
system, 127 totipotent cells, vii transforming growth factor-ß (TGFß),
84 trauma, 152 Treponema pallidum , 157 triplet repeat disorders, 238 , 240 , 241 trophectoderm cells, 68 , 69 , 70 , 82 , 83 ,
101 , 102 , 177 , 201 , 231 , 245 , 246 , 248 , 256
trophoblast cells, 83 , 84 , 85 trophouteronectin (TUN), 84 tubulin, 58 Turner’s syndrome, 241 two cell two gonadotropin theory, 22 type 1 plasminogen activator inhibitor
(PAI-1), 84
ubiquinone, 8 ultrashort GnRH agonist
protocol, 25 ultrashort protocol, 24 ultrasound, 25 , 181 , 183 , 201 , 242 , 243 ,
245 confi rmation of pregnancy, 91 detection of nuchal translucency,
242 screening for age-related
aneuploidy, 242 to confi rm gestational sac, 109
ultraviolet oxidation system, 117 Unc-86, 11 uric acid, 8 urogenital sinus, 29 uterine environment, 82 uterine epithelium, 83 uterine growth factors, 85 uterine prostaglandins (PGF2 and
PGE2), 84 Utrogestan, 26 , 202
vasa eff erentia tubules, 34 vasocongestion, 50 Visible Embryo Project, 85 vitamin B12, 75 vitelline block, 56 volatile organic compounds (VOCs),
114 , 115

Index
277
washed oil, 122 water purifi cation system, in IVF,
117 white blood cells, 5 Whitten’s medium, 259 Wnt genes, 29 , 30 , 87 Wolffi an (mesonephric) duct, failure
of, 152 Wolffi an duct, 29 , 31 World Health Organization (WHO)
laboratory manual, 139 WT1 (+KTS ) isoform, 29 WT1 (–KTS) isoform, 29
Xenopus embryogenesis, 67 Xenopus laevis eggs, 100 X-linked diseases, 240 46XX (Noonan’s syndrome), 153 46XX Klinefelter’s syndrome, 153
Yanagimachi, Ryuzo, 216 Y-microdeletion analysis, 217 yolk sacs, 91 Young’s syndrome, 34 , 152
ZFY transcripts, 66 Zinner’s syndrome, 152
Zoladex, 24 zona drilling (ZD) technique, 216 zona pellucida (ZP), 35 , 39 , 42 , 44 ,
51 , 53 , 54 , 55 , 70 , 82 , 102 , 142 , 161 , 163 , 164 , 167 , 169 , 176 , 182 , 198 , 208 , 216 , 218 , 219 , 224 , 227 , 229 , 245
zona radiata, 39 zygote gene activation, 64 zygote genome, 64 zygotic clock, 67 zygotic gene expression, 66