Embed Size (px)
Citation preview

Electrolyte disorders in Critically ill patients
������������� �������������������� ����� ����������������

“It is the internal environment (not the external world) that provides the physical need for life”
CLAUDE BERNARDCLAUDE BERNARD
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

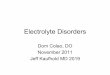
BODY FLUID COMPARTMENTS Arrow represents fluid movement
Review of Medical Physiology, William F. Ganong
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Electrolyte Composition of Body Fluid Compartments
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Composition of body fluids losing continuously
Source Daily Loss Na+ K+ Cl- HCO3-
Saliva 1000 30-80 20 70 30
Gastric 1000-2000 60-80 15 100 0
Pancreas 1000 140 5-10 60-90 40-100Pancreas 1000 140 5-10 60-90 40-100
Bile 1000 140 5-10 100 40
Small Bowel 2000-5000 140 20 100 25-50
Large Bowel 200-1500 75 30 30 0
Sweat 200-1000 20-70 5-10 40-60 0
urine 1500-2000 <10
Frusemide diuresis 75
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Composition of IV fluidsin comparison to Plasma
Fluid Na K Ca Mg Cl Buffers Glucose pH Osm
Plasma141 4.5 5 2 103
HCO3-26Prot-16
0.7-1.1 7.4 290
NS 154 154 6.0 308
1/2NS 77 77 5.0 154
RLRL 130 4 3 109 Lac-28 6.5 274
5%D 50 4.5 252
Plasmalyte140 5 3 98
Acet-27Gluc-23
7.4 294
Gel
3%Saline 513 513 4.5 1026
5%Alb
20%Alb
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Sodium Water Sodium Water disturbances
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Na is the most abundant molecule in ECFNa is the most osmotically active molecule in ECF
S. Osm ( mOsm/kg of water)(2*[Na] + [Glucose/18] + [BUN/2.8]
(Na in meq/L, Glucose in mg/dL, BUN in mg/dL)
Contribution of Gluc and BUN is 5 mOsm/L
(Na in meq/L, Glucose in mg/dL, BUN in mg/dL)
Osmotic pressure and osmolality determinesdistribution of fluid in body compartments
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

OSMOLALITY
280-295 mOsm/kg
Serum
Urine
24 hour urine sample-500-800 mOsm/kgExtreme range-50-1400mOsm/kg
Random urine sample- 300-900mOsm/kg
After overnight fluid restrictionUrine omolality > 3 times serum osmolality (>800)
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Real story in critically ill patients
S. Osm = 2* (140) + 90/18 + 5/2.8= 280 + 5 + 1.7
= 286.7
S. Osm = 2* (145) + 180/18 + 60/2.8= 290 + 10 + 21
= 321
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Na WATER
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Na / water regulation
Thirst ADH RAA Kidney
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Epidemiology of electrolyte disorder in ICUEpidemiology of electrolyte disorder in ICU
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Intensive Care Medicine 2010, 36(2):304-11Incidence and prognosis of dysnatremias present on ICU admission
Funk GC, Lindner G, Druml W, Metnitz B, Schwarz C, Bauer P, Metnitz PG
retrospective study in 77 medical, surgical, and mixed ICUs in Austria, 151,486 adults patients admitted over a period of 10 years (1998-2007).
75% patients had normal sodium levels (Na:135-145) on ICU admission
Incidencehyponatremia-17.7%, Hypernatremia-6.9%
All types and grades of dysnatremia were associated with increased hospital mortality
independent mortality risk rising with increasing severity of both hyponatremia and hypernatremia
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Critical Care 2008, 12:R162
The epidemiology of intensive care unit-acquired hyponatraemiaand hypernatraemia in medical-surgical intensive care units
Henry Thomas Stelfox, Sofia B Ahmed, Farah Khandwala, David Zygun, Reza Shahpori, Kevin Laupland
8142 adults admitted in 3 medical-surgical ICUs Over 6 yearsdocumented to have normal S. sodium levels (133 to 145 mmol/L) on
the first day of ICU admission
Incidence Hyponatremia- 11%, hypernatremia-26%
Median time to develop dysnatremia- 2 days
Median duration of dysnatremia-2 days
More than 1 distinct epi of dysnatremia- 25%(Hyponatremia-16%, hypernatremia-19%)
hospital mortality increased significantlyIndependent of SOI
( hypoNa-28%, hyperNa-34%, normoNa-16%)
Continued…..Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Critical Care 2008, 12:R162
The epidemiology of intensive care unit-acquired hyponatraemiaand hypernatraemia in medical-surgical intensive care units
Henry Thomas Stelfox, Sofia B Ahmed, Farah Khandwala, David Zygun, Reza Shahpori, Kevin Laupland
Continued…..Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Increased risk of hypernatremiaRaised S.creatinine
Mechanical ventilation
Increased risk of both hyper and hyponatremiaLength of stay in ICU
Critical Care 2008, 12:R162
The epidemiology of intensive care unit-acquired hyponatraemiaand hypernatraemia in medical-surgical intensive care units
Henry Thomas Stelfox, Sofia B Ahmed, Farah Khandwala, David Zygun, Reza Shahpori, Kevin Laupland
Length of stay in ICUIncreased APACHE II score
•Dysnatremias develop insidiously over 2 days
•Difficult to identify as clinicians preoccupied with more acute medical issues and other lab investigations
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Critically ill patients prone to
electrolyte disturbanceselectrolyte disturbances
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Disturbance in fluid and electrolyte homeostasissepsis, shock, cardiac failure, acute kidney injury, burn, surgery, C.N.S. disorders
Activation of neuro hormonal system- SNS, RAAS, Vasopressin
Non osmotic release of Vasopressinpain, nausea, medication, hypovolemia
Diuresisiotrogenic- renal and osmotic diuretics
Vasopressin deficiency in sepsis
Insensitivity to insensible losses
Impaired thirst mechanism
Inappropriate administration of fluid and electrolytes
iotrogenic- renal and osmotic diureticsUrea, glucose induced
Hypokalemia, hypercalcemiaDrug induced- aminoglycoside, ampho B
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

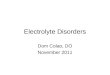
Am J Kidney Dis 2009 Oct, 54:674-679
tonicity balance in patients with Hypernatremia Acquired in the Intensive Care Unit
Gregor L, Nikolaus K, Ulrike Holzinger, Wilfred Druml, christiph schwartz
Solute balance= [Na+K]input – [Na+K]outputContinued…
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

osm
otic
Non
olig
uric
Urea/ glucose
Am J Kidney Dis 2009 Oct, 54:674-679
tonicity balance in patients with Hypernatremia Acquired in the Intensive Care Unit
Gregor L, Nikolaus K, Ulrike Holzinger, Wilfred Druml, christiph schwartz
Causes of ICU acquired hypernatremia
osm
otic
DI
Non
olig
uric
Addition of KCl to 0.9%saline led to positive solute balance in 27% patients
Hypertonic Osm>150
Continued…

•Positive solute balance contributed 56% cases
•Primary reason was inadequate substitution of hypotonic losseswith isotonic or hypertonic fluids
•Impaired sensorium and inability to express thirst leading to
Am J Kidney Dis 2009 Oct, 54:674-679
tonicity balance in patients with Hypernatremia Acquired in the Intensive Care Unit
Gregor L, Nikolaus K, Ulrike Holzinger, Wilfred Druml, christiph schwartz
•Impaired sensorium and inability to express thirst leading to inadequate intake of free water
Community acquired hypernatremia- hypovolemic hypernatria
ICU- euvolemic or hypervolemic hypernatremia
Continued…Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Am J Kidney Dis 2009 Oct, 54:674-679
tonicity balance in patients with Hypernatremia Acquired in the Intensive Care Unit
Gregor L, Nikolaus K, Ulrike Holzinger, Wilfred Druml, christiph schwartz
Characteristics of patients Continued…Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Am J Kidney Dis 2009 Oct, 54:674-679
tonicity balance in patients with Hypernatremia Acquired in the Intensive Care Unit
Gregor L, Nikolaus K, Ulrike Holzinger, Wilfred Druml, christiph schwartz
Characteristics of patientsUbaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Patients admitted over 1 year medical, surgical or neurological ICU
Renal dysfunction, Hypokalaemia, hypercalcemia, mannitol, sodium bicarbonate•more common in cases
hypernatremia ≥150 mmol/l in the ICU
Nephrol Dial Transplant 2008,23:1562-1568Hypernatremia in critically ill patients: too little water and too much salt
Ewout J. Hoorn, Mecheil G.H.Betjes, Joachim Weigel, Robert Zietse
•more common in cases •independently associated with hypernatraemia.
• mortality was higher in case•Hypernatremia was independent predictor
Continued…Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

•Approximately half of cases were polyuric, even when fluid balance was negative+
•Impaired thirst mechanism•Inappropriate iv fluid administration with isotonic fluids
Nephrol Dial Transplant 2008,23:1562-1568Hypernatremia in critically ill patients: too little water and too much salt
Ewout J. Hoorn, Mecheil G.H.Betjes, Joachim Weigel, Robert Zietse
•Aim of treatment- negative solute balance•Hypotonic fluid may aggravate fluid overload
•Diuretic may be considered: combination of loop diuretic and water or thiazide diuretic alone
Continued…Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Potential factors contributing to hypernatremia
Page 1566
Nephrol Dial Transplant 2008,23:1562-1568Hypernatremia in critically ill patients: too little water and too much salt
Ewout J. Hoorn, Mecheil G.H.Betjes, Joachim Weigel, Robert Zietse
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Use of hypotonic fluid is avoided in ICU
Capillary leakiness in sepsis patientsCapillary leakiness in sepsis patients
Fear of hyponatremia as many patient show non osmotic release ofVasopressin
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

JUST ANJUST ANANALYSIS
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

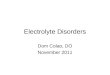
Nephrol Dial Transplant 2008,23:1562-1568Hypernatremia in critically ill patients: too little water and too much salt
Ewout J. Hoorn, Mecheil G.H.Betjes, Joachim Weigel, Robert Zietse
•47-year-old male •(body weight 95 kg)
•cystectomy complicated byfaecal peritonitis.
•Hypernatraemia in1day
Tonicity balance illustrating mechanism of hypernatremia
•Hypernatraemia in1day
•large isotonic volume resuscitation,+ hypertonic fluids (NaHCO3)
•Water loss•Renal: renal insufficiency and
hyperglycaemia •non-renal: wound drains and
colostomy
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Intensive Care Med 2001;27:921-924Tonicity balance, and not electrolyte free water calculations, more accurately
guide therapy for acute change in natremiaA.P.C.P. Carlotti, D. Bohn, J.P. Mallie, M.L. Halperin
14 year old male( weight 40 kg, total body water 24 L)
Operated for craniopharyngioma
During surgery• excreted 4L in 9 hours
TBW* ( [S.Na] /140 ) - 1
• excreted 4L in 9 hours
Over this period •P.[Na] rose from 140 to 157 meq/L
• received 3 L of isotonic saline
•His urine [Na+K] was 50 meq/L.
Free Water deficit: 24* [ (157/140) – 1 ] = 2.9 L
2.9L
2.9L
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Intensive Care Med 2001;27:921-924
Tonicity balance, and not electrolyte free water calculations, more accurately guide therapy for acute change in natremia
A.P.C.P. Carlotti, D. Bohn, J.P. Mallie, M.L. Halperin
4 L urine with 200meq Na= 1.3 L isotonic saline + 2.7 L of EFW
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

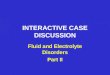
Intensive Care Med 2001;27:921-924Tonicity balance, and not electrolyte free water calculations, more accurately
guide therapy for acute change in natremiaA.P.C.P. Carlotti, D. Bohn, J.P. Mallie, M.L. Halperin
Na 200 mmol
Tonicity balance
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Intensive Care Med 2001;27:921-924Tonicity balance, and not electrolyte free water calculations, more accurately
guide therapy for acute change in natremiaA.P.C.P. Carlotti, D. Bohn, J.P. Mallie, M.L. Halperin
1
3 situations with hypernatremia and negative balance of 2.7 L of EFW
2
3
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPERNATREMIAHYPERNATREMIA
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPERNATREMIA
True/ Relative water deficit
S. Na > 145 meq/L
Clinical manifestation
ThirstThirstLethargy, irritability, restlessness
Spasticity, hyperreflexia, seizure, comaDeath
Cerebral Hemorrhage/ ischemiaInsulin resistance, impaired gluconeogenesis
Cardiac dysfunction
Severity of symptoms correlate with rate and magnitude of change in [Na]
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

APPROACHAPPROACH
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Hypernatremia
Hypertonic saline loadNaHCO3, 3% salineHyperaldosteronismCushing’s syndrome
Primary Na gain
HYPERVOLEMIA
Hypotonicfluid loss
HYPOVOLEMIAISOVOLEMIA
Extra renal lossRenal loss
DiuresisOsmotic
glucose, urea, mannitol, high osmolar feeds
Diuretics- frusemide, thiazide
Insensible lossFever, burn
Diabetes insipidusCDI
NDIrenal disease
Drugs- amphoterecin, aminoglycosides, lithiumElectrolyte disorders- hypokalemia, hypercalcemia
Azotemia out of proportion to decrease in GFR
Catabolic patients withModerate renal
insuficiency on high protein diet and stress
dose steroid
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Excretion of small volume (<800 ml)
Appropriate response to hypernatremia
Excretion of small volume (<800 ml)Of
concentrated urine (Osm U > 800 mOsm/L)
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Hypernatremia
Urine volume
Hypotonicfluid loss
>1000 ml<800 ml
Urine osmolality
< 300300 - 800
HYPOVOLEMIA/ ISOVOLEMIA
Urine osmolality>800
Insensible lossesdiuretics
Response to dDAVP
Osmotic diuresis + complete CDI_ complete NDI
Inheritedlithium
Urine osmoleexcretion /day <900 mOsm/day
>900 mOsm/day
+ complete CDI with hypovolemia+ Partial CDI
- partial NDIRenal tubular disease
Drugselectrolyte disturbances
>800
Response to dDAVP
Solute diuresis
Water diuresis

MANAGEMENTMANAGEMENT

HYPERNATREMIACorrection
Risk : development of brain odema
Chronic hypernatramia- brain cells fully adaptedRisk is more
Rate of correction
Acute hypernatremia: 1-2 meq/L/h ( 10-12 meq/L/day)
Chronic hypernatremia: 0.5 meq/L/h ( 8-10 meq/L/day)
Rate of correction
GOALNa <145
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPERNATREMIACorrection
TBW* ( [S.Na] /140 ) - 1
EFW deficit calculation (L)
Water deficit calculation (L)Water deficit calculation (L)Madias and Adrogue equation
Scan Page 74 JW LEE
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Mind it
Ongoing lossMust be considered
along with calculated water deficit
Formulas assume a closed systemRequire separate account of ongoing losses
as
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

70 kg women Diarrhoea of volume 2 L/ day
S.[Na]= 160meq/L , S.[K]= 3.0meq/L
75 – 160 / (70*50) + 1 = - 2.3 meq/ L
Estimated change in S.[Na] with 1 L of N/2 saline
change of 10 meq/L = 4.3L of N/2 saline has to be given in 24 hours
But ongoing loss = 0.7 L + 2.0 L = 2.7 L / 24 hours
Total volume to be given
4.3 L + 2.7 L = 7.0 L / 24 hours
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Hypernatremia
Hypotonic fluid ± diuretic
Urine output < water replacement
HYPERVOLEMIA Hypotonicfluid loss
HYPOVOLEMIAISOVOLEMIA
Insensible lossDiabetes insipidus
Osmotic diuresis
Insensible lossDiabetes insipidus
Hemodynamically unstableCorrect volume with isotonic saline
Switch over to hypotonic fluid toto correct Na
Remove / treat cause of DIReplace losses with hypotonic fluid
CDIDdavp
NDIlow Na diet + thiazide ± low protein diet ± NSAID
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPERNATREMIAsummary of management
Hemodynamic unstable: resuscitate with isotonic fluid (0.9% saline or RL)
Switch over to hypotonic fluid once resuscitated
Hypovolemic hypernatremia: AIM- positive EFW and solute balance
isovolemic hypernatremia: AIM- positive EFW balance
Replace losses with Hypotonic fluidTreatment of cause: DI
Hypervolemic hypernatremia: AIM- negative EFW and solute balance
Na restriction + Hypotonic fluid + frusemide
CDI: ADH analoguedDAVP: 10-20 ug intranasal bd
or 1-2ug sc bd
NDIremove/ correct causative agent
Thiazide/ indomethacin
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

hypernatremia
Duration of hypernatremia
Absent/ mild neurologic signs
[Na] ≥155 meq/L
Severe neurologic compromise
Initial acute management of
[Na] <155 meq/L
Search for alternative cause of neurologic compromize
Duration of hypernatremia[Na] ≥155 meq/L
5% dextrose
Initial goalFall of [Na] by 1.5-2.0 meq/L/h
for 3-4 hours or until symptoms resolveChange in [Na] can occur rapildlyImmediate attainment to normal
Is not goal
[Na] <155 meq/L
< 2 days
> 2 days
Change in [Na] should not exceed 10 meq/L in first 24 hours
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

DIABETES INSIPIDUS
Hypotonic urine in face of hyperosmolar plasma
CDI- Osm U <200NDI- Osm U 200-500
Water restriction: failure of Osm U to rise by 50 mOsm/ L in first few hours
Vasopressin- CDI Osm U rise by atleast 50% immediately
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPONATREMIAHYPONATREMIA

HYP0NATREMIA
True/ Relative water excess
S. Na < 135 meq/L
Clinical manifestation
headache, nausea lethargy, disorientation, restlessnesslethargy, disorientation, restlessness
Muscle cramp, weakness, depressed reflexes, seizures, comaDeath
Chronic hyponatremia: developing over >48 hours
Adaptative mechanism minimize symptoms
Severity of symptoms correlate with rate and magnitude of fall in [Na]
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

APPROACH APPROACH
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

hyponatremia
Hypertonic HypoNaHyperglycemia
Hypertonic sodium free sol(mannitol)
Hypotonic HypoNa
Isotonic HypoNaPseudohyponatremia
Hyperlipidemiahyperproteinemia
Normal serum osmolality
low serum osmolality
high serum osmolality
Assess serum osmolality
hypotonic Hypovolemichyponatremia
Assess volume status
isovolemichypovolemic hypervolemic
hypotonic isovolemic hyponatremia
hypotonic HypervolemicHyponatremia
CirrhosisCongestive heart failure
Nephrotic syndromeRenal falire
Discussed in next pages

DiuresisOsmotic- glucose, urea, mannitol
Diuretics- thiazide, frusemide
Electrolytes-Hypokalemia, hypercalcemiaDrugs- aminoglycoside, ampho B
hypotonic Hypovolemic Hyponatremia
Adrenal deficiencyMineralocorticoid deficiency
Renalloss
LOSS (both water and Na) = Negative water and Na balance
Salt wasting nephropathyCerebral salt wasting
GI lossnaso gastric aspirate,
abdominal Drains/ fistulathird space loss
(pancreatitis, ileus, obstruction)
Vomiting, diarrhea
Non renalloss
Skin lossfever
open wounds,burns
hemorrhage

Acute psychosisCNS disorders
Hypotonic Isovolemic Hyponatremia
Drug inducedOpiodsNSAIDS
Antipsychotics- haloperidolSSRI- fluoxetine, sertraline
Pain, nausea, stress
SIADH
Impaired free water loss in urine Normal Na loss in urine
hypothyroidism
TCACarbamezapineantineoplastics
Pulmonary diseaseInfections
malignancy
Cortisol deficiency

CORRECTION CORRECTION

PRECAUTION IN CORRECTION
Absolute magnitude of correction in 24 hoursmore important than rate
central pontine myelinosis
Initial rapid rate of correction tapering off after several hoursincurs less risk
thanslow steady correction that exceeds 12 meq/L in 24 hours
Increased riskHypoxemia, hypokalemia, malnutrition, alcoholism
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPONATREMIA
1-2 meq/L/h ( 10-12 meq/L/day)
Rate of correction
Symptomaticor
Acute hyponatremia (change >0.5 meq/L/h or onset in < 48 hours)
0.5 meq/L/h ( 8-10 meq/L/day)Chronic hyponatremia
(Change over > 48 hours or unknown duration)Increased risk of CPM
as adaptive mechanism has occured
120-130 meq/LLower iin patients with s.Na<105GOAL of Correction
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Any saline solution that is hyperosmolar to urine can increase [Na]when
oral water intake is restricted
Mind itRULE FOR CORRECTION
A crystalloid with an osmolarity less than urine osmolaritymay actually worsen hyponatremia,
even if the fluid [Na] is greater than serum [Na]
CONTINUED….
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Na=118
Gain of 154 mOsm will be lost in 300 ml urineGain of 700 ml of EFW
(154* 1000/500= 300 ml, OsmU > 500)
60 years male, febrile encephalopathyBody weight: 60 kg, TBW: 36 L
Develops SIADH
S.[Na]= 118, urine Osm > 500 mOsm/L
Given 1 L of 0.9% saline
ONE RULE FOR CORRECTION
Na=154
Water=1000
Na=0
water= 700 Water= 300
Na=154
Na=115
Na=118
Simultaneous IV loop diuretic can counteract this phenomenon By promoting free water excretion
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPONATREMIACALCULATION OF [Na] deficit
TBW* ( 140 – s.Na)
Na deficit (meq)
Anticipated change in s.Na with 1L of fluidAnticipated change in s.Na with 1L of fluid(Madias and Adrogue equation)
Scan Page 74 JW LEE
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPONATREMIA
Remove or treat cause of hypertonicity
Hypertonic HypoNaHyperglycemia
Hypertonic sodium free sol(mannitol)
Repeat labUse newer method of lab
Isotonic HypoNaPseudohyponatremia
Hyperlipidemiahyperproteinemia
Fluid shift to ICF compartment does not take placeNeuronal cell swelling does not occur
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

hypotonic hyponatremia
Primary polydypsiaBeer potomania
Post TURP
urine osmolality <100 mOsm/L
Assess urine osmolality
Assess volume statusEFW restriction± loop diuretic
Correct hypokalemia
hypovolemic
urine osmolality > 100 mOsm/L
Urine [Na]<10meq/L
Urine [Na]>20meq/L
Renal loss Non renal loss
hypovolemic
TreatmentcIsotonic saline to correct hypovolemia
Correct hypokalemia if present
hypervolemic
IsovolemicContinued
on next page
Continued….
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

hypotonic hyponatremia
Assess volume status
Urine [Na]<10meq/L
Urine [Na]>20meq/L
hypervolemic
urine osmolality > 100 mOsm/L
Urine [Na]>20meq/L
Isovolemic
<10meq/L>20meq/L
Renal failureCirrhosis
Congestive heart failureNephrotic syndrome
EFW restriction(restriction less than urine output)
>20meq/L
SIADHHypothyroidism
Cortisol deficiency,
Administer saline with osmolality more than urine osmolality
Loop diureticADH antagonist
Treat underlying diseaseStop drug causing increased ADHsecretion
Correct hypokalemia if present
TREATMENT
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

HYPONATREMIAsummary of management
Replace calculated Na deficit with isotonic saline or RL
hypotonic Hypovolemic hyponatremiaAIM- positive water and Na balance
hypotonic isovolemic hyponatremiaAIM- negative EFW and positive Na balance
Symptomaticfrusemide ivi + 3% saline
AsymptomaticWater restriction ± Intermittent frusemide ± enteral salt
hypotonic Hypervolemic hyponatremiaAIM- negative EFW and Na balance
Na and EFW restriction + frusemide
ADH antagonist( for chronic SIADH as delayed onset of action)
demeclocycline HCL: 600-1200mg PO dailyPhenytoin sod: 200-300mg PO daily
Lithium: 600-1200mg PO daily
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

hyponatremia
Duration of hyponatremia
Absent/ mild neurologic signs
[Na] < 125 meq/L
Severe neurologic compromise
Initial acute management of
[Na] >125 meq/L
Search for alternative cause of neurologic compromize
Duration of hyponatremia[Na] < 125 meq/L
3% saline ivi
Initial goalincrease [Na] by 1.5-2.0 meq/L/h
for 3-4 hours or until symptoms resolveChange in [Na] can occur rapildlyImmediate attainment to normal
Is not goal
[Na] >125 meq/L
< 2 days
> 2 days
Change in [Na] should not exceed 10 meq/L in first 24 hours and
18 meq/L in first 48 hours
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

SOLUTION= SOLUTE+ SOLVENT
Molality: number of moles of a solute per kilogram of solventMolarity: number of moles of solute per litre of solution
Osmolality: number of osmoles of solute per kilogram of solventOsmolarity: number of osmoles of solute per litre of solutionOsmolarity: number of osmoles of solute per litre of solution
Tonicity = effective osmolality sum of the concentrations of the solutes which have the capacity to exert an
osmotic force across the membrane.
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Free water (FW)Calculated base on osmolality
(Na, Glucose, BUN)
As urea is freely permeable across all cell membraneDoes not contribute to effective osmolality ie tonicity
Electrolyte free water (EFW)Calculation based on S.[Na}
Modified Electrolyte free water (MEFW)Calculation takes into consideration Glucose along with s.[Na]
Ubaidur Rahaman, Senior Resident, CCM, SGPGIMS, Lucknow, India

Thank YouThank You