Embed Size (px)
Citation preview
Electrolyte Electrolyte DisordersDisorders
Resident RoundsResident Rounds
Aric StorckAric Storck
February 26, 2004February 26, 2004
Case 1Case 1 75 yo woman75 yo woman
orthostatic presyncope x 2 daysorthostatic presyncope x 2 days diarrhea x 1 weekdiarrhea x 1 week drinking 2-3 litres of tea a daydrinking 2-3 litres of tea a day
PMHxPMHx HTNHTN
MedsMeds HCTZ 25 mg po odHCTZ 25 mg po od
O/EO/E JVP ASAJVP ASA significant orthostatic drop in BPsignificant orthostatic drop in BP
lablab Na 128Na 128 K 3.1K 3.1 Cr 125Cr 125
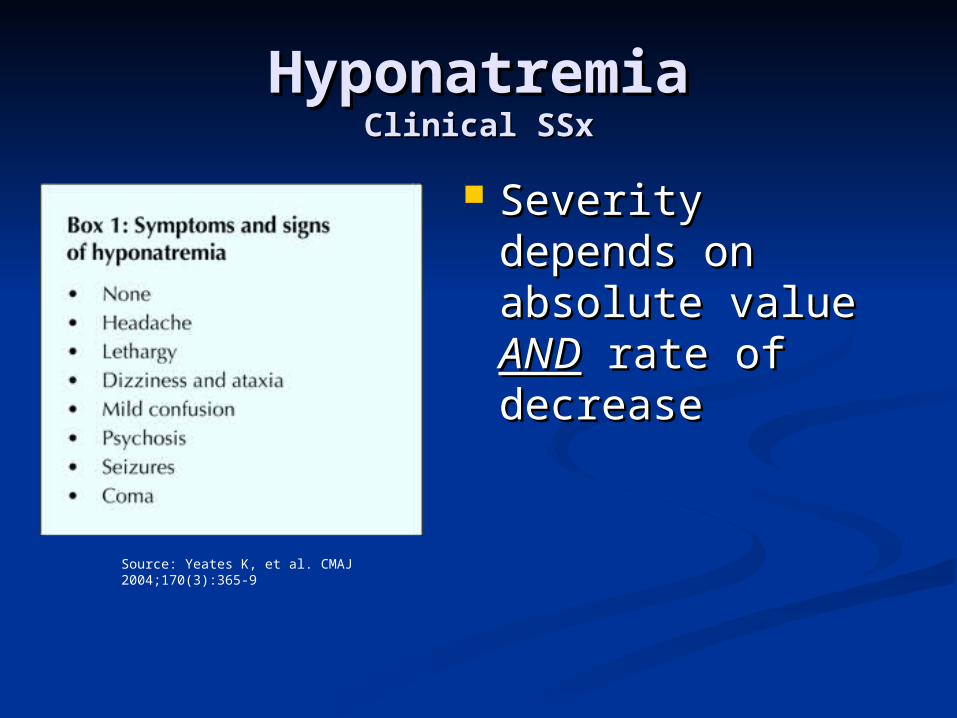
HyponatremiaHyponatremiaClinical SSxClinical SSx
Severity depends Severity depends on absolute value on absolute value ANDAND rate of rate of decreasedecrease
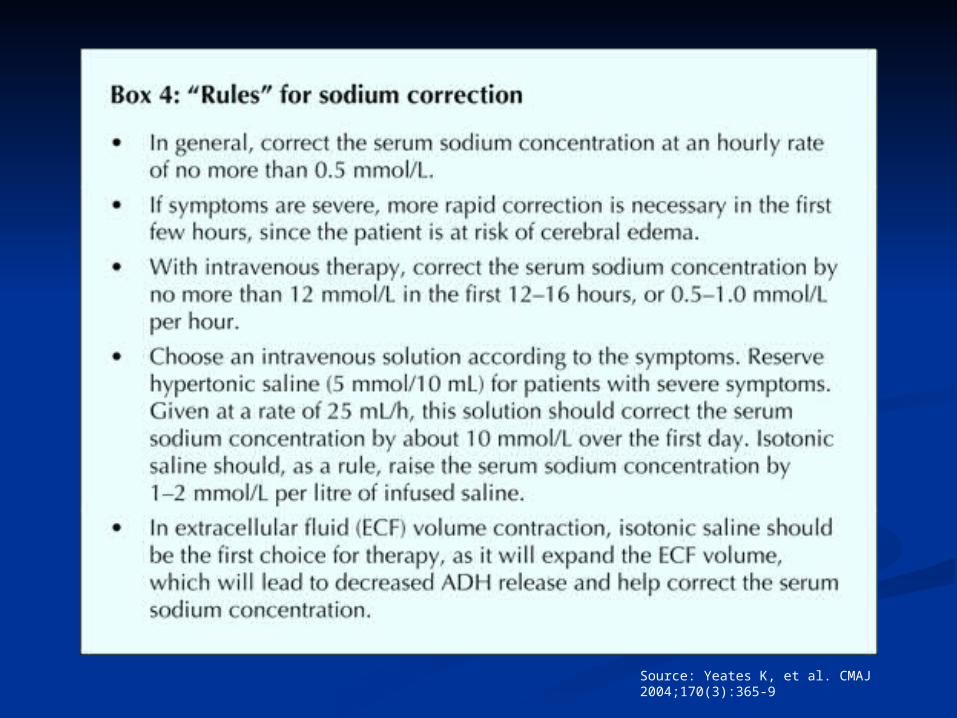
Source: Yeates K, et al. CMAJ 2004;170(3):365-9

SymptomsSymptoms
DeliriumDeliriumComa Coma
SeizuresSeizures
< 120< 120
WeaknessWeaknessLethargyLethargy
RestlessnessRestlessnessConfusionConfusion
125 - 120125 - 120
ThirstThirstAnorexia, N + VAnorexia, N + VMuscle crampsMuscle cramps
130 - 125130 - 125
Decreased tasteDecreased taste135 - 130135 - 130
SymptomsSymptomsSerum NaSerum Na++ (mEq/L) (mEq/L)
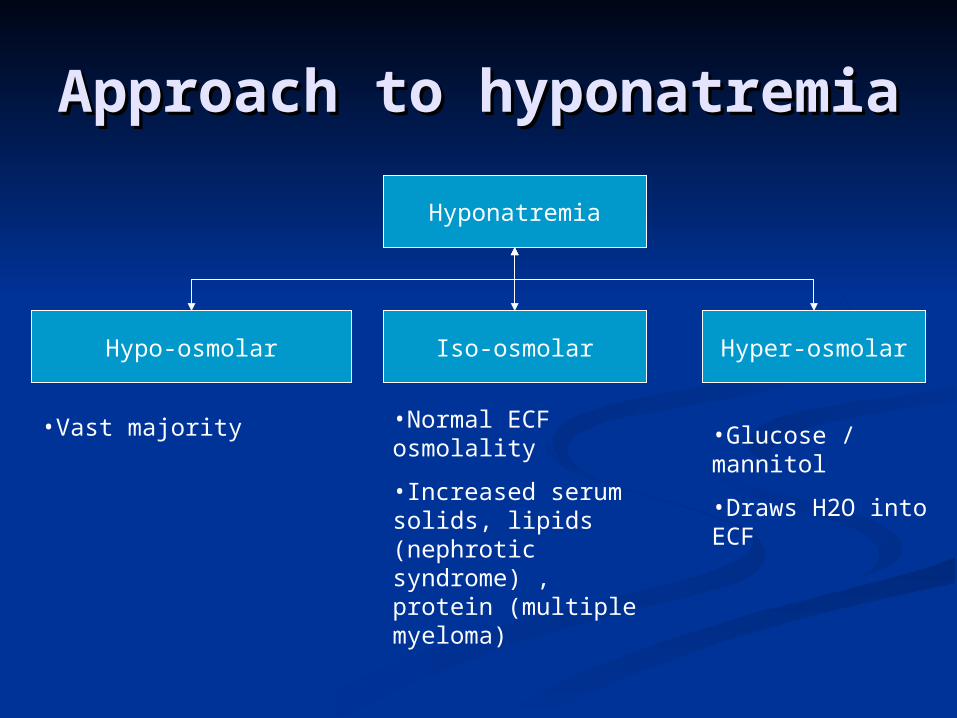
Approach to Approach to hyponatremiahyponatremia
Hypo-osmolar Iso-osmolar Hyper-osmolar
Hyponatremia
•Normal ECF osmolality
•Increased serum solids, lipids (nephrotic syndrome) , protein (multiple myeloma)
•Glucose / mannitol
•Draws H2O into ECF
•Vast majority
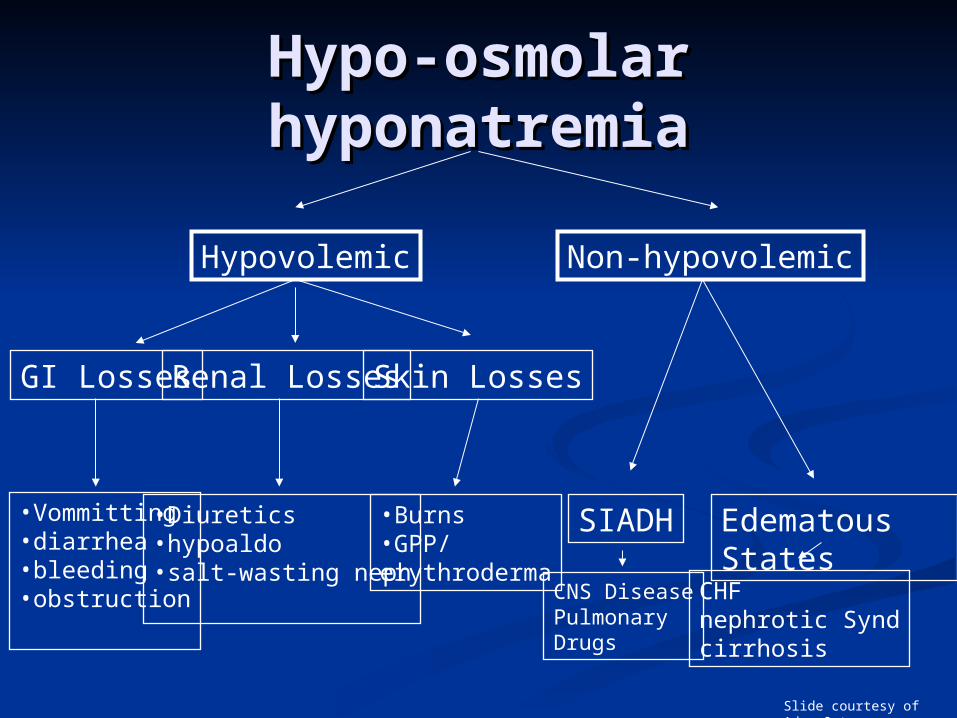
Hypo-osmolar Hypo-osmolar hyponatremiahyponatremia
Non-hypovolemicHypovolemic
GI Losses Renal Losses Skin Losses
SIADH Edematous States•Vommitting•diarrhea•bleeding•obstruction
•Diuretics•hypoaldo•salt-wasting neph
•Burns•GPP/erythroderma
CNS DiseasePulmonary Drugs
CHFnephrotic Syndcirrhosis
Slide courtesy of Adam Oster
Hypovolemic Hypovolemic HyponatremiaHyponatremia
Loss Na > Loss H2OLoss Na > Loss H2O
ADH released (low ECF)ADH released (low ECF) increases tubular reabsorption of H2Oincreases tubular reabsorption of H2O low urine volumelow urine volume
Renin released (low renal perfusion)Renin released (low renal perfusion) kidneys retain sodiumkidneys retain sodium urine sodium low (<20 mmol/L)urine sodium low (<20 mmol/L)
What caused our patient’s What caused our patient’s hyponatremia?hyponatremia? GI lossesGI losses HCTZ (impairs excretion of free HCTZ (impairs excretion of free
water)water) as ECF decreases kidney exchanges as ECF decreases kidney exchanges
K for Na to maintain volume - thus K for Na to maintain volume - thus low Klow K
How will you treat our patientHow will you treat our patient d/c HCTZd/c HCTZ oral rehydration saltsoral rehydration salts IV NS + KCl until no further postural IV NS + KCl until no further postural
dropdrop oral sodium and Koral sodium and K recheck lytes in a few daysrecheck lytes in a few days
Case 2Case 2
58 yo man58 yo man small cell lung small cell lung
cancercancer confusion & confusion &
lethargy x 2 dayslethargy x 2 days
No MedsNo Meds
O/EO/E JVP 3cmJVP 3cm MMMMMM no ascites / no no ascites / no
edemaedema no sign of no sign of
hypothyroidism or hypothyroidism or hypoadrenalismhypoadrenalism
lablab
Na 108Na 108 K 3.9K 3.9 Cr 44Cr 44 urine Na 44urine Na 44
Euvolemic HyponatremiaEuvolemic HyponatremiaDDxDDx
SIADHSIADH hypothyroidismhypothyroidism adrenal insufficiencyadrenal insufficiency psychogenic polydipsiapsychogenic polydipsia
SIADHSIADH
DiagnosisDiagnosis
clinically euvolemicclinically euvolemic normal renal functionnormal renal function normal thyroid (TSH)normal thyroid (TSH) normal adrenal (cortisol stim test)normal adrenal (cortisol stim test) no medications known to cause SIADH-no medications known to cause SIADH-
like syndromelike syndrome
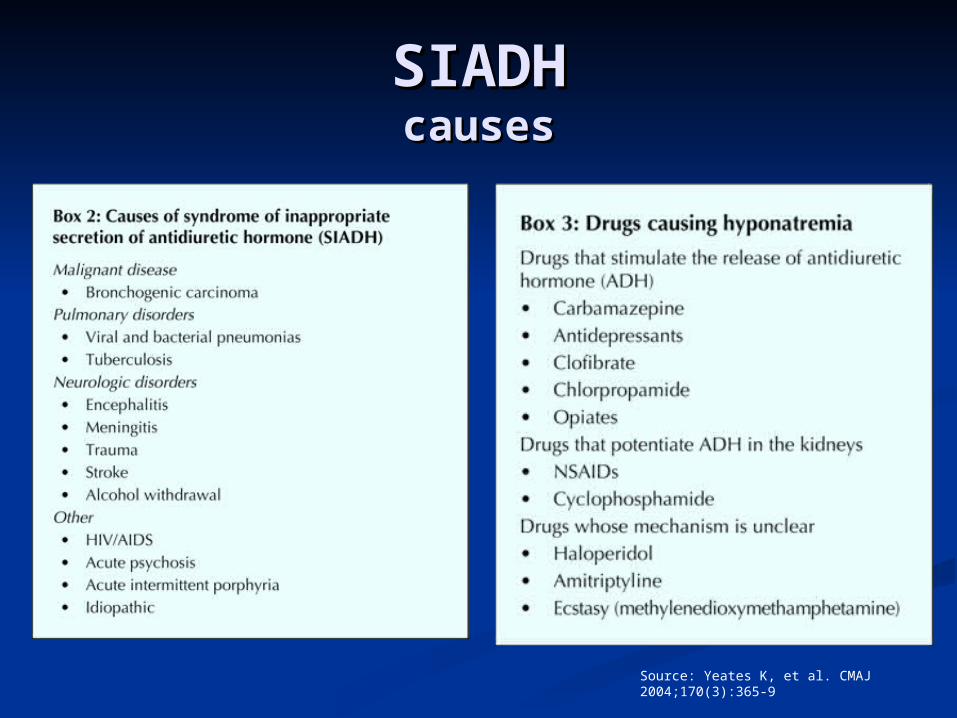
SIADHSIADHcausescauses
Source: Yeates K, et al. CMAJ 2004;170(3):365-9
SIADH - TreatmentSIADH - Treatment acuteacute
hypertonic salinehypertonic saline goal to increase Na by ~5 over 12 hours or until goal to increase Na by ~5 over 12 hours or until
asymptomaticasymptomatic
fluid restrictionfluid restriction 750-1500 ml/d750-1500 ml/d goal to increase Na by ~5 over 12 hoursgoal to increase Na by ~5 over 12 hours
chronicchronic fluid restrictionfluid restriction Li (inhibits renal effects of ADH)Li (inhibits renal effects of ADH) demeclocycline 600 mg po od demeclocycline 600 mg po od
What happens if you use What happens if you use normal saline?normal saline?
More water retained than NaMore water retained than Na
worsening hyponatremiaworsening hyponatremia
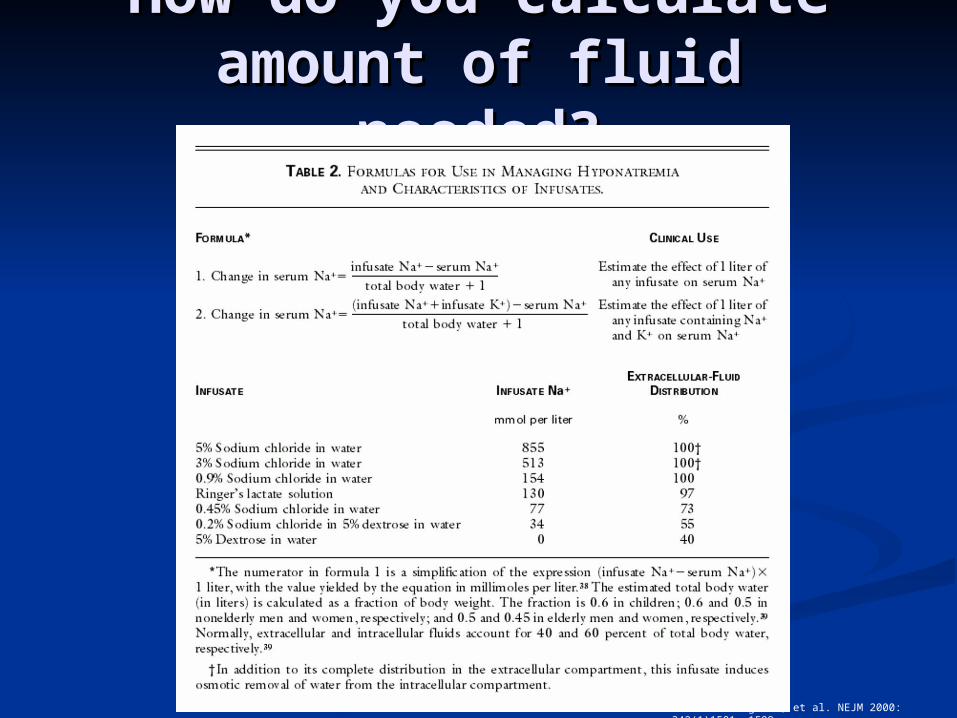
How do you calculate How do you calculate amount of fluid amount of fluid
needed?needed?
Source: Adrogue H, et al. NEJM 2000: 342(1)1581--1589.
Sample calculationSample calculation
Change [Na] per litre 3% HTS = Change [Na] per litre 3% HTS =
(513-108) / (0.6x60 +1) (513-108) / (0.6x60 +1)
=10.8 mmol=10.8 mmol
thus 0.46 litres (5/10.8) over 12 hoursthus 0.46 litres (5/10.8) over 12 hours
==38ml/h x 12 hours38ml/h x 12 hours
Case 3Case 3
45 year old woman45 year old woman alcoholic, HCV, end stage hepatic alcoholic, HCV, end stage hepatic
diseasedisease gross ascites and peripheral edemagross ascites and peripheral edema Na 125Na 125
Hypervolemic Hypervolemic hyponatremiahyponatremia
Increased ECFIncreased ECF CHFCHF cirrhosis / ascitescirrhosis / ascites nephrotic syndromenephrotic syndrome
low effective circulating volumelow effective circulating volume body retains Na and H20body retains Na and H20 low urine Na (<20)low urine Na (<20)
TreatmentTreatment Na and free water restrictionNa and free water restriction
Source: Yeates K, et al. CMAJ 2004;170(3):365-9
PseudohyponatremiaPseudohyponatremia
= falsely low Na+ due to:= falsely low Na+ due to: high serum protein concentrationhigh serum protein concentration high serum lipidshigh serum lipids
was an issue w/ flame photometry but not was an issue w/ flame photometry but not w/ potentiometric measurment techniquesw/ potentiometric measurment techniques
Slide courtesy of Moritz Haager
Redistributive Redistributive HyponatremiaHyponatremia
= dilutional picture due to presence = dilutional picture due to presence of excess osmotically active of excess osmotically active substances drawing water out of substances drawing water out of cells into extracellular spacecells into extracellular space Hyperglycemia (e.g. DKA)Hyperglycemia (e.g. DKA)
Correction = ~3mmol NaCorrection = ~3mmol Na++ decrease for decrease for every 10 mmol increase in glucoseevery 10 mmol increase in glucose
MannitolMannitol
Slide courtesy of Moritz Haager
Case 4Case 4 Your med student saw the pt and Your med student saw the pt and
w/o discussing with you ordered a 1 w/o discussing with you ordered a 1 L bolus of NS X 2 and then 200 cc/hL bolus of NS X 2 and then 200 cc/h
The pts NaThe pts Na+ + corrects to 138 by next corrects to 138 by next AMAM
Pt is sent home asymptomatic 36 hrs Pt is sent home asymptomatic 36 hrs after admissionafter admission
Comes back 3 days later unable to Comes back 3 days later unable to stand, confused, with slurred speechstand, confused, with slurred speech
What’s going on?What’s going on?
Slide courtesy of Moritz Haager
CPMCPM central pontine myelinolysiscentral pontine myelinolysis
PathophysiologyPathophysiology Acute non-inflammatory demyelination in basis Acute non-inflammatory demyelination in basis
pontis and other CNS sites (in ~10%)pontis and other CNS sites (in ~10%) Mechanism unknown; felt to occur due to rapid Mechanism unknown; felt to occur due to rapid
changes in cell volumechanges in cell volume Actual incidence is unknownActual incidence is unknown Risk factorsRisk factors
NaNa++ <120 mEq/L for > 48 hrs <120 mEq/L for > 48 hrs Aggressive IV resuscitation w/ hypertonic salineAggressive IV resuscitation w/ hypertonic saline
Most cases occurred with rates of correction Most cases occurred with rates of correction >> 12 12 mmol/L /24 hrsmmol/L /24 hrs
Hypernatremia during treatmentHypernatremia during treatment
Slide courtesy of Moritz Haager
CPMCPM central pontine myelinolysiscentral pontine myelinolysis
Clinical FeaturesClinical Features Usually neurologic deterioration 48-72 Usually neurologic deterioration 48-72
hrs after rapid Nahrs after rapid Na++ correction correction Confusion, horizontal gaze paralysis, Confusion, horizontal gaze paralysis,
spastic quadriplegia, pseudobulbar palsy, spastic quadriplegia, pseudobulbar palsy, encephalopathy – coma, locked-in encephalopathy – coma, locked-in syndromesyndrome
DxDx MRIMRI
TxTx supportivesupportive
Slide courtesy of Moritz Haager
TreatmentTreatmentsummarysummary
Hypovolemic hyponatremiaHypovolemic hyponatremia Correct with NS (0.9%) which is mildly hypertonic Correct with NS (0.9%) which is mildly hypertonic
compared to pts serumcompared to pts serum
Euvolemic hyponatremia:Euvolemic hyponatremia: Restrict free water intakeRestrict free water intake Identify underlying causeIdentify underlying cause SIADH:SIADH:
Giving normal saline will worsen condition due to free Giving normal saline will worsen condition due to free water retentionwater retention
Can Tx with lithium and demeclocycline Can Tx with lithium and demeclocycline inhibit action inhibit action of ADHof ADH
Hypervolemic hyponatremia:Hypervolemic hyponatremia: Restrict free water intakeRestrict free water intake +/- diuretics +/- diuretics may worsen due to further Na+ loss may worsen due to further Na+ loss dialysis if large amount of fluid needs to be taken dialysis if large amount of fluid needs to be taken
offoffSlide courtesy of M Haager
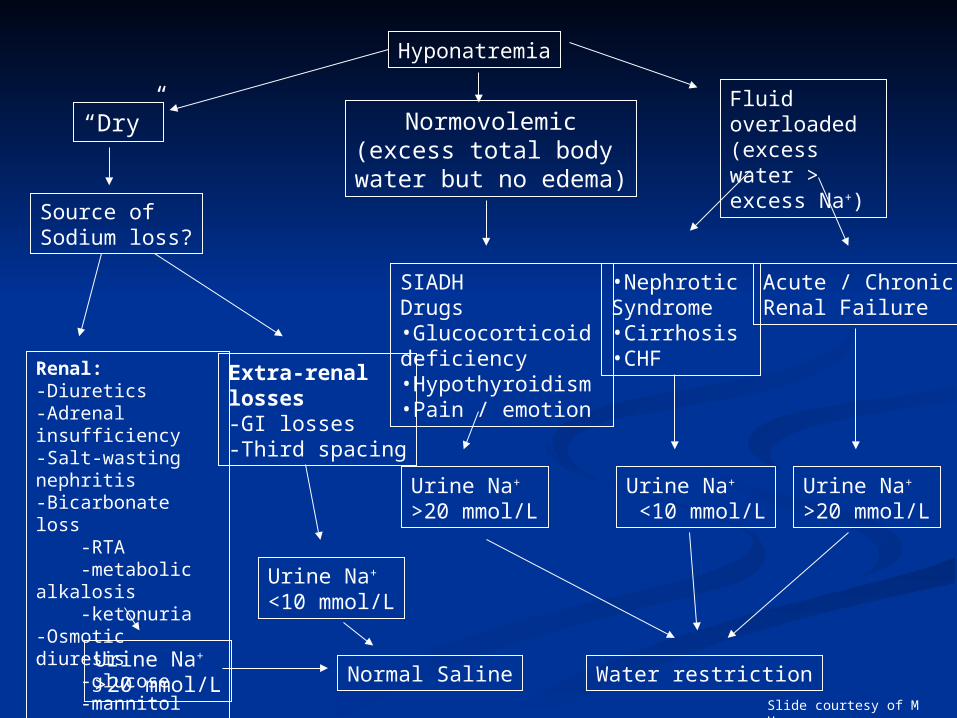
Hyponatremia
“Dry” Normovolemic(excess total body
water but no edema)
Fluid overloaded(excess water >excess Na+)
Source of Sodium loss?
Renal:-Diuretics-Adrenal insufficiency-Salt-wasting nephritis-Bicarbonate loss -RTA -metabolic alkalosis -ketonuria-Osmotic diuresis -glucose -mannitol
Extra-renal losses-GI losses-Third spacing
Urine Na+ >20 mmol/L
Urine Na+ <10 mmol/L
Normal Saline
SIADHDrugs•Glucocorticoid deficiency•Hypothyroidism•Pain / emotion
•Nephrotic Syndrome•Cirrhosis•CHF
Acute / ChronicRenal Failure
Urine Na+ >20 mmol/L
Urine Na+
<10 mmol/LUrine Na+ >20 mmol/L
Water restrictionSlide courtesy of M Haager
Case 5Case 5
93 year old man from nursing home93 year old man from nursing home dementeddemented not eating wellnot eating well less perky than usual - in ER to be less perky than usual - in ER to be
“checked out”“checked out” O/EO/E
JVP down, dry mouthJVP down, dry mouth 97 16 87/53 99% 37.397 16 87/53 99% 37.3
Na = 157Na = 157
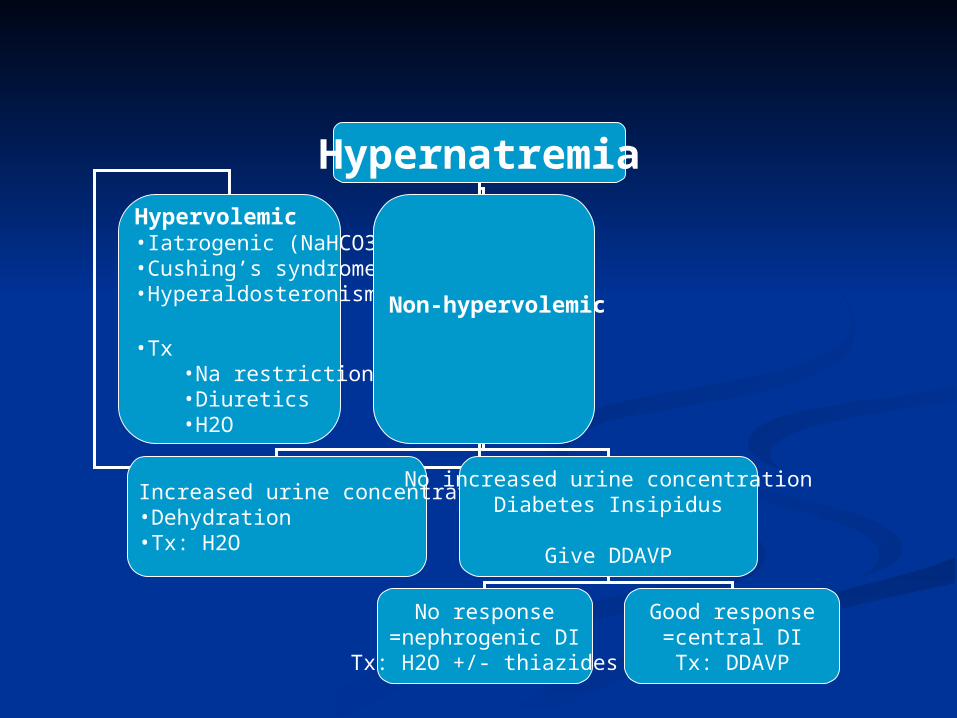
HypernatremiaHypervolemic•Iatrogenic (NaHCO3)•Cushing’s syndrome•Hyperaldosteronism
•Tx•Na restriction•Diuretics•H2O
Non-hypervolemic
Increased urine concentration•Dehydration•Tx: H2O
No increased urine concentrationDiabetes Insipidus
Give DDAVP
No response=nephrogenic DI
Tx: H2O +/- thiazides
Good response=central DITx: DDAVP
HypernatremiaHypernatremia
SymptomsSymptoms anorexiaanorexia N/VN/V fatiguefatigue irritableirritable
SignsSigns lethargylethargy stuporstupor comacoma muscle twitchingmuscle twitching hyperreflexiahyperreflexia spasticityspasticity tremortremor ataxiaataxia focal neurological focal neurological
signssigns
Causes of Causes of HypernatremiaHypernatremia
Reduced H2O intakeReduced H2O intake disorders of thirstdisorders of thirst can’t get H20can’t get H20
Increased H2O lossIncreased H2O loss GIGI
V&DV&D NGNG 3rd spacing3rd spacing
renalrenal DIDI osmotic diuresisosmotic diuresis post-obstructive diuresispost-obstructive diuresis
dermaldermal burnsburns perspirationperspiration
Gain in NaGain in Na exogenous Na intakeexogenous Na intake
NaClNaCl NaHCO3NaHCO3 hypertonic NShypertonic NS salt water drowningsalt water drowning
increased Na increased Na reabsorptionreabsorption
hyperaldosteronismhyperaldosteronism cushing’s diseasecushing’s disease exogenous exogenous
corticosteroidscorticosteroids congenital adrenal congenital adrenal
hyperplasiahyperplasia
Causes of DICauses of DI
CentralCentral idiopathicidiopathic head traumahead trauma cerebral hemorrhagecerebral hemorrhage suprasellar infectionsuprasellar infection granulomatous granulomatous
disordersdisorders
Systemic diseasesSystemic diseases sickle cellsickle cell sarcoidosissarcoidosis amyloidosisamyloidosis
NephrogenicNephrogenic congenital renal congenital renal
disordersdisorders obstructive uropathyobstructive uropathy polycystic diseasepolycystic disease
drugsdrugs amphotericin Bamphotericin B phenytoinphenytoin LiLi aminoglycosidesaminoglycosides methoxyfluranemethoxyflurane
Management of Management of hypernatremiahypernatremia
HypovolemicHypovolemic goal: restore goal: restore
volume deficitsvolume deficits 0.9% NS0.9% NS
EuvolemicEuvolemic DIDI
oral fluidsoral fluids hypotonic saline hypotonic saline
(0.45%)(0.45%) vasopressinvasopressin
HypervolemicHypervolemic increase renal increase renal
sodium excretion > sodium excretion > H20H20
diuretics +/- diuretics +/- hypotonic salinehypotonic saline
may need dialysismay need dialysis
Calculation of water Calculation of water deficitdeficit
Water deficit = Water deficit =
Weight (kg) x Weight (kg) x
( Normal [Na] / Measured [Na] - 1 )( Normal [Na] / Measured [Na] - 1 )
Case 6Case 6
53 year old man53 year old man DM 1, chronic renal DM 1, chronic renal
failurefailure presents via EMS presents via EMS
from homefrom home Wife tells you that Wife tells you that
he has had N/V/D he has had N/V/D for the last 4 days for the last 4 days with decreased po with decreased po intake.intake.
O/EO/E 140, 89/59, 26, 140, 89/59, 26,
94%, 37.394%, 37.3 JVP down, dry MMJVP down, dry MM Slightly tender Slightly tender
abdomenabdomen
What would you What would you like to order?like to order?
lablab
CBCCBC Hb 146Hb 146 WBC 35WBC 35
neutrophils 30neutrophils 30 0.3 bands0.3 bands
Platelets 223Platelets 223
LytesLytes Na 133Na 133 K 7.4K 7.4 HCO3 4HCO3 4 Cl 97Cl 97 Cr 223Cr 223 glucose 43glucose 43
Case 6Case 6ECGECG
HyperkalemiaHyperkalemiaClinical FeaturesClinical Features
CardiacCardiac 2/3 degree heart 2/3 degree heart
blockblock wide complex wide complex
tachycardiastachycardias VFVF asystoleasystole
ECG progressionECG progression peaked T wavespeaked T waves loss of P wavesloss of P waves prolonged PR prolonged PR
intervalinterval widening of QRSwidening of QRS sine wave patternsine wave pattern ventricular ventricular
fibrillationfibrillation asystoleasystole
HyperkalemiaHyperkalemiaNeurological SSxNeurological SSx
Non-specificNon-specific muscle crampsmuscle cramps weaknessweakness paralysisparalysis paresthesiasparesthesias tetanytetany focal neurological deficitsfocal neurological deficits
PotassiumPotassiuma precisely controlled cationa precisely controlled cation
Mostly intracellularMostly intracellular
Precise transcellular Precise transcellular gradients required for gradients required for neuronal transmission neuronal transmission and cardiac conductionand cardiac conduction
Also important in acid-Also important in acid-base balance and base balance and buffering.buffering. K+/H+ pumpK+/H+ pump
Extracellular K Extracellular K controlled by controlled by serum pHserum pH
change in pH of 0.1change in pH of 0.1 0.6mEq change in 0.6mEq change in
K+K+ aldosteronealdosterone insulin insulin catecholaminescatecholamines
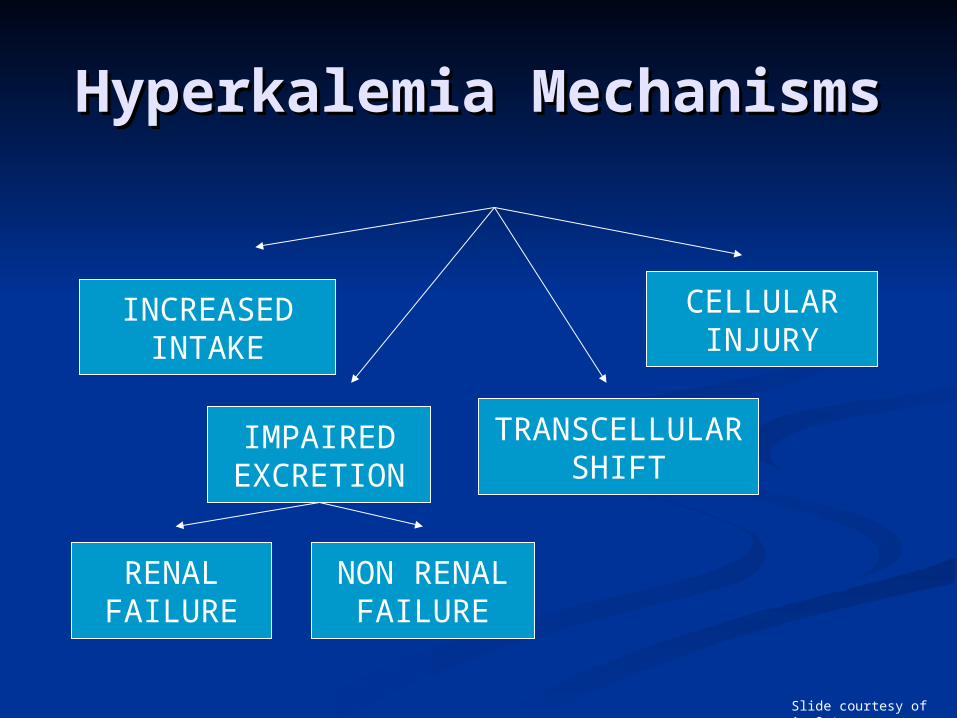
Hyperkalemia Hyperkalemia MechanismsMechanisms
INCREASEDINTAKE
IMPAIREDEXCRETION
TRANSCELLULARSHIFT
CELLULARINJURY
RENALFAILURE
NON RENALFAILURE
Slide courtesy of A. Oster
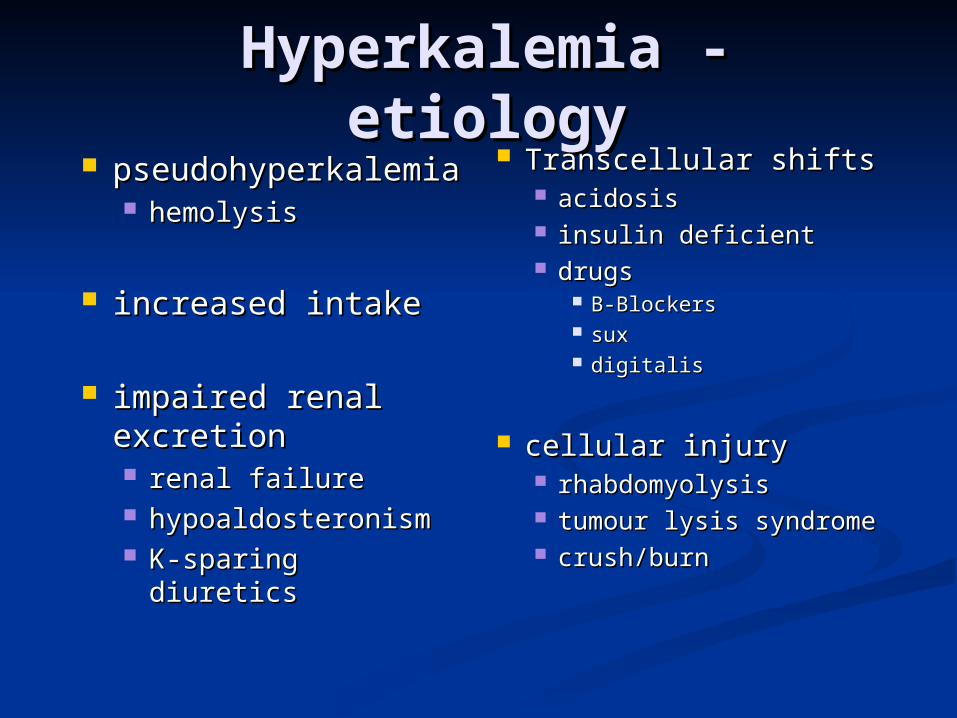
Hyperkalemia - etiologyHyperkalemia - etiology pseudohyperkalempseudohyperkalem
iaia hemolysishemolysis
increased intakeincreased intake
impaired renal impaired renal excretionexcretion renal failurerenal failure hypoaldosteronismhypoaldosteronism K-sparing diureticsK-sparing diuretics
Transcellular shiftsTranscellular shifts acidosisacidosis insulin deficientinsulin deficient drugsdrugs
B-BlockersB-Blockers suxsux digitalisdigitalis
cellular injurycellular injury rhabdomyolysisrhabdomyolysis tumour lysis tumour lysis
syndromesyndrome crush/burncrush/burn
Management PrinciplesManagement Principles
Cardiac monitoringCardiac monitoring stabilize myocardiumstabilize myocardium shift K into cellsshift K into cells decrease GI absorptiondecrease GI absorption treat underlying causetreat underlying cause
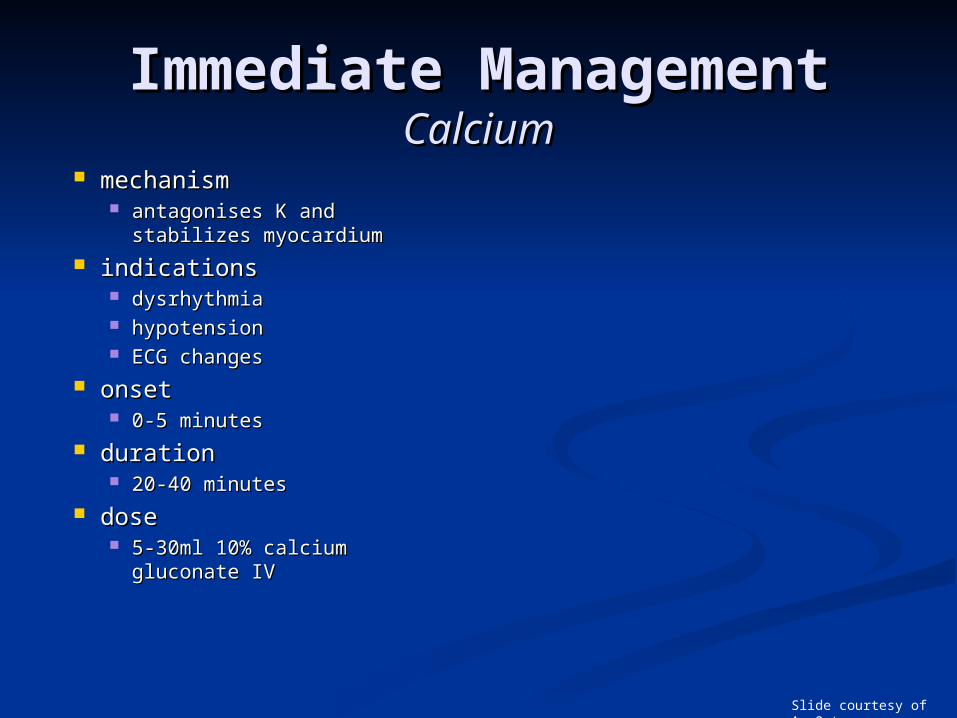
Immediate Immediate ManagementManagement
CalciumCalcium mechanismmechanism antagonises K and stabilizes antagonises K and stabilizes
myocardiummyocardium indicationsindications
dysrhythmiadysrhythmia hypotensionhypotension ECG changesECG changes
onsetonset 0-5 minutes0-5 minutes
durationduration 20-40 minutes20-40 minutes
dosedose 5-30ml 10% calcium 5-30ml 10% calcium
gluconate IVgluconate IV
Slide courtesy of A. Oster
Immediate ManagementImmediate ManagementVentolinVentolin
MechanismMechanism shifts K into cellsshifts K into cells
onsetonset 15 minutes15 minutes
durationduration 2-4 hours2-4 hours
dosedose 5-10mg neb 5-10mg neb
repeat prnrepeat prn
Slide courtesy of A. Oster
Immediate Immediate ManagementManagementGlucose and InsulinGlucose and Insulin mechanismmechanism
shifts K into cellsshifts K into cells onsetonset
15 minutes15 minutes durationduration
4-6 hours4-6 hours dosedose
10-20 units of R10-20 units of R 1 amp D50W1 amp D50W (no D50W if hyperglycemic)(no D50W if hyperglycemic)
Immediate ManagementImmediate Managementbicarbonatebicarbonate
mechanismmechanism shifts K into cellsshifts K into cells only works if only works if
acidoticacidotic
onsetonset 15 minutes15 minutes
durationduration 2 hours2 hours
dosedose 1 amp (44 meq) IV 1 amp (44 meq) IV
push over 5 push over 5 minutesminutes
beware ifbeware if hypertonichypertonic hypernatremichypernatremic alkaloticalkalotic
Delayed TherapyDelayed TherapyExchange ResinsExchange Resins
kayelalate (polystyrene sulfonate)kayelalate (polystyrene sulfonate) mechanismmechanism
ion exchange resinion exchange resin removes K from bodyremoves K from body
onsetonset 1 hour1 hour
durationduration 1-3 hours1-3 hours
dosedose 1g binds 1mEq of K1g binds 1mEq of K oral or rectaloral or rectal 20g in 70% sorbitol po (Rosen)20g in 70% sorbitol po (Rosen) 30g pr retained for 30 minutes30g pr retained for 30 minutes
MechanismMechanism removes K from bloodremoves K from blood can remove 200-300 meqcan remove 200-300 meq
IndicationsIndications renal failurerenal failure unstable patient unresponsive to other unstable patient unresponsive to other
treatmenttreatment
Delayed TherapyDelayed Therapyhemodialysishemodialysis
Case 6Case 6K+ 7.4K+ 7.4
Slide courtesy of A. Oster
Case 6Case 6 K+6.2K+6.2
Slide courtesy of A. Oster
Case 6Case 6K+ 5.5K+ 5.5
Slide courtesy of A. Oster
Case 7Case 7
General surgery rotationGeneral surgery rotation 03:30 - you are awakened from a sound 03:30 - you are awakened from a sound
sleep by a nurse who tells you that Mr. sleep by a nurse who tells you that Mr. X’s potassium is only 3.0.X’s potassium is only 3.0.
Do you care?Do you care? Why do you care?Why do you care? What are you going to do about it?What are you going to do about it?
HypokalemiaHypokalemiaSpectrum of SymptomsSpectrum of Symptoms
AsymptomaticAsymptomatic K 3-3.5K 3-3.5
NeuromuscularNeuromuscular K usually < 2.5K usually < 2.5
lethargylethargy confusionconfusion fasciculationsfasciculations weaknessweakness decreased DTRsdecreased DTRs paralysis (K<2)paralysis (K<2)
CardiovascularCardiovascular usually no symptoms usually no symptoms
in patients without in patients without heart diseaseheart disease
palpitationspalpitations ectopyectopy dysrhythmiasdysrhythmias 1 - 2 degree HB1 - 2 degree HB atrial fibrillationatrial fibrillation ventricular fibrillationventricular fibrillation
GIGI impairs intestinal smooth muscleimpairs intestinal smooth muscle N/VN/V paralytic ileusparalytic ileus
RenalRenal polyuriapolyuria polydipsiapolydipsia
ApproachApproach
DECREASEDINTAKE
TRANSCELLULARSHIFT
INCREASEDLOSSES
GI RENAL
Slide courtesy A. Oster
HypokalemiaHypokalemia Decreased IntakeDecreased Intake
decreased dietary decreased dietary intakeintake
decreased absorptiondecreased absorption
Transcellular ShiftsTranscellular Shifts alkalosisalkalosis insulininsulin B2 agonistsB2 agonists
eg: ventolin - lowers K ~ eg: ventolin - lowers K ~ 0.4 mmol/L x 4 hours0.4 mmol/L x 4 hours
coffeecoffee
Increased LossIncreased Loss renalrenal
hyperaldosteronismhyperaldosteronism renal tubular defectsrenal tubular defects mineralocorticoidsmineralocorticoids glucocorticoids (alter glucocorticoids (alter
GFR)GFR) +++diuretics+++diuretics drugsdrugs
GIGI N/V/DN/V/D
SkinSkin burnsburns perspirationperspiration

His ECG...His ECG...
Slide courtesy A. Oster
HypokalemiaHypokalemia
ECG findingsECG findings small or absent T small or absent T
waveswaves prominent U wavesprominent U waves ST segment ST segment
depressiondepression
Slide courtesy A. Oster
How will you treat him?How will you treat him?
Potassium is an intracellular ionPotassium is an intracellular ion 1 mEq/L decrease in serum K may equal 1 mEq/L decrease in serum K may equal
up to 370 mEq total body deficitup to 370 mEq total body deficit
~50% of administered K excreted in ~50% of administered K excreted in urine - therefore several days to correct urine - therefore several days to correct deficitdeficit
OralOral K-Dur (20mmol/tab)K-Dur (20mmol/tab) KCl KCl
elixir(20mmol/15mlelixir(20mmol/15ml))
K-Phos(4.4mmol/K-Phos(4.4mmol/ml)ml)
useful if useful if hypophosphatemichypophosphatemic
K-Citrate K-Citrate (0.9mmol/ml)(0.9mmol/ml)
useful in RTAuseful in RTA
IVIV KCl KCl
(10/20/40mmol/100cc(10/20/40mmol/100cc))
10-20mEq/h10-20mEq/h >20mEq/h requires >20mEq/h requires
central line and central line and cardiac monitorcardiac monitor
S/E’sS/E’s transient transient
hyperkalemiahyperkalemia burning at IV siteburning at IV site
HypomagnesemiaHypomagnesemia
Magnesium required in Na-K ATP-Magnesium required in Na-K ATP-asease hypomag often co-exists with hypomag often co-exists with
hypokalemiahypokalemia Mg must be corrected along with KMg must be corrected along with K
Cofactor in PTH metabolismCofactor in PTH metabolism often coexists with low Caoften coexists with low Ca
HypomagnesemiaHypomagnesemia
Diuretic useDiuretic use thiazide and loop thiazide and loop
diureticsdiuretics decrease Mg ~25-50%decrease Mg ~25-50%
EtOH abuseEtOH abuse 30-80%30-80%
Renal lossesRenal losses GI lossesGI losses
V/DV/D short bowelshort bowel pancreatitispancreatitis
Endocrine disordersEndocrine disorders DMDM hyperaldosteronismhyperaldosteronism hyperthyroidismhyperthyroidism
PregnancyPregnancy DrugsDrugs
aminoglycosides, B-aminoglycosides, B-agonists, cyclosporine, agonists, cyclosporine, pentamidine, pentamidine, theophyllinetheophylline
Congenital disordersCongenital disorders
HypomagnesemiaHypomagnesemiaclinical featuresclinical features
Non-specificNon-specific
NeuromuscularNeuromuscular weaknessweakness tremortremor hyperreflexiahyperreflexia Chvostek/Chvostek/
TrousseauTrousseau seizuresseizures comacoma
CardiacCardiac supraventricular supraventricular
dysrhythmiasdysrhythmias ventricular ventricular
dysrhythmiasdysrhythmias
ECGECG non-specificnon-specific
long PR/QRS/QTlong PR/QRS/QT ST-T abnormalitiesST-T abnormalities flattened Tflattened T UwaveUwave
HypomagnesemiaHypomagnesemiaManagementManagement
Treat if Treat if Magnesium < 1.2 Magnesium < 1.2
mg/dlmg/dl or, symptomaticor, symptomatic
IVIV Magnesium sulfateMagnesium sulfate
1g = 8.3mEq 1g = 8.3mEq magnesiummagnesium
OralOral Magnesium Magnesium
RougierRougier multiple othersmultiple others cause diarrheacause diarrhea
HypermagnesemiaHypermagnesemia
Very rare …. especially in ERVery rare …. especially in ER
kidneys can excrete >6g / daykidneys can excrete >6g / day
generallygenerally iatrogeniciatrogenic renally insufficientrenally insufficient
HypermagnesemiaHypermagnesemiaClinical FeaturesClinical Features
>3 mg/dl>3 mg/dl N/VN/V weaknessweakness
>4mg/dl>4mg/dl hyporeflexiahyporeflexia loss of DTR’sloss of DTR’s
>5-6mg/dl>5-6mg/dl hypotensionhypotension ECG changesECG changes
QRS widenineQRS widenine QT/PR prolongationQT/PR prolongation conduction conduction
abnormalitiesabnormalities
>9mg/dl>9mg/dl repiratory depressionrepiratory depression comacoma complete heart blockcomplete heart block
HypermagnesemiaHypermagnesemiaTreatmentTreatment
Mild symptoms & Mild symptoms & normal renal normal renal functionfunction ObserveObserve
Moderate Moderate symptomssymptoms IV normal saline & IV normal saline &
furosemidefurosemide watch Kwatch K
Severe symptomsSevere symptoms IV CalciumIV Calcium
antagonizes antagonizes membrane effects of membrane effects of MgMg
reverses respiratory reverses respiratory depression/dysrhytmdepression/dysrhytmias, etcias, etc
DialysisDialysis refractory symptomsrefractory symptoms renal failurerenal failure
Case 8Case 8
55 woman with metastatic breast cancer55 woman with metastatic breast cancer Increasing weakness and confusion x 24 hoursIncreasing weakness and confusion x 24 hours Ataxic this morningAtaxic this morning HeadacheHeadache ThirstyThirsty
VitalsVitals 110 18 100/80 92% 37.0110 18 100/80 92% 37.0
O/E O/E alert but disoriented and confused, GCS 15 alert but disoriented and confused, GCS 15 otherwise unremarkableotherwise unremarkable
Case 8Case 8
LabsLabs CBC CBC
normalnormal electrolyteselectrolytes
normalnormal Calcium 4.5Calcium 4.5 Albumin 30Albumin 30
How do you How do you correct [Ca] for correct [Ca] for albumin?albumin? Add 0.2 for every Add 0.2 for every
10 units albumin is 10 units albumin is below 40below 40
ie: 47ie: 47
Case 8Case 8ECGECG
Characteristic changesCharacteristic changes Short QTShort QT prolongation or PRprolongation or PR QRS wideningQRS widening
Occasionally seeOccasionally see sinus bradycardiasinus bradycardia BBBBBB AV blockAV block cardiac arrestcardiac arrest
Calcium MetabolismCalcium Metabolism 1200g Ca in body1200g Ca in body
99% in bone99% in bone 1% in serum1% in serum
60% protein bound60% protein bound 40% free40% free
parathyroid hormoneparathyroid hormone bone resorptionbone resorption renal Ca reabsorptionrenal Ca reabsorption renal conversion renal conversion
vitamin D to 1,25DHCC)vitamin D to 1,25DHCC) renal phosphate renal phosphate
excretionexcretion
calcitonincalcitonin decreases osteoclastic decreases osteoclastic
activity and enhances activity and enhances skeletal depositionskeletal deposition
HypercalcemiaHypercalcemiaEtiologyEtiology
Most (~90%)Most (~90%) Primary Primary
hyperparathyroidishyperparathyroidismm
MalignanciesMalignancies
OthersOthers medicationsmedications
thiazidesthiazides LiLi Vitamin D toxicityVitamin D toxicity Ca ingestionCa ingestion
granulomatous granulomatous diseasedisease
other endocrine other endocrine disordersdisorders
HypercalcemiaHypercalcemiaClinical FeaturesClinical Features
NeurologicNeurologic fatigue, weaknessfatigue, weakness confusion, lethargyconfusion, lethargy ataxiaataxia comacoma hypotoniahypotonia
CVCV hypertensionhypertension sinus bradycardiasinus bradycardia AV blockAV block ECG abnormalities (short ECG abnormalities (short
QT, BBB)QT, BBB)
RenalRenal polyuria, polydipsiapolyuria, polydipsia pre-renal azotemiapre-renal azotemia nephrolithiasisnephrolithiasis nephrocalcinosisnephrocalcinosis
GIGI N/VN/V pancreatitispancreatitis constipationconstipation ileusileus
HypercalcemiaHypercalcemiaTreatment PrinciplesTreatment Principles
restore intravascular restore intravascular volumevolume Serum calcium will Serum calcium will
decrease with decrease with hydrationhydration
increase renal increase renal calcium eliminationcalcium elimination hydrationhydration fursosemide 40-80mg fursosemide 40-80mg
iv q6-8hiv q6-8h AVOID thiazidesAVOID thiazides
reduction of reduction of osteoclastic activityosteoclastic activity Etidronate/PamidronateEtidronate/Pamidronate PlicamycinPlicamycin calcitonin 4U/kg sc calcitonin 4U/kg sc
q12hq12h
treatment of primary treatment of primary disorderdisorder parathyroidectomyparathyroidectomy treat malignancytreat malignancy withdrawal of medswithdrawal of meds
Case 9Case 9
52 year old woman52 year old woman HTNHTN
B-Blocker, thiazideB-Blocker, thiazide diarrhea x 1 weekdiarrhea x 1 week tingling around mouth and in fingerstingling around mouth and in fingers cramps in arms and legscramps in arms and legs
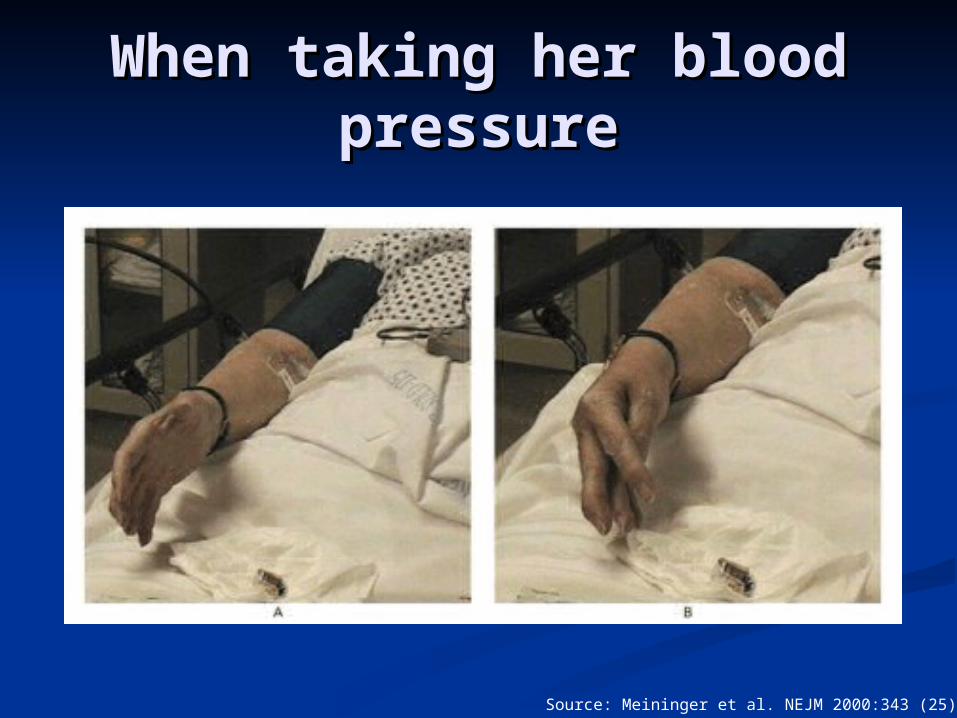
When taking her blood When taking her blood pressurepressure
Source: Meininger et al. NEJM 2000:343 (25): 1855
Case 9Case 9ECGECG
HypocalcemiaHypocalcemiaEtiologyEtiology
PTHPTH PTH insufficiencyPTH insufficiency
primaryprimary secondarysecondary
neck surgeryneck surgery Mg disordersMg disorders pancreatitispancreatitis drugsdrugs
PTHPTH Vitamin D insufficiencyVitamin D insufficiency
malnutritionmalnutrition malabsorptionmalabsorption hepatic/renal diseasehepatic/renal disease
Calcium chelationCalcium chelation hyperphosphatemiahyperphosphatemia citratecitrate alkalosisalkalosis fluoride poisoningfluoride poisoning
HypocalcemiaHypocalcemiaClinical FeaturesClinical Features
NeuromuscularNeuromuscular confusion/anxietyconfusion/anxiety paresthesiasparesthesias weaknessweakness spasmsspasms tetanytetany
Chvostek/TrousseauChvostek/Trousseau hyperreflexiahyperreflexia seizuresseizures
CVCV bradycardiabradycardia decreased decreased
contractilitycontractility hypotensionhypotension CHFCHF
ECGECG QT prolongationQT prolongation
HypocalcemiaHypocalcemia
ManagementManagement IV calcium chlorideIV calcium chloride
10ml amps of 10%10ml amps of 10% 360mg elemental 360mg elemental
CaCa
IV calcium IV calcium gluconategluconate
10ml amps of 10%10ml amps of 10% 93mg elemental 93mg elemental
CaCa
recommended initial recommended initial adult dose is 100-adult dose is 100-300mg300mg pediatric dose is 0.5-pediatric dose is 0.5-
1.0mg/kg of Ca gluconate1.0mg/kg of Ca gluconate lasts 2hourslasts 2hours consider an infusionconsider an infusion
S/E’sS/E’s HTNHTN N/VN/V bradycardia/HBbradycardia/HB tissue necrosis if interstitialtissue necrosis if interstitial
the endthe end