Embed Size (px)
Citation preview

Neurophysiology lecture topics
1. Role of brainstem and reticular formation 2. Ascending and descending tracts
muscle power 3. Maintenance of posture, equilibrium,
coordinationmuscle tone
4. Functions of limbic system and basal ganglia

Brains stem
• Midbrain• Pons• Medulla

Role of brainstem
• Intermediate centre in controlling motor functions • Ascending and descending pathways cross brain stem • Contains vital centres• Contains reticular formation • Plays a vital role in attention, arousal and states of
consciousness • Brainstem injuries easily cause loss of consciousness• Most of the cranial nerves are connected to brainstem• Contain pain pathways • Involved in suprasegmental control of reflexes and muscle tone• Extrapyramodal tracts strats from the brain stme

Reticular formation
• Located in the core of the brainstem
• Network of neurons• Main centre of ascending
and descending tracts• Functions:
consciousness, motor control, pain modulation, cardiovascular control, sleep centres

Ascending pathways
• Somatosensory pathways– Dorsal column – medial lemniscus pathway
– Spinothalamic tracts• Anterior spinothalamic tract• Lateral spinothalamic tract
– Spinocerebellar tracts• Dorsal• Ventral

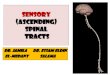
Receptor
Sensory modality
Sensory nerve
Central Connections
Ascending Sensory pathway
Sensory area in the brain
Touch stimulus

Two main ascending pathways
• Dorsal column - medial lemniscus pathway
fast pathway
• Spinothalamic pathwayslow pathway
These two pathways come together at the level of thalamus

Dorsal column pathwaySpinothalamic pathway
Lateral Spinothalamic tract
AnteriorSpinothalamic tract

Dorsal column pathway Spinothalamic pathway
• touch: fine degree• highly localised touch sensations• vibratory sensations• sensations signalling movement• position sense• pressure: fine degree
• Pain• Thermal sensations• Crude touch & pressure• crude localising sensations• tickle & itch• sexual sensations

Dorsal column nuclei(cuneate & gracile nucleus)
Dorsal column
Medial lemniscus
thalamus
thalamocortical tracts
sensory cortex
internal capsule
1st order neuron
2nd order neuron
3rd order neuron

Spinothalamic tracts
thalamus
thalamocortical tracts
sensory cortex
internal capsule
1st order neuron
2nd order neuron
3rd order neuron


Proprioceptive pathways
• Dorsal column – medial lemniscus – thalamocortical pathway (conscious proprioception)
• Spinocerebellar pathway (unconscious proprioception)

Main descending pathways
• Motor pathways
• Corticospinal and corticobulbar tracts
• Starts from the motor cortex

Motor cortex
• Located in the frontal lobe• Precentral gyrus


Motor homunculus
First discoveredbyPenfield

Corticospinal tract (Pyramidal tract)
• Starts from large cortical cells (pyramidal cells) in the primary motor cortex
• These cells are called Betz cells • From these cells starts the motor axon• Divided into
– Lateral corticospinal tract• Major part of the CST, cross to the opposite side
at the level of medulla
– Medial corticospinal tract (or anterior CST) • Minor part, uncrossed tract, at the level of spinal
cord cross to the opposite side

Course of the corticospinal tract
• Descends through– internal capsule– at the medulla
• cross over to the other side
– descends down as the corticospinal tract– ends in each anterior horn cell– synapse at the anterior horn cell

Medulla
motor cortex
internal capsule
Uppermotorneuron
Lowermotorneuron
anterior horn cell

Motor system
• Consists of – Upper motor neuron
• Corticospinal tract (pyramidal tract)• Extrapyramidal tracts
– Lower motor neuron• Alpha motor neuron • Gamma motor neuron

Lower motor neuron
• consists of mainly • alpha motor neuron
– and also gamma motor neuron
alpha motor neuron
gamma motor neuron

alpha motor neuron
gamma motor neuron
corticospinal tract
Arrangement at the anterior horn cell

alpha motor neuron
• this is also called the final common pathway
• Contraction of the muscle occurs through this whether – voluntary contraction through corticospinal tract
or– involuntary contraction through gamma motor
neuron - stretch reflex - Ia afferent

Upper motor neuron
• Consists of – Corticospinal tract (pyramidal tract) – Extrapyramidal tracts

Extrapyramidal tracts
• starts at the brain stem• descends down either ipsilaterally or
contralaterally• ends at the anterior horn cell• modifies the motor functions

Reticulospinal tract
• Starts from the reticular formation
• Maintain normal postural tone
• Controls mainly gamma motorneurons (lesser extent alpha motor neurons)
• Inhibit antigravity muscles (extensor)
• End on interneurons
• Inhibited by cerebral influence
• Mainly ipsilateral

Reticular formation
• Loosely arranged cell bodies in the central core of the brain stem
• Pontine reticular area
• Medullary reticular area
midbrain
pons
medulla
spinal cord

Vestibulospinal tract
• Starts from the vestibular nuclei (present in the medullar region)
• Excitatory to alpha motor neurons of antigravity muscles (extensor)
• End on interneurons
• Regulates posture and balance
• Mainly ipsilateral
• There are inputs from vestibular organs and cerebellum to vestibular nuclei

• Rubrospinal and tectospinal tracts are not functionally important in human nervous system

Uppermotorneuron
Lowermotorneuron
extrapyramidal tracts
pyramidal tracts
alpha motor neurone
gamma motor neurone

Suprasegmental control of reflexes and muscle tone
• Alpha motor neuron is the final pathway• Gamma motor neuron control
• Alpha-gamma coactivation
• Supraspinal control– Pyramidal tract: activation of alpha– Extrapyramidal: mixed effects on alpha and gamma
motor neurons• Net effect: suppression of gamma motor neuron

• There is a complex effect of corticospinal and extrapyramidal tracts on the alpha and gamma motor neurons (in addition to the effect by muscle spindle)
• There are both excitatory and inhibitory effects• Sum effect
– excitatory on alpha motor neuron– Inhibitory on gamma motor neuron
Corticospinal tract
Extrapyramidal tracts
Alpha motor neuron
Gamma motor neuron• Voluntary movement
• Muscle tone
Muscle spindle

Clinical Importance of the motor system examination
• Tests of motor function:– Muscle power
• Ability to contract a group of muscles in order to make an active movement
– Muscle tone• Resistance against passive movement

Basis of tests
• Muscle power– Test the integrity of motor cortex, corticospinal tract
and lower motor neuron
• Muscle tone – Test the integrity of stretch reflex, gamma motor
neuron and the descending control of the stretch reflex

Muscle tone
• Resistance against passive movement
– Gamma motor neuron activate the spindles – Stretching the muscle will activate the stretch reflex – Muscle will contract involuntarily
– Gamma activity is under higher centre inhibition

Clinical situations
• Muscle power– Normal– Reduced (muscle weakness)
• muscle paralysis• muscle paresis
• Muscle tone – Normal– Reduced
• Hypotonia (Flaccidity)– Increased
• Hypertonia (Spasticity)

Main abnormalities
• Muscle Weakness / paralysis– Reduced muscle power
• Flaccidity– Reduced muscle tone
• Spasticity– Increased muscle tone

• Lower motor neuron lesion causes– flaccid paralysis (flaccid weakness)
• Upper motor neuron lesion causes– spastic paralysis (spastic weakness)

Lower motor neuron lesion
• muscle weakness• flaccid paralysis• muscle wasting (disuse atrophy)• reduced muscle tone (hypotonia)• reflexes: reduced or absent• spontaneous muscle contractions
(fasciculations)• plantar reflex: flexor• superficial abdominal reflexes: present

Muscle wasting

Fasciculations

Upper motor neuron lesion
• muscle weakness• spastic paralysis• increased muscle tone (hypertonia)• reflexes: exaggerated• Babinski sign: positive• superficial abdominal reflexes: absent• muscle wasting is very rare• clonus can be seen:
– rhythmical series of contractions in response to sudden stretch
• clasp knife effect can be seen– passive stretch causing initial increased resistance which is
released later

Clasp knife effect
Clonus

Stroke patient walking

Babinski sign• when outer border of the sole of the foot is
scratched• upward movement of big toe • fanning out of other toes
• feature of upper motor neuron lesion• extensor plantar reflex• seen in infants during 1st year of life (because
of immature corticospinal tract)

positive Babinski sign

Site of lesions
Cortex
Internal capsule
Brain stem
Spinal cord
Anterior horn cell
Motor nerve
Neuromuscular junctionMuscle

Site of lesions
monoplegiaonly 1 limb is affected either UL or LL,lower motor neuron lesion
hemiplegiaone half of the body includingUL and LLlesion in the Internal capsule
paraplegiaboth lower limbsthoracic cord lesion
quadriplegia (tetraplegia)all 4 limbs are affected
cervical cord or brain stem lesion

Conditions which cause increased muscle tone
• Spasticity – Stroke
• Rigidity– Parkinsonism
• Lead pipe rigidity• Cogwheel rigidity
• Brainstem lesions – Decerebrate rigidity – Decorticate rigidity

Reticular formation
• A set of network of interconnected neurons located in the central core of the brainstem
• It is made up of ascend ing and descend ing fibers
• It plays a big role in fil ter ing incom ing stim uli to dis crim i nate irrel e vant back ground stim uli
• There are a large number of neurons with great degree of convergence and divergence

Functions
• Maintain consciousness, sleep and arousal
• Reticulospinal pathways are part of the extrapyramidal tracts
• Several nuclei (PAG, NRM) are part of the descending pain modulatory (inhibitory) pathway

Basal ganglia• These are a set of deep nuclei
located in and around the basal part of the brain that are involved in motor control, action selection, and some forms of learning
• Purposeful movement

Basal ganglia• Caudate nucleus • Putamen• Globus pallidus
–(internal and external)• Subthalamic nuclei• Substantia nigra
International Basal Ganglia Society

(Ref. Guyton)


basal ganglia• caudate nucleus• putamen• globus pallidus• subthalamic nuclei• substantia nigra
corpus striatum
lentiformnucleus

• Interconnecting circuitry through these nuclei• These circuits start from the cortex and ends in
the cortex• These circuits are very complex• Their effect is excitatory or inhibitory on motor
functions• They also have a role in cognitive functions.

Cortex
Putamen
globuspallidus
Thalamus

Functions
• eg. – writing letters of alphabet, – cutting papers with scissors, – hammering nails, – passing a football, – Vocalisation– Cognitive control of movement

• Some of these circuits are excitatory and some inhibitory
• This depends on the neurotransmitter involved.
• Inhibitory: dopamine and GABA• Excitatory: Ach• Others: glutamate (from cortical
projections) enkephalin etc

Following pathways are known:
• Dopamine pathway from substantia nigra to caudate nucleus and putamen
• GABA pathway from caudate and putamen to globus pallidus and substantia nigra
• Ach pathway in the caudate and putamen

Cortex
Putamen
globuspallidus
Thalamus
Caudate
Substantia nigra
Subthalamic nucleus
Reticular formation
Dopamine
Thalamus Reticular formation
glutamate
GABA
Interneurons: Ach
stri
atum
GABA
+
+

Functions of Basal Ganglia
• Motor control • Learning• Sensorimotor integration • Reward • Cognition

Basal Ganglia disorders
• Basal ganglia disorders are also called extrapyramidal disorders
• Classical disorder is “Parkinsonism”
• Other disorders: Athetosis, Chorea, Hemiballismus

Parkinsonism• due to destruction of dopamine secreting pathways from
substantia nigra to caudate and putamen.– also called “paralysis agitans” or “shaking palsy” – first described by Dr. James Parkinson in 1817.
• In the west, it affects 1% of individuals after 60 yrs
Classical Clinical features:• Tremor, resting • Rigidity of all the muscles• Akinesia (bradykinesia): very slow movements• Postural instability

– expressionless face– flexed posture– soft, rapid, indistinct speech– slow to start walking– rapid, small steps, tendency to run– reduced arm swinging– impaired balance on turning– resting tremor (3-5 Hz) (pill-rolling tremor)
• diminishes on action
– cogwheel rigidity– lead pipe rigidity– impaired fine movements– impaired repetitive movements


Physiology of Posture
Prof. Vajira Weerasinghe
Dept of Physiology


Dynamic vs static nature of motor control
• Static stability – is dependent on the position of the centre of gravity
with respect to the base of support• whereas dynamic stability
– is dependent more on the moment of inertia of the body

Adult vs child
• In normal standing, a tall adult will have a much larger moment of inertia than a toddler
• Once the centre of gravity moves outside the base of support the body will begin to fall– The adult with the large moment of inertia
will fall much more slowly and will therefore have a longer time to react to prevent the fall
– This is one of the reasons that young children fall more often than adults.

Postural control
• Maintaining static nature of the body

maintenance of posture• mainly to maintain the static
posture• necessary for the stability of
movements• involve a set of reflexes• integrated at spinal cord, brain
stem and cortical level

normal postural control
• three inputs are required– Vision– Proprioception (joint position sense)– Vestibular Mechanism (balance mechanisms)– Cutaneous sensations


Postural reflexes• Spinal cord reflexes
– stretch reflex– positive supporting reaction (magnet reaction)– negative supporting reaction– mass reflex
• Brainstem refelxes – tonic labyrinthine reflex (vestibular)– tonic neck reflexes– labyrinthine righting reflex– neck righting reflex– body-on-head righting reflex– body-on-body righting reflex
• Cortical reflexes – optical righting reflex– placing reactions– hopping reaction

• these reflexes are under higher centre inhibition• transection of spinal cord or brain stem at
different levels release this inhibition • then the relevant reflexes are seen

postural adjustments
vestibular nucleicerebellum
pressure& otherreceptors
neckreceptors
Retina Occulomotor system vestibularsystem
complex pathways

cerebellum
• centre of motor coordination
• cerebellar disorders cause –incoordination or ataxia





structure
• Cerebellum is divided into 3 lobes by 2 transverse fissures– anterior lobe– posterior lobe– flocculonodular lobe


structure
– anterior lobe (paleocerebellum)– large posterior lobe (neocerebellum)– flocculonodular lobe (archicerebellum is the
oldest lobe)

• Anterior cerebellum and part of posterior
cerebellum – receives information from the spinal cord
• Rest of the posterior cerebellum – receives information from the cortex
• Flocculonodular lobe – involved in controlling the balance through
vestibular apparatus

• Functionally cerebellum is divided into 3 areas medial to lateral– lateral zone– intermediate zone– vermis


Cerebellum
Inputs• Corticopontocerebellar (cortical input)• Olivocerebellar• Vestibulocerebellar (balance, muscle tone, posture)• Reticulocerebellar (muscle tone, posture)• Spinocerebellar
• (proprioception)
OutputsThrough deep cerebellar nuclei
Brain stem (extrapyramidal pathways)Thalamus -> CortexBasal ganglia

Neuronal circuitry of the cerebellum
• Main cortical cells in cerebellum are known as Purkinje Cells (large cells).
• There are about 30 million such cells. • These cells constitute a unit which repeats
along the cerebellar cortex.




Functions of cerebellum
• planning of movements• timing & sequencing of movements• particularly during rapid movments such as
during walking, running• from the peripheral feedback & motor cortical
impulses, cerebellum calculates when does a movement should begin and stop

Motor Cortex
ThalamusCerebellum
Muscles
brain stem nuclei
proprioceptivetactilefeedback

‘Error correction’• cerebellum receives two types of information
– intended plan of movement• direct information from the motor cortex
– what actual movements result• feedback from periphery
– these two are compared: an error is calculated
– corrective output signals goes to• motor cortex via thalamus• brain stem nuclei and then down to the anterior horn cell
through extrapyramidal tracts

• ‘Prevention of overshoot’– Soon after a movement has been initiated– cerebellum send signals to stop the movement at
the intended point (otherwise overshooting occurs)
• Ballistic movements– rapid movements of the body, eg. finger movements
during typing, rapid eye movements (saccadic eye movements)
– movements are so rapid it is difficult to decide on feedback
– therefore the movement is preplanned• Cerebellum perform motor learning (memory)

planning of movements
• mainly performed by lateral zones• sequencing & timing
– lateral zones communicate with premotor areas, sensory cortex & basal ganglia to receive the plan
– next sequential movement is planned– predicting the timings of each movement

features of cerebellar disorders
• ataxia – incoordination of movements– ataxic gait
• broad based gait• leaning towards side of the lesion
• dysmetria– cannot plan movements
• past pointing & overshoot• decomposition of movements• intentional tremor

features of cerebellar disorders
• Dysdiadochokinesis (adiadochokinesis) – unable to perform rapidly alternating movements
• dysarthria– slurring of speech
• nystagmus– oscillatory movements of the eye

features of cerebellar disorders
• hypotonia– reduction in tone
• due to reduction in excitatory influence on gamma motor neurons by cerebellum (through vestibulospinal tracts)
• decreased reflexes• head tremor• head tilt
• In unilateral cerebellar lesions, incoordination occurs in the ipsilateral side

• But what finally drives us to action???
• perhaps motivation
• motivation is controlled by limbic system and hypothalamus

Limbic system

limbic system• nuclei
– amygdala– septal nuclei– mammillary body– hypothalamus
• cortical areas– hippocampal gyrus– cingulate gyrus– dentate gyrus– entorhinal, amygdaloid cortex
• paralimbic structures• orbital gyrus, insula, nucelus accumbens, thalamic
nuclei, superior temporal gyrus,
• fibre tracts: fornix, medial forebrain bundle

limbic cortex
• consist of 3 layered cortex (in contrast to 6 layered cortex of the neocortex)

• Limbic system is a link between the brain stem and neocortex
• Limbic structures are connected to each other and with the association cortex and the brain stem

• Medial forebrain bundle is a major efferent connection of the limbic system:
• projected to the hypothalamus, reticular formation. Influence on autonomic and endocrine activity
• Amygdala receives inputs from olfactory pathways
• Connections with the neocortex provide a synthesis of emotional and rational thought

FunctionsLimbic system is also referred to as the
‘emotional brain’
• Emotional (include motor activity)• Behavioural (Motivations, Drives: appetite,
thirst, sexual behaviour, Reward system)• Memory
– Utilizes the hypothalamus to effect the physical manifestations associated with emotions, etc.

Complex role of the limbic system
• as an intermediary between– external events (carried to the CNS via afferents)– our processing of those events (involving cortical
and subcortical brain areas) – our responses to those events (both behavioral and
autonomic)

Role in memory storage
• Working memory—short term – cortical phenomenon
• Explicit (declarative)—factual knowledge– temporal events, stored in hippocampus
• Examples: what innervates biceps femoris m.?
• Implicit (procedural)—learned skills– unconsciously recalled—includes emotional
responses—stored in amygdala (at least in part)• Examples: writing, playing a musical instrument

Hippocampus• is a part of the brain located
inside the temporal lobe• plays a major role memory
consolidation • responsible for spatial memory• might act as a cognitive map —
a neural representation of the layout of the environment.
• In Alzheimer's disease, the hippocampus becomes one of the first regions of the brain to suffer damage















![Ascending pathways 2019 (00000002) [Read-Only]](https://img.pdfslide.us/doc/110x75/617f315aaef80749fc415a93/ascending-pathways-2019-00000002-read-only.jpg)