Embed Size (px)
Citation preview

CVJFM 360deg 25-9-2016 1254am Cranio- vertebral junction Foramen magnum
Great teachers ndash All this is their work I am just the reader of their books
Prof Paolo castelnuovo
Prof Aldo Stamm Prof Mario Sanna
Prof Magnan
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading
From Anteriorly
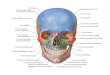
1 The HC divides the condylar region into the tubercular compartment (superior) and the condylar compartment (inferior)
Tubercular compartment contains LPT lateral pharyngeal tubercle PT pharyngeal tubercle
2 The SCG [Supracondylar groove] represents a reliable landmark for hypoglossal canal (HC) identification (red arrow) (Morera et al 2010 )
The tubercular compartment corresponds to the Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull
base you will land up on JT
LPT lateral pharyngeal tubercle OC occipital condyle PT pharyngeal tubercle SCG supracondylar groove
Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
Red rings = hypoglossal canals yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT]
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT] green ring = Jugular tubercle
Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Great teachers ndash All this is their work I am just the reader of their books
Prof Paolo castelnuovo
Prof Aldo Stamm Prof Mario Sanna
Prof Magnan
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading
From Anteriorly
1 The HC divides the condylar region into the tubercular compartment (superior) and the condylar compartment (inferior)
Tubercular compartment contains LPT lateral pharyngeal tubercle PT pharyngeal tubercle
2 The SCG [Supracondylar groove] represents a reliable landmark for hypoglossal canal (HC) identification (red arrow) (Morera et al 2010 )
The tubercular compartment corresponds to the Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull
base you will land up on JT
LPT lateral pharyngeal tubercle OC occipital condyle PT pharyngeal tubercle SCG supracondylar groove
Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
Red rings = hypoglossal canals yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT]
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT] green ring = Jugular tubercle
Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading
From Anteriorly
1 The HC divides the condylar region into the tubercular compartment (superior) and the condylar compartment (inferior)
Tubercular compartment contains LPT lateral pharyngeal tubercle PT pharyngeal tubercle
2 The SCG [Supracondylar groove] represents a reliable landmark for hypoglossal canal (HC) identification (red arrow) (Morera et al 2010 )
The tubercular compartment corresponds to the Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull
base you will land up on JT
LPT lateral pharyngeal tubercle OC occipital condyle PT pharyngeal tubercle SCG supracondylar groove
Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
Red rings = hypoglossal canals yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT]
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT] green ring = Jugular tubercle
Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

From Anteriorly
1 The HC divides the condylar region into the tubercular compartment (superior) and the condylar compartment (inferior)
Tubercular compartment contains LPT lateral pharyngeal tubercle PT pharyngeal tubercle
2 The SCG [Supracondylar groove] represents a reliable landmark for hypoglossal canal (HC) identification (red arrow) (Morera et al 2010 )
The tubercular compartment corresponds to the Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull
base you will land up on JT
LPT lateral pharyngeal tubercle OC occipital condyle PT pharyngeal tubercle SCG supracondylar groove
Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
Red rings = hypoglossal canals yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT]
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT] green ring = Jugular tubercle
Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

1 The HC divides the condylar region into the tubercular compartment (superior) and the condylar compartment (inferior)
Tubercular compartment contains LPT lateral pharyngeal tubercle PT pharyngeal tubercle
2 The SCG [Supracondylar groove] represents a reliable landmark for hypoglossal canal (HC) identification (red arrow) (Morera et al 2010 )
The tubercular compartment corresponds to the Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull
base you will land up on JT
LPT lateral pharyngeal tubercle OC occipital condyle PT pharyngeal tubercle SCG supracondylar groove
Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
Red rings = hypoglossal canals yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT]
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT] green ring = Jugular tubercle
Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The tubercular compartment corresponds to the Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull
base you will land up on JT
LPT lateral pharyngeal tubercle OC occipital condyle PT pharyngeal tubercle SCG supracondylar groove
Jugular tubercle ( JT )
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
Red rings = hypoglossal canals yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT]
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT] green ring = Jugular tubercle
Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
Red rings = hypoglossal canals yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT]
Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT] green ring = Jugular tubercle
Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Line along the lateral pharyngeal tubercle [ LPT ] passes through Jugular tubercle [ JT ] ndash so when you are drilling LPT in anterior skull base you will land up on JT
yellow ring = pharyngeal tubercle [ PT ] blue rings = lateral pharyngeal tubercle [ LPT] green ring = Jugular tubercle
Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Just adding two triangles of petrous bone base around foramen magnum your lower clivus foramen magnum area completes -- just as simple as that
Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Lower clivus devided into 1 tubercular compartment [ Above red line ]2 condylar compartment [ Below red line ]
Hypoglossal canal present at the junction of anterior 13rd amp posterior 23rd
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Lateral skull base view ndash observe the petrous apex
Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Lower clivus + petrous apex in anterior skull base 1 observe the petrous apex in both views
2 hypoglossal canal medial to parapharyngeal carotid amp jugular fossa
Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Behind the RCLM vertebral artery present
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

kinking or looping of the ICAp - when looping present para-pharyngeal carotid comes to pre-styloid compartment ndash previously thought that para-pharyngeal
carotid never comes anterior to styloid mucles ndash which is UNTRUE
From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

From Aldostamm - Fig 4210 - When there is loop of parapharyngeal carotid it goes nearer to the RCLM or anterior arch of atlas
Anterior view The right longus capitis muscle has beenremoved 1 clivus 2 anterior arch of the atlas 3 atlantoaxial joint4 left longus capitis muscle 5 longus colli muscle 6 rectus capitis
anterior muscle 7 carotid artery
Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Hypoglossal is just behind the upper end of parapharyngel carotid ndash very easy way to
identify 12th nerve in paraphayrngeal space ndash DrSatish jain
Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Lower cranial nerves sandwitched betweeb petrosal amp bulb components of jugular fossa - the pars nervosa is anterior to pars venosa and the ica
is the first structure u will encounter in the anterior app
pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

pars nervosa is anterior to pars
venosa
httpsbooksgooglecoinbooksid=e8gKUQgeD24Camppg=PA634amplpg=PA634ampdq=pars+venosaampsource=blampots=SaW2H-2bR0ampsig=lzevzuaK66DT_Nj6PLfLH3orXQYamphl=enampsa=Xampved=0CCsQ6AEwAmoVChMIxqvJ1v2bxwIVC9SOCh1-pQ9sv=onepageampq=pars20venosaampf=false
Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Vetebral venous plexus
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

AAAM anterior atlanto-axial membrane AAOM anterior atlanto-
occipital membrane white arrow superior part of the cruciform
ligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse ligament white circles tectorial
membrane
The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The VAs pass through the transverse foramina of the first six vertebrae and exit from the transverse foramen of C1 running backward and medially over the posterior arch of C1 and pierce the posterior atlanto-
occipital membrane and the spinal dura They are surrounded extracranially by a venous plexus that does not enter the intradural space
CP sympathetic carotid plexus C1 atlas C1TP transverse process of C1 ICAp parapharyngealportion of the internal carotid artery IJV internal jugular vein LCapM longus capitis muscle Mamastoid (tip) OC occipital condyle RCAM rectus capitis anterior muscle SCG superior cervicalganglion SP styloid process VA vertebral artery VVP vertebral venous plexus ZR zygomatic
root XIIcn hypoglossal nerve yellow arrow vagus nerve red arrow accessory nerve black arrow glossopharyngeal nerve white asterisk middle meningeal artery
The extradural segment of VA gives rise to posterior meningeal and posterior spinal arteries and branches to the deep cervical muscles
Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Cadaveric dissection following the removal of the mucosa and pharyngobasilar fascia The middle third of the clivus has been removed to reveal the pons The longus capitis (LC) muscles insert broadly onto the floor
of the sphenoid sinus (removed in this specimen) The pharyngeal raphe (PR) can be seen attaching to the pharyngeal tubercle (PT) of the occipital bone ET eustachian tube BA basilar artery PCA paraclival artery
Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Note how the superior constrictor (SC) muscle finishes at the level of the soft palate Cadaveric dissection following the removal of the longus capitis muscles This step reveals the
anterior longitudinal ligaments (ALL) the anterior atlantooccipital membrane (A AOM) and the anterior rectus capitis muscle (A RC) (SP) AAA anterior arch of the atlas ET eustachian tube
PT pharyngeal tubercle
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longuscapitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint ( AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion
of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane AIManterior intertransversarius muscle AL alar ligament ALL anterior longitudinal ligament Cl
clivus C1 atlas C1TP transverse process of C1 C2 axis D dens JF jugular foramen OC occipitalcondyle PT pharyngeal tubercle RCLM rectus capitis lateralis muscle SCG supracondylar
groove SP styloid process VA vertebral artery blue-sky arrow apical ligament white arrowsuperior part of the cruciform ligament green arrow external ori fi ce of hypoglossal canal black
arrow atlantoaxial joint red arrow atlanto-occipital joint blue arrow lateral atlanto-occipitalligament yellow arrow dura of the posterior cranial fossa and upper spine white asterisk transverse
ligament white circles tectorial membrane
Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Tectorial membrane - posterior border of the supraodontoid space
The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The tectorial membrane (TM) is a thin structure acting as the posterior border of the supraodontoid space It presents an intimate relationship with the dura mater (posteriorly) and with the accessory atlanto-axial and cruciform ligaments (anteriorly) TM fi rmly adheres to the
cranial base and body of the axis but not to the posterior aspect of the dens (Tubbs et al 2011 )
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and upper
spine white asterisk transverse ligament white circles tectorial membrane
Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Posterior most limit of nose is Anterior arch of atlas ndash floor of the nose [ soft palate ] points to anterior arch of atlas The
arch of the atlas is at the most caudal region that can be reached through the transnasal approach If it is necessary to increase the caudal exposure the posterior
superior edge of the hard palate can be drilled away but care should be taken to preserve the oral mucosa under the hard palate
Cadaveric dissection following the removal of the anterior atlantooccipital membrane anterior longitudinal ligament the longus capitis muscles and the anterior rectus capitis muscles This reveals the joint capsule of the atlantooccipital joint (AOJ) This joint capsule has been removed to reveal the joint surfaces The superior constrictor muscle (SC) has been split to show the insertion of the longus coli muscle (LC) The apical ligaments (AP) and alar ligaments (AL) can be seen clearly SP soft palate ET eustachian tube AAA anterior arch of the atlas BA basilar artery
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Transoral exposure of the craniocervical junction region A Mandibular bone and the tongue were excised B The soft palatewas excised and pharyngeal mucosa was retracted bilaterally and clivus was exposed C The clivus atlas and axis were exposed transorally
D Inferior third of the clivus anterior arch of atlas and the anterior part of the axis were excised down to level of the C3 vertebralbody and the dura was also excised correspondingly to demonstrate craniocervical junction region aaa anterior arch of atlas aica
anterior inferior cerebellar artery asa anterior spinal artery at atlas ata anterior tubercle of atlas ax axis ba basilar artery C1 C-1nerve root C2 C-2 nerve root cl clivus d dens dudura hp hard palate iaf-at inferior articular facet of atlas lcap longus capitis
muscle ma mandible mo medulla oblangata mu pharyngeal mucosa pns posterior nasal spine of palatine bone pt palatine tonsilsaf-ax superior articular facet of axis sc spinal cord sp soft palate u uvula V4 intradural segment of vertebral artery vo vomer
Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Note the transverse ligament amp tectorial membrance in both photos
Cadaveric dissection following the removal of the apical and alar ligaments and the odontoid process has been drilled away (OP) This reveals the strong and thick transverse portion of the cruciform ligament (CL) Behind this is located the tectorial membrane (TM) ET eustachian tube SP soft palate HC hypoglossal canal VA vertebral artery BA basilar artery
AAAM anterior atlanto-axial membrane AAOM anterior atlanto-occipital membrane white arrow
superior part of the cruciform ligament yellow arrow dura of the posterior cranial fossa and
upper spine white asterisk transverse ligament white circles tectorial membrane
Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Dentate ligament = DL ndash see in both photos
Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Intradural structures when approached anteriorly
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
The origins of the left and right rami from the vertebral artery as seen with a 01048612 endoscopic view of a cadaveric specimen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

ASA variations The two rami of the ASA originate from a vascular arcaderunning between the two VAs
The left ramus ends on the medulla near the origin of theright one and the right ramus courses separately
ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

ASA variations
Only one ramus gives origin to the ASABoth the right and left rami have a separate course
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach - 11th nerve behind left vertebral artery at cervico-medullary junction
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Intracranial hypoglossal region Anterior endoscopic transnasal-transclival vision is compared with a posterior retrosigmoid endoscopic one
JF jugular foramen JT jugular tubercle IO inferior olive PICA posteroinferior cerebellar artery VA vertebral artery IXcn glossopharygeal nerve Xcn vagus nerve XIcnCR cervical roots of accessory nerve XIcnSR spinal roots of accessory nerve
XIIcn hypoglossal nerveCranial nerves IX and X present a close relationship with the fi rst portion of the PICA They are protected by the arachnoid
membrane (Roche et al 2008 ) The roots of cranial nerve XIcn from the spine pass through the foramen magnum posterior to the vertebral artery Within the hypoglossal canal XIIcn is surrounded by a venous plexus and dural and arachnoid sheets
Branches of the ascending pharyngeal artery coursing through the hypoglossal canal are seen in about 50 of cases (Lang 1995 ) Also branches from the posterior meningeal artery have been described (Janfaza and Nadol 2001 ) The
transcisternal vein to the area of the JF can be seen Also veins to the hypoglossal canal can be present The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

FCB amp JT amp LCNs are at same level from anterior to posterior
FCB = Fibrocartilago basalis JT = Jugular tubercle LCNs Lower cranial nerves ( = 9th 10th 11th )
ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

ASA anterior spinal artery Cadaveric dissection image shows the close up view of the upper cervical spinal cord
The image clearly shows the C1 and C2 nerve rootlets the dentate ligaments (DL) and the vertebral artery (VA) as it enters the foramen magnum ASA anterior spinal artery
anatomist photo
The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The hypoglossal nerve do not exit with VA It can have maximum 3 outlets On the contrary C1 roots exit with the VA
From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

From Laterally
1 Far lateral or Transcondylar approach 2 ITFA with Transcondylar Transtubercular approach
(ITF-A + TC + TT approach)3 Modified trans-cochlear approach type D (MTCD)
From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

From Laterally
2 ITFA with Transcondylar Transtubercular approach(ITF-A + TC + TT approach)
ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

ITFA with Transcondylar [ = TC ] Transtubercular [ = TT ] approach
Here Transcondylar is through Occipital Condyle Transtubercular is through Jugular tubercle amp
lateral pharyngeal tubercle
Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Transcondylar transtubercular extension improves posteroinferolateral and medial exposure
Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Comparison of classic ITFA (zone delimited by the red line) and ITFA with transcondylarndashtranstubercular extension (zone delimited by the blue line) jugular
process of the occipital condyle CF carotid foramen DR digastric ridge JF jugular foramen MT mastoid tip Note hypoglossal nerve at anterior 13rd amp middle 13rd
junction
Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Extreme lateral extension [ Far-lateral ndash Transcondylar ] approach
AFL anterior foramen lacerum C1 atlas CO cochlea ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery
OC occipital condyle pc clinoid process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus V2 maxillary branch of the trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VA vertebral artery VII facial nerve IX glossopharyngeal nerve XI spinal accessory nerve XII
hypoglossal nerve
Far-lateral approach further extends posteroinferolateral exposure
Schematic illustration of the extreme lateral approach (ELA)
Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Inferior view of skull base comparison of classic ITFA of Fisch and modified ITFA with transcondylarndashtranstubercular extension In addition to removal of bone in classic ITFA of Fisch drilling of the jugular
process of the occipital bone and even some of the occipital condyle facilitates control of the area of the jugular bulb Yellow dashed line classic ITFA of Fisch Blue dashed line modified ITFA with transcondylarndash
transtubercular extension CF carotid foramen DR digastric ridge FL foramen lacerum FO foramen ovale JF jugular foramen JP jugular process of the occipital bone MT mastoid tip OC occipital condyle Arrow
stylomastoid foramen
At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

At higher magnified view note the amount of the bone removed in ITFA with transcondylar transtubercular approach CF carotid foramen FM foramen magnum HC hypoglossal canal JF jugular foramen MT
mastoid tip OC occipital condyle SMF stylomastoid foramen
JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

JT jugular tubercle
The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The jugular process and the portion of the occipital condyle have been drilled out The left occipital condyle is identified below the jugular bulb and posterior to the internal jugular vein occipital condyle ICA internal carotid artery IJV internal jugular vein JB jugular bulb
LSC lateral semicircular canal P promontory SS sigmoid sinus
Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Lower clivus + petrous bone [ base ]
Petrous bone devided into three 13rds
Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Lower clivus + petrous bone [ base ] + Zygomatic bone
Petrous bone devided into three 13rds
11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

11th nerve bisects the upper end of IJC whereas vertical part of 7th nerve bisects the jugular bulb The lateral aspect of the jugular bulb sigmoid sinus and internal jugular vein has been removed On the
medial wall of the jugular bulb the inferior petrosal sinus is identified The opening of the posterior condylar vein is seen occipital condyle ICA internal carotid artery JB jugular bulb P promontory
SS sigmoid sinus
occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

occipital condyle IJV internal jugular vein IPS inferior petrosal sinus JB jugular vein PCV posterior condylar vein SS sigmoid sinus
The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The glossopharyngeal nerve has its own dural porus which is situated 0-3 mm upwards from the dural porus of the tenth cranial nerve The vagus and the accessory nerve exit the posterior fossa together in a sleeve of dura through the jugular foramen
The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The glossopharyngeal and vagus nerves are well identified in the cerebellomedullary cistern before
entering the jugular foramen
FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

FN facial nerve ICA internal carotid artery IJV internal jugular vein JB jugular bulb Isc lateral semicircular canal OA occipital artery psc posterior semicircular canal ssc superior
semicircular canal TPC transverse process of the atlas (C1) IX glossopharyngeal nerve XI spinal accessory nerve
11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

11th nerve hitches over the transverse process of atlas -----Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral
artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve
XI spinal accessory nerve
Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Note the relationship among the sigmoid sinus jugular bulb posterior condylar vein vertebral artery and lower cranial nerves C1 atlas C2N C2 nerve JB jugular bulb
PCV posterior condylar vein SS sigmoid sinus TP transverse process of C1 VA vertebral artery X vagus nerve XI spinal accessory nerve
selective neck dissection photo
The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The posterior condylar vein crossing the occipital condyle is notedICA internal carotid artery JB jugular bulb PCV posterior condylar vein
IX glossopharyngeal nerve XI spinal accessory nerve
PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

PCV=CV = condylar vein
After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

After removal of the posterior condylar vein and further removal of the occipital condyle (OC) the hypoglossal nerve (XII) is noted ICA internal carotid artery JB jugular bulb
JT jugular tubercle OC occipital condyle VA vertebral artery XI spinal accessory nerve XII hypoglossal nerve
OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

OC= Occipital condyle JT = Jugular tubercle JP = Jugular process
JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

JP = Jugular process
JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

JT above hypoglossal canal amp OC is below hypoglossal canal
Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Intradural structures when approached laterally by
ITF-A + TC + TT approach
The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The extracranial end of the hypoglossal canal is located immediately above the junction of the anterior and middle one-third of the occipital condyle
Hypoglossal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal nerve JT = Jugular tubercle OC = Occipital condyle
The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The lower cranial nerves have an intimate relationship with the jugular tubercle (three black arrows) When the occipital bone and jugular tubercle are being drilled careful attention should be paid to avoiding damage to the lower cranial nerves Cbl cerebellum ICA internal carotid artery OC occipital condyle TP transverse process of the C1 vertebra VA vertebral artery VIII cochleovestibular nerve IX
glossopharyngeal nerve XI spinal accessory nerve
Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Combined extreme lateral and POTS approach Note the bettercontrol of the lower clivus and the lower cranial nerves after
transection of the sigmoid sinus and drilling of the jugular tubercle
From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

From Laterally
3 Modified trans-cochlear approach type D (MTCD)
Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Schematic drawing of the modified transcochlear approach type D (MTCD)AFL anterior foramen lacerum C1 atlas CO cochlea et eustachian tube gspn greater
superficial petrosal nerve ICA internal carotid artery IJV internal jugular vein Lv vein of Labbeacute mma middle meningeal artery M mandible OC occipital condyle pc clinoid
process pp pterygoid plate sph sphenoid sinus sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus VA vertebral artery V2 maxillary branch of the
trigeminal nerve V3 mandibular branch of the trigeminal nerve za zygomatic arch VII facial nerve IX glossopharyngeal nerve X vagus nerve XI spinal accessory nerve XII hypoglossal
nerve
Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Anatomical dissection showing a transcochlear approach type D with jugular bulb in placeC2N C2 nerve FN facial nerve lCA internal carotid artery IJV internal jugular vein JB jugular bulb SS
sigmoid sinus VA vertebral artery V trigeminal nerve
From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

From Laterally
Far lateral or Transcondylar approach
Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Schematic drawing of the extreme lateral approach AFL anterior foramen lacerum C1 first cervical vertebra CO cochlea et eustachian tube ev emissary vein gps greater petrosal
nerve ICA internal carotid artery JV jugular vein Lv vein of Labbeacute M mandible mma middle meningeal artery oc occipital condyle pc clinoid process pp pterygoid process sph
sphenoid sps superior petrosal sinus TA transverse process of the atlas TS transverse sinus za zygomatic arch V2 maxillary nerve V3 mandibular nerve VII facial nerve IX
glossopharyngeal nerve XII hypoglossal nerve
Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Drawing of the muscles related to the vertebral artery at the suboccipital region Reflection of the sternomastoid and the splenius capitis muscles
reveals the deeper muscles in this area
Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Dissection of the right side The sternomastoid muscle (StM) has been retracted anteriorly The levator scapulae (LS) and the splenius capitis (SpC) muscles can be
identified at a superficial level
Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Reflecting the splenius capitis (SpC) muscle together with the slender deeply attached longissimus capitis (LC) muscle reveals the deep inferior (IO) and
superior (SO) oblique muscles
The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The levator scapulae muscle is divided uncovering the inferior oblique muscle By careful detachment of this inferior oblique muscle muscle and using blunt dissection the vertebral artery can be found An important landmark is the C2 nerve root which
crosses over the artery - ----- in anterior skull base by retracting the rectus capitus lateral muscle we can identify the vetebral artery ndash see the next slide
Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Between suprior oblique SO amp inferior oblique IO you will find the vertebral artery ndash DrSatish jain
A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

A presigmoid craniotomy has been partially performed ex- posing the sigmoid sinus (SS) A suboccipital craniotomy ()
extending caudal to the level of the foramen magnum is performed
The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The VA at the level of the transverse process of the atlas is located on the medial side of the rectus capitis lateralis muscle
[ RCLM ]
First Longus capitis muscle seen Next longus coli amp rectus capitus anterior seen
Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Schematic drawing showing the relationship between the oblique muscles and the vertebral artery between C1 and C2
The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The transverse process of the atlas (TPC1) forms an importantlandmark in this region
Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Course of the vertebral artery (VA) after leaving the transverseprocess of the axis The foramen transversarium of the atlas (hatched
lines) has been opened Pa posterior arch of the atlas
While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

While mobilizing the vertebral artery the periosteum ofthe posterior arch of the atlas is elevated and used to pro-tect the artery and to avoid
bleeding from the surroundingvenous plexus
C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

C2 nerve root below the 11th nerve in posterior triangle clearance in SLD
the C2 nerve root is seen crossingthe vertebral artery (VA)
External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

External view of the relationship between the parapharyngeal portion of the internal carotid artery and the vertebral artery A vertebral window between the transverse processes is needed to visualize the vertebral bed Note that the posterior belly of the digastric muscle has been cut
C1TP transverse process of C1 C2 second cervical root CC carotid canal DMpb posterior bellyof the digastric muscle FA facial artery ICAp parapharyngeal portion of the internal carotidartery IJV internal jugular vein SCG superior cervical ganglion SG spinal ganglionSHM stylohyoid muscle SP styloid process SPM stylopharyngeus muscle VA vertebral arteryVIIcn facial nerve IXcn glossopharyngeal nerve Xcn vagus nerve XIcn accessory nerve XIIcnhypoglossal nerve
C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

C2N = DR2
In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

In about half the cases the accessory nerve crosses posteromedial to the internal jugular vein In all cases it passes anterolateral to the transverse process of the atlas Note the close relation between the vertebral artery and the internal jugular vein In extensive cases of posteriorly located glomus tumors the vertebral artery may be involved
At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

At a higher magnification the C2 nerve root is seen crossingthe vertebral artery (VA)
To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

To gain intradural access the artery bends again anteromediallyto pierce the dura posteromedial to the occipital condyle At this point the
dura is firmly attached to the artery
11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

11th nerve behind left vertebral artery at cervico-medullary junction ndash listen lecture at 2325 min in this Prof Amin Kassam video https
wwwyoutubecomwatchv=QoMCqwJ6Ke0
Through anterior skull base approach
Through endoscopic lateral skull base approach ndash The entrance of the vertebral artery is the boundary between the foramen magnum and the spinal part of the accessory nerve
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
Endoscopic lateral skull base approach
intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

intra operative photograph through operating microscope during removal of posterior fossa arachnoid cyst -showing medulla oblnagata-cervical spinal cord -cerebellar tonsils-vertebral artery-hypoglossal nerve -accessory nerve -1st cervical nerve root -PICA loopeafter removal of cyst wall
The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The accessory nerve (XI) is closely related to the vertebral artery (VA) at the point of dural entrance Note the dura attached to the artery at this level
In far lateral approach
The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The segment of the vertebral artery located between the C1 transverse process and the dural entrance gives rise to muscular branches and the posterior meningeal artery which can be safely coagulated The PICA
ocasionally arises extradural and could be inadvertently injured
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at httpneuroc99sldcutextMicrosurgicalPICAhtm
The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The PICA ocasionally arises extradural and could be inadvertently injured ndash see the total material regarding this topic at
httpneuroc99sldcutextMicrosurgicalPICAhtm
Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Although the dural opening is performed after drilling of the occipital condyle it has been opened before to expose the neurovascular structures The hypoglossal nerve arises from the
preolivar sulcus and runs laterally to the hypoglossal canal From this view the hypoglossal nerve is covered by the roots of the accesory nerve
The posterior condylar emissary vein which travels from the jugular bulb to the extraduralvenous plexus may be injured and hemostasis if it is necessary The degree of occipital
condyle removal vary widely although posterior and medial one third of the condyle usually isenough for ventrolateral tumors If more than 50 of the condyle is resected the
craniovertevral junction becomes unstable and occipitocervical stabilization is required
Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Subperiosteal separation of the suboccipital muscles identifies the vertebral arteryMT mastoid tip Pa periosteum of the artery VA vertebral artery
How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

How to cauterisestop bleeding from PCV ( posterior condylar vein ) amp peri-vertebral
venous plexus -
Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Vertebral artery exposure A Step 1 subperiosteal dissection of the posteroinferior aspect of the C1 posterior arch
B Step 2 subperiosteal dissection of the posterior aspect of the C1 posterior arch C Step 3 subperiosteal dissection of the posterosuperior aspect of the C1 posterior arch
D Step 4 dissection of the inferior aspect of the horizontal and oblique portions of the VA V3 segment
E Step 5 dissection of the posterior aspect of the oblique and horizontal portions of the VA V3 segment
F Step 6 dissection of the superior aspect of the horizontal and oblique portions of the VA V3 segment
Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Intradural structures when approached laterally
PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

PICA can be seen running between spinal and cranial portions of the accessory nerves (CN XI ndash S CN XI ndash C)
Endoscopic lateral skull base
Endoscopic anterior skull base
Lateral skull base ndash far lateral approach
The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

The occipital condyle (OC) is partially drilled
Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Opening the dura posterior and parallel to the sigmoid sinus
A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

A general view showing the different structures exposed after opening the dura A cuff of adherent dura is left attached to the vertebral artery (VA) Note the close proximity of the spinal accessory nerve (XIs) to the artery and the dura at this level The lower cranial nerves in relation to the posterior inferior cerebellar artery are appreciated
The cerebellum is gently retracted to expose the different structures at the cerebellopontine angle
At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

At a higher magnification the nerves IXminusXI are seen coursingtoward the jugular foramen The two bundles of the hypoglossal nerve(XII) are closely related to the vertebral artery (VA) before they unite tocourse in the hypoglossal canal in the partially drilled occipital condyle
(OC) XIs spinal accessory nerve
Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Changing the tilt of the microscope the two vertebral arteriesand the vertebrobasilar junction (VBJ) are exposed Note the control
of the ventrolateral surface of the medulla (Med) VA vertebral arteryVAc contralateral vertebral artery
Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Panoramic view of the posterior fossa exposed through the extreme lateral approach
At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

At higher magnification the ventrolateral surface of themedulla (Med) is well seen
PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

PSA amp ASA With a more downward angulation of the microscope the upper part of the spinal cord (SpC) is well controlled The posterior spinal artery (PSA) is also seen
Anterior spinal arteries ndash Courtesy Dr Julio Ceacutesar Peacuterez Mexico
From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

From Posteriorly
Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Suboccipital craniotomy
See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

See this video click - httpsyoutubeSIF4Sd0z33o - CERVICO-MEDULLARY EPIDERMOID-microsurgical removal-dr suresh duganiHUBLI KARNATAKINDIA
Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Vertebral artery
V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

V1 V2 V3 V4
V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

V1 V2 V3 V4
V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

V1 V2 V3 V4
Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

Schematic drawing and selective injection of the vertebral artery in lateral projection (subtracted form ) OB occipital bone V1 first segment of the vertebral artery V2 second segment of the vertebral artery V3h horizontal third segment of the vertebral artery V3v
vertical third segment of the vertebral artery V4 fourth segment of the vertebral artery
bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

bull V3 Segmentbull The V3 segment extends from the transverse foramen of the axis to the dural penetration by thebull vertebral artery it is further subdivided into two parts a proximal vertical part (V3v) and a distalbull horizontal part (V3h) The V3 segment possesses four vascular loops (Figs 336 337 340)bull bull The inferomedial loop appears at the transverse foramen of the axis and directs the artery laterallybull and slightly posteriorly and upwardbull bull The inferolateral loop directs the artery distinctly upward and slightly anterior toward thebull transverse foramen of the atlasbull bull The superolateral loop is located at the point where the V3v turns into a horizontal position in thebull sulcus of the posterior arch of the atlas and becomes V3h (Figs 338a 339a 340) The V3v andbull V3h parts each have two constant branchesbull ndash The muscular artery of V3v arises at the inferolateral arterial loop it communicates with thebull branches of the ascending pharyngeal arterybull ndash The radiculomuscular artery of V3v arises below the transverse foramen of the atlas and givesbull rise to the medial branch (a radiculomedullary artery) vascularizing the C2 ganglion the C2bull nerve and the spinal cord and the lateral branch a muscular branch for the suboccipital musclesbull ndash The muscular artery of V3h vascularizes the muscles of the deep muscular layer andbull communicates with the branches of the occipital arterybull ndash The posterior meningeal artery of V3h arises at the superomedial loop and vascularizes thebull neighboring portion of the posterior fossa dura the falx cerebelli and the posterior portion of thebull tentoriumbull bull The superomedial loop surrounds the lateral mass of the atlas and brings the V3 to its dural
foramen
A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

A Surgical approach to the vertebral artery ndash pre and retrosigmoid approaches ( Dr Laligam Sekhar) B Saphenous vein graft of the vertebral
artery ( Dr Laligam Sekhar)
For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading

For Other powerpoint presentatioins of ldquo Skull base 360deg rdquo
I will update continuosly with date tag at the end as I am getting more amp more information
click
wwwskullbase360in - you have to login to slidesharenet with Facebook account for downloading