Embed Size (px)
Citation preview

C
UU
I
PEER-REVIEW REPORTS
Do Grossly Identifiable Ganglia Lie Along the Spinal Accessory Nerve? A Gross andHistologic Study with Potential Neurosurgical SignificanceR. Shane Tubbs1, Jeffrey R. Lancaster1, Martin M. Mortazavi1, Marios Loukas2, Mohammadali M. Shoja3,
Eyas M. Hattab4, Aaron A. Cohen-Gadol5
ugons
icicrSsStditfatwt
M
Wi3swmtdTcatstcfgaswm
aw
�
�
INTRODUCTION
Because focal enlargements may be seenduring various approaches to the poste-rior cranial fossa and may be mistaken fortumors or other pathology (5), we aimedto understand the true nature of thesestructures better through an anatomicstudy. Some authors (11) have encoun-tered head pain as a response to intraop-erative stimulation of the spinal accessorynerve (SAN). Some investigators have re-ported occasional grossly visible gangliaassociated with the SAN (4, 5). However,the literature on this subject is very scarce,and a general consensus regarding thesignificance of such focal enlargements isnot readily available. This lack of consen-sus is evidenced by the fact that popularanatomy and physiology textbooks stillreport that the SAN is a purely motor
Key words� Innervations� Nerve supply� Neurosurgery� Sternocleidomastoid� Trapezius
Abbreviations and AcronymsSAN: Spinal accessory nerve
From 1PediatricNeurosurgery,
hildren’s Hospital, Birmingham, Alabama, USA;2Department of Anatomical Sciences, St. George’s
niversity, Grenada; 3Neuroscience Research Center, Tabrizniversity of Medical Sciences, Tabriz, Iran; and
4Department of Pathology and Laboratory Medicine,mmunohistochemistry Laboratory, and 5Department ofNeurological Surgery, Goodman Campbell Brain and Spine,Indiana University, Indianapolis, Indiana, USA
To whom correspondence should be addressed:Aaron A. Cohen-Gadol, M.D., M.Sc.[E-mail: [email protected]]
Citation: World Neurosurg. (2012) 77, 2:349-351.DOI: 10.1016/j.wneu.2011.04.030
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter © 2012 Elsevier Inc.All rights reserved.
nerve, and the presence of SAN ganglia is g
WORLD NEUROSURGERY 77 [2]: 349-351
sually ignored. However, the presence ofanglia (nerve cell bodies located outsidef the central nervous system) along aerve suggests that the nerve contains aensory function (9).
Based on investigations of the SAN andts musculature, some authors have con-luded that there is a strong phylogeneticnclination for the SAN to lose its sensoryells by their migration into the dorsaloots of adjacent cervical nerves (12).treeter (13) found that there are moreensory cells in the SAN of a fetus than theAN of an adult (3, 10, 16). Fahmy (3) men-ioned that ganglion cells were more “abun-ant and conspicuous” in a 3-month-old
nfant compared with an adult but basedhis on a single specimen. Further supportor the sensory hypothesis comes fromnother study in rats that concluded thathe “architectural features of neuronsithin the [SAN] ganglion are similar to
hose of neurons in other sensory gan-
� OBJECTIVE: To elucidate further thebeen observed along the spinal accesposterior cranial fossa.
� METHODS: Dissection of the postedult cadavers with attention to the SAith it.
RESULTS: Grossly, four specimensments associated with the SAN wistructures were in intimate contact wof the SAN in all specimens and meright-sided male specimen had two fowere found within 1 cm of the forameneuronal cells were identified within tThese focal enlargements are best detopias within the leptomeninges aroun
CONCLUSIONS: The focal enlargemtermed ganglia. These structures do nobe mistaken for pathology of the post
lia” (16). y
, FEBRUARY 2012 ww
ETHODS
e dissected the posterior cranial fossan 27 adult cadavers (54 sides) aged9 –78 years at the time of death. Of thesepecimens, 18 were formalin-fixed, and 9ere unembalmed; 12 specimens wereale, and 15 were female. The bone over
he posterior fossa was removed with arill (Midas Rex; Medtronic, Fort Worth,exas, USA), and the cerebellum wasarefully removed. Brainstem retractionllowed identification of the SAN. No pa-hology was observed in the area of dis-ection of any specimen. The SAN wasraced from its entrance into the posteriorranial fossa until its exit via the jugularoramen. Observations were made forrossly identifiable focal enlargementslong this nerve. When identified, mea-urements of these structures were madeith microcalipers, and the focal enlarge-ents were submitted for histologic anal-
tomy of focal enlargements that havenerve (SAN) as it courses within the
cranial fossa was performed on 27nd any focal enlargements associated
%) were found to have focal enlarge-the posterior cranial fossa. Thesee dorsal aspect of the spinal portion
ed a mean diameter of 1.9 mm. Oneenlargements. All focal enlargementsagnum. Histologically, no ganglion or
focal enlargements in any specimen.bed as ectopic glial nests or hetero-e SAN.
located along the SAN should not bentain neural structures and should notfossa.
anasory
riorN a
(14.8thinith thasurcaln mhesescrid th
entst co
erior
sis (hematoxylin and eosin staining).
w.WORLDNEUROSURGERY.org 349

R
Gfacmmsowpmadrtsfrwm
apcimlg
mdap
(otr
in con
PEER-REVIEW REPORTS
R. SHANE TUBBS ET AL. SPINAL ACCESSORY NERVE GANGLIA
Statistical analysis between sides andgenders was performed using Statisticafor Windows (StatSoft, Tulsa, Oklahoma,USA) with significance set at P � 0.05.
ESULTS
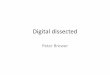
rossly, four specimens (14.8%) wereoundto have focal enlargements associ-ted with the SAN within the posteriorranial fossa (Figure 1). Focal enlarge-ents were found on two left sides in oneale and one female specimen, one right
ide in a male specimen, and bilaterally inne female specimen. These structuresere in intimate contact with the spinalortion of the SAN in all specimens andeasured 1–2.2 mm (mean 1.92 mm) in di-
meter. All focal enlargements were foundorsal to the spinal portion of the SAN. Oneight-sided male specimen was seen to havewo focal enlargements: one dorsal to thepinal portion of the SAN and one smallerocal enlargement adjacent to the cranialoot of the SAN. All focal enlargementsere found within 8.5 mm of the foramenagnum.Grossly, these focal enlargements were
ssociated with the SAN but did not ap-ear to be embedded within it. Histologi-ally, no ganglion or neuronal cell wasdentified within these focal enlarge-
ents in any specimen. These focal en-argements were best described as ectopic
Figure 1. Spinal accessory nerve ganglia(arrows) seen on the right side of a malecadaveric specimen. The brainstem has beendissected to show the lower cranial nervesnear the foramen magnum. Vertebral a.,vertebral artery; IX, glossopharyngeal nerve;X, vagus nerve; XI, accessory nerve.
lial nests or heterotopias within the lepto-
350 www.SCIENCEDIRECT.com
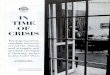
eninges around the SAN (Figure 2). Ad-itionally, pale blue structures were notedt the periphery, and these representedolyglucosan bodies (corpora amylacea)
Figure 2. Left-sided spinal accessory nerve (SANwith surrounding blood vessels. The SAN is in tlongitudinally. Histologically, the ganglia are not
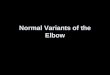
Figure 3. Left-sided spinal accessory nerve gangli
corpora amylacea (large blue-colored cells) at the peripheryWORLD NEUROSURGE
Figure 3). No statistical significance wasbserved for an increased frequency of
hese focal enlargements between left oright sides or between genders.
lia (hematoxylin and eosin, �5) in the centerest part of the field and is travelingtact with the nerve.
n in Figure 2 now at �50 magnification. The
) ganghe low
a show
indicate chronicity.RY, DOI:10.1016/j.wneu.2011.04.030

1
1
1
1
1
1
1
1
Cacc
r
CD
J
A
PEER-REVIEW REPORTS
R. SHANE TUBBS ET AL. SPINAL ACCESSORY NERVE GANGLIA
DISCUSSION
None of the ganglia found along the SAN inour study contained neural structures. Theterm ganglion should not be used to describethese structures. The polyglucosan bodies(corpora amylacea) seen in these focal en-largements signify the chronicity of thesefocal enlargements, which also should notbe mistaken for tumors. Corpora amylaceaare small hyaline structures of unknownsignificance that are derived from degener-ate cells and occur more frequently with ad-vancing age. Some authors have suggestedthat such ganglia along the SAN are respon-sible for various clinical findings. Ray andWolff (11) directly stimulated the SAN inneurosurgical patients. Patients reportedpain “. . . low in the back of the head and inthe upper cervical regions of the same side.”The conclusion of these authors was thatthe SAN transmits nociception from themusculature it innervates. In a relatedstudy, researchers examined the SAN anddescribed its complicated anatomy, whichinvolves adhesions, or anastomoses, be-tween the SAN and the cervical plexus (1).
Because the SAN innervates the sterno-cleidomastoid and trapezius muscles in hu-mans, it is a logical extension to assumethat the nerve could also carry propriocep-tive signals from these same muscles (6,16). Windle (17), in a study of the same sub-ject in cats and monkeys, added that al-though there is likely proprioception fromthe sternocleidomastoid and trapeziusmuscles, it is doubtful that the SAN alonecarries proprioception for these muscles.To support this idea, Corbin and Harrison(2) identified a proprioceptive function ofthe SAN in cats. Sensory microgangliatransmitting proprioception in the SAN asanastomotic connections of the dorsalroots of upper cervical nerves have been re-ported (4, 5, 14, 15).
The way in which the afferent sensorypathways travel to their final location makesunderstanding of such pathways difficult.One of the problems faced when studyingthe SAN is its two-part anatomy. This par-
WORLD NEUROSURGERY 77 [2]: 349-351
sisting of a cranial and a spinal root (16). Toadd to the intricacy, Ouaknine and Nathan(8) and Oh et al. (7) reported four varioustypes of anastomotic connections in whichthe SAN fuses with the posterior roots of C1.Another confounding issue is that the gan-glia cells of the SAN have been reported tohave a “migrating anatomy” throughout fe-tal growth. Fahmy (3) reported that “[t]heganglion crest is at first continuous, butsubsequently becomes subdivided . . . [andthat it is] conceivable that these cells have atendency for distal migration.”
Although we did not identify neural cellswithin these structures, it is possible thatsuch cells may have migrated during devel-opment to other sites (eg, dorsal root gan-glia). All of our specimens were adults; alarger study of specimens from children orfetuses is in order to verify this idea. None-theless, and based on our study, these focalenlargements in adults should not be mis-taken for pathology.
CONCLUSIONS
Although no ganglion cells were identifiedin the spinal accessory ganglia, it remainsto be seen if any sensory fibers may traversesuch structures.
REFERENCES
1. Bremner-Smith AT, Unwin AJ, Williams WW: Sen-sory pathways in the spinal accessory nerve. J BoneJoint Surg Br 81:226-228, 1999.
2. Corbin KB, Harrison F: Proprioceptive componentsof cranial nerves: the spinal accessory nerve. J CompNeurol 69:315-328, 1938.
3. Fahmy N: A note on the intracranial and extracranialparts of the IXth, Xth, and XIth nerves. J Anat 61:298-301, 1926.
4. Lang J: Clinical Anatomy of the Posterior CranialFossa and Its Foramina. Stuttgart: Thieme MedicalPublishers; 1991.
, FEBRUARY 2012 ww
6. Mills KR, Newham DJ, Edwards RHT: Muscle pain.In: Wall PD, Melzack R, eds. Textbook of Pain. Ed-inburgh: Churchill Livingstone; 1984:319-330.
7. Oh CS, Chung IH, Koh KS, Kim HJ, Nam KI: Mor-phologic study of the connections between the ac-cessory nerve and the posterior root of the first cer-vical nerve. Clin Anat 15:267-270, 2002.
8. Ouaknine G, Nathan H: Anastomotic connectionsbetween the eleventh nerve and the posterior root ofthe first cervical nerve in humans. J Neurosurg 38:189-197, 1973.
9. Pearson AA: The spinal accessory nerve in humanembryos. J Comp Neurol 68:243-266, 1937.
0. Ranson SW: The structure of the spinal ganglia andof the spinal nerves. J Comp Neurol 22:159-169,1912.
1. Ray BS, Wolff HG: Experimental studies on head-ache: Pain-sensitive structures on the head and theirsignificance in headache. Arch Surg 41:813-856,1940.
2. Strauss WL, Howell AB: The spinal accessory nerveand its musculature. Quart Rev Biol 11:387-405,1936.
3. Streeter GL: The development of the cranial and spi-nal nerves in the occipital region of the human em-bryo. Am J Anat 4:83-116, 1904.
4. Tubbs RS, Loukas M, Slappey JB, Shoja MM, OakesWJ, Salter EG: Clinical anatomy of the C1 dorsal rootganglion, and ramus: a review and anatomicalstudy. Clin Anat 20:624-627, 2007.
5. Tubbs RS, Loukas M, Yalcin B, Shoja MM, Cohen-Gadol AA: Classification and clinical anatomy of thefirst spinal nerve: surgical implications. J NeurosurgSpine 10:390-394, 2009.
6. Wetmore C, Elde R: Detection and characterizationof a sensory microganglion associated with the spi-nal accessory nerve: a scanning laser confocal mi-croscopic study of the neurons and their processes. JComp Neurol 305:148-163, 1991.
7. Windle WF: The sensory components of the spi-nal accessory nerve. J Comp Neurol 53:115-127,1931.
onflict of interest statement: The authors declare that therticle content was composed in the absence of anyommercial or financial relationships that could beonstrued as a potential conflict of interest.
eceived 8 December 2010; accepted 27 April 2011
itation: World Neurosurg. (2012) 77, 2:349-351.OI: 10.1016/j.wneu.2011.04.030
ournal homepage: www.WORLDNEUROSURGERY.org
vailable online: www.sciencedirect.com
ticular nerve has the unique feature of con-5. Lang J: Clinical Anatomy of the Cervical Spine. Stutt-
gart: Thieme Medical Publishers; 1993.1878-8750/$ - see front matter © 2012 Elsevier Inc.All rights reserved.
w.WORLDNEUROSURGERY.org 351