Embed Size (px)
DESCRIPTION
Case record...Aicardi syndrome
Citation preview

CLINICAL PICTURE:
11 years old female patient presented with congenital left sided hemiaplasia and Lennox Gastaut syndrome. The patient's family gave a history of west syndrome during the first year of the patient's life. Fundus examination revealed chorioretinal lacunae. EEG examination revealed 1.5 C/S slow spike/slow wave discharge of Lennox Gastaut syndrome. The patient's scholastic achievement was very poor.
RADIOLOGICAL FINDINGS:
Figure 1. Precontrast MR T1 images showing a huge right sided intraventricular /parenchymal cyst associated with agenesis of the septum pellucidum. The corpus callosum is markedly hypoplastic and deficient. The cerebral cortex is lissencephalic. Notice the right sided hemimegalencephaly and the subependymal nodular heterotopia. Subcortical band heterotopia can also be appreciated.
Figure 2. Precontrast MR T1 images showing a huge right sided intraventricular /parenchymal cyst associated with agenesis of the septum pellucidum. The corpus callosum is markedly hypoplastic and deficient. The cerebral cortex is lissencephalic. Notice the right sided hemimegalencephaly and the subependymal nodular heterotopia.
CASE OF THE WEEK
PROFESSOR YASSER METWALLY
CLINICAL PICTURE
RADIOLOGICAL FINDINGS

Figure 3. MR T2 images showing a huge right sided intraventricular /parenchymal cyst associated with agenesis of the septum pellucidum. The corpus callosum is markedly hypoplastic and deficient. The cerebral cortex is lissencephalic. Notice the right sided hemimegalencephaly and the subependymal nodular heterotopia. Subcortical band heterotopia can also be appreciated.
Figure 4. Precontrast MR T1 images showing A huge right sided intraventricular /parenchymal cyst. The cerebral cortex is lissencephalic. Notice the right sided hemimegalencephaly and the subependymal nodular heterotopia. Subcortical band heterotopia can also be appreciated.

Figure 5. Precontrast MR T1 images showing a huge right sided intraventricular /parenchymal cyst. The corpus callosum is markedly hypoplastic and deficient. The cerebral cortex is lissencephalic. Notice the subependymal nodular heterotopia and hypoplasia of the optic nerve. The cerebellum and brain stem are also hypoplastic.
Figure 6. Precontrast MR T1 images showing a huge right sided intraventricular /parenchymal cyst. The cerebral cortex is lissencephalic. Notice the right sided hemimegalencephaly and the subependymal nodular heterotopia.
Figure 7. Precontrast MR T1 images showing marked hypoplasia of the cerebellum and brain stem.

Criteria that are highly suggestive of Aicardi syndrome
Partial or complete callosal agenesis
Cortical dysplasia
Gross asymmetry of the hemispheres
Periventricular or subcortical heterotopias
Cysts of the choroid plexus or around the third ventricle is highly suggestive of AS
DIAGNOSIS: AICARDI SYNDROME ASSOCIATED WITH MULTIPLE CORTICAL DYSPLASIAS THAT INCLUDE HEMIMEGALENCEPHALY, LISSENCEPHALY, HETEROTOPIAS, AND SEPTO-OPTIC DYSPLASIA.
DISCUSSION:
The Aicardi syndrome (AS) is classically defined as a triad of abnormalities that includes agenesis of the corpus callosum, infantile spasms, and chorioretinal lacunae (1,2). Other eye defects and costovertebral and other malformations occur frequently. The syndrome has been observed exclusively in individuals with two X chromosomes, and only one familial case is known (3,4).
Progress in neuroimaging has revealed that the central nervous system malformation in AS is not limited to agenesis of the corpus callosum but consists of a complex of abnormalities characterized by severe neuronal migration defects with periventricular and subcortical heterotopias, cortical polymicrogyria, and a tendency toward the development of cystic formations in the choroid plexuses and in other parts of the brain (3-5). The migration anomalies may even be more important for the definition of AS than callosal agenesis, which is a non- specific finding. Similarly, the eye abnormalities are often complex, and defects of closure of the primitive cupula are commonly present (6-8).
The incidence of AS is unknown. More than 300 cases are known to this writer, and at least 170 cases have been published. In series of infantile spasms, AS may account for up to 4% of cases (9), but a selection bias is probable in series originating from tertiary referral centers.
CLASSICAL FINDINGS IN AICARDI SYNDROME
The classical picture of AS has been outlined in several articles (3,6, 1 0, I 1). The seizures are typically infantile spasms. These have been the only seizure type in 86 of 184 patients (47%) and have been associated with other seizures, especially partial motor attacks, in 65 of 184 patients (35%) (6). The partial seizures often begin before the infantile spasms, at times as early as the first few days of life (6,12). The age at first seizure was less than 3 months in 68% of 146 patients and less than I month in 23%. The age at the first spasm in 137 patients was less than I month in 18% and less than 3 months in 56%. Typical tonic spasms have been reported even during the neonatal period, and AS is one possible cause of the "early infantile epileptic encephalopathy" described by Ohtahara et al. (13). Partial seizures and infantile spasms often occur in association, a focal or lateralized tonic or clonic seizure being followed by a similarly lateralized cluster of spasms. The focal seizure is manifested on the EEG by a localized discharge of repetitive spikes lasting 10-30 s. The spasms follow immediately after the spikes and are associated with a series of slow complexes, often with a superimposed fast rhythm that is usually of higher amplitude on the side of the initial
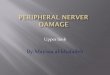
Figure 8. Chorioretinal lacunae
DIAGNOSIS:
DISCUSSION

partial discharge. The complexes occur 6- 20 s apart, and no paroxysmal activity appears between them. The initial partial seizure and the spasms that follow appear to represent a single attack that usually occurs on awakening or on changing from slow wave to REM sleep (12,14). Such periodic spasms are also associated with other brain malformations (14).
Typical hypsarrhythmia is rare in AS (18% of 137 cases). The most common interictal EEG abnormality is an asymmetrical pseudo-periodic tracing with bursts of paroxysmal irregular slow and sharp waves of 3- to 6-s duration, separated by a relatively flat EEG for 5-20 s. Such bursts may occur independently over each hemisphere or may remain unilateral, with various abnormalities over the other hemisphere, the so-called "split-brain" EEG (6). The tracings more commonly evolve into multifocal paroxysmal abnormalities than into typical hypsarrhythmia. At a late stage, spike-and- wave complexes are unusual (6,9).
The choroidal lacunae are multiple rounded whitish or pinkish areas ranging in size from one-tenth to several disc diameters. They are in the same plane as the retina, so that vessels do not bend on crossing their border. Pigment deposits may be visible at their periphery and may increase with age (6,15). The largest lacunae tend to cluster around the disc, whereas small pinkish lesions tend to be more peripheral. They are usually bilateral, but unilateral lacunae can be seen even when the opposite eye is not microphthalmic. Typical lacunae are probably pathognomonic of AS. Colobomata are a very common finding and are of significance for the diagnosis, especially when lacunae are few or atypical. Unlike the lacunae, they are frequently unilateral. Colobomatous discs are surrounded by pigmented rings in many cases. Other eye abnormalities, including persistence of the primary vitreous, anterior synechiae, and microphthalmia, are not uncommon. In one patient, the appearance was that of retinal detachment suggestive of the Walker- Warburg syndrome. Interestingly, despite the very abnormal ophthalmoscopic aspect, useful vision is often preserved as far as can be assessed. The ERG has been found normal or only mildly altered in several patients. The visual evoked potentials are usually present but abnormal, probably as a result of the cortical abnormalities. The fundoscopic appearance results from thinning of the choroid and sclera in the areas corresponding to the lacunae where the pigment epithelium is depigmented or hypopigmented (7), with degeneration of the rods and cones (8). There is no evidence of inflammatory lesions, and the appearance is suggestive of an early developmental disorder.
Agenesis of the corpus callosum was complete in 137 of 152 patients for whom the information was available and was partial in 15 (10%). Partial agenesis is usually posterior (6), but cases of agenesis of both the genu and the splenium, with preservation of the body of the callosum, are known (16). The ventricular contour is not smooth as it is in most cases of callosal agenesis and the ventricles, including the third ventricle, have markedly irregular contours. In most cases there is also marked asymmetry between the two hemispheres, the larger one commonly but not consistently contralateral to a hemiplegia when present or to the side most involved by the spasms. Various abnormalities of the posterior fossa have also been reported (6).
The neurologic and mental impairment in AS is almost always very marked. The estimated survival rate in one study (17) was 75% at 6 years and 40% at 15 years. Epilepsy persists in most patients as infantile spasms, which is unusual with other causes. Approximately one-third of patients are unable to feed themselves and only one-quarter are able to walk. Only rare patients can use two-word sentences (3). One patient had relatively well-developed language at age 14 years (17). According to McGregor et al. (17), a worse prognosis was correlated with larger lacunar size. Hemiplegia is commonly present but it is seldom isolated, and some degree of contralateral involvement is the rule. Mild microcephaly is common but is never present at birth. Indeed, some infants have large heads that may result from hydrocephalus or from the development of large intracranial cysts. Although an occasional patient has been operated on for shunting of hydrocephalus due to aqueductal stenosis or for drainage of a cyst, this is seldom justified because the cysts do not usually continue to increase in postnatal life and ventricular dilatation usually remains static even when marked.
NEW FINDINGS IN AICARDI SYNDROME
Over the past few years the diagnosis of AS has been facilitated by modern imaging techniques. These have shown that agenesis of the corpus callosum is virtually never an isolated finding but is part of a complex of developmental abnormalities. Migration anomalies are probably present in all cases. They include periventricular and/or subcortical nodular heterotopias, which are responsible for the irregular contours of the lateral ventricles, and cortical dysplasia with thickening of the cortical plate and abnormal rectilinear or blurred interface between gray and white matter involving one or both hemispheres to a variable degree. These dysplastic areas probably correspond pathologically to polymicrogyria (3, 5,15,18,19). Periventricular heterotopias are easily detectable, but the diagnosis of subcortical heterotopias and cortical dysplasia requires high-quality MRI. Cysts are frequently revealed on MRI. They can involve the glomus of the choroid plexus on one or both sides and/or the region of the third ventricle and pineal gland, where they may be single or multiple and may be quite large (Fig. 1). The cysts give a slightly more intense signal than CSF and their walls may enhance with gadolinium contrast. Cysts around the third ventricle were probably responsible for the distorted appearance of this ventricle on MRI or CT scan, which could not result from heterotopias. Cysts of the cerebral hemispheres are uncommon. Cysts of the posterior fossa have been reported (3,6). Most of them correspond to partial agenesis of the cerebellar vermis, to a megacisterna magna, or to arachnoid cysts. True intraparenchymal cysts are uncommon. The combination of cysts of the choroid plexus in association with agenesis of the corpus callosum permits the antenatal diagnosis of AS (20). Solid tumors, especially papillomas of the choroid plexus, have been reported in several patients (3,6) and may be multiple (21). Peripheral embryonic tumors have also been described (22,23).

The combination of partial or complete callosal agenesis, cortical dysplasia, gross asymmetry of the hemispheres, periventricular or subcortical heterotopias, and cysts of the choroid plexus or around the third ventricle is highly suggestive of AS (3). Incomplete forms in which one or several components are lacking are not uncommon. Such forms are confirmed as AS by the presence of other typical manifestations, especially choroidal lacunae. There is probably no good reason to single out one component of the malformation complex so that cases without callosal agenesis but with heterotopias and/or cortical dysplasia can be diagnosed when other cardinal features are present. Two such cases (both with lacunae and one with vertebral abnormalities) are known to this author.
Criteria that are highly suggestive of Aicardi syndrome
Partial or complete callosal agenesis
Cortical dysplasia
Gross asymmetry of the hemispheres
Periventricular or subcortical heterotopias
Cysts of the choroid plexus or around the third ventricle is highly suggestive of AS
PATHOLOGY
Pathologic data on AS are scanty, and detailed microscopic examination of the brain is available for only two cases (5,18). Total or partial absence of the corpus callosum was found in all verified cases, usually with the presence of Probst bundles. Other structures may be lacking, such as the first cranial nerve and the mammary bodies. Other commissures, e.g., the fornix or the anterior commissure (6), may be absent, but this is inconstant.
Abnormalities of gyration were found in all studied cases (5-7,15,18). Their macroscopic aspect is variable, but microgyria is found microscopically and is of the unlayered type (18), taking the form of a thin, undulating cellular ribbon without any laminar organization. Fusion of the molecular layers of facing convolutions may result in the appearance of a pachygyric cortex (5). Heterotopias include subcortical neurons scattered in the white matter. Cysts have been reported in several cases (3,18,24) and were of ependymal origin.
Pathologic findings are consistent with an etiologic factor acting before the end of the migration period and the development of the corpus callosum, which is complete by 14 weeks of gestational age (25).
NOSOLOGIC LIMITS OF AS: THE PROBLEM OF INCOMPLETE FORMS
Figure 1. Huge cyst in a case of Aicardi syndrome. The cyst probably arises from the pineal area and develops into the left parietooccipital lobe, displacing and compressing the lateral ventricle. Note also agenesis of the corpus callosum and abnormal appearance of the posterior cortex on both sides, suggestive of migration disorder.
Figure 2. Image shows a cross-section of an eye in a patient with Aicardi syndrome. The arrow indicates chorioretinal lacunae.

Because there is no laboratory marker specific for AS, the classical triad remains the cornerstone of diagnosis. The existence of incomplete forms, however, seems likely, and cases without callosal agenesis have been already discussed. In addition to the two cases above, six cases of possible AS without callosal agenesis are known (6). All six had infantile spasms and choroidal lacunae, and four had irregular ventricular contours on CT. None of these patients underwent an MRI. Cases without infantile spasms have been reported (6) and may not be rare. Recognition of the spasms may be difficult because they are often quite asymmetrical and atypical and are frequently associated with partial seizures, which may be the predominant seizure type. Isolated partial seizures are not unusual at onset or late in the course, but they may be absent altogether.
The existence of AS cases without lacunae is particularly difficult to accept, because these are considered pathognomonic for the syndrome. There are, however, female patients with a suggestive brain malformation,, infantile spasms, and other abnormalities who might represent atypical forms. I know of three such patients who presented with infantile spasms and agenesis of the corpus callosum. Two of these had periventricular heterotopias on CT scan and an asymmetrical burst-suppression pattern on EEG. One girl had bilateral colobomata of the disk and another a small pigmented retinal area on one side. None of them had undergone MRI.
GENETIC AND CYTOGENETIC DATA
The original hypothesis that AS is an X-linked dominant disorder that is lethal at an early stage of gestation for affected hemizygous male conceptuses appears most compatible with the observed data (2,3,6). Only females are affected, with the exception of two phenotypical males with two X chromosomes (26). The male child with an XY karyotype reported by Curatolo et al. (27) is too atypical to be included (6,28, 29). This hypothesis is also consistent with the sporadic occurrence of the syndrome. Only one instance of familial recurrence in two sisters is reported (4) and this remains difficult to explain because no chromosomal abnormality was found in these patients. Another finding difficult to reconcile with the hypothesis is the occurrence of AS in only one of a pair of monozygotic twins, the co-twin being completely normal as a young adult (30). If this report is confirmed, it might be explained by extreme nonrandom inactivation of the abnormal X chromosome in the normal twin or, less probably, by a postzygotic mutation during early embryonic development.
The strong suspicion of an abnormality of an X chromosome in patients with AS has been reinforced by the finding of skewed X inactivation in the lymphocytes of some patients (31). Patients with nonrandom inactivation were found to be more severely affected than those with a random pattern, suggesting that selection against abnormal cells in the developing neural tissue led to aberrant brain development. However, a normal inactivation pattern has been found in other cases (30,32).
A possible locus for AS on the short arm of the X chromosome has been suggested by several case reports of eye abnormalities with callosal agenesis or other brain abnormalities (33-36) associated with translocations or other chromosomal abnormalities at Xp22.3. However, none of the reported patients had the typical triad of AS, even though microphthalmia (3), chorioretinal lesions reminiscent of the lacunae (Aughton et al., personal communication, 1991), other eye abnormalities (33,34), agenesis of the corpus callosum (36) or other brain defects (35), and costovertebral malformations (33) were present in variable associations. Four of these children also had focal dermal hypoplasia or Golz disease, a sex linked disorder with lethality for hemizygous males mapping at Xp22.3 (36). Such cases suggest that the Xp22.3 region is involved in the genesis of both Golz syndrome and AS. They could represent contiguous gene syndromes involving both loci. Intensive search for an AS gene in the Xp22.3 region is being pursued.
SUMMARY
AS is an uncommon malformation complex that affects mostly the eyes and the central nervous system. Brain malformation constitutes the core of the syndrome. Agenesis of the corpus callosum is the most easily detectable but probably not the most characteristic feature. Migration anomalies, including periventricular and subcortical nodular heterotopias and cortical dysplasia, and a tendency towards the formation of ependymal cysts in the glomus of the choroid plexuses and/or near of the third ventricle, are major components of the complex and may occur even in the presence of a complete corpus callosum. The resulting seizures, usually asymmetrical infantile spasms, and mental retardation constitute a severe disability with a much reduced life expectancy. The syndrome is probably due to a chromosomal accident involving one X chromosome. The Xp22.3 region is a prime candidate for location of one or several responsible genes, and demonstration of a DNA abnormality in this region will permit a better definition of the limits of the syndrome and perhaps help our understanding of some aspects of the development of the central nervous system.
AS is an uncommon malformation complex that affects mostly the eyes and the central nervous system. Brain malformation constitutes the core of the syndrome. Agenesis of the corpus callosum is the most easily detectable but probably not the most characteristic feature. Migration anomalies, including periventricular and subcortical nodular heterotopias and cortical dysplasia, and a tendency towards the formation of ependymal cysts in the glomus of the choroid plexuses and/or near of the third ventricle, are major components of the complex and may occur even in the presence of a complete corpus callosum. The
SUMMARY

resulting seizures, usually asymmetrical infantile spasms, and mental retardation constitute a severe disability with a much reduced life expectancy. The syndrome is probably due to a chromosomal accident involving one X chromosome. The Xp22.3 region is a prime candidate for location of one or several responsible genes, and demonstration of a DNA abnormality in this region will permit a better definition of the limits of the syndrome and perhaps help our understanding of some aspects of the development of the central nervous system.
The diagnosis of AS is based upon the classic triad of corpus callosal agenesis, chorioretinal lacunae and infantile spasm. But there is a range of costovertebral, ocular and cerebral abnormalities associated with this disorder.(2) The cerebral gray-matter heterotopias and other cortical malformations act as epileptogenic foci.(2) Their seizures typically start in early childhood and are usually intractable. Besides infantile spasm, other seizure types are also demonstrated. Dissociated burst-suppression or burst-suppression pattern appearing asymmetrically in either cerebral hemisphere is a characteristic EEG finding in AS.(8) The developmental delay in AS is generally profound, involving both motor and language skills. Chevrie and Aicardi in their analysis of 184 patients of AS observed that none had acquired meaningful speech.(9) But of late a larger spectrum of the disease has been recognized and it had been found that higher functioning AS individuals do exist.(2) Most of the AS cases die at an early age primarily due to aspiration pneumonitis. But some do live into their adolescent years and even in their twenties.(2) Good visual function in AS patients do occur if the fovea is uninvolved with chorioretinal lacunae.
Cerebral heterotopias, interhemispheric cysts, optic nerve coloboma, microphthalmia, thoracolumbar kyphoscoliosis are the known associated features in AS. Severe psychomotor impairment and absence of meaningful speech had also been noted. (3,4,5,6)
Addendum
A new version of this PDF file (with a new case) is uploaded in my web site every week (every Saturday and remains available till Friday.)
To download the current version follow the link "http://pdf.yassermetwally.com/case.pdf". You can also download the current version from my web site at "http://yassermetwally.com". To download the software version of the publication (crow.exe) follow the link:
http://neurology.yassermetwally.com/crow.zip The case is also presented as a short case in PDF format, to download the short case follow the link:
http://pdf.yassermetwally.com/short.pdf At the end of each year, all the publications are compiled on a single CD-ROM, please contact the author to know more
details. Screen resolution is better set at 1024*768 pixel screen area for optimum display. For an archive of the previously reported cases go to www.yassermetwally.net, then under pages in the right panel, scroll
down and click on the text entry "downloadable case records in PDF format" Also to view a list of the previously published case records follow the following link (http://wordpress.com/tag/case-record/)
or click on it if it appears as a link in your PDF reader
References
1. Aicardi J, Lefebvre J, Lerique-Koechlin A. A new syndrome: spasms in flexion, callosal agenesis, ocular abnormalities. Electroencephalogr Clin Neurophysiol 1965;19:609-10.
2. Aicardi J, Chevrie JJ, Rousselie F. Le syndrome agdndsie calleuse, spasmes en flexion, lacunes chorioretiniennes. Arch Franc Pgdiatr 1969;26: 1103-20.
3. Aicardi J, Chevrie JJ. The Aicardi syndrome. In: Lassonde M, Jeeves MA, eds. Callosal agenesis: the natural split brain. New York: Plenum Press, 1995.
4. Molina JA, Mateos F, Merino M, Epifanio JL, Gorrono M. Aicardi syndrome in two sisters. J Pediatr 1989;115:282-3.
5. Billette de Villemeur T, Robain 0, Chiron C. Unlayered polymicrogyria and agenesis of the corpus callosum: a relevant association? Acta Neuropathol (Berl) 1992;83:265-70.
6. Chevrie JJ, Aicardi J. The Aicardi syndrome;, In: Meldrum BS, ed. Recent advances in epilepsy, Vol. 3. Edinburgh: Churchill Livingstone, 1986: 189-210.
7. McMahon RG, Bell RA, Moore RW, Ludwin SK. Aicardi syndrome. A clinicopathological study. Arch Ophthalmol 1984;102:250-3.
8. Del Pero RA, Mets MB, Tripathy RC, Torezynski E. Anomalies of retinal architecture in Aicardi syndrome. Arch Ophthalmol 1986;104:1659-64.
REFERENCES

9. Aicardi J. Epilepsy in children, 2nd ed. New York: Raven Press, 1994:l-3.
10. Donnenfeld AE, Packer RJ, Zackai EH, Chee CM, Sellinger B, Emmanuel BS. Clinical, cytogenetic and pedigree findings in 18 cases of Aicardi syndrome. Am J Med Genet 1989;32:461-7.
11. Yamagata T, Momoi M, Miyamoto S, Kobayashi S, Kamoshita S. Multi-institutional survey of the Aicardi syndrome in Japan. Brain Dev 1990;12: 760-5.
12. Bour F, Chiron C, Dulac 0, Plouin P. Caractres electrocliniques des crises dans le syndrome d'Aicardi. Rev EEG Neurophysiol Clin 1986;16: 341-53.
13. Ohtahara S, Ohtsuka Y, Yamatogi Y, Oka E. The early infantile epileptic encephalopathy with suppression burst: developmental aspects. Brain Dev 1987;9:371-6.
14. Gobbi G, Bruno L, Pini A, Rossi PG, Tassinari CA. Periodic spasms: an unclassified type of epi- leptic seizure in childhood. Dev Med Child Neural 1987;29:766-75.
15. De Jong JGY, Delleman JW, Houben M, et al. Agenesis of the corpus callosum, infantile spasms, ocular anomalies (Aicardi's syndrome): clinical and pathological findings. Neurology 1976;26: 1152-8.
16. Aicardi J, Chevrie JJ, Baraton J. Agenesis of the corpus callosum. In: Vinken PJ, Bruyn GW, eds. Handbook of clinical neurology, Vol. 6. Brain malformations. Amsterdam: North-Holland, 1987:149-73.
17. McGregor DL, Menezes A, Buncic JR. Aicardi syndrome (AS): natural history and predictors of severity. Can J Neurol Sci 1993;20(suppl 2):S36.
18. Ferrer 1, Cusi MV, Liarte A, Campistol J. A Golgi study of the polymicrogyric cortex in Aicardi syndrome. Brain Dev 1986;8:518-25.
19. Baieari P, Marki A, Thelen M, Laub MC. MR imaging in Aicardi,s syndrome. Am J Neuroradiol 1988;9:805-6.
20. Roland EH, Flodmark 0, Hill A. Neurosonographic features of Aicardi syndrome. J Child Neurol 1989;4:307-10.
21. Hamano K, Matsubara T, Shibata S, et al. Aicardi syndrome accompanied by auditory disturbances and multiple brain tumors. Brain Dev 199 1; 13:438- 41.
22. Tanaka T, Takahura H, Takashima S, Kodama T, Hasegawa H. A rare case of Aicardi syndrome with severe brain malformation and hepatoblastoma. Brain Dev 1985;7:507-12.
23. Togawa T, Mimaki T, Ono J. Aicardi syndrome associated with embryonal carcinoma. Pediatr Neural 1989;5:45-7.
24. Brihaye L, Gillet P, Parmentier R, Peetrons A. Agenesie de la commissure calleuse associee A un kyste dpendymaire. Arch Suisses Neurol Psychi- atr 1956;77:415-31.
25. Barkovich A, Norman D. Anomalies of the corpus callosum: correlation with further anomalies of the brain. Am J Neuroradiol 1988;9:493-501.
26. Hopkins IJ, Humphrey 1, Keith CG, Susman M, Webb GC, Turner EK. The Aicardi syndrome in a 47XXY male. Aust Paediatr J 1979;15:278-80.
27. Curatolo P, Libutti G, Dalla Piccola B. Aicardi syndrome in a male infant. J Pediatr 1980;96: 286-7.
28. Aicardi J. The Aicardi syndrome in a male infant [Letter]. J Pediatr 1980;97:1040-41.
29. Hunter AGW. Aicardi syndrome in a male infant [Reply]. J Pediatr 1980;97:1041.
30. Costa T, Greer W, Duckworth M, Rysiecki M, Musarella M, Ray P. Monozygotic twins discordant for Aicardi syndrome [Abstract]. Am J Hum Genet 1990;47(suppl 5)202:14.
31. Neidich JA, Nussbaum RL, Packer RJ, Emanuel BS, Puck JM. Heterogeneity of clinical severity and molecular lesions in Aicardi syndrome. J Pediatr 1990; 1 16:911-7.
32. Wieacker P, Zimmer J, Ropeers HH. X-inactivation pattern in two syndromes with probable X-linked dominant, male lethal inheritance. Clin Genet 1985;28:238-42.
33. Ropers HH, Zuffardi 0, Biancai E, Tiepolo L. Agenesis of corpus callosum, ocular and skeletal anomalies (X-linked dominant Aicardi's syndrome) in a girl with balanced X/3 translocation. Hum Genet 1982;61:364-8.
34. Donnenfeld AE, Graham JM, Packer RJ, Aquino R, Berg SZ, Emanuel BS. Microphthalmia and chorioretinal lesions in a girl

with an Xp22.2 pter deletion and partial 3p trisomy: clinical observations relevant to Aicardi syndrome gene localization. Am J Med Genet 1990;37:182-6.
35. Al-Gazali LI, Muller RF, Caine A, et al. An XX male and two (X;Y) females with linear skin defects and congenital microphthalmia: a new syndrome at Xp22.3. J Med Genet 1988;25:638-9.
36. Friedman PA, Rao KW, Jeplin SW, Aylsworth AS. Provisional deletion mapping of the focal dermal hypoplasia (FDH) gene to Xp22.31 [Abstract]. Am J Hum Genet 1988;43:A50.
32- Metwally, MYM: Textbook of neuroimaging, A CD-ROM publication, (Metwally, MYM editor) WEB-CD agency for electronic publication, version 9.4a October 2008