CARCINOMA BASE OF TONGUE
CARCINOMA BASE OF TONGUE
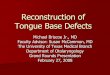
ANATOMYBase of tongue Posterior 1/3 rd tongue
Boundaries
- Anterior: Circumvallate papillae - Lateral : Glossotonsillar
sulci - Posterior : Epiglottis - Superior : Soft palate - Inferior
: Hyoid and epiglottis
Vallecula Transition zone between base of tongue and
epiglottis
Muscles : Genioglossus, Styloglossus, Hyoglossus and
Palatoglossus
Sensory supply : Glossopharyngeal nerve (IX)
Motor supply: Hypoglossal nerve except for the palatoglossal
muscle supplied by the Pharyngeal branch of the vagusArterial
supply: Lingual artery
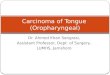
Lymphatic drainage:
Primary drainage Level II (Jugulodigastric nodes)Also to
retropharyngeal and parapharyngeal nodesRetropharygeal is divided
into lateral (Rouviers) and medial nodesParapharyngeal nodes are
called junctional nodes as it occurs on the junction of the spinal
accessory (level V) and upper internal jugular lymphatic chains
Risk FactorsTobacco AlcoholHPVGarnaes et al, attributed a rise
in eastern Denmark in the incidence of squamous cell carcinomas of
the base of the tongue between 2000 and 2010 (by 5.4% per year) to
an increase in the number of such tumors (by 8.1% per year) that
were positive for human papillomavirus.MarijuanaEnvironmental
exposure to PAH, asbestos
Clinical PresentationDysphagiaOdynophagiaSensation of mass in
the throatMass/Node in the neckReferred pain to the
earHemoptysis
ROUTES OF SPREADLocal: spreads to rest of tongue musculature,
epiglottis, pre - epiglottic space, tonsils, faucial pillars,
hypopharynx
Lymphatic: Unilateral or bilateral cervical node metastasis in
majority of cases. Distant: Lungs, liver , bone
DIAGNOSISRoutine blood investigations( CBC, LFT, RFT)Palpation
under anaesthesiaFlexible fibreoptic laryngoscopyChest Xray:
Pulmonary metastasis or 2nd primaryCT : Bone invasion and occult
nodal disease in the neckPET-CT: Disease recurrence/ persistence
after RT and distant metastasisMRI : Soft tissue extension and
perineural spreadFNAC of neck nodesBiopsy of the primary lesion
HISTOLOGYMajority squamous cell carcinomasRest are Minor
salivary gland tumours - Mucoepidermoid carcinoma - Adenoid
carcinoma - Adenoid cystic carcinoma - Clear cell carcinoma
STAGINGPrimary tumour (T)T1: Tumor 2 cm or less in greatest
dimension T2: Tumor more than 2 cm but not more than 4 cm in
greatest dimension
T3: Tumor more than 4 cm in greatest dimension or extension to
lingual surface of epiglottis
T4a: Moderately advanced local disease. Tumor invades the
larynx, extrinsic muscle of tongue, medial pterygoid, hard palate,
or mandible
T4b: Very advanced local disease. Tumor invades lateral
pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull
base or encases carotid arter
Regional lymph nodes (N)NX: Regional lymph nodes cannot be
assessed N0; No regional lymph node metastasisN1: Metastasis in a
single ipsilateral lymph node, 3 cm or less in greatest
dimension
N2a: Metastasis in a single ipsilateral lymph node, more than 3
cm but not more than 6 cm in greatest dimension N2b: Metastasis in
multiple ipsilateral lymph nodes, not more than 6 cm in greatest
dimension N2c: Metastasis in bilateral or contralateral lymph
nodes, not more than 6 cm in greatest dimensionN3: Metastasis in a
lymph node, more than 6 cm in greatest dimension
Distant metastasis (M) M0: No distant metastasis M1: Distant
metastasis
STAGETNMSTAGE IT1NOMOSTAGE IIT2NOMOSTAGE
IIIT3NOMOT1/T2/T3N1MOSTAGE IVAT4aNO/N1MOT1/T2/T3N2MOSTAGE IVBAny
TN3M0T4bAny NMOSTAGE IVCAny TAny NM1
TREATMENT MODALITIESSurgery As single modality orRadiotherapy in
combination
Chemotherapy - Induction CT - Concurrent chemo RT Sequential
(ICT concurrent CRT) postoperative adjuvant concurrent chemoRT
Targeted therapy- Alone or combined with RT or palliative CT
GENERAL PRINCIPLES OF TREATMENTStage I and II Early stage
disease Stage III and IV Locoregionally advanced disease
Early stage disease Surgery or RT Locoregionally advanced
diseaseSurgery followed by RT +/- chemotherapyRT + chemotherapy
Recurrent / metastatic disease - Chemotherapy - Palliative or
supportive care
18
SURGERYLimited role due to inherent morbidity of a near total or
total glossectomy needed for large midline tumours
Well lateralized tumours with minimal cervical lymphadenopathy
Partial glossectomy
B/L cervical lymph node dissection is done always due to high
propensity for occult microscopic nodal involvment
Tumours arising from vallecula which are in close proximity to
larynx Supraglottic or total laryngectomy
Surgical approachesMidline mandibulotomy- Splitting the lip,
madible and oral tongue midlineLateral mandibulotomy - Dividing the
mandible near the angle and approaching the base of tongue from the
sideFloor drop procedure - Elevating the inner periosteum from the
mandible from angle to angle which releases the entire floor of
mouth and oral tongue into the neck exposing the base of
tongueTransoral approaches - Laser surgery - Robotic surgery
Radiotherapy BrachytherapyEBRT
BrachytherapyIndicationGiven as boost following EBRT Pre
treatment tumour extent should be delineated before EBRT because
regression is not always uniformContraindication:- Distant
metastasis- Tumors very close to or involving bonePt not suitable
for anesthesia
TechniqueClassical Plastic loop techniqueAdvantages:This allows
a wider separation between the sources - can be used to treat
larger volumes. Remote after-loading that reduces the risk of
exposureIn case of local oedema inducing the risk of displacement
of the plastic tubes, one can wait for an acceptable local status
before loading the iridium wire.Self retaining assembly, no
suturing required
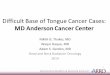
Done under general anesthesiaThe loop is formed by passing a
hollow stainless steel needle through the skin into the tongue. A
parallel stainless steel needle forms the other limb of the loop.A
nylon guide wire is introduced to form the loopThe stainless steel
needles are then removed.The plastic tube that has to be implanted
is tied to guide wire and pulled through, ultimately forming the
loop.Plastic or Lead button are introduced at skin end of tube to
fix it.
On completion of the implant orthogonal radiographs are taken to
show the position of the plastic tube loops.GTV is defined.CTV is
drawn giving a margin of 1-1.5 cmPTV is same as the CTVBasal dose
between the sources calculated.Mean basal dose calculated from
basal dose.85% isodose volume of mean basal dose should ideally
cover the PTV( reference volume) and get the prescribed dose for
adequate tumor control
Brachytherapy guidelinesABS guidelinesEBRT of 45 to 60 Gy
followed by HDR boost of 3-4 Gy per fraction for 6 to 10 doses
GEC and ESTRO guidelinesEBRT of 45 to 50 Gy followed by HDR
boost of 30 to 35 Gy
EBRTIndication - Sole modality in early stage tumours - Adjuvant
to surgery - Concurrent chemotherapy - Palliative EBRT
EBRTRadiotherapy Simulation CT based with IV contrast - Patients
are positioned supine with a rigid head holder - Extended head
position is used - Shoulder traction to position it as caudally as
possible to allow adequate neck exposure - Tongue immobilization -
Bite blocks - Head immobilized with a tight thermoplastic mask -
Images are taken from the calvarium to carina
Conventional techniqueIrradiation portals should encompass the
primary tumor and its local and regional extensions, with a margin
for the CTV (approximately 0.7 cm) and for the PTV(approximately
0.5 cm).Neck portals should extend superiorly until C1 for N0, and
the base of skull (retrostyloid space) in case of N+ diseaseThe
primary tumor and both sides of the upper neck are irradiated using
a conventional lateral parallel-opposed technique for the upper
neck in case of a T2N2b BOT tumor. Both sides of the lower neck are
generally irradiated through a single anteroposterior field,
sometimes with a midline block.
Standard beam arrangments (3DCRT) - Parallel opposed lateral
upper fields - Low neck/Supraclavicular field treated with single
anterior or AP-PA fields
DEFINITIVE RT
High risk - 66 to 70 Gy/ 35F/ 7 weeksConcomitant boost
accelerated RT - 72 Gy /6 weeks( 1.8Gy/F for large field; 1.5 Gy
boost as second daily fraction during the last 12 treatment
days)Hyperfractionation - 81.6 Gy/7 weeks(1.2 Gy/F twice daily)Low
risk - 44 to 50 Gy/ 25F/5 weeks
DOSE CONSTRAINTSTemporal lobe: < 60 GyOptic nerve and chiasma
: < 50 GyBrainstem : < 54 GySpinal cord :< 45 GyMandible
:< 70 GyParotid gland :