Embed Size (px)
Citation preview
TRANSHYOID APPROACH IN SURGERY OF TONGUEBASE NEOPLASMS
INTRODUCTION
Tongue base neoplasms are characterized in generally
by a bad prognosis (1, 2).
This situation is the result of late presentation to the
specialist and of the difficulties often encountered in
correct diagnostication of this disease.
Early simptomatology is poor, advanced stages being
almost constantly characterised by the presence of
adenopaty.
The principles of treatment suffered many
transformations and readaptations in last decades, even
today still being characterized by heterogenity of
therapeutic models used in different institutions world
wide.
Traditional methods include unimodal treatment,
consisting of surgery or radiation therapy alone, and
combined treatment which uses the combination
between these two methods.
34
Journal of Experimental Medical & Surgical Research
Cercetãri Experimentale & Medico-Chirurgicale
Year XVIII · Nr.1/2011 · Pag. 34 - 38E x p e r i m e n t a l
M e d i c a l S u r g i c a l
R E S E A R C H
J O U R N A L o f
Correspondence to: R.D. Cristescu, Clinica ORL Timiºoara, Bd. Revolutiei 6, 300054 Timisoara, email: [email protected].
SUMMARY: The treatment of tongue base neoplasms is evolving continuously, remainingcontroversial in the same time, as it was 25 years ago.From the variety of technicues utilized in tongue base tumor surgery, tumor resection usingtranshyoid approach provides similar oncologic results with other surgical technicues ,having the advantage of superior functional results.A retrospective study was conducted on 35 patients treated surgically for tongue baseneoplasms in ENT Department Timisoara between 1998 and 2010.All cases were stadialised according to the UICC. Four patients wee classified in stage II, 12 patients in stage III and 19 patients in stage IV.Most common histological type encountered was the squamous cell carcinoma.Tumor resection was performed using the transhyoid approach in all cases.Surgical treatment remains an useful alternative in tongue base cancer therapy, offeringexcellet results especially when associated with adjuvant therapies.Keywords: tongue base, neoplasms, transhyoid approach.
Rezumat: Tratamentul neoplasmelor bazei de limba evolueaza continuu, ramanand inacelasi timp controversat, la fel ca si in urma cu 25 ani.In cadrul diverselor tehnici chirurgicale destinate acestei patologii, metoda aborduluitranshioidian ofera rezultate oncologice similare celorlalte tehnici, detinand avantajul unorrezultate functionale superioare.A fost realizat un studiu retrospectiv pe 35 pacienti tratati chirurgical pentru neoplasme alebazei de limba in Clinica O.R.L. Timisoara intre anii 1998 - 2010.Cazurile au fost stadializate conform sistemului UICC de stadializare.Patru pacienti au fostincadrati in stadiul II, 12 pacienti in stadiul III si 19 pacienti in stadiul IV.Cel mai frecvent diagnostic histopatologic a fost carcinomul scuamocelular.S- a realizat rezectia tumorala prin abord transhioidian in toate cazurile.Tratamentul chirurgical ramane in continuare o alternativa eficienta in tratamentulneoplaziilor bazei limbii, oferind rezultate excelente atunci cand este utilizat in asociere cucelelalte metode terapeutice.Cuvinte cheie: baza limbii, neoplasme, abord transhioidian..
R.D. Cristescu1 , S. Cotulbea1, S. Lupescu1, A. H. Marin1,G. Iovanescu1, V. Draganescu1,H. Stefanescu1,C. Doros1,N. Balica1,Anamaria Mag1, Andreea Ruja2
Received for publication: 11.11.2010
Revised: 08.01.2012
1. - Clinica ORL Timisoara-Universitatea de Medicina si Farmacie "Victor Babes" 2. - Clinica de Odontoterapie si Endodontie-Facultatea de Medicina Dentara
Recently, combining radiotherapy with chemotherapy
in various radiochemotherapic protocols ,is gaining
popularity as a preffered option of treatment, due to the
advantage of superior preservation for organs and their
functions, but prohibitive prices are still limiting their use
on a large scale.
The selection of adequate therapy for these patients
depends on the stage of the disease, type of tumour and
the associated comorbidities.
For tumours in early stages (T1), radiotherapy is the
treatment of first choice because of its excellent
therapeutic results combined with minimal added
morbidity.
More advanced stages (T2,T3,T4) need combined
treatment, represented by surgery and postoperative
radiotherapy, associated or not with chemotherapy.
Among various techniques used in the surgery of
tongue base neoplasms, tumor resection using the
transhyoid approach offers certain advantages, making
this technique very useful ,especially when combinated
with radiation therapy.
This study presents the experience of the ENT
Department Timisoara in the treatment of tongue base
neoplasms using the transhyoid approach.
MATERIALS AND METHODS
A retrospective chart review was performed in 35
patients who were surgically treated for tongue base
neoplasms at the ENT Department of Timisoara between
1998 and 2010.
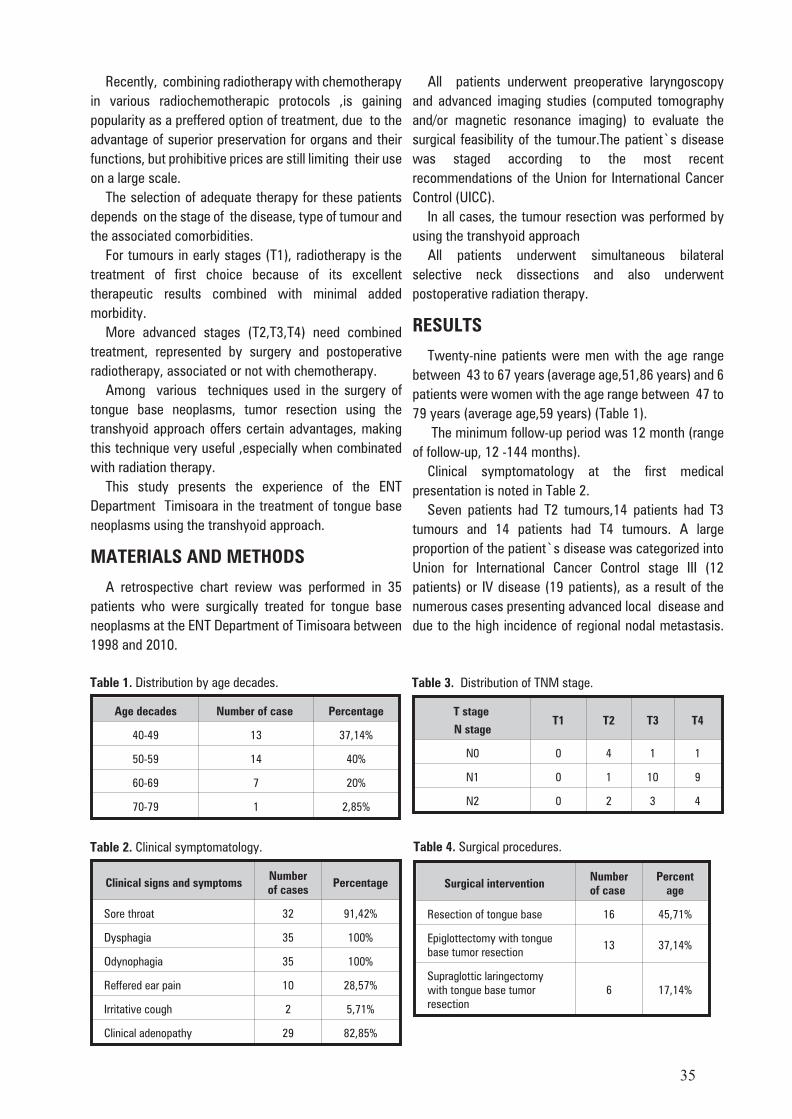
All patients underwent preoperative laryngoscopy
and advanced imaging studies (computed tomography
and/or magnetic resonance imaging) to evaluate the
surgical feasibility of the tumour.The patient`s disease
was staged according to the most recent
recommendations of the Union for International Cancer
Control (UICC).
In all cases, the tumour resection was performed by
using the transhyoid approach
All patients underwent simultaneous bilateral
selective neck dissections and also underwent
postoperative radiation therapy.
RESULTS
Twenty-nine patients were men with the age range
between 43 to 67 years (average age,51,86 years) and 6
patients were women with the age range between 47 to
79 years (average age,59 years) (Table 1).
The minimum follow-up period was 12 month (range
of follow-up, 12 -144 months).
Clinical symptomatology at the first medical
presentation is noted in Table 2.
Seven patients had T2 tumours,14 patients had T3
tumours and 14 patients had T4 tumours. A large
proportion of the patient`s disease was categorized into
Union for International Cancer Control stage III (12
patients) or IV disease (19 patients), as a result of the
numerous cases presenting advanced local disease and
due to the high incidence of regional nodal metastasis.
35
Age decades Number of case Percentage
40-49 13 37,14%
50-59 14 40%
60-69 7 20%
70-79 1 2,85%
Table 1. Distribution by age decades.
Clinical signs and symptomsNumberof cases
Percentage
Sore throat 32 91,42%
Dysphagia 35 100%
Odynophagia 35 100%
Reffered ear pain 10 28,57%
Irritative cough 2 5,71%
Clinical adenopathy 29 82,85%
Table 2. Clinical symptomatology.
T stage
N stageT1 T2 T3 T4
N0 0 4 1 1
N1 0 1 10 9
N2 0 2 3 4
Table 3. Distribution of TNM stage.
Surgical intervention Numberof case
Percentage
Resection of tongue base 16 45,71%
Epiglottectomy with tongue base tumor resection
13 37,14%
Supraglottic laringectomywith tongue base tumorresection
6 17,14%
Table 4. Surgical procedures.
Only 4 patients were categorized as stage II and no
patient`s disease was categorized as stage I (Table 3).
All interventions were performed under general
anesthesia.Tracheotomy was done in all cases, either
preoperatively or intraoperatively.
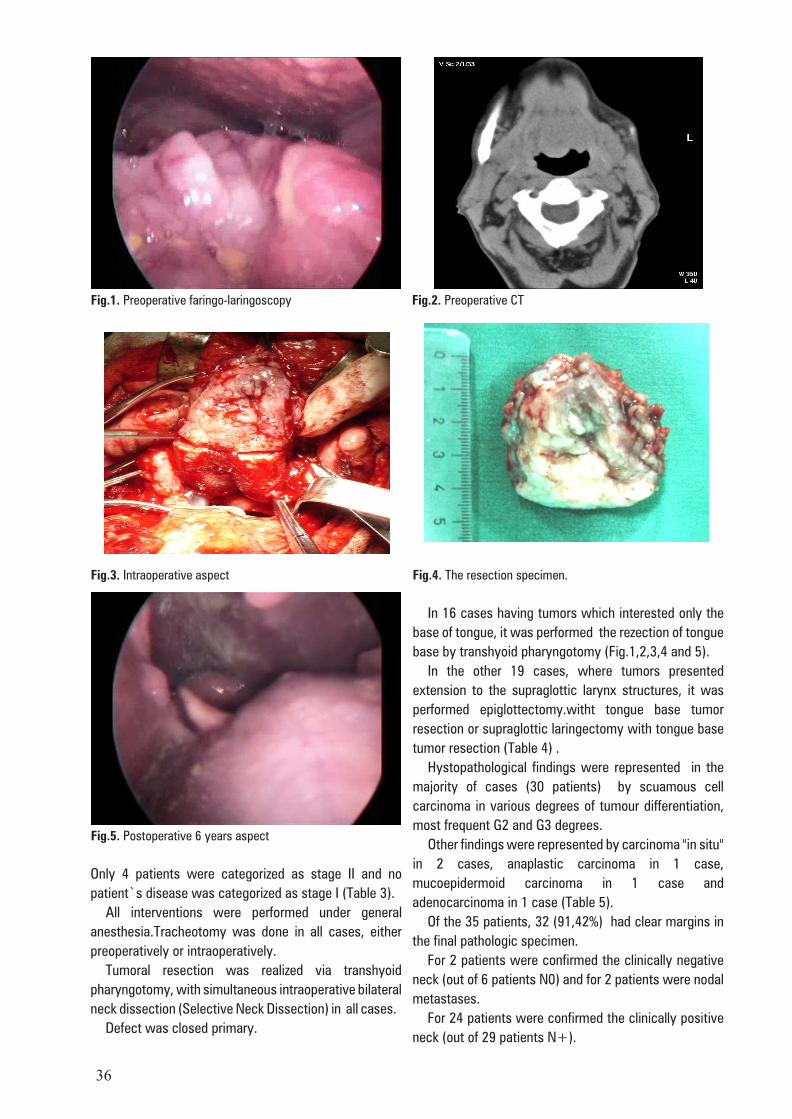
Tumoral resection was realized via transhyoid
pharyngotomy, with simultaneous intraoperative bilateral
neck dissection (Selective Neck Dissection) in all cases.
Defect was closed primary.
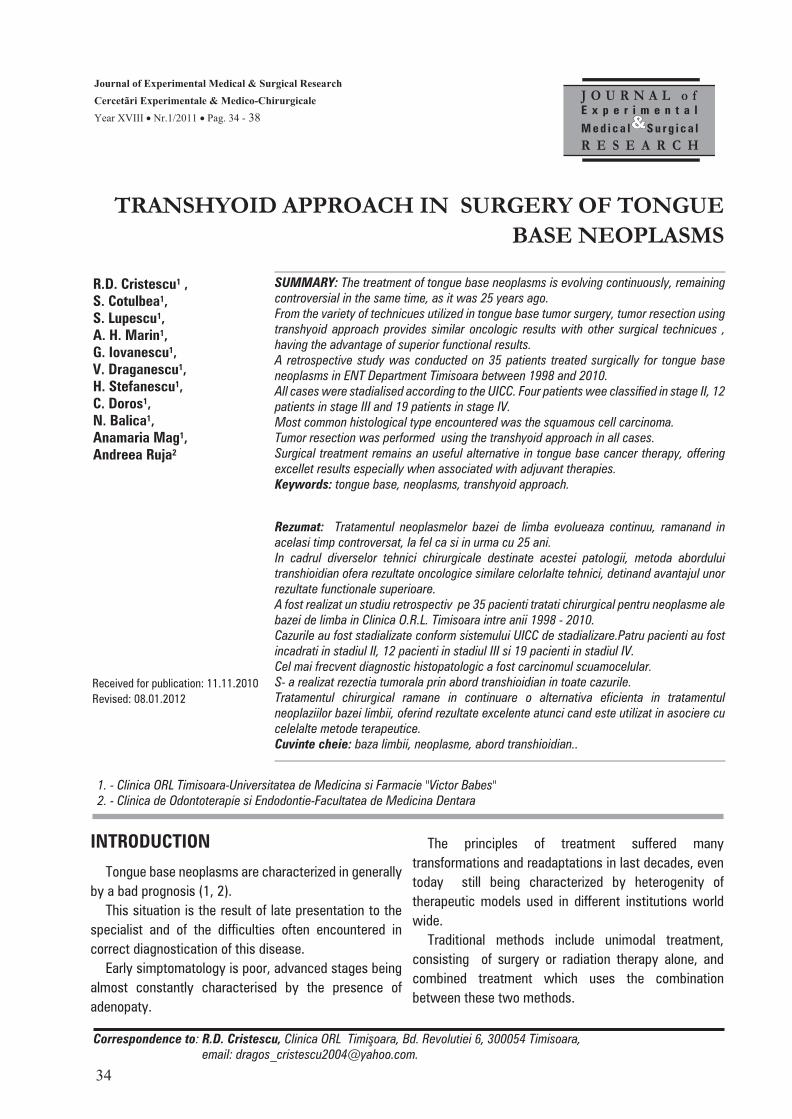
In 16 cases having tumors which interested only the
base of tongue, it was performed the rezection of tongue
base by transhyoid pharyngotomy (Fig.1,2,3,4 and 5).
In the other 19 cases, where tumors presented
extension to the supraglottic larynx structures, it was
performed epiglottectomy.witht tongue base tumor
resection or supraglottic laringectomy with tongue base
tumor resection (Table 4) .
Hystopathological findings were represented in the
majority of cases (30 patients) by scuamous cell
carcinoma in various degrees of tumour differentiation,
most frequent G2 and G3 degrees.
Other findings were represented by carcinoma "in situ"
in 2 cases, anaplastic carcinoma in 1 case,
mucoepidermoid carcinoma in 1 case and
adenocarcinoma in 1 case (Table 5).
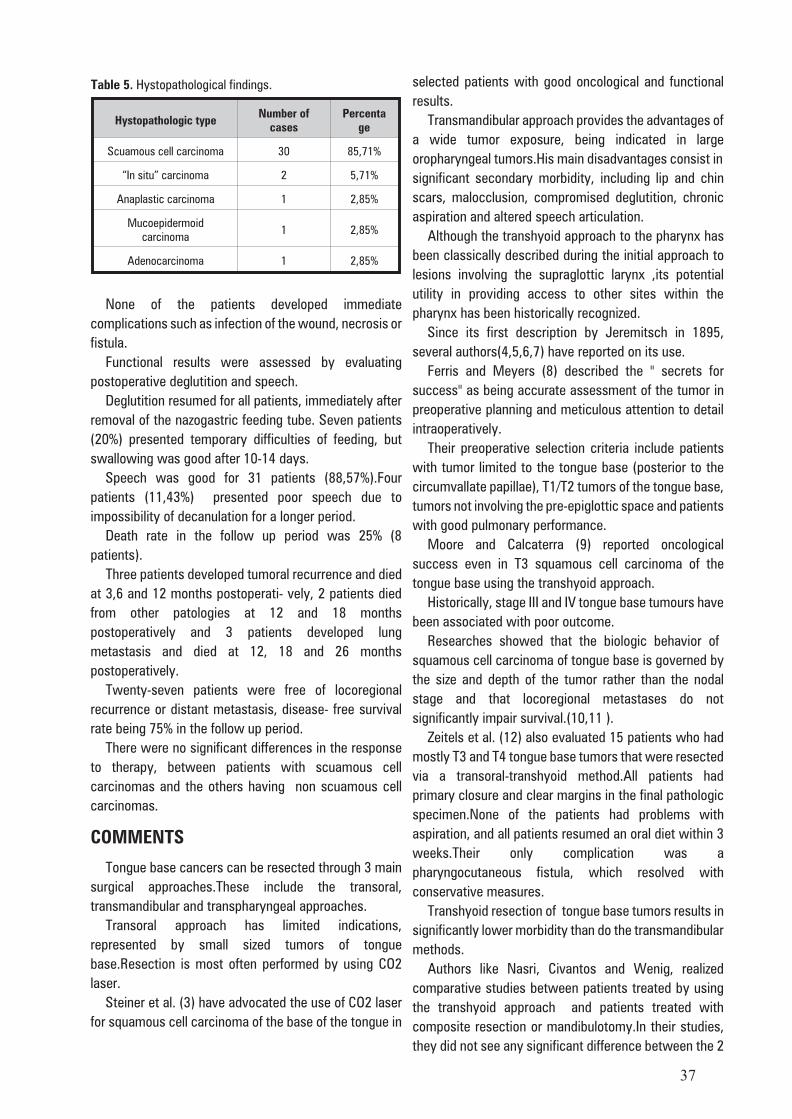
Of the 35 patients, 32 (91,42%) had clear margins in
the final pathologic specimen.
For 2 patients were confirmed the clinically negative
neck (out of 6 patients N0) and for 2 patients were nodal
metastases.
For 24 patients were confirmed the clinically positive
neck (out of 29 patients N+).
36
Fig.1. Preoperative faringo-laringoscopy
Fig.2. Preoperative CT
Fig.4. The resection specimen.
Fig.3. Intraoperative aspect
Fig.5. Postoperative 6 years aspect
None of the patients developed immediate
complications such as infection of the wound, necrosis or
fistula.
Functional results were assessed by evaluating
postoperative deglutition and speech.
Deglutition resumed for all patients, immediately after
removal of the nazogastric feeding tube. Seven patients
(20%) presented temporary difficulties of feeding, but
swallowing was good after 10-14 days.
Speech was good for 31 patients (88,57%).Four
patients (11,43%) presented poor speech due to
impossibility of decanulation for a longer period.
Death rate in the follow up period was 25% (8
patients).
Three patients developed tumoral recurrence and died
at 3,6 and 12 months postoperati- vely, 2 patients died
from other patologies at 12 and 18 months
postoperatively and 3 patients developed lung
metastasis and died at 12, 18 and 26 months
postoperatively.
Twenty-seven patients were free of locoregional
recurrence or distant metastasis, disease- free survival
rate being 75% in the follow up period.
There were no significant differences in the response
to therapy, between patients with scuamous cell
carcinomas and the others having non scuamous cell
carcinomas.
COMMENTS
Tongue base cancers can be resected through 3 main
surgical approaches.These include the transoral,
transmandibular and transpharyngeal approaches.
Transoral approach has limited indications,
represented by small sized tumors of tongue
base.Resection is most often performed by using CO2
laser.
Steiner et al. (3) have advocated the use of CO2 laser
for squamous cell carcinoma of the base of the tongue in
selected patients with good oncological and functional
results.
Transmandibular approach provides the advantages of
a wide tumor exposure, being indicated in large
oropharyngeal tumors.His main disadvantages consist in
significant secondary morbidity, including lip and chin
scars, malocclusion, compromised deglutition, chronic
aspiration and altered speech articulation.
Although the transhyoid approach to the pharynx has
been classically described during the initial approach to
lesions involving the supraglottic larynx ,its potential
utility in providing access to other sites within the
pharynx has been historically recognized.
Since its first description by Jeremitsch in 1895,
several authors(4,5,6,7) have reported on its use.
Ferris and Meyers (8) described the " secrets for
success" as being accurate assessment of the tumor in
preoperative planning and meticulous attention to detail
intraoperatively.
Their preoperative selection criteria include patients
with tumor limited to the tongue base (posterior to the
circumvallate papillae), T1/T2 tumors of the tongue base,
tumors not involving the pre-epiglottic space and patients
with good pulmonary performance.
Moore and Calcaterra (9) reported oncological
success even in T3 squamous cell carcinoma of the
tongue base using the transhyoid approach.
Historically, stage III and IV tongue base tumours have
been associated with poor outcome.
Researches showed that the biologic behavior of
squamous cell carcinoma of tongue base is governed by
the size and depth of the tumor rather than the nodal
stage and that locoregional metastases do not
significantly impair survival.(10,11 ).
Zeitels et al. (12) also evaluated 15 patients who had
mostly T3 and T4 tongue base tumors that were resected
via a transoral-transhyoid method.All patients had
primary closure and clear margins in the final pathologic
specimen.None of the patients had problems with
aspiration, and all patients resumed an oral diet within 3
weeks.Their only complication was a
pharyngocutaneous fistula, which resolved with
conservative measures.
Transhyoid resection of tongue base tumors results in
significantly lower morbidity than do the transmandibular
methods.
Authors like Nasri, Civantos and Wenig, realized
comparative studies between patients treated by using
the transhyoid approach and patients treated with
composite resection or mandibulotomy.In their studies,
they did not see any significant difference between the 2
37
Hystopathologic typeNumber of
casesPercenta
ge
Scuamous cell carcinoma 30 85,71%
“In situ” carcinoma 2 5,71%
Anaplastic carcinoma 1 2,85%
Mucoepidermoidcarcinoma
1 2,85%
Adenocarcinoma 1 2,85%
Table 5. Hystopathological findings.
groups in disease-free survival, status of surgical
margins, recurrences, or complications.However , they
did observed significantly superior postoperative speech
and swallowing function in the transhyoid group.
Association of postoperative radiation therapy to the
surgical resection improves substantially the rates of
local control in these cases (13,14).
CONCLUSIONS
Among various techniques used in the surgery of
tongue base neoplasms, tumor resection using the
transhyoid approach offers the advantages of an
excellent tumor exposure, low postoperative morbidity,
and local control rates similar to the other techniques.
The advantages of the transhyoid approach to the
neoplasms of tongue base in conjunction with neck
dissection and postoperative radiation therapy, include
excellent long- term patient survival, improved
swallowing and speech function, outstanding tumor
exposure, and minimal cosmetic deformity.
38
References:1. Alvi A, J. Johnson.Development of distant metastasis after treatment of advanced-stage head and neck cancer.Head Neck
1997;19:500-505.2. American Joint Committee on Cancer (including base of tongue, soft palate, and uvula). In: AJCC Cancer Staging Atlas. Greene, F,
Compton, C, Fritz, A, Shah, J, Winchester D, editors. New York ; Springer; 2006: 27-40.3. Steiner W, Fierek O, Ambrosch P, Hommerisch CP, Kron M.Transoral laser microsurgery for squamous cell carcinoma of the base
of tongue. Arch Otolaryngol Head and Neck Surg 2003; 129(1):36-43.4. Nasri S, Oh Y, Calcaterra TC. Transpharyngeal approach to the base of tongue tumors: a comparative study. Laryngoscope
1996;106: 945-950.5. Metternich FU, Puder C, Brusis T. Suprahyoid pharyngotomy for surgical therapy of malignant and benign oral and
hypopharyngeal tumors.HNO 1996; 44:242-245.6. Schechter GL, Sly DE, Roper AL, et al.Set-back tongue flap for carcinoma of the tongue base. Arch Otolaryngol. 1980;
106:6680671.7. Weber PC, Johnson JT, Meyers EN. The suprahyoid approach for squamous cell carcinoma of the base of the tongue.
Laryngoscope. 1992;102:637-640.8. Ferris FL, Meyers RN. Suprahyoid pharyngotomy. Operatives technicues in Otolaryngology. Head and Neck Surgery 2005;
16(1):49-54.9. Moore DM, Calcaterra TC. Cancer of the tongue base treated by a transpharyngeal approach.Ann Otol Rhinol Laryngol
1990;9:300-303.10. Freeman DE, Mendenhall WM, Parsons JT, Million RR.Does neck stage influence local control in squamous cell carcinoma of the
head and neck ? Int J Radiat Oncol Biol Phys. 1992; 23: 733-736.11. Richard JM, Sancho-Garnier H, Micheau C, Saravane D, Cachin Y. Prognostic factors in cervical lymph node metastasis in upper
respiratory and digestive tract carcinomas: study of 1,713 cases during a 15-year period. Laryngoscope. 1987; 97: 97-101.12. Zeitels SM, Vaughan CW, Ruh S.Suprahyoid pharyngotomy for oropharynx cancer including the tongue base. Arch Otolaryngol
Head Neck Surg. 1991;117:757-760.13. Nisi K, et al. Adjuvant radiotherapy for squamous cell carcinoma of the tongue base: improved local-regional disease control
compared with surgery alone.International J Radiat Oncol Biol Phys 1998; 41:371-377.14. Weber P, Myers E, Johnson J.Squamous cell carcinoma of the base of tongue. Eur Arch Oto-rhino-laryngol 1993; 250:63-68.





























