Embed Size (px)
DESCRIPTION
Blood respiratory function & jaundice
Citation preview

Biochemistry of blood. Respiratory function of erythrocytes. Pathobiochemistry of blood.

Red Blood Cells (erythrocytes)
The most numerous type in the blood.
•Features:•The erythrocytes doesn’t contain nucleus, chromatine•The erythrocytes doesn’t contain mytochondrias, thus АТP producing due to the anaerobic glycolisis till to the lactate (90%).•The glycolisis has features. During it the 2,3 BPG will be produced, not 1,3 BPG. This compound need for joining О2 to hemoglobin: low concentration of 2,3 BPG will increase the affinity hemoglobin (Нв) to О2.• The PPP is the main path for producing of reductive equivalents NADPН2 for taking part in glycolisis

Red blood cells are responsible for the
transport of oxygen and carbon dioxide. In adult humans the
hemoglobin (Hb) molecule consists of four polypeptides: two alpha (α) chains of
141 amino acids and two beta (β) chains of 146
amino acids Each of these is attached the
prosthetic group heme. There is one atom of iron at
the center of each heme. One molecule of oxygen can
bind to each heme. The reaction is reversible.

Transport of oxygen by hemoglobinHemoglobin has all the requirements of an ideal respiratory pigment:-It can transport large quantities of oxygen.-It has great solubility.-It can take up and release oxygen at appropriate partial pressures.-It is a powerful buffer.

Oxygenation and oxidation• When hemoglobin carries oxygen, the Hb is
oxygenated. The iron atom in Hb is still in the ferrous state.
• Oxidized hemoglobin is called Met-Hb; then iron is in ferric state and the oxygen carrying capacity is lost.

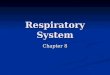
Oxygen Dissociation Curve (ODC)• The ability of hemoglobin to load and unload
oxygen at physiological pO2 (partial pressure of oxygen).
• At the oxygen tension in the pulmonary alveoli, the Hb is 97% saturated with oxygen. Normal blood with 15mg/dl of Hb can carry 20ml of O2/dl of blood.
• In the tissue capillaries, where the pO2 is only 40mm of Hg, the Hb is about 60% saturated. So physiologically, 40% of oxygen is released.


H+, CO2, BPG
Hb Equilibrium
b
b a
a
R (high affinity)
O2
T(low affinity)

Cooperativity
Oxygen binding to one subunit of Hb, increases the affinity of the other subunits for additional oxygens. In other words, the first one is the hardest, the rest are easy.
Anaemia Anaemia is a shortage of RBCs and/or the
amount of haemoglobin in them.

Carbon Dioxide Transport

Carbon dioxide (CO2) combines with water forming carbonic acid, which dissociates into a hydrogen ion (H+) and a bicarbonate ions:
CO2 + H2O ↔ H2CO3 ↔ H+ + HCO3− 95% of the CO2 generated in the tissues is carried in
the red blood cells: It probably enters (and leaves) the cell by diffusing
through transmembrane channels in the plasma membrane. (One of the proteins that forms the channel is the D antigen that is the most important factor in the Rh system of blood groups.)
Once inside, about one-half of the CO2 is directly bound to hemoglobin (at a site different from the one that binds oxygen).

The rest is converted — following the equation above — by the enzyme carbonic anhydrase into bicarbonate ions that diffuse back out into the plasma
and hydrogen ions (H+) that bind to the protein portion of
the hemoglobin (thus having no effect on pH).
Only about 5% of the CO2 generated in the tissues dissolves directly in the plasma.
When the red cells reach the lungs, these reactions are reversed and CO2 is released to the air of the alveoli.


The ability of hemoglobin to release oxygen, is affected by pH, CO2 and by the differences in the oxygen-rich environment of the lungs and the oxygen-poor environment of the tissues. The pH in the tissues is considerably lower (more acidic) than in the lungs. Protons are generated from the reaction between carbon dioxide and water to form bicarbonate: CO2 + H20 -----------------> HCO3- + H+This increased acidity serves a two fold purpose. - First, protons are lower the affinity of hemoglobin for oxygen,
allowing easier release into the tissues. As all four oxygens are released, hemoglobin binds to two protons. This helps to maintain equilibrium towards the right side of the equation. This is known as the Bohr effect, and is vital in the removal of carbon dioxide as waste because CO2 is insoluble in the bloodstream. The bicarbonate ion is much more soluble, and can thereby be transported back to the lungs after being bound to hemoglobin.
- If hemoglobin couldn’t absorb the excess protons, the equilibrium would shift to the left, and carbon dioxide couldn’t be removed

Bohr Effect (pH)
100 mm O2
20 mm O2

In the lungs, this effect works in the reverse direction. In the presence of the high oxygen concentration in the lungs, lead to the proton affinity decreasing. As protons are shed, the reaction is driven to the left, and CO2 forms as an insoluble gas to be expelled from the lungs. The proton poor hemoglobin now has a greater affinity for oxygen, and the cycle continues.


CO2 effect
20 mm CO2
80 mm CO2

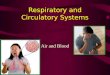
Effect of BPGBPGEffect
pO2 (mm Hg)
0 20 40 60 80 100 120 140 160
0
20
40
60
80
100
pO2 vs p50=8pO2 vs p50=26
Hb alone
Hb + BPG
BPG is the main player in Hb cooperativity.
High altitude increases BPG, pushing curve further to right

Myoglobin and Hemoglobin
Mb is monomer, Hb is a tetramer (ex. a2b2). Hb subunits are structurally similar to Mb, with 8
a-helical regions, no b-strands and no interior water.
Both contain one heme prosthetic group per chain.
Both Mb and Hb contain proximal and distal histidines.
Affinity of Mb for oxygen is high, affinity of Hb for oxygen is lower and more variable.

The iron atom may either be in the Fe2+ or Fe3+ state, but ferrihemoglobin (methemoglobin) (Fe3+) cannot bind oxygen. In binding, oxygen temporarily oxidizes Fe to (Fe3+), so iron must exist in the +2 oxidation state in order to bind oxygen. The body reactivates hemoglobin found in the inactive (Fe3+) state by reducing the iron center.


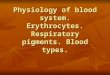
Sickle cell hemoglobin (HbS)
G lu-
G lu-
H b A 1
G lu-
H b S (h e te ro z y g o u s)S ic k le ce ll tra it
H b S (h o m o zy g o u s)
S ic k le c e ll d isea se

Polymerization of HbS
Association shown in previous figure is repeated over and over to produce large, rod-like aggregates that bind oxygen poorly and distort shape of erythrocytes.\\

Sickle cell trait is usually asymptomatic, but strenuous exercise at altitude could elicit sickling and destruction of erythrocytes. This lowers serum Hb and hematocrit, while raising Hb breakdown products such as bilirubin, which can accumulate to form gallstones.

a-Thalassemias
Rare, since a-gene is duplicated (four genes per diploid chromosome set).
Usually more severe than b-thalassemia because there is no substitute for b-gene in adults. Almost all b- thalassemias are deletions
In thalassemia intermedia (o/o) - appearance of HbH (4) In thalassemia major (o/oo), Hb Bart’s (4) is predominant (usually lethal). BPG is ineffective in HbH & Hb Bart’s.

Thalassemias
More common, since gene is present in only one copy per chromosome.
Less severe than thalassemia, since chain can effectively substitute in adults.
The chain can also persist into adulthood (HPFH).
In thalassemia major (0/0) excess chains do not form soluble homotetramers.





Plasma Bilirubin• Normal plasma bilirubin level ranges from 0.2-0.8
mg/dl. The unconjugated bilirubin is about 0.2-0.6 mg/dl, while conjugated bilirubin is only 0- 0.2.
• If the level of plasma bilirubin exceeds 1 mg/dl, the condition is called hyperbilirubinemia.
• Levels between 1 and 2 mg/dl are indicative oflatent jaundice.• When the bilirubin level exceeds 2 mg/dl, it diffuses
into tissues producing yellowish discoloration of skin and mucous membrane resulting in jaundice.
• Van den Bergh test is a test for detection ofbilirubin.

Hyperbilribunemias• Depending on the nature of the
bilirubin elevated, the condition may be grouped into conjugated or unconjugated hyperbilirubinemia.
• Based on the cause it may also be classified into congenital and acquired.

1- Congenital Hyperbilirubinemias
• They results from abnormal uptake, conjugation or excretion of bilirubin due to inherited defects.
Crigler-Najjar syndrome: Here the defect is in conjugation. In type 1 (Congenital non-hemolytic jaundice), there is sever
deficiency of UDP glucuronyl transferase. The disease is often fatal and the children die before the age 2. Jaundice usually appears within the first 24 hours of life. Unconjugated bilirubin level increases to more than 20mg/dl, and hence Kernicterus is resulted.

2- Acquired HyperbilirubinemiasPhysiological Jaundice:It is also called as neonatal hyperbilirubinemia.
In all newborn infants after the second day of life, mild jaundice appears.
This transient hyperbilirubinemia is due to an accelerated rate of destruction of RBCs and also because of the immature hepatic system of conjugation of bilirubin.
In such cases, bilirubin does not increase above5mg/dl.It disappears by the second week of life.

3- Hemolytic JaundiceA) Hemolytic Disease of the Newborn:This condition results from incompatibility betweenmaternal and fetal blood groups.Rh+ve fetus may produce antibodies in Rh-ve mother, leading to Rh incompatibility.When blood level of bilirubin is more than 20mg/dl, thecapacity of albumin to bind bilirubin is exceeded.In young children before the age of 1 year, the blood- brain barrier is not fully matured, and therefore free bilirubin enters the brain (Kernicterus).It is deposited in brain, leading to mental retardation.

B) Hemolytic Diseases of Adults: This condition is seen in increased rate ofhemolysis. It usually occurs in adults. The characteristic features are increase in
unconjugated bilirubin in blood, absence of bilirubinuria and excessive excretion of UBG in urine and SBG in feces.
Common causes are:1.Congenital spherocytosis.• Autoimmune hemolytic anemias.• Toxins like carbon tetrachloride.

4- Hepatocellular Jaundice• The most common cause is viral hepatitis,caused by hepatitis viruses A, B, C, D, or G.
• Conjugation in liver is decreased and hencefree bilirubin is increased in circulation.

5- Obstructive Jaundice• Conjugated bilirubin is increased in blood, and it is excreted in urine.
• UBG will be decreased in urine or even absent.
• Since no pigment are entering into the gut, the feces become clay colored.• The common causes are:
1. Intrahepatic cholestasis. This may be due to cirrhosis or hepatoma.
2. Extrahepatic obstruction. This may be due to stones in the gallbladder or biliary tract; carcinoma of head of pancreas.




Kidney in AB equilibrium