Embed Size (px)
Citation preview

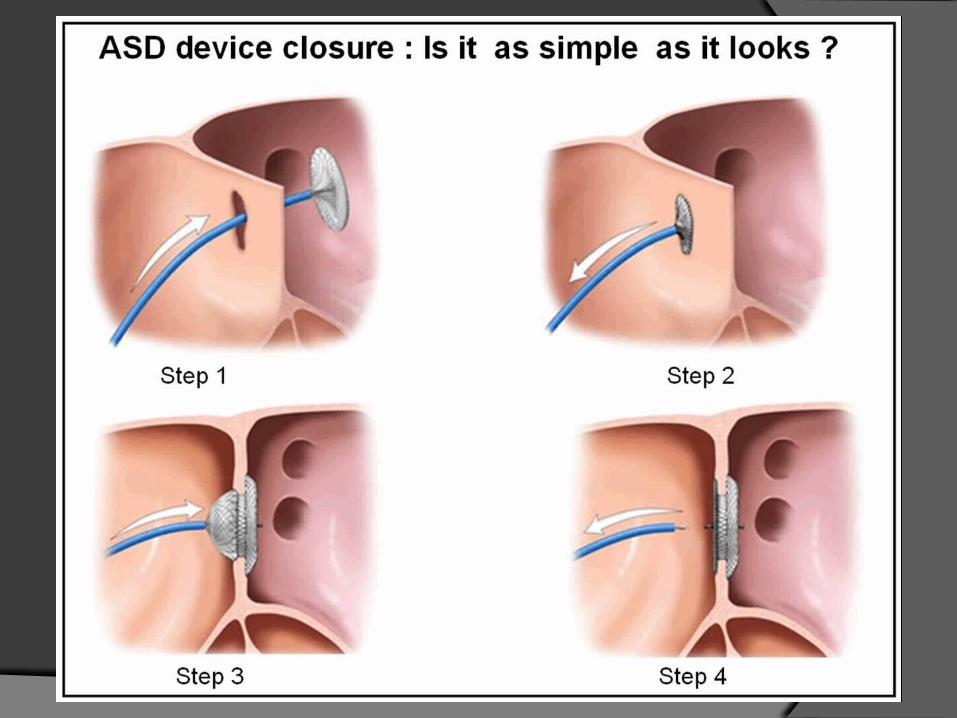
ATRIAL SEPTAL DEFECTS
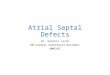
Epidemiology of Congenital Heart Disease in India. R Bhardwaj et al. Cong heart dis 2014
CONTENT
Embryology Classification/Types Natural History Timing ,Indications For Intervention
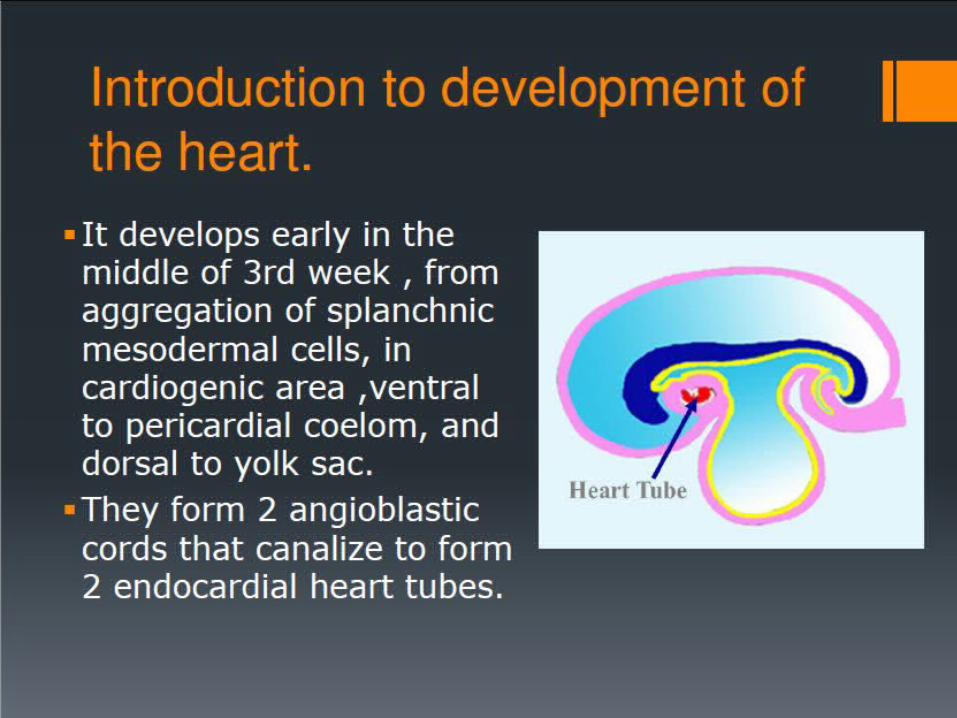
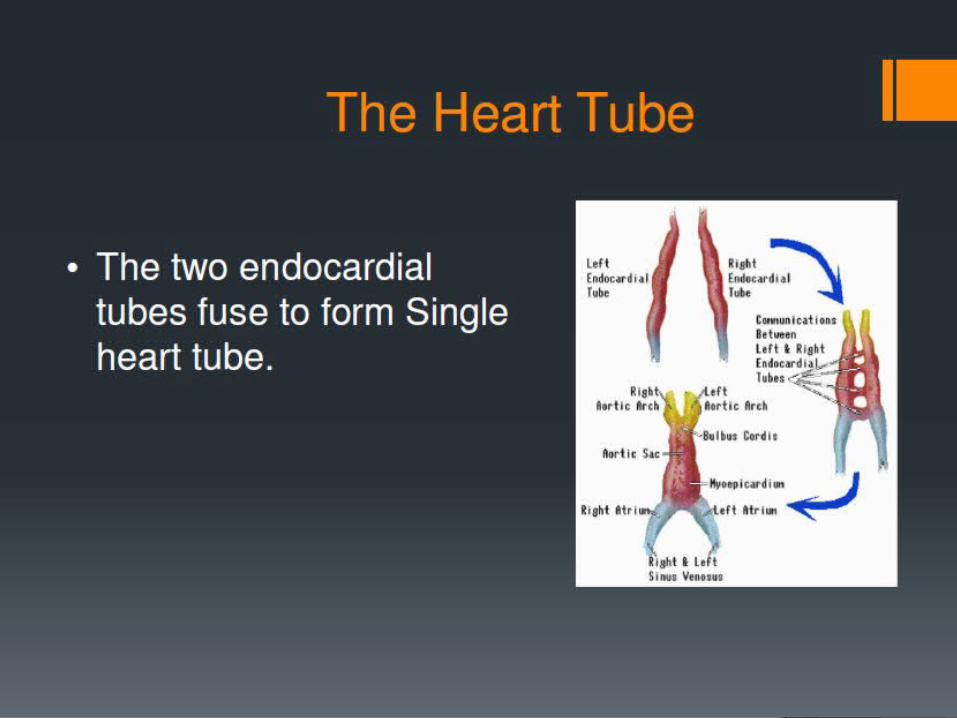
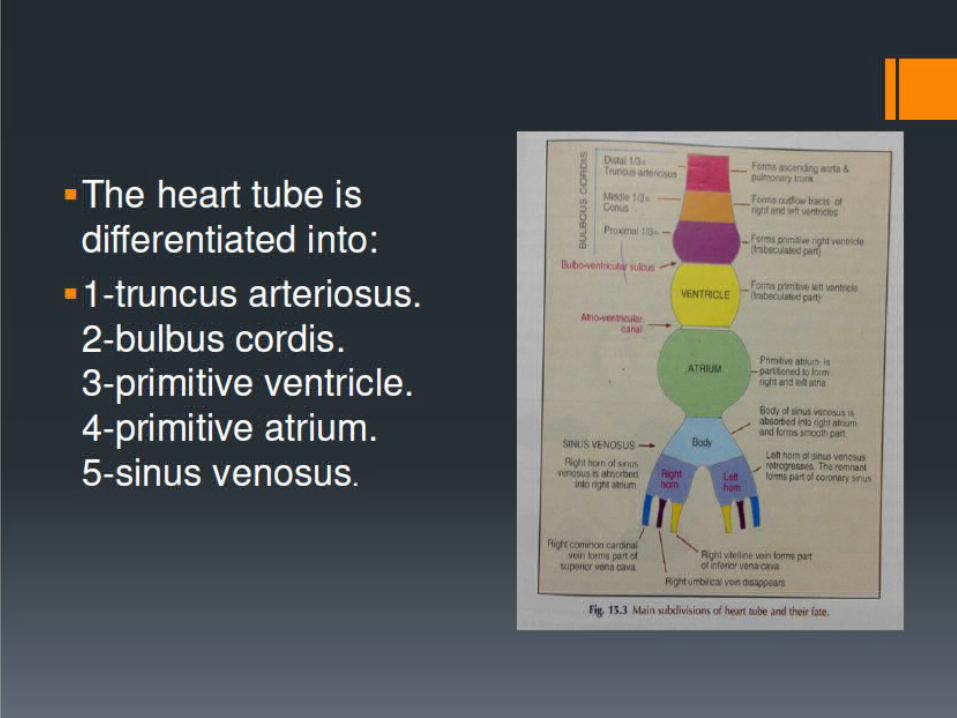
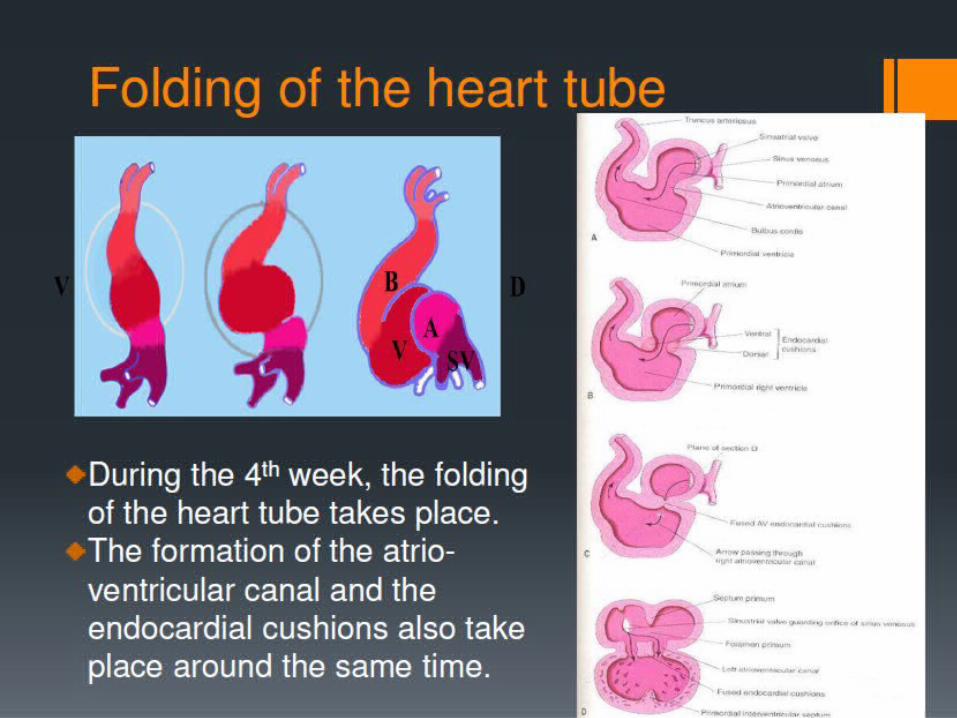
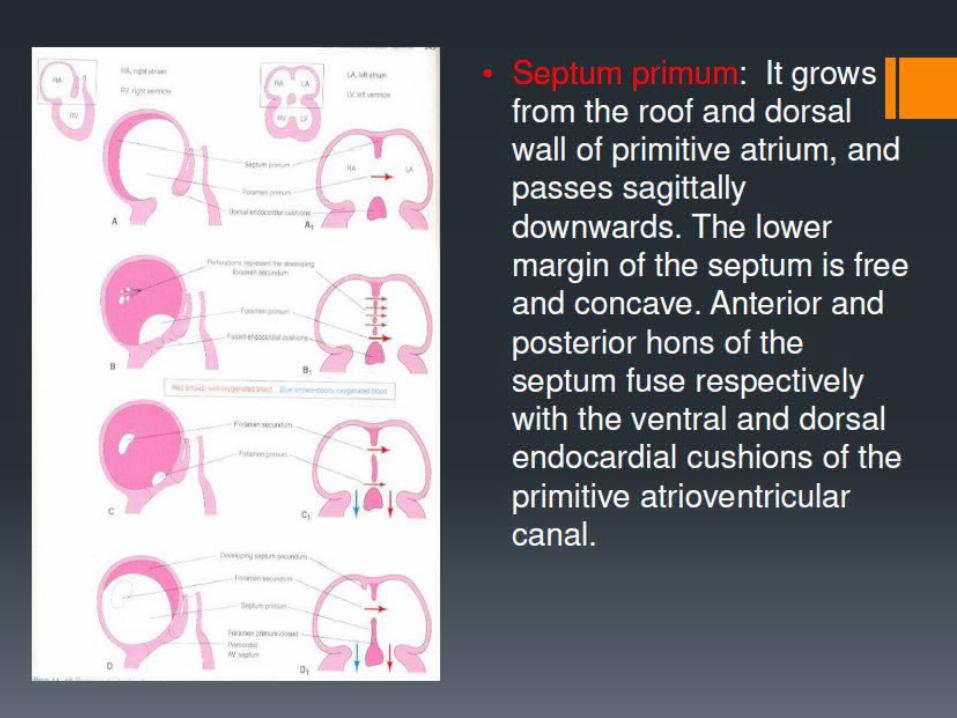
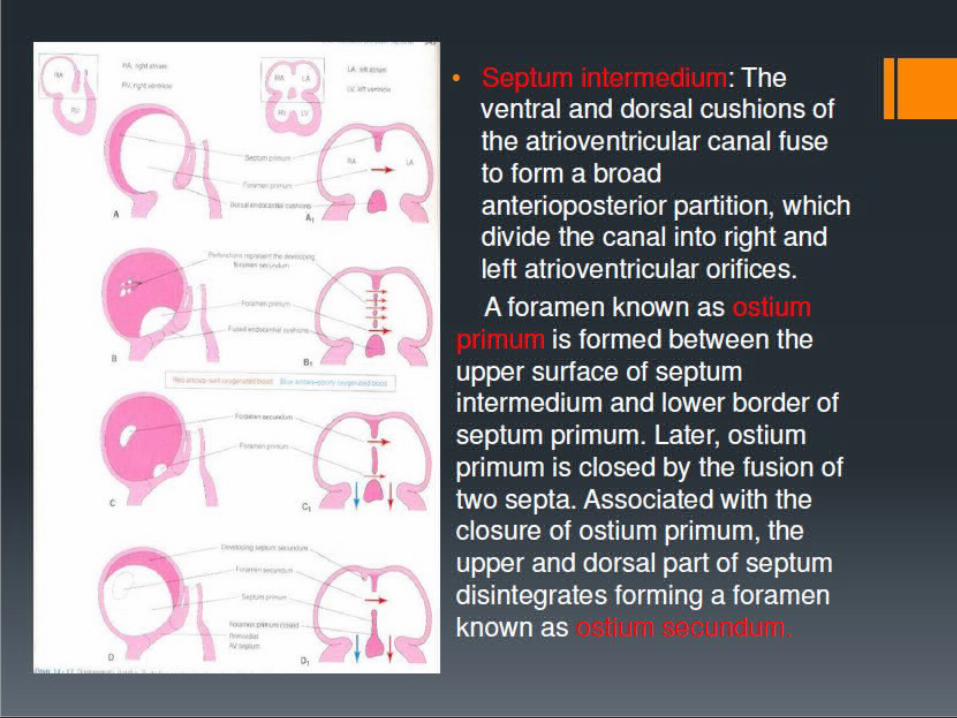
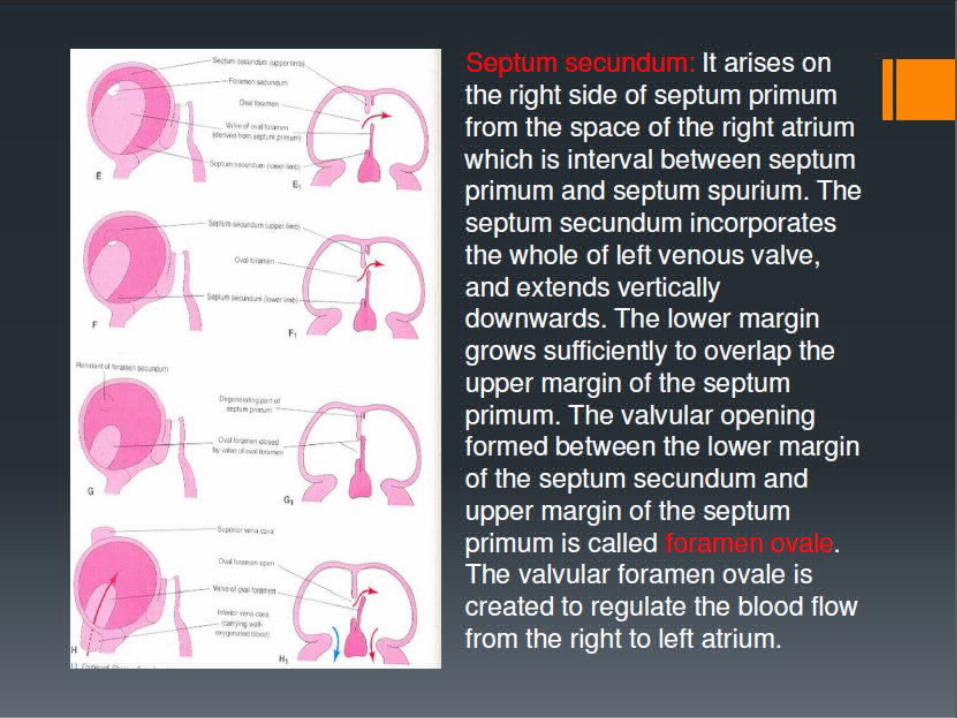
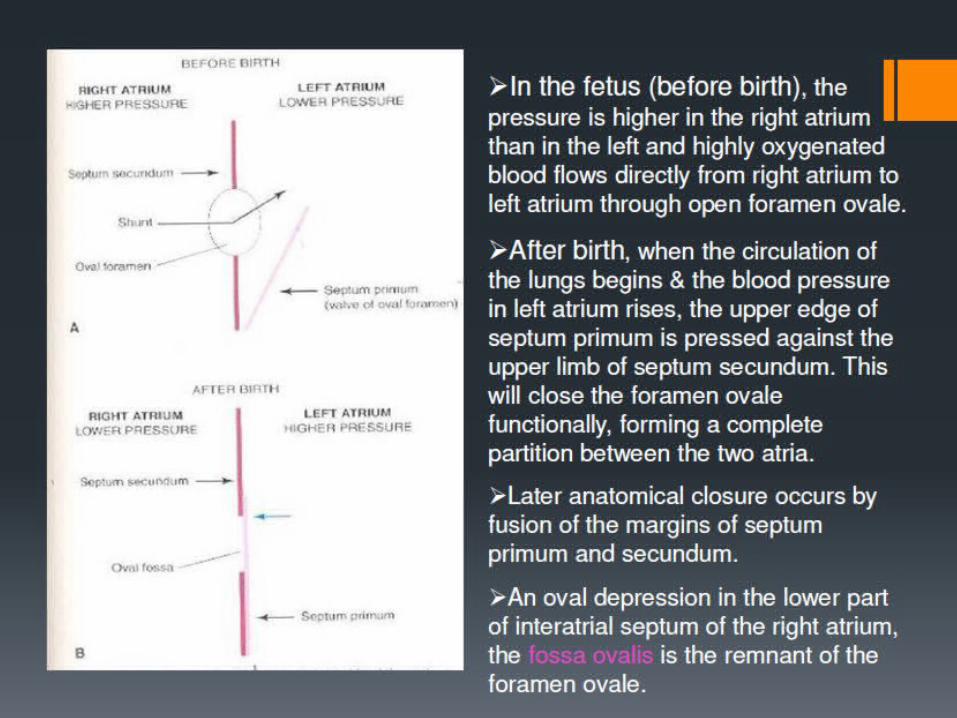
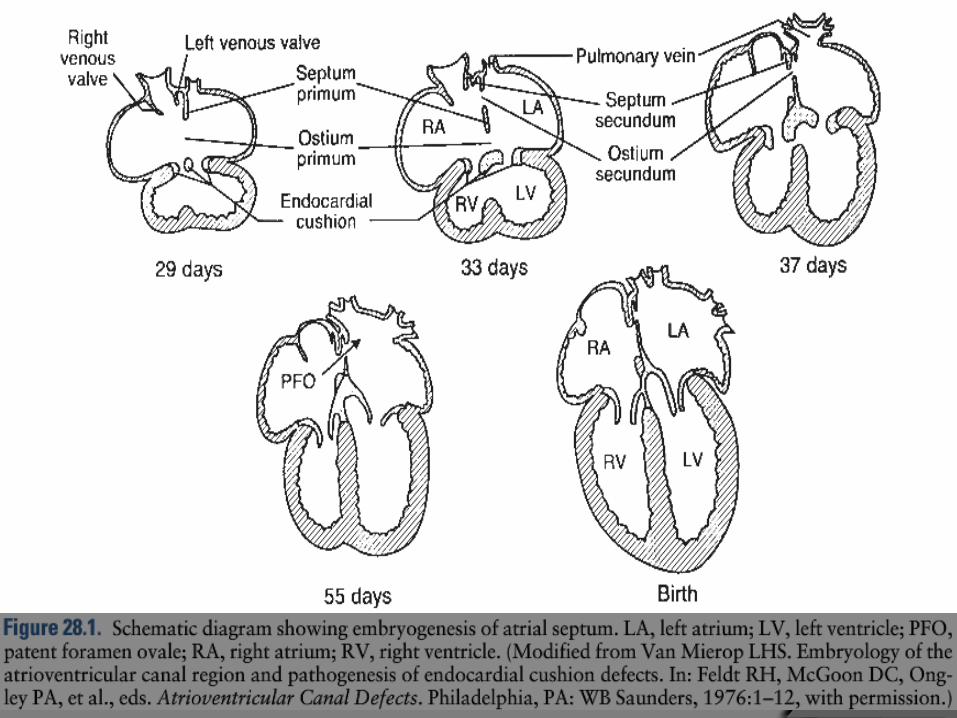
EMBRYOLOGY
CLASSIFICATION
Ostium Secundum (85%) Ostium Primum (6%) Sinus Venosus (8%) Common atrium (1pt)
CRAIG & SELZER 1968 (Circulation)
CLASSIFICATION
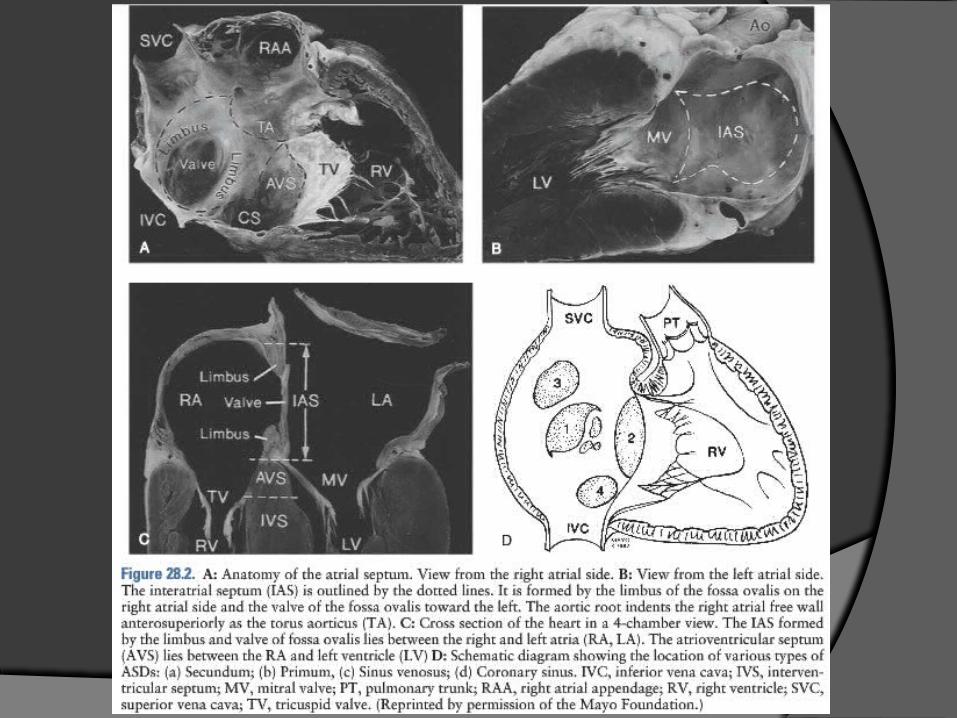
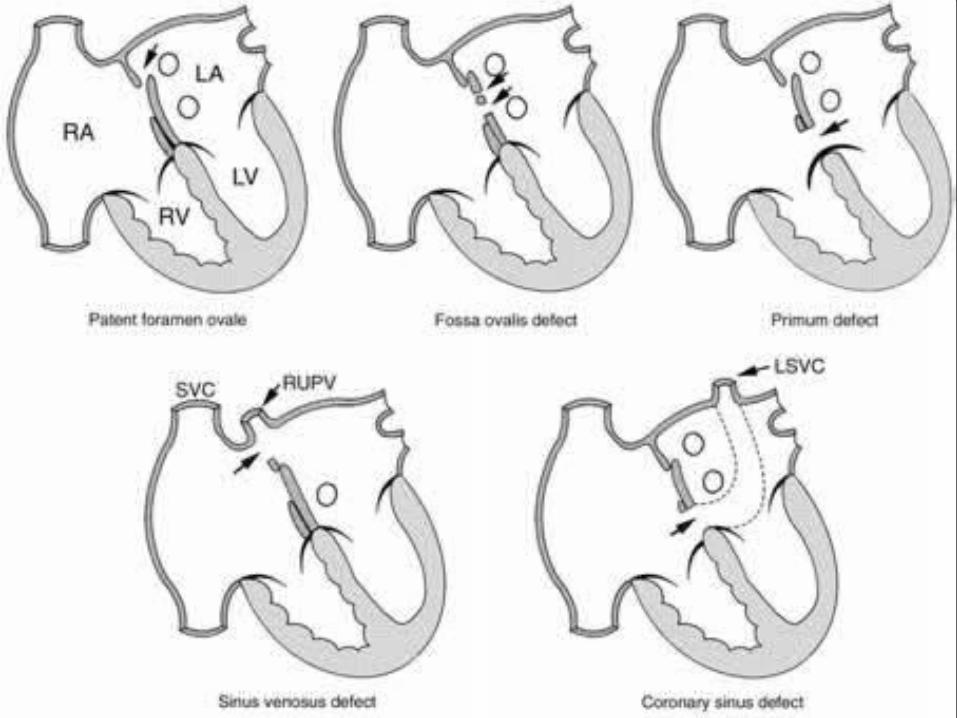
Ostium secundum defects (75%- 85% of ASDs) are located in the region of the fossa ovalis.
Ostium primum defects (10 - 15%) occur in the lower portion of the atrial septum.
Sinus venosus defects (5 - 10%) are located near the orifice of the superior vena cava.
Sinus venosus defects of IVC type (1%). Coronary sinus (1%) septal defect (in which a
defect between the coronary sinus and the left atrium allows a left-to-right shunt to occur through an “unroofed” coronary sinus).
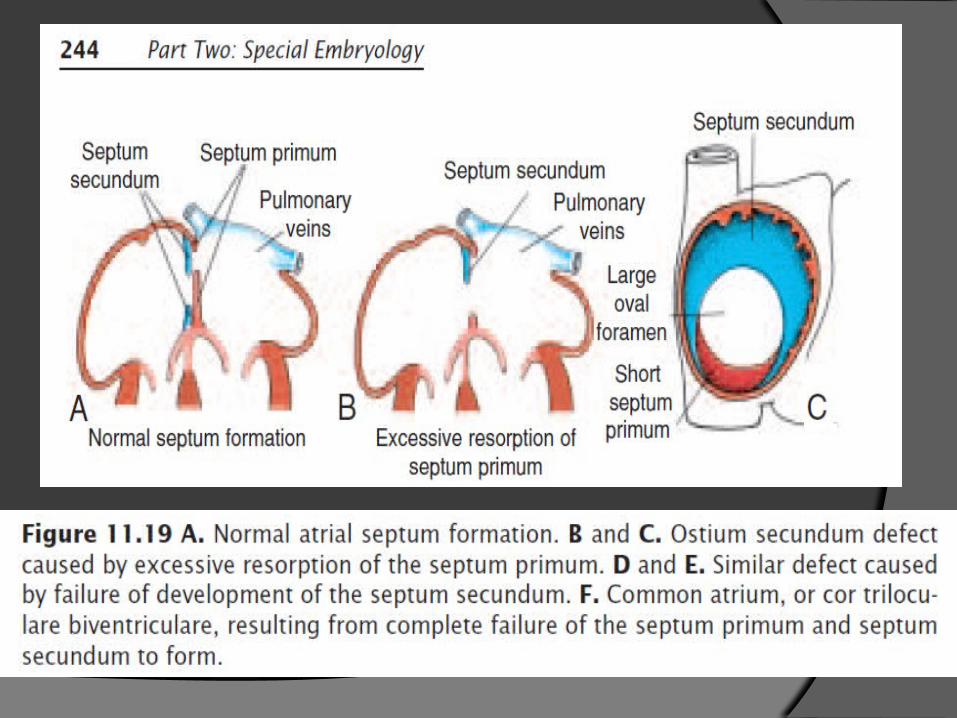
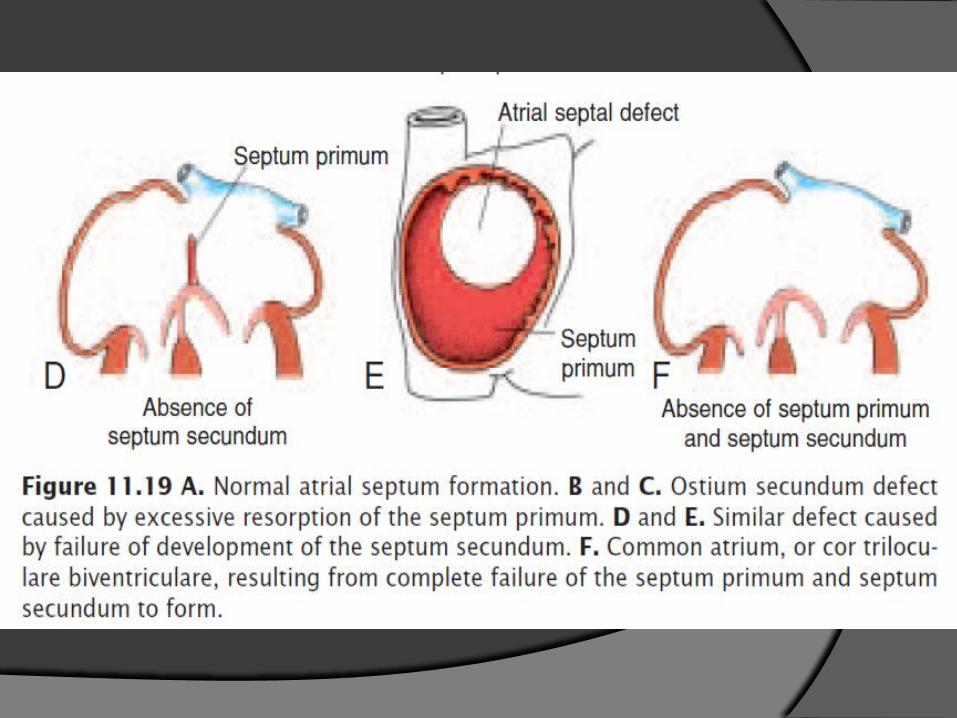
Ostium secundum defect Excessive cell death and resorption of the septum
primum or Inadequate development of the septum
secundum.
Ostium primum defect Failure of EC to fuse completely
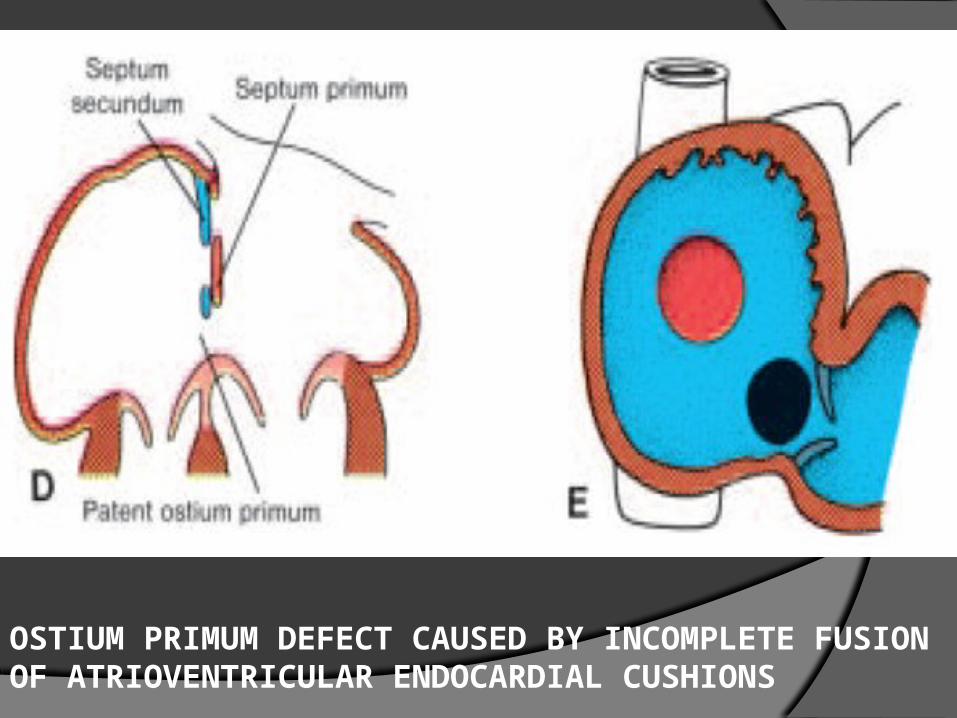
OSTIUM PRIMUM DEFECT CAUSED BY INCOMPLETE FUSION OF ATRIOVENTRICULAR ENDOCARDIAL CUSHIONS
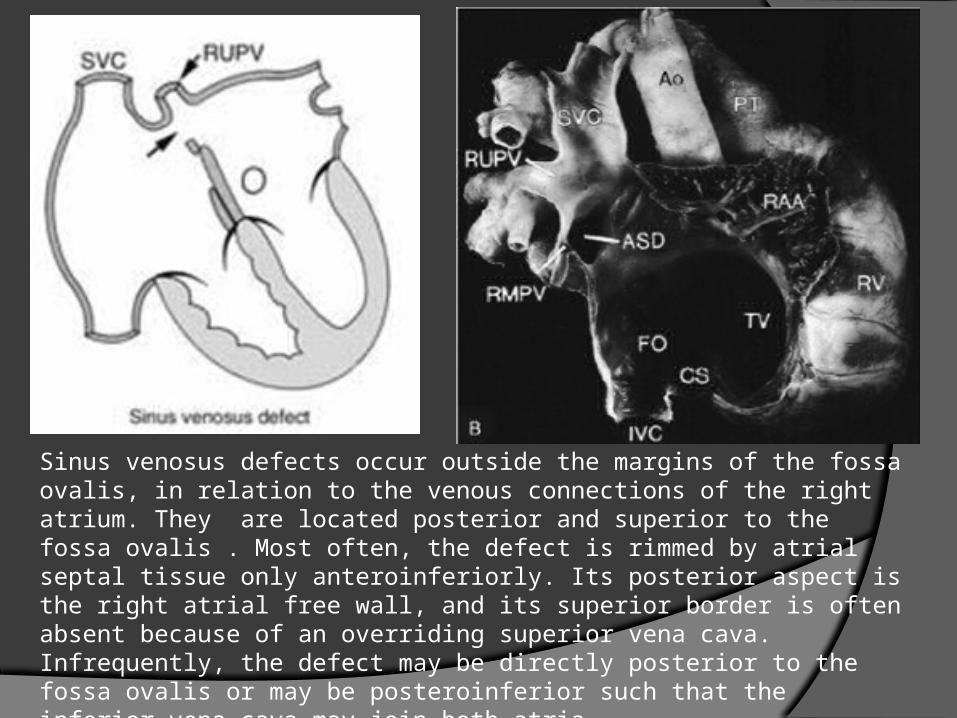
Sinus venosus defects occur outside the margins of the fossa ovalis, in relation to the venous connections of the right atrium. They are located posterior and superior to the fossa ovalis . Most often, the defect is rimmed by atrial septal tissue only anteroinferiorly. Its posterior aspect is the right atrial free wall, and its superior border is often absent because of an overriding superior vena cava. Infrequently, the defect may be directly posterior to the fossa ovalis or may be posteroinferior such that the inferior vena cava may join both atria
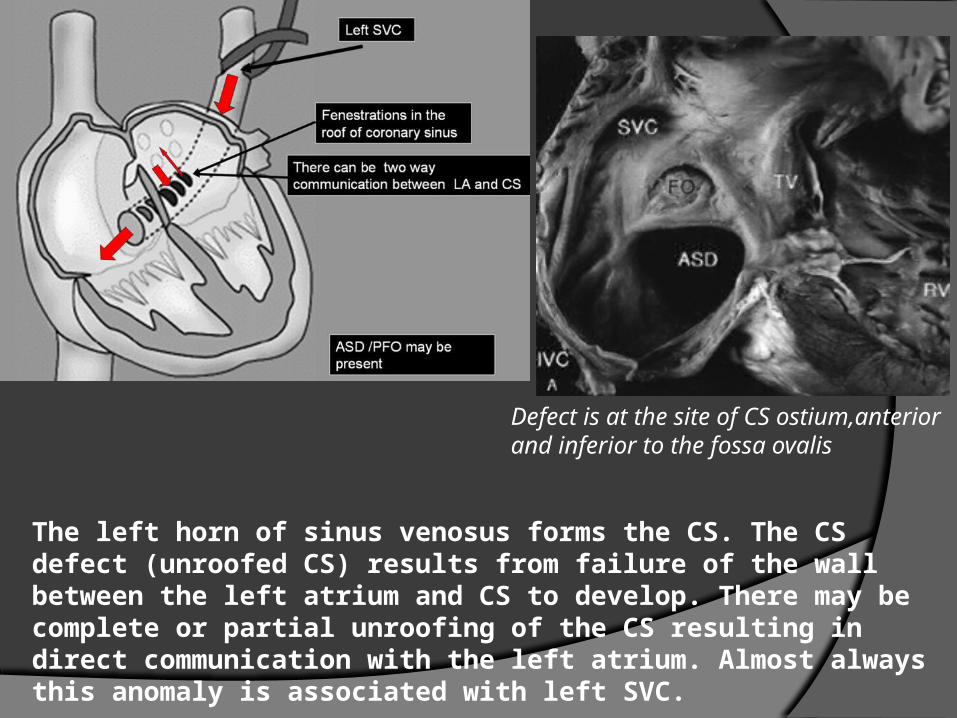
The left horn of sinus venosus forms the CS. The CS defect (unroofed CS) results from failure of the wall between the left atrium and CS to develop. There may be complete or partial unroofing of the CS resulting in direct communication with the left atrium. Almost always this anomaly is associated with left SVC.
Defect is at the site of CS ostium,anterior and inferior to the fossa ovalis
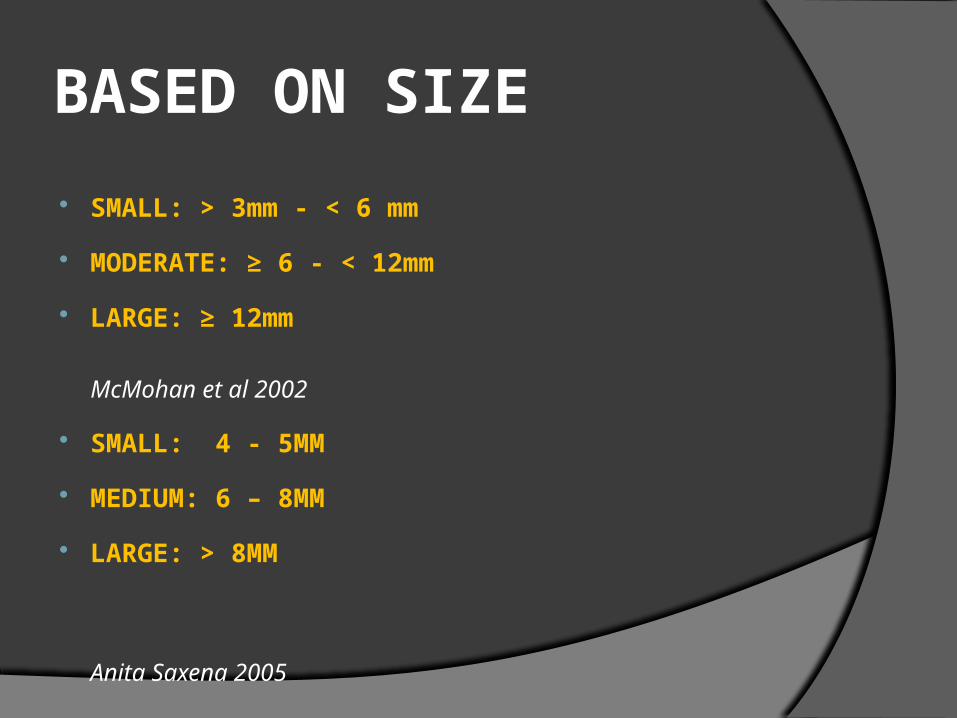
BASED ON SIZE
SMALL: > 3mm - < 6 mm
MODERATE: ≥ 6 - < 12mm
LARGE: ≥ 12mm
McMohan et al 2002
SMALL: 4 - 5MM
MEDIUM: 6 – 8MM
LARGE: > 8MM
Anita Saxena 2005
INCIDENCE
ASD constitutes 8-10% of congenital heart defects in children.
Incidence = 56 per 100,000 live births Recent estimates are much higher (100 per
100,000 live births), likely due to increased recognition in the era of common use of echocardiography
female:male ratio for secundum ASD = 2:1 For sinus venosus ASD= 1:1
GENETICS
The genetic basis of ASD is not completely understood.
In the majority of cases this is a sporadic lesion,yet some homeobox gene defects have been found to explain some of the well known familial cases of ASDs, such as NKX2-chromosome-5, which has an autosomal dominant inheritence and AV conduction defect.
GENETICS
Other genetic syndromes with skeletal abnormalities HOLT-ORAM Syndrome,which is acused by mutations in the transcription factor TBX5, essential in development of both the heart and upper limbs.
ASD can be part of many other syndromes like DOWN syndrome and Nooonan syndrome

NATURAL HISTORY
A. SPONTANEOUS CLOSURE
Spontaneous closure has been reported to occur in anywhere between 14–66% of ASDs.
Predictors of Closure
1. Smaller size
2. Earlier age at diagnosis (< 2yrs)
Cockerham et al 1983 (age) 87 children Underwent cath < 4 yrs of age for a
significant secundum ASD Spontaneous closure occurred in 22 % of
those who underwent cath in age <1 yr Those who were 2-4 yrs at time of cath
rate of spontaneous closure decreased to 3%
The group advocated to wait till 4 years of age for elective closure.
Radzik et al 1993 (size) 2-D echo based ASD < 5 mm including PFO = 87 %
SPONATNOUS CLOSURE > 8 mm- NO SPONTANEOUS
CLOSURE
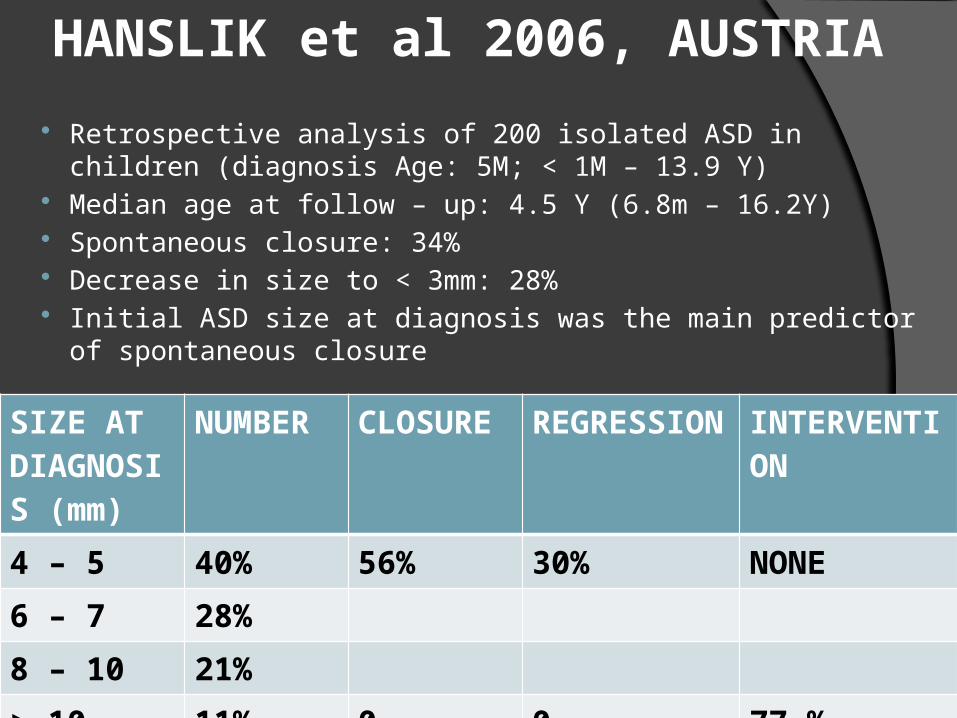
HANSLIK et al 2006, AUSTRIA
Retrospective analysis of 200 isolated ASD in children (diagnosis Age: 5M; < 1M – 13.9 Y)
Median age at follow – up: 4.5 Y (6.8m – 16.2Y) Spontaneous closure: 34% Decrease in size to < 3mm: 28% Initial ASD size at diagnosis was the main predictor of spontaneous
closure
SIZE AT DIAGNOSIS (mm)
NUMBER CLOSURE REGRESSION
INTERVENTION
4 – 5 40% 56% 30% NONE
6 – 7 28%
8 – 10 21%
> 10 11% 0 0 77 %
Whether ASD enlarge in size with time????
GROWTH OF ISOLATED OSTIUM SECUNDUM DEFECTS
McMohan et al. Heart 2002;87:256–259 104 pts with isolated secundum ASD at Texas Children Hospital,
Houston between 1991 - 1998 Reviewed retrospectively all patients presenting to the Texas
Children’s Hospital with isolated secundum ASD and assessed the change in maximal defect diameter as measured by sequential echocardiographic studies.
The rate of change in size (mm/year) of ASD, age at diagnosis, and interval of follow up were recorded.
The mean age at diagnosis of the ASD was 4.5 years (range 0.1–71 years).
The mean interval between echocardiograms was 3.1 years (range 0.7–8.1 years).
OVERALL GROUP 29% had large ASD, 38% had moderate sized ASD, and 33%
had small sized ASD. 66% had increase in the size of ASD at a rate of 0.8mm/year
(0.2 – 6.4mm/year) with 30% having > 50% increase in ASD size.
ASD size decreased in 15 patients (14%) Unchanged in 21 (20%). The rate of growth was independent of age at diagnosis, ranging
from 0.72 mm/year for the 2–4 year age group to 1.29 mm/year for the 4–6 year age group, which was not significant (p = 0.9).
The mean duration of follow up was 4.2 years (range 1.8–7.7 years) for defects that increased > 20 mm, indicating a tendency for continued ASD growth with time.
Strong correlation between the initial size and the final size of defects with a r2 = 0.61.
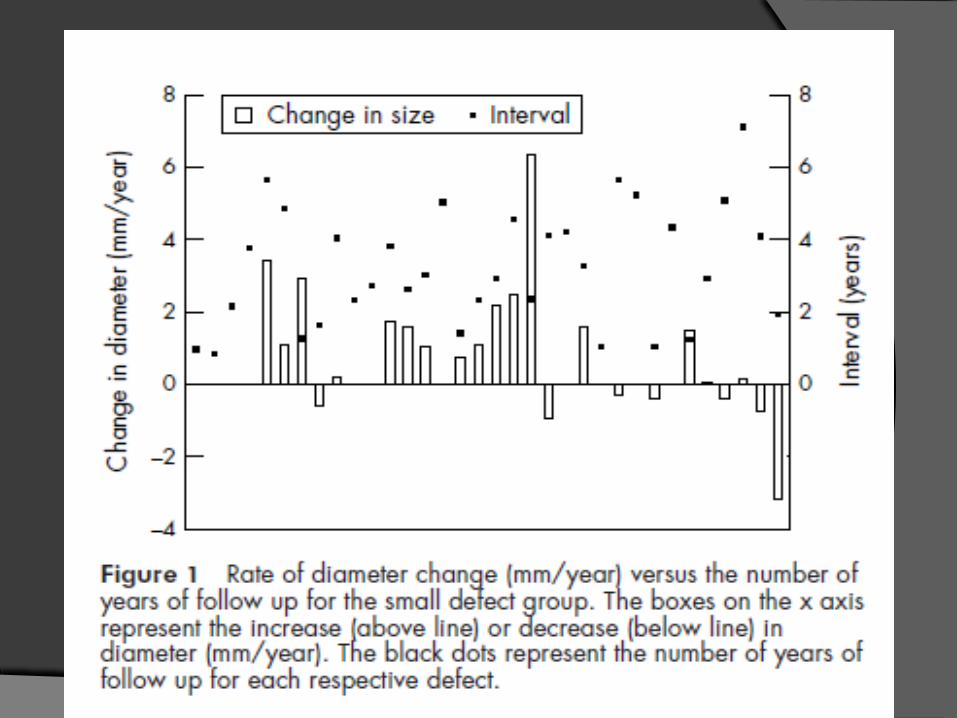
SMALL SIZED ASD 34 (33% of total defects) Three (10%) defects closed spontaneously. Seventeen (50%) defects increased in size. Seven (20%) of these defects increased from the small to
the moderate group and three (9%) defects increased from the small to the large group.
In ASDs that increased from the small to the large group, the diameters increased from 3 mm to 22 mm, 3 mm to 17 mm, and 3 mm to 15 mm.
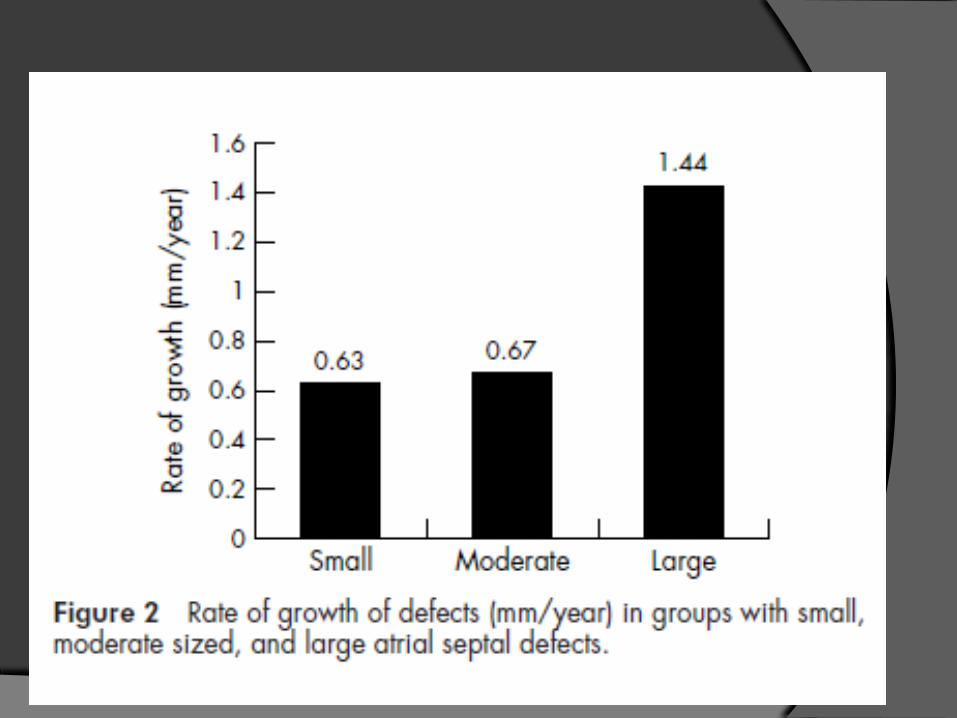
The mean rate of increase in ASD size was 0.63 (1.6) mm/year for defects in this group (fig 2).
The mean follow up was 3.2 years (range 0.9–7.1 years).
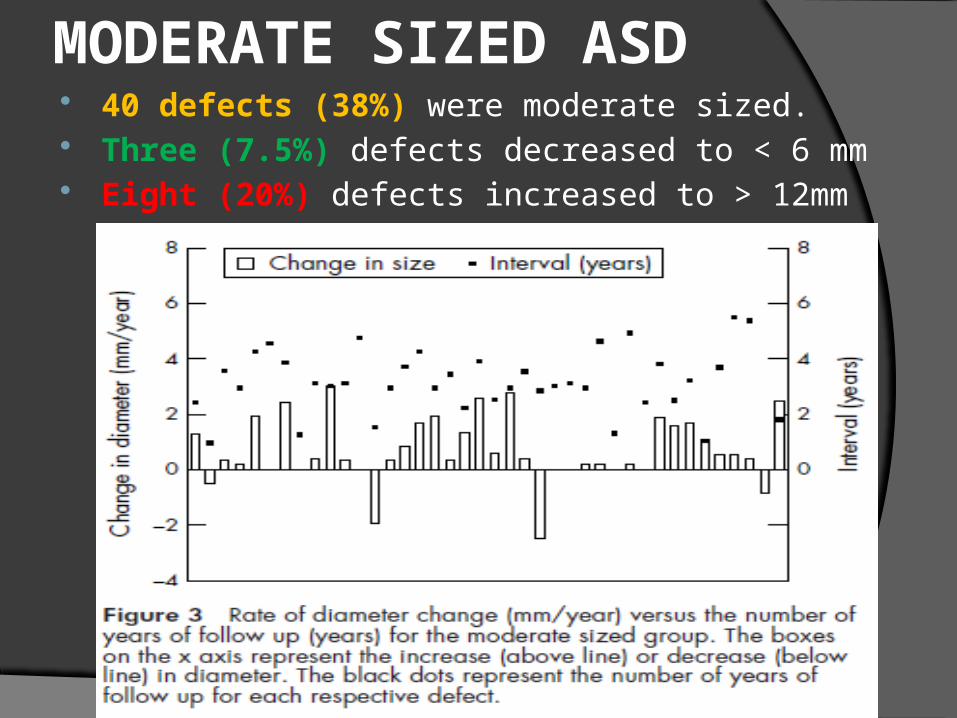
MODERATE SIZED ASD 40 defects (38%) were moderate sized. Three (7.5%) defects decreased to < 6 mm Eight (20%) defects increased to > 12mm
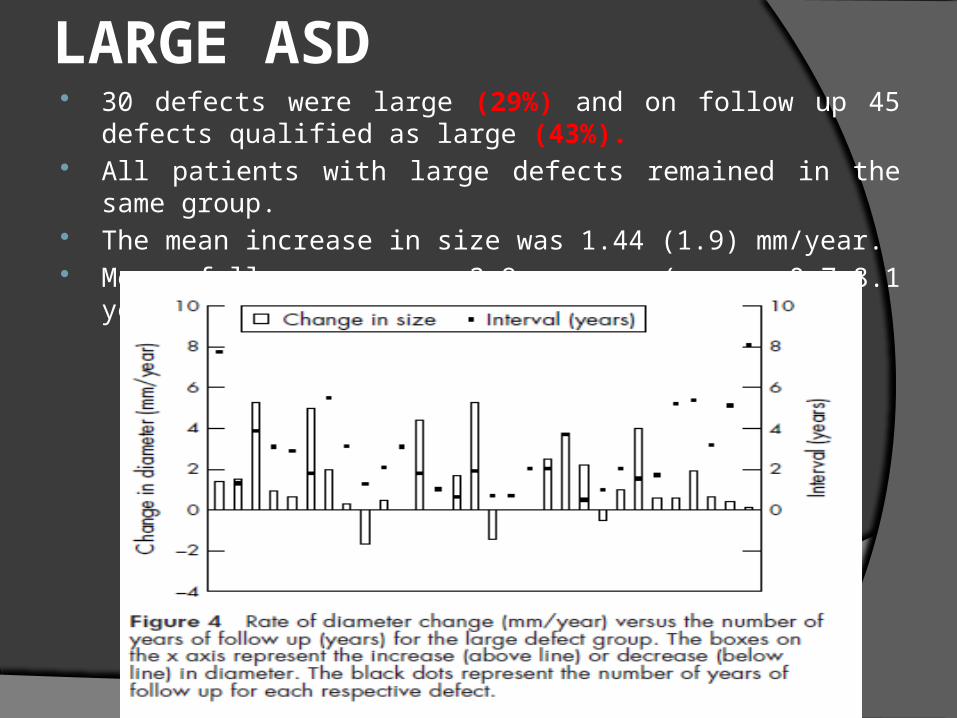
LARGE ASD 30 defects were large (29%) and on follow up 45 defects qualified as
large (43%). All patients with large defects remained in the same group. The mean increase in size was 1.44 (1.9) mm/year. Mean follow up was 2.9 years (range 0.7–8.1 years).
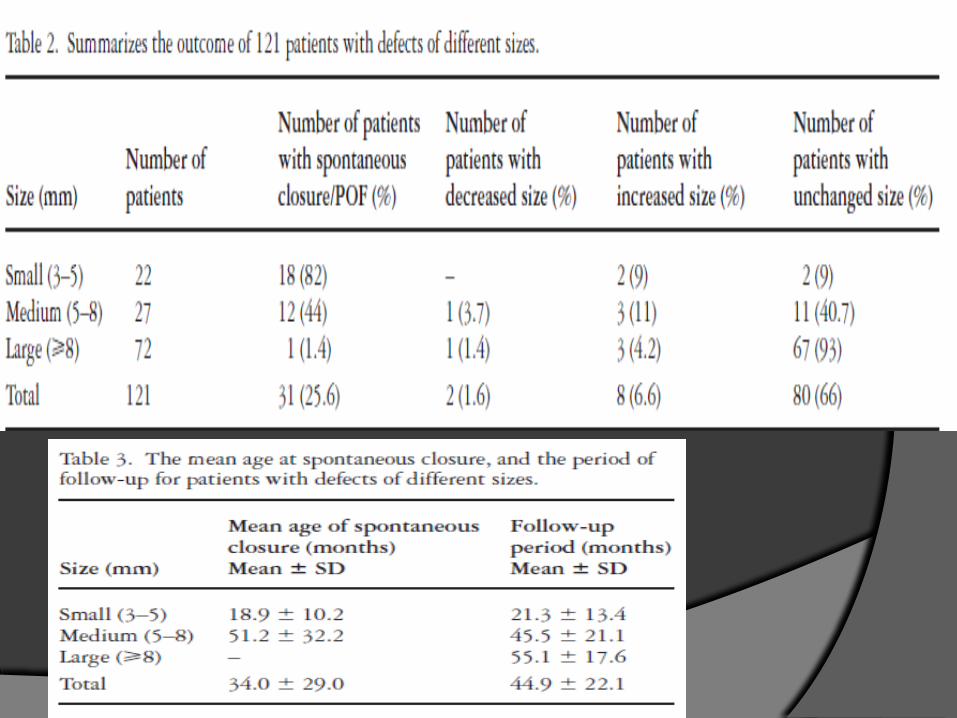
Nawal Azhari. Cardiol Young 2004; 14: 148–155
Retrospective analysis of 121 cases isolated secundum ASDs between 1990 – 2003
18.2% - 3 to 5 mm, 22.3% - 5 to 8 mm, and 59.5% - > 8 mm Mean age at diagnosis was 23.0 ± 24.3 M (1 day
to 11 years). 25.6% had spontaneous closure
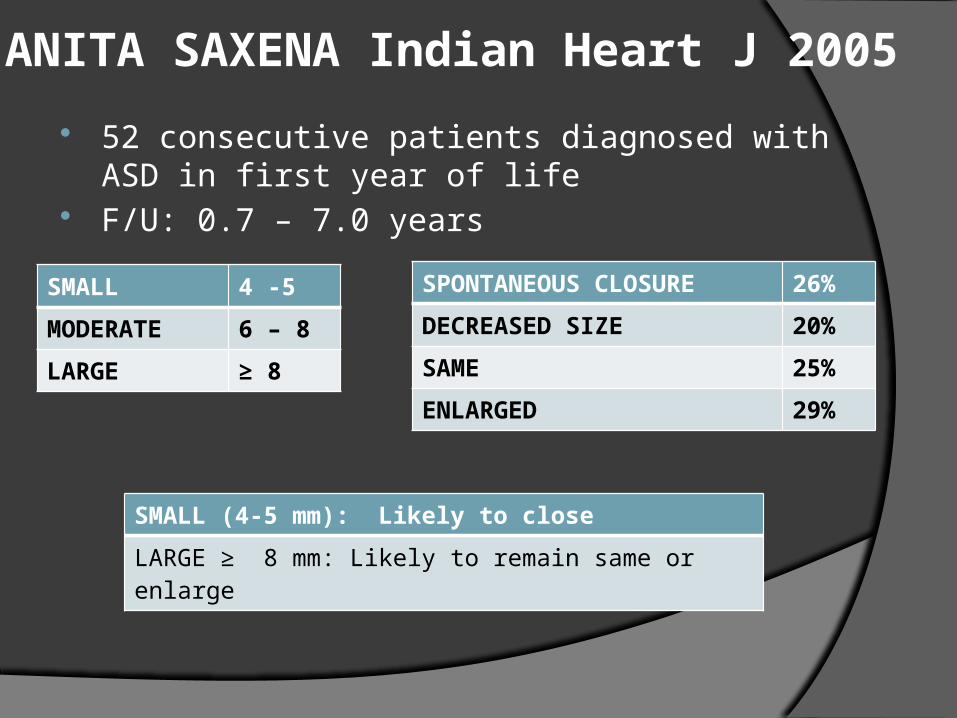
ANITA SAXENA Indian Heart J 2005 52 consecutive patients diagnosed with ASD in first year of
life F/U: 0.7 – 7.0 years
SMALL 4 -5
MODERATE 6 – 8
LARGE ≥ 8
SPONTANEOUS CLOSURE 26%
DECREASED SIZE 20%
SAME 25%
ENLARGED 29%
SMALL (4-5 mm): Likely to close
LARGE ≥ 8 mm: Likely to remain same or enlarge
Summary
Defects larger than 8-10 mm are less likely to close spontaneously and most likely will require surgical or transcatheter closure ,regardless of the age at diagnosis.
ASDs diagnosed after the first 4 yrs of life are less likely to spontaneously close and they can present later in life with several complications.
COMPLICATIONS
COMPLICATIONS
Symptoms of exercise intolerance and fatigue/CCF
Atrial arrhythmias Pulmonary hypertension Systemic embolization Reduced life expectancy
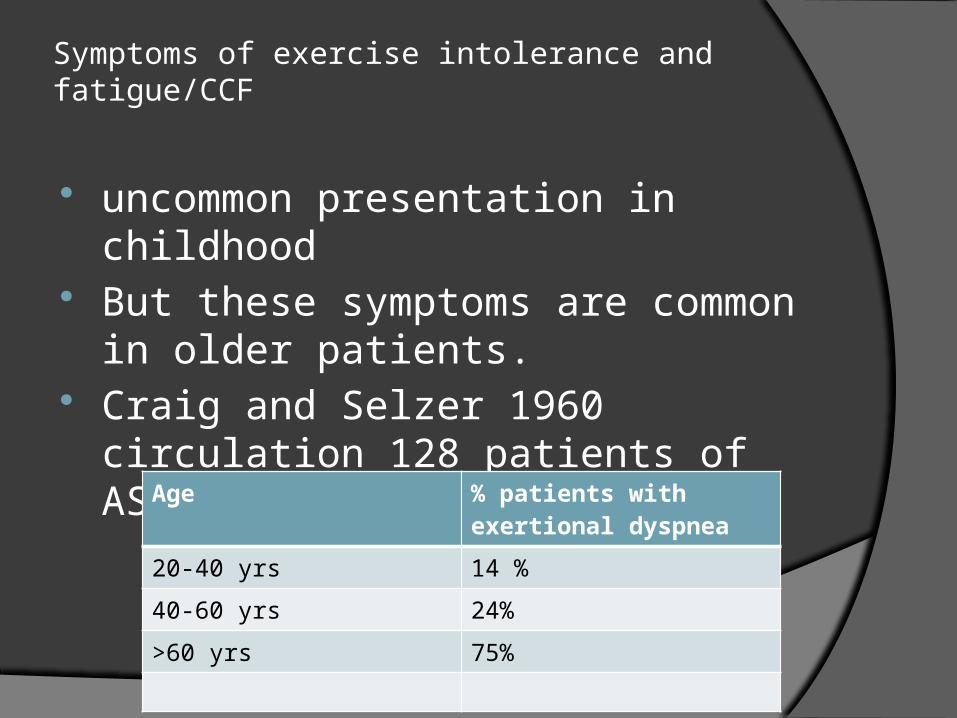
Symptoms of exercise intolerance and fatigue/CCF
uncommon presentation in childhood But these symptoms are common in
older patients. Craig and Selzer 1960 circulation 128
patients of ASD >18-68 yrs age
Age % patients with exertional dyspnea
20-40 yrs 14 %
40-60 yrs 24%
>60 yrs 75%
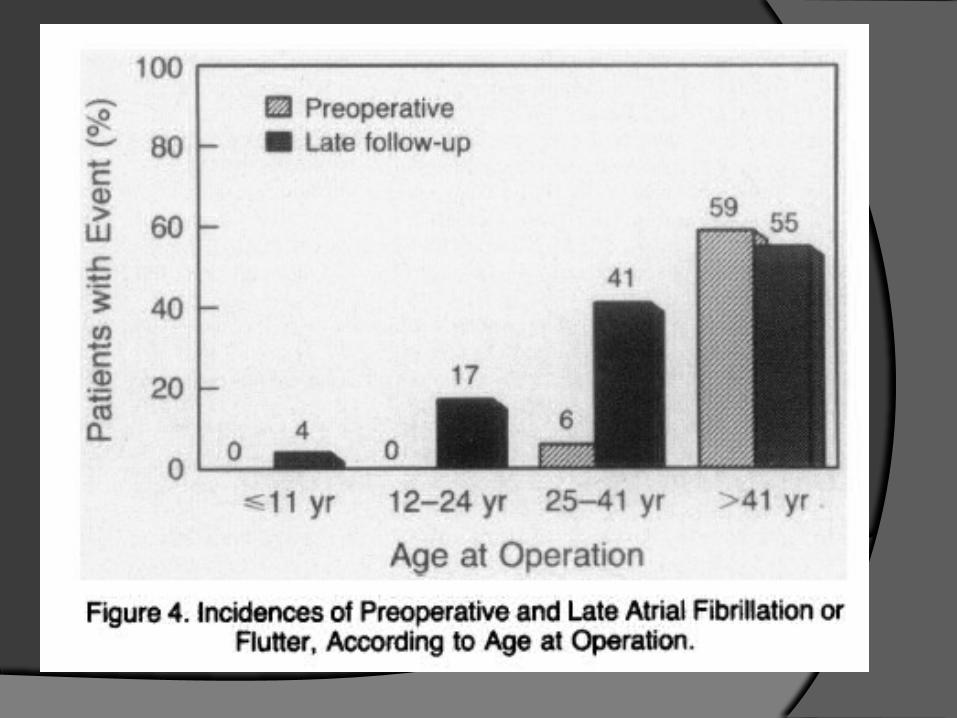
Atrial arrythmias Right atrial dilatation secondary to chronic
stretching and volume overload predisposes older patients to atrial arrhythmias such as AF and less commonly Afl, this can exacerbate signs and symptoms of CCF.
They are one of the most common presenting symptoms in the 4th to 5th decade of life.
Incidence has been reported to be >50% in patients older than 60 yrs (Berger F et al 1999)
In series by Craig and Selzer 1960 circulation , 80% of ASD patients above 40 yrs age had chronic atrial tachyarrhythmias
JAMES GAULT, Circulation, Volume XXXVII, February 1968
62 pts > 40 years (46.5 years)
CLINICAL FEATURES 94% were symptomatic at initial presentation
1. Dyspnea – 90%
2. Fatigue – 48%
3. Palpitations – 43%
4. Edema – 28%
5. Angina – 8% NYHA II - 45% NYHA III – 43.5%
82% in NYHA II/III had PAH with > 50% having severe PAH
Severe PAH with balanced or reversed shunt: 13%
Pulmonary hypertension Most serious complication Not common in young age According to craig and selzer 14 -18 % between 20-
40 yrs age develop PAH It is still debatable that whether this is caused by the
presence of large shunts or due to other predisposing conditions such as thromboembolic phenomenon.
Eissenmenger is infrequent and usually occurs late in life
In a series BY konstantinides et al, mean age was 56 yrs
IS IT SEEN EXCLUSIVELY IN OLDER PATIENTS????
PULMONARY HYPERTENSION IN ASD
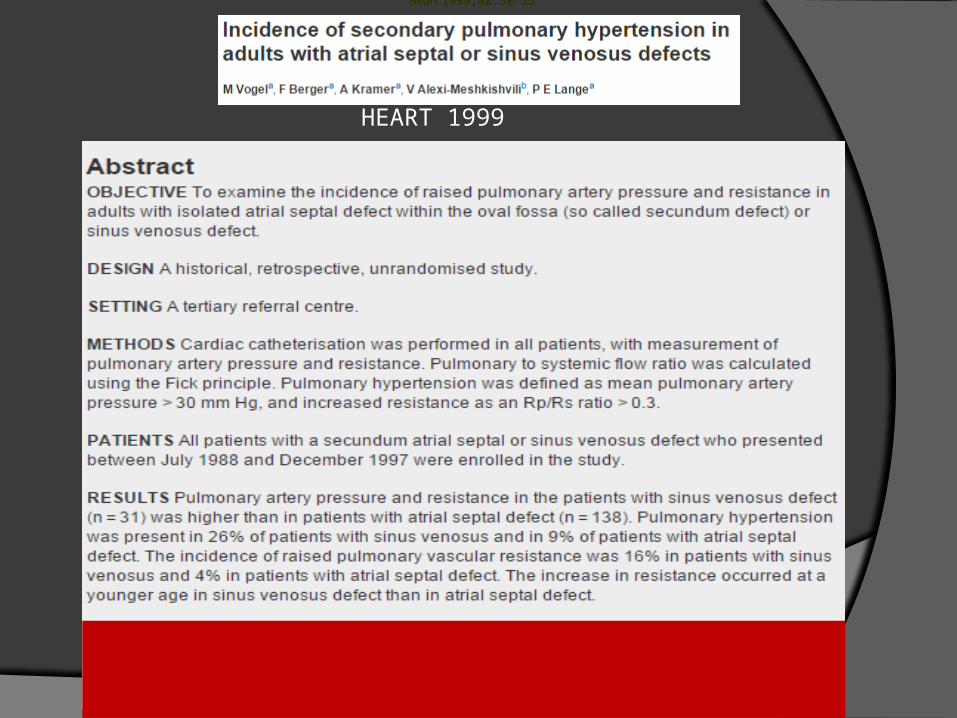
HEART 1999
Heart 1999;82:30-33 Heart 1999;82:30-33 Heart 1999;82:30-33
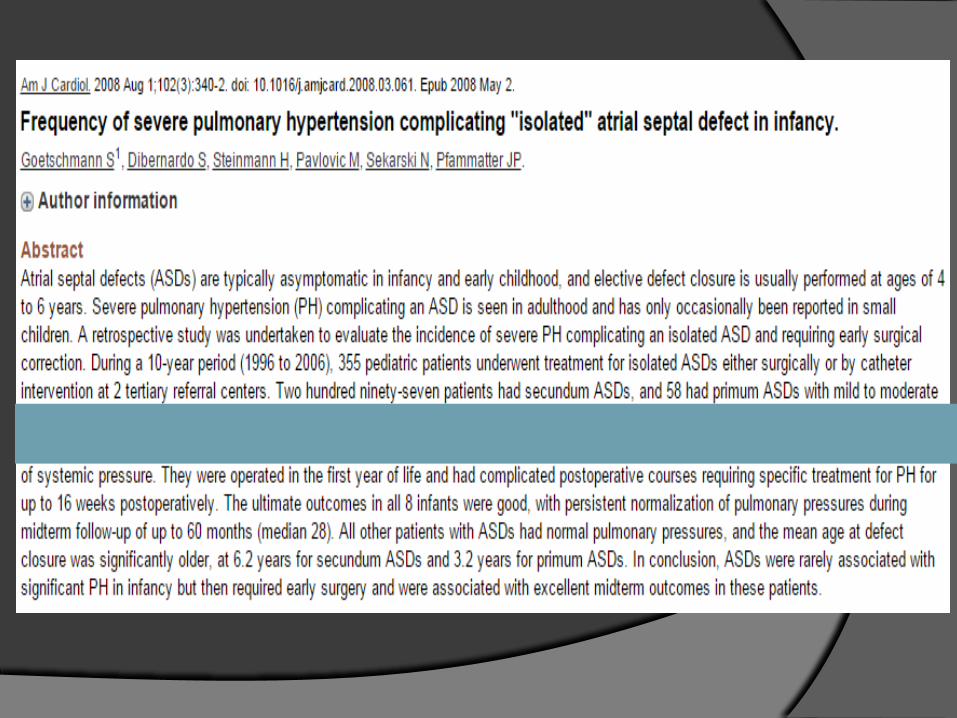
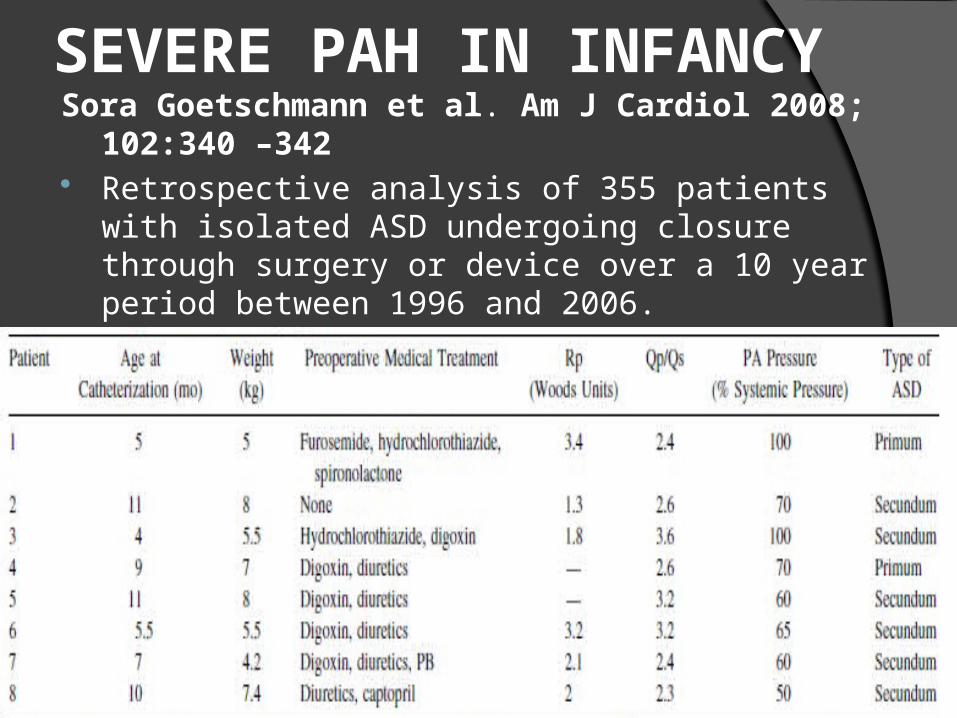
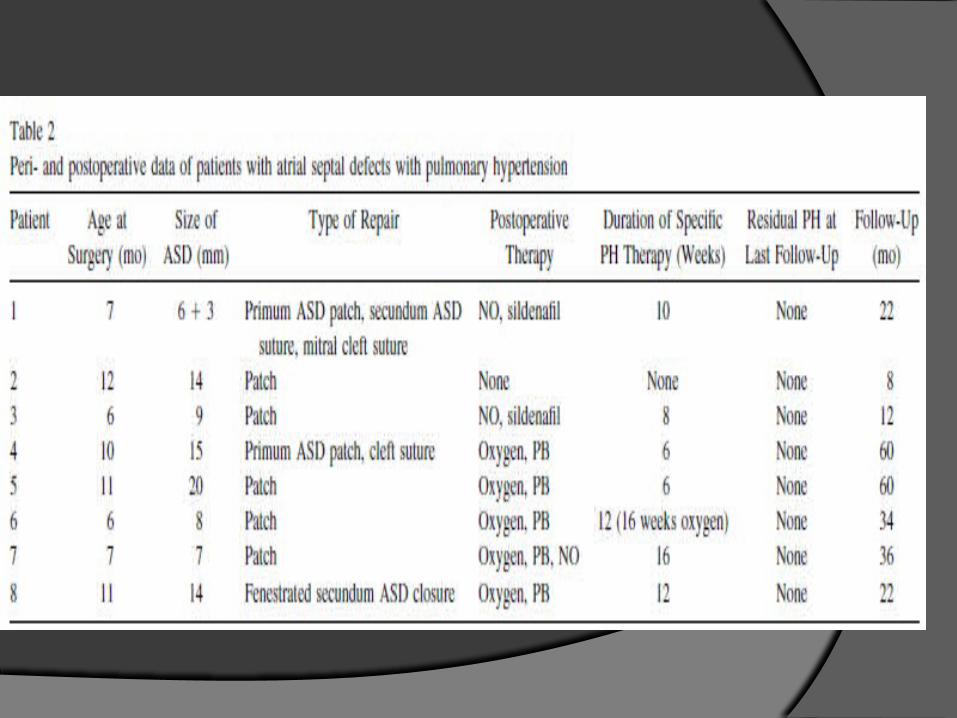
SEVERE PAH IN INFANCYSora Goetschmann et al. Am J Cardiol 2008; 102:340 –342 Retrospective analysis of 355 patients with isolated ASD
undergoing closure through surgery or device over a 10 year period between 1996 and 2006.
2.2% of the total study population had severe PAH (> 50 % of systemic pressure)
MORTALITY
Secondary to pulmonary artery thrombosis, congestive heart failure, paradoxical embolism and recurrent respiratory tract infections.
It is now difficult these days to estimate age of survival in patients with unrepaired ASDs in the modern era of surgical and catheter interventions.
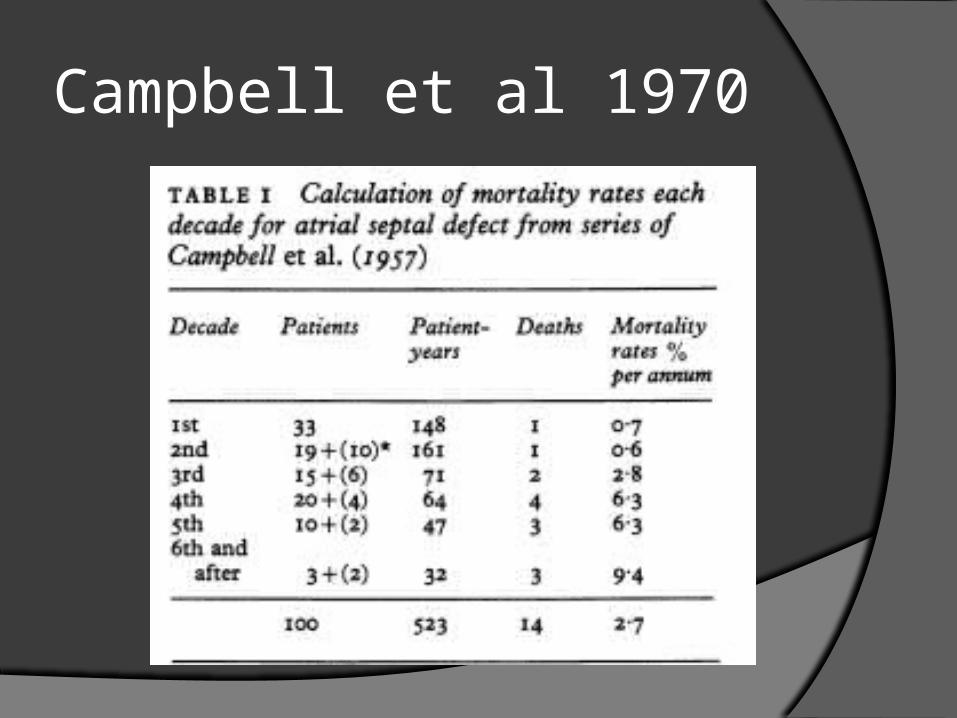
Campbell et al 1970
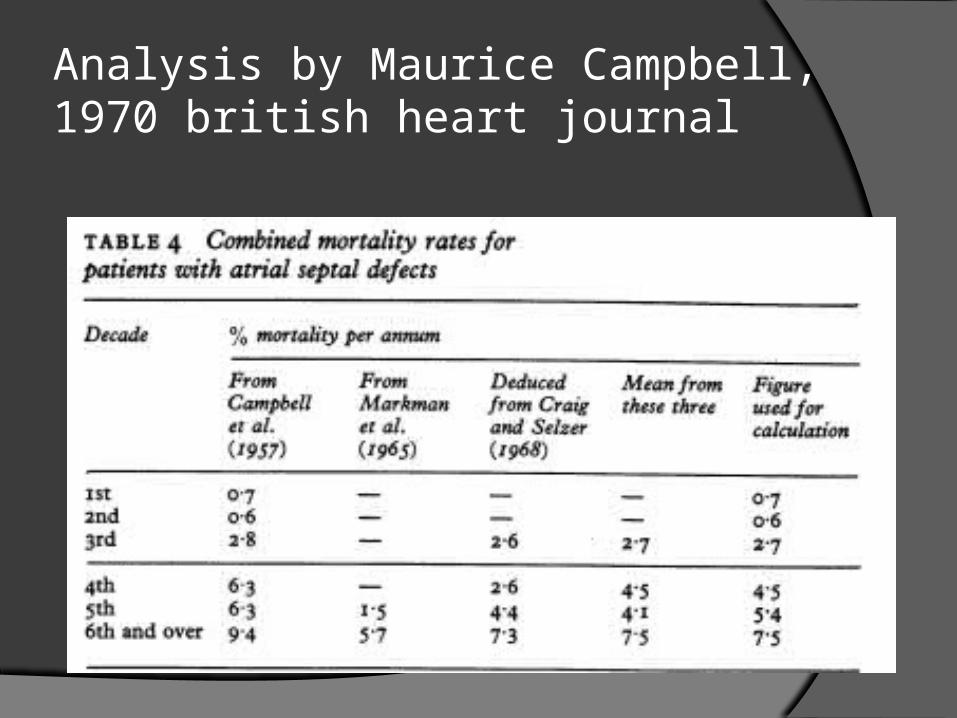
Analysis by Maurice Campbell, 1970 british heart journal
TREATMENT
Management issues
Management questions arise once an ASD is found.
Whether to close it?? Or just observe? What is the appropriate timing?? What are the options for closure??
ACC AHA Recommendations for Interventional and Surgical Therapy- CLASS 1
1. Closure of an ASD either percutaneously or surgically is indicated for right atrial and RV enlargement with or without symptoms. (Level of Evidence: B)
2. A sinus venosus, coronary sinus, or primum ASD should be repaired surgically rather than by percutaneous closure. (Level of Evidence: B)
3. Surgeons with training and expertise in CHD should perform operations for various ASD closures. (Level of Evidence: C)
Class 2A recommendations 1. Surgical closure of secundum ASD is
reasonable when concomitant surgical repair/replacement of a tricuspid valve is considered or when the anatomy of the defect precludes the use of a percutaneous device. (Level of Evidence: C)
2. Closure of an ASD, either percutaneously or surgically, is reasonable in the presence of: a. Paradoxical embolism. (Level of Evidence: C) b. Documented orthodeoxia-platypnea. (Level of
Evidence: B)
Class 2B recommendations Closure of an ASD, either percutaneously or
surgically, may be considered in the presence of
net left-to-right shunting, Qp/Qs>1.5 pulmonary artery pressure less than two thirds
systemic levels, PVR less than two thirds systemic vascular
resistance, or when responsive to either pulmonary
vasodilator therapy or test occlusion of the defect. (Level of Evidence: C)
Class 3 recommendation
Patients with severe irreversible PAH and no evidence of a left-to-right shunt should not undergo ASD closure. (Level of Evidence: B)
IDEAL AGE FOR CLOSURE
In asymptomatic child: 2-4 years (Class I). For sinus venosus defect surgery may be delayed to
4-5 years (Class IIa). Symptomatic ASD in infancy (congestive heart failure,
severe pulmonary artery hypertension): seen in about 8%-10% of cases. Rule out associated lesions (e.g., total anomalous pulmonary venous drainage, left ventricular inflow obstruction, aorto-pulmonary window). Early closure is recommended (Class I).
If presenting beyond ideal age: Elective closure irrespective of age as long as there is right heart volume overload and pulmonary vascular resistance is in operable range (Class I).
What to do for small defects???
Closure of small defects without any right sided cardiac enlargement is controversial.
While these patients may remain asymptomatic well into their fourth and fifth decades of life, there is concern about increase of the left to right shunt at an older age due to reduced LV compliance as a result of CAD, systemic HTN, or valvular heart disease.
Routine follow up of these patients during adulthood is recommended.
And should include assessment for atrial arrhythmias, paradoxical embolic events and an echocardiogram every 2-3 yearly.
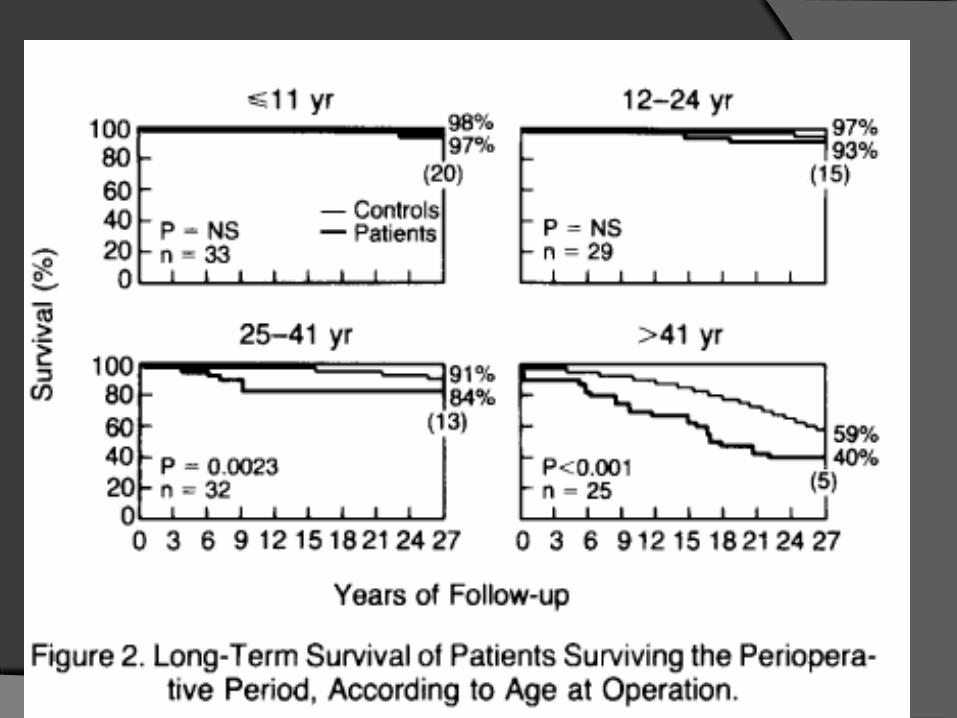
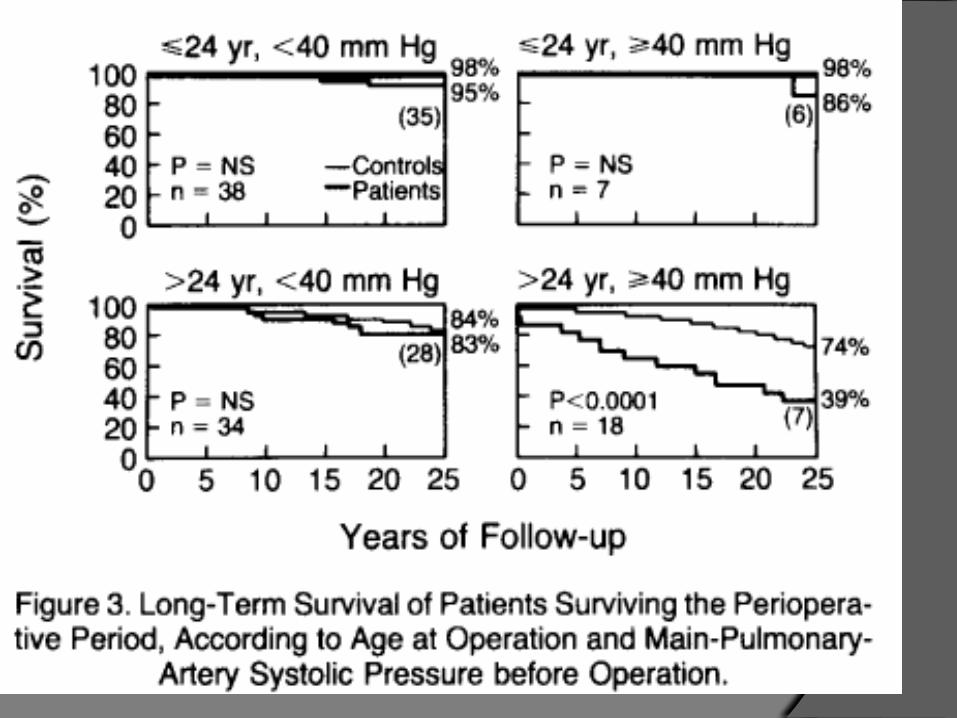
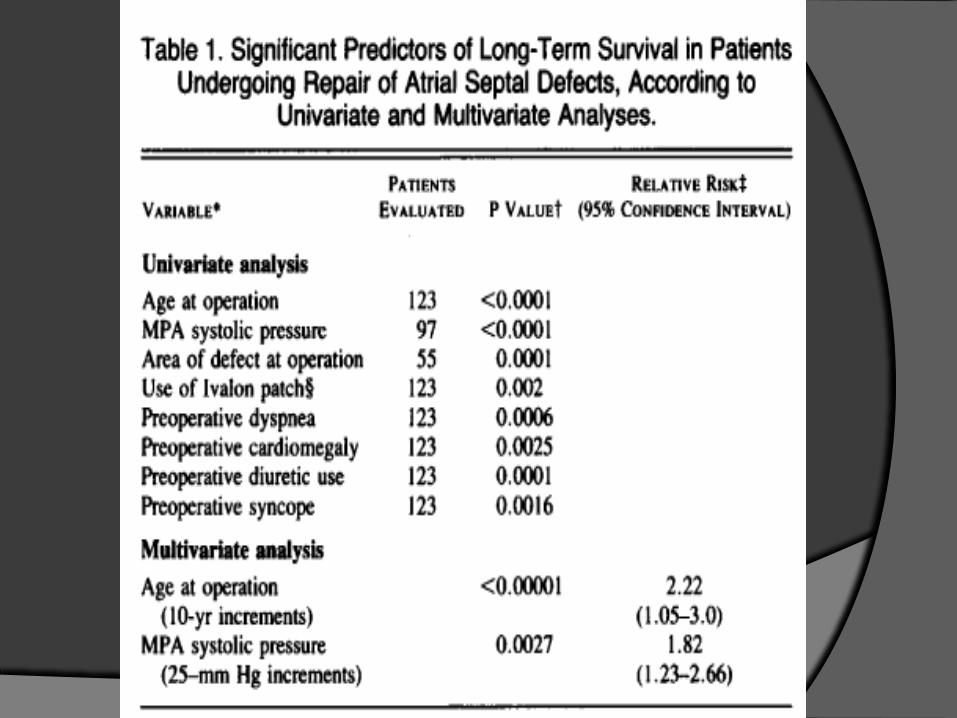
Murphy et al NEJM 1990
123 pts who underwent surgical closure of ASD at MAYO clinic between 1956 – 1960.
F/U: 27 – 32Y Operative mortality: 3.3% Survival
5y: 97% 10y: 90%
15y: 88% 20y: 83%
25y:81% 30y: 74%
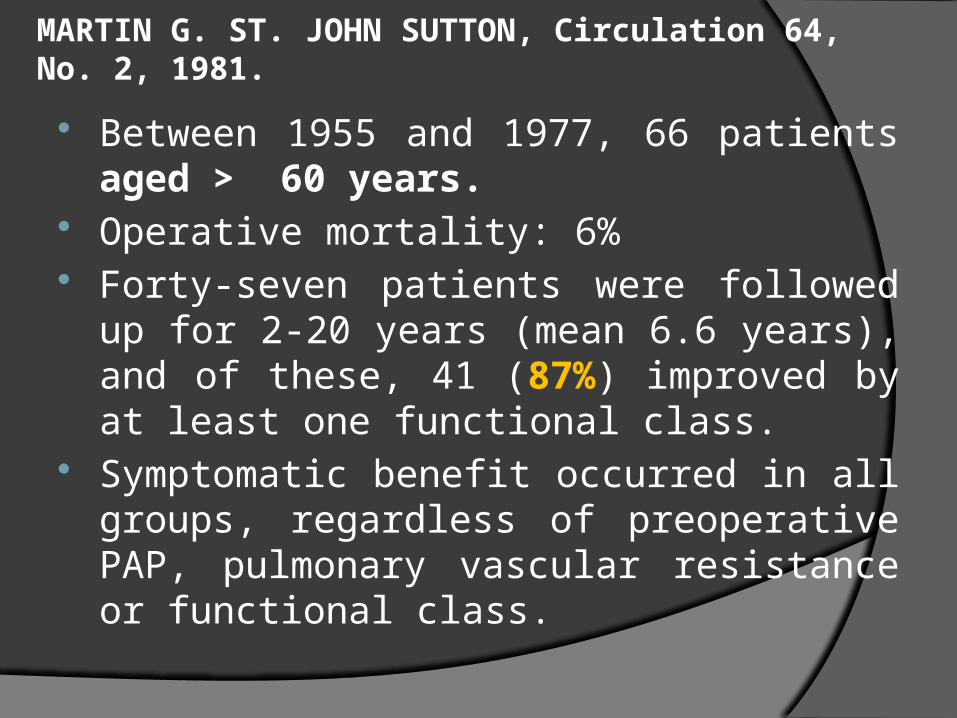
MARTIN G. ST. JOHN SUTTON, Circulation 64, No. 2, 1981.
Between 1955 and 1977, 66 patients aged > 60 years.
Operative mortality: 6% Forty-seven patients were followed up for 2-20
years (mean 6.6 years), and of these, 41 (87%) improved by at least one functional class.
Symptomatic benefit occurred in all groups, regardless of preoperative PAP, pulmonary vascular resistance or functional class.
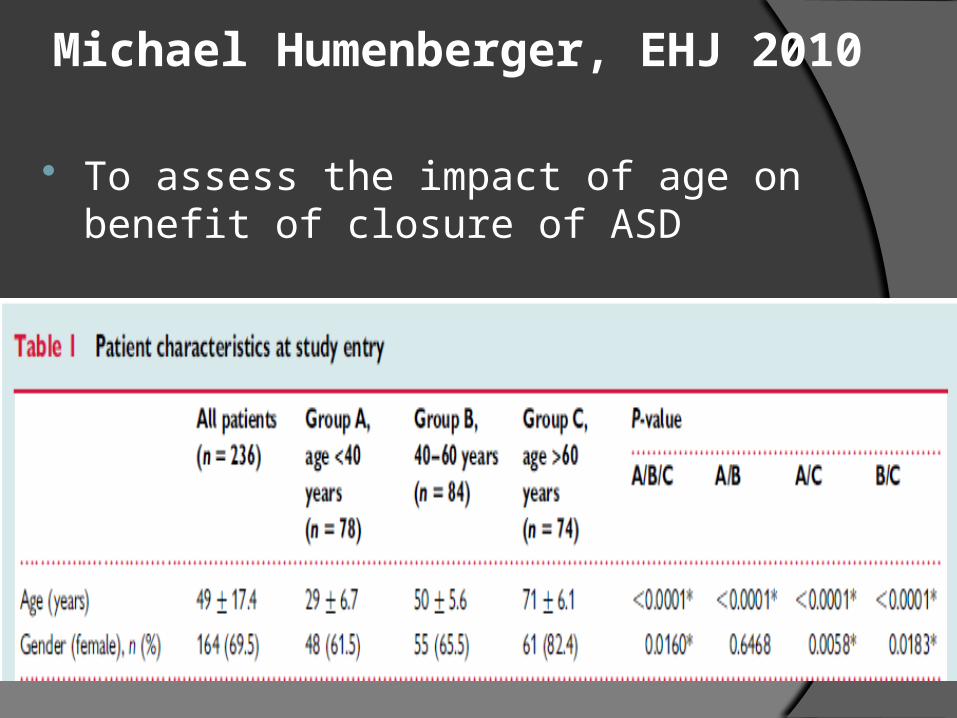
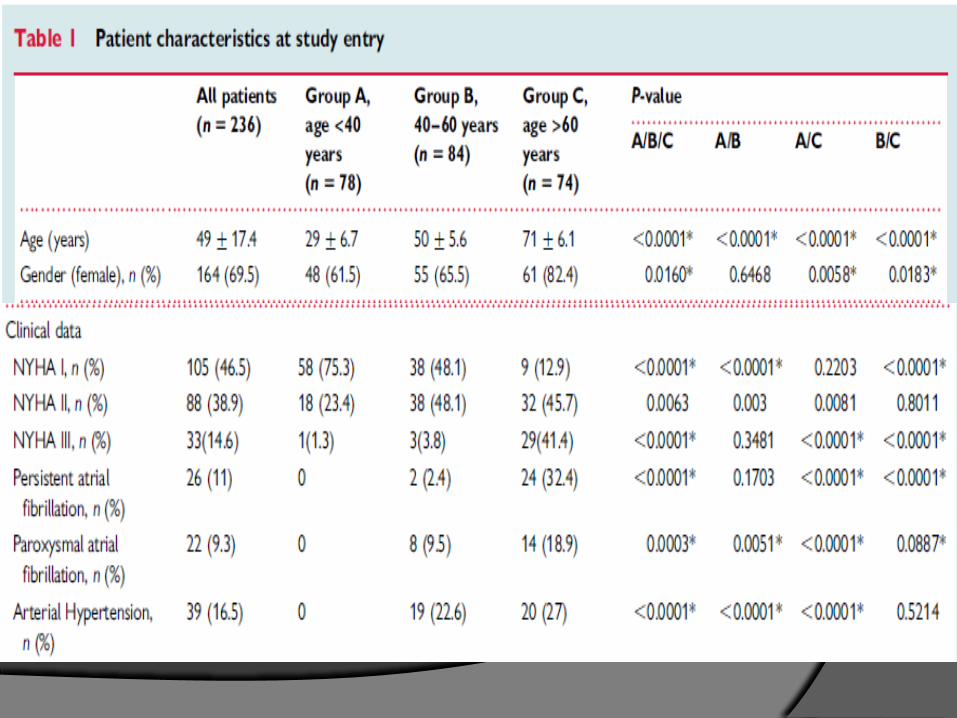
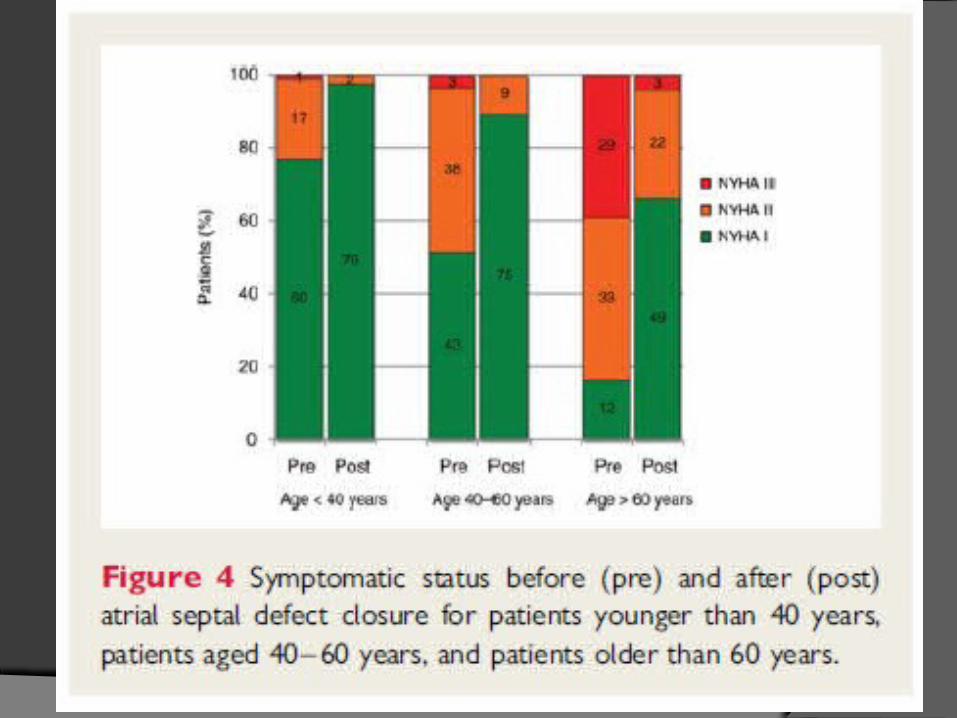
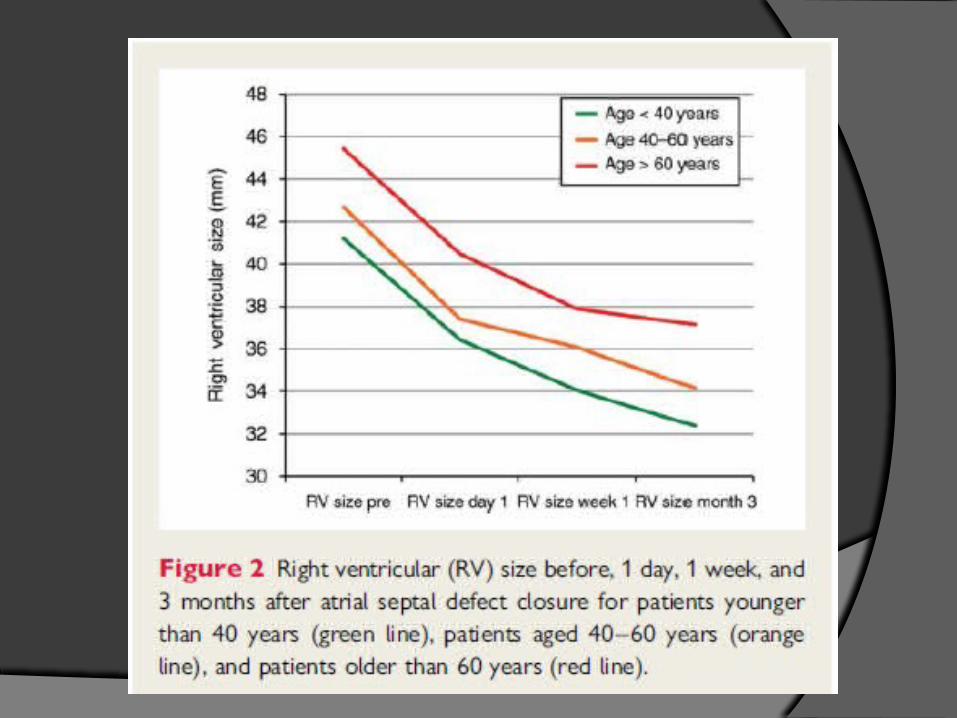
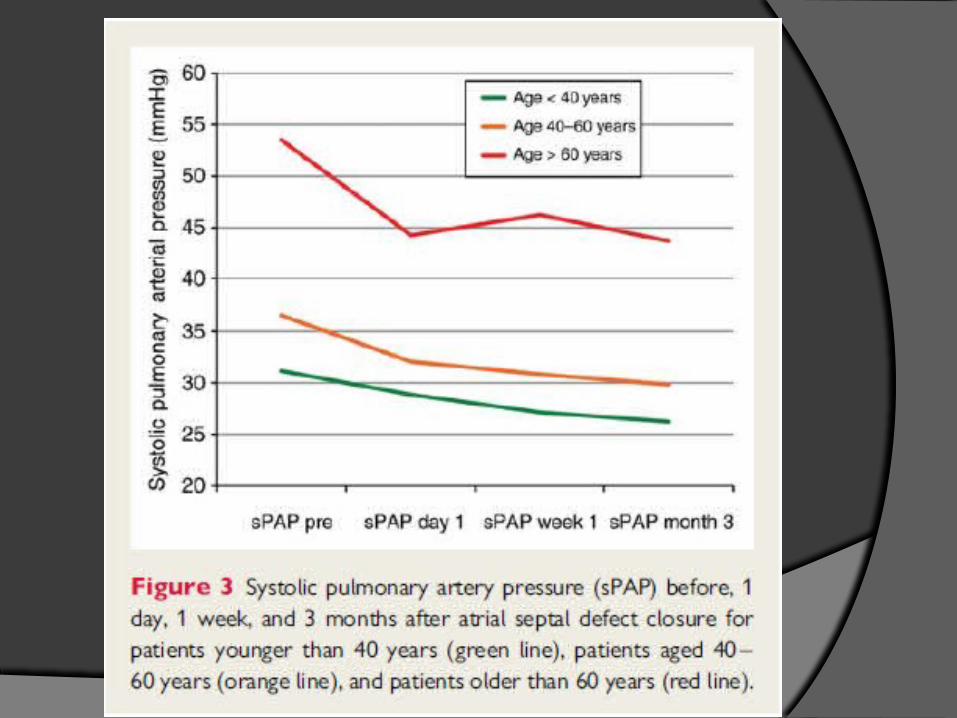
Michael Humenberger, EHJ 2010
To assess the impact of age on benefit of closure of ASD
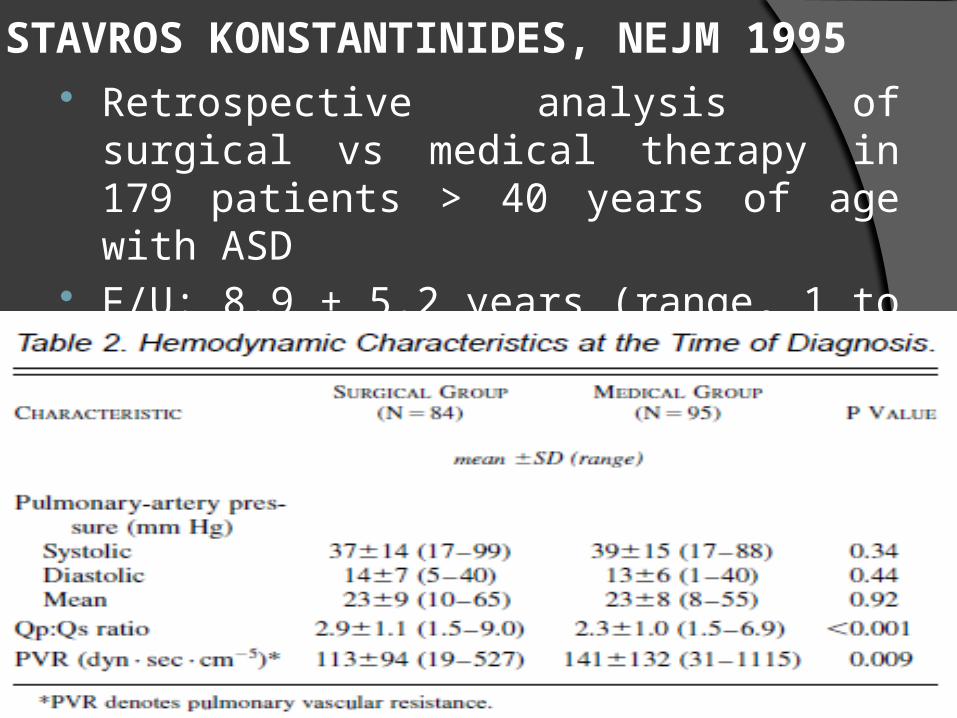
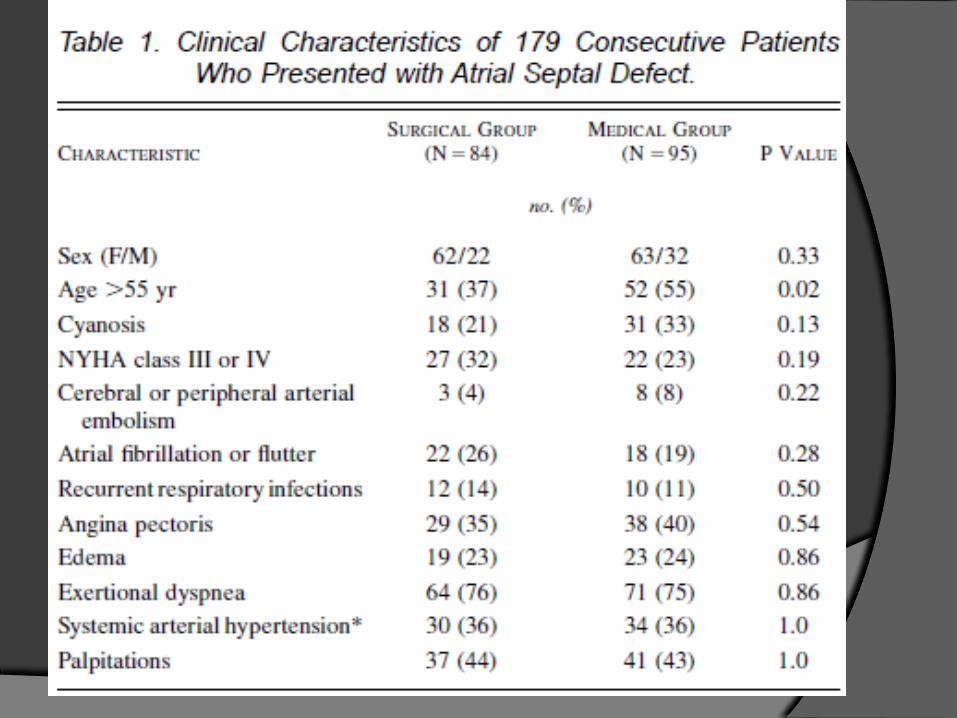
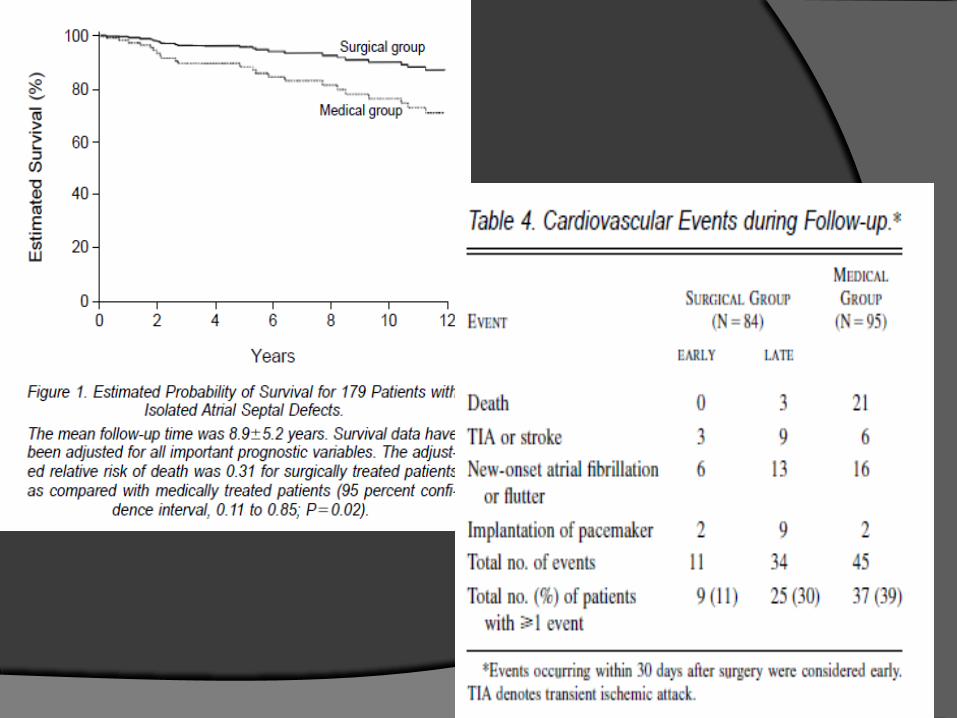
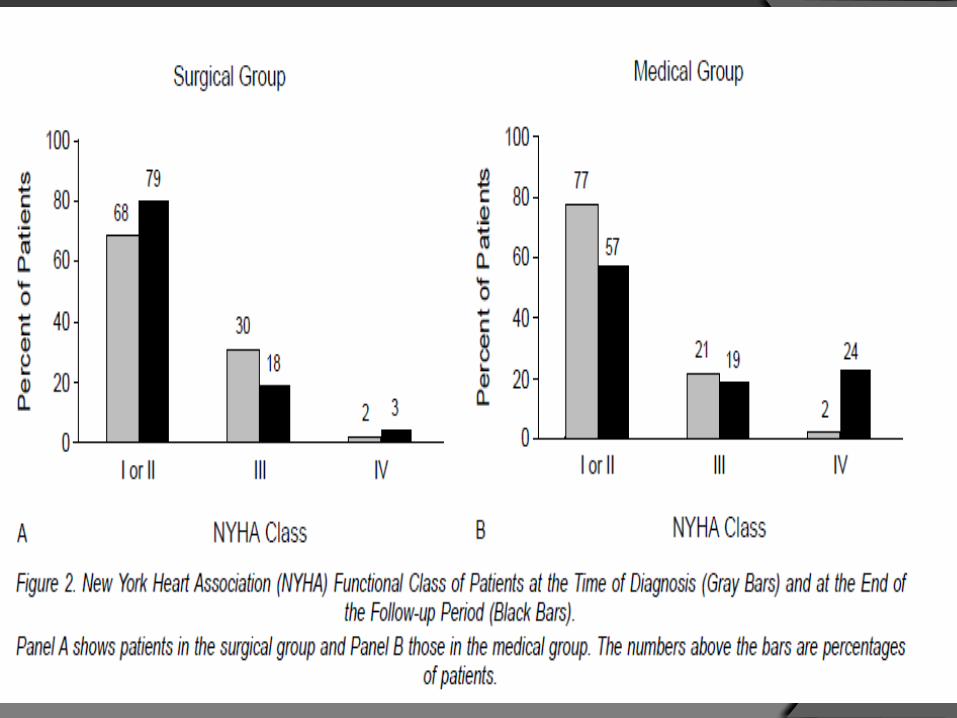
STAVROS KONSTANTINIDES, NEJM 1995 Retrospective analysis of surgical vs medical
therapy in 179 patients > 40 years of age with ASD
F/U: 8.9 ± 5.2 years (range, 1 to 26)
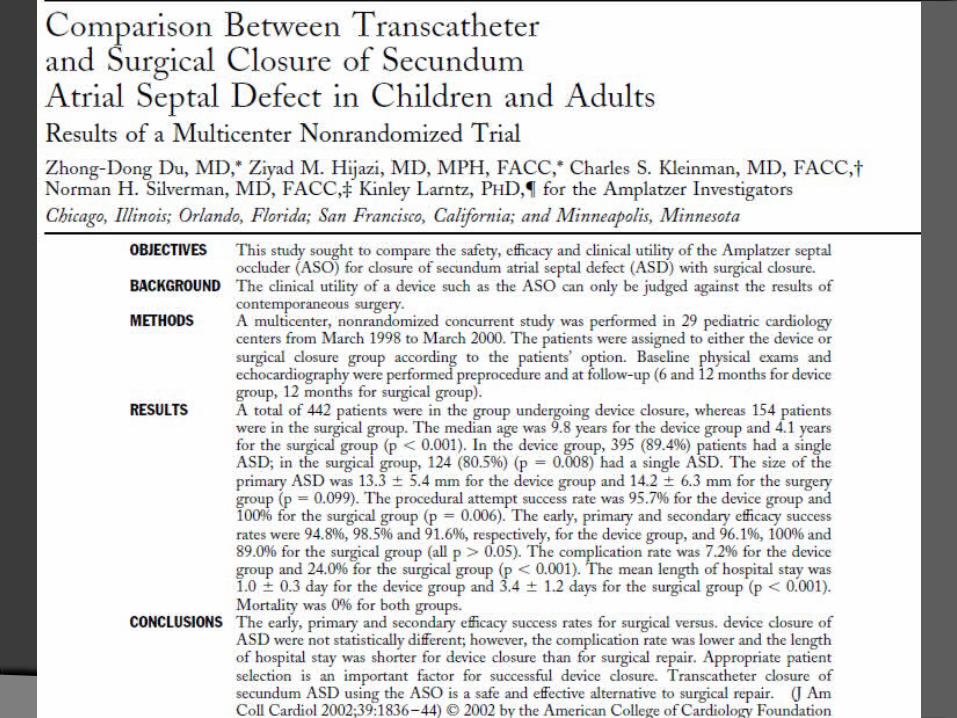
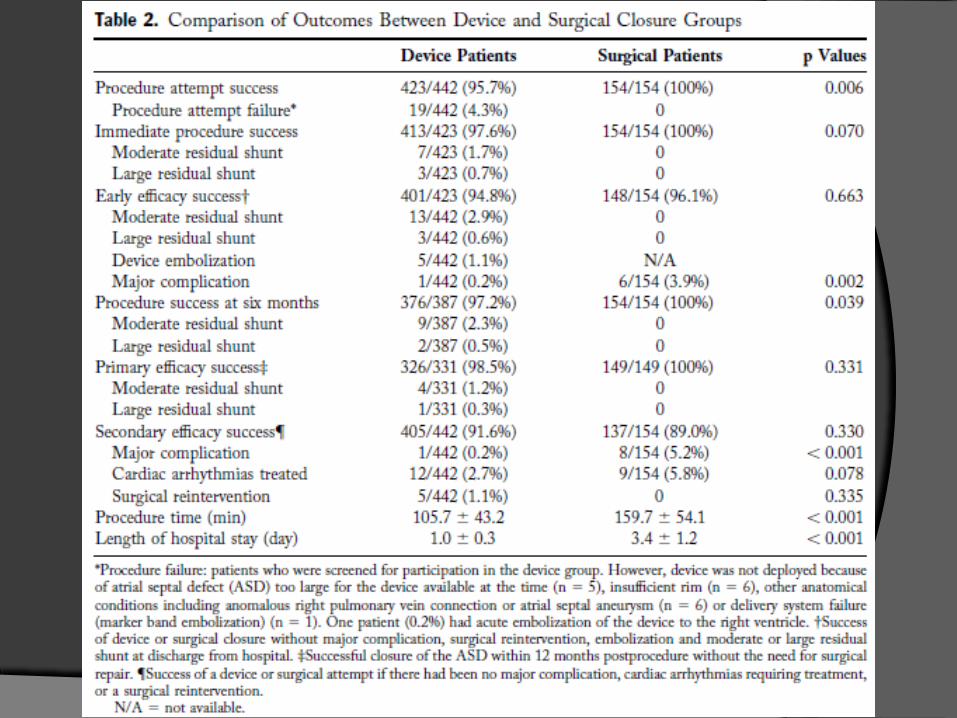
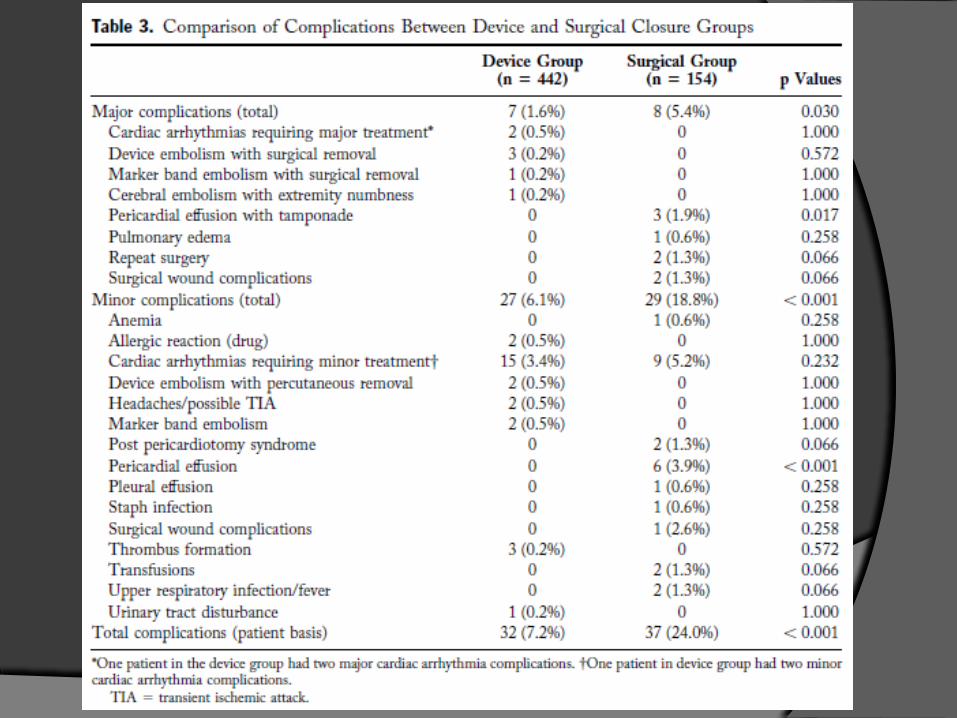
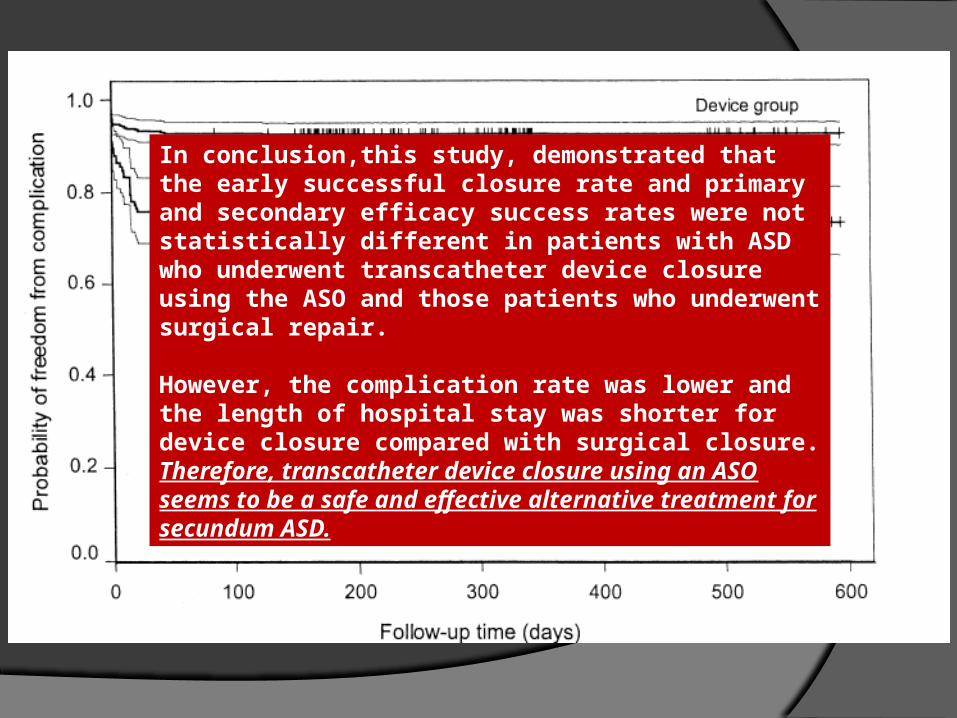
In conclusion,this study, demonstrated that the early successful closure rate and primary and secondary efficacy success rates were not statistically different in patients with ASD who underwent transcatheter device closure using the ASO and those patients who underwent surgical repair.
However, the complication rate was lower and the length of hospital stay was shorter for device closure compared with surgical closure.Therefore, transcatheter device closure using an ASO seems to be a safe and effective alternative treatment for secundum ASD.
TAKE –HOME MESSAGES ASD is a common congenital disorder Ostium secundum is the most common ASD Patient selection is the most important step
in management ACC AHA recommendations should be
followed to decide the management strategy Any kind of closure is safe and effective and
associated with improved life expectancy
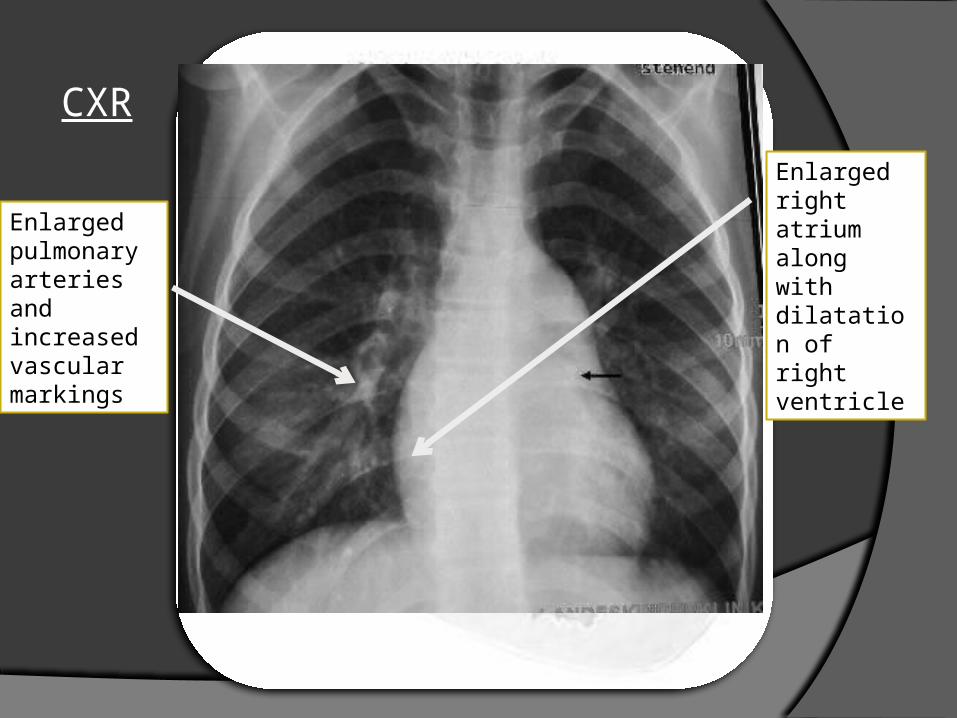
CXR
Enlarged pulmonary arteries and increased vascular markings
Enlarged right atrium along with dilatation of right ventricle
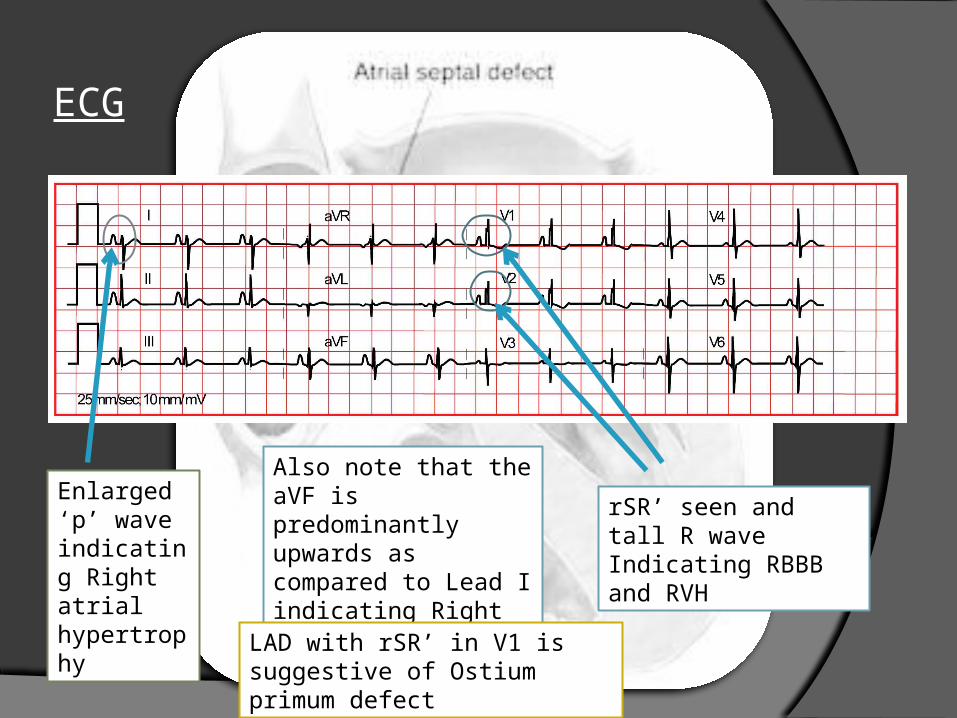
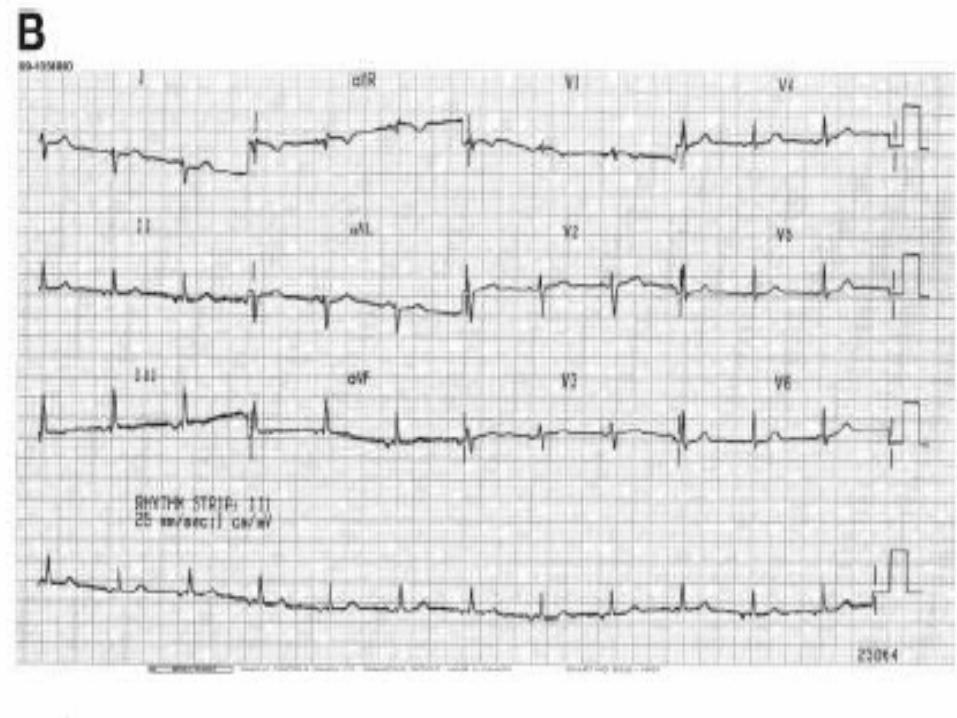
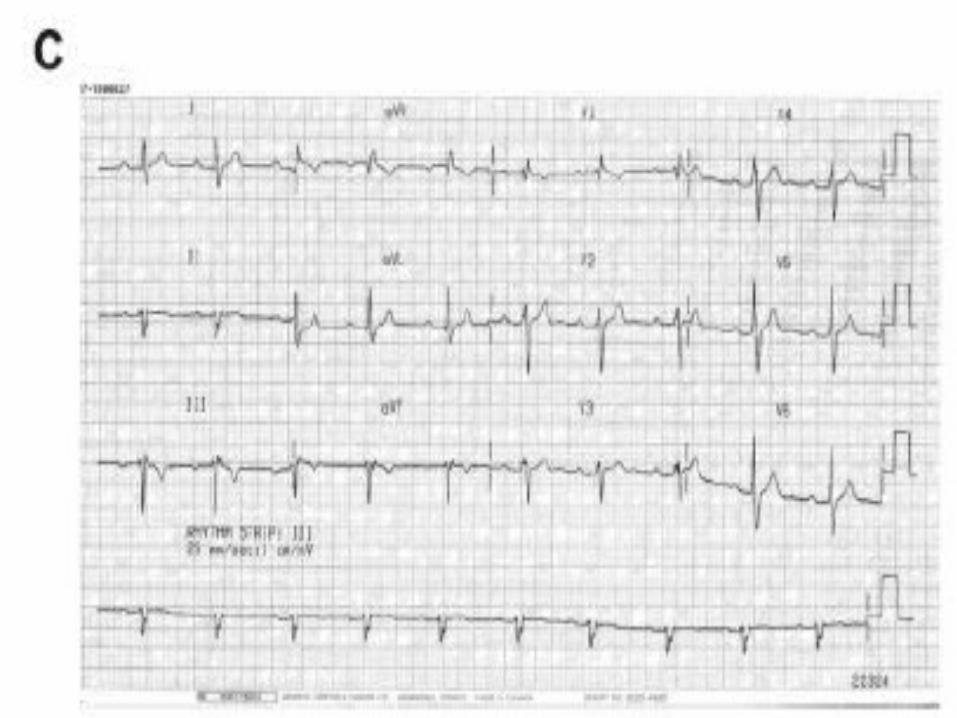
ECG
Enlarged ‘p’ wave indicating Right atrial hypertrophy
rSR’ seen and tall R waveIndicating RBBB and RVH
Also note that the aVF is predominantly upwards as compared to Lead I indicating Right Axis Deviation
LAD with rSR’ in V1 is suggestive of Ostium primum defect
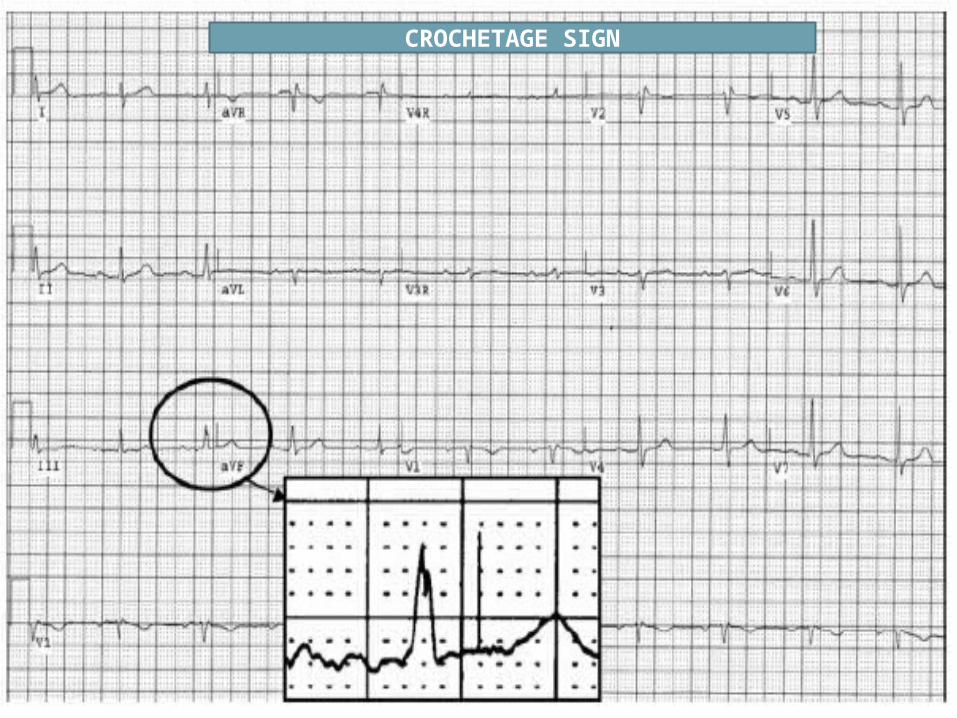
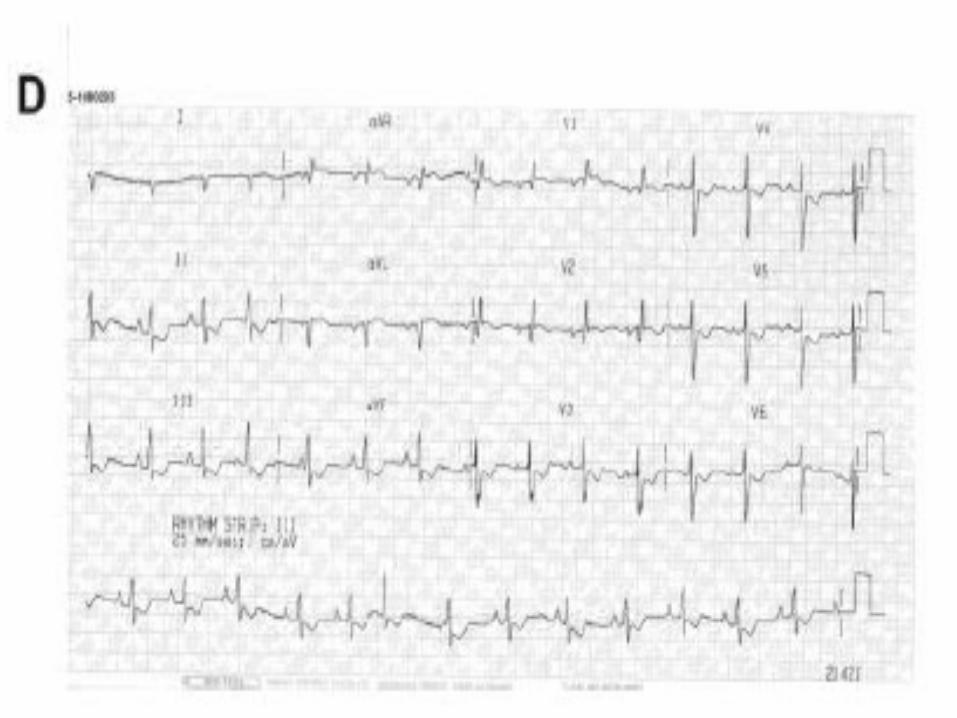
CROCHETAGE SIGN

THANKYOU !!