Embed Size (px)
Citation preview
ALTERED LEVEL OF CONSCIOUSNESS
EMET ProgramDr Ian Turner FACEM

APPROACH
Immediate interventions
Differential diagnoses
Clinical clues to diagnoses
Best initial tests to clarify diagnosis
Diagnostic tests
Definitive Management
CASE 1
74 M from home
Witnessed fall with headstrike when going to bed last night
Now unresponsive
36.3C, HR 62, 155/80, RR 12, SaO2 92%, GCS 6 (M3V2E1), BSL 6

IMMEDIATE INTERVENTIONS
Support/secure airway, protect neck
Optimise SaO2
IV access
DIFFERENTIAL DIAGNOSES
Intracranial bleed
C-spine injury
Aspiration

CLINICAL CLUES
Description of fall
Risk factors for bleed
Signs of head injury
Pupil responses
Localising neurology

INITIAL TESTS
BSL
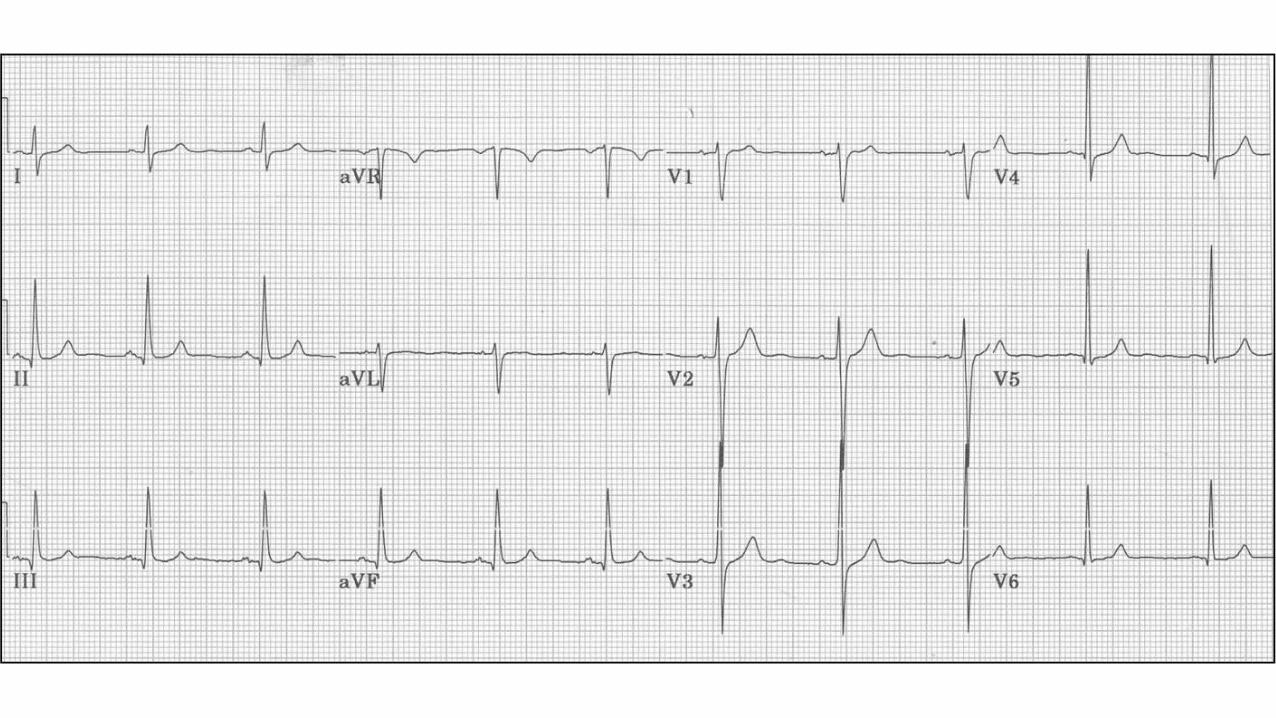
ECG
Blood gas
CXR
BLOOD GAS
pH 7.21
PaCO2 71
PaO2 72
HCO3 27
SaO2 93%



DIAGNOSTIC TESTS
Aetiology of fall – Falls Ix
Sequelae of fall – CT brain, CT C-spine



DEFINITIVE MANAGEMENT
Severe head injury:
Protect airway
Lower ICP – ventilation, mannitol/hypertonic saline, surgery, reverse anticoagulation
Avoid extremes of BP
Protect from further injury – Head up, BSL/temp control, seizure prevention, feed
Aspiration pneumonia/pneumonitis:
ABs
Speech assessment

CASE 2
73 F lives alone
Found by daughter unconscious on floor at home
Recent complaints of abdominal pain and increasing lethargy
38.9C, HR 110, 81/40, RR 18, SaO2 88%, GCS 9 (M4V3E2), BSL HIGH
IMMEDIATE INTERVENTIONS
Support/secure airway
Optimise SaO2
IV fluid

DIFFERENTIAL DIAGNOSES
DKA/HHS
Sepsis – multiple sources to consider: intra-abdo, chest
Intracranial event
Rhabdomyolysis / renal failure
CLINICAL CLUES
Collateral history
Past history – diabetes
Abdominal pain history
Recent infective features

INITIAL TESTS
BSL
Blood gas
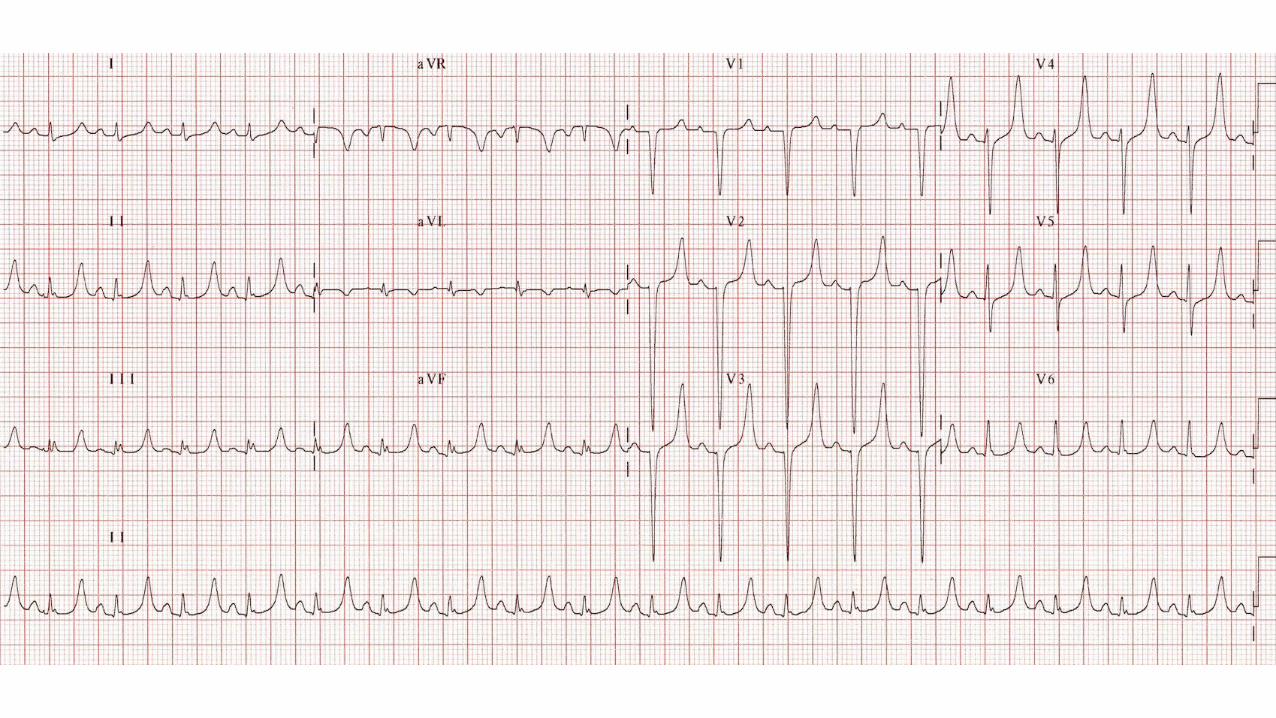
ECG
FWT
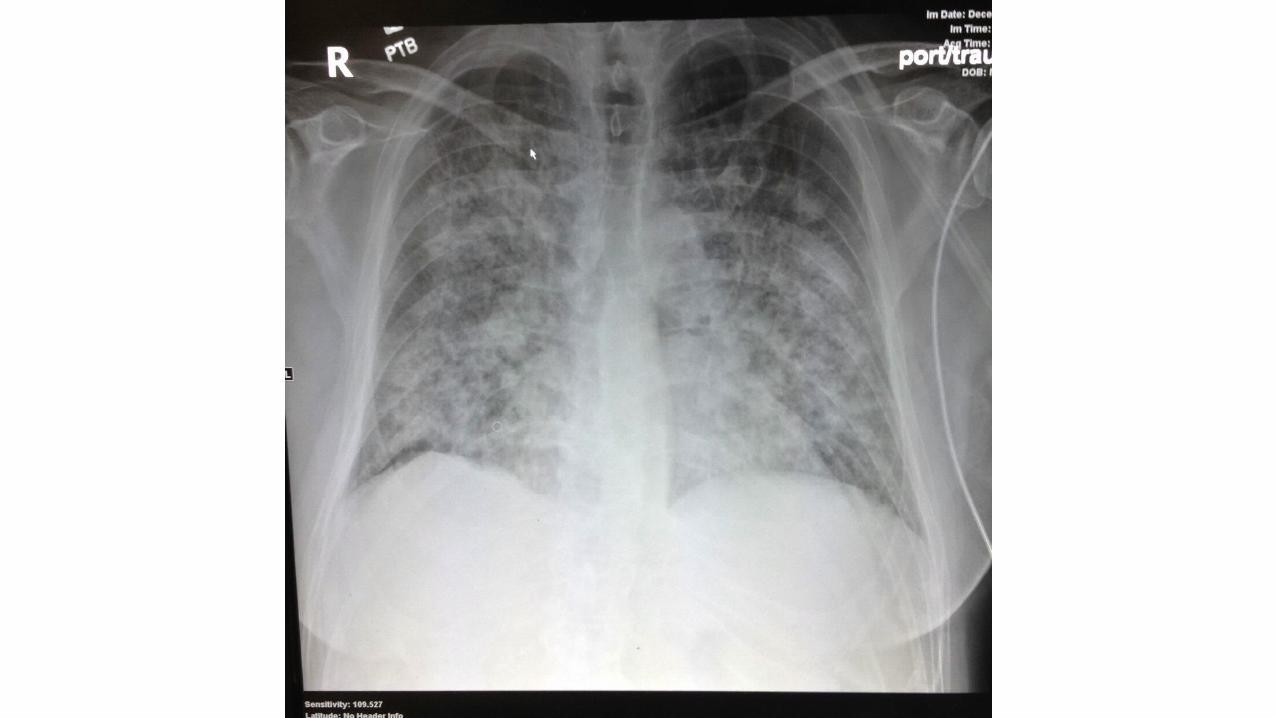
CXR
BLOOD GAS
pH 7.34
PaCO2 42
HCO3 20
Glucose 55
Na 134
Cl 101
K+ 3.2

BLOOD GAS
pH 7.05
PaCO2 66
HCO3 18
Glucose 52
Na 131
Cl 92
K+ 6.0

FWT
No ketones
Blood 2+
No leuks
Glucose 3+
Nitrites NEG

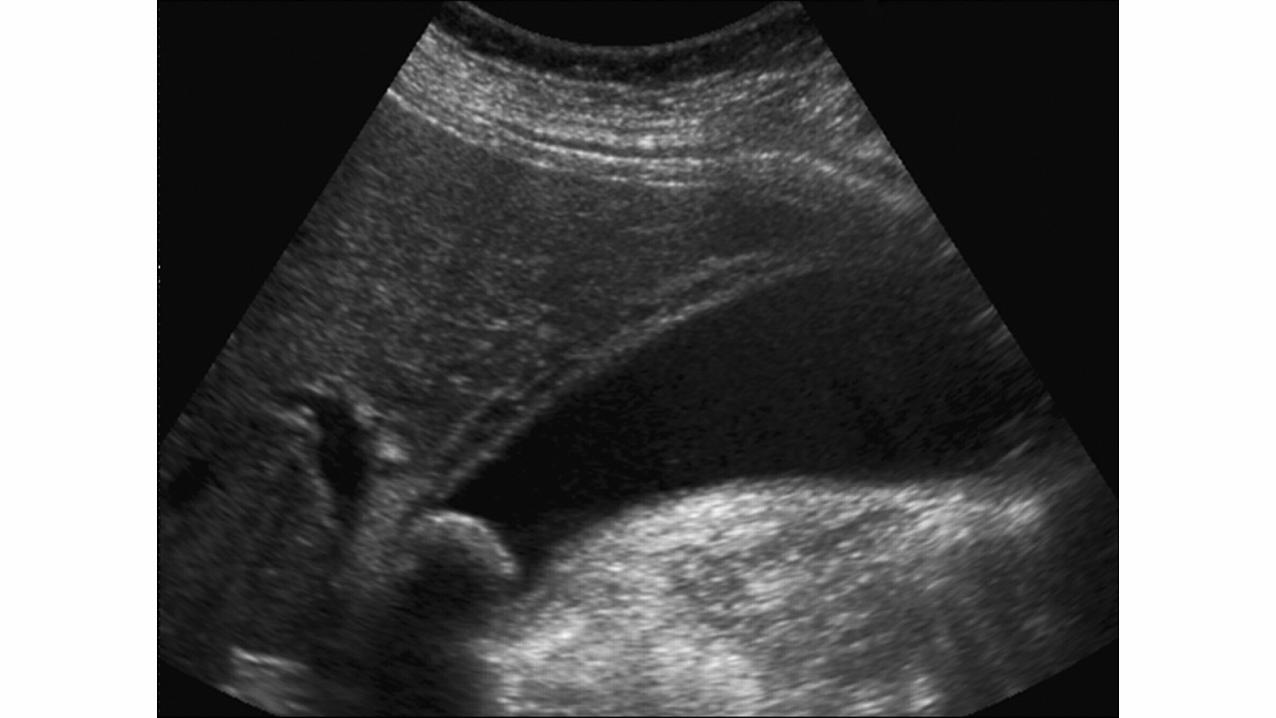
DIAGNOSTIC TESTS
Source identification – CXR, MSU, abdominal imaging
Rhabdomyolysis, renal failure – CK, UEC, coags, FWT
Intracranial pathology – CT


BIOCHEMISTRY
Na 136
K 6.4
Cl 99
HCO3 16
Ur 8.9
Cr 211
CK 11000




DEFINITIVE MANAGEMENT
DKA/HHS:
Fluid resus and replacement, controlled BSL lowering, K+ supplementation
Sepsis:
early antibiotics, vasopressors, source control
Rhabdomyolysis:
aggressive IV fluids, forced diuresis (UO >100mL/hr), electrolyte management
Cholecystitis:
ABs, surgery, CT-guided drainage
Ischaemic gut:
surgery
CASE 3
19 F
Bought to ED by parents
Thin, agitated, confused
39C, HR 125, 152/97, RR 24, SaO2 100%, GCS 13 (M5V4E4), BSL 9

IMMEDIATE INTERVENTIONS
De-escalate
Monitor
Restrain +/- sedate
Sedate +/- restrain
DIFFERENTIAL DIAGNOSES
CNS infection
Toxidrome
Endocrinopathy
Intracranial lesion
Environmental
Psychiatric disorder (+/– in combination with the above)
CLINICAL CLUES
Collateral history
Medication exposures
Toxidrome exam findings

INITIAL TESTS
BSL
Blood gas
ECG
CXR
BLOOD GAS
pH 7.47
PaCO2 30
HCO3 26
Glucose 9
Na 128
Cl 96
K+ 4.6

BLOOD GAS AND BIOCHEMISTRY pH 7.60
PaCO2 41
HCO3 40
Na 119
K 2.1
Cl 67
BSL 6.7



DIAGNOSTIC TESTS
CNS infection – CT/MRI, lumbar puncture
Toxidrome – generally clinical
Endocrinopathy – blood gas, biochemistry
Intracranial lesion – CT/MRI
Psychiatric disorder – clinical picture


LUMBAR PUNCTURE
Colour – mildly turbid
Opening pressure – 220 mm H2O
WCC – 400/mL
RCC – 10/mL
Protein – 1.2g/L (0.18 – 0.45g/L)
CSF glucose – 2.2mmol/L (2.5-3.5mmol/L)
Gram stain – no organisms seen

LUMBAR PUNCTURE
Colour – clear
Opening pressure – 170 mm H2O
WCC – 111/mL
RCC – 8/mL
Protein – 0.75g/L (0.18 – 0.45g/L)
CSF glucose – 3.0mmol/L (2.5-3.5mmol/L)
Gram stain – no organisms seen


DEFINITIVE MANAGEMENT CNS infection:
antibiotics/virals, steroids
Toxidrome:
cease agent, prevent seizures, supportive care
Endocrinopathy:
seek specialist advice
Intracranial lesion:
protect airway, lower ICP, avoid extremes of BP, protect from further injury
Environmental:
control temperature, supportive care, prevent complications
Psychiatric disorder:
determine location of treatment, need for sectioning, CAT review