Embed Size (px)
Citation preview
Be Confident…!!!!
Acid – Base Disturbances
Acid–base imbalance is an abnormality of the human body's normal balance of acids and bases that
causes the plasma pH to deviate out of the normal range (7.35 to 7.45).
Ordinarily, chemical and physiological buffer systems maintain the hydrogen ion concentration of body
fluids within very narrow pH ranges. Abnormal conditions may disturb the acid-base balance. For
example:
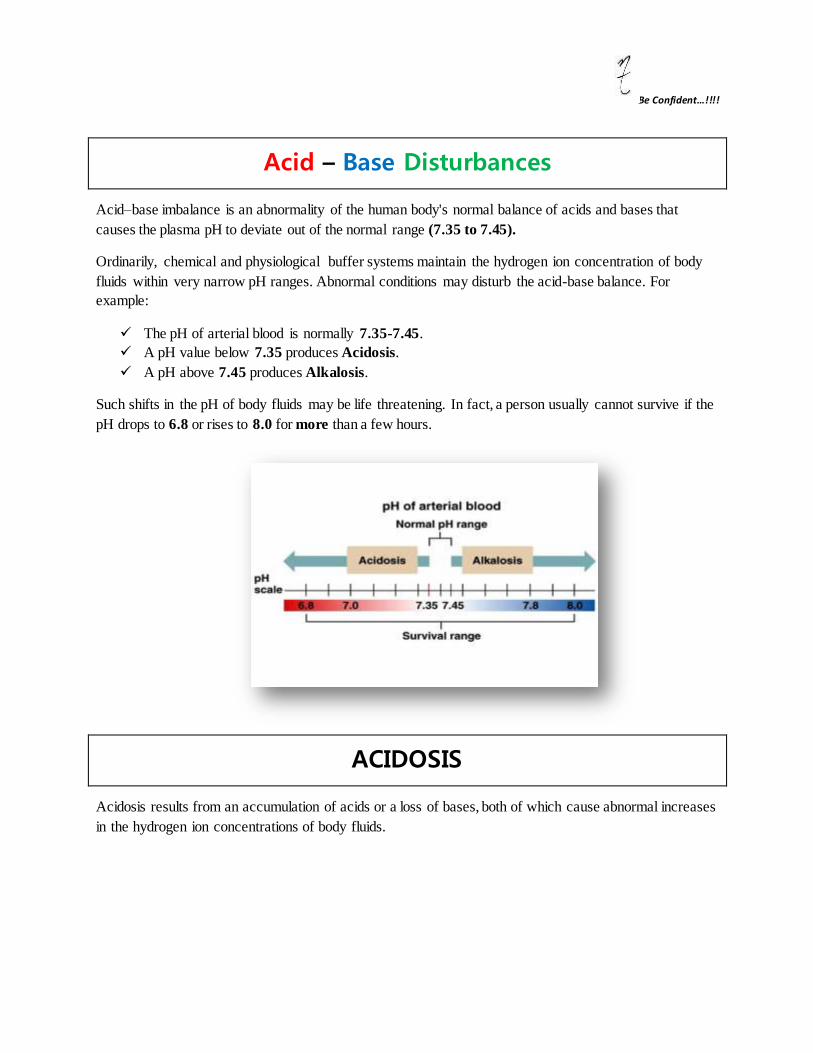
The pH of arterial blood is normally 7.35-7.45.
A pH value below 7.35 produces Acidosis.
A pH above 7.45 produces Alkalosis.
Such shifts in the pH of body fluids may be life threatening. In fact, a person usually cannot survive if the
pH drops to 6.8 or rises to 8.0 for more than a few hours.
ACIDOSIS
Acidosis results from an accumulation of acids or a loss of bases, both of which cause abnormal increases
in the hydrogen ion concentrations of body fluids.

ALKALOSIS
Alkalosis results from a loss of acids or an accumulation of bases accompanied by a decrease in hydrogen
ion concentrations.
TYPES OF DISTRUBANCES
There Are Four Basic Types of Imbalance/Disturbances:
1. Respiratory Acidosis 2. Respiratory Alkalosis 3. Metabolic Acidosis 4. Metabolic Alkalosis
If PaCO2 primarily ↑, pH tends to be ↓— Respiratory Acidosis
If PaCO2 primarily ↓, pH tends to be ↑— Respiratory Alkalosis
If [HCO3-] primarily ↓, pH tends to be ↓— Metabolic Acidosis
If [HCO3-] primarily ↑, pH tends to be ↑— Metabolic Alkalosis
Respiratory Acidosis

Respiratory acidosis is a condition in which a build-up of carbon dioxide in the blood produces a shift in the body's pH balance and causes the body's system to become more acidic.
This condition is brought about by a problem either involving the lungs and respiratory system or signals from the brain that control breathing.
There is primary increase in Pco2 with compensatory increase in HCO3 −; pH usually low but may be near normal. (Ventilatory failure; Respiratory failure; Acidosis – respiratory)
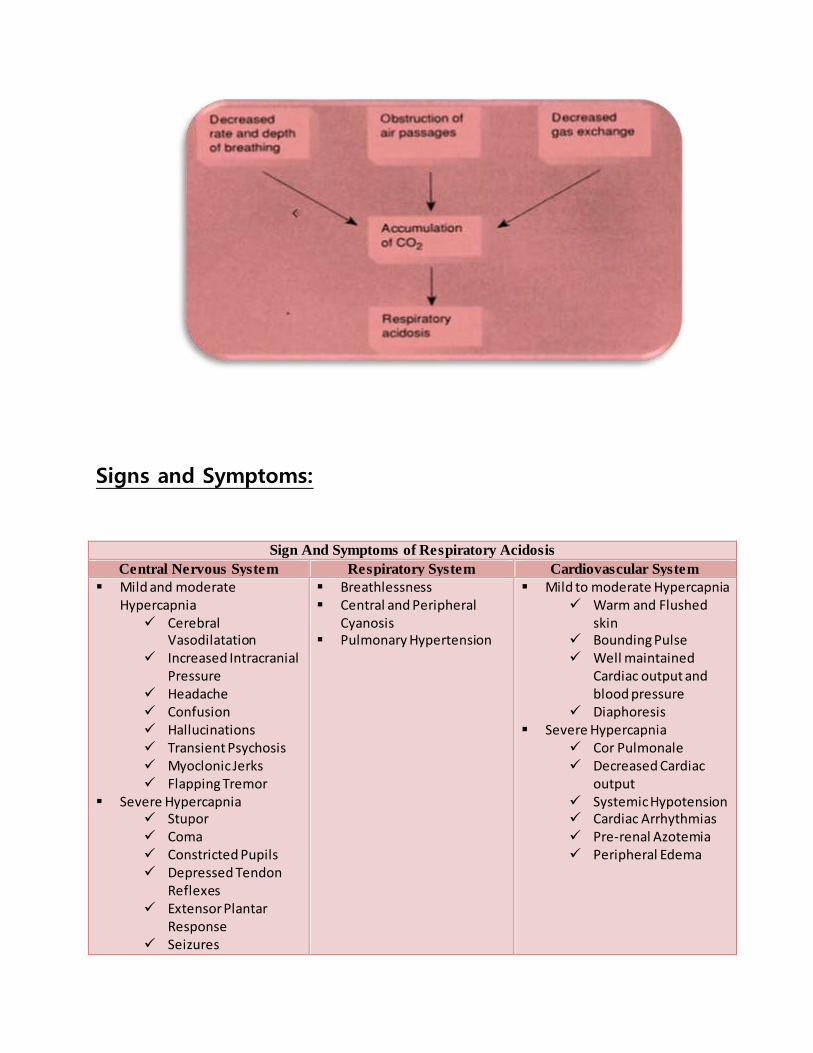
Mechanism:
Carbon dioxide is produced constantly as the body burns energy, and this CO2 will accumulate
rapidly if the lungs do not adequately dispel it through alveolar ventilation.
Alveolar hypoventilation thus leads to an increased PaCO2 (called Hypercapnia). The increase in PaCO2 in turn decreases the HCO3−/PaCO2 ratio and decreases pH resulting respiratory acidosis.
Types of Respiratory Acidosis:

1- Acute Respiratory Acidosis
2- Chronic Respiratory Acidosis
1. Acute Respiratory Acidosis:
Acute respiratory acidosis, the PaCO2 is elevated above the upper limit of the reference range
(over 6.3 kPa or 47 mm Hg) with an accompanying Acidemia (pH <7.35).
Acute respiratory acidosis occurs when an abrupt failure of ventilation occurs. This failure in ventilation may be caused by:
Depression of the central respiratory center by cerebral disease or drugs. Inability to ventilate adequately due to neuromuscular disease (e.g., myasthenia
gravis, amyotrophic lateral sclerosis, Guillain-Barré syndrome, muscular dystrophy). Airway obstruction related to asthma or chronic obstructive pulmonary disease
(COPD) exacerbation.
2. Chronic Respiratory Acidosis:
Chronic respiratory acidosis, the PaCO2 is elevated above the upper limit of the reference
range, with a normal blood pH (7.35 to 7.45) or near-normal pH secondary to renal compensation and an elevated serum bicarbonate (HCO3− >30 mm Hg).
Chronic respiratory acidosis may be secondary to many disorders, including COPD. Hypoventilation in COPD involves multiple mechanisms, including
Decreased responsiveness to hypoxia and Hypercapnia Increased ventilation-perfusion mismatch leading to increased dead space ventilation Decreased diaphragm function secondary to fatigue and hyperinflatio
Chronic respiratory acidosis also may be secondary to: Obesity hypoventilation syndrome (i.e., Pickwickian syndrome) Neuromuscular disorders such as amyotrophic lateral sclerosis Severe restrictive ventilatory defects as observed in interstitial fibrosis and thoracic
deformities
Causes:
Hypoventilation
Diseases of the airways (such as asthma and chronic obstructive lung disease), which send air
into and out of the lungs
Diseases of the chest (such as scoliosis), which make the lungs less efficient at filling and
emptying
Diseases affecting the nerves and muscles that "signal" the lungs to inflate or deflate
Drugs that suppress breathing (including powerful pain medicines, such as narcotics, and
"downers," such as benzodiazepines), especially when combined with alcohol
Severe obesity, which restricts how many the lungs, can expand.
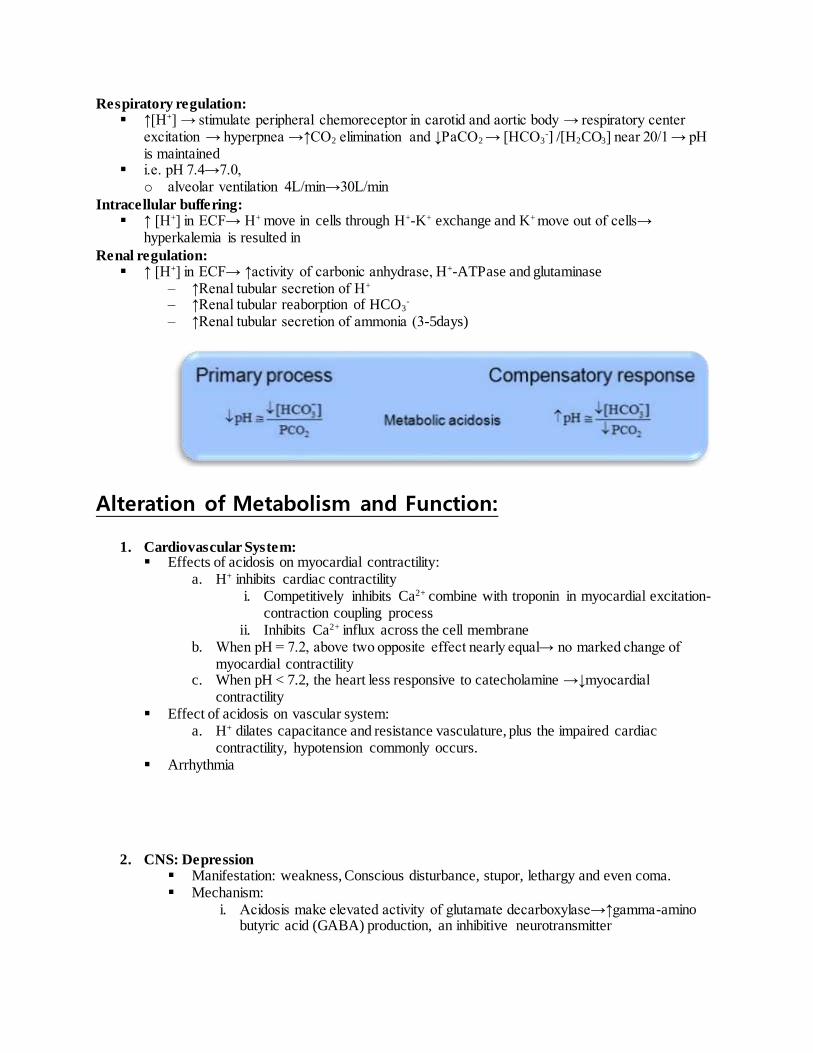
Signs and Symptoms:
Sign And Symptoms of Respiratory Acidosis
Central Nervous System Respiratory System Cardiovascular System
Mild and moderate Hypercapnia
Cerebral Vasodilatation
Increased Intracranial Pressure
Headache Confusion Hallucinations Transient Psychosis Myoclonic Jerks Flapping Tremor
Severe Hypercapnia Stupor Coma Constricted Pupils Depressed Tendon
Reflexes Extensor Plantar
Response Seizures
Breathlessness Central and Peripheral
Cyanosis Pulmonary Hypertension
Mild to moderate Hypercapnia Warm and Flushed
skin Bounding Pulse Well maintained
Cardiac output and blood pressure
Diaphoresis Severe Hypercapnia
Cor Pulmonale Decreased Cardiac
output Systemic Hypotension Cardiac Arrhythmias Pre-renal Azotemia Peripheral Edema

Papilledema
Compensation:
Problem: Increase pCO2 and these results in a decrease blood pH (high H+) [H+] stimulates kidney to generate and retain bicarbonate
Respiratory acidosis is compensated for by the development of a metabolic alkalosis
Compensation is complete ([HCO3] levels out) in 2-4 days
Final HCO3 can be calculated from the following equation: HCO3 mmol/L = 0.44 X pCO2 mmHg + 7.6 (+/-2).
Limit of compensation is a HCO3 of 45 mmol/L
Alteration of Metabolism and Function:
• Also include dysfunction of cardiovascular system and CNS.
• Respiratory acidosis usually has more profound impacts on CNS than metabolic acidosis with the
same plasma pH
– CO2 readily across blood-brain-barrier, and elevated level of CO2 can make
vasodilatation of cerebral blood vessel→↑ cerebral blood volume and intracranial
pressure
– HCO3- is water-soluble, and cannot pass through blood-brain-barrier as easy as CO2→ the
pH value of cerebrospinal fluid in respiratory acidosis is usually lower than that of
metabolic acidosis
RESPIRATORY ALKALOSIS
Respiratory alkalosis is a condition where the amount of carbon dioxide found in the blood drops to a
level below normal range. This condition produces a shift in the body's pH balance and causes the body's
system to become more alkaline (basic). This condition is brought on by rapid, deep breathing called

hyperventilation. There is a primary decrease in Pco2 with or without compensatory decrease in HCO3 −
pH high or near normal. (Alkalosis – respiratory)
Mechanism:
Respiratory alkalosis generally occurs when some stimulus makes a person hyperventilate. The increased
breathing produces increased alveolar respiration, expelling CO2 from the circulation. This alters the
dynamic chemical equilibrium of carbon dioxide in the circulatory system, and the system reacts
according to Le Chatelier's principle. Circulating hydrogen ions and bicarbonate are shifted through the
carbonic acid (H2CO3) intermediate to make more CO2 via the enzyme carbonic anhydrase .The net
result of this is decreased circulating hydrogen ion concentration, and thus increased pH (alkalosis). There
is also a decrease in ionized blood calcium concentration.
Types of Respiratory Alkalosis:
1. Acute Respiratory Alkalosis: It occurs rapidly. During acute respiratory alkalosis, the person may lose consciousness where the rate of
ventilation will resume to normal.
2. Chronic Respiratory Alkalosis: It is a more long-standing condition. For every 10 mM drop in pCO2 in blood, there is a corresponding 5 mM of bicarbonate
ion drop. The drop of 5 mM of bicarbonate ion is a compensation effect which reduces the alkalosis effect of the drop in pCO2 in blood. This is termed metabolic compensation.
Causes:
Hyperventilation

Intracerebral hemorrhage, meningitis, stroke Salicylate and Progesterone drug usage Anxiety, hysteria, stress and pain Cirrhosis of the liver Sepsis Elevated body temperature sexual activity, which may induce excessive breathing due to excitation Hypoxia
Any lung disease that leads to shortness of breath can also cause respiratory alkalosis.
Sign and Symptoms:
SIGN AND SYMPTOMS OF RESPIRATORY ALKALOSIS
Central Nervous System Cardiovascular System Neuromuscular System
Cerebral vasoconstriction Reduction in intracranial
pressure Light-headedness Confusion Increased deep tendon
reflexes Generalized seizures
Chest oppression Angina pectoris Ischemic
electrocardiographic changes Normal or decreased blood
pressure Cardiac arrhythmias Peripheral vasoconstriction
Numbness and paresthesias
of the extremities Circumoral numbness Laryngeal spasm Manifestations of tetany
Muscle cramps Carpopedal spasm Trousseau’s sign

Chvostek’s sign
Compensation:
Problem: decrease pCO2 causing increase blood pH (low H+) Increase pH stimulates the kidney to excrete bicarbonate
o respiratory alkalosis is compensated for by the development of a metabolic acidosis If the condition has been present for 7 days or more full compensation may occur. Compensation is complete ([HCO3] levels out) in 7-10 days. The limit of compensation is a HCO3 of 12 mmol/L
Alteration of Metabolism and Function:
• Similar to that of metabolic alkalosis
• Respiratory alkalosis usually has more profound impacts on CNS than metabolic alkalosis with the same plasma pH
– The decrease in CO2 content of blood causes constriction of cerebral blood vessel→↓
cerebral blood volume and regional cerebral ischemia
METABOLIC ACIDOSIS
Metabolic acidosis results from all conditions that decrease the pH of the body fluids below 7.35, with the exception of conditions resulting from altered function of the respiratory system.
Mechanism:

As hydrogen ions accumulate in the body fluids, buffers first resist a decline in pH. If the buffers cannot compensate for the increase in hydrogen ions, the respiratory center helps regulate the body fluid pH. The reduced pH stimulates the respiratory center, which causes hyperventilation. During hyperventilation, carbon dioxide is eliminated at a greater rate. The elimination of carbon dioxide also eliminates excess hydrogen ions and helps maintain the pH of the body fluids within a normal range.
If metabolic acidosis persists for many hours and if the kidneys are functional, the kidneys can also help compensate for metabolic acidosis. They begin to secrete hydrogen ions at a greater rate and increase the rate of bicarbonate ion reabsorption. Symptoms of metabolic acidosis appear if the respiratory and renal systems are not able to maintain the pH of the body fluids within its normal range.
Causes:
• Central change: ↓ [HCO3-]
1. Direct excessive loss of HCO3- :
i. Diarrhea, intestinal suction or intestinal or biliary fistula ii. Proximal renal tubular acidosis
a. caused by impaired reabsorption of HCO3- in the proximal tubule
iii. Treatment with carbonic anhydrase inhibitor 2. Indirect loss of HCO3
- for buffering increased nonvolatile acid i. Excessive intake of nonvolatile acid:
a. acetylsalicylic acid (aspirin) b. Methanol c. Ammonium chloride
ii. Excessive production of nonvolatile acid: a. Lactic acidosis
Hypoxia Shock, cardiac arrest, severe anemia, pulmonary edema, carbon
monoxide poisoning Severe liver dysfunction
b. Ketoacidosis Diabetes alcoholism Fasting and starvation
iii. Decreased renal excretion of acid: a. Renal dysfunction b. Distal renal tubular acidosis caused by reduced H+ secretion in the distal nephron
Types of Metabolic Acidosis:
1. Increased AG type Caused by increased nonvolatile acids, but the fixed acids containing chloride are
excluded.
2. Normal AG type Direct loss of HCO3-

Excessive intake of acidic salt containing chloride
Sign And Symptoms:
SIGNS AND SYMPTOMS OF METABOLIC ACIDOSIS
Respiratory
System
Cardiovascular
System
Metabolism Central
Nervous
System
Skeleton
Respiratory distress and dyspnea
Decreased strength of respiratory muscles and promotion of muscle fatigue
Impairment of cardiac contractility, arteriolar dilation, vasoconstriction
Reductions in cardiac output, arterial blood pressure, and hepatic and renal blood flow
Sensitization to reentrant arrhythmias and reduction in threshold for ventricular fibrillation
Increased sympathetic discharge but attenuation of cardiovascular responsiveness to catecholamines
Increased metabolic demands
Insulin resistance
Inhibition of anaerobic glycolysis
Reduction in adenosine triphosphate synthesis
Hyperkalemia Increased
protein degradation
Impaired metabolism
Inhibition of cell volume regulation
Progressive obtundation
Coma
Osteomalacia Fractures
Compensation: Blood buffering:
Increased H+ is combined immediately by the base salt of bicarbonate and non-bicarbonate buffer system
H++HCO3-→H2CO3→CO2+H2O
Respiratory regulation: ↑[H+] → stimulate peripheral chemoreceptor in carotid and aortic body → respiratory center
excitation → hyperpnea →↑CO2 elimination and ↓PaCO2 → [HCO3-] /[H2CO3] near 20/1 → pH
is maintained i.e. pH 7.4→7.0,
o alveolar ventilation 4L/min→30L/min
Intracellular buffering: ↑ [H+] in ECF→ H+ move in cells through H+-K+ exchange and K+ move out of cells→
hyperkalemia is resulted in
Renal regulation: ↑ [H+] in ECF→ ↑activity of carbonic anhydrase, H+-ATPase and glutaminase
– ↑Renal tubular secretion of H+ – ↑Renal tubular reaborption of HCO3
- – ↑Renal tubular secretion of ammonia (3-5days)
Alteration of Metabolism and Function:
1. Cardiovascular System: Effects of acidosis on myocardial contractility:
a. H+ inhibits cardiac contractility i. Competitively inhibits Ca2+ combine with troponin in myocardial excitation-
contraction coupling process ii. Inhibits Ca2+ influx across the cell membrane
b. When pH = 7.2, above two opposite effect nearly equal→ no marked change of myocardial contractility
c. When pH < 7.2, the heart less responsive to catecholamine →↓myocardial contractility
Effect of acidosis on vascular system: a. H+ dilates capacitance and resistance vasculature, plus the impaired cardiac
contractility, hypotension commonly occurs. Arrhythmia
2. CNS: Depression Manifestation: weakness, Conscious disturbance, stupor, lethargy and even coma. Mechanism:
i. Acidosis make elevated activity of glutamate decarboxylase→↑gamma-amino butyric acid (GABA) production, an inhibitive neurotransmitter

ii. Acidosis makes decreased activity of biological oxidases in
mitochondria→↓ATP production in brain.
METABOLIC ALKOLOSIS
Metabolic alkalosis refers to primary increase in plasma HCO3- concentration, the pH tends to be
increased.
Causes:
Central change: ↑ [HCO3-]:
• Excessive gain of HCO3- :
Excessive ingestion of NaHCO3 Infusion of large amounts of stocked blood (full of citrate)
• Excessive loss of H+ : excessive loss of H+ via stomach
o Vomiting, gastric suction excessive loss of H+ via kidney
o Aldosteronism(↑ADS), cushing’s syndrome (↑glucocorticoid) o Thiazide and loop diuretics
hypokalemia
• Volume contraction: Volume contraction→plasma HCO3
- concentrated → contraction alkalosis Loss of body fluid Diuretic therapy
Sign and Symptoms:
SIGNS AND SYMPTOMS OF METABOLIC
Central
Nervous System
Headache, Lethargy, Stupor Delirium, Tetany, Seizures Potentiation of hepatic encephalopathy
Cardiovascular System
Supraventricular and ventricular arrhythmias Potentiation of digitalis toxicity Positive inotropic ventricular effect
Respiratory System Hypoventilation with attendant Hypercapnia and hypoxemia
Neuromuscular System
Chvostek’s sign, Trousseau’s sign Weakness (severity depends on degree of potassium depletion)
Metabolic Effects
Increased organic acid and ammonia production Hypokalemia, Hypocalcemia, Hypomagnesemia Hypophosphatemia
Renal (Associated Potassium Depletion)
Polyuria, Polydipsia Urinary concentration defect Cortical and medullary renal cysts
Compensation:

• Blood buffering – During metabolic alkalosis, ↓[H+]ECF and ↑ [OH-]ECF→ OH- can be buffered by weak
acids, such as H2CO3→↑ [HCO3-]
• Ion exchange between intra- and extra-cell – In alkalosis, ↓[H+]ECF →through H+- K+ exchange, H+ shift out of cells and K+shift into
cells→hypokalemia
• Respiratory regulation – ↓[H+] →inhibition of respiratory center →↓alveolar ventilation→ ↑PaCO2 or [H2CO3] →
[HCO3-]/ [H2CO3] approach 20/1
– Respiratory regulation is limited and seldom make complete compensation • ↓Alveolar ventilation → ↑ PaCO2 →but when PaCO2 >60mmHg, respiratory
center is excited→respiration deepen and quicken→↑CO2 expiration
so compensatory limit of secondary increase of PaCO2 is 55mmHg
• Renal regulation – ↓[H+] → ↓the activity of carbonic anhydrase and glutaminase in renal tubular cell → ↓
renal secretion of H+ and ammonia, ↓renal reabsorption of HCO3- →↓ [HCO3- ] in plasma→ [HCO3
-]/ [H2CO3] approach 20/1 – The increased renal excretion of HCO3- peaks at 3-5 days, so this regulation is not useful
for acute metabolic alkalosis.
Alteration of Metabolism and Function:
• Mild metabolic alkalosis—asymptomatic or manifestation unrelated with alkalosis • Severe metabolic alkalosis—many alterations of metabolism and function
1. Dysfunction of CNS: Hyperexcitability Manifestation: Dysphoria, mental confusion Mechanism:
– ↑pH→↑the activity of gamma-aminobutyric acid transaminase (↑decomposition of GABA) and ↓the activity of glutamate decarboxylase (↓production of GABA)→↓GABA( a inhibitory neurotransmitter) → hyperexcitability of CNS
– ↑pH→ left-shift of oxygen-Hb dissociation→cerebral hypoxia

2. Left-shift of oxygen-Hb dissociation: Left-shift of oxygen-Hb dissociation curve→ O2 saturation of Hb increase at
the same PaO2→releasing of O2 bound by Hb in tissue decrease → tissue hypoxia is resulted in.
3. Hypocalcemia:
Manifestation: tetany, carpopedal spasm, convulsion Mechnism:
o Free Ca2++ abumin combined ca2+ 4. Hypokalemia:
Mechanism o alkalosis→H+ shift out of cells and K+ shift into cells through H+-K+
exchange o alkalosis→↓renal excretion of H+ and ↑renal excretion of K+
References:
1- http://www.mhhe.com/biosci/ap/foxhumphys/student/olc/u-reading5.html
2- http://www.authorstream.com/Presentation/ADahal-400878-respiratory-acidosis-alkalosis-
education-ppt-powerpoint/ 3- file:///C:/Users/Nayyab/Downloads/Documents/adk1_06.pdf