Embed Size (px)
Citation preview
Critical Care Medicine
Apollo Hospitals
Chennai
Ramesh Venkataraman, AB(Int Med), AB (CCM)
Consultant, Critical Care Medicine
Department of Critical Care Medicine, Apollo Hospitals
Apollo Hospitals
Understanding Acid-Base Disturbances – Gaps, Deficits and Differences
Department of Critical Care Medicine, Apollo Hospitals
Understanding Acid-base
Three approaches
Conceptual evolution
Limitations
Comparison
Understanding acid-base
Relative diagnostic efficacy
Prognostic value
Conclusion
Department of Critical Care Medicine, Apollo Hospitals
Bronsted-Lowry Theory (1923)
Acid - a substance which
donates a hydrogen ion
Volatile vs. Non volatile
(Carbonic vs. Noncarbonic)
Base – a substance which
accepts the H+ from the acid
Acid vs. Base

Department of Critical Care Medicine, Apollo Hospitals
Acid Homeostasis
Noncarbonic acid
(Metabolic)
Dissolved CO2 + H2O ↔ H2CO3 ↔ HCO3- + H+
Carbonic Acid
(Respiratory)

Department of Critical Care Medicine, Apollo Hospitals
Henderson-Hasselbalch equation
pH = 6.10+log([HCO3
-]/0.03xPCO2)
Simplified into the Henderson equation
[H+] = 24 x (PCO2 /[HCO3
-])
Physiologic approach
1. Acid base status determined by net H+ balance
2. Blood pH determined by
PaCO2 – Respiratory component
Bicarbonate – Metabolic component
3. Uses only carbonic acid/bicarbonate buffer system

Department of Critical Care Medicine, Apollo Hospitals
Primary Disorder And Compensation
Increased Acid – Acidemia
Metabolic – Decreased Bicarbonate
Respiratory – Increased Carbonic acid (PCO2)
Increased Alkali – Alkalemia
Metabolic – Increased Bicarbonate
Respiratory – Decreased Carbonic acid (PCO2)
Dissolved CO2 + H2O ↔ H2CO3 ↔ HCO3- + H+
PCO2 and Bicarbonate go in the same direction in case of
compensation

Department of Critical Care Medicine, Apollo Hospitals
Metabolic Acidosis
Normal
Na
K
Cations
Cl
HCO3
Anions
Prot
PO4
Na
K
Cations
Cl
HCO3
Anions
Prot
PO4 AG
Na
K
Cations
Cl
HCO3
Anions
Prot
PO4 AG AG
High AG acidosis Normal AG acidosis
Department of Critical Care Medicine, Apollo Hospitals
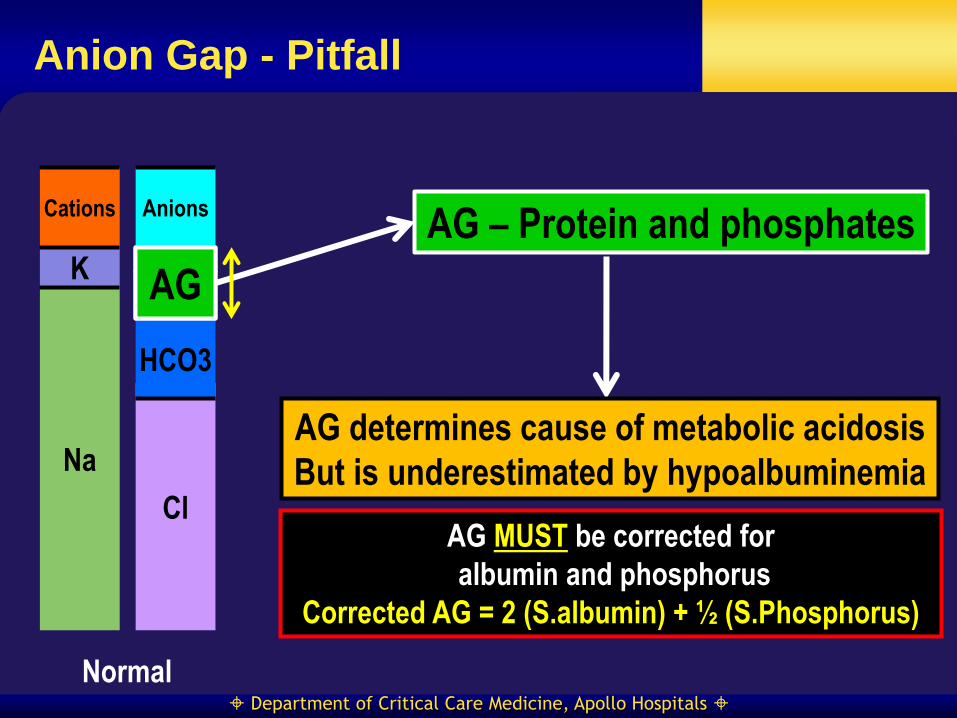
Anion Gap - Pitfall
AG – Protein and phosphates
AG MUST be corrected for
albumin and phosphorus
Corrected AG = 2 (S.albumin) + ½ (S.Phosphorus)
AG determines cause of metabolic acidosis
But is underestimated by hypoalbuminemia
Normal
Na
K
Cations
Cl
HCO3
Anions
Prot
PO4
AG

Department of Critical Care Medicine, Apollo Hospitals
Is bicarbonate a good indicator?
Metabolic derangement
Change in bicarbonate
Change in alveolar ventilation
Altered renal
acidification Altered
HCO3/CO2
equilibrium
Bicarbonate doesn’t accurately reflect
the degree of primary metabolic derangement
Kurtz I et al: Am J Physiol Renal Physiol
294: (2008) F1009 – F1031

Department of Critical Care Medicine, Apollo Hospitals
(Un)Physiological Approach?
Plasma bicarbonate affected by changes in PaCO2
One component influences other
“Standard” bicarbonate calculation
Sustained changes in PaCO2 modify renal
acidification
Chronic hypercapnia increases plasma bicarbonate
Failure of quantitation of buffers other than
bicarbonate
Isohydric principle
Level of bicarbonate qualitatively reflects status of all buffers
Quantifies magnitude but no insight into cause

Department of Critical Care Medicine, Apollo Hospitals
Base Excess Approach
Also advocates centrality of H+/ HCO3-
Base excess - metabolic component Assumes 100% oxygenation, 37oC and PCO2 40mmHg
Measure of the contribution of all the ECF buffers
INDEPENDENT of respiratory component
Three relevant acid-base variables
pH
PCO2
Base Excess (BE)
Department of Critical Care Medicine, Apollo Hospitals
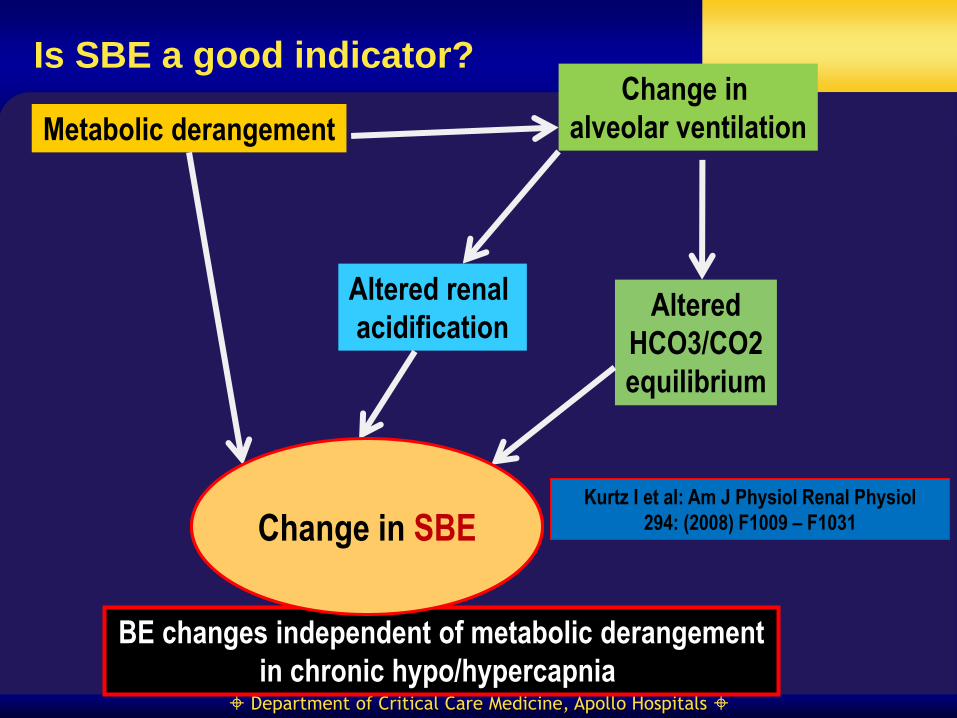
Is SBE a good indicator?
Metabolic derangement
Change in BE
Change in
alveolar ventilation
Altered renal
acidification Altered
HCO3/CO2
equilibrium
BE changes independent of metabolic derangement
in chronic hypo/hypercapnia
Kurtz I et al: Am J Physiol Renal Physiol
294: (2008) F1009 – F1031 Change in SBE

Department of Critical Care Medicine, Apollo Hospitals
Base Excess has Deficits!!!!!
BE changes with changes in PCO2 invivo
Increased PCO2 causes negative BE
Equilibration occurs across entire extracellular fluid
space (Whole blood + interstitial fluid)
Extracellular or Standard BE
Diluting blood threefold with its own plasma (Hb 5g/dl)
At best a “GUESSTIMATE”
Accurate ONLY when constant hemoglobin “assumed”
Does not help identify the cause

Department of Critical Care Medicine, Apollo Hospitals
(Mis)understanding acid-base
The serum potassium varies with changes in pH due
to exchange of K+ for H+
Serum K+ concentration is in mmol/L (i.e. 10-3) but that H+
concentration varies in nanomolar range (i.e. 10-9)
Department of Critical Care Medicine, Apollo Hospitals
(Mis)understanding Acid-base
Vomiting causes metabolic alkalosis by loss of
H+ Why can’t the correction be done with H2O to replenish
the H+?
Saline-induced acidosis - “Dilutional” acidosis Decrease in bicarbonate cannot cause hyperchloremia
How does sodium bicarbonate rectify acidosis?
Fernandez PC, et al. KI 1989; 36: 747-52
Garella S, et al. NEJM 1973; 289: 121-6
Androgue HJ, et al. JCI 1983; 71: 867-83
Department of Critical Care Medicine, Apollo Hospitals
Stewart’s definition of acid
H+ = OH- - Acid-Base Neutral Acidic solution – H+ > OH-
Basic solution – H+ < OH-
Acids when added to a solution increase H+
Dissociate to yield an anion and H
HA = [H+] [A-]
Complete or partial
Associate with hydroxyl ion
H+ concentration by itself is not a reliable measure of
acidity, alkalinity or neutrality

Department of Critical Care Medicine, Apollo Hospitals
Determinants of ECF acid-base
[H+] [OH-] = K`w
[H+] [A-] = KA [HA]
[AH] [A-] = [ATOT]
[H+] [HCO3-] = Kc pCO2
[H+] [CO3--] = K3 [HCO3
-]
[SID] + [H+] - [HCO3-] - [A-] - [CO3
--] - [OH-] = 0
Department of Critical Care Medicine, Apollo Hospitals
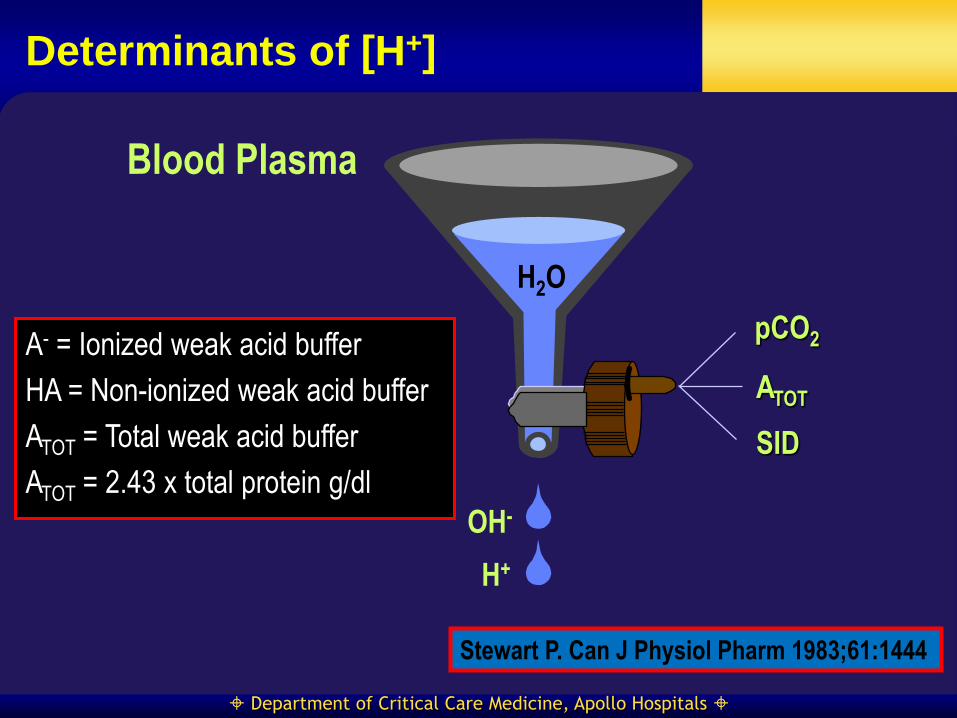
H2O
OH-
H+
Determinants of [H+]
Blood Plasma
pCO2
ATOT
SID
Stewart P. Can J Physiol Pharm 1983;61:1444
A- = Ionized weak acid buffer
HA = Non-ionized weak acid buffer
ATOT = Total weak acid buffer
ATOT = 2.43 x total protein g/dl
Department of Critical Care Medicine, Apollo Hospitals
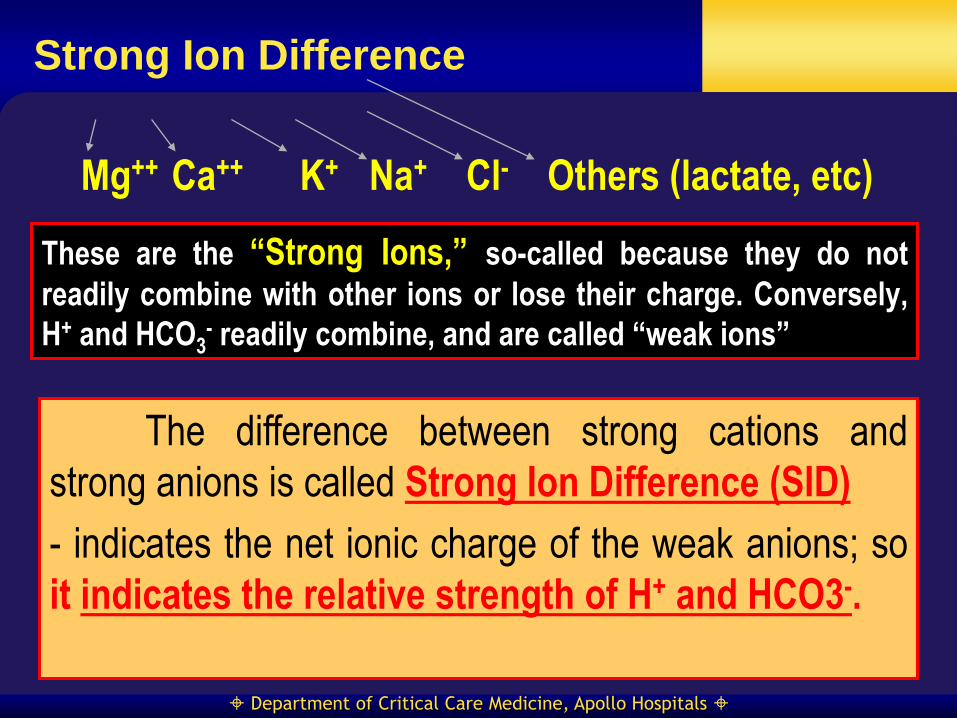
Strong Ion Difference
These are the “Strong Ions,” so-called because they do not
readily combine with other ions or lose their charge. Conversely,
H+ and HCO3- readily combine, and are called “weak ions”
Na+ Cl- K+
The difference between strong cations and
strong anions is called Strong Ion Difference (SID)
- indicates the net ionic charge of the weak anions; so
it indicates the relative strength of H+ and HCO3-.
Mg++ Ca++ Others (lactate, etc)
Department of Critical Care Medicine, Apollo Hospitals
Aqueous Solutions
Water
Dissociation
H2O H+ + OH-
Physico - Chemical Approach
H+ and HCO3 – are only DEPENDENT variables
Acids increase water dissociation
1. Determinant of H+ is water dissociation
2. Water dissociation – Determined by SID, ATOT and
PCO2

Department of Critical Care Medicine, Apollo Hospitals
Physico-chemical Approach
Both H+ and HCO3- are dependent variables
Bicarbonate – just a gap filler between strong cations
and anions
Metabolic component – Strong Ion Difference and ATOT
Respiratory component – PCO2
Six acid-base disorders
SID – increase and decrease – alkalosis and acidosis
ATOT – increase and decrease – acidosis and alkalosis
Respiratory
Department of Critical Care Medicine, Apollo Hospitals
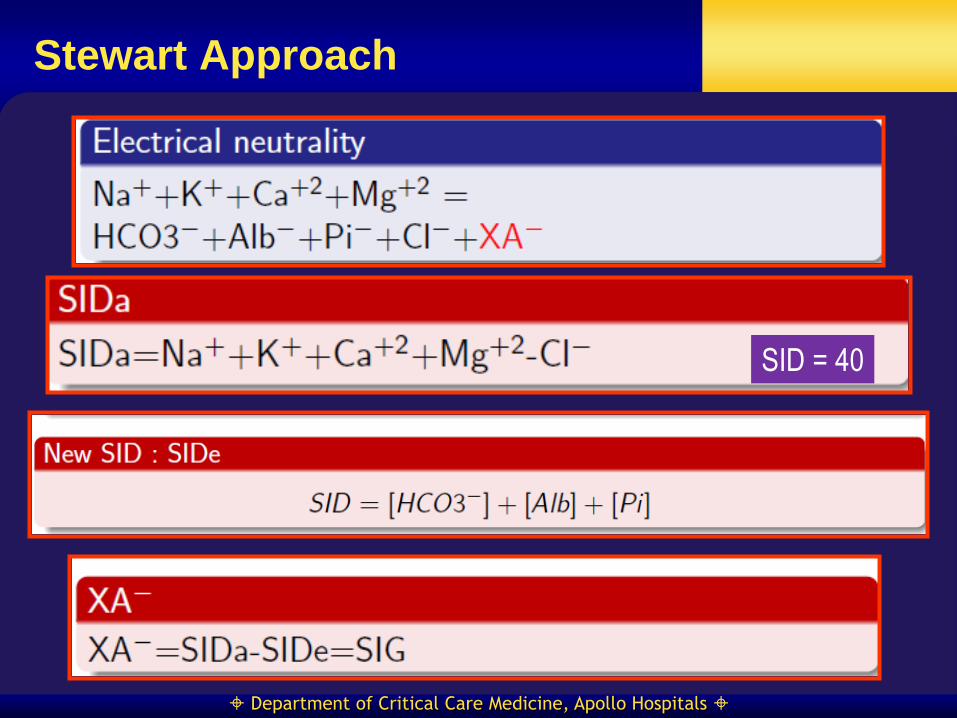
Stewart Approach
SID = 40

Department of Critical Care Medicine, Apollo Hospitals
SID vs. AG
Na
K
Cations
Cl
HCO3
Anions
Normal
SIDa Prot
PO4
AG SIDe
AG = (Na+ + K+) – (Cl- + HCO3-)
SIDa (40) = (Na+ + K+) – Cl-
SIDe = Bicarbonate + ATOT-
SIDa = SIDe
SIG = 0

Department of Critical Care Medicine, Apollo Hospitals
SIG vs. AG acidosis
Na
K
Cations
Cl
HCO3
Anions
High AG or SIG acidosis
SIDa Prot
PO4 AG SIDe
SIG
AG increased
SIDa unchanged
SIDe decreased
SIG increased
Department of Critical Care Medicine, Apollo Hospitals
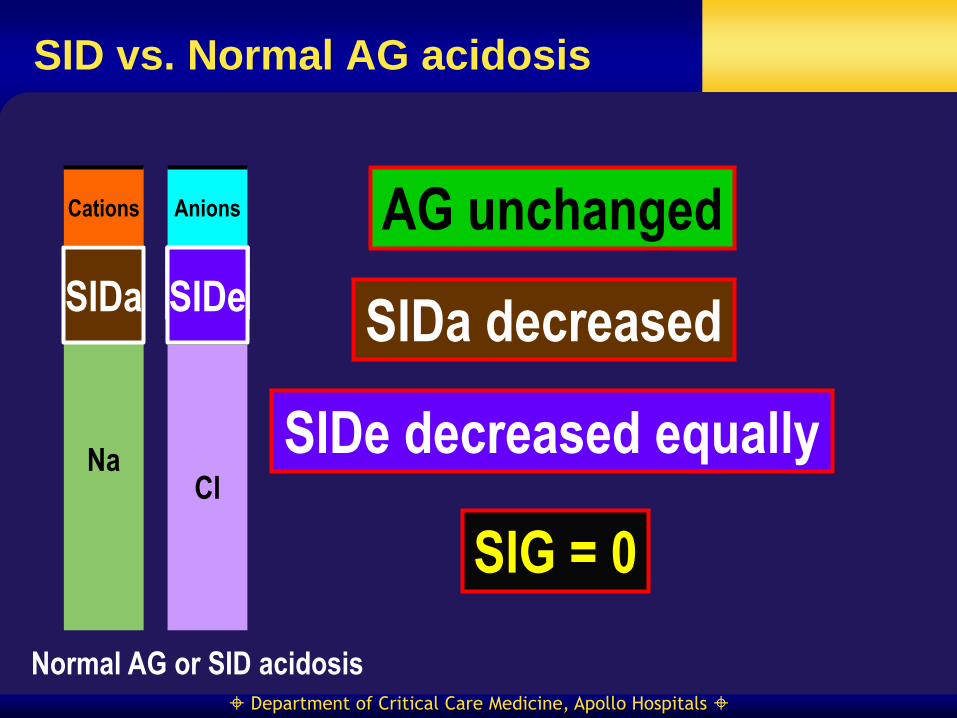
SID vs. Normal AG acidosis
Na
K
Cations
Cl
HCO3
Anions
Normal AG or SID acidosis
SIDa Prot
PO4
AG unchanged
SIDa decreased
SIDe decreased equally
SIG = 0
AG SIDe
Department of Critical Care Medicine, Apollo Hospitals
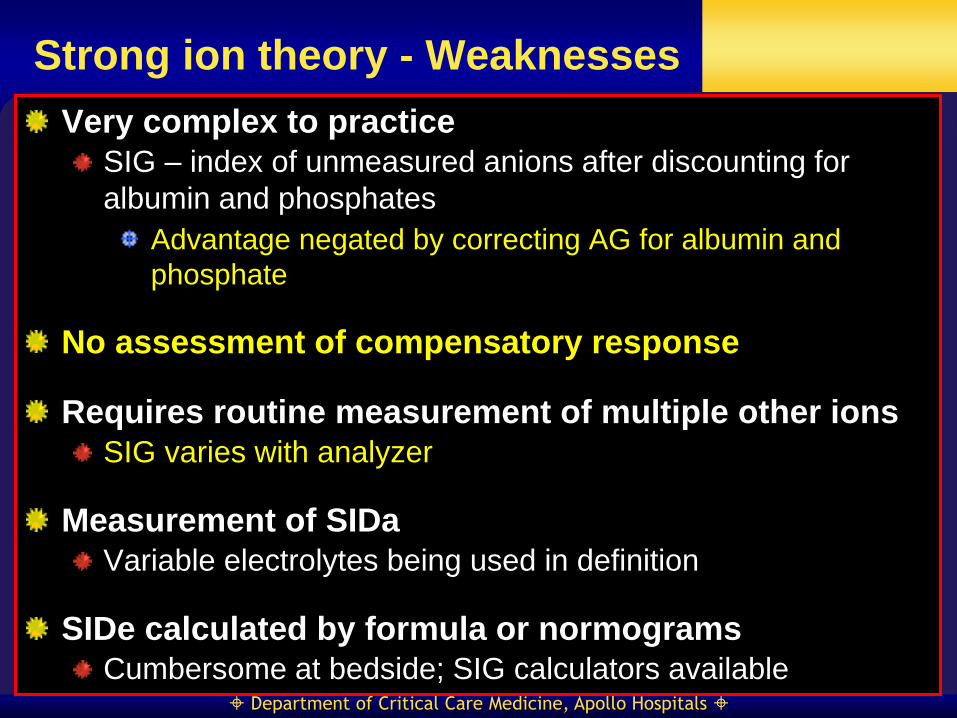
Strong ion theory - Weaknesses
Very complex to practice
SIG – index of unmeasured anions after discounting for
albumin and phosphates
Advantage negated by correcting AG for albumin and
phosphate
No assessment of compensatory response
Requires routine measurement of multiple other ions
SIG varies with analyzer
Measurement of SIDa
Variable electrolytes being used in definition
SIDe calculated by formula or normograms
Cumbersome at bedside; SIG calculators available

Department of Critical Care Medicine, Apollo Hospitals
Classification too complex
Normal SIDa Decreased SIDa
Decreased SIDa
But no SIG Decreased SIDe
Increased SIG
Decreased SIDe
No SIG
High ATOT acidosis
Low ATOT alkalosis
Department of Critical Care Medicine, Apollo Hospitals
More Confusion
Clinical relevance of ATOT acidosis and alkalosis?
No regulation of albumin to maintain acid-base status invivo
Changes in serum albumin do not correlate with changes in
pH or PCO2
Stewart approach – blending of diagnosis and cause
Mathematically accurate but no validation on cause
and effect relationship
Adrogue HJ et al: Kidney Int. 2009; 76: 1239 - 1247
Department of Critical Care Medicine, Apollo Hospitals
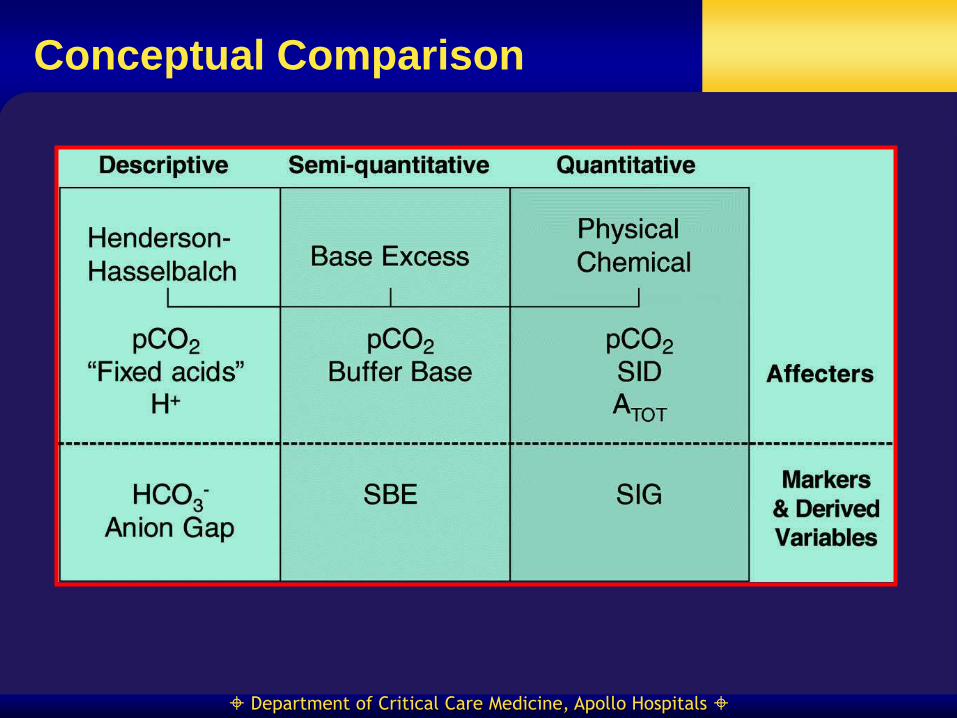
Conceptual Comparison

Department of Critical Care Medicine, Apollo Hospitals
SIG vs AG
1. AG = [Na+] [K+] – [Cl-] – [HCO3- ]
2. SIDa = Na++K+-Cl-
3. SIDe = HCO3- + A-
4. SIG = SIDa - SIDe [{Na+ + K+ -Cl}- -( HCO3- + A- )]
Combining above 4 equations
SIG = [Na+] [K+] – [Cl-] – [HCO3- ] - [A-]
SIG = AG - [A-]
where [A-]= 2.8 (albumin g/dL)+ 0.6(phosphate mg/dL) at pH 7.4
SIG approximates AGcorr

Department of Critical Care Medicine, Apollo Hospitals
Diagnostic Accuracy
Dubin A, et al. CCM 2007; 35:1264-1270

Department of Critical Care Medicine, Apollo Hospitals
Diagnostic and prognostic value
Discordant ABG interpretation - 26 %1
Stewart method superior in identifying patients with high
lactate levels
Can be rectified by incorporating albumin levels in AG
calculations
No difference in quantifying complex acid-base
disorders when AG corrected for albumin 2,3
Conflicting data on prognostic value of SID and SIG1,4,5
1. Balasubramanyan N, et al. CCM 1999; 27(8):1577
2. Moviat M, et al. CCM 2003; 7(3):R41
3. Lautrette A, et al. Minerva Anesthes 2013; 79(10): 1164
4. Cisack RJ et al. ICM 2002; 28(7): 864
5. Kaplan LJ et al. SHOCK 2008; 29(6): 662
Department of Critical Care Medicine, Apollo Hospitals
Conclusion
Difficult to explain and understand metabolic acid-
base disturbances using bicarbonate-based
approaches
Need to invoke complex mechanisms and hormones
Physico – chemical approach lends itself for easy
explanation and understanding
Blending of diagnosis and cause a concern
More cumbersome
If AG corrected for albumin, no difference between
approaches in diagnostic efficacy
Data conflicting on relative prognostic value of
variables derived from all three approaches
Department of Critical Care Medicine, Apollo Hospitals
Understanding Acid- base
Final Verdict!!!

Department of Critical Care Medicine, Apollo Hospitals

Department of Critical Care Medicine, Apollo Hospitals
Physico - chemical Principles
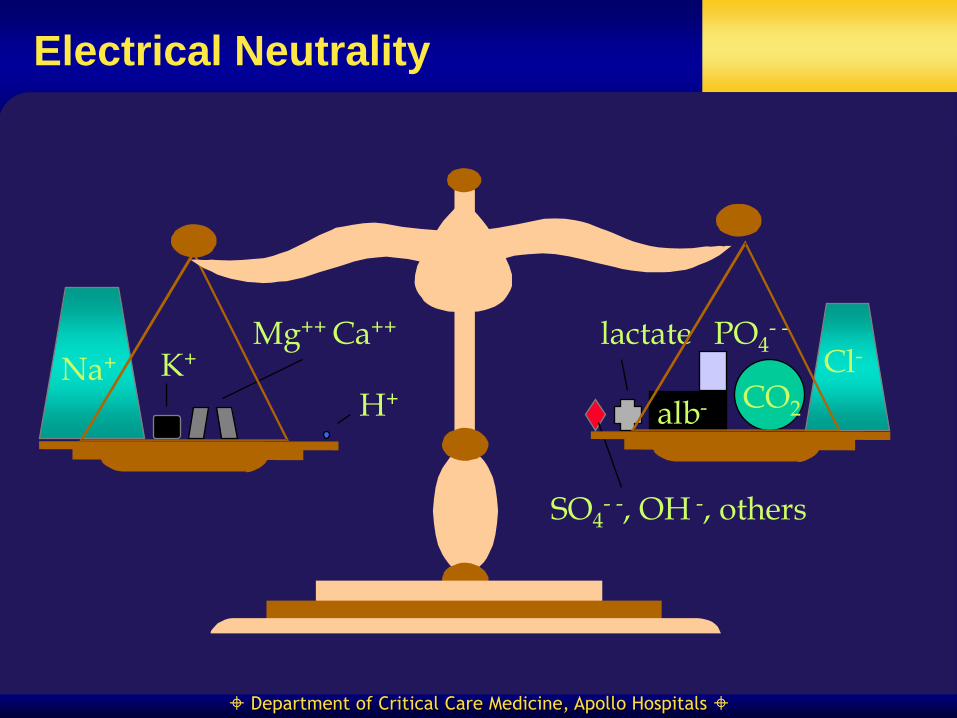
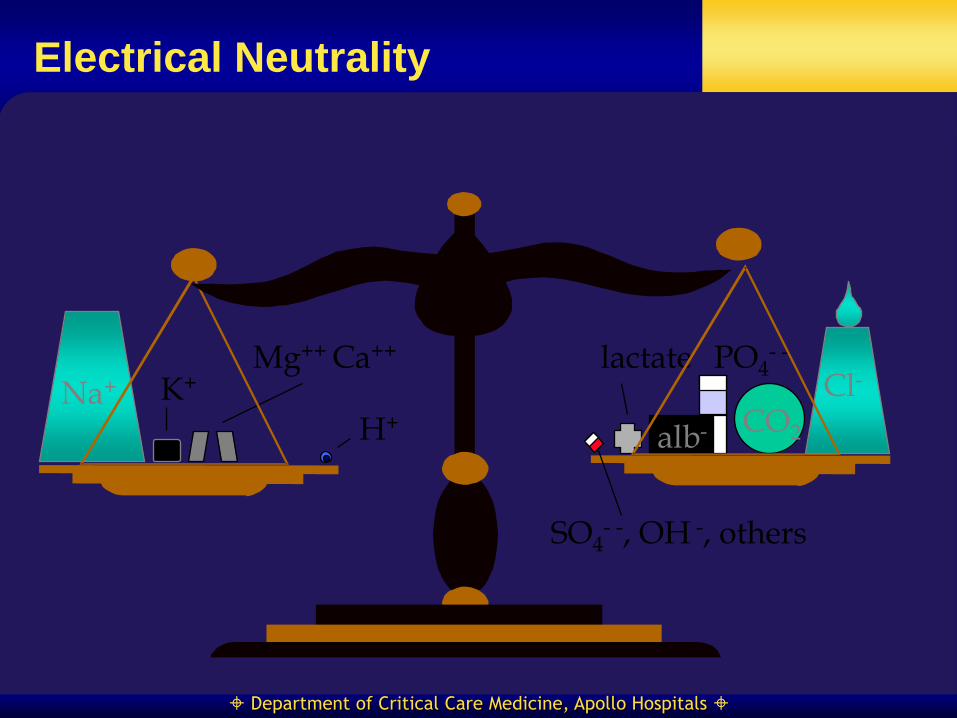
Electrical Neutrality In macroscopic aqueous solutions, the sum of all positively
charged ions must equal the sum of all negatively charged
ions
Conservation of Mass The amount of a substance remains constant unless it is
added or removed or unless it is generated or destroyed
Department of Critical Care Medicine, Apollo Hospitals
Na+ K+ Mg++ Ca++
H+
Cl-
alb- CO2
lactate
SO4- -, OH -, others
PO4- -
Electrical Neutrality

Department of Critical Care Medicine, Apollo Hospitals
Electrical Neutrality
[H+] [OH-] = K`w
[H+] [A-] = KA [AH]
[AH] [A-] = [ATOT]
[H+] [HCO3-] = Kc pCO2
[H+] [CO3--] = K3 [HCO3
-]
[SID] + [H+] - [HCO3-] - [A-] - [CO3
--] - [OH-] = 0
Stewart P. Can J Physiol Pharm 1983;61:1444
Department of Critical Care Medicine, Apollo Hospitals
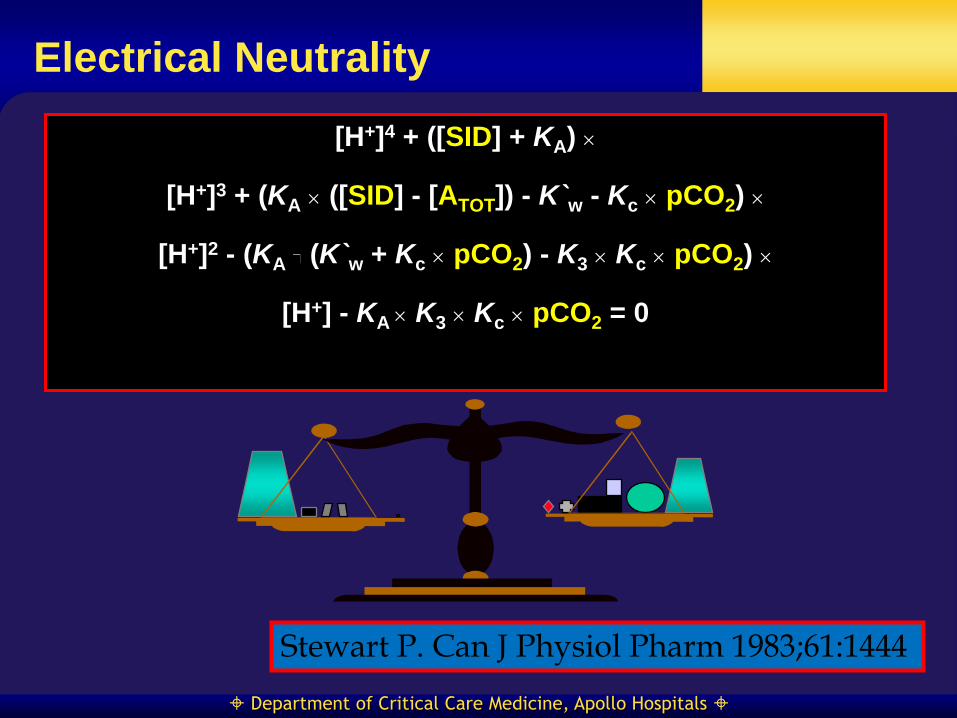
Electrical Neutrality
[H+]4 + ([SID] + KA)
[H+]3 + (KA ([SID] - [ATOT]) - K`w - Kc pCO2)
[H+]2 - (KA (K`w + Kc pCO2) - K3 Kc pCO2)
[H+] - KA K3 Kc pCO2 = 0
Stewart P. Can J Physiol Pharm 1983;61:1444

Department of Critical Care Medicine, Apollo Hospitals
SBE vs SID
The standard base excess
corresponds to the change
in SID required to restore
the plasma (in vivo) to pH
7.40 with pCO2 of 40 mm
Hg
R2=0.9527
-10
-8
-6
-4
-2
0
2
4
6
-8 -6 -4 -2 0 2 4
A/V SIDe
A/V
SB
E
Kellum et al. J Crit Care 1997; 12: 7-12

Department of Critical Care Medicine, Apollo Hospitals
Saline Acidosis
SID = 40
SID = 32
Serum Na+ 140 mEq/L
Total Body Na+:
140 x 42 = 5880 mEq
Serum Cl- 100 mEq/L
Total Body Cl-:
100 x 42 = 4220 mEq
Add 10L of 0.9% saline
5880 + 1540 = 7420
7420/52 = 142.7 mEq/L
Add 10L of 0.9% saline
4220 + 1540 = 5760
5760/52 = 110.7 mEq/L

Department of Critical Care Medicine, Apollo Hospitals
Electrical Neutrality
How does Saline cause acidosis?
....by decreasing the SID and increasing water
dissociation.

Department of Critical Care Medicine, Apollo Hospitals
Electrical Neutrality
Na+
alb- CO2
lactate
SO4- -, OH -, others
K+ Mg++ Ca++
H+
PO4- -
Cl- Cl-

Department of Critical Care Medicine, Apollo Hospitals
Saline Acidosis
SO4- -, OH -, others
Cl-
Na+
alb- CO2
lactate
K+ Mg++ Ca++
H+
PO4- -
alb-
Department of Critical Care Medicine, Apollo Hospitals
Electrical Neutrality
Cl- Na+
alb- CO2
lactate
SO4- -, OH -, others
K+ Mg++ Ca++
H+
PO4- -

Department of Critical Care Medicine, Apollo Hospitals
Further Implications
How does sodium bicarbonate increase the plasma pH?
....by increasing plasma Na+ and thus SID
Department of Critical Care Medicine, Apollo Hospitals
Sodium Bicarbonate
HCO3- is a dependent variable. It does not
have a Vd. Its concentration is set by the
prevailing pCO2, SID and ATOT.
NaHCO3 increases the plasma pH by
increasing the Na+ and thereby the SID.
This results in decreased water dissociation
and increased pH.

Department of Critical Care Medicine, Apollo Hospitals
More Acid-Base Questions
Why do patient’s with NG drainage develop alkalemia?
Distinguish H+ loss as HCl from H+ loss as H2O
Department of Critical Care Medicine, Apollo Hospitals
Geocentric Universe
Department of Critical Care Medicine, Apollo Hospitals
Copernicus

Department of Critical Care Medicine, Apollo Hospitals
HCO3-
H+
CO2
Cl-
Buffers
Geocentric Universe
Department of Critical Care Medicine, Apollo Hospitals
CO2
SID
ATOT
H+
HCO
3-
A-
Post-Copernicus

Department of Critical Care Medicine, Apollo Hospitals
Changing Practice
Saline causes acidosis, especially in the critically ill
NaHCO3 only works by increasing the serum Na+ (relative
to Cl-)
Lactate is a strong acid but NaL is a salt. Lactate is
acidifying; ATP hydrolysis is not.
Base excess is a reliable measure of metabolic acid-base
status relative to baseline
The anion gap (when the corrected “normal range” is used)
is a reliable measure of missing anions
Department of Critical Care Medicine, Apollo Hospitals
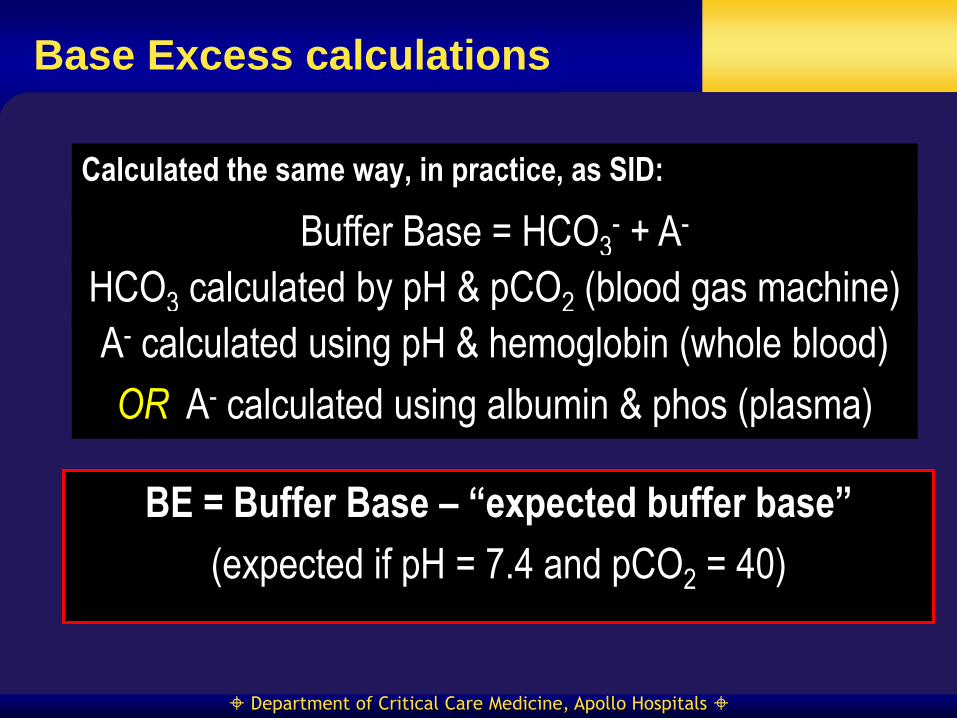
Base Excess calculations
Calculated the same way, in practice, as SID:
Buffer Base = HCO3- + A-
HCO3 calculated by pH & pCO2 (blood gas machine)
BE = Buffer Base – “expected buffer base”
(expected if pH = 7.4 and pCO2 = 40)
A- calculated using pH & hemoglobin (whole blood)
OR A- calculated using albumin & phos (plasma)
Department of Critical Care Medicine, Apollo Hospitals
Tight regulation to maintain this level Chemical buffering
Control of PaCO2 - alveolar ventilation
Control of plasma bicarbonate
Renal H+ excretion
Buffers
Uses SOLELY the carbonic acid/bicarbonate buffer system to
assess acid-base status Abundance
Physiological pre-eminence
Both components undergo homeostatic control