Embed Size (px)
Citation preview
Venous Access Devices
Continuing Education
Venous Access Devices In both the hospital and outpatient settings,
venous access devices are a critical component in patient care.
One size does not fit all and each device, type and duration should be tailored to the needs of each individual to provide safe and reliable care.
There are a variety of options available and are generally broken down into peripheral and central venous access devices (CVAD).
Peripheral IV Lines
PHOTO REFERENCE: http://faculty.mercer.edu/summervill_j/jeanchiang/Mvc-098s.jpg
Peripheral IV Lines Peripheral catheters are the most commonly used
venous access device. It is a short catheter inserted through the skin
into a vein, primarily the superficial veins of the hand or forearm, and in some cases the foot.
It has the least complications and is cost effective for short term use.
These catheters are not recommended when the therapy is a vesicant, chemotherapy, parenteral nutrition or when the pH is <5 or >9.
Peripheral IV Indications
Peripheral catheters are appropriate venous access devices for short term therapies, generally less than 7 days.
Hydration, diuretics, steroids, gamma globulin, and some antibiotics are frequently prescribed for peripheral infusion.
Parenteral Nutrition, vesicants, chemotherapy or medications and solutions with a pH <5 or > 9 are not recommended.
Peripheral access is also useful short term for patients who cannot absorb medications or take orally due to illness.
The CDC Guidelines state that another VAD may be more appropriate for use if the therapy will last longer than 6 days.
Peripheral IV Site Selection
When selecting access, the most distal site on the extremity is recommended and working upward with future catheter insertions.
Peripheral catheters should not be placed over a joint or any point of flexion, below previous sites, or in bruised, infiltrated or phlebotic areas.
Metacarpal, cephalic, basilic, and median veins are most recommended due to their size and location.
The antecubital veins should be preserved as long as possible and should not routinely be used for IV therapy due to greater risk of phlebitis and infiltration.
Patient age, history of IV drug abuse, obesity and a medical history limiting use of an affected extremity are factors that may make access difficult.
Warm compresses and placing the extremity in a dependent position may help to locate a vein for cannulation.
The smallest and shortest gauge catheter should be chosen as it causes the least amount of trauma to the vessel, promotes proper hemodilution of the medication, and allows adequate blood flow around the catheter.
One catheter should be used for each insertion attempt and aseptic technique must be maintained.
Peripheral IV Site Selection Cont.
It is recommended by INS (Infusion Nurses Society) that a Nurse makes only 2 attempts at IV access. o If unsuccessful, a second experienced nurse should assess patient and only
attempt if there is a viable vein. o If 3rd attempt is unsuccessful, the MD needs notified.
In the past, site rotation of a peripheral catheter was recommended every 72-96 hours. o 2011 Infusion Nursing Standards of Practice recommend the nurse consider
peripheral catheter replacement when clinically indicated. The decision should be based on assessment of the patient’s
condition: o assess site, skin and vein integrity o length and type of prescribed therapy o venue of care o integrity and patency of the VAD o dressing o stabilization device
This is based on several studies that proved peripheral IV catheters have an increased risk of phlebitis after 72 hrs. If this does not occur the IV site needs assessed at least daily and documented as to the condition of the site.
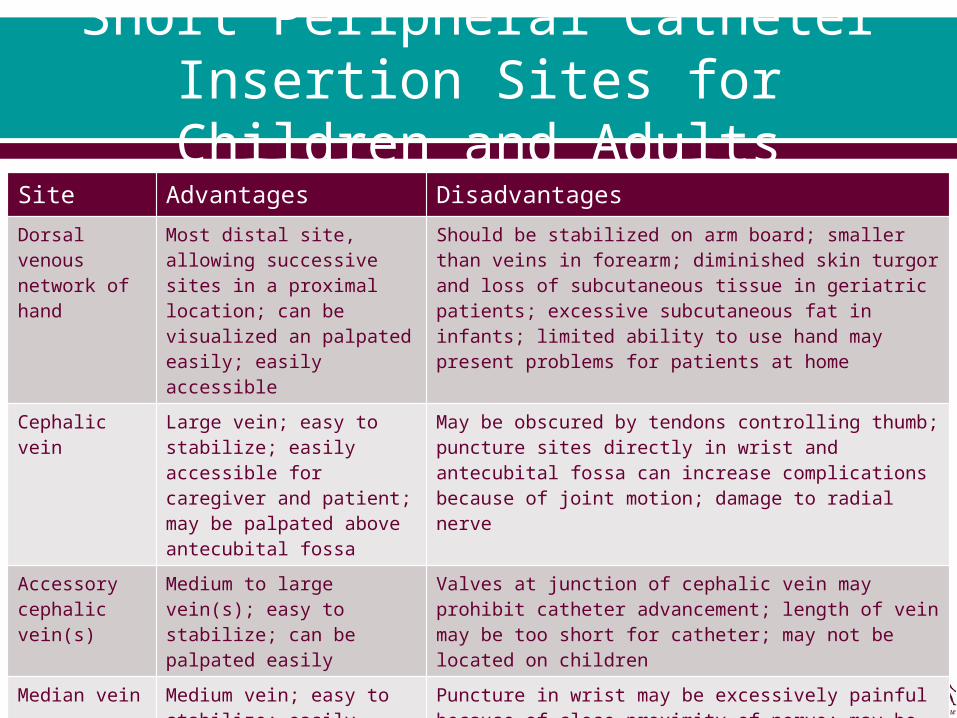
Short Peripheral Catheter Insertion Sites for Children and
AdultsSite Advantages Disadvantages
Dorsal venous network of hand
Most distal site, allowing successive sites in a proximal location; can be visualized an palpated easily; easily accessible
Should be stabilized on arm board; smaller than veins in forearm; diminished skin turgor and loss of subcutaneous tissue in geriatric patients; excessive subcutaneous fat in infants; limited ability to use hand may present problems for patients at home
Cephalic vein Large vein; easy to stabilize; easily accessible for caregiver and patient; may be palpated above antecubital fossa
May be obscured by tendons controlling thumb; puncture sites directly in wrist and antecubital fossa can increase complications because of joint motion; damage to radial nerve
Accessory cephalic vein(s)
Medium to large vein(s); easy to stabilize; can be palpated easily
Valves at junction of cephalic vein may prohibit catheter advancement; length of vein may be too short for catheter; may not be located on children
Median vein Medium vein; easy to stabilize; easily accessible for caregiver and patient
Puncture in wrist may be excessively painful because of close proximity of nerve; may be slightly more difficult to palpate and visualize
Basilic vein Large vein; can be palpated easily; may be available after other sites have been exhausted
More difficult to access because of location; may be difficult to patient to access and observe site; puncture site directly in antecubital fossa may result in increased complications because of joint motion; cannot be palpated above antecubital fossa
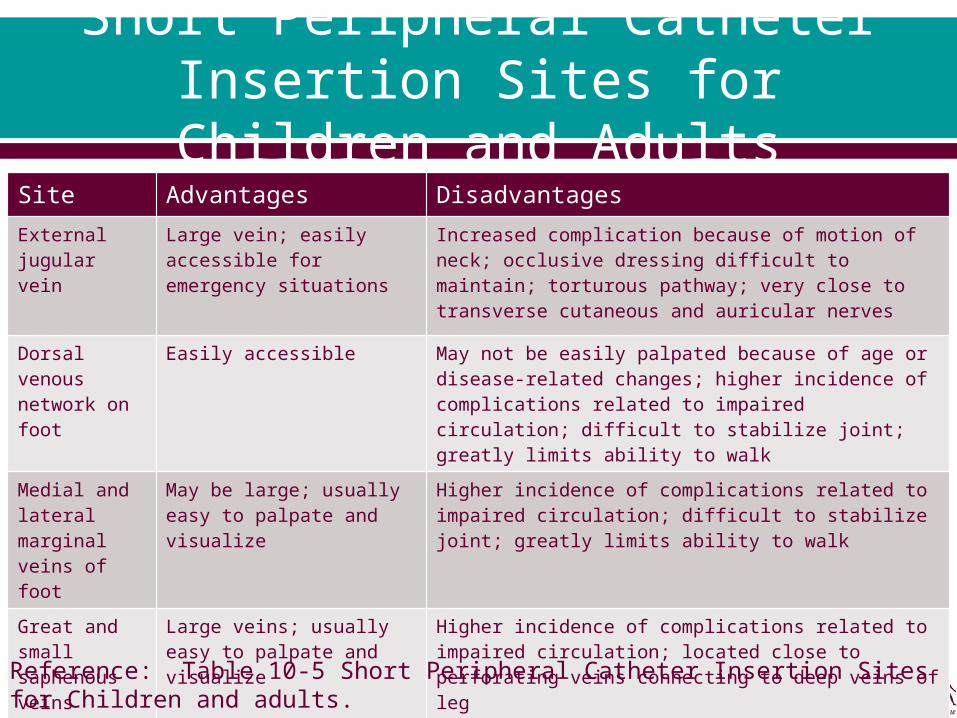
Short Peripheral Catheter Insertion Sites for Children and
AdultsSite Advantages Disadvantages
External jugular vein
Large vein; easily accessible for emergency situations
Increased complication because of motion of neck; occlusive dressing difficult to maintain; torturous pathway; very close to transverse cutaneous and auricular nerves
Dorsal venous network on foot
Easily accessible May not be easily palpated because of age or disease-related changes; higher incidence of complications related to impaired circulation; difficult to stabilize joint; greatly limits ability to walk
Medial and lateral marginal veins of foot
May be large; usually easy to palpate and visualize
Higher incidence of complications related to impaired circulation; difficult to stabilize joint; greatly limits ability to walk
Great and small saphenous veins
Large veins; usually easy to palpate and visualize
Higher incidence of complications related to impaired circulation; located close to perforating veins connecting to deep veins of leg
Reference: Table 10-5 Short Peripheral Catheter Insertion Sites for Children and adults. Page 165 Infusion Nurses Book.
Flushing of peripheral IV catheter
INS guidelines for flushing a peripheral catheter no longer include the use of heparin lock solution.
A minimum of 2mls of Preservative free 0.9% Sodium chloride should be used before and after medications and solutions.
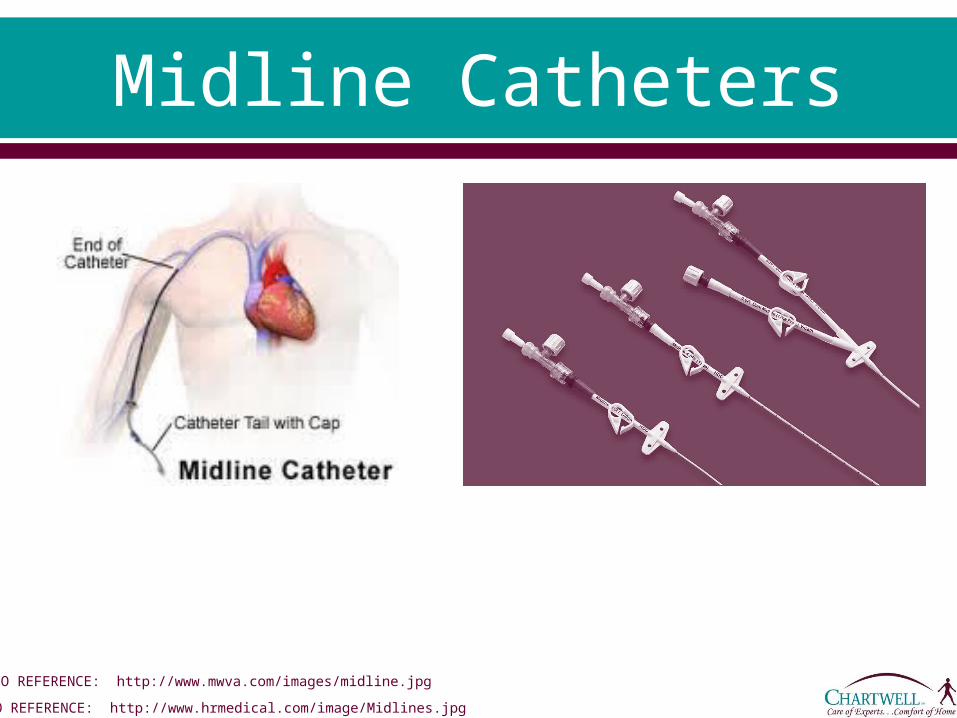
Midline Catheters
PHOTO REFERENCE: http://www.hrmedical.com/image/Midlines.jpg
PHOTO REFERENCE: http://www.mwva.com/images/midline.jpg
Midline Catheters A Midline is simply a long peripheral catheter typically 3-11
inches in length (8-25cm) inserted into the antecubital or upper arm vein.
Unlike the PICC line which terminates in the central circulation, the tip of the midline catheter resides in the basilic, cephalic or brachial vein distal to the shoulder at or below the axillary line. The basilic vein access is preferred due to its larger diameter.
Insertion costs for PICC and Midline Catheters are similar, however the Midline tends to be a less favorable choice due to limitations in dwell time and use.
Midlines have an advantage over short peripheral access because they do not require frequent site changes and have less risk of phlebitis due to larger vein access.
Midline catheters tend to have lower infection rates than PICCs and other CVADs.
Typical sizes are 1.9 Fr.-5 Fr. and are available in both single and double lumen and polyurethane and silicone materials.
Midline Catheter Indications
Midline catheters are generally used for venous access between 1-4 weeks duration and for neonates 6-10 days.
They can be used in any inpatient or outpatient setting. According to INS standards, any infusate that can be used
for short peripheral access is appropriate for Midline use. Hydration, blood products, pain medications, diuretics and
some antibiotics are typical therapies used for midlines. It is not appropriate to infuse vesicants, parenteral
nutrition, or solutions with a pH<5 or >9 or an osmolality >600 mOsm/L through a midline catheter.
INS does not recommend routine blood specimen collection from a peripheral or midline catheter.
Midline Catheter Placement
As with any VAD, peripheral and midline catheters should be placed by trained and qualified health care professionals and by physician or authorized prescribers’ order.
Both can be inserted at bedside. The CDC guidelines for hand hygiene should be followed
to decontaminate hands prior to inserting any IV Catheter. Standard precautions for the health care worker should be
followed to prevent blood contamination. If hair removal is necessary, per the INS guidelines,
scissors are recommended and only surgical clippers with a disposable head can be used. o Shaving can cause a micro abrasion creating an environment for
infection.
Midline Catheter Placement Cont.
The CDC recommends use of 2% chlorhexidine based scrub but 70% alcohol and 1-2% povidone iodine solution can be used if allergic to chlorhexidine.
An analysis was done involving 8 different studies comparing the cleansing solutions and the outcome proved to be a significant decrease in bloodstream infections when chlorhexidine based scrub was used.
For chlorhexidine to be affective it should be applied with friction for a minimum of 30 seconds and be allowed to air-dry for a minimum of 30 seconds. The area prepped should be 2-3 inches in diameter.
Ideally the Midline catheter should be placed in a patient’s non-dominate arm 1-1 ½ inches above or below the anticubital fossa and following manufacturers’ guidelines.
Once the insertion site is chosen the length of the catheter is measured against the distance from the insertion site. o The catheter may require trimming so as not to extend
beyond the axillary vein. Insertion techniques vary among manufacturers
but CXR is not needed to confirm placement. Measurements of accessed arm and catheter
length should be taken and documented.
Midline Catheter Placement Cont.
Midline Catheter Securement
It is important that stabilization of the short or long peripheral catheter be done to minimize loss of catheter, infiltration and the development of mechanical phlebitis.
Studies have shown there is a significant reduction in complications and prolonged dwell time with a manufactured securement device and is the recommended choice.
Taping methods can be used. o Anchor tape should only be applied to the wings of the
catheter and not the skin-catheter junction site as it inhibits visualization and can be a potential source of infection.
When possible, dressings should be transparent semi permeable (TSM) so the site can be assessed daily or with every use of the catheter.
Flushing a Midline Catheter
Preservative free 0.9% Sodium chloride should be used before and after medications and solutions.o INS recommends a minimum of 3mls NSS and 3mls
10U/ml heparin lock solution.
Complications of Peripheral and Midline Catheters
Infiltration is a frequent complication of peripheral IV access, and more common than in CVADs (central venous access devices) due to the shorter nature of the catheter and smaller veins used.
It is the leaking of IV fluid into surrounding tissue from a dislodged catheter or vein rupture on insertion.
Common symptoms of infiltration can be o cool blanched skin that may feel tauto edema, tenderness, and discomfort o A stoppage or change in IV flow rateo leaking at insertion site ao sometimes burning occurs depending on the solution being infused.
Once it is determined there is an infiltrate, stop the infusion, remove the IV catheter and elevate the extremity.
Warm compresses increase vasodilatation and disperse the extra fluid while cool compresses cause vasoconstriction and limit the spread of IV solution. o Warm or cold compresses should be used according to your institutions policy and procedures or
according to the pharmacological characteristics of the infusion. Some medications can be an irritant causing tissue damage while most IV fluids
cause minimal damage. The amount of solution that infiltrated should be estimated and documented. Among others, Phlebitis, infection, and occlusion are other complications of
peripheral IV access and CVADS and will be addressed further in this learning module.

Infiltration ScaleGrade Clinical Criteria
0 No symptoms
1 Skin blanchedEdema <1 inch in any directionCool to touchWith or without pain
2 Skin blanchedEdema 1-6 inches in any directionCool to touchWith or without pain
3 Skin blanched, translucentGross edema >6 inches in any directionCool to touchMild-moderate painPossible numbness
4 Skin blanched, translucentSkin tight, leakingSkin discolored, bruised, swollenGross edema >6 inches in any directionDeep pitting tissue edemaCirculatory impairmentModerate-severe painInfiltration of any amount of blood product, irritant, or vesicant
Reference: Box 23-3 Infiltration Scale. Page 470 Infusion Nurses Book.
Midline Catheter Removal
Upon removal of a peripheral catheter digital pressure should be applied until homeostasis is achieved, and a dressing should be applied to the access site.
With removal of a Midline catheter, a petroleum based ointment and a sterile dressing should be applied to the access site to seal the skin-to-vein tract and decrease the risk of air embolus.

![Four categories which guide further evaluation ......HPV/ p16 – cervical cancer EBV genome – nasopharyngeal cancer t(15:19) – midline carcinoma (t[11;22] [q24;q12]) – peripheral](https://img.pdfslide.us/doc/110x75/5f0e374f7e708231d43e2b60/four-categories-which-guide-further-evaluation-hpv-p16-a-cervical-cancer.jpg)



![Lethal midline granuloma: a case report...midline reticulosis [3]. The term ‘Lethal midline granuloma’ was first described by McBride in 1897 [4]. Grossly, the lesion looks like](https://img.pdfslide.us/doc/110x75/613653db0ad5d2067647f3c3/lethal-midline-granuloma-a-case-report-midline-reticulosis-3-the-term-alethal.jpg)