www.mercer.com
Health Reform: Implications for employers
06 October 2009
John Sinclair, [email protected]
513-632-2603
2Mercer webcast
Agenda
Current legislative state of play
Potential impact on employers
The surcharge: a tipping point for radical change or exit?
Considerations for improving quality and cost efficiency
Your questions!
Current legislative state of play
4Mercer webcast
Health reform – state of playCongress faces tough decisions
House of Representatives– House Ways and Means, Education and Labor panels passed own
versions of HR 3200– House Energy and Commerce panel approved its version after intra-party
debate on costs– House leaders working to “reunite” the three versions, ready single bill for
full debate and vote on House floor
Senate– HELP Committee approved left-leaning bill by party-line vote – Finance Committee debating more moderate proposal to address
conservative Democrats’ concerns and garner some GOP support Committee members filed over 560 amendments
5Mercer webcast
President Obama takes a leadership role
“I am not the first President to take up this cause, but I am determined to be the last” President Obama, September 9, 2009
His guidance:– Do not increase the federal deficit – Rein in rising health care costs– Improve access to coverage
6Mercer webcast
Health reform – state of playWhat’s next?
Ultimate goal is a final health reform bill by the end of the year
Plan A: Seek 60 votes in the Senate
Plan B: Democrats could fast-track reform through Senate without GOP support– “Reconciliation” trigger can be pulled if talks with GOP fail
Reform could pass Senate by 51 votes, far less than normally needed, with debate limited
But reconciliation isn’t a slam dunk - “Byrd droppings” – extraneous provisions can be challenged- Limited duration- Political considerations
7Mercer webcast
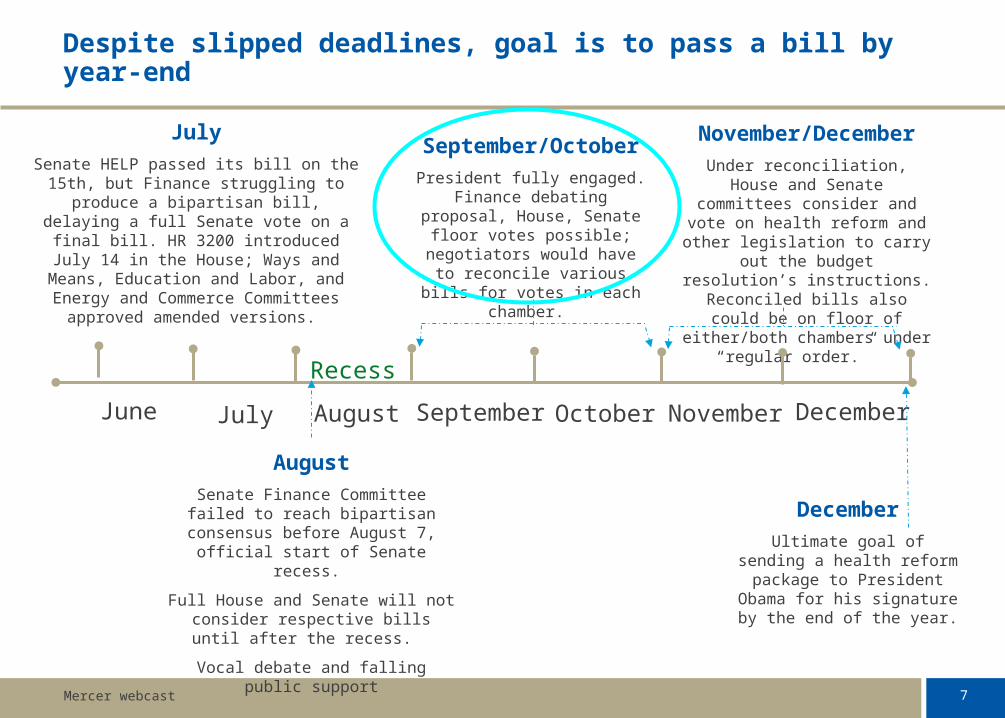
Despite slipped deadlines, goal is to pass a bill by year-end
July
Senate HELP passed its bill on the 15th, but Finance struggling to produce a bipartisan bill, delaying a full Senate vote on a final bill. HR 3200 introduced July 14 in the House; Ways
and Means, Education and Labor, and Energy and Commerce Committees approved
amended versions.
December
Ultimate goal of sending a health reform package to President Obama for his
signature by the end of the year.
November/December
Under reconciliation, House and Senate committees
consider and vote on health reform and other legislation to
carry out the budget resolution’s instructions.
Reconciled bills also could be on floor of either/both
chambers under “regular order.”
August
Senate Finance Committee failed to reach bipartisan consensus before August 7, official start of Senate
recess.
Full House and Senate will not consider respective bills until after
the recess.
Vocal debate and falling public support
September/October
President fully engaged. Finance debating proposal, House, Senate floor votes
possible; negotiators would have to reconcile various
bills for votes in each chamber.
June July August September October November December
Recess
8Mercer webcast
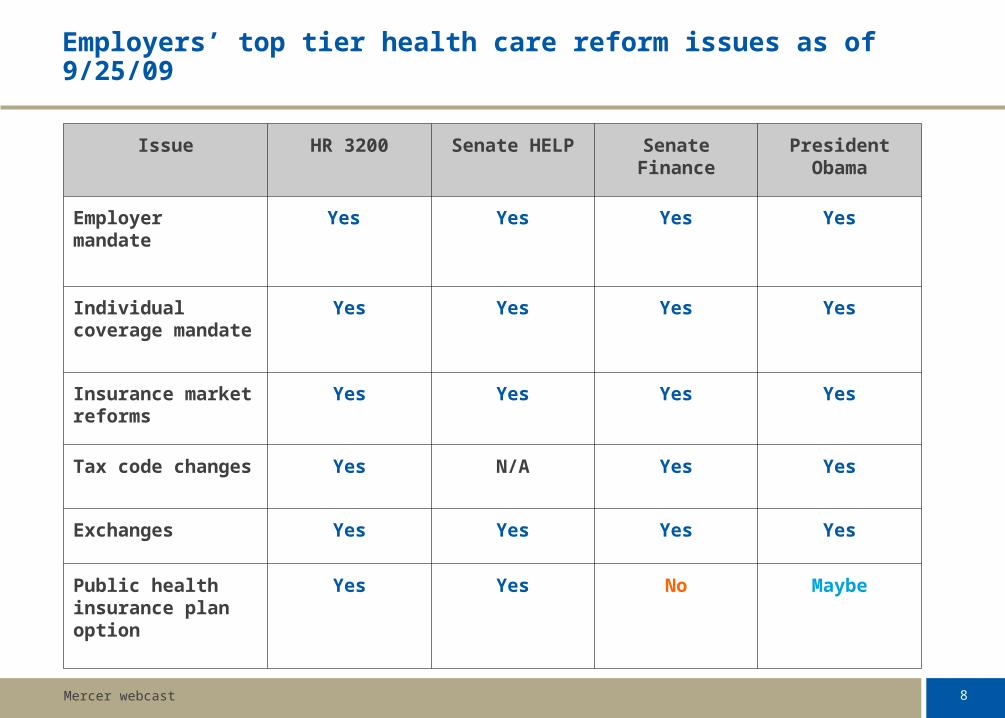
Employers’ top tier health care reform issues as of 9/25/09
Issue HR 3200 Senate HELP Senate Finance
President Obama
Employer mandate
Yes Yes Yes Yes
Individual coverage mandate
Yes Yes Yes Yes
Insurance market reforms
Yes Yes Yes Yes
Tax code changes
Yes N/A Yes Yes
Exchanges Yes Yes Yes Yes
Public health insurance plan option
Yes Yes No Maybe
Potential impact on employers
10Mercer webcast
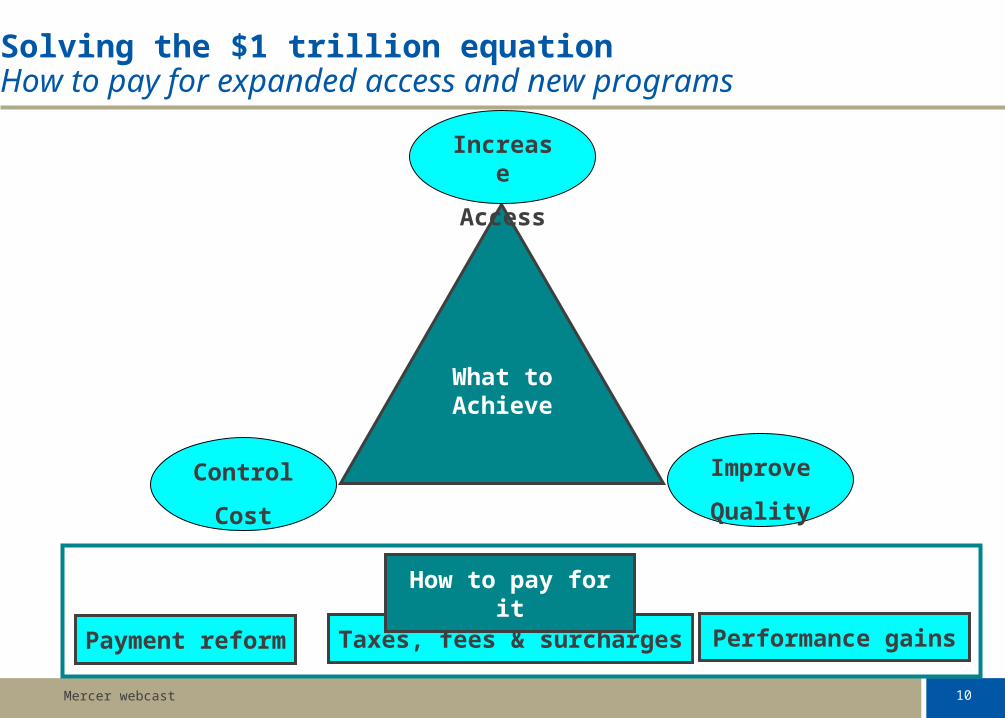
Solving the $1 trillion equationHow to pay for expanded access and new programs
Control
Cost
Increase
Access
Improve
Quality
Payment reform Performance gainsTaxes, fees & surcharges
What to Achieve
How to pay for it
11Mercer webcast
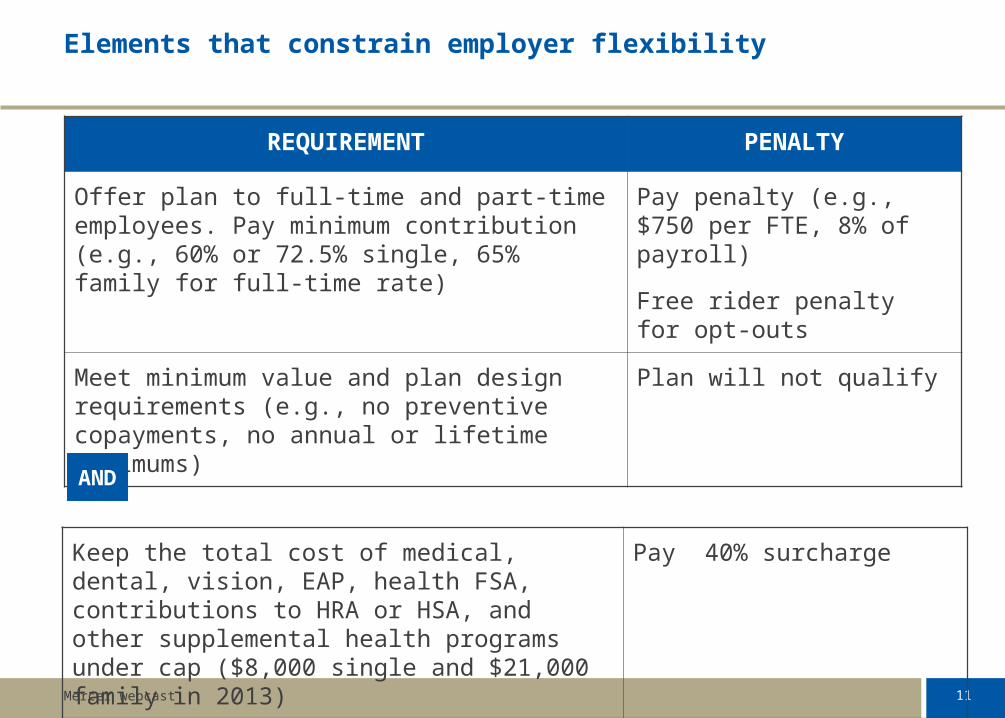
Elements that constrain employer flexibility
REQUIREMENT PENALTY
Offer plan to full-time and part-time employees. Pay minimum contribution (e.g., 60% or 72.5% single, 65% family for full-time rate)
Pay penalty (e.g., $750 per FTE, 8% of payroll)
Free rider penalty for opt-outs
Meet minimum value and plan design requirements (e.g., no preventive copayments, no annual or lifetime maximums)
Plan will not qualify
Keep the total cost of medical, dental, vision, EAP, health FSA, contributions to HRA or HSA, and other supplemental health programs under cap ($8,000 single and $21,000 family in 2013)
Pay 40% surcharge
AND
12Mercer webcast
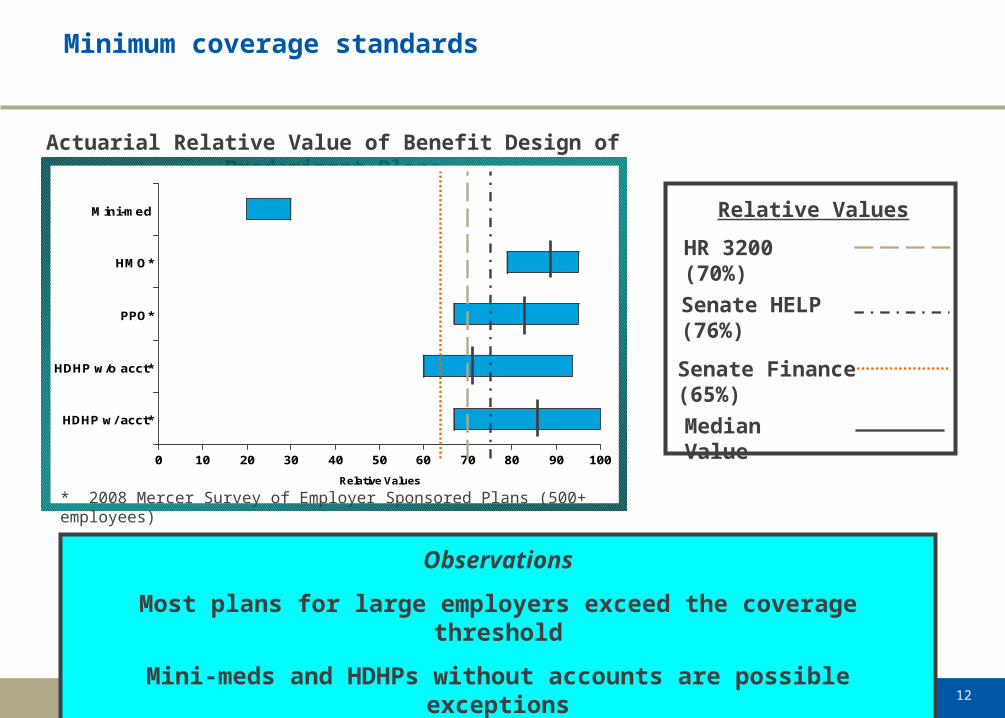
Minimum coverage standards
Actuarial Relative Value of Benefit Design of Predominant Plans
0 10 20 30 40 50 60 70 80 90 100
Relative Values
HDHP w/ acct*
HDHP w/o acct*
PPO*
HMO*
Mini-med
* 2008 Mercer Survey of Employer Sponsored Plans (500+ employees)
HR 3200 (70%)
Median Value
Senate HELP (76%)
Senate Finance
(65%)
Relative Values
Observations
Most plans for large employers exceed the coverage threshold
Mini-meds and HDHPs without accounts are possible exceptions
13Mercer webcast
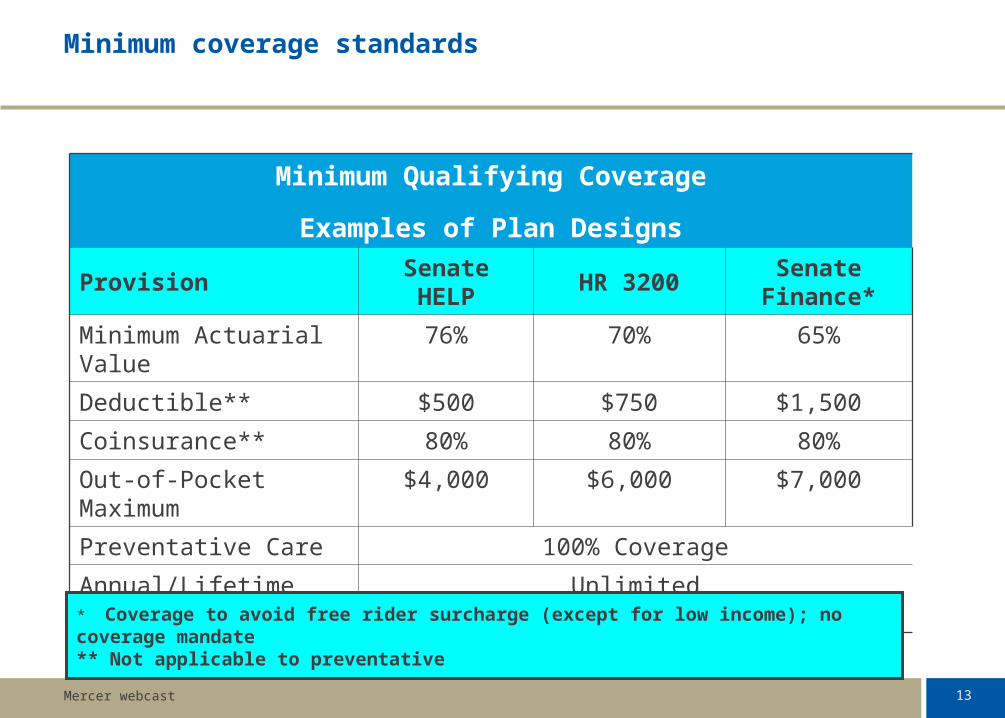
Minimum coverage standards
Minimum Qualifying Coverage
Examples of Plan Designs
Provision Senate HELP HR 3200Senate
Finance*
Minimum Actuarial Value 76% 70% 65%
Deductible** $500 $750 $1,500
Coinsurance** 80% 80% 80%
Out-of-Pocket Maximum $4,000 $6,000 $7,000
Preventative Care 100% Coverage
Annual/Lifetime Maximum
Unlimited
* Coverage to avoid free rider surcharge (except for low income); no coverage mandate** Not applicable to preventative
14Mercer webcast
Impact of the surcharge
Initially, Congress appeared concerned about supplemental “executive” benefits, but now the focus is on high-cost plans– Potential 40% surcharge on high-cost plans (e.g., over $8,000 single and
$21,000 family by 2013)
High-cost plans are not just a function of generous plan design– Influencing factors: population characteristics, experience, location,
mandates, collectively bargained benefits– Proposal recognizes some factors by increasing thresholds for pre-65
retirees, workers in high-risk industries, some high-cost locations
25% of all employers will be subject to a surcharge in 2013 if trend continues at current pace
High-cost plans are not “gold plated” plans for executives – Average salary of employers offering a high-cost plan: $42,504– Average salary for employers who do not have a high-cost plan: $41,926
15Mercer webcast
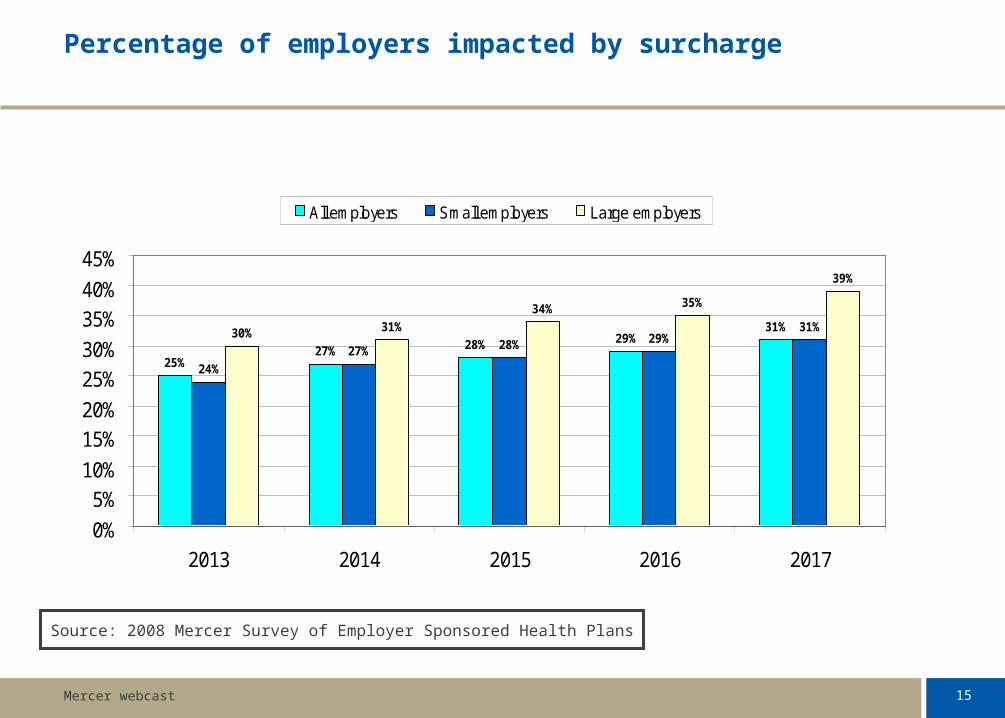
Percentage of employers impacted by surcharge
25%27% 28% 29%
31%
24%
27% 28% 29%31%30% 31%
34% 35%
39%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
2013 2014 2015 2016 2017
All employers Small employers Large employers
Source: 2008 Mercer Survey of Employer Sponsored Health Plans
16Mercer webcast
Impact of the surcharge
The surcharge could be a powerful change agent to improve quality, cost efficiency and patient compliance – Would require significant changes to current approach– Achieves fundamental goal of reform
OR, it could be a tipping point that drives employers to drop coverage– Provide benefit allowance– Sponsor third-party “direct-to-consumer” service that packages
health, financial security and personal services
17Mercer webcast
Maintain the Status quo or consider Plan B?
Restructure overall benefit program and redistribute “excess” cost to compensation, voluntary benefits, retirement savings, work/life– Implement core medical plan that meets minimum actuarial value– Shift dental, vision and supplemental health coverages to voluntary– Put preventive dental in core medical– Restructure behavioral health to include health aspects of EAP and
change remaining EAP benefits to a work/life program
Develop lean health care programs focused on delivery excellence– Tight, quality-driven networks (e.g., domestic tourism, medical
homes)– Create narrow pharmacy benefit based on outcomes and cost
efficiency– Strengthen design incentives for consumer behavior change and
compliance
18Mercer webcast
Parting thoughts
The overall debate will continue to be intense for the next month– The employer’s role is an essential part of the debate on how to
expand access, control cost and improve quality– Employers are at risk for being seen as a direct and indirect source
of revenue to fund reform
Our goal is to help employers– Be well informed about potential elements, risks and opportunities– Take action, if desired, in communicating concerns to legislators– Make smart short-term decisions for 2010 and 2011 – Begin thinking about longer-term impact
Benefits HR strategy Organization cost

www.mercer.com
Recommended

















